The Paradox Effect of Calcification in Carotid Atherosclerosis: Microcalcification Is Correlated with Plaque Instability


 , , , ,
, , , , 

Abstract
1. Introduction
2. Results
2.1. Clinical Data
2.2. Calcification and Risk Factors
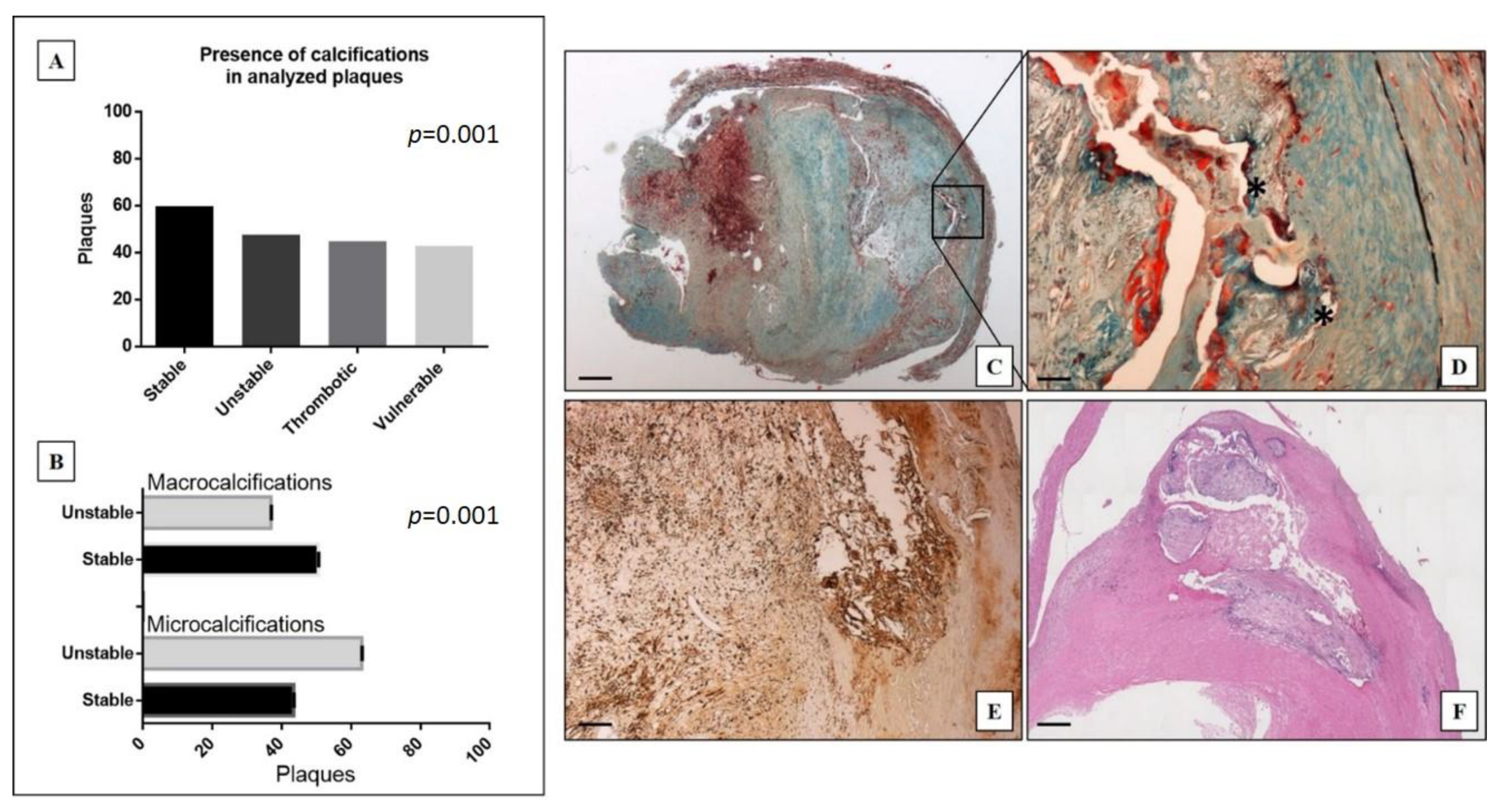
2.3. Histological Findings
2.4. Plaques with Microcalcifications vs. Those with Macrocalcifications
3. Discussion
4. Material and Methods
4.1. Cases Selection
4.2. Histology
4.3. Histological Classification
4.4. TMA Construction
4.5. Immunohistochemistry
4.6. Risk Factors Definition
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alexopoulos, N.; Raggi, P. Calcification in atherosclerosis. Nat. Rev. Cardiol. 2009, 6, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Shioi, A.; Ikari, Y. Plaque Calcification during Atherosclerosis Progression and Regression. J. Atheroscler. Thromb. 2018, 25, 294–303. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, J.W.; Blaha, M.J.; DeFilippis, A.P.; Budoff, M.J.; Nasir, K.; Blumenthal, R.S.; Jones, S.R. Coronary Artery Calcium Progression: An Important Clinical Measurement? J. Am. Coll. Cardiol. 2010, 56, 1613–1622. [Google Scholar] [CrossRef] [PubMed]
- Tesauro, M.; Mauriello, A.; Rovella, V.; Annicchiarico-Petruzzelli, M.; Cardillo, C.; Melino, G.; Di Daniele, N. Arterial ageing: From endothelial dysfunction to vascular calcification. J. Intern. Med. 2017, 281, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Jinnouchi, H.; Sato, Y.; Sakamoto, A.; Cornelissen, A.; Mori, M.; Kawakami, R.; Gadhoke, N.V.; Kolodgie, F.D.; Virmani, R.; Finn, A.V. Calcium deposition within coronary atherosclerotic lesion: Implications for plaque stability. Atherosclerosis 2020, 306, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Mauriello, A.; Servadei, F.; Biondi-Zoccai, G.; Giacobbi, E.; Anemona, L.; Bonanno, E.; Casella, S. Coronary calcification identifies the vulnerable patient rather than the vulnerable Plaque. Atherosclerosis 2013, 229, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Bischetti, S.; Scimeca, M.; Bonanno, E.; Federici, M.; Anemona, L.; Menghini, R.; Casella, S.; Cardellini, M.; Ippoliti, A.; Mauriello, A. Carotid plaque instability is not related to quantity but to elemental composition of calcification. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 768–774. [Google Scholar] [CrossRef]
- Demer, L.L.; Tintut, Y. Inflammatory, Metabolic, and Genetic Mechanisms of Vascular Calcification. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 715–723. [Google Scholar] [CrossRef]
- Scimeca, M.; Anemona, L.; Granaglia, A.; Bonfiglio, R.; Urbano, N.; Toschi, N.; Santeusanio, G.; Schiaroli, S.; Mauriello, S.; Tancredi, V.; et al. Plaque calcification is driven by different mechanisms of mineralization associated with specific cardiovascular risk factors. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1330–1336. [Google Scholar] [CrossRef]
