
Extension of Collagen Deposition in COVID-19 Post Mortem Lung Samples and Computed Tomography Analysis Findings

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patients and Samples Inclusion
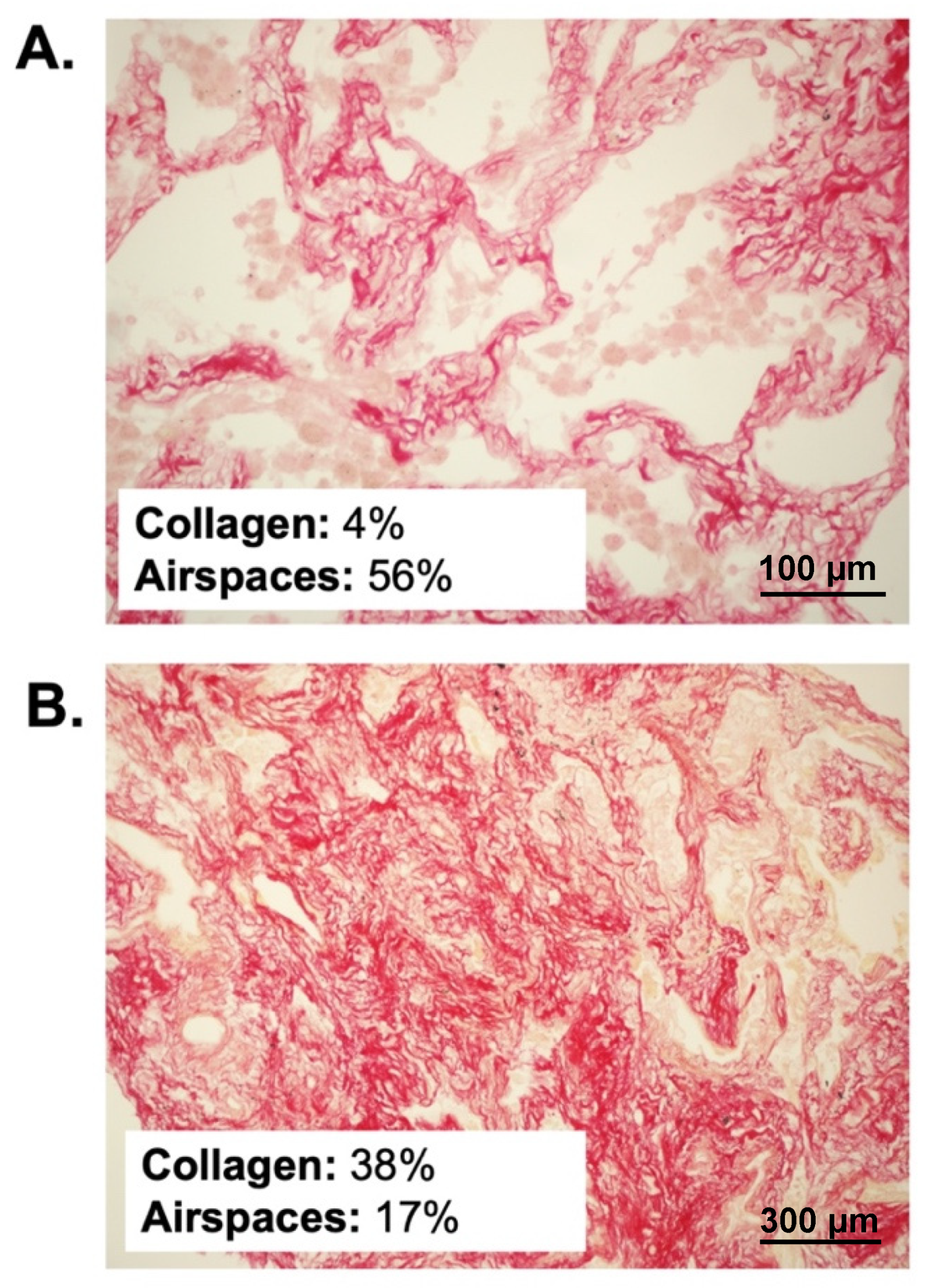
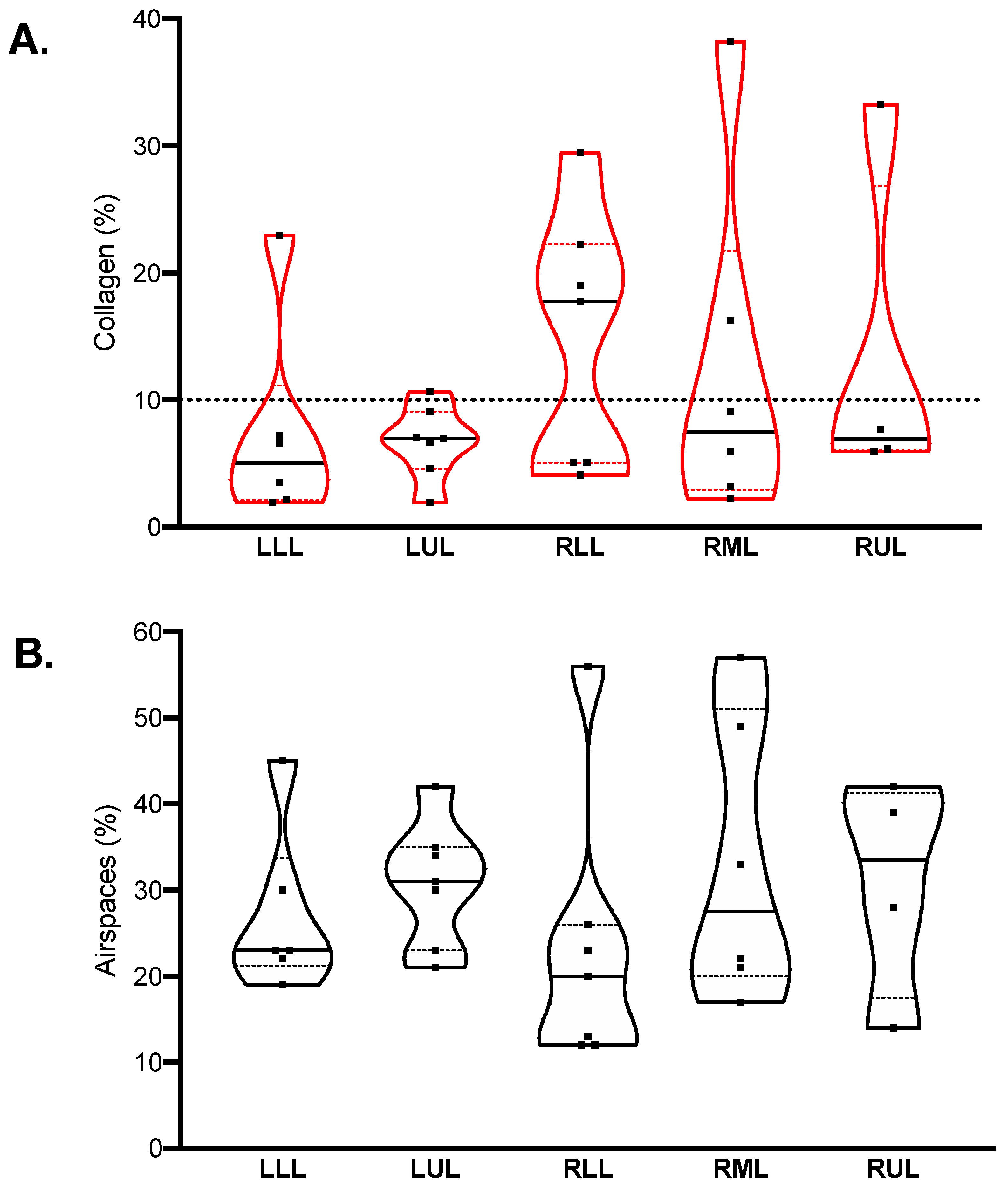
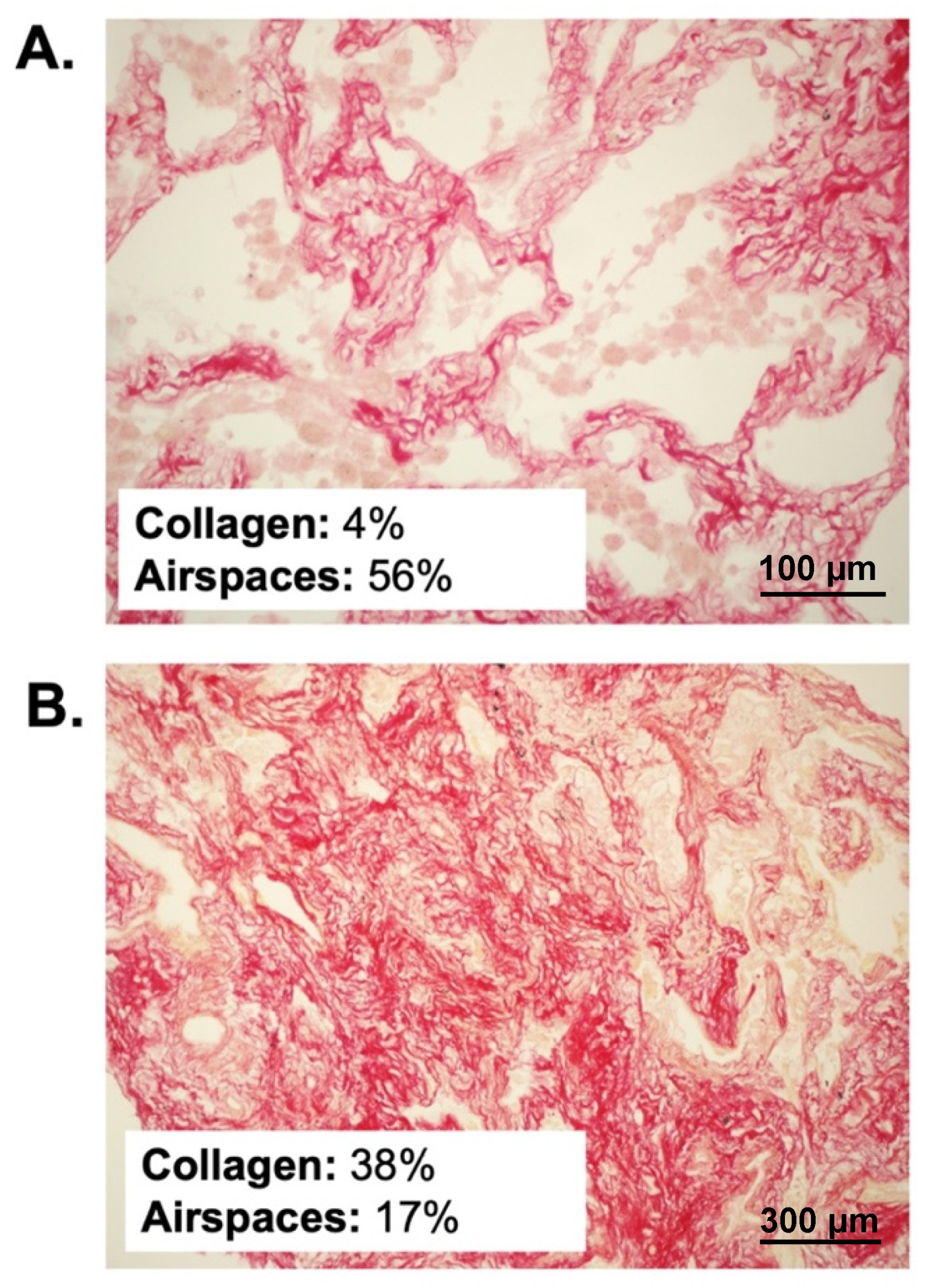
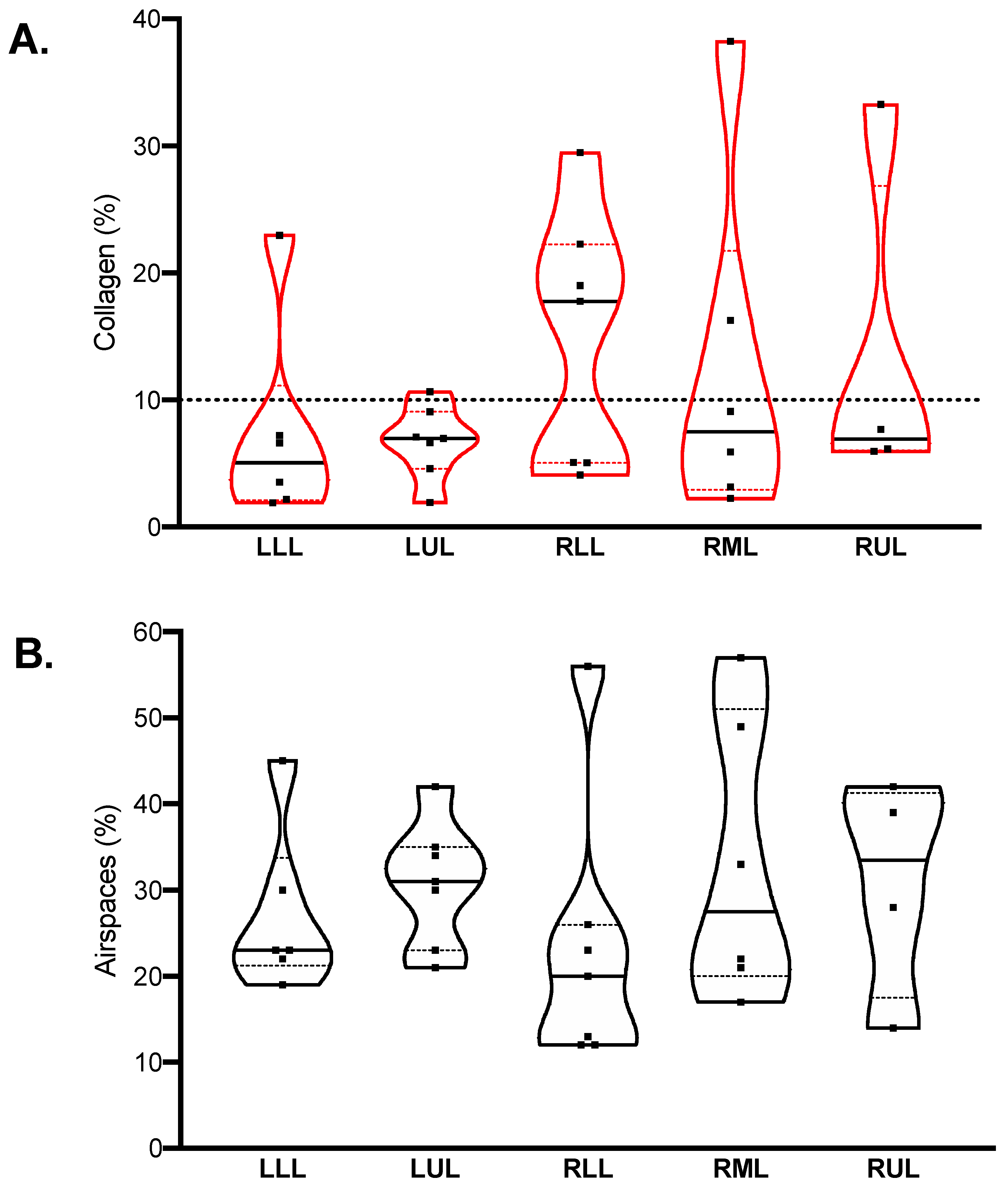
2.2. Quantitative Histopathological Analysis
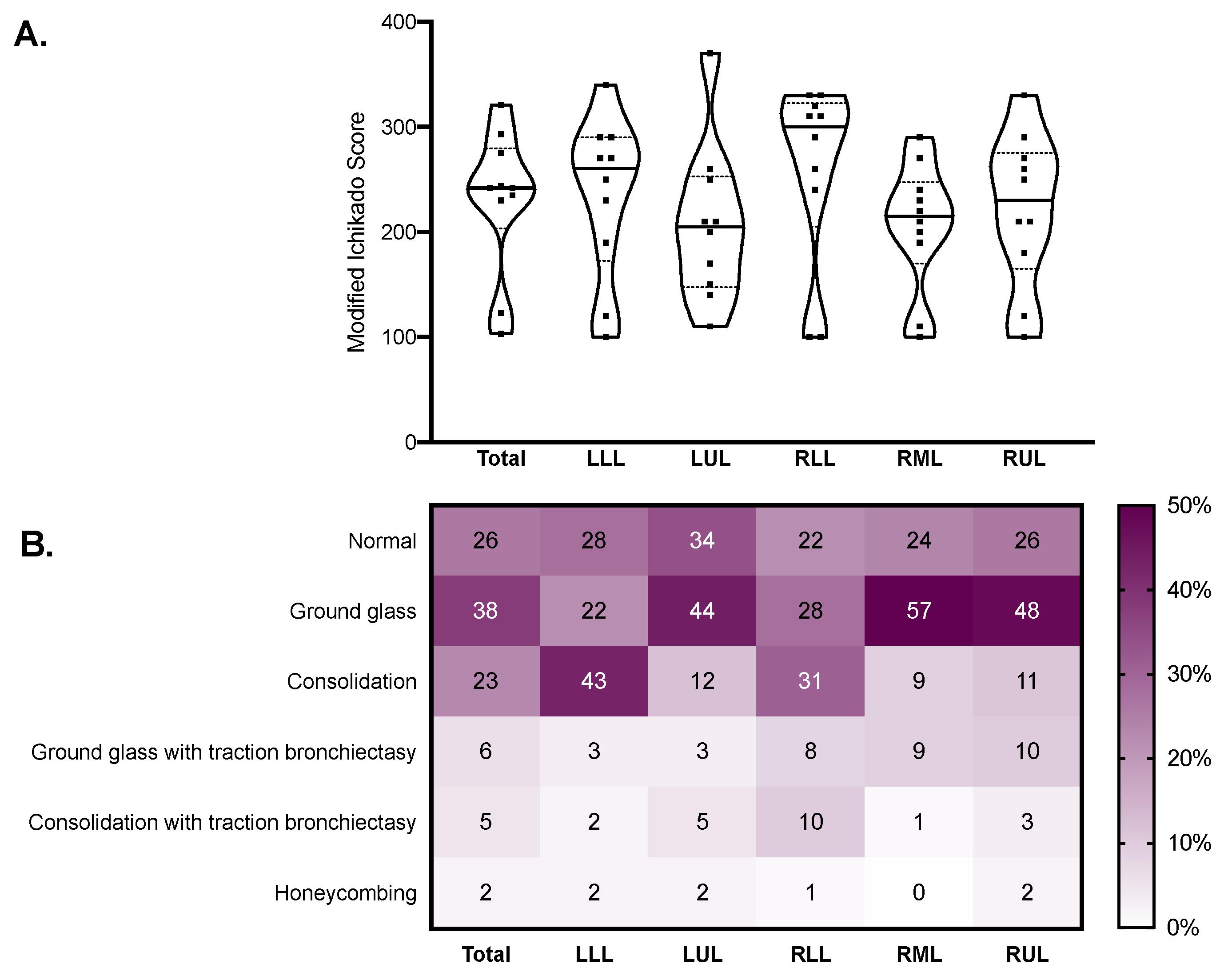
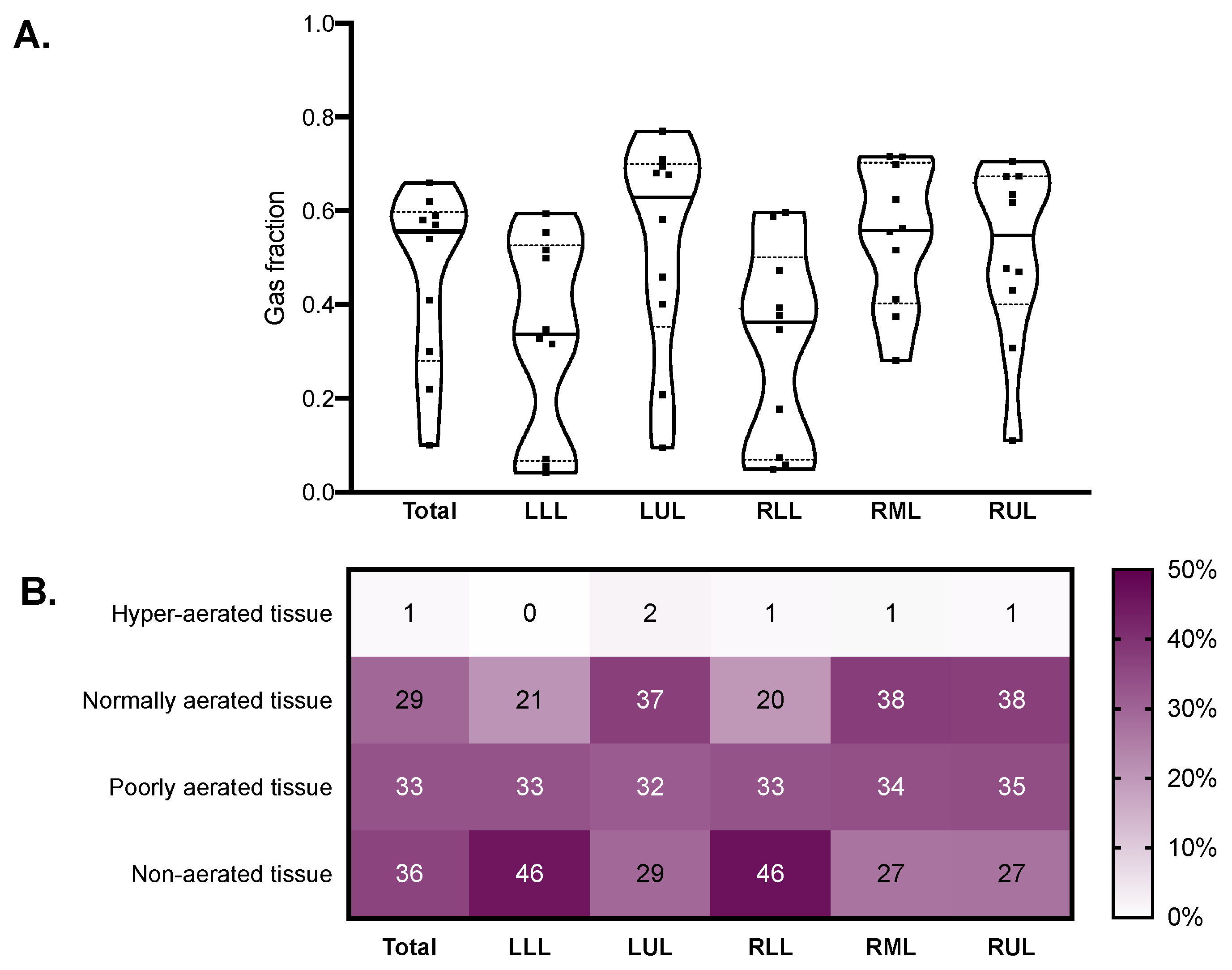
2.3. Qualitative CT Assessment and Quantitative CT Analysis
2.4. Receiver Operating Characteristics Analysis
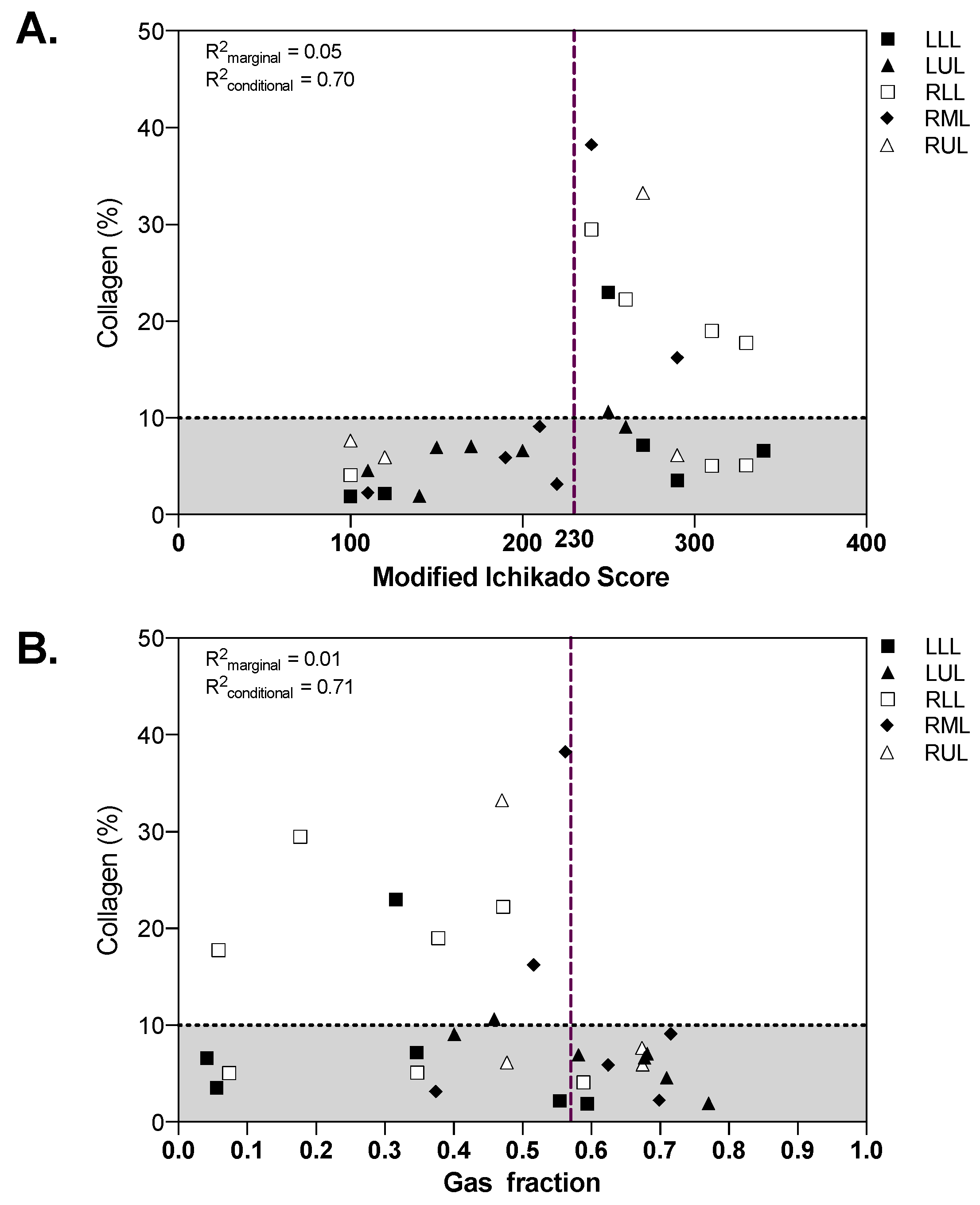
2.5. Associations between Qualitative and Quantitative CT Analysis and Histopathology
3. Discussion
4. Methods
4.1. Postmortem Sampling Procedure
4.2. Histologic Analysis and Quantification of Collagen Deposition and Aeration on Lung Samples
4.3. Computed Tomography Acquisition and Segmentation
4.4. Computed Tomography Qualitative Assessment
4.5. Computed Tomography Quantitative Analysis
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet Lond. Engl. 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef] [PubMed]
- Chiumello, D.; Busana, M.; Coppola, S.; Romitti, F.; Formenti, P.; Bonifazi, M.; Pozzi, T.; Palumbo, M.M.; Cressoni, M.; Herrmann, P.; et al. Physiological and Quantitative CT-Scan Characterization of COVID-19 and Typical ARDS: A Matched Cohort Study. Intensive Care Med. 2020. [Google Scholar] [CrossRef]
- Robba, C.; Battaglini, D.; Ball, L.; Patroniti, N.; Loconte, M.; Brunetti, I.; Vena, A.; Giacobbe, D.R.; Bassetti, M.; Rocco, P.R.M.; et al. Distinct Phenotypes Require Distinct Respiratory Management Strategies in Severe COVID-19. Respir. Physiol. Neurobiol. 2020, 279, 103455. [Google Scholar] [CrossRef]
- Grillo, F.; Barisione, E.; Ball, L.; Mastracci, L.; Fiocca, R. Lung Fibrosis: An Undervalued Finding in COVID-19 Pathological Series. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Tonelli, R.; Marchioni, A.; Tabbì, L.; Fantini, R.; Busani, S.; Castaniere, I.; Andrisani, D.; Gozzi, F.; Bruzzi, G.; Manicardi, L.; et al. Spontaneous Breathing and Evolving Phenotypes of Lung Damage in Patients with COVID-19: Review of Current Evidence and Forecast of a New Scenario. J. Clin. Med. 2021, 10, 975. [Google Scholar] [CrossRef]
