A Tetra-Panel of Serum Circulating miRNAs for the Diagnosis of the Four Most Prevalent Tumor Types

 and
and 
Abstract
1. Introduction
2. Results
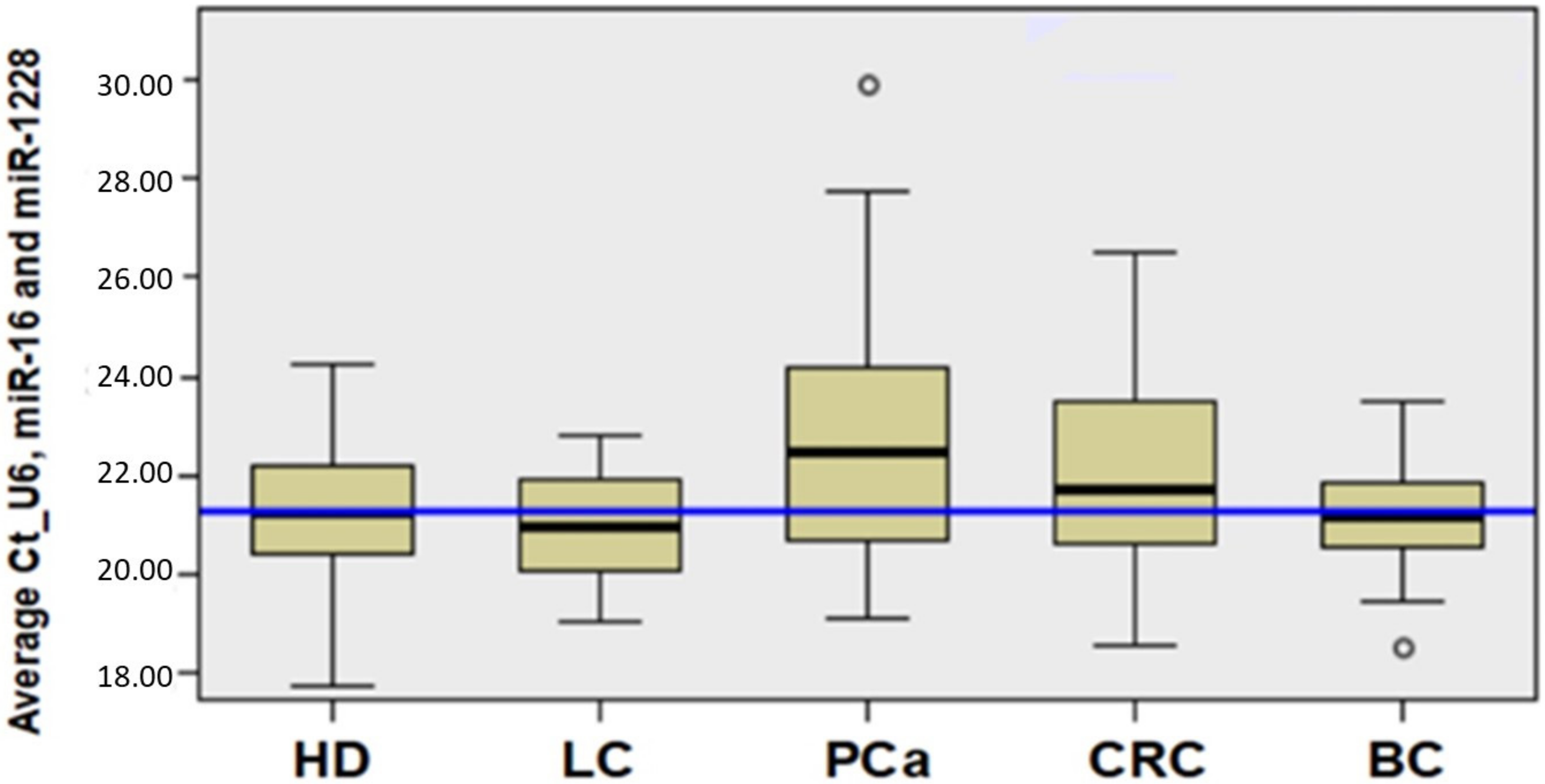
2.1. Average of Expression Levels of Housekeeping Genes U6snRNA, miRNA-16, and miRNA-1228 as Reference in the Serum of HDs and Cancer Patients
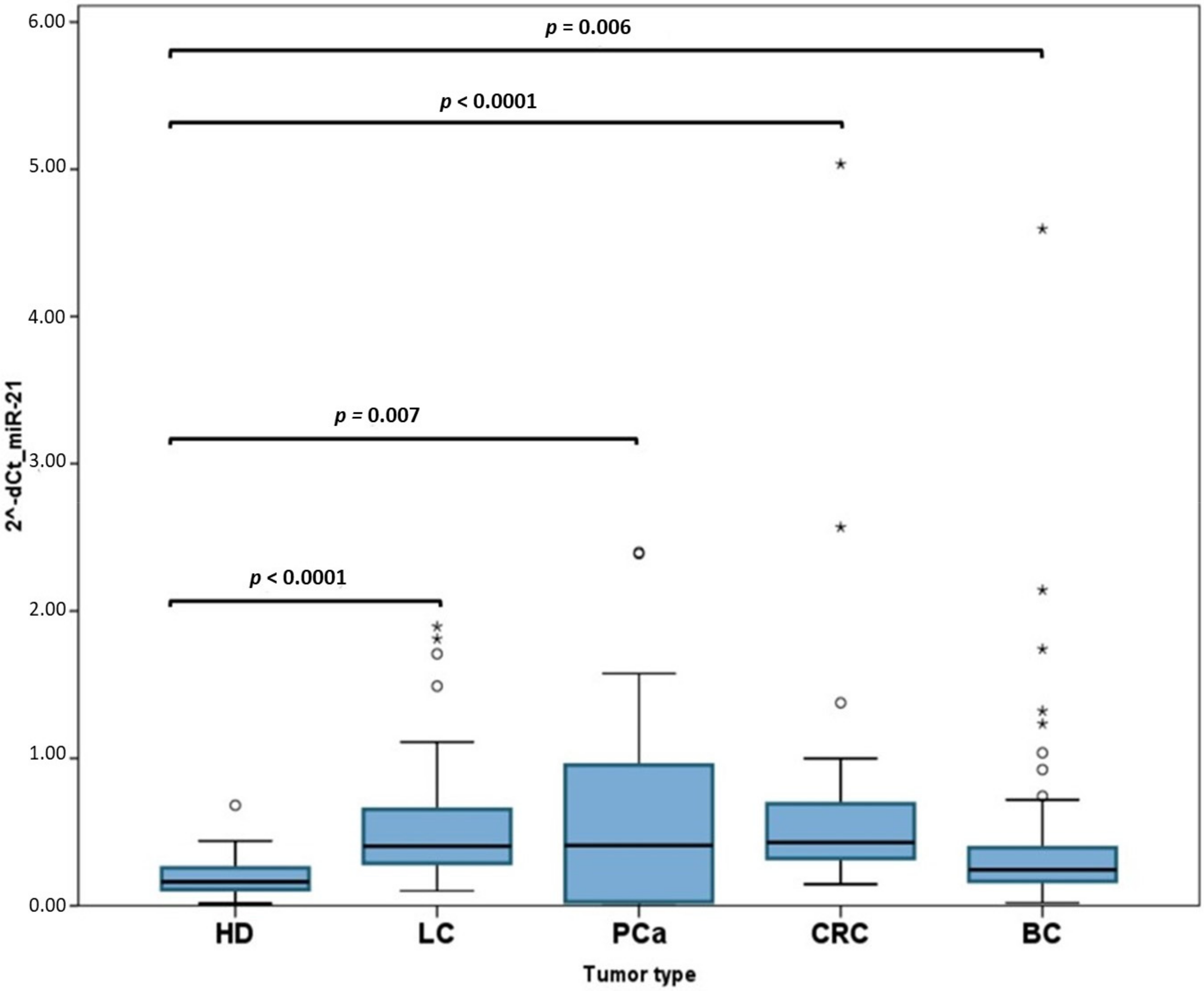
2.2. Analysis of miR-21
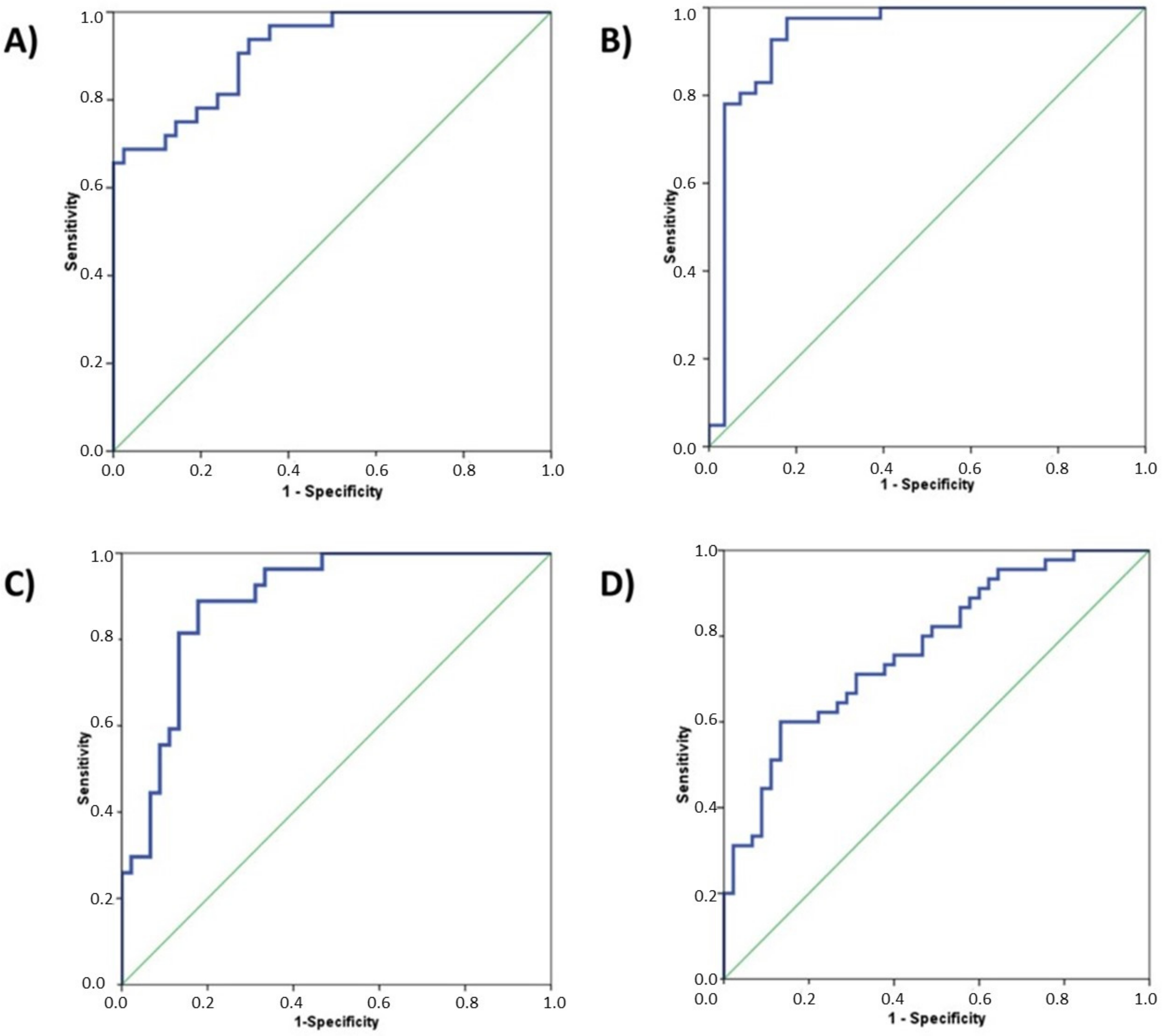
2.3. Definition of Circulating miRNA Panels to Identify Cancer Patients
2.4. Multivariate Analysis
2.5. Analysis of Variation of the Tumor-Selected Circulating-miRNA Depending on Tumor Stage
3. Discussion
4. Patients and Methods
4.1. Ethics Statement
4.2. Patients’ Characteristics
4.3. MiRNAs Selection for Each Tumor Type
4.4. Blood Collection and RNA Extraction
4.5. Conversion of total RNA into cDNA
4.6. cDNA Pre-Amplification
4.7. Quantification of Circulating miRNAs by Quantitative Reverse Transcription-Polymerase Chain Reaction (qRT-PCR)
4.8. Statistical Analysis
4.9. miRNA Target-Interactions Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.W.; Tabar, L.; Olsen, A.H.; Vitak, B.; Allgood, P.C.; Chen, T.H.; Yen, A.M.; Smith, R.A. Absolute numbers of lives saved and overdiagnosis in breast cancer screening, from a randomized trial and from the Breast Screening Programme in England. J. Med. Screen. 2010, 17, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Ozturk, M.A.; Moschetta, M.; Karathanasi, A.; Zakynthinakis-Kyriakou, N.; Katsanos, K.H.; Christodoulou, D.K.; Pavlidis, N. The Developing Story of Predictive Biomarkers in Colorectal Cancer. J. Pers. Med. 2019, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Huang, D.; Ni, S.; Peng, Z.; Sheng, W.; Du, X. Plasma microRNAs are promising novel biomarkers for early detection of colorectal cancer. Int J. Cancer 2010, 127, 118–126. [Google Scholar] [CrossRef]
