
Saliva Proteomics as Fluid Signature of Inflammatory and Immune-Mediated Skin Diseases

 , ,
, , 

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Identify the Research Question
2.2. Identify Relevant Studies
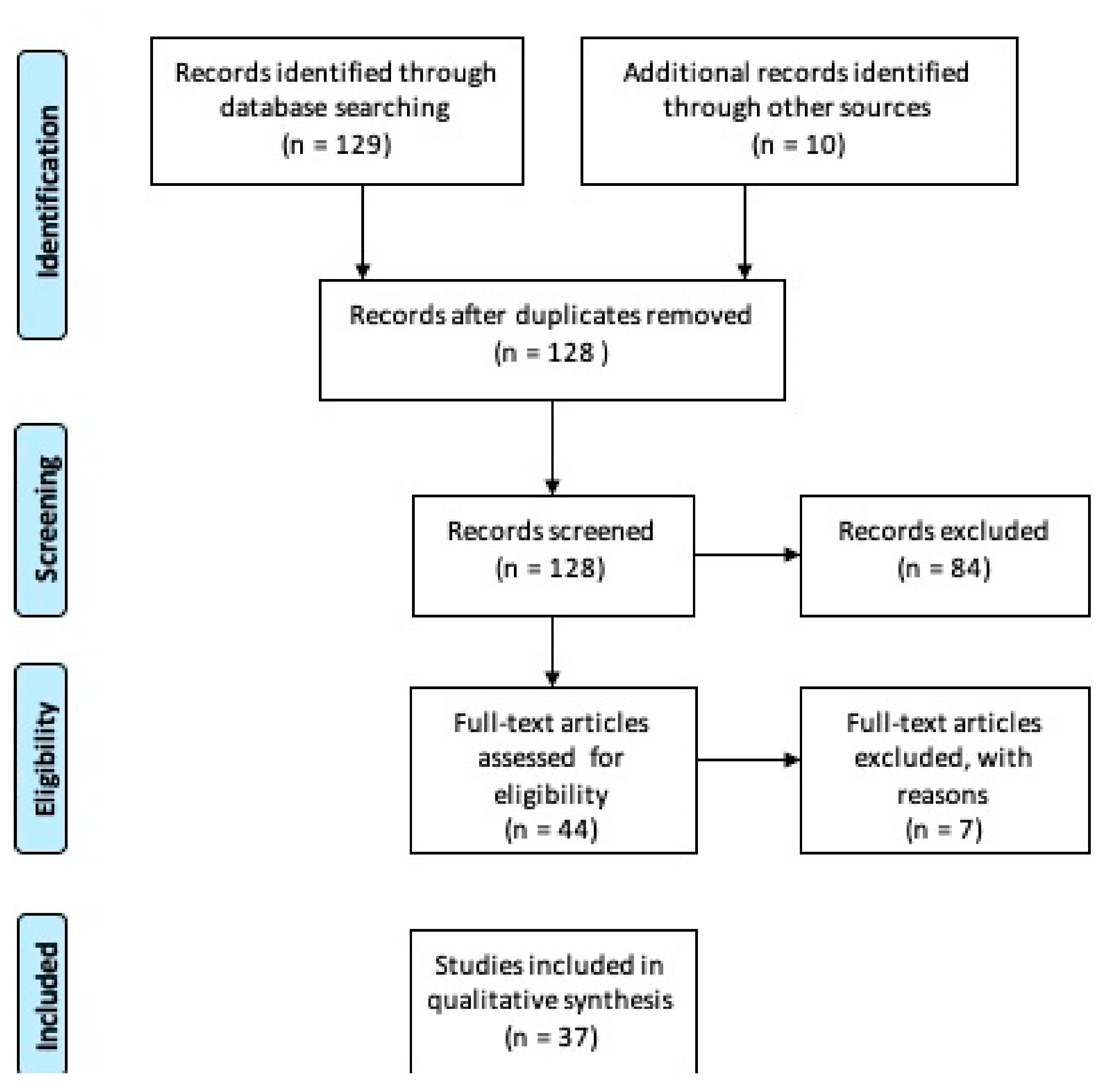
2.3. Study Selection
2.4. Data Extraction
3. Results
4. Discussion
- Psoriasis
- Atopic dermatitis
- Blistering diseases
- Lichen planus
- Vitiligo
4.1. Psoriasis
4.2. Oral Lichen Planus
4.3. Blistering Diseases
4.4. Vitiligo
4.5. Atopic Dermatitis
5. Conclusions
Funding
Conflicts of Interest
References
- Khurshid, Z.; Zafar, M.S.; Khan, R.S.; Najeeb, S.; Slowey, P.D.; Rehman, I.U. Role of Salivary Biomarkers in Oral Cancer Detection. Adv. Clin. Chem. 2018, 86, 23–70. [Google Scholar] [CrossRef] [PubMed]
- Bekes, K.; Mitulović, G.; Meißner, N.; Resch, U.; Gruber, R. Saliva proteomic patterns in patients with molar incisor hypomineralization. Sci. Rep. 2020, 10, 7560. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, W.L.; Dawes, C. The salivary proteome: Challenges and perspectives. Proteom. Clin. Appl. 2011, 5, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Vitorino, R.; Lobo, M.J.; Ferrer-Correira, A.J.; Dubin, J.R.; Tomer, K.B.; Domingues, P.M.; Amado, F.M. Identification of human whole saliva protein components using proteomics. Proteomics 2004, 4, 1109–1115. [Google Scholar] [CrossRef]
- Orti, V.; Mertens, B.; Vialaret, J.; Gibert, P.; Relaño-Ginés, A.; Lehmann, S.; Deville de Périère, D.; Hirtz, C. Data from a targeted proteomics approach to discover biomarkers in saliva for the clinical diagnosis of periodontitis. Data Brief. 2018, 18, 294–299. [Google Scholar] [CrossRef]
- Cabras, T.; Manconi, B.; Castagnola, M.; Sanna, M.T.; Arba, M.; Acharya, S.; Ekström, J.; Carlén, A.; Messana, I. Proteomics of the acid-soluble fraction of whole and major gland saliva in burning mouth syndrome patients. Arch. Oral Biol. 2019, 98, 148–155. [Google Scholar] [CrossRef]
- Katsiougiannis, S.; Wong, D.T. The Proteomics of Saliva in Sjögren’s Syndrome. Rheum. Dis. Clin. N. Am. 2016, 42, 449–456. [Google Scholar] [CrossRef]
- Rao, P.V.; Reddy, A.P.; Lu, X.; Dasari, S.; Krishnaprasad, A.; Biggs, E.; Roberts, C.T.; Nagalla, S.R. Proteomic identification of salivary biomarkers of type-2 diabetes. J. Proteome Res. 2009, 8, 239–245. [Google Scholar] [CrossRef]
- Minarowski, Ł.; Sands, D.; Minarowska, A.; Karwowska, A.; Sulewska, A.; Gacko, M.; Chyczewska, E. Thiocyanate concentration in saliva of cystic fibrosis patients. Folia Histochem. Cytobiol. 2008, 46, 245–246. [Google Scholar] [CrossRef][Green Version]
- Ren, R.; Sun, Y.; Zhao, X.; Pu, X. Recent advances in biomarkers for Parkinson’s disease focusing on biochemicals, omics and neuroimaging. Clin. Chem. Lab. Med. 2015, 53, 1495–1506. [Google Scholar] [CrossRef]
- Manconi, B.; Liori, B.; Cabras, T.; Vincenzoni, F.; Iavarone, F.; Lorefice, L.; Cocco, E.; Castagnola, M.; Messana, I.; Olianas, A. Top-down proteomic profiling of human saliva in multiple sclerosis patients. J. Proteom. 2018, 187, 212–222. [Google Scholar] [CrossRef]
- Castagnola, M.; Scarano, E.; Passali, G.C.; Messana, I.; Cabras, T.; Iavarone, F.; Di Cintio, G.; Fiorita, A.; De Corso, E.; Paludetti, G. Salivary biomarkers and proteomics: Future diagnostic and clinical utilities. Acta Otorhinolaryngol. Ital. 2017, 37, 94–101. [Google Scholar] [CrossRef]
- Ai, J.; Smith, B.; Wong, D.T. Saliva Ontology: An ontology-based framework for a Salivaomics Knowledge Base. BMC Bioinform. 2010, 11, 302. [Google Scholar] [CrossRef]
- Rylander-Rudqvist, T.; Håkansson, N.; Tybring, G.; Wolk, A. Quality and Quantity of Saliva DNA Obtained from the Self-administrated Oragene Method—A Pilot Study on the Cohort of Swedish Men. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1742–1745. [Google Scholar] [CrossRef]
- Gaździcka, J.; Gołąbek, K.; Strzelczyk, J.K.; Ostrowska, Z. Epigenetic Modifications in Head and Neck Cancer. Biochem. Genet. 2019, 58, 213–244. [Google Scholar] [CrossRef]
- Esteves, C.V.; de Campos, W.G.; de Souza, M.M.; Lourenço, S.V.; Siqueira, W.L.; Lemos-Júnior, C.A. Diagnostic potential of saliva proteome analysis: A review and guide to clinical practice. Braz. Oral Res. 2019, 33, e043. [Google Scholar] [CrossRef]