- Bösmüller, H.; Matter, M.; Fend, F.; Tzankov, A. The Pulmonary Pathology of COVID-19. Virchows Arch. Int. J. Pathol. 2021, 478, 137–150. [Google Scholar] [CrossRef]
- Konopka, K.E.; Nguyen, T.; Jentzen, J.M.; Rayes, O.; Schmidt, C.J.; Wilson, A.M.; Farver, C.F.; Myers, J.L. Diffuse Alveolar Damage (DAD) Resulting from Coronavirus Disease 2019 Infection Is Morphologically Indistinguishable from Other Causes of DAD. Histopathology 2020, 77, 570–578. [Google Scholar] [CrossRef]
- Barisione, E.; Grillo, F.; Ball, L.; Bianchi, R.; Grosso, M.; Morbini, P.; Pelosi, P.; Patroniti, N.A.; De Lucia, A.; Orengo, G.; et al. Fibrotic Progression and Radiologic Correlation in Matched Lung Samples from COVID-19 Post-Mortems. Virchows Arch. Int. J. Pathol. 2021, 478, 471–485. [Google Scholar] [CrossRef]
- Oldani, S.; Ravaglia, C.; Bensai, S.; Bertolovic, L.; Ghirotti, C.; Puglisi, S.; Martinello, S.; Sultani, F.; Colinelli, C.; Piciucchi, S.; et al. Pathophysiology of Light Phenotype SARS-CoV-2 Interstitial Pneumonia: From Histopathological Features to Clinical Presentations. Pulmonology 2021. [Google Scholar] [CrossRef] [PubMed]
- Doglioni, C.; Ravaglia, C.; Chilosi, M.; Rossi, G.; Dubini, A.; Pedica, F.; Piciucchi, S.; Vizzuso, A.; Stella, F.; Maitan, S.; et al. COVID-19 Interstitial Pneumonia: Histological and Immunohistochemical Features on Cryobiopsies. Respir. Int. Rev. Thorac. Dis. 2021, 1–11. [Google Scholar] [CrossRef]
- Ball, L.; Vercesi, V.; Costantino, F.; Chandrapatham, K.; Pelosi, P. Lung Imaging: How to Get Better Look inside the Lung. Ann. Transl. Med. 2017, 5, 294. [Google Scholar] [CrossRef] [Green Version]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-Associated Acute Respiratory Distress Syndrome: A Multicentre Prospective Observational Study. