Serum Matrix Metalloproteinases and Left Atrial Remodeling—The Hoorn Study

 , , ,
, , ,
Abstract
1. Introduction
2. Results
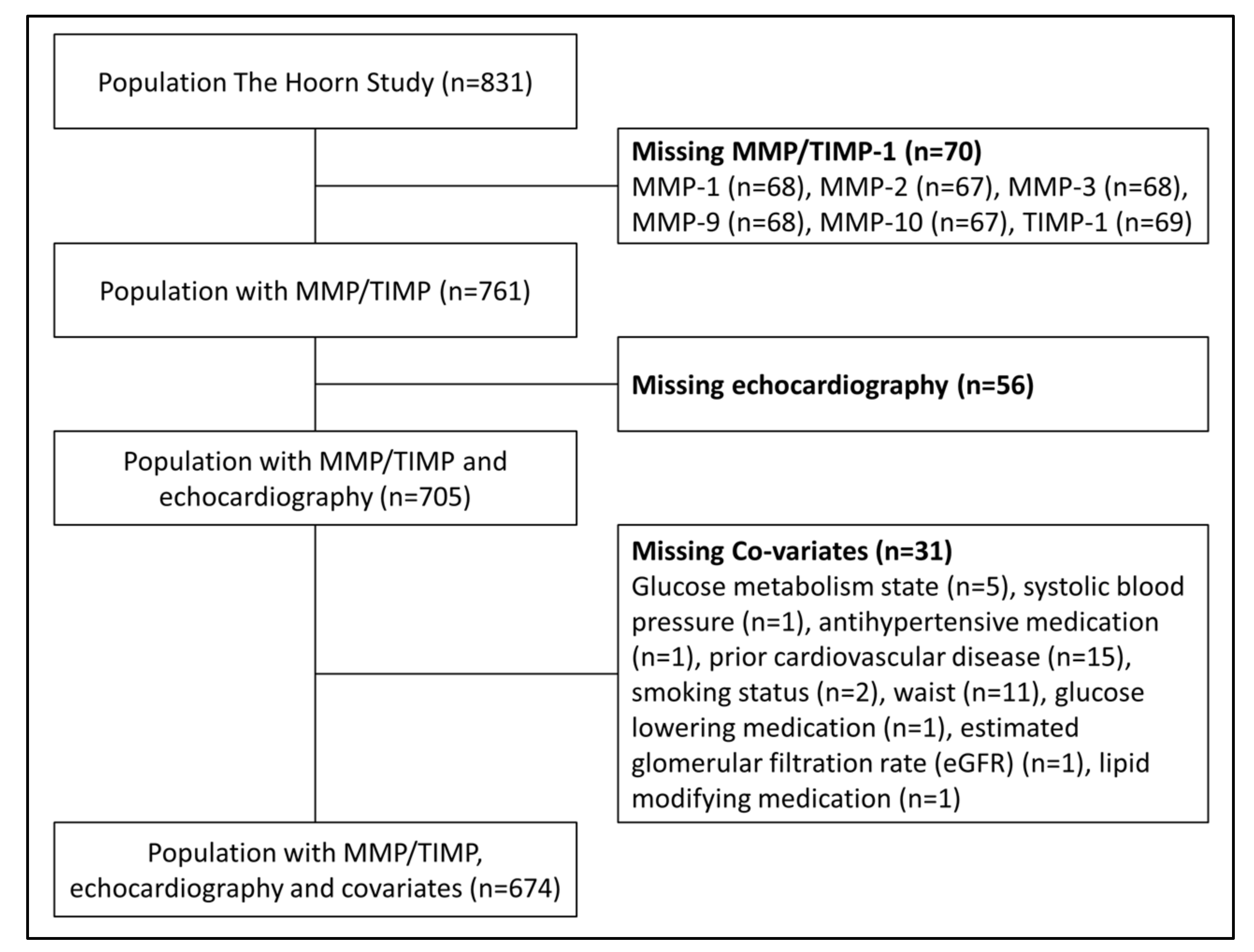
2.1. Study Population
2.2. Characteristics of the Study Population According to Tertiles of LA Volume Index
2.3. Association between Serum MMPs and TIMP-1 and LA Volume Index
2.4. Stratification According to Sex
2.5. TIMP-1
2.6. Additional Analyses
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Measurement of Serum MMPs and TIMP-1
4.3. Echocardiography
4.4. Covariates
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Takemoto, Y.; Barnes, M.E.; Seward, J.B.; Lester, S.J.; Appleton, C.A.; Gersh, B.J.; Bailey, K.R.; Tsang, T.S. Usefulness of left atrial volume in predicting first congestive heart failure in patients > or = 65 years of age with well-preserved left ventricular systolic function. Am. J. Cardiol. 2005, 96, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.A.; Lavie, C.J.; Milani, R.V.; Ventura, H.O. Left atrial volume index predictive of mortality independent of left ventricular geometry in a large clinical cohort with preserved ejection fraction. Mayo Clin. Proc. 2011, 86, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Hoit, B.D. Matrix metalloproteinases and atrial structural remodeling. J. Am. Coll. Cardiol. 2003, 42, 345–347. [Google Scholar] [CrossRef]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovas. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Visse, R.; Nagase, H. Matrix metalloproteinases and tissue inhibitors of metalloproteinases: Structure, function, and biochemistry. Circ. Res. 2003, 92, 827–839. [Google Scholar] [CrossRef]
- Spinale, F.G. Matrix metalloproteinases: Regulation and dysregulation in the failing heart. Circ. Res. 2002, 90, 520–530. [Google Scholar] [CrossRef]
- Montalvo, C.; Villar, A.V.; Merino, D.; Garcia, R.; Ares, M.; Llano, M.; Cobo, M.; Hurle, M.A.; Nistal, J.F. Androgens contribute to sex differences in myocardial remodeling under pressure overload by a mechanism involving TGF-beta. PLoS ONE 2012, 7, e35635. [Google Scholar] [CrossRef]
- Coronado, M.J.; Brandt, J.E.; Kim, E.; Bucek, A.; Bedja, D.; Abston, E.D.; Shin, J.; Gabrielson, K.L.; Mitzner, W.; Fairweather, D. Testosterone and interleukin-1beta increase cardiac remodeling during coxsackievirus B3 myocarditis via serpin A 3n. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H1726–H1736. [Google Scholar] [CrossRef]
- Giannakos, E.; Vardali, E.; Bartekova, M.; Fogarassyova, M.; Barancik, M.; Radosinska, J. Changes in activities of circulating MMP-2 and MMP-9 in patients suffering from heart failure in relation to gender, hypertension and treatment: A cross-sectional study. Physiol. Res. 2016, 65, S149–S152. [Google Scholar] [CrossRef]
