Isolated Lung Perfusion in the Management of Acute Respiratory Distress Syndrome


Abstract
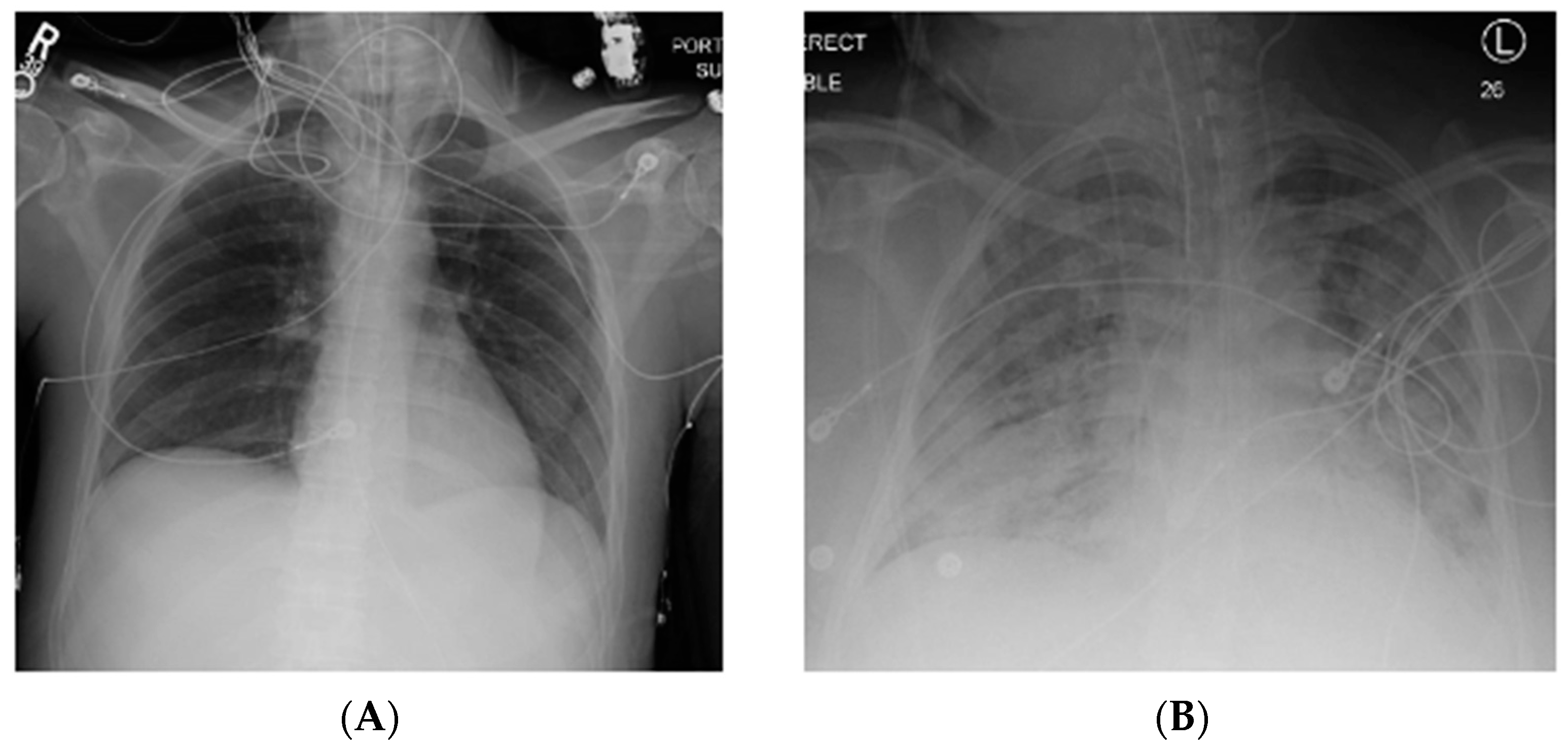
1. Acute Respiratory Distress Syndrome
2. Isolated Lung Perfusion and ARDS
3. Ex Vivo Lung Perfusion (EVLP) History
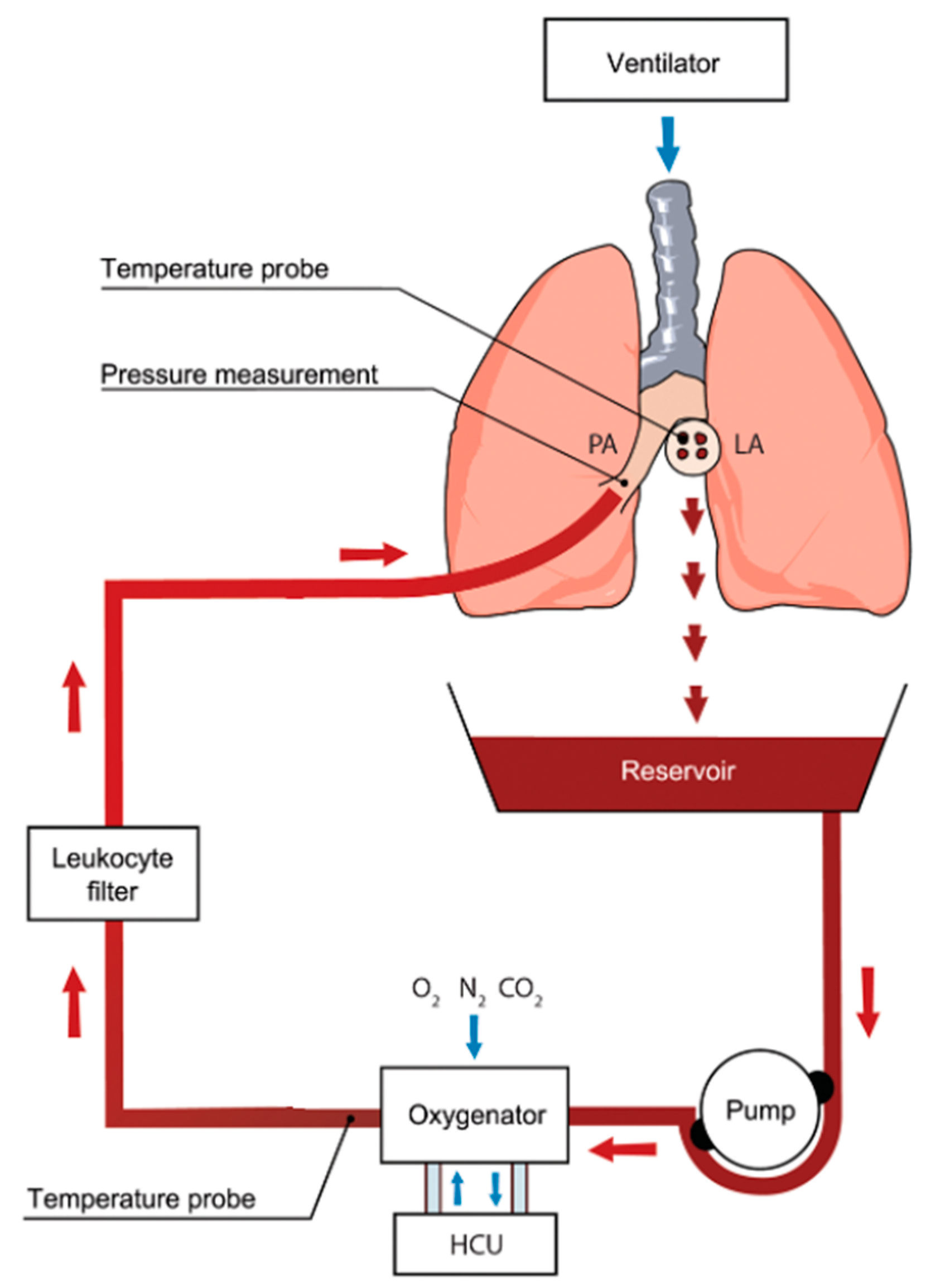
4. EVLP Technique
5. Investigational Therapies During EVLP
6. Molecular and Cellular Changes During EVLP
7. In Vivo Lung Perfusion (IVLP) History
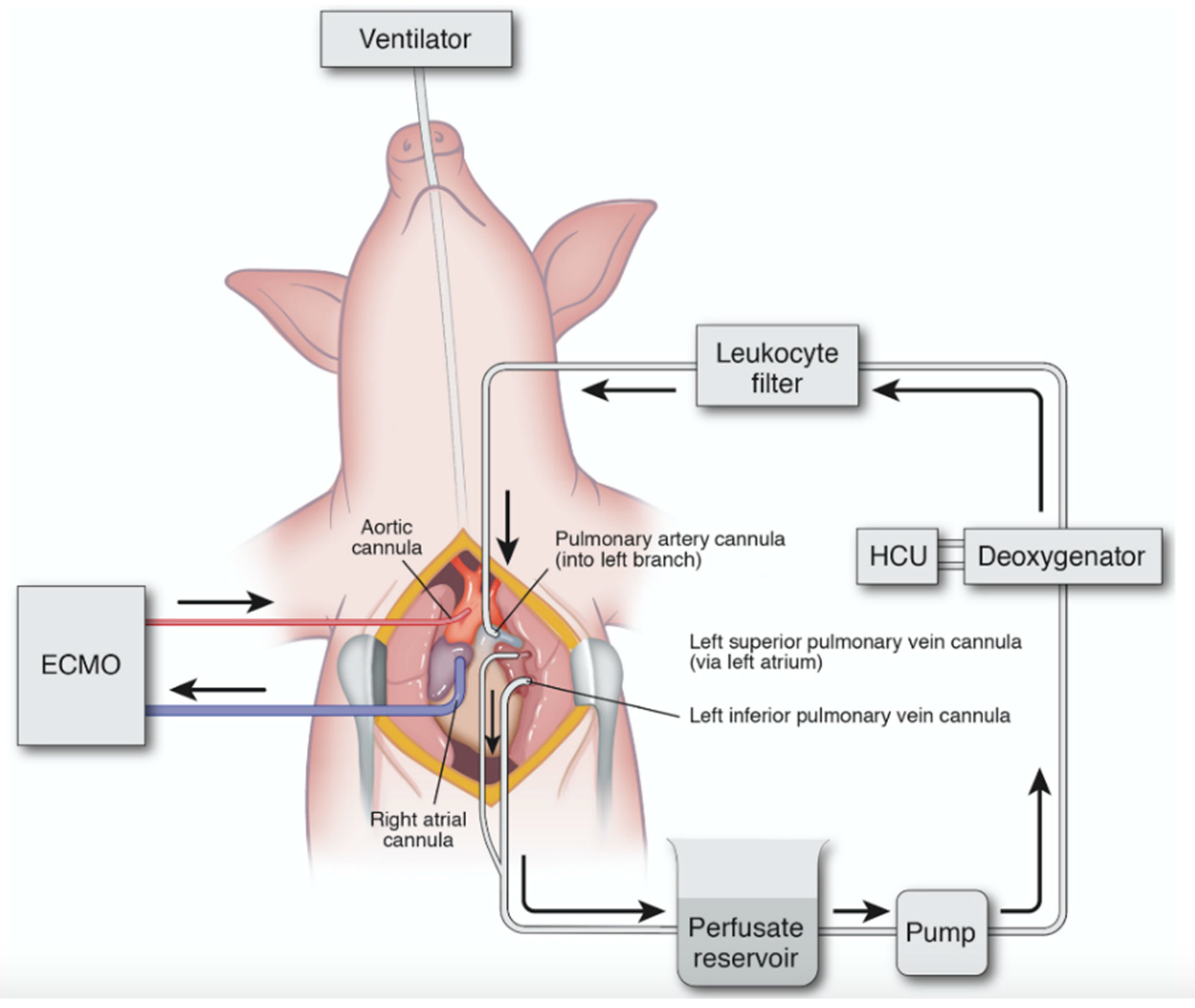
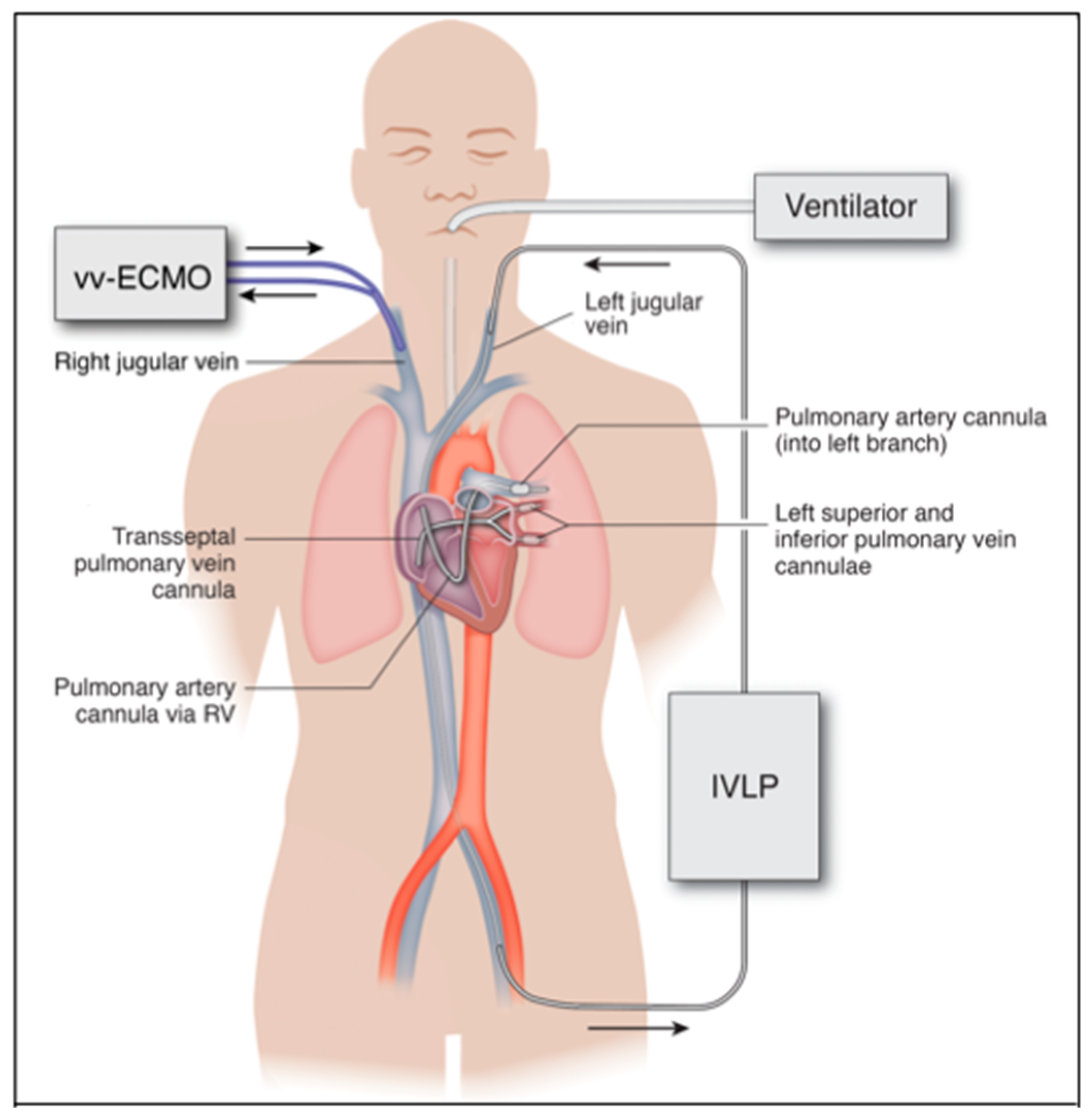
8. IVLP Technique
9. Investigations of IVLP in ARDS
10. Clinical Translation and Future Direction of IVLP
Author Contributions
Funding
Conflicts of Interest
References
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar] [CrossRef]
- Matthay, M.A. The Acute Respiratory Distress Syndrome. N. Engl. J. Med. 1996, 334, 1469–1470. [Google Scholar] [CrossRef]
- Mokra, D.; Mikolka, P.; Košútová, P.; Mokry, J. Corticosteroids in Acute Lung Injury: The Dilemma Continues. Int. J. Mol. Sci. 2019, 20, 4765. [Google Scholar] [CrossRef] [PubMed]
- Umbrello, M.; Formenti, P.; Bolgiaghi, L.; Chiumello, D. Current Concepts of ARDS: A Narrative Review. Int. J. Mol. Sci. 2016, 18, 64. [Google Scholar] [CrossRef]
- Ashbaugh, D.; Bigelow, D.B.; Petty, T.; Levine, B. Acute respiratory distress in adults. Lancet 1967, 290, 319–323. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.M.P.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Eworuke, E.; Major, J.M.; McClain, L.I.G. National incidence rates for Acute Respiratory Distress Syndrome (ARDS) and ARDS cause-specific factors in the United States (2006–2014). J. Crit. Care 2018, 47, 192–197. [Google Scholar] [CrossRef]
- Herridge, M.; Moss, M.; Hough, C.L.; Hopkins, R.O.; Rice, T.W.; Bienvenu, O.J.; Azoulay, E. Recovery and outcomes after the acute respiratory distress syndrome (ARDS) in patients and their family caregivers. Intensiv. Care Med. 2016, 42, 725–738. [Google Scholar] [CrossRef]
- Bice, T.; Carson, S.S. Acute Respiratory Distress Syndrome: Cost (Early and Long-Term). Semin. Respir. Crit. Care Med. 2019, 40, 137–144. [Google Scholar] [CrossRef]
- Brodie, D.; Bacchetta, M. Extracorporeal Membrane Oxygenation for ARDS in Adults. N. Engl. J. Med. 2011, 365, 1905–1914. [Google Scholar] [CrossRef] [PubMed]
