Abstract
Mastocytosis is rare disease in which genetic predisposition is not fully understood. The aim of this study was to analyze associations between mastocytosis and single nucleotide polymorphisms (SNPs) by a genome-wide association study (GWAS) approach. A total of 234 patients were enrolled in our study, including 141 with cutaneous mastocytosis (CM; 78 children and 63 adults) and 93 with systemic mastocytosis (SM, all adults). The control group consisted of 5606 healthy individuals. DNA samples from saliva or blood were genotyped for 551 945 variants using DNA microarrays. The prevalence of certain SNPs was found to vary substantially when comparing patients and healthy controls: rs10838094 of 5OR51Q1 was less frequently detected in CM and SM patients (OR = 0.2071, p = 2.21 × 10−29), rs80138802 in ABCA2 (OR = 5.739, p = 1.98 × 10−28), and rs11845537 in OTX2-AS1 (rs11845537, OR = 6.587, p = 6.16 × 10−17) were more frequently detected in CM in children and adults. Additionally, we found that rs2279343 in CYP2B6 and rs7601511 in RPTN are less prevalent in CM compared to controls. We identified a number of hitherto unknown associations between certain SNPs and CM and/or SM. Whether these associations are clinically relevant concerning diagnosis, prognosis, or prevention remains to be determined in future studies.
1. Introduction
Mastocytosis is a heterogeneous group of diseases defined by the abnormal accumulation of clonal mast cells (MC) in the skin, bone marrow, and/or other visceral organs. The diagnosis of systemic mastocytosis (SM) is based on WHO criteria, including the basal serum tryptase level, histopathological and immunophenotypic (CD2/CD25) features of MCs, and somatic KIT mutations in codon 816. Mastocytosis can be divided into 7 variants: cutaneous mastocytosis (CM), indolent systemic mastocytosis (ISM), smoldering SM (SSM), SM with an associated hematological neoplasm (SM-AHN), aggressive SM (ASM), MC leukemia (MCL), and MC sarcoma (MCS) [1].
The majority of children with CM have a favorable prognosis. In contrast, in adults, mastocytosis usually presents as SM, and sometimes progresses to an aggressive disease [2,3,4,5,6,7,8].
In most patients with SM, somatic mutations in the KIT gene are found, the most prevalent in SM being D816V (rs121913507, D [GAC] > V [GTC]). The protein product of KIT (KIT = CD117) is a transmembrane receptor for the stem cell factor, a major regulator of MC differentiation and survival. The KIT D816V mutation results in SCF-independent differentiation of MCs. KIT D816V is detected in more than 80% of all adults with SM. In children with CM, this mutation is less frequent (35%) and other mutations, located in gene regions encoding the external cellular domain of KIT, are more commonly found in childhood patients (45%) [7,9,10].
Genetic studies performed so far in CM and SM focused on the gene polymorphisms of cytokines and their receptors (IL-13, IL-6, IL6R, IL-31, IL4R, VEGFA), TLRs and variants of the KIT gene. These studies have shown that some cytokine or cytokine receptor gene polymorphisms may be associated with the presence of SM and/or CM [11,12,13,14,15,16]. Other studies performed in ISM found associations of SM disease with SNPs in RAB27A, ETS1, ITGB1, MLL3, and ITGAV genes [17].
In advanced SM, additional recurrent somatic mutations involving genes encoding factors regulating splicing, signaling transmission, and epigenetic processes have recently been described [17,18,19,20,21]. The most frequently mutated genes are TET-2, DNMT3A, and ASXL1 [18,19,20,21,22].
In our study, we analyzed the genetic background of CM and SM using a genome wide association technique.
2. Results
2.1. Comparison of All Mastocytosis Patients with the Controls
Of the 281 811 analyzed SNPs, 9 showed a statistically different frequency in mastocytosis patients. Four of the SNPs were more frequently found in mastocytosis patients compared to controls: rs80138802 in ABCA2 (OR = 5.739, (95% CI; 4.156–7.925), p = 1.98 × 10−27), rs11845537 in OTX2-AS1 (OR = 5.625, (95% CI; 3.859–8.199), p = 1.60 × 10−18), rs1611207 in HLA-V (OR = 2.105, (95% CI; 1.717–2.581), p = 7.25 × 10−8), and rs1778155 in PDE4DIP (OR = 2.032, (95% CI; 1.649–2.504), p = 3.26 × 10−6) genes (Table 1, Figure 1).