- Scimeca, M.; Urbano, N.; Rita, B.; Mapelli, S.N.; Catapano, C.V.; Carbone, G.M.; Ciuffa, S.; Tavolozza, M.; Schillaci, O.; Mauriello, A.; et al. Prostate Osteoblast-Like Cells: A Reliable Prognostic Marker of Bone Metastasis in Prostate Cancer Patients. Contrast Media Mol. Imaging 2018, 2018, 9840962. [Google Scholar] [CrossRef]
- Bonfiglio, R.; Scimeca, M.; Urbano, N.; Bonanno, E.; Schillaci, O. Breast microcalcifications: Biological and diagnostic perspectives. Future Oncol. 2018, 14, 3097–3099. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Bonfiglio, R.; Varone, F.; Ciuffa, S.; Mauriello, A.; Bonanno, E. Calcifications in prostate cancer: An active phenomenon mediated by epithelial cells with osteoblast-phenotype. Microsc. Res. Tech. 2018, 81, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, T.; Dweck, M.R.; Narula, N.; Pisapia, D.; Narula, J.; Strauss, H.W. Coronary Artery Calcification: From Mech-anism to Molecular Imaging. JACC Cardiovasc. Imaging 2017, 10, 582–593. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, F.; Sakakura, K.; Yahagi, K.; Joner, M.; Virmani, R. Has Our Understanding of Calcification in Human Coronary Atherosclerosis Progressed? Arterioscler. Thromb. Vasc. Biol. 2014, 34, 724–736. [Google Scholar] [CrossRef]
- Hutcheson, J.D.; Goettsch, C.; Bertazzo, S.S.; Maldonado, N.; Ruiz, J.L.; Goh, W.; Yabusaki, K.; Faits, T.; Bouten, C.C.; Franck, G.; et al. Genesis and growth of extracellular-vesicle-derived microcalcification in atherosclerotic plaques. Nat. Mater. 2016, 15, 335–343. [Google Scholar] [CrossRef]
- Lomashvili, K.A.; Cobbs, S.; Hennigar, R.A.; Hardcastle, K.I.; O’Neill, W.C. Phosphate-Induced Vascular Calcification: Role of Pyrophosphate and Osteopontin. J. Am. Soc. Nephrol. 2004, 15, 1392–1401. [Google Scholar] [CrossRef]
- Pugliese, G.; Iacobini, C.; Fantauzzi, C.B.; Menini, S. The dark and bright side of atherosclerotic calcification. Atherosclerosis 2015, 238, 220–230. [Google Scholar] [CrossRef]
- Jinnouchi, H.; Guo, L.; Sakamoto, A.; Torii, S.; Sato, Y.; Cornelissen, A.; Kuntz, S.; Paek, K.H.; Fernandez, R.; Fuller, D.; et al. Diversity of macrophage phenotypes and responses in atherosclerosis. Cell. Mol. Life Sci. 2019, 77, 1919–1932. [Google Scholar] [CrossRef]
- Spagnoli, L.G.; Mauriello, A.; Sangiorgi, G.; Fratoni, S.; Bonanno, E.; Schwartz, R.S.; Piepgras, D.G.; Pistolese, R.; Ippoliti, A.; Holmes, D.R. Extracranial Thrombotically Active Carotid Plaque as a Risk Factor for Ischemic Stroke. JAMA 2004, 292, 1845–1852. [Google Scholar] [CrossRef]
