Clinicopathologic Characteristics of Breast Cancer According to the Infiltrating Immune Cell Subtypes



Abstract
1. Introduction
2. Results
2.1. Basal Characteristics of Breast Cancer Patients
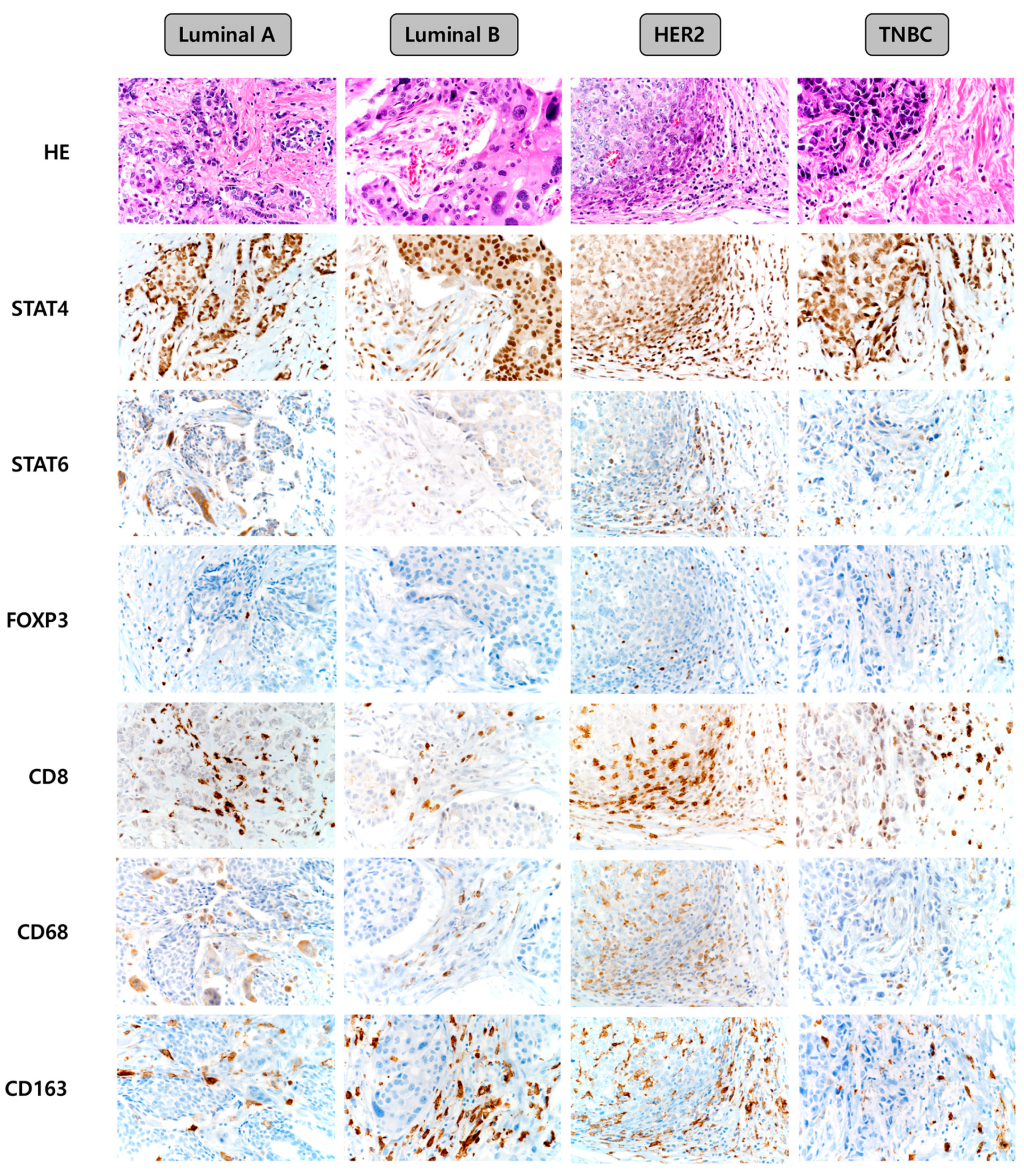
2.2. Expression of Immune Cell Subtype-Related Proteins