- Chen, X.; Ba, Y.; Ma, L.; Cai, X.; Yin, Y.; Wang, K.; Guo, J.; Zhang, Y.; Chen, J.; Guo, X.; et al. Characterization of microRNAs in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef]
- Faraldi, M.; Gomarasca, M.; Sansoni, V.; Perego, S.; Banfi, G.; Lombardi, G. Normalization strategies differently affect circulating miRNA profile associated with the training status. Sci. Rep. 2019, 9, 1584. [Google Scholar] [CrossRef]
- Sanders, I.; Holdenrieder, S.; Walgenbach-Brünagel, G.; von Ruecker, A.; Kristiansen, G.; Müller, S.C.; Ellinger, J. Evaluation of reference genes for the analysis of serum miRNA in patients with prostate cancer, bladder cancer and renal cell carcinoma. Int. J. Urol. 2012, 19, 1017–1025. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Z.; Liao, B.Y.; Yu, L.; Gao, X.; Lu, S.; Wang, S.; Dai, Z.; Zhang, X.; Chen, Q.; et al. Human miR-1228 as a stable endogenous control for the quantification of circulating microRNAs in cancer patients. Int. J. Cancer 2014, 135, 1187–1194. [Google Scholar] [CrossRef]
- Rinnerthaler, G.; Hackl, H.; Gampenrieder, S.P.; Hamacher, F.; Hufnagl, C.; Hauser-Kronberger, C.; Zehentmayr, F.; Fastner, G.; Sedlmayer, F.; Mlineritsch, B.; et al. miR-16-5p Is a Stably-Expressed Housekeeping MicroRNA in Breast Cancer Tissues from Primary Tumors and from Metastatic Sites. Int. J. Mol. Sci. 2016, 17, 156. [Google Scholar] [CrossRef]
- Vanderburgh, D. Breast cancer screening. Politics Life Sci. 2018, 37, 135–140. [Google Scholar] [CrossRef]
- Stewart, R.W.; Lizama, S.; Peairs, K.; Sateia, H.F.; Choi, Y. Screening for prostate cancer. Semin. Oncol. 2017, 44, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Sateia, H.F.; Choi, Y.; Stewart, R.W.; Peairs, K.S. Screening for lung cancer. Semin. Oncol. 2017, 44, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Sateia, H.F.; Peairs, K.S.; Stewart, R.W. Screening for colorectal cancer. Semin. Oncol. 2017, 44, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, J.D.; Fisher, P.G.; Gibbs, P. Early detection of cancer: Past, present, and future. Am. Soc. Clin. Oncol. Educ. Book 2015, 35, 57–65. [Google Scholar] [CrossRef]