- Kondo, T. Cancer biomarker development and two-dimensional difference gel electrophoresis (2D-DIGE). Biochim. Biophys. Acta Proteins Proteom. 2019, 1867, 2–8. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, X.; Di, Y.P. Fast and Efficient Measurement of Clinical and Biological Samples Using Immunoassay-Based Multiplexing Systems. In Molecular Toxicology Protocols; Keohavong, P., Singh, K.P., Gao, W., Eds.; Springer: New York, NY, USA, 2020; pp. 129–147. ISBN 978-1-0716-0223-2. [Google Scholar]
- Lin, A.V. Direct ELISA. In ELISA: Methods and Protocols; Hnasko, R., Ed.; Springer: New York, NY, USA, 2015; pp. 61–67. ISBN 978-1-4939-2742-5. [Google Scholar]
- Navazesh, M. Methods for Collecting Saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Khurshid, Z.; Zohaib, S.; Najeeb, S.; Zafar, M.S.; Slowey, P.D.; Almas, K. Human Saliva Collection Devices for Proteomics: An Update. Int. J. Mol. Sci. 2016, 17, 846. [Google Scholar] [CrossRef]
- Schipper, R.; Loof, A.; de Groot, J.; Harthoorn, L.; Dransfield, E.; van Heerde, W. SELDI-TOF-MS of saliva: Methodology and pre-treatment effects. J. Chromatogr. B 2007, 847, 45–53. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Fadel, H.T.; Flytström, I.; Calander, A.M.; Bergbrant, I.M.; Heijl, L.; Birkhed, D. Profiles of dental caries and periodontal disease in individuals with or without psoriasis. J. Periodontol. 2013, 84, 477–485. [Google Scholar] [CrossRef]
- Campanati, A.; Moroncini, G.; Ganzetti, G.; Pozniak, K.N.; Goteri, G.; Giuliano, A.; Martina, E.; Liberati, G.; Ricotti, F.; Gabrielli, A.; et al. Adalimumab Modulates Angiogenesis in Psoriatic Skin. Eur. J. Inflamm. 2013, 11, 489–498. [Google Scholar] [CrossRef]
- Giannoni, M.; Consales, V.; Campanati, A.; Ganzetti, G.; Giuliodori, K.; Postacchini, V.; Liberati, G.; Azzaretto, L.; Vichi, S.; Guanciarossa, F.; et al. Homocysteine plasma levels in psoriasis patients: Our experience and review of the literature. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1781–1785. [Google Scholar] [CrossRef]
- Luchetti, M.M.; Benfaremo, D.; Campanati, A.; Molinelli, E.; Ciferri, M.; Cataldi, S.; Capeci, W.; Di Carlo, M.; Offidani, A.M.; Salaffi, F.; et al. Clinical outcomes and feasibility of the multidisciplinary management of patients with psoriatic arthritis: Two-year clinical experience of a dermo-rheumatologic clinic. Clin. Rheumatol. 2018, 37, 2741–2749. [Google Scholar] [CrossRef]
- Bardazzi, F.; Magnano, M.; Campanati, A.; Loconsole, F.; Carpentieri, A.; Potenza, C.; Bernardini, N.; Di Lernia, V.; Carrera, C.; Raone, B.; et al. Biologic Therapies in HIV-infected Patients with Psoriasis: An Italian Experience. Acta Derm. Venereol. 2017, 97, 989–990. [Google Scholar] [CrossRef]
- Asa’ad, F.; Fiore, M.; Alfieri, A.; Pigatto, P.D.M.; Franchi, C.; Berti, E.; Maiorana, C.; Damiani, G. Saliva as a Future Field in Psoriasis Research. BioMed Res. Int. 2018, 2018, 7290913. [Google Scholar] [CrossRef]
- Soudan, R.A.; Daoud, S.A.; Mashlah, A.M. Study of some salivary changes in cutaneous psoriatic patients. Saudi Med. J. 2011, 32, 386–389. [Google Scholar]
- Belstrøm, D.; Eiberg, J.M.; Enevold, C.; Grande, M.A.; Jensen, C.A.J.; Skov, L.; Hansen, P.R. Salivary microbiota and inflammation-related proteins in patients with psoriasis. Oral Dis. 2020, 26, 677–687. [Google Scholar] [CrossRef]
- Ganzetti, G.; Campanati, A.; Santarelli, A.; Sartini, D.; Molinelli, E.; Brisigotti, V.; Di Ruscio, G.; Bobyr, I.; Emanuelli, M.; Offidani, A. Salivary interleukin-1β: Oral inflammatory biomarker in patients with psoriasis. J. Int. Med. Res. 2016, 44, 10–14. [Google Scholar] [CrossRef]
- Ganzetti, G.; Campanati, A.; Santarelli, A.; Pozzi, V.; Molinelli, E.; Minnetti, I.; Brisigotti, V.; Procaccini, M.; Emanuelli, M.; Offidani, A. Periodontal disease: An oral manifestation of psoriasis or an occasional finding? Drug Dev. Res. 2014, 75 (Suppl. 1), S46–S49. [Google Scholar] [CrossRef] [PubMed]
- Ganzetti, G.; Campanati, A.; Santarelli, A.; Pozzi, V.; Molinelli, E.; Minnetti, I.; Brisigotti, V.; Procaccini, M.; Emanuelli, M.; Offidani, A. Involvement of the oral cavity in psoriasis: Results of a clinical study. Br. J. Dermatol. 2015, 172, 282–285. [Google Scholar] [CrossRef]