- Morales-Quinteros, L.; Camprubí-Rimblas, M.; Bringué, J.; Bos, L.T.; Schultz, M.J.; Artigas, A. The role of hypercapnia in acute respiratory failure. Intensiv. Care Med. Exp. 2019, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Broccard, A.F.; Hotchkiss, J.R.; Vannay, C.; Markert, M.; Sauty, A.; Feihl, F.; Schaller, M.-D. Protective Effects of Hypercapnic Acidosis on Ventilator-induced Lung Injury. Am. J. Respir. Crit. Care Med. 2001, 164, 802–806. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, D.; Hassett, P.; Contreras, M.; Higgins, B.D.; McKeown, S.T.W.; McAuley, D.F.; O’Brien, T.; Laffey, J.G. Hypercapnic acidosis attenuates pulmonary epithelial wound repair by an NF-kappaB dependent mechanism. Thorax 2009, 64, 976–982. [Google Scholar] [CrossRef]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Papazian, L.; Aubron, C.; Brochard, L.; Chiche, J.-D.; Combes, A.; Dreyfuss, D.; Forel, J.-M.; Guérin, C.; Jaber, S.; Dessap, A.M.; et al. Formal guidelines: Management of acute respiratory distress syndrome. Ann. Intensiv. Care 2019, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Hardesty, R.L.; Griffith, B.P. Autoperfusion of the heart and lungs for preservation during distant procurement. J. Thorac. Cardiovasc. Surg. 1987, 93, 11–18. [Google Scholar] [CrossRef]
- Cypel, M.; Yeung, J.C.; Liu, M.; Anraku, M.; Chen-Yoshikawa, T.F.; Karolak, W.; Sato, M.; Laratta, J.; Azad, S.; Madonik, M.; et al. Normothermic Ex Vivo Lung Perfusion in Clinical Lung Transplantation. N. Engl. J. Med. 2011, 364, 1431–1440. [Google Scholar] [CrossRef]
- Mehaffey, J.H.; Charles, E.J.; Sharma, A.K.; Salmon, M.; Money, D.; Schubert, S.; Stoler, M.H.; Tribble, C.G.; Laubach, V.E.; Roeser, M.E.; et al. Ex Vivo Lung Perfusion Rehabilitates Sepsis-Induced Lung Injury. Ann. Thorac. Surg. 2017, 103, 1723–1729. [Google Scholar] [CrossRef]
- Mehaffey, J.H.; Charles, E.J.; Schubert, S.; Salmon, M.; Sharma, A.K.; Money, D.; Stoler, M.H.; Laubach, V.E.; Tribble, C.G.; Roeser, M.E.; et al. In vivo lung perfusion rehabilitates sepsis-induced lung injury. J. Thorac. Cardiovasc. Surg. 2018, 155, 440–448.e2. [Google Scholar] [CrossRef] [PubMed]
- Loor, G. EVLP: Ready for Prime Time? Semin. Thorac. Cardiovasc. Surg. 2019, 31, 1–6. [Google Scholar] [CrossRef]
- Cypel, M. Isolated lung perfusion. Front. Biosci. 2012, 4, 2226. [Google Scholar] [CrossRef]