- Collier, P.; Watson, C.J.; Voon, V.; Phelan, D.; Jan, A.; Mak, G.; Martos, R.; Baugh, J.A.; Ledwidge, M.T.; McDonald, K.M. Can emerging biomarkers of myocardial remodelling identify asymptomatic hypertensive patients at risk for diastolic dysfunction and diastolic heart failure? Eur. J. Heart Fail. 2011, 13, 1087–1095. [Google Scholar] [CrossRef]
- Collier, P.; Watson, C.J.; Waterhouse, D.F.; Dawkins, I.R.; Patle, A.K.; Horgan, S.; Conlon, C.M.; O’Hanlon, R.; Baugh, J.A.; Ledwidge, M.T.; et al. Progression of left atrial volume index in a population at risk for heart failure: A substudy of the STOP-HF (St Vincent’s Screening TO Prevent Heart Failure) trial. Eur. J. Heart Fail. 2012, 14, 957–964. [Google Scholar] [CrossRef]
- Hung, C.S.; Chou, C.H.; Wu, X.M.; Chang, Y.Y.; Wu, V.C.; Chen, Y.H.; Chang, Y.S.; Tsai, Y.C.; Su, M.J.; Ho, Y.L.; et al. Circulating tissue inhibitor of matrix metalloproteinase-1 is associated with aldosterone-induced diastolic dysfunction. J. Hypertens. 2015, 33, 1922–1930. [Google Scholar] [CrossRef] [PubMed]
- Lewkowicz, J.; Knapp, M.; Tankiewicz-Kwedlo, A.; Sawicki, R.; Kaminska, M.; Waszkiewicz, E.; Musial, W.J. MMP-9 in atrial remodeling in patients with atrial fibrillation. Ann. Cardiol. Angeiol. 2015, 64, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.S.; Park, S.; Park, S.I.; Oh, Y.T.; Choi, E.; Kim, J.Y.; Rhee, Y. Cardiac Dysfunction in Association with Increased Inflammatory Markers in Primary Aldosteronism. Endocrinol. Metab. 2016, 31, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Martos, R.; Baugh, J.; Ledwidge, M.; O’Loughlin, C.; Conlon, C.; Patle, A.; Donnelly, S.C.; McDonald, K. Diastolic heart failure: Evidence of increased myocardial collagen turnover linked to diastolic dysfunction. Circulation 2007, 115, 888–895. [Google Scholar] [CrossRef]
- Park, J.Y.; Ryu, S.K.; Choi, J.W.; Ho, K.M.; Jun, J.H.; Rha, S.W.; Park, S.M.; Kim, H.J.; Choi, B.G.; Noh, Y.K.; et al. Association of inflammation, myocardial fibrosis and cardiac remodelling in patients with mild aortic stenosis as assessed by biomarkers and echocardiography. Clin. Exp. Pharmacol. Physiol. 2014, 41, 185–191. [Google Scholar] [CrossRef]
- Sanchis, L.; Andrea, R.; Falces, C.; Llopis, J.; Morales-Ruiz, M.; Lopez-Sobrino, T.; Perez-Villa, F.; Sitges, M.; Sabate, M.; Brugada, J. Prognosis of new-onset heart failure outpatients and collagen biomarkers. Eur. J. Clin. Investig. 2015, 45, 842–849. [Google Scholar] [CrossRef]
- Sonmez, O.; Ertem, F.U.; Vatankulu, M.A.; Erdogan, E.; Tasal, A.; Kucukbuzcu, S.; Goktekin, O. Novel fibro-inflammation markers in assessing left atrial remodeling in non-valvular atrial fibrillation. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2014, 20, 463–470. [Google Scholar]