- Martina, E.; Campanati, A.; Diotallevi, F.; Offidani, A. Saliva and Oral Diseases. J. Clin. Med. 2020, 9, 466. [Google Scholar] [CrossRef] [PubMed]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Flisiak, I.; Kołodziej, J.K.U.; Kotowska-Rodziewicz, A.; Klimiuk, A.; Zalewska, A. Enhanced Inflammation and Nitrosative Stress in the Saliva and Plasma of Patients with Plaque Psoriasis. J. Clin. Med. 2020, 9, 745. [Google Scholar] [CrossRef]
- Skutnik-Radziszewska, A.; Maciejczyk, M.; Fejfer, K.; Krahel, J.; Flisiak, I.; Kołodziej, U.; Zalewska, A. Salivary Antioxidants and Oxidative Stress in Psoriatic Patients: Can Salivary Total Oxidant Status and Oxidative Status Index Be a Plaque Psoriasis Biomarker? Oxidative Med. Cell. Longev. 2020, 2020, 9086024. [Google Scholar] [CrossRef]
- Bahramian, A.; Falsafi, P.; Abbasi, T.; Ghanizadeh, M.; Abedini, M.; Kavoosi, F.; Kouhsoltani, M.; Noorbakhsh, F.; Dabbaghi Tabriz, F.; Rajaeih, S.; et al. Comparing Serum and Salivary Levels of Vitamin D in Patients with Recurrent Aphthous Stomatitis and Healthy Individuals. J. Dent. 2018, 19, 295–300. [Google Scholar]
- Bottoni, U.; Tiriolo, R.; Pullano, S.A.; Dastoli, S.; Amoruso, G.F.; Nisticò, S.P.; Fiorillo, A.S. Infrared Saliva Analysis of Psoriatic and Diabetic Patients: Similarities in Protein Components. IEEE Trans. Biomed. Eng. 2016, 63, 379–384. [Google Scholar] [CrossRef]
- Li, Y.; Lin, P.; Wang, S.; Li, S.; Wang, R.; Yang, L.; Wang, H. Quantitative analysis of differentially expressed proteins in psoriasis vulgaris using tandem mass tags and parallel reaction monitoring. Clin. Proteom. 2020, 17, 30. [Google Scholar] [CrossRef]
- McCartan, B.E.; Healy, C.M. The reported prevalence of oral lichen planus: A review and critique. J. Oral Pathol. Med. 2008, 37, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Thorn, J.J.; Holmstrup, P.; Rindum, J.; Pindborg, J.J. Course of various clinical forms of oral lichen planus. A prospective follow-up study of 611 patients. J. Oral Pathol. 1988, 17, 213–218. [Google Scholar] [CrossRef]
- Campanati, A.; Brandozzi, G.; Giangiacomi, M.; Simonetti, O.; Marconi, B.; Offidani, A.M. Lichen striatus in adults and pimecrolimus: Open, off-label clinical study. Int. J. Dermatol. 2008, 47, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.S.; Gould, A.; Kurago, Z.; Fantasia, J.; Muller, S. Diagnosis of oral lichen planus: A position paper of the American Academy of Oral and Maxillofacial Pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 332–354. [Google Scholar] [CrossRef]
- Buajeeb, W.; Okuma, N.; Thanakun, S.; Laothumthut, T. Direct Immunofluorescence in Oral Lichen Planus. J. Clin. Diagn. Res. 2015, 9, ZC34–ZC37. [Google Scholar] [CrossRef]
- Lodi, G.; Scully, C.; Carrozzo, M.; Griffiths, M.; Sugerman, P.B.; Thongprasom, K. Current controversies in oral lichen planus: Report of an international consensus meeting. Part 1. Viral infections and etiopathogenesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 40–51. [Google Scholar] [CrossRef]
- Van der Meij, E.H.; Mast, H.; van der Waal, I. The possible premalignant character of oral lichen planus and oral lichenoid lesions: A prospective five-year follow-up study of 192 patients. Oral Oncol. 2007, 43, 742–748. [Google Scholar] [CrossRef]
- Radwan-Oczko, M.; Zwyrtek, E.; Owczarek, J.E.; Szcześniak, D. Psychopathological profile and quality of life of patients with oral lichen planus. J. Appl. Oral Sci. 2018, 26, e20170146. [Google Scholar] [CrossRef]
- Talungchit, S.; Buajeeb, W.; Lerdtripop, C.; Surarit, R.; Chairatvit, K.; Roytrakul, S.; Kobayashi, H.; Izumi, Y.; Khovidhunkit, S.P. Putative salivary protein biomarkers for the diagnosis of oral lichen planus: A case-control study. BMC Oral Health 2018, 18, 42. [Google Scholar] [CrossRef]
- Souza, M.M.; Florezi, G.P.; Nico, M.; de Paula, F.; Paula, F.M.; Lourenço, S.V. Salivary proteomics in lichen planus: A relationship with pathogenesis? Oral Dis. 2018, 24, 784–792. [Google Scholar] [CrossRef]
- De Carvalho, G.C.; Domingues, R.; de Sousa Nogueira, M.A.; Calvielli Castelo Branco, A.C.; Gomes Manfrere, K.C.; Pereira, N.V.; Aoki, V.; Sotto, M.N.; Da Silva Duarte, A.J.; Sato, M.N. Up-regulation of Proinflammatory Genes and Cytokines Induced by S100A8 in CD8+ T Cells in Lichen Planus. Acta Derm. Venereol. 2016, 96, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Darczuk, D.; Krzysciak, W.; Vyhouskaya, P.; Kesek, B.; Galecka-Wanatowicz, D.; Lipska, W.; Kaczmarzyk, T.; Gluch-Lutwin, M.; Mordyl, B.; Chomyszyn-Gajewska, M. Salivary oxidative status in patients with oral lichen planus. J. Physiol. Pharmacol. 2016, 67, 885–894. [Google Scholar] [PubMed]
