Digital Phenotyping in Bipolar Disorder: Which Integration with Clinical Endophenotypes and Biomarkers?




Abstract
1. Introduction
Aims of the Paper
2. Materials and Methods
2.1. Search Sources and Strategies
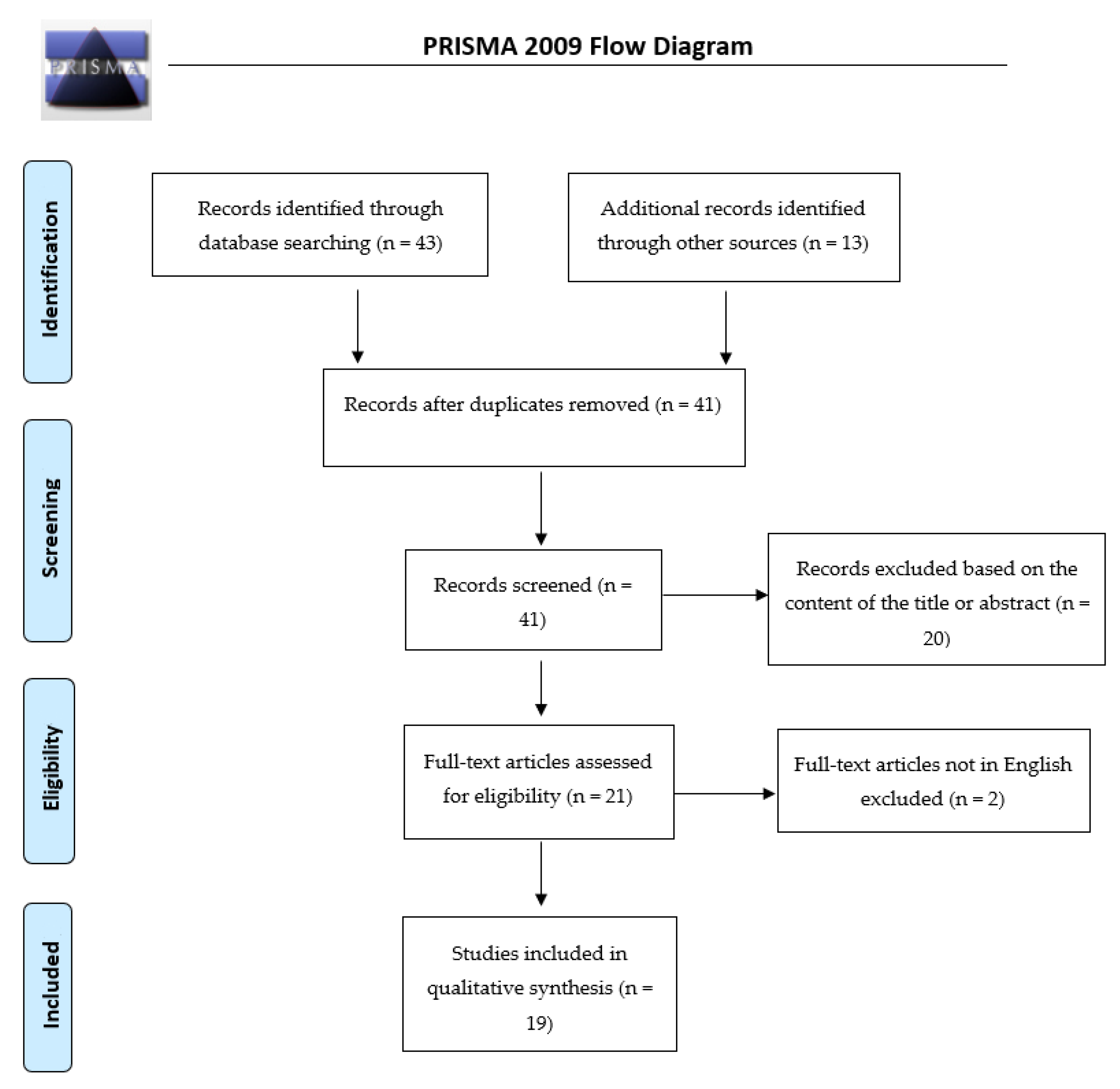
2.2. Study Selection
2.3. Data Extraction and Management
2.4. Characteristics of Included Studies
3. Results
3.1. Studies Investigating the Development of Mood Prediction Algorithms by Using a Digital Phenotyping Approach
3.2. Studies Investigating the Association between Mobile Phone Keyboard Metadata and Mood Disorders
3.3. Studies Evaluating the Relationship between Specific Patterns of Speech Features and Mood Disturbances
3.4. Studies Investigating the Correlations between Automatically Generated Objective Smartphone Data and Mood
3.5. Studies Investigating the Development of Healthcare Apps for BD
3.6. Studies Investigating All Further Future Applications of the Digital Phenotyping in the Treatment of BD
4. Discussion
4.1. Key Findings and Comparison with the Literature
4.2. Main Strengths and Limitations
4.3. Relevance of the Findings and Implications for Practice and Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Maine Avenue, DC, USA, 2013. [Google Scholar]
- Harrison, P.; Cipriani, A.; Harmer, C.J.; Nobre, A.C.; Saunders, K.E.A.; Goodwin, G.M.; Geddes, J.R. Innovative approaches to bipolar disorder and its treatment. Ann. N. Y. Acad. Sci. 2016, 1366, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Rowland, T.; Marwaha, S. Epidemiology and risk factors for bipolar disorder. Ther. Adv. Psychopharmacol. 2018, 8, 251–269. [Google Scholar] [CrossRef] [PubMed]
- Dome, P.; Rihmer, Z.; Gonda, X. Dome Suicide Risk in Bipolar Disorder: A Brief Review. Medicina 2019, 55, 403. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.F.; Miles, J.; Walters, K.; King, M.; Osborn, D.P.J. A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr. Scand. 2015, 131, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.R. Digital phenotyping: Technology for a new science of behavior. JAMA 2017, 318, 1215–1216. [Google Scholar] [CrossRef] [PubMed]
- Onnela, J.-P.; Rauch, S.L. Harnessing Smartphone-Based Digital Phenotyping to Enhance Behavioral and Mental Health. Neuropsychopharmacology 2016, 41, 1691–1696. [Google Scholar] [CrossRef]
- Brietzke, E.; Hawken, E.R.; Idzikowski, M.; Pong, J.; Kennedy, S.H.; Brietzke, E. Integrating digital phenotyping in clinical characterization of individuals with mood disorders. Neurosci. Biobehav. Rev. 2019, 104, 223–230. [Google Scholar] [CrossRef]
- Jain, S.H.; Powers, B.W.; Hawkins, J.B.; Brownstein, J.S. The digital phenotype. Nat. Biotechnol. 2015, 33, 462–463. [Google Scholar] [CrossRef]
- Lydon-Staley, D.M.; Barnett, I.; Satterthwaite, T.D.; Bassett, D.S. Digital phenotyping for psychiatry: Accommodating data and theory with network science methodologies. Curr. Opin. Biomed. Eng. 2019, 9, 8–13. [Google Scholar] [CrossRef]
