Naltrexone Use in Treating Hypersexuality Induced by Dopamine Replacement Therapy: Impact of OPRM1 A/G Polymorphism on Its Effectiveness

 ,
, 
Abstract
1. Introduction
2. Material and Methods
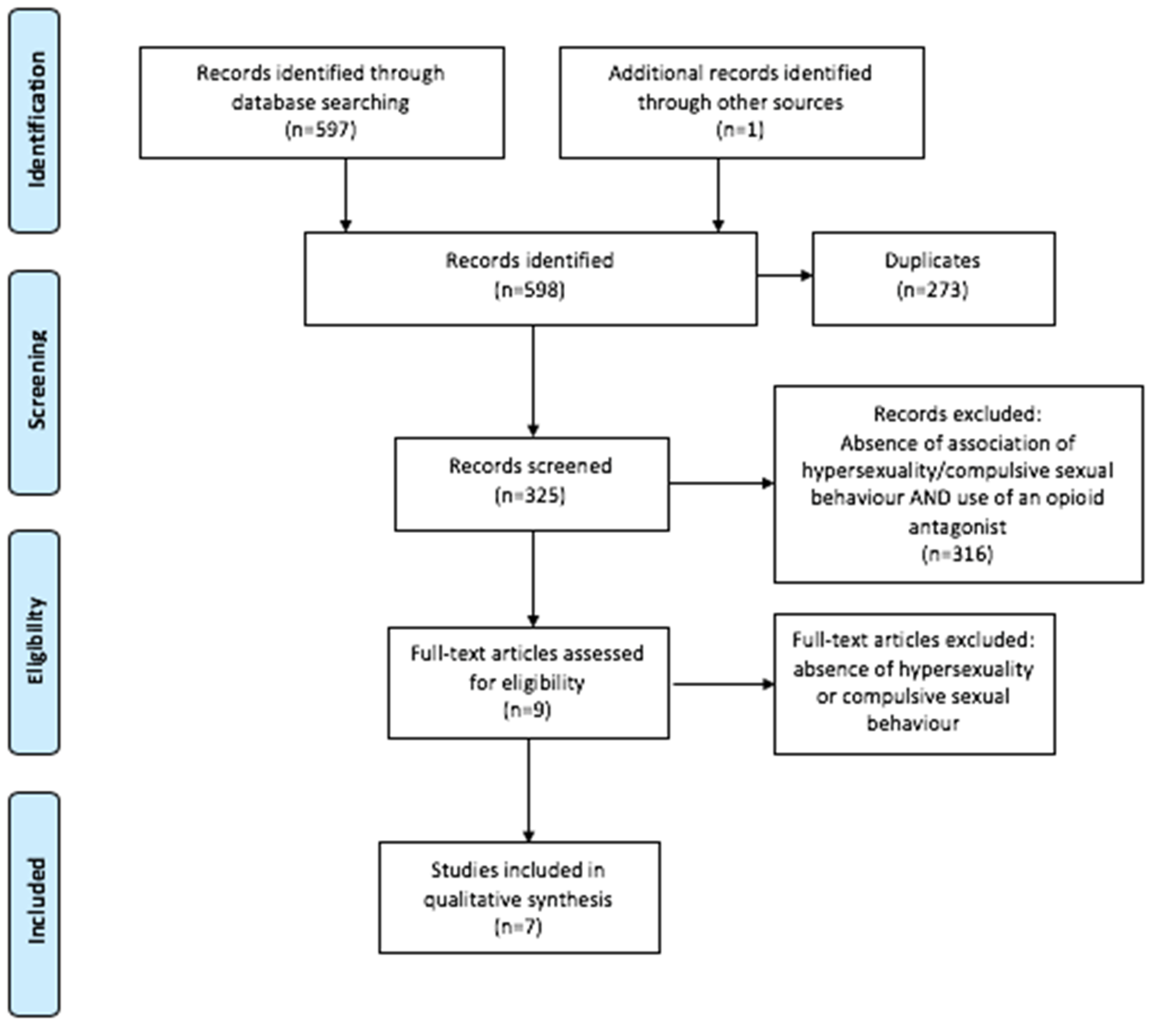
2.1. Systematic Review
2.1.1. Search Strategy
2.1.2. Eligibility Criteria
- The targeted problem was hypersexuality;
- The medication was an opioid antagonist;
- The article involved human beings; and
- The full article was either in English or French.