- Mauriello, A.; Sangiorgi, G.; Virmani, R.; Servadei, F.; Trimarchi, S.; Holmes, D.R.; Kolodgie, F.; Biondi-Zoccai, G.; Leuzzi, C.; Spagnoli, L.G. Evidence of a topographical link between unstable carotid plaques and luminal stenosis: Can we better stratify asymptomatic patients with significant plaque burden? Int. J. Cardiol. 2012, 155, 309–311. [Google Scholar] [CrossRef]
- Mauriello, A.; Servadei, F.; Sangiorgi, G.; Anemona, L.; Giacobbi, E.; Liotti, D.; Spagnoli, L.G. Asymptomatic carotid plaque rupture with unexpected thrombosis over a non-canonical vulnerable lesion. Atherosclerosis 2011, 218, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Spagnoli, L.G.; Bonanno, E.; Sangiorgi, G.; Mauriello, A. Role of Inflammation in Atherosclerosis. J. Nucl. Med. 2007, 48, 1800–1815. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, F.; Joner, M.; Prati, F.; Virmani, R.; Narula, J. Clinical classification of plaque morphology in coronary disease. Nat. Rev. Cardiol. 2014, 11, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Cardellini, M.; Rovella, V.; Scimeca, M.; Anemona, L.; Bischetti, S.; Casella, S.; Saggini, A.; Bonanno, E.; Ballanti, M.; Davato, F.; et al. Chronic Kidney Disease Is Linked to Carotid Nodular Calcification, An Unstable Plaque Not Correlated to Inflammation. Aging Dis. 2019, 10, 71–81. [Google Scholar] [CrossRef]
- Pini, R.; Faggioli, G.; Fittipaldi, S.; Vasuri, F.; Longhi, M.; Gallitto, E.; Pasquinelli, G.; Gargiulo, M.; Stella, A. Relationship between Calcification and Vulnerability of the Carotid Plaques. Ann. Vasc. Surg. 2017, 44, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Kwee, R.M. Systematic review on the association between calcification in carotid plaques and clinical ischemic symptoms. J. Vasc. Surg. 2010, 51, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Urbano, N.; Scimeca, M.; Crocco, A.; Mauriello, A.; Bonanno, E.; Schillaci, O. 18F-Choline PET/CT Identifies High-Grade Prostate Cancer Lesions Expressing Bone Biomarkers. J. Clin. Med. 2019, 8, 1657. [Google Scholar] [CrossRef]
- Cheong, B.Y.C.; Wilson, J.M.; Spann, S.J.; Pettigrew, R.I.; Preventza, O.A.; Muthupillai, R. Coronary artery calcium scoring: An evidence-based guide for primary care physicians. J. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Greenland, P.; Blaha, M.J.; Budoff, M.J.; Erbel, R.; Watson, K.E. Coronary Calcium Score and Cardiovascular Risk. J. Am. Coll. Cardiol. 2018, 72, 434–447. [Google Scholar] [CrossRef]
- Proudfoot, D.; Shanahan, C.M.; Weissberg, P.L. Vascular calcification: New insights into an old problem. J. Pathol. 1998, 185, 1–3. [Google Scholar] [CrossRef]