- Jacobson, N.C.; Summers, B.J.; Wilhelm, S. Digital Biomarkers of Social Anxiety Severity: Digital Phenotyping Using Passive Smartphone Sensors. J. Med. Internet Res. 2020, 22, e16875. [Google Scholar] [CrossRef]
- Barnett, I.; Torous, J.; Staples, P.; Sandoval, L.; Keshavan, M.; Onnela, J.-P. Relapse prediction in schizophrenia through digital phenotyping: A pilot study. Neuropsychopharmacology 2018, 43, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Picard, R.W.; Huffman, J.C.; Nock, M.K. Digital phenotyping of suicidal thoughts. Depress. Anxiety 2018, 35, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.S.; Karmakar, C.; Tamouza, R.; Tran, T.; Yearwood, J.; Hamdani, N.; Laouamri, H.; Richard, J.-R.; Yolken, R.; Berk, M.; et al. Precision psychiatry with immunological and cognitive biomarkers: A multi-domain prediction for the diagnosis of bipolar disorder or schizophrenia using machine learning. Transl. Psychiatry 2020, 10, 1–13. [Google Scholar] [CrossRef]
- Ozomaro, U.; Wahlestedt, C.; Nemeroff, C.B. Personalized medicine in psychiatry: Problems and promises. BMC Med. 2013, 11, 132. [Google Scholar] [CrossRef]
- Perna, G.; Grassi, M.; Caldirola, D.; Nemeroff, C.B. The revolution of personalized psychiatry: Will technology make it happen sooner? Psychol. Med. 2017, 48, 705–713. [Google Scholar] [CrossRef]
- Salagre, E.; Dodd, S.; Aedo, A.; Rosa, A.; Amoretti, S.; Pinzon, J.; Reinares, M.; Berk, M.; Kapczinski, F.P.; Vieta, E.; et al. Toward Precision Psychiatry in Bipolar Disorder: Staging 2.0. Front. Psychiatry 2018, 9, 641. [Google Scholar] [CrossRef]
- McInnis, M.; Gideon, J.; Provost, E.M. Digital Phenotyping in Bipolar Disorder. Eur. Neuropsychopharmacol. 2017, 27, S440. [Google Scholar] [CrossRef]
- Cho, C.-H.; Lee, T.; Kim, M.-G.; In, H.P.; Kim, L.; Lee, H.-J. Mood Prediction of Patients With Mood Disorders by Machine Learning Using Passive Digital Phenotypes Based on the Circadian Rhythm: Prospective Observational Cohort Study. J. Med. Internet Res. 2019, 21, e11029. [Google Scholar] [CrossRef]
- Zulueta, J.; Piscitello, A.; Rasic, M.; Easter, R.; Babu, P.; Langenecker, S.A.; McInnis, M.G.; Ajilore, O.; Nelson, P.C.; Ryan, K.A.; et al. Predicting Mood Disturbance Severity with Mobile Phone Keystroke Metadata: A BiAffect Digital Phenotyping Study. J. Med. Internet Res. 2018, 20, e241. [Google Scholar] [CrossRef]
- Hidalgo-Mazzei, D.; Hassani, H.; Ostacher, M.; Graham, A.; Busk, J.; Faurholt-Jepsen, M.; Frost, M.; Bardram, J.E.; Kessing, L.V.; Winther, O. Forecasting Mood in Bipolar Disorder From Smartphone Self-assessments: Hierarchical Bayesian Approach. JMIR mHealth uHealth 2020, 8, e15028. [Google Scholar] [CrossRef]
- Dargél, A.A.; Mosconi, E.; Masson, M.; Plaze, M.; Taieb, F.; Von Platen, C.; Buivan, T.P.; Henry, C. Toi Même: A mHealth Platform for Measuring Bipolar Illness Activity-Feasibility Study Protocol. JMIR Res. Protoc. 2020, 9, e18818. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Zheng, L.; Zhang, C.; Yu, P.S.; Piscitello, A.; Zulueta, J.; Leow, A.D. Deepmood: Modeling mobile phone typing dynamics for mood detection. In Proceedings of the 23rd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Halifax, NS, Canada, 13–17 August 2017; pp. 747–755. [Google Scholar]