- Sundstrom, J.; Evans, J.C.; Benjamin, E.J.; Levy, D.; Larson, M.G.; Sawyer, D.B.; Siwik, D.A.; Colucci, W.S.; Wilson, P.W.; Vasan, R.S. Relations of plasma total TIMP-1 levels to cardiovascular risk factors and echocardiographic measures: The Framingham heart study. Eur. Heart J. 2004, 25, 1509–1516. [Google Scholar] [CrossRef]
- Takahashi, R.; Negishi, K.; Watanabe, A.; Arai, M.; Naganuma, F.; Ohyama, Y.; Kurabayashi, M. Serum syndecan-4 is a novel biomarker for patients with chronic heart failure. J. Cardiol. 2011, 57, 325–332. [Google Scholar] [CrossRef]
- Zile, M.R.; Jhund, P.S.; Baicu, C.F.; Claggett, B.L.; Pieske, B.; Voors, A.A.; Prescott, M.F.; Shi, V.; Lefkowitz, M.; McMurray, J.J.; et al. Plasma biomarkers reflecting profibrotic processes in heart failure with a preserved ejection fraction: Data from the prospective comparison of ARNI with ARB on management of heart failure with preserved ejection fraction study. Circ. Heart Fail. 2016, 9, e002551. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imag. 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Solomonov, I.; Zehorai, E.; Talmi-Frank, D.; Wolf, S.G.; Shainskaya, A.; Zhuravlev, A.; Kartvelishvily, E.; Visse, R.; Levin, Y.; Kampf, N.; et al. Distinct biological events generated by ECM proteolysis by two homologous collagenases. Proc. Natl. Acad. Sci. USA 2016, 113, 10884–10889. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, J.; Solomonov, I.; Zehorai, E.; Sagi, I. Multilevel regulation of matrix metalloproteinases in tissue homeostasis indicates their molecular specificity in vivo. Matrix Biol. J. Int. Soc. Matrix Biol. 2015, 44-46, 191–199. [Google Scholar] [CrossRef]
- Boyd, D.F.; Thomas, P.G. Towards integrating extracellular matrix and immunological pathways. Cytokine 2017, 98, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Dobaczewski, M.; Chen, W.; Frangogiannis, N.G. Transforming growth factor (TGF)-beta signaling in cardiac remodeling. J. Mol. Cell. Cardiol. 2011, 51, 600–606. [Google Scholar] [CrossRef]
- Egerstedt, A.; Berntsson, J.; Smith, M.L.; Gidlof, O.; Nilsson, R.; Benson, M.; Wells, Q.S.; Celik, S.; Lejonberg, C.; Farrell, L.; et al. Profiling of the plasma proteome across different stages of human heart failure. Nat. Commun. 2019, 10, 5830. [Google Scholar] [CrossRef]
- Spinale, F.G. Myocardial matrix remodeling and the matrix metalloproteinases: Influence on cardiac form and function. Physiol. Rev. 2007, 87, 1285–1342. [Google Scholar] [CrossRef]
- Kararigas, G.; Dworatzek, E.; Petrov, G.; Summer, H.; Schulze, T.M.; Baczko, I.; Knosalla, C.; Golz, S.; Hetzer, R.; Regitz-Zagrosek, V. Sex-dependent regulation of fibrosis and inflammation in human left ventricular remodelling under pressure overload. Eur. J. Heart Fail. 2014, 16, 1160–1167. [Google Scholar] [CrossRef]