- Abdolsamadi, H.; Rafieian, N.; Goodarzi, M.T.; Feradmal, J.; Davoodi, P.; Jazayeri, M.; Taghavi, Z.; Hoseyni, S.M.; Ahmadi-Motamayel, F. Levels of salivary antioxidant vitamins and lipid peroxidation in patients with oral lichen planus and healthy individuals. Chonnam Med. J. 2014, 50, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Rivarola de Gutierrez, E.; Di Fabio, A.; Salomón, S.; Lanfranchi, H. Topical treatment of oral lichen planus with anthocyanins. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e459–e466. [Google Scholar] [CrossRef]
- Tvarijonaviciute, A.; Aznar-Cayuela, C.; Rubio, C.P.; Tecles, F.; Ceron, J.J.; López-Jornet, P. Salivary Antioxidant Status in Patients with Oral Lichen Planus: Correlation with Clinical Signs and Evolution during Treatment with Chamaemelum nobile. BioMed Res. Int. 2018, 2018, 5187549. [Google Scholar] [CrossRef]
- Skrinjar, I.; Vidranski, V.; Brzak, B.L.; Vidovic Juras, D.; Andabak Rogulj, A.; Brailo, V.; Vucicevic Boras, V. Salivary Cortisol Levels in Patients with Oral Lichen Planus—A Pilot Case-Control Study. Dent. J. 2019, 7, 59. [Google Scholar] [CrossRef]
- Mansourian, A.; Najafi, S.; Nojoumi, N.; Parhami, P.; Moosavi, M.S. Salivary Cortisol and Salivary Flow Rate in Clinical Types of Oral Lichen Planus. SkinMed 2018, 16, 19–22. [Google Scholar]
- Lopez-Jornet, P.; Zavattaro, E.; Mozaffari, H.R.; Ramezani, M.; Sadeghi, M. Evaluation of the Salivary Level of Cortisol in Patients with Oral Lichen Planus: A Meta-Analysis. Medicina 2019, 55, 213. [Google Scholar] [CrossRef]
- Nadendla, L.K.; Meduri, V.; Paramkusam, G.; Pachava, K.R. Association of salivary cortisol and anxiety levels in lichen planus patients. J. Clin. Diagn. Res. 2014, 8, ZC01–ZC03. [Google Scholar] [CrossRef]
- Rödström, P.O.; Jontell, M.; Hakeberg, M.; Berggren, U.; Lindstedt, G. Erosive oral lichen planus and salivary cortisol. J. Oral Pathol. Med. 2001, 30, 257–263. [Google Scholar] [CrossRef]
- Koray, M.; Dülger, O.; Ak, G.; Horasanli, S.; Uçok, A.; Tanyeri, H.; Badur, S. The evaluation of anxiety and salivary cortisol levels in patients with oral lichen planus. Oral Dis. 2003, 9, 298–301. [Google Scholar] [CrossRef]
- Stojanovich, L. Stress and autoimmunity. Autoimmun. Rev. 2010, 9, A271–A276. [Google Scholar] [CrossRef]
- Wei, W.; Sun, Q.; Deng, Y.; Wang, Y.; Du, G.; Song, C.; Li, C.; Zhu, M.; Chen, G.; Tang, G. Mixed and inhomogeneous expression profile of Th1/Th2 related cytokines detected by cytometric bead array in the saliva of patients with oral lichen planus. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 142–151. [Google Scholar] [CrossRef]
- Hodge, D.R.; Peng, B.; Cherry, J.C.; Hurt, E.M.; Fox, S.D.; Kelley, J.A.; Munroe, D.J.; Farrar, W.L. Interleukin 6 supports the maintenance of p53 tumor suppressor gene promoter methylation. Cancer Res. 2005, 65, 4673–4682. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Sharifi, R.; Sadeghi, M. Interleukin-6 levels in the serum and saliva of patients with oral lichen planus compared with healthy controls: A meta-analysis study. Cent. Eur. J. Immunol. 2018, 43, 103–108. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Sharifi, R.; Mirbahari, S.; Montazerian, S.; Sadeghi, M.; Rostami, S. A systematic review and meta-analysis study of salivary and serum interleukin-8 levels in oral lichen planus. Adv. Dermatol. Allergol. 2018, 35, 599–604. [Google Scholar] [CrossRef]
- Baggiolini, M.; Clark-Lewis, I. Interleukin-8, a chemotactic and inflammatory cytokine. FEBS Lett. 1992, 307, 97–101. [Google Scholar] [CrossRef]
- Rhodus, N.L.; Cheng, B.; Myers, S.; Miller, L.; Ho, V.; Ondrey, F. The feasibility of monitoring NF-κB associated cytokines: TNF-α, IL-1α, IL-6, and IL-8 in whole saliva for the malignant transformation of oral lichen planus. Mol. Carcinog. 2005, 44, 77–82. [Google Scholar] [CrossRef]
- Campanati, A.; Ganzetti, G.; Giuliodori, K.; Molinelli, E.; Offidani, A. Biologic Therapy in Psoriasis: Safety Profile. Curr. Drug Saf. 2016, 11, 4–11. [Google Scholar] [CrossRef]