- Gideon, J.; Provost, E.M.; McInnis, M. Mood state prediction from speech of varying acoustic quality for individuals with bipolar disorder. In Proceedings of the 2016 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Shanghai, China, 20–25 March 2016; Institute of Electrical and Electronics Engineers (IEEE): New York, NY, USA, 2016; pp. 2359–2363. [Google Scholar]
- Karam, Z.N.; Provost, E.M.; Singh, S.; Montgomery, J.; Archer, C.; Harrington, G.; McInnis, M.G. Ecologically valid long-term mood monitoring of individuals with bipolar disorder using speech. In Proceedings of the 2014 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Florence, Italy, 4–9 May 2014; Institute of Electrical and Electronics Engineers (IEEE): New York, NY, USA, 2014; pp. 4858–4862. [Google Scholar]
- Muaremi, A.; Gravenhorst, F.; Grünerbl, A.; Arnrich, B.; Tröster, G. Assessing Bipolar Episodes Using Speech Cues Derived from Phone Calls. In Proceedings of the International Symposium on Pervasive Computing Paradigms for Mental Health, Tokyo, Japan, 8–9 May 2014; Springer: Cham, Switzerland, 2014; pp. 103–114. [Google Scholar]
- Abdullah, S.; Matthews, M.; Frank, E.; Doherty, G.; Gay, G.; Choudhury, T. Automatic detection of social rhythms in bipolar disorder. J. Am. Med. Inform. Assoc. 2016, 23, 538–543. [Google Scholar] [CrossRef]
- Beiwinkel, T.; Kindermann, S.; Maier, A.; Kerl, C.; Moock, J.; Barbian, G.; Rössler, W.; Faurholt-Jepsen, M.; Mayora, O.; Buntrock, C. Using Smartphones to Monitor Bipolar Disorder Symptoms: A Pilot Study. JMIR Ment. Health 2016, 3, e2. [Google Scholar] [CrossRef]
- Grunerbl, A.; Muaremi, A.; Osmani, V.; Bahle, G.; Ohler, S.; Troster, G.; Mayora, O.; Haring, C.; Lukowicz, P. Smartphone-Based Recognition of States and State Changes in Bipolar Disorder Patients. IEEE J. Biomed. Health Inform. 2014, 19, 140–148. [Google Scholar] [CrossRef]
- Palmius, N.; Tsanas, A.; Saunders, K.E.A.; Bilderbeck, A.C.; Geddes, J.R.; Goodwin, G.M.; De Vos, M. Detecting Bipolar Depression From Geographic Location Data. IEEE Trans. Biomed. Eng. 2016, 64, 1761–1771. [Google Scholar] [CrossRef] [PubMed]
- Bardram, J.E.; Frost, M.; Szántó, K.; Faurholt-Jepsen, M.; Vinberg, M.; Kessing, L.V. Designing mobile health technology for bipolar disorder. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Paris, France, 27 April–2 May 2013; pp. 2627–2636. [Google Scholar]
- Alvarez-Lozano, J.; Osmani, V.; Mayora, O.; Frost, M.; Bardram, J.; Faurholt-Jepsen, M.; Kessing, L.V. Tell me your apps and I will tell you your mood. In Proceedings of the 7th International Conference on PErvasive Technologies Related to Assistive Environments, Rhodes, Greece, 27–30 May 2014; Association for Computing Machinery: New York, NY, USA, 2014; pp. 1–7. [Google Scholar]