- Petrov, G.; Regitz-Zagrosek, V.; Lehmkuhl, E.; Krabatsch, T.; Dunkel, A.; Dandel, M.; Dworatzek, E.; Mahmoodzadeh, S.; Schubert, C.; Becher, E.; et al. Regression of myocardial hypertrophy after aortic valve replacement: Faster in women? Circulation 2010, 122, S23–S28. [Google Scholar] [CrossRef]
- Villar, A.V.; Llano, M.; Cobo, M.; Exposito, V.; Merino, R.; Martin-Duran, R.; Hurle, M.A.; Nistal, J.F. Gender differences of echocardiographic and gene expression patterns in human pressure overload left ventricular hypertrophy. J. Mol. Cell. Cardiol. 2009, 46, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Voloshenyuk, T.G.; Gardner, J.D. Estrogen improves TIMP-MMP balance and collagen distribution in volume-overloaded hearts of ovariectomized females. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 299, R683–R693. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Cui, C.; Lainscak, M.; Zhang, X.; Li, J.; Huang, J.; Zhang, H.; Zheng, Z.; Hu, S. Type-specific dysregulation of matrix metalloproteinases and their tissue inhibitors in end-stage heart failure patients: Relationship between MMP-10 and LV remodelling. J. Cell. Mol. Med. 2011, 15, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.S.; Chou, C.H.; Liao, C.W.; Lin, Y.T.; Wu, X.M.; Chang, Y.Y.; Chen, Y.H.; Wu, V.C.; Su, M.J.; Ho, Y.L.; et al. Aldosterone Induces tissue inhibitor of metalloproteinases-1 expression and further contributes to collagen accumulation: From clinical to bench studies. Hypertension 2016, 67, 1309–1320. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Lein, M.; Laube, C.; Lichtinghagen, R. Blood specimen collection methods influence the concentration and the diagnostic validity of matrix metalloproteinase 9 in blood. Clin. Chim. Acta Int. J. Clin. Chem. 2001, 314, 241–244. [Google Scholar] [CrossRef]
- Jung, K.; Meisser, A.; Bischof, P. Blood sampling as critical preanalytical determinant to use circulating MMP and TIMP as surrogate markers for pathological processes. Int. J. Cancer 2005, 116, 1000–1001. [Google Scholar] [CrossRef]
- Mannello, F.; Luchetti, F.; Canonico, B.; Papa, S. Effect of anticoagulants and cell separation media as preanalytical determinants on zymographic analysis of plasma matrix metalloproteinases. Clin. Chem. 2003, 49, 1956–1957. [Google Scholar] [CrossRef]
- Makowski, G.S.; Ramsby, M.L. Use of citrate to minimize neutrophil matrix metalloproteinase-9 in human plasma. Anal. Biochem. 2003, 322, 283–286. [Google Scholar] [CrossRef]
- Verspaget, H.W.; Kuyvenhoven, J.P.; van Hoek, B. Preanalytical conditions and circulating matrix metalloproteinases. Transplantation 2005, 79, 745–746. [Google Scholar] [CrossRef]