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Inui, S.; Fujikawa, A.; Jitsu, M.; Kunishima, N.; Watanabe, S.; Suzuki, Y.; Umeda, S.; Uwabe, Y. Chest CT Findings in Cases from the Cruise Ship “Diamond Princess” with Coronavirus Disease 2019 (COVID-19). Radiol. Cardiothorac. Imaging 2020, 2, e200110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-Month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiology 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Madri, J.; Furthmayr, H. Collagen Polymorphism in the LungAn Immunochemical Study of Pulmonary Fibrosis. Hum. Pathol. 1980, 11, 353–366. [Google Scholar] [CrossRef]
- Ichikado, K.; Suga, M.; Muranaka, H.; Gushima, Y.; Miyakawa, H.; Tsubamoto, M.; Johkoh, T.; Hirata, N.; Yoshinaga, T.; Kinoshita, Y.; et al. Prediction of Prognosis for Acute Respiratory Distress Syndrome with Thin-Section CT: Validation in 44 Cases. Radiology 2006, 238, 321–329. [Google Scholar] [CrossRef]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal Pulmonary Function in COVID-19 Patients at Time of Hospital Discharge. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef]
- González, J.; Benítez, I.D.; Carmona, P.; Santisteve, S.; Monge, A.; Moncusí-Moix, A.; Gort-Paniello, C.; Pinilla, L.; Carratalá, A.; Zuil, M.; et al. Pulmonary Function and Radiological Features in Survivors of Critical COVID-19: A 3-Month Prospective Cohort. Chest 2021. [Google Scholar] [CrossRef] [PubMed]
- Truffaut, L.; Demey, L.; Bruyneel, A.V.; Roman, A.; Alard, S.; De Vos, N.; Bruyneel, M. Post-Discharge Critical COVID-19 Lung Function Related to Severity of Radiologic Lung Involvement at Admission. Respir. Res. 2021, 22, 29. [Google Scholar] [CrossRef] [PubMed]
- Burnham, E.L.; Janssen, W.J.; Riches, D.W.H.; Moss, M.; Downey, G.P. The Fibroproliferative Response in Acute Respiratory Distress Syndrome: Mechanisms and Clinical Significance. Eur. Respir. J. 2014, 43, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchioni, A.; Tonelli, R.; Ball, L.; Fantini, R.; Castaniere, I.; Cerri, S.; Luppi, F.; Malerba, M.; Pelosi, P.; Clini, E. Acute Exacerbation of Idiopathic Pulmonary Fibrosis: Lessons Learned from Acute Respiratory Distress