Table 1.
Comparison of the frequency of single nucleotide polymorphisms (SNPs) in mastocytosis patients (n = 234) and control groups (n = 5606).
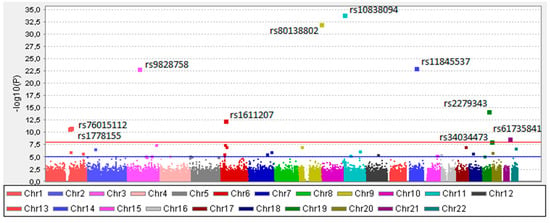
Figure 1.
The “Manhattan” plot for the genome-wide association study of all analyzed mastocytosis patients. On the x-axis, each color represents different chromosomes. The log10 of the unadjusted p-values (without multiple testing corrections) are shown at the y-axis. The blue line indicates the suggestive association threshold (10−5), while red line indicates GWAS significant threshold (10−8).
Five polymorphisms were found to be less frequently detectable in mastocytosis than in controls: rs61735841 in FTCD (OR = 0.026; 95% CI 0.003612–0.1833; p = 4.34 × 10−5), rs10838094 in OR51Q1 (OR = 0.2071; 95% CI 0.1572–0.2728; p = 2.21 × 10−29), rs2279343 in CYP2B6, OR = 0.2795; 95%CI; 0.199–0.3924; p = 2.32 × 10−10), rs76015112 in RPTN (OR = 2.965; 95% CI 0.205–0.4289; p = 2.94 × 10−7) genes and rs9828758 (OR = 0.1467; 95% CI 0.095–0.23; p = 2.94 × 10−7) near RP11 gene (Table 1, Figure 1, Figures S3 and S4).
Tables S1–S5 provides an analysis of the frequency of genotypes, alleles, and their mode of inheritance and expression frequencies in SM and CM patients. Apart from the rs80138802 A > C, ABCA2 gene polymorphism, where a recessive mode of inheritance was found, the other gene polymorphisms showed a dominant mode of inheritance.
2.2. Comparison of Patients with SM and Controls
When analyzing patients with SM (88 ISM and 3 SSM), only 3 SNPs were identified to be more or less prevalent in SM patients compared to the controls. Two SNPs, rs2857596 (OR = 2.582 (95% CI; 1.909–3.492), p = 2.45 ×10−5) located near NRC3 and rs498404 (OR = 2.697 (95% CI; 0.1634–3.716) p = 2.46 × 10−5) near TTC398 genes were more frequently detected, whereas rs10838094 in OR51Q1 (OR = 0.2761 (95% CI; 0.1864–0.4088, p = 1.83 × 10−6) was less frequently detected in SM patients compared to controls (Table 2, Figures S1 and S2).
Table 2.
Comparison of the frequency of SNPs in patients with systemic disease (n = 93) and control groups (n = 5606).
2.3. Comparison of CM Patients with Controls
We found that 6 SNPs were differently expressed in CM (both children and adults) patients compared to the controls. Two SNPs were more frequently detected: ABCA2 (rs80138802, OR = 6.969 (95% CI; 4.749–10.23), p = 4.20 × 10−25) and OTX2-AS1 (rs11845537, OR = 6.587 (95% CI; 4.235–10.24) p = 6.16 × 10−17), and 4 SNPs were less frequently identified compared to controls: OR51B5 (rs10838094, OR = 0.1646 (95% CI; 0.1119–0.2421), p = 3.28 × 10−20), CYP2B6 (rs2279343, OR = 0.181 (95% CI; 0.1073–0.3053), p = 3.26 × 10−8), RPTN (rs76015112, OR = 0.1427 (95% CI; 0.0732–0.2783), p = 1.35 × 10−6), and rs9828758 (OR = 0.1454 (95% CI; 0.0862–0.2452), p = 3.68 × 10−12) located near the RP11 gene (Table 3).
Table 3.
Comparison of the frequency of SNPs in patients with cutaneous mastocytosis (n = 141) and control groups (n = 5606).