- Faurholt-Jepsen, M.; Frost, M.; Ritz, C.; Christensen, E.M.; Jacoby, A.S.; Mikkelsen, R.L.; Knorr, U.; Bardram, J.E.; Vinberg, M.; Kessing, L.V. Daily electronic self-monitoring in bipolar disorder using smartphones—The MONARCA I trial: A randomized, placebo-controlled, single-blind, parallel group trial. Psychol. Med. 2015, 45, 2691–2704. [Google Scholar] [CrossRef]
- Faurholt-Jepsen, M.; Busk, J.; Þórarinsdóttir, H.; Frost, M.; Bardram, J.E.; Vinberg, M.; Kessing, L.V. Objective smartphone data as a potential diagnostic marker of bipolar disorder. Aust. N. Zeal. J. Psychiatry 2018, 53, 119–128. [Google Scholar] [CrossRef]
- Faurholt-Jepsen, M.; Frost, M.; Christensen, E.M.; Bardram, J.E.; Vinberg, M.; Kessing, L.V. The effect of smartphone-based monitoring on illness activity in bipolar disorder: The MONARCA II randomized controlled single-blinded trial. Psychol. Med. 2019, 50, 838–848. [Google Scholar] [CrossRef]
- Scott, J.; Hidalgo-Mazzei, D.; Strawbridge, R.; Young, A.H.; Resche-Rigon, M.; Etain, B.; Andreassen, O.A.; Bauer, M.; Bennabi, D.; Blamire, A.M.; et al. Prospective cohort study of early biosignatures of response to lithium in bipolar-I-disorders: Overview of the H2020-funded R-LiNK initiative. Int. J. Bipolar Disord. 2019, 7, 20. [Google Scholar] [CrossRef]
- Cho, C.-H.; Ahn, Y.-M.; Kim, S.J.; Ha, T.H.; Jeon, H.J.; Cha, B.; Moon, E.; Park, D.Y.; Baek, J.H.; Kang, H.-J.; et al. Design and Methods of the Mood Disorder Cohort Research Consortium (MDCRC) Study. Psychiatry Investig. 2016, 14, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Faurholt-Jepsen, M.; Vinberg, M.; Frost, M.; Christensen, E.M.; Bardram, J.E.; Kessing, L.V. Daily electronic monitoring of subjective and objective measures of illness activity in bipolar disorder using smartphones—The MONARCA II trial protocol: A randomized controlled single-blind parallel-group trial. BMC Psychiatry 2014, 14, 309. [Google Scholar] [CrossRef]
- Assoc, A.P. Diagnostic and Statistical Manual of Mental Disorders. Alzheimer Dis. Assoc. Disord. 1988, 2, 144–145. [Google Scholar] [CrossRef]
- McInnis, M.; Assari, S.; Kamali, M.; Ryan, K.; Langenecker, S.A.; Saunders, E.F.H.; Versha, K.; Evans, S.J.; O’Shea, K.S.; Provost, E.M.; et al. Cohort Profile: The Heinz C. Prechter Longitudinal Study of Bipolar Disorder. Int. J. Epidemiol. 2017, 47, 28–28n. [Google Scholar] [CrossRef] [PubMed]
- Langenecker, S.A.; Saunders, E.F.; Kade, A.M.; Ransom, M.T.; McInnis, M.G. Intermediate: Cognitive phenotypes in bipolar disorder. J. Affect. Disord. 2010, 122, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Rush, A.; Trivedi, M.H.; Ibrahim, H.M.; Carmody, T.J.; Arnow, B.; Klein, D.N.; Markowitz, J.C.; Ninan, P.T.; Kornstein, S.; Manber, R.; et al. The 16-Item quick inventory of depressive symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): A psychometric evaluation in patients with chronic major depression. Biol. Psychiatry 2003, 54, 573–583. [Google Scholar] [CrossRef]