- Li, Y.; Sun, Z.; Zhang, L.; Yan, J.; Shao, C.; Jing, L.; Li, L.; Wang, Z. Role of Macrophages in the Progression and Regression of Vascular Calcification. Front. Pharmacol. 2020, 11, 661. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.J. Macrophage Polarization. Annu. Rev. Physiol. 2017, 79, 541–566. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Bonfiglio, R.; Menichini, E.; Albonici, L.; Urbano, N.; De Caro, M.T.; Mauriello, A.; Schillaci, O.; Gambacurta, A.; Bonanno, E. Microcalcifications Drive Breast Cancer Occurrence and Development by Macrophage-Mediated Epithelial to Mesenchymal Transition. Int. J. Mol. Sci. 2019, 20, 5633. [Google Scholar] [CrossRef]
- Barrett, T.J. Macrophages in Atherosclerosis Regression. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 20–33. [Google Scholar] [CrossRef]
- Mundy, G.R. The effects of TGF-beta on bone. Ciba Found Symp. 1991, 157, 137–151. [Google Scholar]
- Erlebacher, A.; Filvaroff, E.H.; Ye, J.-Q.; Derynck, R. Osteoblastic Responses to TGF-β during Bone Remodeling. Mol. Biol. Cell 1998, 9, 1903–1918. [Google Scholar] [CrossRef] [PubMed]
- Shapouri-Moghaddam, A.; Mohammadian, S.; Vazini, H.; Taghadosi, M.; Esmaeili, S.-A.; Mardani, F.; Seifi, B.; Mohammadi, A.; Afshari, J.T.; Sahebkar, A. Macrophage plasticity, polarization, and function in health and disease. J. Cell. Physiol. 2018, 233, 6425–6440. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Rosenkrans, Z.T.; Wang, J.; Cai, W. PET imaging of macrophages in cardiovascular diseases. Am. J. Transl. Res. 2020, 12, 1491–1514. [Google Scholar] [PubMed]
- Cocker, M.S.; Spence, J.D.; Hammond, R.; Wells, G.; Dekemp, R.A.; Lum, C.; Adeeko, A.; Yaffe, M.J.; Leung, E.; Hill, A.; et al. [18F]-NaF PET/CT Identifies Active Calcification in Carotid Plaque. JACC Cardiovasc. Imaging 2017, 10, 486–488. [Google Scholar] [CrossRef]
- Høilund-Carlsen, P.F.; Sturek, M.; Alavi, A.; Gerke, O. Atherosclerosis imaging with 18F-sodium fluoride PET: State-of-the-art review. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1538–1551. [Google Scholar] [CrossRef]
- Barut, O.; Ahlqvist, J.; Garoff, M.; Johansson, E.; Johansson, M.; Wester, P.; Jäghagen, E.L. Calcifications in the neck region of patients with carotid artery stenosis: A computed tomography angiography study of topographic anatomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Scimeca, M.; Bonfiglio, R.; Urbano, N.; Cerroni, C.; Anemona, L.; Montanaro, M.; Fazi, S.; Schillaci, O.; Mauriello, A.; Bonanno, E. Programmed death ligand 1 expression in prostate cancer cells is associated with deep changes of the tumor inflammatory infiltrate composition. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 297.e19–297.e31. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n (%) or Mean (SD) | |
|---|---|
| Total Age | n = 687 68.8 (6.9) |
| Gender Male Female | 476 (69.3%) 211 (30.7%) |
| Cerebrovascular disease Symptomatic patients Ipsilateral major stroke TIA Asymptomatic patients | 311 (45.3%) 117 (17.0%) 194 (28.2%) 376 (54.7%) |