A comparison of the results found in CM or SM patients with controls indicated that only rs10838094 in OR51B5 gene is less frequent in both groups, with strong statistic p value (2.40 × 10−25 for CM and 6.71 × 10−12 for SM) (Table 2 and Table 3, Figures S1 and S2).
The SNPs rs2857596 and rs498404 were more prevalent in SM, whereas rs80138802 in ABCA2 and rs11845537 in OTX2-AS1 genes were more frequently detected in CM patients. Additionally, we found that in CM patients (but not SM patients), the polymorphisms rs2279343 in CYP2B6 and rs76015112 in RPTN genes were statistically less frequently detected than in controls.
2.4. Comparison of Children and Adult Patients with Cutaneous Mastocytosis with Controls
When we separately compared adults with CM (adCM) and children with CM (chCM) with the control group, we found differences in the frequency of several SNPs. In both groups, two polymorphisms were expressed more frequently than in the control group (rs80138802 in the ABCA2 gene and rs11845537 in the OTX2-AS1 gene). Additionally, in children with CM, 2 SNPs were statistically less frequent (rs10838094 in OR51Q1 gene and rs9828758) (Table 4A,B).
Table 4.
Comparison of the frequency of SNPs in the adult (A) and child patients (B) with cutaneous mastocytosis (n = 63) and the control groups (n = 5606).
We also compared our data with previously published results. In particular, we examined the genes of cytokines, growth factors, and transcription factors described as potential factors associated with mastocytosis (Table S6), genes involved in epigenetic processes, transcription and cell proliferation (Table S7), and genes where the differences in expression were described in indolent systemic mastocytosis (Table S11). Most of the analyzed genes showed significant differences in prevalence when analyzed separately. However, after correcting the data for false discovery rates and multivariate testing, no significant correlations were found (Tables S8–S10 and S12–S14).
3. Discussion
In recent years, genetic background has been implicated in the pathogenesis of CM and SM. However, only little is known about specific genes and SNPs contributing to the clinical course and prognosis in mastocytosis patients. The results of our study suggest that there is an association between mastocytosis and 9 SNPs which were not described in mastocytosis contexts so far. Four SNPs were more prevalent (in ABCA2, OTX2-AS1, HLA-V, and PDE4DIP genes) and 5 were less prevalent (in RPTN, CYP2B6, OR51Q1, FTCD, and rs9828758 near RP11 genes) in mastocytosis patients compared to a control cohort. Further studies on these SNPs may lead to new insights into the pathogenesis of mastocytosis and the development of new preventive or interventional medication.
Genotypes CC and CA of the ABCA2 (rs80138802 A > C) gene were more frequent in patients than in the controls and were inherited in recessive mode. These polymorphisms were especially more frequent in CM patients. An attractive hypothesis would be that patients with the ABCA2 (rs80138802 A > C) genotype have an increased risk of developing CM. An association between this genotype and adulthood CM, as well as childhood CM, was found. In the SM group of patients, this allele is also more prevalent, but the association did not reach statistical significance (p = 0.001482, Table 2).
ABCA1 and ABCA2 genes (ABCA—ATP Binding Cassette Subfamily A Member) encode the membrane transporters involved in lipid metabolism and drug elimination. The overexpression of ATP-binding cassette transporters is a major adaptive advantage used by tumor cells to evade the accumulation of cytotoxic agents. The expression of ABC transporters has thus been linked with multidrug resistance phenotypes through the efflux of small drugs via ATP-dependent transport [23,24]. One of the drugs affected is imatinib, which is sometimes applied in patients with KIT D816V-negative SM [2,25,26,27].
However, the role of ABC transporters has not been studied in detail in the mastocytosis context so far. In particular, it remains unknown whether this gene polymorphism plays a role in the resistance of neoplastic (mast) cells against TKI D816V-targeting drugs, like midostaurin or avapritinib.
Several other gene SNPs were also found to be more prevalent in patients with CM and/or SM, including OTX2-AS1 (rs11845537 G > A), PDE4DIP (rs1778155 C > T), HLA-V (29759876 A > G), RPTN (152129094 G > A), CYP2B6 (rs2279343 G > A, OR51Q1 (rs10838094 A > G), and FTCD (47558552 A > G). So far, little is known about the function and clinical implications of these genes, and no studies exploring the impact of these SNPs in the mastocytosis context are available.