- Punch, J.D.; Hayes, D.H.; Laporte, F.B.; McBride, V.; Seely, M.S. Organ Donation and Utilization in the United States, 1996–2005. Am. J. Transplant. 2007, 7, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Yang, J.; Fu, S.; Zhao, H. Application of ex vivo lung perfusion (EVLP) in lung transplantation. J. Thorac. Dis. 2018, 10, 4637–4642. [Google Scholar] [CrossRef]
- Valapour, M.; Skeans, M.A.; Smith, J.M.; Edwards, L.B.; Cherikh, W.S.; Uccellini, K.; Israni, A.K.; Snyder, J.J.; Kasiske, B.L. OPTN/SRTR 2015 Annual Data Report: Lung. Am. J. Transplant. 2017, 17, 357–424. [Google Scholar] [CrossRef]
- Steen, S.; Sjöberg, T.; Pierre, L.; Liao, Q.; Eriksson, L.; Algotsson, L. Transplantation of lungs from a non-heart-beating donor. Lancet 2001, 357, 825–829. [Google Scholar] [CrossRef]
- Steen, S.; Liao, Q.; Wierup, P.N.; Bolys, R.; Pierre, L.; Sjöberg, T. Transplantation of lungs from non-heart-beating donors after functional assessment ex vivo. Ann. Thorac. Surg. 2003, 76, 244–252. [Google Scholar] [CrossRef]
- Steen, S.; Ingemansson, R.; Eriksson, L.; Pierre, L.; Algotsson, L.; Wierup, P.; Liao, Q.; Eyjolfsson, A.; Gustafsson, R.; Sjöberg, T. First Human Transplantation of a Nonacceptable Donor Lung After Reconditioning Ex Vivo. Ann. Thorac. Surg. 2007, 83, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Wierup, P.; Haraldsson, Å.; Nilsson, F.; Pierre, L.; Scherstén, H.; Silverborn, M.; Sjöberg, T.; Westfeldt, U.; Steen, S. Ex Vivo Evaluation of Nonacceptable Donor Lungs. Ann. Thorac. Surg. 2006, 81, 460–466. [Google Scholar] [CrossRef]
- Ali, A.; Cypel, M. Ex-vivo lung perfusion and ventilation. Curr. Opin. Organ. Transplant. 2019, 24, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, P.G.; Davis, R.D.; D’ovidio, F.; Weyan, M.J.; Camp, P.C.; Cantu III, E.; Griffith, B.P. Normothermic Ex Vivo Lung Perfusion as an Assessment of Marginal Donor Lungs–The NOVEL Lung Trial. J. Hear. Lung Transplant. 2013, 32, S16–S17. [Google Scholar] [CrossRef]
- Sanchez, P.; Davis, R.; D’Ovidio, F.; Cantu, E.; Weyant, M.; Camp, P.; Griffith, B. The NOVEL Lung Trial One-Year Outcomes. J. Hear. Lung Transplant. 2014, 33, S71–S72. [Google Scholar] [CrossRef]
- Cypel, M.; Keshavjee, S. Extracorporeal lung perfusion (ex-vivo lung perfusion). Curr. Opin. Organ. Transplant. 2016, 21, 329–335. [Google Scholar] [CrossRef]
- Tane, S.; Noda, K.; Shigemura, N. Ex Vivo Lung Perfusion. Chest 2017, 151, 1220–1228. [Google Scholar] [CrossRef]