Syndrome? Crit. Care Lond. Engl. 2018, 22, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchioni, A.; Tonelli, R.; Rossi, G.; Spagnolo, P.; Luppi, F.; Cerri, S.; Cocconcelli, E.; Pellegrino, M.R.; Fantini, R.; Tabbì, L.; et al. Ventilatory Support and Mechanical Properties of the Fibrotic Lung Acting as a “Squishy Ball”. Ann. Intensive Care 2020, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Liu, Y.; Xiao, Y.; Tian, Q.; Fan, B.; Zhao, H.; Chen, W. Follow-up Study on Pulmonary Function and Lung Radiographic Changes in Rehabilitating Severe Acute Respiratory Syndrome Patients After Discharge. Chest 2005, 127, 2119–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; Li, J.; Liu, H.; Han, N.; Ju, J.; Kou, Y.; Chen, L.; Jiang, M.; Pan, F.; Zheng, Y.; et al. Long-Term Bone and Lung Consequences Associated with Hospital-Acquired Severe Acute Respiratory Syndrome: A 15-Year Follow-up from a Prospective Cohort Study. Bone Res. 2020, 8, 8. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.W.; Fidler, L.; Marcoux, V.; Johannson, K.A.; Assayag, D.; Fisher, J.H.; Hambly, N.; Kolb, M.; Morisset, J.; Shapera, S.; et al. Practical Considerations for the Diagnosis and Treatment of Fibrotic Interstitial Lung Disease During the Coronavirus Disease 2019 Pandemic. Chest 2020, 158, 1069–1078. [Google Scholar] [CrossRef]
- Protti, A.; Iapichino, G.E.; Milesi, M.; Melis, V.; Pugni, P.; Comini, B.; Cressoni, M.; Gattinoni, L. Validation of Computed Tomography for Measuring Lung Weight. Intensive Care Med. Exp. 2014, 2, 31. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, S.; Natt, B.; Bime, C.; Knox, K.S.; Glassberg, M.K. Antifibrotics in COVID-19 Lung Disease: Let Us Stay Focused. Front. Med. 2020, 7, 539. [Google Scholar] [CrossRef]
- Wu, X.; Liu, X.; Zhou, Y.; Yu, H.; Li, R.; Zhan, Q.; Ni, F.; Fang, S.; Lu, Y.; Ding, X.; et al. 3-Month, 6-Month, 9-Month, and 12-Month Respiratory Outcomes in Patients Following COVID-19-Related Hospitalisation: A Prospective Study. Lancet Respir. Med. 2021. [Google Scholar] [CrossRef]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem Examination of COVID-19 Patients Reveals Diffuse Alveolar Damage with Severe Capillary Congestion and Variegated Findings in Lungs and Other Organs Suggesting Vascular Dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Schaller, T.; Hirschbühl, K.; Burkhardt, K.; Braun, G.; Trepel, M.; Märkl, B.; Claus, R. Postmortem Examination of Patients With COVID-19. JAMA 2020. [Google Scholar] [CrossRef]
- Calvaruso, V.; Burroughs, A.K.; Standish, R.; Manousou, P.; Grillo, F.; Leandro, G.; Maimone, S.; Pleguezuelo, M.; Xirouchakis, I.; Piero Guerrini, G.; et al. Computer-Assisted Image Analysis of Liver Collagen: Relationship to Ishak Scoring and Hepatic Venous Pressure Gradient. Hepatology 2009, 49, 1236–1244. [Google Scholar] [CrossRef] [PubMed]
- Calvaruso, V.; Dhillon, A.P.; Tsochatzis, E.; Manousou, P.; Grillo, F.; Germani, G.; Patch, D.; O’Beirne, J.; Burroughs, A.K. Liver Collagen Proportionate Area Predicts Decompensation in Patients with Recurrent Hepatitis C Virus Cirrhosis after Liver Transplantation: Collagen Proportionate Area and Liver Decompensation. J. Gastroenterol. Hepatol. 2012, 27, 1227–1232. [Google Scholar] [CrossRef]
- Mehrad, M.; Colby, T.V.; Rossi, G.; Cavazza, A. Transbronchial Cryobiopsy in the Diagnosis of Fibrotic Interstitial Lung Disease. Arch. Pathol. Lab. Med. 2020, 144, 1501–1508. [Google Scholar] [CrossRef] [Green Version]
- Ruifrok, A.C.; Johnston, D.A. Quantification of Histochemical Staining by Color Deconvolution. Anal. Quant. Cytol. Histol. 2001, 23, 291–299. [Google Scholar]
- Ichikado, K.; Johkoh, T.; Ikezoe, J.; Takeuchi, N.; Kohno, N.; Arisawa, J.; Nakamura, H.; Nagareda, T.; Itoh, H.; Ando, M. Acute Interstitial Pneumonia: High-Resolution CT Findings Correlated with Pathology. AJR Am. J. Roentgenol. 1997, 168, 333–338. [Google Scholar] [CrossRef] [Green Version]
- Ichikado, K.; Suga, M.; Müller, N.L.; Taniguchi, H.; Kondoh, Y.; Akira, M.; Johkoh, T.; Mihara, N.; Nakamura, H.; Takahashi, M.; et al. Acute Interstitial Pneumonia: Comparison of High-Resolution Computed Tomography Findings between Survivors and Nonsurvivors. Am. J. Respir. Crit. Care Med. 2002, 165, 1551–1556. [Google Scholar] [CrossRef]