Some of the associations were striking. For example, polymorphism rs11845537 G > A of the OTX2-AS1 gene was frequently observed both in adults and in children with CM. In fact, patients with an A allele were found to have a 6 to 7 times higher prevalence of mastocytosis compared to the controls. The genotype AA and AG were more frequent in both children and adult patients and the allele A was also found to be inherited in a dominant mode.
OTX2 antisense RNA 1 (head to head) long-noncoding RNA, is a transcription factor known to play an important role in controlling the expression of the OTX2-AS1 gene. OTX2 is an epigenetic factor, playing a role in transcription repression, chromatin remodeling, histone modification, and cell cycle regulation [24,28]. Increased amounts of OTX2-AS1 were observed in exosomes in bladder cancers [28]. Somatic mutation of the genes which play a role in epigenetic regulation of gene expression are described in the advanced form of mastocytosis. So far, however, the potential role and impact of the OTX2-AS1 gene in mastocytosis remain unknown [29].
So far, several gene SNPs located in cytokine genes, their receptors, and toll-like receptors have been identified in mastocytosis [11,12,13,14,15]. Other genes were described in the context of epigenetic processes regulation in mastocytosis [19,20,21,22]. We performed analyses of those genes in our study. Most of the analyzed genes showed significant differences in the prevalence when analyzed separately. However, the analysis using the correction for the false discovery rate showed insignificant results.
Our data add another set of potentially important and clinically interesting gene SNPs in mastocytosis. However, it is difficult to define the real impact of these SNPs for several reasons. First, the number of patients analyzed in each subgroup was too small to draw definitive conclusions regarding the pathogenetic impact of these SNPs. Second, our data need to be verified and confirmed in other independent prospective studies. Third, preclinical models exploring the potential functional role of these SNPs are lacking. Therefore, we regard our study as an interesting starting point of biomedical research where each of the identified gene SNP that clusters in distinct forms of CM and/or SM should be validated in future studies.
In conclusion, the results of our study suggest associations between mastocytosis variants and SNP which have not been described so far and which may potentially have clinical and prognostic implications. Our results are promising but require further validation in larger studies with several more patients with mastocytosis from other EU countries. Additional future research using gene sequencing techniques and in vitro studies on the functional role of identified SNPs on mast cell physiology are needed and planned.
4. Patients and Methods
4.1. Patient Groups
The patients included in this study were recruited between 2008 and 2019 from patients seen at the Medical University of Gdansk in Poland, the University Medical Center in Groningen in the Netherlands, and the Medical University in Vienna, Austria.
A total of 234 patients were included. Of these patients, 141 were diagnosed with CM and 93 with SM based on WHO criteria [1,2,3,4]. Of the patients with CM (all from Poland), 78 were children (42 boys and 36 girls, mean age 4.2 ± 3.5 years) and 63 were adults (50 females and 13 males, age range 18–72 years; mean age 37.6 ± 13.7 years), of which 74 (94.9%) presented with maculopapular cutaneous mastocytosis (MPCNM) and 4 (5.1%) with diffuse cutaneous mastocytosis (DCM). All adult patients with CM presented with MPCM; adult patients were checked for SM and they did not fulfil SM criteria. Of the 93 patients with SM (29 males and 64 females, age range 25–76 years; mean age 40.2 ± 8.2), 88 were diagnosed with ISM, 3 with smoldering systemic mastocytosis (SSM), one with ASM, and one with MCL.
Of the 93 SM patients, 20 (all with ISM) were from the University Medical Center in Groningen in the Netherlands, 23 were from the Medical University in Austria (MCL, ASM, SSM), and 50 patients (all with ISM) were from Poland.
The study protocol was approved by the Independent Bioethics Committee for Scientific Research of the Medical University of Gdansk, (NKBBN/331/2017), Groningen (METc 2008/340), and Vienna (1184/2014). All subjects provided written, informed consent prior to their participation in the study.