- Wallinder, A.; Ricksten, S.-E.; Silverborn, M.; Hansson, C.; Riise, G.C.; Liden, H.; Jeppsson, A.; Dellgren, G. Early results in transplantation of initially rejected donor lungs after ex vivo lung perfusion: A case-control study. Eur. J. Cardio-Thoracic Surg. 2013, 45, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Van Raemdonck, D.E.; Rega, F.; Rex, S.; Neyrinck, A. Machine perfusion of thoracic organs. J. Thorac. Dis. 2018, 10, S910–S923. [Google Scholar] [CrossRef]
- Kondo, T.; Chen-Yoshikawa, T.F.; Ohsumi, A.; Hijiya, K.; Motoyama, H.; Sowa, T.; Ohata, K.; Takahashi, M.; Yamada, T.; Sato, M.; et al. β2-Adrenoreceptor Agonist Inhalation During Ex Vivo Lung Perfusion Attenuates Lung Injury. Ann. Thorac. Surg. 2015, 100, 480–486. [Google Scholar] [CrossRef]
- Hijiya, K.; Chen-Yoshikawa, T.F.; Kondo, T.; Motoyama, H.; Ohsumi, A.; Nakajima, D.; Sakamoto, J.; Ohata, K.; Takahashi, M.; Tanaka, S.; et al. Bronchodilator Inhalation During Ex Vivo Lung Perfusion Improves Posttransplant Graft Function After Warm Ischemia. Ann. Thorac. Surg. 2017, 103, 447–453. [Google Scholar] [CrossRef]
- Sakuma, T.; Gu, X.; Wang, Z.; Maeda, S.; Sugita, M.; Sagawa, M.; Osanai, K.; Toga, H.; Ware, L.B.; Folkesson, G.; et al. Stimulation of alveolar epithelial fluid clearance in human lungs by exogenous epinephrine. Crit. Care Med. 2006, 34, 676–681. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Valenza, F.; Rosso, L.; Coppola, S.; Froio, S.; Colombo, J.; Dossi, R.; Fumagalli, J.; Salice, V.; Pizzocri, M.; Conte, G.; et al. β-Adrenergic agonist infusion during extracorporeal lung perfusion: Effects on glucose concentration in the perfusion fluid and on lung function. J. Hear. Lung Transplant. 2012, 31, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Emaminia, A.; Lapar, D.J.; Zhao, Y.; Steidle, J.F.; Harris, D.A.; Laubach, V.E.; Linden, J.; Kron, I.L.; Lau, C.L. Adenosine A2A agonist improves lung function during ex vivo lung perfusion. Ann Thorac. Surg. 2011, 92, 1840–1846. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.L.; Sharma, A.K.; Mas, V.R.; Gehrau, R.C.; Mulloy, D.P.; Zhao, Y.; Lau, C.L.; Kron, I.L.; Huerter, M.E.; Laubach, V.E.; et al. Ex Vivo Perfusion With Adenosine A2A Receptor Agonist Enhances Rehabilitation of Murine Donor Lungs After Circulatory Death. Transplant. 2015, 99, 2494–2503. [Google Scholar] [CrossRef] [PubMed]