2.1.3. Article Selection
2.1.4. Data Extraction
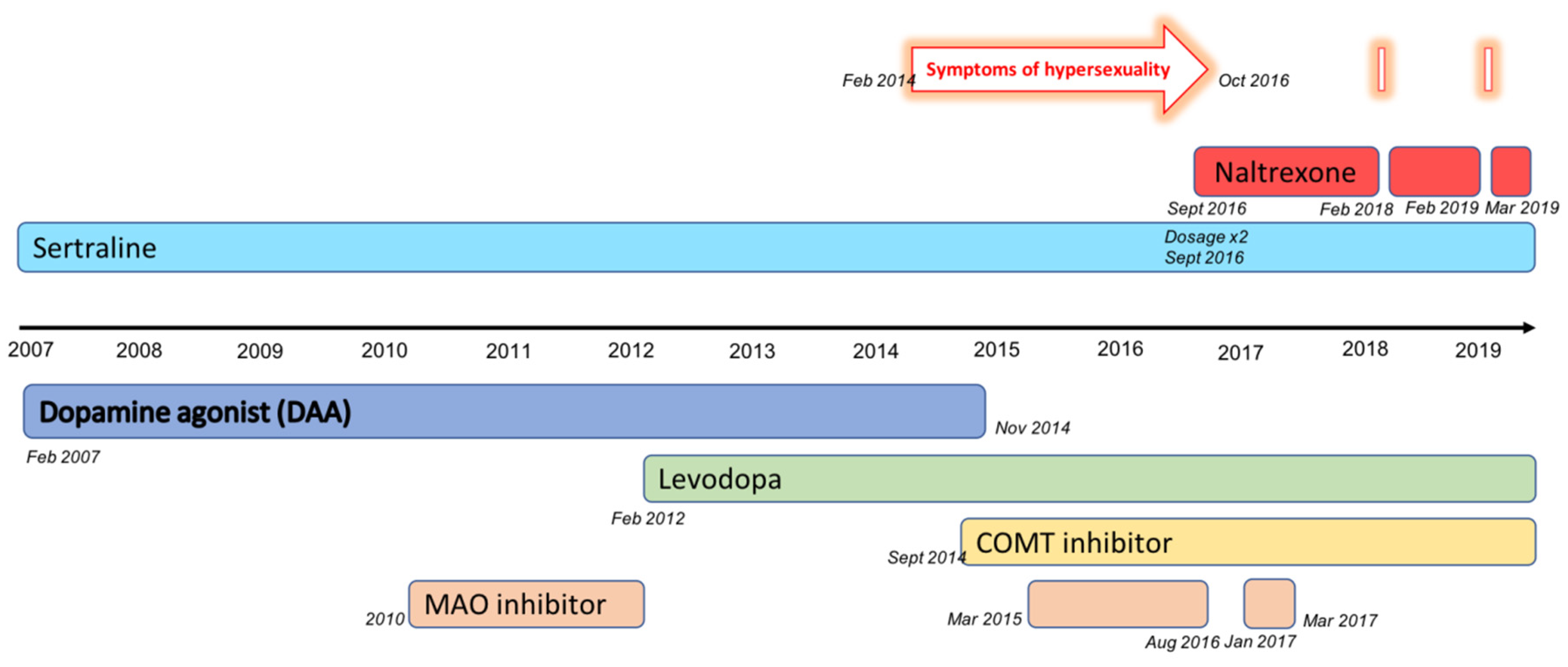
2.2. Case Report
3. Results
3.1. Systematic Review
3.2. Case Presentation
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CBT | Cognitive and behavioral therapy |
| DAA | Dopamine agonist |
| DOR | Delta opioid receptor |
| DSM-IV | Diagnostic and statistical manual, fourth edition |
| DRT | Dopamine replacement therapy |
| ICD | Impulse control disorder |
| COMT | Catechol-O-methyltransferase |
| KOR | Kappa opioid receptor |
| MAO | Monoamine oxidase |
| MeSH | Medical subject heading |
| MOR | Mu opioid receptor |
| OPRM1 | Opioid receptor mu 1 |
| PD | Parkinson’s disease |
| PRISMA | Preferred reporting items for systematic reviews and meta-analyses |
| SNP | Single nucleotide polymorphism |
References
- Grall-Bronnec, M.; Victorri-Vigneau, C.; Donnio, Y.; Leboucher, J.; Rousselet, M.; Thiabaud, E.; Zreika, N.; Derkinderen, P.; Challet-Bouju, G. Dopamine Agonists and Impulse Control Disorders: A Complex Association. Drug Saf. 2018, 41, 19–75. [Google Scholar] [CrossRef]
- Gatto, E.M.; Aldinio, V. Impulse Control Disorders in Parkinson’s Disease. A Brief and Comprehensive Review. Front. Neurol. 2019, 10, 351. [Google Scholar] [CrossRef]
- Weintraub, D.; Potenza, M.N. Impulse Control Disorders in Parkinson’s Disease. Curr. Neurol. Neurosci. Rep. 2006, 6, 302–306. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, D.; Claassen, D.O. Impulse Control and Related Disorders in Parkinson’s Disease. In International Review of Neurobiology; Elsevier: Amsterdam, The Netherlands, 2017; Volume 133, pp. 679–717. [Google Scholar]
- Voon, V.; Fernagut, P.-O.; Wickens, J.; Baunez, C.; Rodriguez, M.; Pavon, N.; Juncos, J.L.; Obeso, J.A.; Bezard, E. Chronic Dopaminergic Stimulation in Parkinson’s Disease: From Dyskinesias to Impulse Control Disorders. Lancet Neurol. 2009, 8, 1140–1149. [Google Scholar] [CrossRef]
- Atmaca, M. Drug-Induced Impulse Control Disorders: A Review. Curr. Clin. Pharmacol. 2014, 9, 70–74. [Google Scholar] [CrossRef]
- Nakum, S.; Cavanna, A.E. The Prevalence and Clinical Characteristics of Hypersexuality in Patients with Parkinson’s Disease Following Dopaminergic Therapy: A Systematic Literature Review. Parkinsonism Relat. Disord. 2016, 25, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Aarons, S.; Peisah, C.; Wijeratne, C. Neuropsychiatric Effects of Parkinson’s Disease Treatment: Psychiatric Effects Parkinson’s Treatment. Australas. J. Ageing 2012, 31, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Papay, K.; Xie, S.X.; Stern, M.; Hurtig, H.; Siderowf, A.; Duda, J.E.; Minger, J.; Weintraub, D. Naltrexone for Impulse Control Disorders in Parkinson Disease. Neurology 2014, 83, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Voon, V.; Napier, T.C.; Frank, M.J.; Sgambato-Faure, V.; Grace, A.A.; Rodriguez-Oroz, M.; Obeso, J.; Bezard, E.; Fernagut, P.-O. Impulse Control Disorders and Levodopa-Induced Dyskinesias in Parkinson’s Disease: An Update. Lancet Neurol. 2017, 16, 238–250. [Google Scholar] [CrossRef]
- Maréchal, E.; Denoiseux, B.; Thys, E.; Crosiers, D.; Pickut, B.; Cras, P. Impulse Control Disorders in Parkinson’s Disease: An Overview from Neurobiology to Treatment. J. Neurol. 2015, 262, 7–20. [Google Scholar] [CrossRef]