4.2. Control Group
Control donors were recruited between 2010 and 2012 within the research project TESTOPLEK and registered as the POPOLOUS collection at the Biobank Lab of The Department of Molecular Biophysics of The University of Lodz, Poland. Each donor gave written, informed consent to participate. Saliva was collected into Oragene OG-500 DNA collection/storage receptacles (DNA Genotek, Kanata, Canada) from each individual. The approval for this study was obtained from The University of Lodz’s Review Board (32/KBBN-UL/I/2018). All procedures were performed in accordance with the Declaration of Helsinki (ethical principles for medical research involving human subjects) [30,31].
From over 6047 adult individuals throughout Poland, a total of 5606 participants were involved in a matched control group of the study. The exclusion criteria were diabetes, myeloid disorders, bone marrow transplantation, and cancer. There were 2860 (51%) females and 2746 (49%) males, aged from 22 to 77 years (42.86 ± 14.85 and 42.03 ± 14.72, respectively).
Based on mitochondrial DNA (mtDNA) studies Poles can be considered as genetically homogenous, with the same pattern as other population within European countries (e.g., The Netherlands, Austria, Spain, Portugal, Sardinia and Russia) [32].
4.3. DNA Isolation
The samples of the peripheral blood (patient’s) or saliva (control) were collected and stored at −80 °C.
Genomic DNA was extracted from 200 µL of blood using the Magna Pure LC 2.0 (Roche, Rotkreuz, Switzerland) with the DNA Isolation Kit I High Performance protocol launched.
Genomic DNA from saliva samples was manually isolated from 500 µL using the manufacturer’s instructions (PrepitL2P, PD-PR-052, DNA Genotek, Kanata, ON, Canada). The elution volume was 50 µL.
A total of 234 DNA samples from patients and 5606 from control group were quantified using broad range Quant-iT™ dsDNA Broad Range Assay Kit (Invitrogen™, Carlsbad, CA, USA). All DNA samples underwent quality control in PCR reaction for sex determination [33].
4.4. Microarrays Analysis
DNA samples were genotyped for 558 231 SNPs using the 24 × 1 Infinium HTS Human Core Exome (Illumina Inc., San Diego, CA, USA) microarrays according to the protocol provided by the manufacturer.
4.5. Statistical Methods
A preliminary statistical analysis of the database containing the results of the genotyping of 5840 individuals for 558,231 SNPs was carried out in the PLINK 1.9 program. From the statistical analysis, 276,420 SNPs were excluded because:
- (1)
- 16,119 variants were removed due to missing genotype data;
- (2)
- 3340 variants were removed due to Hardy–Weinberg exact test;
- (3)
- 256,961 variants were removed due to minor allele threshold.
To discover and validate genetic risk-factors for mastocytosis, the chi-square statistic with odds ratio and 95% confidence interval for 2 × 2 contingency tables were calculated using PLINK 1.9. To adjust for multiple testing, the thresholds of p < 1 × 10−5 and p < 5 × 10−8 were used for suggestive and genome-wide significant associations, respectively [34]. Regional associations were visualized with the Haploview or LocusZoom web tool (http://locuszoom.org/).
5. Conclusions
The results of our study suggest an association between mastocytosis and 9 SNPs which were not described in mastocytosis so far, which may be important for the pathogenesis of the disease. Moreover, 4 SNPs were more prevalent (ABCA2, OTX2-AS1, HLA-V, and PDE4DIP) and 5 were found to have less prevalence (RPTN, CYP2B6, OR51Q1, FTCD genes, and rs9828758).
In the future, for each identified variant, we plan to perform in vitro evaluation of its effects on mast cell physiology, and, in case if these variant would be found non-causal, to sequence adjacent loci for other functional variants linked to the reported ones
Supplementary Materials
The following are available online at https://www.mdpi.com/1422-0067/21/15/5506/s1.
Author Contributions
Conceptualization: B.N., D.S., M.S.-K., M.N., Methodology, Software and Statistic: M.S.-K., M.S., D.S., contribute to the conception and design of the work: M.S.-K., M.S., Clinical data collection: M.N., A.G., M.L., M.G.-N., P.V., J.N.G.O.E., J.v.D., Control group collection and analysis: M.S., D.S., M.S.-K., Writing & Original Draft Preparation—B.N., M.N., P.V., Review & Editing final version: B.N., M.S.-K., D.S., M.L., A.G., L.K., M.G.-N., R.J.N., P.V., J.v.D., J.N.G.O.E. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the Polish Ministry of Science and Higher Education—grants no ST 02-0066/07/253, ST 02-0141/07/231 and DIR/WK/2017/01. POPULOUS collection was financed by the Polish POIG Grant number: 01.01.02-10-005/08 TESTOPLEK from the European Regional Development Fund. P.V. was supported by the Austrian Science Fund (FWF)—grants P32470, F4701-B20 and F4704-B20.