- Ball, L.; Brusasco, C.; Corradi, F.; Paparo, F.; Garlaschi, A.; Herrmann, P.; Quintel, M.; Pelosi, P. Lung Hyperaeration Assessment by Computed Tomography: Correction of Reconstruction-Induced Bias. BMC Anesthesiol. 2016, 16, 67. [Google Scholar] [CrossRef] [Green Version]
- Genders, T.S.S.; Spronk, S.; Stijnen, T.; Steyerberg, E.W.; Lesaffre, E.; Hunink, M.G.M. Methods for Calculating Sensitivity and Specificity of Clustered Data: A Tutorial. Radiology 2012, 265, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Schielzeth, H. A General and Simple Method for Obtaining R2 from Generalized Linear Mixed-Effects Models. Methods Ecol. Evol. 2013, 4, 133–142. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population (n = 10) | |
|---|---|
| General characteristics | |
| Age, median (IQR) | 72 (60–77) |
| Sex (male), n (%) | 7 (70) |
| Time from onset of symptoms to ICU admission, median (IQR), days | 11 (8–16) |
| Time from hospital admission to ICU admission, median (IQR), days | 9 (3–13) |
| Time from ICU admission to death, median (IQR), days | 17 (10–27) |
| Time from last CT scan to death, median (IQR), days | 4 (3–4) |
| Comorbidities | |
| Hypertension, n (%) | 6 (60) |
| Diabetes, n (%) | 1 (10) |
| Smoker, n (%) | 2 (20) |
| Ischemic cardiopathy, n (%) | 1 (10) |
| Specific treatments received | |
| Methylprednisolone, n (%) | 9 (90) |
| Tocilizumab, n (%) | 3 (30) |
| Hydroxychloroquine, n (%) | 8 (80) |
| Leading cause of death | |
| Refractory hypoxemia, n (%) | 7 (70) |
| Cardiocirculatory failure, n (%) | 3 (30) |
| Oxygenation | |
| PaO2/FiO2 ratio at ICU admission, median (IQR), mmHg | 173 (112–310) |
| PaO2/FiO2 ratio the day of death, median (IQR), mmHg | 77 (55–99) |
| Variable | Total | Left Lower Lobe | Left Upper Lobe | Right Lower Lobe | Right Middle Lobe | Right Upper Lobe |
|---|---|---|---|---|---|---|
| Volume (mL), median (IQR) | 2682 (2131–3554) | 410 (395–641) | 708 (518–1048) | 504 (468–594) | 269 (238–395) | 679 (503–892) |