- Song, T.; Liang, Y.; Cao, Z.; Du, W.; Li, Y. Computational Analysis of Specific MicroRNA Biomarkers for Noninvasive Early Cancer Detection. Biomed. Res. Int. 2017, 2017, 4680650. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Ryan, B.M.; Robles, A.I.; Harris, C.C. Genetic variation in microRNA networks: The implications for cancer research. Nat. Rev. Cancer 2010, 10, 389–402. [Google Scholar] [CrossRef]
- Calin, G.A.; Dumitru, C.D.; Shimizu, M.; Bichi, R.; Zupo, S.; Noch, E.; Aldler, H.; Rattan, S.; Keating, M.; Rai, K.; et al. Frequent deletions and down-regulation of micro- RNA genes miR15 and miR16 at 13q14 in chronic lymphocytic leukemia. Proc. Natl. Acad. Sci. USA 2002, 99, 15524–15529. [Google Scholar] [CrossRef]
- Esquela-Kerscher, A.; Slack, F.J. Oncomirs-microRNAs with a role in cancer. Nat. Rev. Cancer 2006, 6, 259–269. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, Y.; Jin, X.; Wang, Z.; Wu, Y.; Zhao, D.; Chen, G.; Li, D.; Wang, X.; Cao, H.; et al. A circulating miRNA signature as a diagnostic biomarker for non-invasive early detection of breast cancer. Breast Cancer Res. Treat. 2015, 154, 423–434. [Google Scholar] [CrossRef]
- Wang, S.Y.; Shiboski, S.; Belair, C.D.; Cooperberg, M.R.; Simko, J.P.; Stoppler, H.; Cowan, J.; Carroll, P.R.; Blelloch, R. miR-19, miR-345, miR-519c-5p serum levels predict adverse pathology in prostate cancer patients eligible for active surveillance. PLoS ONE 2014, 9, e98597. [Google Scholar] [CrossRef] [PubMed]
- Nadal, E.; Truini, A.; Nakata, A.; Lin, J.; Reddy, R.M.; Chang, A.C.; Ramnath, N.; Gotoh, N.; Beer, D.G.; Chen, G. A Novel Serum 4-microRNA Signature for Lung Cancer Detection. Sci. Rep. 2015, 5, 12464. [Google Scholar] [CrossRef]