- Wagner, C.E.; Pope, N.H.; Charles, E.J.; Huerter, M.E.; Sharma, A.K.; Salmon, M.D.; Carter, B.T.; Stoler, M.H.; Lau, C.L.; Laubach, V.E.; et al. Ex vivo lung perfusion with adenosine A2A receptor agonist allows prolonged cold preservation of lungs donated after cardiac death. J. Thorac. Cardiovasc. Surg. 2015, 151, 538–545. [Google Scholar] [CrossRef]
- Charles, E.J.; Mehaffey, J.H.; Sharma, A.K.; Zhao, Y.; Stoler, M.H.; Isbell, J.M.; Lau, C.L.; Tribble, C.G.; Laubach, V.E.; Kron, I.L. Lungs donated after circulatory death and prolonged warm ischemia are transplanted successfully after enhanced ex vivo lung perfusion using adenosine A2B receptor antagonism. J. Thorac. Cardiovasc. Surg. 2017, 154, 1811–1820. [Google Scholar] [CrossRef]
- Huerter, M.E.; Sharma, A.K.; Zhao, Y.; Charles, E.J.; Kron, I.L.; Laubach, V.E. Attenuation of Pulmonary Ischemia-Reperfusion Injury by Adenosine A2B Receptor Antagonism. Ann. Thorac. Surg. 2016, 102, 385–393. [Google Scholar] [CrossRef][Green Version]
- Mehaffey, J.H.; Charles, E.J.; Narahari, A.K.; Schubert, S.; Laubach, V.E.; Teman, N.R.; Lynch, K.R.; Kron, I.L.; Sharma, A.K. Increasing circulating sphingosine-1-phosphate attenuates lung injury during ex vivo lung perfusion. J. Thorac. Cardiovasc. Surg. 2018, 156, 910–917. [Google Scholar] [CrossRef]
- Harada, M.; Oto, T.; Otani, S.; Miyoshi, K.; Okada, M.; Iga, N.; Nishikawa, H.; Sugimoto, S.; Yamane, M.; Miyoshi, S. A neutrophil elastase inhibitor improves lung function during ex vivo lung perfusion. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Chen, M.; Tian, F.; Tikkanen, J.; Ding, L.; Cheung, H.Y.A.; Nakajima, D.; Wang, Z.; Mariscal, A.; Hwang, D.; et al. α 1 -Anti-trypsin improves function of porcine donor lungs during ex-vivo lung perfusion. J. Hear. Lung Transplant. 2018, 37, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Cypel, M.; Liu, M.; Rubacha, M.; Yeung, J.C.; Hirayama, S.; Anraku, M.; Sato, M.; Medin, J.; Davidson, B.L.; De Perrot, M.; et al. Functional Repair of Human Donor Lungs by IL-10 Gene Therapy. Sci. Transl. Med. 2009, 1, 4ra9. [Google Scholar] [CrossRef] [PubMed]
- Yeung, J.C.; Wagnetz, D.; Cypel, M.; Rubacha, M.; Koike, T.; Chun, Y.-M.; Hu, J.; Waddell, T.K.; Hwang, D.M.; Liu, M.; et al. Ex Vivo Adenoviral Vector Gene Delivery Results in Decreased Vector-associated Inflammation Pre- and Post–lung Transplantation in the Pig. Mol. Ther. 2012, 20, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Tavasoli, F.; Liu, M.; Machuca, T.N.; Bonato, R.; Grant, D.R.; Cypel, M.; Keshavjee, S.; Grasemann, H. Increased Arginase Expression and Decreased Nitric Oxide in Pig Donor Lungs after Normothermic Ex Vivo Lung Perfusion. Biomolecules 2020, 10, 300. [Google Scholar] [CrossRef] [PubMed]