- Huckvale, K.; Venkatesh, S.; Christensen, H. Toward clinical digital phenotyping: A timely opportunity to consider purpose, quality, and safety. Npj Digit. Med. 2019, 2, 1–11. [Google Scholar] [CrossRef]
- Pew Research. Mobile Fact Sheet. 2018. Available online: http://www.pewinternet.org/fact-sheet/mobile/ (accessed on 14 June 2019).
- Torous, J.; Kiang, M.V.; Lorme, J.; Onnela, J.-P. New Tools for New Research in Psychiatry: A Scalable and Customizable Platform to Empower Data Driven Smartphone Research. JMIR Ment. Health 2016, 3, e16. [Google Scholar] [CrossRef]
- Smith, D.G. Digital phenotyping approaches and mobile devices enhance CNS biopharmaceutical research and development. Neuropsychopharmacology 2018, 43, 2504–2505. [Google Scholar] [CrossRef]
- Marwaha, S.; Price, C.; Scott, J.; Weich, S.; Cairns, A.; Dale, J.; Winsper, C.; Broome, M.R. Affective instability in those with and without mental disorders: A case control study. J. Affect. Disord. 2018, 241, 492–498. [Google Scholar] [CrossRef]
- Selby, E.A.; Yen, S.; Spirito, A. Time varying prediction of thoughts of death and suicidal ideation in adolescents: Weekly ratings over 6-month follow-up. J. Clin. Child Adolesc. Psychol. 2012, 42, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Glenn, T.; Monteith, S.; Bauer, R.; Whybrow, P.C.; Geddes, J.R. Ethical perspectives on recommending digital technology for patients with mental illness. Int. J. Bipolar Disord. 2017, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.R. The NIMH Research Domain Criteria (RDoC) Project: Precision Medicine for Psychiatry. Am. J. Psychiatry 2014, 171, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Insel, T.R. Digital phenotyping: A global tool for psychiatry. World Psychiatry 2018, 17, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Onnela, J.-P.; Keshavan, M. New dimensions and new tools to realize the potential of RDoC: Digital phenotyping via smartphones and connected devices. Transl. Psychiatry 2017, 7, e1053. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, J.; Larsen, M.E.; Proudfoot, J.; Christensen, H. Mobile Apps for Bipolar Disorder: A Systematic Review of Features and Content Quality. J. Med. Internet Res. 2015, 17, e198. [Google Scholar] [CrossRef] [PubMed]
- Klugman, C.M.; Dunn, L.B.; Schwartz, J.; Cohen, I.G. The Ethics of Smart Pills and Self-Acting Devices: Autonomy, Truth-Telling, and Trust at the Dawn of Digital Medicine. Am. J. Bioeth. 2018, 18, 38–47. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Study Design | Sample Features | Diagnostic Criteria | Objectives | Methodology | Main Findings |
|---|---|---|---|---|---|---|
| [15] | Prospective cohort study | 60 pts | BD-rapid cycling (n = 51) HC (n = 9) |
|
|
|
| [16] | Prospective observational cohort study | 55 pts | MDD (n = 18) BD-I (n = 18) BD-II (n = 19) (DSM-5) |
|
|
|
| [17] | Prospective cohort study | 9 pts (8 F, 1 M) | BD-I (n = 5) BD-II (n = 4) (DSM-IV-TR) |