- Hofsli, E.; Sjursen, W.; Prestvik, W.S.; Johansen, J.; Rye, M.; Tranø, G.; Wasmuth, H.H.; Hatlevoll, I.; Thommesen, L. Identification of serum microRNA profiles in colon cancer. Br. J. Cancer 2013, 108, 1712–1719. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Tórtola, Á.; Prats-Quílez, F.; González-Lucas, D.; Bañuls, M.J.; Maquieira, Á.; Wheeler, G.; Dalmay, T.; Griol, A.; Hurtado, J.; Bohlmann, H.; et al. Experimental study of the evanescent-wave photonic sensors response in presence of molecular beacon conformational changes. J. Biophotonics 2018, 11, e201800030. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Tórtola, Á.; Prats-Quílez, F.; González-Lucas, D.; Bañuls, M.J.; Maquieira, Á.; Wheeler, G.; Dalmay, T.; Griol, A.; Hurtado, J.; García-Rupérez, J. High sensitivity and label-free oligonucleotides detection using photonic bandgap sensing structures biofunctionalized with molecular beacon probes. Biomed. Opt. Express 2018, 9, 1717–1727. [Google Scholar] [CrossRef]
- Iorio, M.V.; Ferracin, M.; Liu, C.G.; Veronese, A.; Spizzo, R.; Sabbioni, S.; Magri, E.; Pedriali, M.; Fabbri, M.; Campiglio, M.; et al. MicroRNA gene expression deregulation in human breast cancer. Cancer Res. 2005, 65, 7065–7070. [Google Scholar] [CrossRef]
- Iorio, M.V.; Visone, R.; Di Leva, G.; Donati, V.; Petrocca, F.; Casalini, P.; Taccioli, C.; Volinia, S.; Liu, C.G.; Alder, H.; et al. MicroRNA signatures in human ovarian cancer. Cancer Res. 2007, 67, 8699–8707. [Google Scholar] [CrossRef]
- Asangani, I.A.; Rasheed, S.A.; Nikolova, D.A.; Leupold, J.H.; Colburn, N.H.; Post, S.; Allgayer, H. MicroRNA-21 (miR-21) post-transcriptionally downregulates tumor suppressor Pdcd4 and stimulates invasion, intravasation and metastasis in colorectal cancer. Oncogene 2008, 27, 2128–2136. [Google Scholar] [CrossRef]