- Bosco, D.; Plastino, M.; Colica, C.; Bosco, F.; Arianna, S.; Vecchio, A.; Galati, F.; Cristiano, D.; Consoli, A.; Consoli, D. Opioid Antagonist Naltrexone for the Treatment of Pathological Gambling in Parkinson Disease. Clin. Neuropharmacol. 2012, 35, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Barone, P.; Trojano, L.; Vitale, C. Pathological Gambling in Parkinson’s Disease. A Comprehensive Review. Parkinsonism Relat. Disord. 2013, 19, 645–653. [Google Scholar] [CrossRef]
- Kovanen, L.; Basnet, S.; Castrén, S.; Pankakoski, M.; Saarikoski, S.T.; Partonen, T.; Alho, H.; Lahti, T. A Randomised, Double-Blind, Placebo-Controlled Trial of As-Needed Naltrexone in the Treatment of Pathological Gambling. Eur. Addict. Res. 2016, 22, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Garbutt, J.C.; Greenblatt, A.M.; West, S.L.; Morgan, L.C.; Kampov-Polevoy, A.; Jordan, H.S.; Bobashev, G.V. Clinical and Biological Moderators of Response to Naltrexone in Alcohol Dependence: A Systematic Review of the Evidence: Moderators of Naltrexone Response. Addiction 2014, 109, 1274–1284. [Google Scholar] [CrossRef]
- Chamorro, A.-J.; Marcos, M.; Mirón-Canelo, J.-A.; Pastor, I.; González-Sarmiento, R.; Laso, F.-J. Association of Μ-Opioid Receptor (OPRM1) Gene Polymorphism with Response to Naltrexone in Alcohol Dependence: A Systematic Review and Meta-Analysis: Naltrexone and A118G OPRM1. Addict. Biol. 2012, 17, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Piquet-Pessôa, M.; Fontenelle, L.F. Opioid Antagonists in Broadly Defined Behavioral Addictions: A Narrative Review. Expert Opin. Pharmacother. 2016, 17, 835–844. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W. Opioid Antagonists in the Treatment of Impulse-Control Disorders. J. Clin. Psychiatry 1998, 59, 165–171. [Google Scholar] [CrossRef]
- Soyka, M.; Rösner, S. Opioid Antagonists for Pharmacological Treatment of Alcohol Dependence—A Critical Review. Curr. Drug Abuse Rev. 2008, 1, 280–291. [Google Scholar] [CrossRef]
- Weintraub, D. Dopamine and Impulse Control Disorders in Parkinson’s Disease. Ann. Neurol. 2008, 64 (Suppl. 2), S93–S100. [Google Scholar] [CrossRef]
- Kalivas, P.W.; Volkow, N.D. The Neural Basis of Addiction: A Pathology of Motivation and Choice. Am. J. Psychiatry 2005, 162, 1403–1413. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A. Neurobiology of Addiction. Biochem. Pharmacol. 2008, 75, 266–322. [Google Scholar] [CrossRef] [PubMed]
- Aboujaoude, E.; Salame, W.O. Naltrexone: A Pan-Addiction Treatment? CNS Drugs 2016, 30, 719–733. [Google Scholar] [CrossRef] [PubMed]
- Nelis, E.A.; Berendse, H.W.; van den Heuvel, O.A. Hypersexuality and other impulse control disorders in Parkinson’s disease. Ned. Tijdschr. Geneeskd. 2016, 160, A9359. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), 4th ed.; American Psychiatric Association: Arlington, VA, USA, 2000; Volume 1. [Google Scholar]
- Goodman, A. Sexual Addiction: Designation and Treatment. J. Sex Marital Ther. 1992, 18, 303–314. [Google Scholar] [CrossRef]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A Method for Estimating the Probability of Adverse Drug Reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef]