|
|
|
| [18] | RCT | 84 pts (52F, 32M), 21–71yy | BD (unspecified type) (ICD-10) |
|
|
|
| [19] | nonrandomized trial | 93 pts | BD-I BD-II (DSM-5) |
|
|
|
| [22] | Pilot study, 8-weeks prospective | 40 pts | BD-I (n = 7) BD-II (n = 5) BD-NOS (n = 8) HC (n = 20) (DSM-IV-TR) |
|
|
|
| [23] | Prospective cohort study | 37 pts | BD-rapid-cycling BD-I BD-II |
|
|
|
| [24] | Pilot study | 6 pts | BD-I with a history of rapid cycling (i.e., characterized by 4 or more episodes per year of mania, hypomania, or depression) |
|
|
|
| [25] | Pilot study | 12 pts, 18–65yy | BD (unspecified type) |
|
|
|
| [26] | Pilot study, 4-week prospective | 9 enrolled pts (5 F, 4 M), of which 7 included pts (5 F, 2 M), 24–65 yy | BD-I (n = 1) BD-II (n = 5) BD-NOS (n = 1) |
|
|
|
| [27] | Pilot study, 12-months prospective | 32 enrolled pts, of which 12 included pts | BD-I or BD-II (DSM-IV-TR), at least 18 years of age, sufficient knowledge of the German language, and basic competence in using mobile devices |
|
|
|
| [28] | Pilot study | 10 pts, 18–65 yy | BD (unspecified type) (ICD- 10) willingness and ability to deal with modern smart-phones |
|
|
|
| [29] | Prospective community study | 49 enrolled pts, of which 36 included (27 F, 9 M) | BD unspecified type (n = 22) HC (n = 14) (DSM-IV-TR) |
|
|
|
| [30] | 14-week field trial | 14 enrolled pts, of which 12 included (7 F, 5 M), 20–51yy | BD (unspecified type) |
|
|
|
| [31] | RCT | 18 enrolled pts (age and gender unspecified) | BD (unspecified type) |
|
|
|
| [32] | RCT | 123 enrolled pts, of which 78 included, 18–60 yy | BD (unspecified type) (ICD-10) |
|
|
|
| [33] | Prospective cohort study | 66 pts | BD (unspecified type) (n = 29) HC (n = 37) (ICD-10) |
|
|
|
| [34] | RCT | 735 enrolled pts, of which 129 included | BD (unspecified type) (ICD-10) |
|
|
|
| [35] | Prospective cohort study | 300 included pts | BD Type I (DSM-V) agreed to commence a trial of lithium treatment |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orsolini, L.; Fiorani, M.; Volpe, U. Digital Phenotyping in Bipolar Disorder: Which Integration with Clinical Endophenotypes and Biomarkers? Int. J. Mol. Sci. 2020, 21, 7684. https://doi.org/10.3390/ijms21207684
Orsolini L, Fiorani M, Volpe U. Digital Phenotyping in Bipolar Disorder: Which Integration with Clinical Endophenotypes and Biomarkers? International Journal of Molecular Sciences. 2020; 21(20):7684. https://doi.org/10.3390/ijms21207684
Chicago/Turabian StyleOrsolini, Laura, Michele Fiorani, and Umberto Volpe. 2020. "Digital Phenotyping in Bipolar Disorder: Which Integration with Clinical Endophenotypes and Biomarkers?" International Journal of Molecular Sciences 21, no. 20: 7684. https://doi.org/10.3390/ijms21207684
APA StyleOrsolini, L., Fiorani, M., & Volpe, U. (2020). Digital Phenotyping in Bipolar Disorder: Which Integration with Clinical Endophenotypes and Biomarkers? International Journal of Molecular Sciences, 21(20), 7684. https://doi.org/10.3390/ijms21207684