- Volinia, S.; Calin, G.A.; Liu, C.G.; Ambs, S.; Cimmino, A.; Petrocca, F.; Visone, R.; Iorio, M.; Roldo, C.; Ferracin, M.; et al. A microRNA expression signature of human solid tumors defines cancer gene targets. Proc. Natl. Acad. Sci. USA 2006, 103, 2257–2261. [Google Scholar] [CrossRef]
- Wu, K.; Li, L.; Li, S. Circulating microRNA-21 as a biomarker for the detection of various carcinomas: An updated meta-analysis based on 36 studies. Tumor Biol. 2015, 36, 1973–1981. [Google Scholar] [CrossRef]
- Halvorsen, A.R.; Bjaanæs, M.; LeBlanc, M.; Holm, A.M.; Bolstad, N.; Rubio, L.; Peñalver, J.C.; Cervera, J.; Mojarrieta, J.C.; López-Guerrero, J.A.; et al. A unique set of 6 circulating microRNAs for early detection of non-small cell lung cancer. Oncotarget 2016, 7, 37250–37259. [Google Scholar] [CrossRef] [PubMed]
- Shaker, O.; Maher, M.; Nassar, Y.; Morcos, G.; Gad, Z. Role of microRNAs -29b-2, -155, -197 and -205 as diagnostic biomarkers in serum of breast cancer females. Gene 2015, 560, 77–82. [Google Scholar] [CrossRef]
- Zhang, H.; Li, B.; Zhao, H.; Chang, J. The expression and clinical significance of serum miR-205 for breast cancer and its role in detection of human cancers. Int. J. Clin. Exp. Med. 2015, 8, 3034–3043. [Google Scholar]
- Sathianathen, N.J.; Kuntz, K.M.; Alarid-Escudero, F.; Lawrentschuk, N.L.; Bolton, D.M.; Murphy, D.G.; Weight, C.J.; Konety, B.R. Incorporating Biomarkers into the Primary Prostate Biopsy Setting: A Cost-Effectiveness Analysis. J. Urol. 2018, 20, 1215–1220. [Google Scholar] [CrossRef]
- Singh, P.K.; Preus, L.; Hu, Q.; Yan, L.; Long, M.D.; Morrison, C.D.; Nesline, M.; Johnson, C.S.; Koochekpour, S.; Kohli, M.; et al. Serum microRNA expression patterns that predict early treatment failure in prostate cancer patients. Oncotarget 2014, 5, 824–840. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.H.; Mitchell, P.S.; Kroh, E.M.; Dowell, A.E.; Chéry, L.; Siddiqui, J.; Nelson, P.S.; Vessella, R.L.; Knudsen, B.S.; Chinnaiyan, A.M.; et al. Circulating microRNA profiling identifies a subset of metastatic prostate cancer patients with evidence of cancer-associated hypoxia. PLoS ONE 2013, 8, e69239. [Google Scholar] [CrossRef]