- Lonati, C.; Bassani, G.A.; Brambilla, D.; Leonardi, P.; Carlin, A.; Faversani, A.; Gatti, S.; Valenza, F. Influence of ex vivo perfusion on the biomolecular profile of rat lungs. FASEB J. 2018, 32, 5532–5549. [Google Scholar] [CrossRef] [PubMed]
- Hsin, M.K.; Zamel, R.; Cypel, M.; Wishart, D.; Han, B.; Keshavjee, S.; Liu, M. Metabolic Profile of Ex Vivo Lung Perfusate Yields Biomarkers for Lung Transplant Outcomes. Ann. Surg. 2018, 267, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Cypel, M.; Juvet, S.C.; Saito, T.; Zamel, R.; Machuca, T.N.; Hsin, M.; Kim, H.; Waddell, T.K.; Liu, M.; et al. Higher M30 and high mobility group box 1 protein levels in ex vivo lung perfusate are associated with primary graft dysfunction after human lung transplantation. J. Hear. Lung Transplant. 2018, 37, 240–249. [Google Scholar] [CrossRef]
- Elgharably, H.; Okamoto, T.; Ayyat, K.S.; Niikawa, H.; Meade, S.; Farver, C.; Chan, E.R.; Aldred, M.A.; McCurry, K.R. Human Lungs Airway Epithelium Upregulate MicroRNA-17 and MicroRNA-548b in Response to Cold Ischemia and Ex Vivo Reperfusion. Transplantation 2020. [Google Scholar] [CrossRef]
- Yeung, J.C.; Zamel, R.; Klement, W.; Bai, X.-H.; Machuca, T.N.; Waddell, T.K.; Liu, M.; Cypel, M.; Keshavjee, S. Towards donor lung recovery-gene expression changes during ex vivo lung perfusion of human lungs. Am. J. Transplant. 2018, 18, 1518–1526. [Google Scholar] [CrossRef]
- Wong, A.; Zamel, R.; Yeung, J.; Bader, G.D.; Dos Santos, C.C.; Bai, X.; Wang, Y.; Keshavjee, S.; Liu, M. Potential therapeutic targets for lung repair during human ex vivo lung perfusion. Eur. Respir. J. 2020, 55, 1902222. [Google Scholar] [CrossRef]
- Johnston, M.R.; Christensen, C.W.; Minchin, R.F.; Rickaby, D.A.; Linehan, J.H.; Schuller, H.M.; Boyd, M.R.; Dawson, C.A. Isolated total lung perfusion as a means to deliver organ-specific chemotherapy: Long-term studies in animals. Surgery 1985, 98, 35–44. [Google Scholar]
- Johnston, M.R.; Minchin, R.; Shull, J.H.; Thénot, J.P.; McManus, B.M.; Terrill, R.; Boyd, M.R. Isolated lung perfusion with adriamycin. A preclinical study. Cancer 1983, 52, 404–409. [Google Scholar] [CrossRef]