Acknowledgments
Thank you to A. Siewierska-Górska and E. Kępka for their excellent technical assistance.
Conflicts of Interest
The authors: B.N., M.S.-K., D.S., M.L., A.G., L.K., M.G.-N., R.J.N., J.v.D., J.N.D.O.E. declare no conflict of interest. P.V. has no study-related COI. Unrelated COI of P.V.: P.V. received honoraria from BMS-Celgene, Incyte, Novartis, Pfizer, Blueprint, and Deciphera, and a research grant from Pfizer and Celgene.
References
- Valent, P.; Horny, H.P.; Escribano, L.; Longley, B.J.; Li, C.Y.; Schwartz, L.B.; Marone, G.; Nunez, R.; Akin, C.; Sotlar, K.; et al. Diagnostic criteria and classification of mastocytosis: A consensus proposal. Leuk Res. 2001, 25, 603–625. [Google Scholar] [CrossRef]
- Valent, P.; Akin, C.; Escribano, L.; Fodinger, M.; Hartmann, K.; Brockow, K.; Castells, M.; Sperr, W.R.; Kluin-Nelemans, H.C.; Hamdy, N.A.; et al. Standards and standardization in mastocytosis: Consensus statements on diagnostics, treatment recommendations and response criteria. Eur. J. Clin. Investig. 2007, 37, 435–453. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Akin, C.; Hartmann, K.; Nilsson, G.; Reiter, A.; Hermine, O.; Sotlar, K.; Sperr, W.R.; Escribano, L.; George, T.I.; et al. Advances in the Classification and Treatment of Mastocytosis: Current Status and Outlook toward the Future. Cancer Res. 2017, 77, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Akin, C.; Metcalfe, D.D. Mastocytosis: 2016 updated WHO classification and novel emerging treatment concepts. Blood 2017, 129, 1420–1427. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, K.; Escribano, L.; Grattan, C.; Brockow, K.; Carter, M.C.; Alvarez-Twose, I.; Matito, A.; Broesby-Olsen, S.; Siebenhaar, F.; Lange, M.; et al. Cutaneous manifestations in patients with mastocytosis: Consensus report of the European Competence Network on Mastocytosis; the American Academy of Allergy, Asthma & Immunology; and the European Academy of Allergology and Clinical Immunology. J. Allergy Clin. Immunol. 2016, 137, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Theoharides, T.C.; Valent, P.; Akin, C. Mast Cells, Mastocytosis, and Related Disorders. N. Engl. J. Med. 2015, 373, 1885–1886. [Google Scholar] [CrossRef]
- Arock, M.; Sotlar, K.; Akin, C.; Broesby-Olsen, S.; Hoermann, G.; Escribano, L.; Kristensen, T.K.; Kluin-Nelemans, H.C.; Hermine, O.; Dubreuil, P.; et al. KIT mutation analysis in mast cell neoplasms: Recommendations of the European Competence Network on Mastocytosis. Leukemia 2015, 29, 1223–1232. [Google Scholar] [CrossRef]
- Lange, M.; Lugowska-Umer, H.; Niedoszytko, M.; Wasag, B.; Limon, J.; Zawrocki, A.; Nedoszytko, B.; Sobjanek, M.; Plata-Nazar, K.; Nowicki, R. Diagnosis of Mastocytosis in Children and Adults in Daily Clinical Practice. Acta Derm. Venereol. 2016, 96, 292–297. [Google Scholar] [CrossRef]
- Bibi, S.; Langenfeld, F.; Jeanningros, S.; Brenet, F.; Soucie, E.; Hermine, O.; Damaj, G.; Dubreuil, P.; Arock, M. Molecular defects in mastocytosis: KIT and beyond KIT. Immunol. Allergy Clin. N. Am. 2014, 34, 239–262. [Google Scholar] [CrossRef]
- Soucie, E.; Brenet, F.; Dubreuil, P. Molecular basis of mast cell disease. Mol. Immunol. 2015, 63, 55–60. [Google Scholar] [CrossRef]
- Daley, T.; Metcalfe, D.D.; Akin, C. Association of the Q576R polymorphism in the interleukin-4 receptor alpha chain with indolent mastocytosis limited to the skin. Blood 2001, 98, 880–882. [Google Scholar] [CrossRef] [PubMed]