- Casanova-Salas, I.; Rubio-Briones, J.; Calatrava, A.; Mancarella, C.; Masiá, E.; Casanova, J.; Fernández-Serra, A.; Rubio, L.; Ramírez-Backhaus, M.; Armiñán, A.; et al. Identification of miR-187 and miR-182 as biomarkers of early diagnosis and prognosis in patients with prostate cancer treated with radical prostatectomy. J. Urol. 2014, 192, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Zhu, Y.; Gao, J.; Fu, J.; Liu, C.; Liu, Y.; Song, C.; Zhu, S.; Leng, Y.; Wang, G.; et al. MicroRNA-29a promotes colorectal cancer metastasis by regulating matrix metalloproteinase 2 and E-cadherin via KLF4. Br. J. Cancer 2014, 110, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Pu, X.X.; Huang, G.L.; Guo, H.Q.; Guo, C.C.; Li, H.; Ye, S.; Ling, S.; Jiang, L.; Tian, Y.; Lin, T.Y. Circulating miR-221 directly amplified from plasma is a potential diagnostic and prognostic marker of colorectal cancer and is correlated with p53 expression. J. Gastroenterol. Hepatol. 2010, 25, 1674–1680. [Google Scholar] [CrossRef]
- Kozomara, A.; Birgaoanu, M.; Griffiths-Jones, S. miRBase: From microRNA sequences to function. Nucleic Acids Res. 2019, 47, D155–D162. [Google Scholar] [CrossRef]
- Fan, Y.; Siklenka, K.; Arora, S.K.; Ribeiro, P.; Kimmins, S.; Xia, J. miRNet-dissecting miRNA-target interactions and functional associations through network-based visual analysis. Nucleic Acids Res. 2016, 44, W135–W141. [Google Scholar] [CrossRef] [PubMed]
- Tilford, C.A.; Siemers, N.O. Gene set enrichment analysis. Methods Mol. Biol. 2009, 563, 99–121. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Type | miRNA | AUC | p-Value | 95% CI | |
|---|---|---|---|---|---|
| LC | miR-21 | 0.821 | 0.000012 | 0.720 | 0.923 |
| miR-205 | 0.597 | 0.185027 | 0.458 | 0.737 | |
| miR-429 | 0.786 | 0.000097 | 0.670 | 0.902 | |