- Peeters, S.A.; Engelen, L.; Buijs, J.; Chaturvedi, N.; Fuller, J.H.; Jorsal, A.; Parving, H.H.; Tarnow, L.; Theilade, S.; Rossing, P.; et al. Circulating matrix metalloproteinases are associated with arterial stiffness in patients with type 1 diabetes: Pooled analysis of three cohort studies. Cardiovasc. Diabetol. 2017, 16, 139. [Google Scholar] [CrossRef]
- Rutters, F.; Nijpels, G.; Elders, P.; Stehouwer, C.D.A.; van der Heijden, A.A.; Groeneveld, L.; t Hart, L.M.; Dekker, J.M.; Beulens, J.W.J. Cohort profile: The Hoorn studies. Int. J. Epidemiol. 2018, 47, 396–396j. [Google Scholar] [CrossRef] [PubMed]
- Mooy, J.M.; Grootenhuis, P.A.; de Vries, H.; Valkenburg, H.A.; Bouter, L.M.; Kostense, P.J.; Heine, R.J. Prevalence and determinants of glucose intolerance in a Dutch caucasian population. The Hoorn study. Diabetes Care 1995, 18, 1270–1273. [Google Scholar] [CrossRef]
- Henry, R.M.; Kamp, O.; Kostense, P.J.; Spijkerman, A.M.; Dekker, J.M.; van Eijck, R.; Nijpels, G.; Heine, R.J.; Bouter, L.M.; Stehouwer, C.D.; et al. Left ventricular mass increases with deteriorating glucose tolerance, especially in women: Independence of increased arterial stiffness or decreased flow-mediated dilation: The Hoorn study. Diabetes Care 2004, 27, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.S.; et al. Recommendations for chamber quantification: A report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J. Am. Soc. Echocardiogr. 2005, 18, 1440–1463. [Google Scholar]
- Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabetic Med. 1998, 15, 539–553. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of diet in renal disease study group. Annal. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- National Kidney, F. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Spijkerman, A.M.; Adriaanse, M.C.; Dekker, J.M.; Nijpels, G.; Stehouwer, C.D.; Bouter, L.M.; Heine, R.J. Diabetic patients detected by population-based stepwise screening already have a diabetic cardiovascular risk profile. Diabetes Care 2002, 25, 1784–1789. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Demographics | Lowest Tertile (n = 224) | Middle Tertile (n = 225) | Highest Tertile (n = 225) | ptrend | |||
|---|---|---|---|---|---|---|---|
| Women, % | 105 | (46.9) | 113 | (50.2) | 118 | (52.4) | 0.24 † |
| Age, years | 67.4 | ±6.1 | 67.9 | ±6.5 | 69.8 | ±7.9 | <0.01 |
| Obesity | |||||||
| BMI, kg/m2 | 27.3 | ±3.6 | 27.6 | ±3.9 | 27.1 | ±3.6 | 0.55 |
| Waist, cm | 95.3 | ±11.1 | 95.3 | ±11.1 | 95.2 | ±11.6 | 0.95 |
| Blood pressure | |||||||
| Systolic blood pressure | 140.5 | ±18.9 | 139.8 | ±19.8 | 144.0 | ±21.9 | 0.06 |
| Diastolic blood pressure, mmHg | 83.4 | ±10.4 | 83.4 | ±11.1 | 82.7 | ±11.2 | 0.46 |