- Nedoszytko, B.; Niedoszytko, M.; Lange, M.; van Doormaal, J.; Glen, J.; Zablotna, M.; Renke, J.; Vales, A.; Buljubasic, F.; Jassem, E.; et al. Interleukin-13 promoter gene polymorphism -1112C/T is associated with the systemic form of mastocytosis. Allergy 2009, 64, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Rausz, E.; Szilagyi, A.; Nedoszytko, B.; Lange, M.; Niedoszytko, M.; Lautner-Csorba, O.; Falus, A.; Aladzsity, I.; Kokai, M.; Valent, P.; et al. Comparative analysis of IL6 and IL6 receptor gene polymorphisms in mastocytosis. Br. J. Haematol. 2013, 160, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Nedoszytko, B.; Lange, M.; Renke, J.; Niedoszytko, M.; Zablotna, M.; Glen, J.; Nowicki, R. The Possible Role of Gene Variant Coding Nonfunctional Toll-Like Receptor 2 in the Pathogenesis of Mastocytosis. Int. Arch. Allergy Immunol. 2018, 177, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Glen, J.; Zablotna, M.; Nedoszytko, B.; Sokolowska-Wojdylo, M.; Rebala, K.; Lugowska-Umer, H.; Niedoszytko, M.; Gorska, A.; Sikorska, M.; et al. Interleukin-31 Polymorphisms and Serum IL-31 Level in Patients with Mastocytosis: Correlation with Clinical Presen-tation and Pruritus. Acta Derm. Venereol. 2017, 97, 47–53. [Google Scholar] [CrossRef]
- Orfao, A.; Garcia-Montero, A.C.; Sanchez, L.; Escribano, L. Recent advances in the understanding of mastocytosis: The role of KIT mutations. Br. J. Haematol. 2007, 138, 12–30. [Google Scholar] [CrossRef]
- Niedoszytko, M.; Oude Elberink, J.N.; Bruinenberg, M.; Nedoszytko, B.; de Monchy, J.G.; te Meerman, G.J.; Weersma, R.K.; Mulder, A.B.; Jassem, E.; van Doormaal, J.J. Gene expression profile, pathways, and transcriptional system regulation in indolent systemic mastocytosis. Allergy 2011, 66, 229–237. [Google Scholar] [CrossRef]
- Traina, F.; Visconte, V.; Jankowska, A.M.; Makishima, H.; O’Keefe, C.L.; Elson, P.; Han, Y.; Hsieh, F.H.; Sekeres, M.A.; Mali, R.S.; et al. Single nucleotide polymorphism array lesions, TET2, DNMT3A, ASXL1 and CBL mutations are present in systemic mastocytosis. PLoS ONE 2012, 7, e43090. [Google Scholar] [CrossRef]
- Schwaab, J.; Schnittger, S.; Sotlar, K.; Walz, C.; Fabarius, A.; Pfirrmann, M.; Kohlmann, A.; Grossmann, V.; Meggendorfer, M.; Horny, H.P.; et al. Comprehensive mutational profiling in advanced systemic mastocytosis. Blood 2013, 122, 2460–2466. [Google Scholar] [CrossRef]
- Damaj, G.; Joris, M.; Chandesris, O.; Hanssens, K.; Soucie, E.; Canioni, D.; Kolb, B.; Durieu, I.; Gyan, E.; Livideanu, C.; et al. ASXL1 but not TET2 mutations adversely impact overall survival of patients suffering systemic mastocytosis with associated clonal hematologic non-mast-cell diseases. PLoS ONE 2014, 9, e85362. [Google Scholar] [CrossRef]
- Jawhar, M.; Schwaab, J.; Schnittger, S.; Sotlar, K.; Horny, H.P.; Metzgeroth, G.; Muller, N.; Schneider, S.; Naumann, N.; Walz, C.; et al. Molecular profiling of myeloid progenitor cells in multi-mutated advanced systemic mastocytosis identifies KIT D816V as a distinct and late event. Leukemia 2015, 29, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Jawhar, M.; Schwaab, J.; Schnittger, S.; Meggendorfer, M.; Pfirrmann, M.; Sotlar, K.; Horny, H.P.; Metzgeroth, G.; Kluger, S.; Naumann, N.; et al. Additional mutations in SRSF2, ASXL1 and/or RUNX1 identify a high-risk group of patients with KIT D816V(+) advanced systemic mastocytosis. Leukemia 2016, 30, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Davies, W.; Tew, K.D. ATP-binding Cassette transporter-2 (ABCA2) as a Therapeutic Target. Biochem Pharmacol 2018, 151, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Reactome Pathways Database. Available online: https://reactome.org/ (accessed on 22 June 2020).