- Moore, T.J.; Glenmullen, J.; Mattison, D.R. Reports of Pathological Gambling, Hypersexuality, and Compulsive Shopping Associated with Dopamine Receptor Agonist Drugs. JAMA Intern. Med. 2014, 174, 1930–1933. [Google Scholar] [CrossRef]
- Reyes, D.; Kurako, K.; Galvez-Jimenez, N. Rasagiline Induced Hypersexuality in Parkinson’s Disease. J. Clin. Neurosci. Off. J. Neurosurg. Soc. Australas. 2014, 21, 507–508. [Google Scholar] [CrossRef]
- Potenza, M.N.; Balodis, I.M.; Derevensky, J.; Grant, J.E.; Petry, N.M.; Verdejo-Garcia, A.; Yip, S.W. Gambling Disorder. Nat. Rev. Dis. Primer 2019, 5, 1–21. [Google Scholar] [CrossRef]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Perez Lloret, S.; Weintraub, D.; Sampaio, C. Update on Treatments for Nonmotor Symptoms of Parkinson’s Disease—An Evidence-based Medicine Review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurobiology of Addiction: A Neurocircuitry Analysis. Lancet Psychiatry 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Darcq, E.; Kieffer, B.L. Opioid Receptors: Drivers to Addiction? Nat. Rev. Neurosci. 2018, 19, 499–514. [Google Scholar] [CrossRef] [PubMed]
- Fields, H.L.; Margolis, E.B. Understanding Opioid Reward. Trends Neurosci. 2015, 38, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Carroll, F.I.; Carlezon, W.A. Development of Kappa Opioid Receptor Antagonists. J. Med. Chem. 2013, 56, 2178–2195. [Google Scholar] [CrossRef] [PubMed]
- Schlosburg, J.E.; Whitfield, T.W.; Park, P.E.; Crawford, E.F.; George, O.; Vendruscolo, L.F.; Koob, G.F. Long-Term Antagonism of κ Opioid Receptors Prevents Escalation of and Increased Motivation for Heroin Intake. J. Neurosci. 2013, 33, 19384–19392. [Google Scholar] [CrossRef]
- Srisurapanont, M.; Jarusuraisin, N. Naltrexone for the Treatment of Alcoholism: A Meta-Analysis of Randomized Controlled Trials. Int. J. Neuropsychopharmacol. 2005, 8, 267–280. [Google Scholar] [CrossRef]
- Kranzler, H.R. Efficacy of Naltrexone and Acamprosate for Alcoholism Treatment: A Meta-Analysis. Alcohol. Clin. Exp. Res. 2001, 25, 1335–1341. [Google Scholar] [CrossRef]
- Bouza, C.; Angeles, M.; Magro, A.; Muñoz, A.; Amate, J.M. Efficacy and Safety of Naltrexone and Acamprosate in the Treatment of Alcohol Dependence: A Systematic Review. Addict. Abingdon Engl. 2004, 99, 811–828. [Google Scholar]
- Bostwick, J.M.; Bucci, J.A. Internet Sex Addiction Treated with Naltrexone. Mayo Clin. Proc. 2008, 83, 226–230. [Google Scholar] [CrossRef]
- Raymond, N.C.; Grant, J.E.; Coleman, E. Augmentation with Naltrexone to Treat Compulsive Sexual Behavior: A Case Series. Ann. Clin. Psychiatry Off. J. Am. Acad. Clin. Psychiatr. 2010, 22, 56–62. [Google Scholar]
- Rodriguez-Oroz, M.C.; Jahanshahi, M.; Krack, P.; Litvan, I.; Macias, R.; Bezard, E.; Obeso, J.A. Initial Clinical Manifestations of Parkinson’s Disease: Features and Pathophysiological Mechanisms. Lancet Neurol. 2009, 8, 1128–1139. [Google Scholar] [CrossRef]
- Connolly, B.S.; Lang, A.E. Pharmacological Treatment of Parkinson Disease: A Review. JAMA 2014, 311, 1670. [Google Scholar] [CrossRef] [PubMed]