| Hypertension | 143 | (63.8) | 149 | (66.2) | 171 | (76.0) | <0.01 † |
| Antihypertensive medication | 57 | (25.4) | 79 | (35.1) | 113 | (50.2) | <0.01 † |
| RAS inhibitors | 19 | (8.5) | 22 | (9.8) | 39 | (17.3) | <0.01 † |
| Cholesterol | |||||||
| Total cholesterol, mmol/L | 5.8 | ±1.1 | 5.7 | ±1.0 | 5.6 | ±1.0 | 0.02 |
| HDL cholesterol, mmol/L | 1.39 | ±0.40 | 1.40 | ±0.39 | 1.44 | ±0.44 | 0.18 |
| LDL cholesterol, mmol/L | 3.7 a | ±1.0 | 3.7 b | ±0.9 | 3.5 | ±0.9 | 0.03 |
| Triglycerides, mmol/L | 1.4 | (1.0–2.0) | 1.3 | (1.0–1.8) | 1.3 | (0.9–1.8) | <0.01 |
| Lipid modifying medication | 37 | (16.5) | 41 | (18.2) | 34 | (15.1) | 0.69 † |
| Glucose metabolism | |||||||
| HbA1c, % | 6.03 b | ±0.63 | 6.01 | ±0.82 | 6.03 | ±0.70 | 0.99 |
| Fasting plasma glucose, mmol/L | 6.24 | ±1.40 | 6.29 | ±1.51 | 6.48 | ±1.44 | 0.09 |
| Glucose lowering medication | 8 | (3.6) | 13 | (5.8) | 16 | (7.1) | 0.10 † |
| Glucose metabolism status | |||||||
| Normal | 100 | (44.6) | 101 | (44.9) | 72 | (32.0) | <0.01 † |
| Intermediate hyperglycaemia | 71 | (31.7) | 49 | (21.8) | 49 | (21.8) | |
| Type 2 diabetes mellitus | 53 | (23.7) | 75 | (33.3) | 104 | (46.2) | |
| Other CVD risk factors | |||||||
| Prior CVD | 92 | (41.1) | 108 | (48.0) | 120 | (53.3) | 0.01 † |
| Atrial fibrillation | 0 | (0.0) | 0 | (0.0) | 16 b | (7.1) | <0.01 † |
| Current smoking | 40 | (17.9) | 31 | (13.8) | 28 | (12.4) | 0.10 † |
| Kidney function | |||||||
| albuminuria | 17 | (7.6) | 14 | (6.2) | 37 | (16.4) | <0.01 † |
| eGFR (mL/min/1.73 m2) | 64.2 | ±10.6 | 65.8 | ±9.7 | 64.9 | ±11.4 | 0.53 |
| Echocardiographic data | |||||||
| LA volume index, mL/m2 | 17.4 | (15.9–18.7) | 22.0 | (21.0–23.4) | 29.9 | (26.8–34.5) | * |
| LV ejection fraction, % a | 62.8 c | ±7.3 | 62.4 d | ±7.2 | 59.7 d | ±9.7 | <0.01 |
| LV end diastolic diameter, mm | 49.7 a | ±5.2 | 50.2 b | ±5.7 | 52.1 | ±6.4 | <0.01 |
| Inter ventricular septum, mm | 9.4 b | ±2.1 | 9.6 b | ±2.2 | 10.3 | ±2.9 | <0.01 |
| Posterior wall thickness, mm | 8.8 a | ±1.4 | 8.9 b | ±1.4 | 9.3 | ±1.7 | <0.01 |
| LV mass index, gr/m2 | 83 a | ±20 | 88 b | ±22 | 101 | ±31 | <0.01 |
| E/A ratio | 0.81 | ± 0.19 | 0.84 | ±0.23 | 0.88 | ±0.35 | <0.01 |
| Wall motion abnormalities | 10 | (4.5) | 12 | (5.3) | 22 | (9.8) | 0.05 |
| Matrix metalloproteinases | |||||||
| MMP-1, ng/mL | 11.3 | (5.5–19.3) | 10.9 | (6.4–21.3) | 12.7 | (6.8–21.9) | 0.22 |
| MMP-2, ng/mL | 96 | (88–108) | 98 | (89–109) | 104 | (91–114) | <0.01 |
| MMP-3, ng/mL | 12.3 | (7.8–18.3) | 10.5 | (7.2–15.8) | 10.5 | (7.0–15.4) | 0.09 |
| MMP-9, ng/mL | 54 | (34–85) | 49 | (31–79) | 46 | (31–73) | <0.01 |
| MMP-10, pg/mL | 831 | (608–1243) | 838 | (616–1119) | 852 | (638–1232) | 0.88 |
| TIMP-1, ng/mL | 321 | (268–370) | 302 | (266–346) | 307 | (262–347) | 0.10 |