| Attenuation (HU), median (IQR) | −555 (−595–−301) | −337 (−517–−71) | −629 (−696–−401) | −362 (−472–−73) | −559 (−699–−412) | −547 (−674–−431) |
| Weight (g), median (IQR) | 1460 (1239–1917) | 301 (260–376) | 336 (305–375) | 355 (285–510) | 139 (115–167) | 304 (263–419) |
| Vgas (mL), median (IQR) | 1389 (701–2278) | 132 (29–323) | 414 (225–744) | 176 (34–218) | 148 (102–263) | 374 (236–538) |
| Gas Fraction, median (IQR) | 0.56 (0.30–0.59) | 0.34 (0.07–0.52) | 0.63 (0.40–0.70) | 0.36 (0.07–0.47) | 0.56 (0.41–0.70) | 0.55 (0.43–0.67) |
| Hyperaerated tissue (%), median (IQR) | 0.6 (0.2–1.3) | 0.2 (0.1–0.3) | 1.1 (0.2–2.4) | 0.1 (0.1–0.4) | 0.7 (0.3–1.5) | 0.6 (0.2–1.1) |
| Normally aerated tissue (%), median (IQR) | 28.7 (12.6–49.6) | 14.1 (4.1–40.3) | 43.1 (20.7–53.0) | 16.4 (2.4–36.3) | 41.3 (17.2–57.5) | 37.8 (19.4–60.4) |
| Poorly aerated tissue (%), median (IQR) | 33.7 (30.6–36.0) | 31.4 (28.8–37.0) | 32.1 (26.2–35.4) | 29.4 (27.6–37.3) | 34.5 (28.8–40.7) | 33.6 (31.0–40.2) |
| Nonaerated tissue (%), median (IQR) | 34.2 (16.3–53.8) | 49.4 (23.2–69.4) | 25.4 (13.3–41.0) | 47.2 (26.0–70.3) | 24.0 (14.2–41.5) | 22.9 (11.7–45.7) |
| Parameter | AUC (95% CI) | Cut-Off | Sensitivity, % (95% CI) | Specificity, % (95% CI) | |||
|---|---|---|---|---|---|---|---|
| Qualitative Analysis | |||||||
| Normal lung (estimated %) | 0.742 | (0.567–0.919) | <25 | 100 | (66.4–100) | 47.6 | (10.4–84.8) |
| Ground glass opacities (estimated %) | 0.648 | (0.451–0.845) | >25 | 77.8 | (45.1–100) | 52.4 | (22.0–82.7) |
| Consolidation (estimated %) | 0.685 | (0.496–0.875) | >5 | 100.0 | (66.4–100) | 42.9 | (10.1–75.6) |
| Ground glass with traction bronchiectasis (estimated %) | 0.688 | (0.461–0.915) | >5 | 55.6 | (29.5–81.6) | 76.2 | (55.5–96.9) |
| Consolidation with traction bronchiectasis (estimated %) | 0.521 | (0.288–0.754) | >15 | 11.1 | (0.0–33.6) | 95.2 | (87.0–100) |
| Honeycombing (estimated %) | 0.563 | (0.329–0.798) | >5 | 22.2 | (0.0–51.5) | 90.5 | (74.0–100) |
| Modified Ichikado score | 0.746 | (0.572–0.920) | >230 | 100.0 | (66.4–100) | 66.7 | (41.0–92.3) |