- Oroszi, G.; Anton, R.F.; O’Malley, S.; Swift, R.; Pettinati, H.; Couper, D.; Yuan, Q.; Goldman, D. OPRM1 Asn40Asp Predicts Response to Naltrexone Treatment: A Haplotype-Based Approach. Alcohol. Clin. Exp. Res. 2009, 33, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Hoehe, M.R.; Köpke, K.; Wendel, B.; Rohde, K.; Flachmeier, C.; Kidd, K.K.; Berrettini, W.H.; Church, G.M. Sequence Variability and Candidate Gene Analysis in Complex Disease: Association of Mu Opioid Receptor Gene Variation with Substance Dependence. Hum. Mol. Genet. 2000, 9, 2895–2908. [Google Scholar] [CrossRef]
- Crist, R.C.; Berrettini, W.H. Pharmacogenetics of OPRM1. Pharmacol. Biochem. Behav. 2014, 123, 25–33. [Google Scholar] [CrossRef]
- Arias, A.; Feinn, R.; Kranzler, H.R. Association of an Asn40Asp (A118G) Polymorphism in the Mu-Opioid Receptor Gene with Substance Dependence: A Meta-Analysis. Drug Alcohol Depend. 2006, 83, 262–268. [Google Scholar] [CrossRef]
- Coller, J.K.; Beardsley, J.; Bignold, J.; Li, Y.; Merg, F.; Sullivan, T.; Cox, T.C.; Somogyi, A.A. Lack of Association between the A118G Polymorphism of the Mu Opioid Receptor Gene (OPRM1) and Opioid Dependence: A Meta-Analysis. Pharm. Pers. Med. 2009, 2, 9–19. [Google Scholar]
- Glatt, S.J.; Bousman, C.; Wang, R.S.; Murthy, K.K.; Rana, B.K.; Lasky-Su, J.A.; Zhu, S.C.; Zhang, R.; Li, J.; Zhang, B.; et al. Evaluation of OPRM1 Variants in Heroin Dependence by Family-Based Association Testing and Meta-Analysis. Drug Alcohol Depend. 2007, 90, 159–165. [Google Scholar] [CrossRef]
- Chen, D.; Liu, L.; Xiao, Y.; Peng, Y.; Yang, C.; Wang, Z. Ethnic-Specific Meta-Analyses of Association between the OPRM1 A118G Polymorphism and Alcohol Dependence among Asians and Caucasians. Drug Alcohol Depend. 2012, 123, 1–6. [Google Scholar] [CrossRef]
- Schwantes-An, T.-H.; Zhang, J.; Chen, L.-S.; Hartz, S.M.; Culverhouse, R.C.; Chen, X. Association of the OPRM1 Variant Rs1799971 (A118G) with Non-Specific Liability to Substance Dependence in a Collaborative de Novo Meta-Analysis of European-Ancestry Cohorts. Behav. Genet. 2016, 46, 151–169. [Google Scholar] [CrossRef]
- Cormier-Dequaire, F.; Bekadar, S.; Anheim, M.; Lebbah, S. Suggestive Association between OPRM1 and Impulse Control Disorders in Parkinson’s Disease: OPRM1 AND ICDS IN PARKINSON’S DISEASE. Mov. Disord. 2018, 33, 1878–1886. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-G.; Kim, C.-M.; Choi, S.-W.; Jae, Y.-M.; Lee, H.-G.; Son, B.-K.; Kim, J.-G.; Choi, Y.-S.; Kim, H.-O.; Kim, S.-Y.; et al. A Mu Opioid Receptor Gene Polymorphism (A118G) and Naltrexone Treatment Response in Adherent Korean Alcohol-Dependent Patients. Psychopharmacology 2008, 201, 611. [Google Scholar] [CrossRef] [PubMed]
- Oslin, D.W.; Berrettini, W.; Kranzler, H.R.; Pettinati, H.; Gelernter, J.; Volpicelli, J.R.; O’Brien, C.P. A Functional Polymorphism of the Mu-Opioid Receptor Gene Is Associated with Naltrexone Response in Alcohol-Dependent Patients. Neuropsychopharmacology 2003, 28, 1546–1552. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Title, Authors, Date | Study Design | Sample Size | Characteristics of Participants | Objectives | Methods | Results |
|---|---|---|---|---|---|---|