| Risk factors Hypertension Diabetes Smoking habit Hypercholesterolemia Hypertriglyceridemia Low-HDL | 483 (70.3%) 197 (28.7%) 459 (66.8%) 457 (66.5%) 339 (49.3%) 289 (42.1%) |
| Drugs Statins Diuretics | 412 (60.0) 275 (40.0) |
| Associated vascular disease Previous myocardial infarction Peripheral arterial diseas Aortic aneurysm | 137 (19.9) 185 (26.6) 34 (4.9) |
| Histological type of carotid plaque Stable plaques Unstable plaques Thrombotic plaque With a thrombus in organization TCFA Calcified nodule | 339 (49.3%) 348 (50.7%) 117 (17.0) 126 (18.3%) 84 (12.2%) 21 (3.1%) |
| Absence of Calcification n = 318 | Presence of Calcification n = 369 | Univariate Analysis p | Multivariate Analysis p | |
|---|---|---|---|---|
| Age, mean (SD) | 68.3 (6.9) | 69.4 (6.7) | 0.25 | 0.07 |
| Gender Male Female | 237 (74.5%) 81 (25.5%) | 239 (64.8%) 130 (35.2%) | 0.11 | 0.05 |
| Hypertension | 211 (66.3%) | 261 (70.7%) | 0.51 | 0.51 |
| Diabetes | 94 (29.6%) | 98 (26.6%) | 0.71 | 0.84 |
| Smoking habit | 201 (63.2%) | 246 (66.7%) | 0.31 | 0.82 |
| Hypercholesterolemia | 209 (65.7%) | 234 (63.4%) | 0.86 | 0.10 |
| Hypertriglyceridemia | 138 (43.4%) | 190 (51.5%) | 0.29 | 0.97 |
| Low HDL Statins | 118 (37.1%) 189 (59.4%) | 166 (45.0%) 223 (60.4%) | 0.19 0.67 | 0.13 0.12 |
| Microcalcification n= 152 | Macrocalcification n= 217 | Univariate Analysis p | Multivariate Analysis p | |
|---|---|---|---|---|
| Age, mean (SD) | 69.7 (7.5) | 69.1 (6.4) | 0.59 | 0.11 |
| Gender Male Female | 107 (7046%) 45 (29.6%) | 132 (60.8%) 85 (39.2%) | 0.07 | 0.35 |
| Hypertension | 105 (69.1%) | 156 (71.9%) | 0.69 | 0.84 |
| Diabetes | 42 (27.6%) | 56 (25.8%) | 0.81 | 0.24 |
| Smoking habit | 103 (67.8%) | 143 (65.9%) | 0.80 | 0.25 |
| Hypercholesterolemia | 99 (65.1%) | 135 (62.1%) | 0.77 | 0.96 |
| Hypertriglyceridemia | 77 (51.7%) | 113 (52.1%) | 0.91 | 0.60 |
| Low HDL Statins | 73 (48.0%) 93 (61.2%) | 93 (42.9%) 130 (59.9%) | 0.63 0.74 | 0.89 0.35 |
| Microcalcification | Macrocalcification | p-Value | |
|---|---|---|---|
| CD86 | 2.28 + 0.82 | 8.22 + 2.28 | 0.02 |
| CD163 | 11.60 + 3.91 | 33.56 + 7.55 | 0.01 |
| CD44 | 6.17 + 3.12 | 3.40 + 0.95 | 0.41 |
| CD53 | 53.62 + 13.72 | 52.70 + 7.57 | 0.95 |
| CD57 | 4.61 + 2.82 | 4.13 + 1.26 | 0.88 |
| CD197 | 3.04 + 1.80 | 0.95 + 0.19 | 0.27 |
| IL2 | 30.39 + 8.54 | 47.80 + 7.84 | 0.14 |
| IL6 | 48.15 + 11.54 | 65.13 + 6.70 | 0.22 |
| IL10 | 8.62 + 7.38 | 5.23 + 1.59 | 0.66 |
| IL17 | 19.88 + 7.20 | 31.21 + 6.38 | 0.25 |
| IL23 | 12.2 + 7.4 | 29.6 + 4.8 | 0.06 |
| TGF-β | 10.09 + 5.50 | 24.37 + 4.00 | 0.04 |
| Antibody | Characteristics | Antigen Retrieval and Dilution |
|---|---|---|
| CD3 | Rabbit Monoclonal, clone 2GV6; Ventana, Tucson, AZ, USA | pH 7.8, 1:100 |
| CD68 | Rabbit Monoclonal, clone KP-1; Ventana, Tucson, AZ, USA | pH 7.8, 1:100 |