| miR-200b | 0.705 | 0.005186 | 0.577 | 0.833 | |
| miR-203 | 0.587 | 0.237571 | 0.449 | 0.724 | |
| miR-125b | 0.877 | 2.6858 × 10−7 | 0.785 | 0.969 | |
| miR-34 | 0.669 | 0.020907 | 0.534 | 0.805 | |
| PCa | miR-21 | 0.902 | 1.7668 × 10−8 | 0.809 | 0.994 |
| miR-141 | 0.753 | 0.000394 | 0.635 | 0.870 | |
| miR-375 | 0.720 | 0.002074 | 0.596 | 0.843 | |
| miR-125b | 0.832 | 0.000003 | 0.734 | 0.930 | |
| miR-182 | 0.895 | 2.8917 × 10−8 | 0.824 | 0.967 | |
| CRC | miR-21 | 0.913 | 1.4479 × 10−8 | 0.848 | 0.978 |
| miR-92a | 0.809 | 0.000022 | 0.694 | 0.924 | |
| miR-29a | 0.579 | 0.277441 | 0.441 | 0.717 | |
| miR-210 | 0.633 | 0.068360 | 0.494 | 0.772 | |
| miR-221 | 0.882 | 1.5783 × 10−7 | 0.804 | 0.960 | |
| miR-200c | 0.547 | 0.516238 | 0.407 | 0.687 | |
| miR-155 | 0.202 | 0.000042 | 0.095 | 0.308 | |
| BC | miR-21 | 0.771 | 0.000010 | 0.676 | 0.866 |
| miR-155 | 0.324 | 0.004121 | 0.213 | 0.436 | |
| miR-205 | 0.649 | 0.014643 | 0.535 | 0.764 | |
| Lung Cancer (LC); Prostate Cancer (PCa); Colorectal Cancer (CRC); Breast Cancer (BC) | |||||
| Tumor Type | miRNAs | AUC | p-Value | 95% CI | |
|---|---|---|---|---|---|
| LC | miR-21 miR-429 miR-200b miR-125b | 0.914 | 1.2217 × 10−9 | 0.853459 | 0.975410 |
| PCa | miR-21 miR-141 miR-375 miR-125b miR-182 | 0.937 | 8.5464 × 10−10 | 0.866459 | 1.000000 |
| CRC | miR-21 miR-92a miR-221 | 0.891 | 3.1869 × 10-−8 | 0.818095 | 0.964621 |
| BC | miR-21 miR-205 | 0.773 | 0.000008 | 0.677906 | 0.867773 |
| Tumor Type | n | Median Age (years) (Range) | Gender (M, Males; F, Females) (%) | Diagnosis (n) | Stage (n) |
|---|---|---|---|---|---|
| HDs | 45 | 56.5 (50–73) | M, 29 (64%) F, 16 (36%) | - | - |
| CRC | 27 | 70.5 (43–86) | M, 18 (67%) F, 9 (33%) | ADC (24) SRCC (1) Tubular ADC (1) MC (1) | I-IIA (15) IIIB-IV (12) |
| BC | 45 | 57 (36–87) | F, 45 (100%) | IDC (35) ILC (5) DC in situ (4) PC (1) | 0 (8) IA (13) IIA-IIB (22) IIIA-IIIB (2) |