| A case of kleptomania and compulsive sexual behavior treated with naltrexone Grant, J.E., Kim, S.W. 2001 | Case report | n = 1 | Male patient, 58 years old. Kleptomania since he was 11, and compulsive sexual behavior since his fifties. Antidepressants and psychotherapy for 10 years were ineffective. | (-) | Disappearance with naltrexone of his urges to steal and to have sex (from 25 mg to 150 mg per day). Relapse at the same intensity as before 3 days after the discontinuation of treatment, with a remission 4 days after restarting naltrexone. Stability for the 20 weeks of follow-up with 150 mg of naltrexone per day. Naltrexone was well tolerated. No data about genetics. | |
| Treatment of compulsive sexual behavior with naltrexone and serotonin reuptake inhibitors: two case studies Raymond, N.C., Grant, J.E., Kim, S.W. 2002 | Case report | n = 2 | Case 1: A 42 year old woman reporting compulsive sexual behavior, associated with depression and anxiety symptoms. She had an history of cocaine use disorder. Fluoxetine (60 mg/day) was effective on depression and anxiety symptoms but not on sexual urges. Case 2: A 62 year old male reporting intermittent compulsive sexual behavior for 20 years. Several antidepressants were ineffective on sexual urges (fluoxetine, bupropion, citalopram, buspirone). | (-) | Case 1: Decrease of compulsive sexual behavior 2 weeks after naltrexone initiation (50 mg/day) and almost complete remission of sexual urges at 100 mg/day. Naltrexone was well tolerated. No data about genetics. Case 2: Diminution of intrusive thoughts about sex and control over compulsive sexual behavior after one month with naltrexone (50 mg/day). Remission for the 8 months of follow-up with 100 mg of naltrexone per day. Naltrexone was well tolerated. No data about genetics. | |
| Naltrexone in the treatment of adolescent sexual offenders Ryback, R.S. 2004 | Open-ended prospective study | n = 21 | Male adolescents participating in an inpatient adolescent sexual offenders’ program. Inclusion criteria: Masturbating ≥3 times per day; feeling unable to control arousal; spending more than 30% of awake time in sexual fantasies; or interfering in their functioning | To investigate whether naltrexone can decrease sexual arousal | Naltrexone was given for 2 months to all participants, then stopped for 13 of them (according to the initial study design). Monitoring was made using a fantasy-tracking log and a masturbation log. Outcome: over 30% decrease in any self-reported criterion for at least 4 months | Significant clinical improvement for 15 out of 21 patients, with an average dose of 160 mg/day. Dosages above 200 mg/day were not more useful. Discontinuation of naltrexone in 13 of the patients resulted in the reoccurrence of symptoms. No data about genetics. |
| Internet sex addiction treated with Naltrexone Bostwick, J.M., Bucci, J.A. 2008 | Case report | n = 1 | Male patient who first met a psychiatrist for sexual addiction at age 24 and was followed for 7 years. Diagnosis of sexual addiction defined as compulsive sexual behavior persisting despite serious negative consequences. Antidepressant, individual, and group psychotherapy were ineffective. | (-) | Nearly complete remission for more than three years (time of follow-up) with naltrexone from 50 mg to 150 mg per day. Naltrexone was well tolerated. No data about genetics. | |