| Lobe weight (g) | 0.624 | (0.389–0.859) | >263 | 77.8 | (62.9–92.7) | 52.4 | (32.4–72.3) |
| Gas fraction | 0.725 | (0.547–0.903) | <0.57 | 100.0 | (66.4–100) | 57.1 | (26.3–88.0) |
| Hyperaerated tissue (%) | 0.762 | (0.584–0.940) | <0.2 | 77.8 | (57.0–98.6) | 81.0 | (62.3–99.6) |
| Normally aerated tissue (%) | 0.667 | (0.465–0.868) | <40 | 88.9 | (68.9–100) | 61.9 | (29.5–94.3) |
| Poorly aerated tissue (%) | 0.661 | (0.432–0.891) | >41 | 44.4 | (25.4–63.5) | 95.2 | (86.5–100) |
| Nonaerated tissue (%) | 0.593 | (0.356–0.829) | >24 | 77.8 | (37.9–100) | 57.1 | (24.0–90.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ball, L.; Barisione, E.; Mastracci, L.; Campora, M.; Costa, D.; Robba, C.; Battaglini, D.; Micali, M.; Costantino, F.; Cittadini, G.; et al. Extension of Collagen Deposition in COVID-19 Post Mortem Lung Samples and Computed Tomography Analysis Findings. Int. J. Mol. Sci. 2021, 22, 7498. https://doi.org/10.3390/ijms22147498
Ball L, Barisione E, Mastracci L, Campora M, Costa D, Robba C, Battaglini D, Micali M, Costantino F, Cittadini G, et al. Extension of Collagen Deposition in COVID-19 Post Mortem Lung Samples and Computed Tomography Analysis Findings. International Journal of Molecular Sciences. 2021; 22(14):7498. https://doi.org/10.3390/ijms22147498
Chicago/Turabian StyleBall, Lorenzo, Emanuela Barisione, Luca Mastracci, Michela Campora, Delfina Costa, Chiara Robba, Denise Battaglini, Marco Micali, Federico Costantino, Giuseppe Cittadini, and et al. 2021. "Extension of Collagen Deposition in COVID-19 Post Mortem Lung Samples and Computed Tomography Analysis Findings" International Journal of Molecular Sciences 22, no. 14: 7498. https://doi.org/10.3390/ijms22147498
APA StyleBall, L., Barisione, E., Mastracci, L., Campora, M., Costa, D., Robba, C., Battaglini, D., Micali, M., Costantino, F., Cittadini, G., Patroniti, N., Pelosi, P., Fiocca, R., & Grillo, F. (2021). Extension of Collagen Deposition in COVID-19 Post Mortem Lung Samples and Computed Tomography Analysis Findings. International Journal of Molecular Sciences, 22(14), 7498. https://doi.org/10.3390/ijms22147498