- Radi, G.; Campanati, A.; Diotallevi, F.; Bianchelli, T.; Offidani, A. Novel Therapeutic Approaches and Targets for Treatment of Psoriasis. Curr. Pharm. Biotechnol. 2021, 22, 7–31. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Ramezani, M.; Mahmoudiahmadabadi, M.; Omidpanah, N.; Sadeghi, M. Salivary and serum levels of tumor necrosis factor-alpha in oral lichen planus: A systematic review and meta-analysis study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, e183–e189. [Google Scholar] [CrossRef]
- Gavala, A.; Venetsanou, K.; Kittas, C.; Manolis, E.; Yiambides, A.; Myrianthefs, P.; Baltopoulos, G. Decreased whole blood TNFα production capacity after acute alcohol exposure and LPS stimulation ex vivo. Crit. Care 2010, 14, P13. [Google Scholar] [CrossRef]
- Mozaffari, H.R.; Sharifi, R.; Hayati, M.; Imani, M.M.; Lopez-Jornet, P.; Golshah, A.; Moradpoor, H.; Rezaei, R.; Sadeghi, M. Evaluation of serum and salivary interferon-γ levels in patients with oral lichen planus: A systematic review and meta-analysis of case-control studies. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Corbaux, C.; Joly, P. Bullous Diseases. In Adverse Reactions to Biologics; Puig, L., Gulliver, W., Eds.; Current Problems in Dermatology; Karger: Basel, Switzerland, 2018; Volume 53, pp. 64–69. [Google Scholar] [CrossRef]
- Murrell, D.F.; Peña, S.; Joly, P.; Marinovic, B.; Hashimoto, T.; Diaz, L.A.; Sinha, A.A.; Payne, A.S.; Daneshpazhooh, M.; Eming, R.; et al. Diagnosis and management of pemphigus: Recommendations of an international panel of experts. J. Am. Acad. Dermatol. 2020, 82, 575–585.e1. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, D.; Lorenzini, G.; Drakoulakos, D.; Belazi, M.; Mihailidou, E.; Velkos, G.; Mourellou-Tsatsou, O.; Antoniades, D. Detection of pemphigus desmoglein 1 and desmoglein 3 autoantibodies and pemphigoid BP180 autoantibodies in saliva and comparison with serum values. Eur. J. Oral Sci. 2006, 114, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Kelly, C.; Challacombe, S.J.; Donaldson, A.N.; Bhogal, B.S.; Setterfield, J.F. Serum and salivary IgG and IgA antibodies to desmoglein 3 in mucosal pemphigus vulgaris. Br. J. Dermatol. 2016, 175, 113–121. [Google Scholar] [CrossRef]
- De, D.; Khullar, G.; Handa, S.; Joshi, N.; Saikia, B.; Minz, R.W. Correlation between salivary and serum anti-desmoglein 1 and 3 antibody titres using ELISA and between anti-desmoglein levels and disease severity in pemphigus vulgaris. Clin. Exp. Dermatol. 2017, 42, 648–650. [Google Scholar] [CrossRef] [PubMed]
- Koopai, M.; Mortazavi, H.; Khatami, A.; Khodashenas, Z. Salivary and Serum Anti-Desmoglein 1 and 3 ELISA and Indirect Immunofluorescence in Pemphigus Vulgaris: Correlations with Serum ELISA, Indirect Immunofluorescence and Disease Severity. Acta Dermatovenerol. Croat. 2018, 26, 91–99. [Google Scholar]
- Mortazavi, H.; Khatami, A.; Seyedin, Z.; Vasheghani Farahani, I.; Daneshpazhooh, M. Salivary desmoglein enzyme-linked immunosorbent assay for diagnosis of pemphigus vulgaris: A noninvasive alternative test to serum assessment. Biomed. Res. Int. 2015, 2015, 698310. [Google Scholar] [CrossRef]
- Russo, I.; Saponeri, A.; Michelotto, A.; Alaibac, M. Salivary Samples for the Diagnosis of Pemphigus vulgaris Using the BIOCHIP Approach: A Pilot Study. In Vivo 2017, 31, 97–99. [Google Scholar] [CrossRef][Green Version]
- Ezzedine, K.; Eleftheriadou, V.; Whitton, M.; van Geel, N. Vitiligo. Lancet 2015, 386, 74–84. [Google Scholar] [CrossRef]
- Sehgal, V.N.; Dube, B. Secretion of blood group specific substances in saliva of vitiligo patients. A preliminary report. Br. J. Dermatol. 1967, 79, 704–705. [Google Scholar] [CrossRef]
- Orciani, M.; Campanati, A.; Caffarini, M.; Ganzetti, G.; Consales, V.; Lucarini, G.; Offidani, A.; Di Primio, R. T helper (Th)1, Th17 and Th2 imbalance in mesenchymal stem cells of adult patients with atopic dermatitis: At the origin of the problem. Br. J. Dermatol. 2017, 176, 1569–1576. [Google Scholar] [CrossRef]
- Thijs, J.L.; van Seggelen, W.; Bruijnzeel-Koomen, C.; de Bruin-Weller, M.; Hijnen, D. New Developments in Biomarkers for Atopic Dermatitis. J. Clin. Med. 2015, 4, 479–487. [Google Scholar] [CrossRef]