| Model | Overall | Men | Women | p-interaction | |
|---|---|---|---|---|---|
| β (95% CI) | β (95% CI) | β (95% CI) | Sex and MMP/TIMP | ||
| MMP-1 (SD) | 1 | 0.01 (−0.02; 0.03) | 0.03 (0.00; 0.06) | −0.01 (−0.04; 0.02) | 0.09 |
| 2 | 0.00 (−0.02; 0.02) | 0.02 (−0.01; 0.05) | −0.02 (−0.05; 0.01) | 0.06 | |
| 3 | 0.01 (−0.02; 0.03) | 0.03 (0.00; 0.06) | −0.02 (−0.05; 0.02) | 0.05 | |
| MMP-2 (SD) | 1 | 0.04 (0.01; 0.06) † | - | - | 0.58 |
| 2 | 0.03 (0.01; 0.05) * | - | - | 0.45 | |
| 3 | 0.03 (0.00; 0.05) * | - | - | 0.46 | |
| MMP-3 (SD) | 1 | −0.03 (−0.06; 0.00) * | - | - | 0.97 |
| 2 | −0.04 (−0.07; −0.10) † | - | - | 0.84 | |
| 3 | −0.04 (−0.07; −0.01) * | - | - | 0.86 | |
| MMP-9 (SD) | 1 | −0.04 (−0.06; −0.02) † | - | - | 0.47 |
| 2 | −0.04 (−0.06; −0.02) † | - | - | 0.46 | |
| 3 | −0.04 (−0.06; −0.02) † | - | - | 0.46 | |
| MMP-10 (SD) | 1 | 0.01 (−0.01; 0.03) | −0.01 (−0.04; 0.02) | 0.03 (0.00; 0.07) * | 0.07 |
| 2 | 0.01 (−0.01; 0.03) | −0.01 (−0.04; 0.02) | 0.04 (0.00; 0.07) * | 0.04 | |
| 3 | 0.01 (−0.01; 0.04) | −0.01 (−0.04; 0.03) | 0.04 (0.01; 0.07) * | 0.05 | |
| TIMP-1 (SD) | 1 | −0.01 (−0.04; 0.01) | 0.00 (−0.03; 0.03) | −0.04 (−0.08; 0.00) * | 0.10 |
| 2 | −0.02 (−0.04; 0.01) | 0.00 (−0.03; 0.03) | −0.05 (−0.09; −0.01) † | 0.03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Linssen, P.B.C.; Brunner-La Rocca, H.-P.; Schalkwijk, C.G.; Beulens, J.W.J.; Elders, P.J.M.; van der Heijden, A.A.; Slieker, R.C.; Stehouwer, C.D.A.; Henry, R.M.A. Serum Matrix Metalloproteinases and Left Atrial Remodeling—The Hoorn Study. Int. J. Mol. Sci. 2020, 21, 4944. https://doi.org/10.3390/ijms21144944
Linssen PBC, Brunner-La Rocca H-P, Schalkwijk CG, Beulens JWJ, Elders PJM, van der Heijden AA, Slieker RC, Stehouwer CDA, Henry RMA. Serum Matrix Metalloproteinases and Left Atrial Remodeling—The Hoorn Study. International Journal of Molecular Sciences. 2020; 21(14):4944. https://doi.org/10.3390/ijms21144944
Chicago/Turabian StyleLinssen, Pauline B. C., Hans-Peter Brunner-La Rocca, Casper G. Schalkwijk, Joline W. J. Beulens, Petra J. M. Elders, Amber A. van der Heijden, Roderick C. Slieker, Coen D. A. Stehouwer, and Ronald M. A. Henry. 2020. "Serum Matrix Metalloproteinases and Left Atrial Remodeling—The Hoorn Study" International Journal of Molecular Sciences 21, no. 14: 4944. https://doi.org/10.3390/ijms21144944
APA StyleLinssen, P. B. C., Brunner-La Rocca, H.-P., Schalkwijk, C. G., Beulens, J. W. J., Elders, P. J. M., van der Heijden, A. A., Slieker, R. C., Stehouwer, C. D. A., & Henry, R. M. A. (2020). Serum Matrix Metalloproteinases and Left Atrial Remodeling—The Hoorn Study. International Journal of Molecular Sciences, 21(14), 4944. https://doi.org/10.3390/ijms21144944