- Beckers, P.A.J.; Versteegh, M.I.; Van Brakel, T.J.; Braun, J.; Van Putte, B.; Maat, A.P.; Vergauwen, W.; Rodrigus, I.; Hengst, W.D.; Lardon, F.; et al. Multicenter Phase II Clinical Trial of Isolated Lung Perfusion in Patients With Lung Metastases. Ann. Thorac. Surg. 2019, 108, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Hengst, W.A.D.; Hendriks, J.; Balduyck, B.; Rodrigus, I.; Vermorken, J.B.; Lardon, F.; Versteegh, M.I.; Braun, J.; Gelderblom, H.; Schramel, F.M.; et al. Phase II Multicenter Clinical Trial of Pulmonary Metastasectomy and Isolated Lung Perfusion with Melphalan in Patients with Resectable Lung Metastases. J. Thorac. Oncol. 2014, 9, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, P.R.; Iskender, I.; Machuca, T.; Hwang, D.; Deperrot, M.; Liu, M.; Keshavjee, S.; Waddell, T.K.; Cypel, M. Modified in vivo lung perfusion allows for prolonged perfusion without acute lung injury. J. Thorac. Cardiovasc. Surg. 2014, 147, 774–782. [Google Scholar] [CrossRef]
- Wang, H.; Bodenstein, M.; Markstaller, K. Overview of the Pathology of Three Widely Used Animal Models of Acute Lung Injury. Eur. Surg. Res. 2008, 40, 305–316. [Google Scholar] [CrossRef]
- Guenthart, B.A.; O’Neill, J.D.; Kim, J.; Queen, D.; Chicotka, S.; Fung, K.; Simpson, M.; Donocoff, R.; Salna, M.; Marboe, C.C.; et al. Regeneration of severely damaged lungs using an interventional cross-circulation platform. Nat. Commun. 2019, 10, 1985. [Google Scholar] [CrossRef]
- Byler, M.R.; Haywood, N.; Money, D.T.; Zhang, A.; Beller, J.P.; Charles, E.J.; Chancellor, W.Z.; Dahl, J.; Ta, H.; Zhao, Y.; et al. Two hours of protocol-driven in vivo lung perfusion improves lung function in sepsis model of acute respiratory distress syndrome. Presented at the 100th Annual Meeting (Virtual Event) of the American Association for Thoracic Surgery, 22 May 2020; Thoracic Breakout Session 2. Available online: https://www.webcastregister.live/aats_embed/catalogfilter4?day=Presentation (accessed on 23 May 2020).
- Calfee, C.S.; Delucchi, K.; Parsons, P.E.; Thompson, B.T.; Ware, L.B.; Matthay, M.A.; Network, N.A. Subphenotypes in acute respiratory distress syndrome: Latent class analysis of data from two randomised controlled trials. Lancet Respir. Med. 2014, 2, 611–620. [Google Scholar] [CrossRef]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab treatment in COVID-19: A single center experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef]