| PCa | 40 | 66 (46–78) | M, 40 (100%) | ADC (40) | cT1c (35) cT2a (5) |
| LC | 44 | 61 (51–82) | M, 31 (70%) F, 13 (30%) | ADC (33) SCC (8) SC (1) NC (2) | IA-IB (28) IIA-IIB (7) IIIA-IV (9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pastor-Navarro, B.; García-Flores, M.; Fernández-Serra, A.; Blanch-Tormo, S.; Martínez de Juan, F.; Martínez-Lapiedra, C.; Maia de Alcantara, F.; Peñalver, J.C.; Cervera-Deval, J.; Rubio-Briones, J.; et al. A Tetra-Panel of Serum Circulating miRNAs for the Diagnosis of the Four Most Prevalent Tumor Types. Int. J. Mol. Sci. 2020, 21, 2783. https://doi.org/10.3390/ijms21082783
Pastor-Navarro B, García-Flores M, Fernández-Serra A, Blanch-Tormo S, Martínez de Juan F, Martínez-Lapiedra C, Maia de Alcantara F, Peñalver JC, Cervera-Deval J, Rubio-Briones J, et al. A Tetra-Panel of Serum Circulating miRNAs for the Diagnosis of the Four Most Prevalent Tumor Types. International Journal of Molecular Sciences. 2020; 21(8):2783. https://doi.org/10.3390/ijms21082783
Chicago/Turabian StylePastor-Navarro, Belén, María García-Flores, Antonio Fernández-Serra, Salvador Blanch-Tormo, Fernando Martínez de Juan, Carmen Martínez-Lapiedra, Fernanda Maia de Alcantara, Juan Carlos Peñalver, José Cervera-Deval, José Rubio-Briones, and et al. 2020. "A Tetra-Panel of Serum Circulating miRNAs for the Diagnosis of the Four Most Prevalent Tumor Types" International Journal of Molecular Sciences 21, no. 8: 2783. https://doi.org/10.3390/ijms21082783
APA StylePastor-Navarro, B., García-Flores, M., Fernández-Serra, A., Blanch-Tormo, S., Martínez de Juan, F., Martínez-Lapiedra, C., Maia de Alcantara, F., Peñalver, J. C., Cervera-Deval, J., Rubio-Briones, J., García-Rupérez, J., & López-Guerrero, J. A. (2020). A Tetra-Panel of Serum Circulating miRNAs for the Diagnosis of the Four Most Prevalent Tumor Types. International Journal of Molecular Sciences, 21(8), 2783. https://doi.org/10.3390/ijms21082783