- Kojima, R.; Matsuda, A.; Nomura, I.; Matsubara, O.; Nonoyama, S.; Ohya, Y.; Saito, H.; Matsumoto, K. Salivary cortisol response to stress in young children with atopic dermatitis. Pediatr. Dermatol. 2013, 30, 17–22. [Google Scholar] [CrossRef]
- Mizawa, M.; Yamaguchi, M.; Ueda, C.; Makino, T.; Shimizu, T. Stress evaluation in adult patients with atopic dermatitis using salivary cortisol. BioMed Res. Int. 2013, 2013, 138027. [Google Scholar] [CrossRef]


{kind=link}
| First Author (Ref.), Year | Type of Molecules Studied in Saliva | Method Used for Analysis | Type of Study | Number of Patients | Results |
|---|---|---|---|---|---|
| H Fadel, 2013 [26] | Unstimulated salivary SR -Stimulated salivary SR -Salivary pH | -Unstimulated and paraffin-stimulated saliva samples collection, for the determination of secretion rate and buffer capacity | -Case-control study | -89 patients with mild-to-moderate psoriasis -54 individuals without psoriasis | Individuals with psoriasis had low salivary pH, compared to the control group. |
| F Asa’ad, 2018 [31] | 2-IgA -CRP -sAA -Haptoglobin -K+ -TNFα -TGF-β1 -IL-1β -MCP-1 | -Salivary level of IgA was assessed by radial immunodiffusion -Levels of salivary CRP and Haptoglobin were determined by an immunoturbidimetric method -sAA and K+ levels were analyzed using ISE (Ion Selective Electrode) technology for electrolyte measurements and LISA 500 plus systems for sAA -TNFα, TGF-β1, IL-1β, MCP-1 were assessed by using multianalyte ELISA Arrays | Review | -60 patients with psoriasis and 40 individuals without psoriasis, enrolled in the study concerning IgA, CRP, Haptoglobin. -20 patients with uncomplicated psoriasis and 20 individuals without psoriasis, enrolled in the study concerning sAA and K+ -60 patients with psoriasid and 45 patients without psoriasis, enrolled in the study concerning TNFα, TGF-β1, IL-1β, MCP-1 | No statistically significant difference in the salivary level of IgA between psoriasis patients and healthy controls. Psoriasis patients with PASI > 10 had tendency to show lower levels of IgA, compared to patients with a PASI < 10. Patients with psoriasis had higher levels of CRP, Haptoglobin, sAA, K+, TNFα, TGF-β1, IL-1β, MCP-1, compared with controls. |
| R A Soudan, 2011 [32] | -K+ -Na+ -Cl− -sAA | -ISE (Ion Selective Electrode) technology for K+, Cl−, Na+ measurement. -LISA 500 plus system for sAA measurement. | -Case-control study | -20 patients with uncomplicated psoriasis -20 individuals without psoriasis | Psoriatics had significantly higher K+ and sAA concentrations than the controls, whereas there was no significant rise in the other salivary ions studied. |
| D Belstrom, 2020 [33] | -NGAL (neutrophil gelatinase-associated lipocalin)-Transferrin | Stimulated saliva samples were characterized by means of next-generation sequencing of the 16S rRNA gene. Salivary levels of NGAL and transferrin were quantified using immunoassays. | -Case-control study | -27 patients with psoriasis -58 patients with periodontitis -52 orally healthy individuals | Significantly lower mean salivary levels of NGAL and transferrin were identified in patients with psoriasis, compared to patients with periodontitis and orally healthy controls. |
| G Ganzetti, 2016 [34] | -IL-1β | -IL-1β levels were evaluated via an enzyme-linked immunosorbent assay kit | -Case-control study | -25 patients with psoriasis -20 individuals without psoriasis | At baseline, patients had significantly higher salivary IL1β levels than controls. In patients with psoriasis, TNF-a inhibitor treatment resulted in significantly reduced IL1β levels compared with baseline, but IL1β levels remained significantly higher than in control subjects even after treatment. |
| G Ganzetti, 2015 [35] | -IL-1β -IL-6-TGF -β1- IL-8 -TNF-β -IFN-χ -IL-17A -IL-4 -IL-10 -MCP-1 -MIP-1α,β | Multi-Analyte ELISA array Kit | -Case-control study | -60 patients with psoriasis -45 individuals without psoriasis | Patients with active psoriasis had significantly higher salivary IL1β, TNF-α, TGF-β, and MCP-1 levels than healthy controls. |
| A Skutnik-Radziszewska, 2020 [38] | -TNF-α -IL-2-IFN -χ -IL-10 | ELISA | -Case-control study | -30 patients with psoriasis and hyposalivation -30 patients with psoriasis and normal secretion of saliva -60 individuals without psoriasis | The levels of tumor necrosis factor-alpha (TNF-α), interleukin-2 (IL-2), and interferon-gamma (INF-γ) were significantly higher, whereas interleukin-10 (IL-10) content was considerably lower in unstimulated and stimulated saliva of patients with psoriasis compared to the controls. |