- Ramadan, K.; Del Sorbo, L.; Cypel, M. In vivo lung perfusion as a platform for organ repair in acute respiratory distress syndrome. J. Thorac. Dis. 2019, 11, 30–34. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Timing | Occurs Within 7 Days of Known Insult or the Initial Decline in Respiratory Status |
|---|---|
| Imaging | Bilateral opacities noted on either CXR or CT scan that are not otherwise explained by fluid overload or cardiac failure |
| Categorization | Mild: PaO2/FiO2 = 200–300 mmHg Moderate: PaO2/FiO2 = 100–200 mmHg Severe: PaO2/FiO2 < 100 mmHg Assessed with PEEP 5 or greater |
| Sepsis |
|---|
| Pneumonia |
| Aspiration |
| Ventilator-induced lung injury |
| Pancreatitis |
| Trauma and burn Injury |
| Blood product administration |
| Cardiopulmonary bypass |
| Ischemia-reperfusion injury following lung transplantation |
| COVID-19 infection |
| Parameter | OCS | XPS |
|---|---|---|
| Perfusate | RBC + OCS solution | Steen solution |
| Perfusion goal | 1.5–2.0 L/min | 40% cardiac output |
| Portable? | Yes | No |
| Starting temperature | 34 °C | 32 °C |
| Target temperature | 37 °C | 37 °C |
| Respiratory rate | 12 | 7 |
| Tidal volume | 6 mL/kg | 7 mL/kg |
| PEEP | 5 cm H2O | 5 cm H2O |
| FiO2 | 21% | 21% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haywood, N.; Byler, M.R.; Zhang, A.; Roeser, M.E.; Kron, I.L.; Laubach, V.E. Isolated Lung Perfusion in the Management of Acute Respiratory Distress Syndrome. Int. J. Mol. Sci. 2020, 21, 6820. https://doi.org/10.3390/ijms21186820
Haywood N, Byler MR, Zhang A, Roeser ME, Kron IL, Laubach VE. Isolated Lung Perfusion in the Management of Acute Respiratory Distress Syndrome. International Journal of Molecular Sciences. 2020; 21(18):6820. https://doi.org/10.3390/ijms21186820
Chicago/Turabian StyleHaywood, Nathan, Matthew R. Byler, Aimee Zhang, Mark E. Roeser, Irving L. Kron, and Victor E. Laubach. 2020. "Isolated Lung Perfusion in the Management of Acute Respiratory Distress Syndrome" International Journal of Molecular Sciences 21, no. 18: 6820. https://doi.org/10.3390/ijms21186820
APA StyleHaywood, N., Byler, M. R., Zhang, A., Roeser, M. E., Kron, I. L., & Laubach, V. E. (2020). Isolated Lung Perfusion in the Management of Acute Respiratory Distress Syndrome. International Journal of Molecular Sciences, 21(18), 6820. https://doi.org/10.3390/ijms21186820