- Alvarez-Twose, I.; Matito, A.; Morgado, J.M.; Sanchez-Munoz, L.; Jara-Acevedo, M.; Garcia-Montero, A.; Mayado, A.; Caldas, C.; Teodosio, C.; Munoz-Gonzalez, J.I.; et al. Imatinib in systemic mastocytosis: A phase IV clinical trial in patients lacking exon 17 KIT mutations and review of the literature. Oncotarget 2017, 8, 68950–68963. [Google Scholar] [CrossRef]
- Ustun, C.; DeRemer, D.L.; Akin, C. Tyrosine kinase inhibitors in the treatment of systemic mastocytosis. Leuk Res. 2011, 35, 1143–1152. [Google Scholar] [CrossRef]
- Valent, P.; Akin, C.; Sperr, W.R.; Mayerhofer, M.; Fodinger, M.; Fritsche-Polanz, R.; Sotlar, K.; Escribano, L.; Arock, M.; Horny, H.P.; et al. Mastocytosis: Pathology, genetics, and current options for therapy. Leuk Lymphoma 2005, 46, 35–48. [Google Scholar] [CrossRef]
- Berrondo, C.; Flax, J.; Kucherov, V.; Siebert, A.; Osinski, T.; Rosenberg, A.; Fucile, C.; Richheimer, S.; Beckham, C.J. Expression of the Long Non-Coding RNA HOTAIR Correlates with Disease Progression in Bladder Cancer and Is Contained in Bladder Cancer Patient Urinary Exosomes. PLoS ONE 2016, 11, e0147236. [Google Scholar] [CrossRef]
- Jung, H.; Chae, Y.C.; Kim, J.Y.; Jeong, O.S.; Kook, H.; Seo, S.B. Regulatory role of G9a and LSD1 in the Transcription of Olfactory Receptors during Leukaemia Cell Differentiation. Sci. Rep. 2017, 7, 46182. [Google Scholar] [CrossRef]
- Strapagiel, D.; Sobalska, M.; Słomka, M.; Marciniak, B. Biobank Lodz—DNA Based Biobank at the University of Lodz, Poland. Open J. Bioresour. 2016, 3, e6. [Google Scholar] [CrossRef]
- Dobrowolska, S.; Michalska-Madej, J.; Słomka, M.; Sobalska-Kwapis, M.; Strapagiel, D. Biobank Łódź®—Population based biobank at the University of Łódź, Poland. Eur. J. Transl. Clin. Med. 2019, 2, 85–95. [Google Scholar] [CrossRef]
- Jarczak, J.; Grochowalski, L.; Marciniak, B.; Lach, J.; Slomka, M.; Sobalska-Kwapis, M.; Lorkiewicz, W.; Pulaski, L.; Strapagiel, D. Mitochondrial DNA variability of the Polish population. Eur. J. Hum. Genet. 2019. [Google Scholar] [CrossRef] [PubMed]
- Strapagiel, D.; Slomka, M.; John, S.; Gina, S. Method for Determination of Gender. Patent 232652, 4 February 2019. [Google Scholar]
- Risch, N.; Merikangas, K. The future of genetic studies of complex human diseases. Science 1996, 273, 1516–1517. [Google Scholar] [CrossRef] [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).