| A Skutnik-Radziszewska, 2020 [39] | -Peroxidase (Px) -Catalase (Cat) -Superoxide Dismutase (SOD) | The activity of antioxidant enzymes (Px, CAT, and SOD) was measured in NWS (unstimulated saliva), SWS (stimulated saliva), and erythro- cytes by performing Redox Analysis. Absorbance/fluorescence was measured with an Infinite M200 PRO Multimode Tecan microplate reader. | -Case-control study | -40 patients with psoriasis -40 individuals without psoriasis | The concentration of Px, CAT, and SOD was significantly higher in NWS of patients with plaque psoriasis vs. healthy subjects. In SWS of psoriatic patients, there was a considerably higher concentration of Px and CAT. |
| A Bahramian, 2018 [40] | -Vitamine D | Vitamin D total (25-hydroxy vitamin D) kit was used with the electrochemiluminescence technique to determine and compare salivary and serum levels of vitamin D between the healthy individuals and those with RAS. | -Case-control study | -26 patients with RAS (Recurrent aphtous stomatitis) -26 healthy individuals | The serum levels of vitamin D in patients with RAS were significantly less than that in healthy individuals; however, there were no significant differences in salivary vitamin D levels between patients with RAS and healthy individuals. There was a significant and positive correlation between serum and salivary levels of vitamin D in all patients. |
| U Bottoni, 2016 [41] | -Saliva proteomic components | It was performed attenuated total reflection (ATR) in conjunction with infrared spectroscopy. | -Case-control study | -35 patients with psoriasis -20 patients with diabetes -20 healthy individuals | There were differences in the secondary structure composition of proteins between psoriatic and diabetic patients as compared to the control group. Saliva spectra of the control group and that of the palmoplantar psoriatic patients differ from plaque psoriasis and diabetic patient spectra because of the absence of the amide II band and the presence of different secondary protein-structure conformations. |
| Y Li, 2020 [42] | -Differential expressed proteins (DEPs) | Tandem mass tags (TMTs) coupled with liquid chromatography–mass spectrometry (LC–MS)/MS. | -Case-control study | -11 patients with psoriasis -11 individuals without psoriasis | A total of 4562 differentially expressed proteins (DEPs) between PV lesional tissues and healthy tissues were identified. |
| First Author [Ref.], Year | Type of Molecules Studied in Saliva | Method Used for Analysis | Type of Study | Number of Patients | Results |
|---|---|---|---|---|---|
| Andreadis, 2006 [78] | Anti-Desmoglein 1 and desmoglein 3 antibodies in PV; -Anti-BP180 antibodies in BP. | ELISA | Case-control study (?) | -12 patients with MMP; -12 patients with BP; -10 patients with PV; -10 healthy controls. | ELISA analysis of Dsg3 and Dsg1 in saliva is a highly sensitive and specific test that is suitable for diagnostic purposes, monitoring of disease activity and early detection of pemphigus relapses, as there is a high concordance between serum and salivary levels of the proteins. |
| Ali, 2016 [79] | Anti-Dsg3 IgA antibodies in PV. | ELISA | Case-control study (?) | -23 patients with PV -17 healthy subjects -9 disease controls | Assay of salivary IgG antibodies to Dsg3 offers a diagnostic alternative to serum in the diagnosis and monitoring of PV. The role of anti-Dsg3 IgA antibodies requires further elucidation in the pathogenesis of PV. |
| De, 2017 [80] | -Anti-Dsg1 and 3 antibodies in PV. | ELISA | Case-control study (?) | -43 patients with PV; -5 controls | There was a statistically significant correlation between serum and salivary Dsg1 levels and between serum and salivary Dsg3 levels. There was no correlation between serum or salivary Dsg1 and Dsg3 levels with the objective component of the oral mucosal Autoimmune Bullous Skin Disorder Intensity Score (ABSIS). |
| Koopai, 2018 [81] | -Anti-Dsg1 and anti-Dsg3 antibodies in PV. | ELISA | Cross-sectional study | -50 patients with PV | Moderate significant correlation between Dsg1 and Dsg3 levels present on saliva detected by ELISA technique and PV severity. |