| Augmentation with naltrexone to treat compulsive sexual behavior: a case series Raymond, N.C., Grant, J.E., Coleman, E. 2010 | Retrospective study | n = 19 | Male outpatients with compulsive sexual behavior consulting in a sexual health clinic in Minnesota. | To investigate whether naltrexone can reduce urges and compulsive sexual behavior | Treatment with naltrexone. Assessment with a Clinical Global Impression (CGI) scale. | Reduction in compulsive sexual behavior for 17 out of 19 patients (CGI score of 1 or 2, “very much improved” or “much improved”). Mean effective dose for the 17 patients was 104 (+/− 41) mg per day. Naltrexone was well tolerated. No data about genetics. |
| Treatment of compulsive pornography use with naltrexone: a case report Kraus, S.W., Meshberg-Cohen, S. 2015 | Case report | n = 1 | Male in his thirties with compulsive masturbation to pornography with numerous failed attempts to quit. Effectiveness of several weeks of cognitive-behavioral therapy (CBT) on his use of pornography (−70%) but not on sexual urges. | (-) | Initiation of naltrexone 50 mg/day after 10 weeks of CBT was more effective on craving, with an associated decrease in pornography use. No data about genetics. | |
| Compulsive sexual behaviors treated with naltrexone monotherapy Camacho, M., Moura, A.M., Oliveira-Maia, A.J. 2018 | Case report | n = 1 | 27 year old man with compulsive sexual behaviors (significant amount of time and money spent for his fantasies, loss of control, associated with anxiety and depression symptoms). Antidepressants, mood stabilizers, and neuroleptics were ineffective. | (-) | Treatment with fluoxetine and aripiprazole at the time of inclusion. Reduction of sexual fantasies and control increase with naltrexone 50 mg/day and nearly complete remission for 10 months with naltrexone 100 mg/day. Naltrexone was well tolerated. No data about genetics. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verholleman, A.; Victorri-Vigneau, C.; Laforgue, E.; Derkinderen, P.; Verstuyft, C.; Grall-Bronnec, M. Naltrexone Use in Treating Hypersexuality Induced by Dopamine Replacement Therapy: Impact of OPRM1 A/G Polymorphism on Its Effectiveness. Int. J. Mol. Sci. 2020, 21, 3002. https://doi.org/10.3390/ijms21083002
Verholleman A, Victorri-Vigneau C, Laforgue E, Derkinderen P, Verstuyft C, Grall-Bronnec M. Naltrexone Use in Treating Hypersexuality Induced by Dopamine Replacement Therapy: Impact of OPRM1 A/G Polymorphism on Its Effectiveness. International Journal of Molecular Sciences. 2020; 21(8):3002. https://doi.org/10.3390/ijms21083002
Chicago/Turabian StyleVerholleman, Audrey, Caroline Victorri-Vigneau, Edouard Laforgue, Pascal Derkinderen, Celine Verstuyft, and Marie Grall-Bronnec. 2020. "Naltrexone Use in Treating Hypersexuality Induced by Dopamine Replacement Therapy: Impact of OPRM1 A/G Polymorphism on Its Effectiveness" International Journal of Molecular Sciences 21, no. 8: 3002. https://doi.org/10.3390/ijms21083002
APA StyleVerholleman, A., Victorri-Vigneau, C., Laforgue, E., Derkinderen, P., Verstuyft, C., & Grall-Bronnec, M. (2020). Naltrexone Use in Treating Hypersexuality Induced by Dopamine Replacement Therapy: Impact of OPRM1 A/G Polymorphism on Its Effectiveness. International Journal of Molecular Sciences, 21(8), 3002. https://doi.org/10.3390/ijms21083002