| CD86 | Rabbit Monoclonal, clone C86/2160R (ab234401); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| CD163 | Rabbit Monoclonal, clone EPR19518 (ab182422); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| CD44 | Rabbit Monoclonal, clone EPR18668 (ab189524); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| CD53 | Rabbit Monoclonal, clone EPR4342(2), (ab134094); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| CD57 | Mouse Monoclonal, clone NK-1 (ab233872); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| CD197 | Rabbit Monoclonal, clone EPR23192-57 (ab253187), Abcam, Cambridge, UK | pH 7.8, 1:100 |
| IL2 | Rabbit Monoclonal, clone EPR6452 (ab205859); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| IL6 | Mouse Monoclonal (ab9324); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| IL10 | Rabbit Polyclonal (ab34843); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| IL17 | Rabbit Polyclonal (ab9565); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| IL23 | Rabbit Polyclonal (ab45420); Abcam, Cambridge, UK | pH 7.8, 1:100 |
| TGF-β | Rabbit Monoclonal, clone EPR21143 (ab215715); Abcam, Cambridge, UK | pH 7.8, 1:100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montanaro, M.; Scimeca, M.; Anemona, L.; Servadei, F.; Giacobbi, E.; Bonfiglio, R.; Bonanno, E.; Urbano, N.; Ippoliti, A.; Santeusanio, G.; et al. The Paradox Effect of Calcification in Carotid Atherosclerosis: Microcalcification Is Correlated with Plaque Instability. Int. J. Mol. Sci. 2021, 22, 395. https://doi.org/10.3390/ijms22010395
Montanaro M, Scimeca M, Anemona L, Servadei F, Giacobbi E, Bonfiglio R, Bonanno E, Urbano N, Ippoliti A, Santeusanio G, et al. The Paradox Effect of Calcification in Carotid Atherosclerosis: Microcalcification Is Correlated with Plaque Instability. International Journal of Molecular Sciences. 2021; 22(1):395. https://doi.org/10.3390/ijms22010395
Chicago/Turabian StyleMontanaro, Manuela, Manuel Scimeca, Lucia Anemona, Francesca Servadei, Erica Giacobbi, Rita Bonfiglio, Elena Bonanno, Nicoletta Urbano, Arnaldo Ippoliti, Giuseppe Santeusanio, and et al. 2021. "The Paradox Effect of Calcification in Carotid Atherosclerosis: Microcalcification Is Correlated with Plaque Instability" International Journal of Molecular Sciences 22, no. 1: 395. https://doi.org/10.3390/ijms22010395
APA StyleMontanaro, M., Scimeca, M., Anemona, L., Servadei, F., Giacobbi, E., Bonfiglio, R., Bonanno, E., Urbano, N., Ippoliti, A., Santeusanio, G., Schillaci, O., & Mauriello, A. (2021). The Paradox Effect of Calcification in Carotid Atherosclerosis: Microcalcification Is Correlated with Plaque Instability. International Journal of Molecular Sciences, 22(1), 395. https://doi.org/10.3390/ijms22010395