| Mortazavi, 2015 [82] | -Anti-Dsg1 and anti-Dsg3 antibodies in PV. | ELISA | Case-control study |
-86 untreated PV; -80 age- and sex-matched PV-free controls. | Salivary anti-Dsg 1 and 3 ELISA with high specificities (98.9%) could be suggested as safe and noninvasive methods for the diagnosis of PV when obtaining a blood sample is difficult. |
| Russo, 2017 [83] | -Anti-Dsg1 and anti-Dsg3 antibodies in PV. | ELISA and BIOCHIP Approach | Pilot study | -8 patients with PV | Autoantibodies to DSG3 were detected in 8 out of 8 salivary samples by ELISA and in 6 out of 8 salivary samples by the BIOCHIP approach. Autoantibodies to DSG1 were negative in all salivary samples using both ELISA and BIOCHIP. There were no positive results in the negative control group. In conclusion, the results of this pilot study indicate a lack of correlation between serum and salivary results using both ELISA and BIOCHIP, indicating that saliva may not be the ideal substrate for the laboratory diagnosis of PV using these approaches. |
| First Author [Ref.], year | Type of Molecules Studied in Saliva | Method Used for Analysis | Type of Study | Number of Patients | Results |
|---|---|---|---|---|---|
| Sehgal, 1967 [85] | Not declared. | Not declared. | -Case-control study | -76 patients with vitiligo. -370 normal controls | The study revealed an increased predilection for the secretors to develop the disease as compared to non-secretors. More investigations in this connection are indicated which may further enrich our information as regards the transmission and course of the disease |
| First Author [Ref.], Year | Demography | Time and Duration of Collection | Storage of Sample | Kind of Sample | Salivary Analysis |
|---|---|---|---|---|---|
| Mizawa M, 2013 [88] | 30 adults (15 males and 15 females; age, 15–62 years; mean age, 29.6 years) SCORAD index (mean ± SE) ranged from 9.9 to 80.3 (46.7 ± 3.2) | 9–11 a.m. 5 min | Centrifugation Supernatant stored at −80 °C | Twisted cotton dental cord (Salimetrics LLC, State College, PA, USA) | linked immunosorbent assay kits (1-3002; Salimetrics LLC, State College, PA, USA) plate reader (450 nm measurement wavelength; ARVO MX; Perkin Elmer Life Science, Boston, MA, USA) |
| Kojima R, 2013 [89] | 38 young children (24 boys and 14 girls) median age 16.5 months, range 3–66 months) SCORAD INDEX median (range) mild [n12] 16 (8–25) moderate [n14] 40 (26–48) severe [n12] 64.5 (51–86) | 10 a.m.–3 p.m. 5 min before venipuncture 15–20 min after venipuncture 1 min under the tongue | Centrifugation 15 min at 1800× g Supernatant stored at −30 °C | Sorbette sampling device (Salimetrics, State College, PA, USA) | salivary cortisol enzyme-linked immunosorbent assay kit (Salimetrics), according to the manufacturer’s protocol. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campanati, A.; Martina, E.; Diotallevi, F.; Radi, G.; Marani, A.; Sartini, D.; Emanuelli, M.; Kontochristopoulos, G.; Rigopoulos, D.; Gregoriou, S.; et al. Saliva Proteomics as Fluid Signature of Inflammatory and Immune-Mediated Skin Diseases. Int. J. Mol. Sci. 2021, 22, 7018. https://doi.org/10.3390/ijms22137018
Campanati A, Martina E, Diotallevi F, Radi G, Marani A, Sartini D, Emanuelli M, Kontochristopoulos G, Rigopoulos D, Gregoriou S, et al. Saliva Proteomics as Fluid Signature of Inflammatory and Immune-Mediated Skin Diseases. International Journal of Molecular Sciences. 2021; 22(13):7018. https://doi.org/10.3390/ijms22137018
Chicago/Turabian StyleCampanati, Anna, Emanuela Martina, Federico Diotallevi, Giulia Radi, Andrea Marani, Davide Sartini, Monica Emanuelli, George Kontochristopoulos, Dimitris Rigopoulos, Stamatis Gregoriou, and et al. 2021. "Saliva Proteomics as Fluid Signature of Inflammatory and Immune-Mediated Skin Diseases" International Journal of Molecular Sciences 22, no. 13: 7018. https://doi.org/10.3390/ijms22137018
APA StyleCampanati, A., Martina, E., Diotallevi, F., Radi, G., Marani, A., Sartini, D., Emanuelli, M., Kontochristopoulos, G., Rigopoulos, D., Gregoriou, S., & Offidani, A. (2021). Saliva Proteomics as Fluid Signature of Inflammatory and Immune-Mediated Skin Diseases. International Journal of Molecular Sciences, 22(13), 7018. https://doi.org/10.3390/ijms22137018