According to the Breast Cancer Molecular Subtype
2.3. Correlations among the Expression Statuses of Immune Cell Subtype-Related Proteins
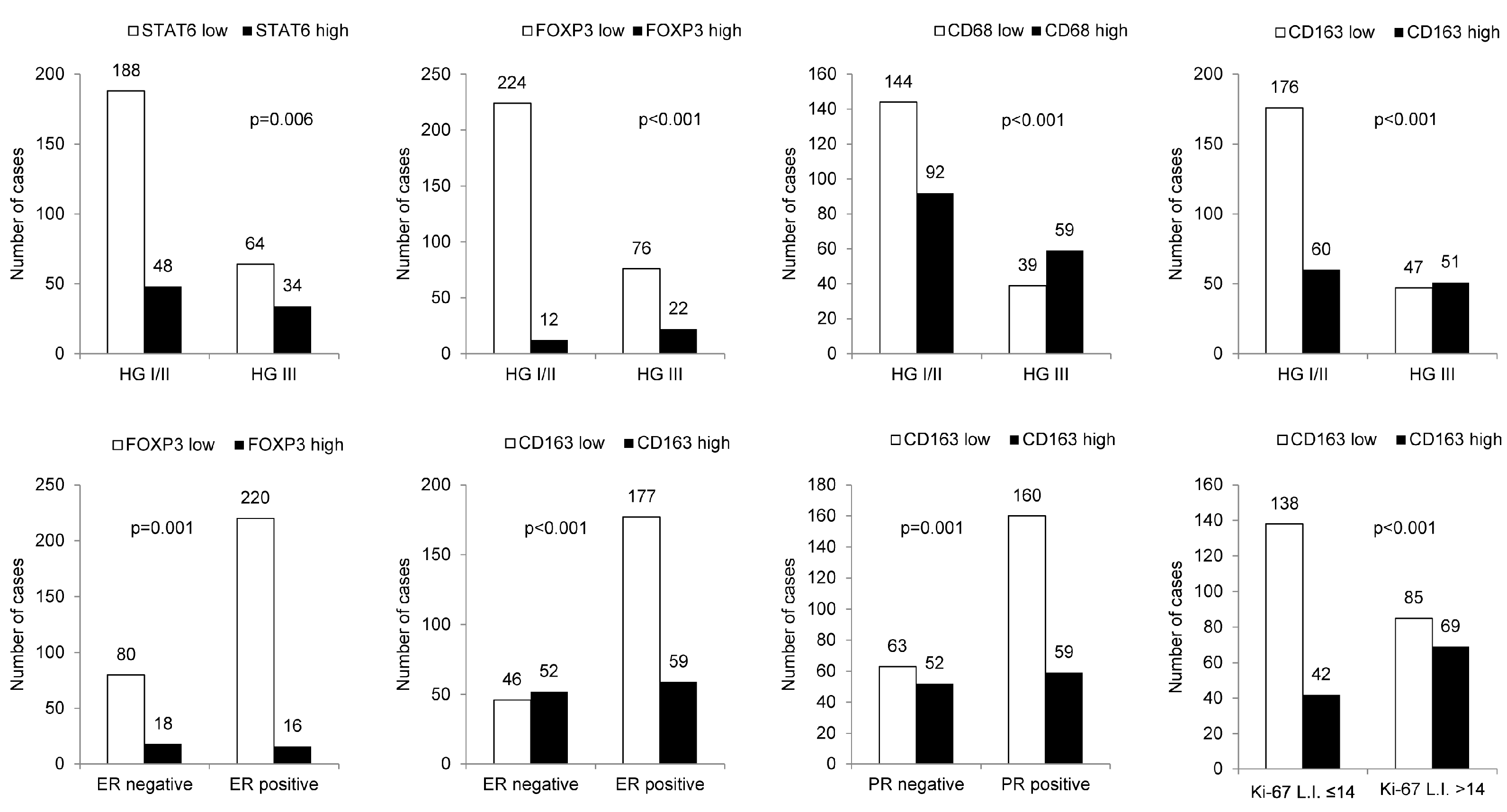
2.4. Correlation between Clinicopathologic Parameters and the Expression Statuses of Immune Cell Subtype-Related Proteins
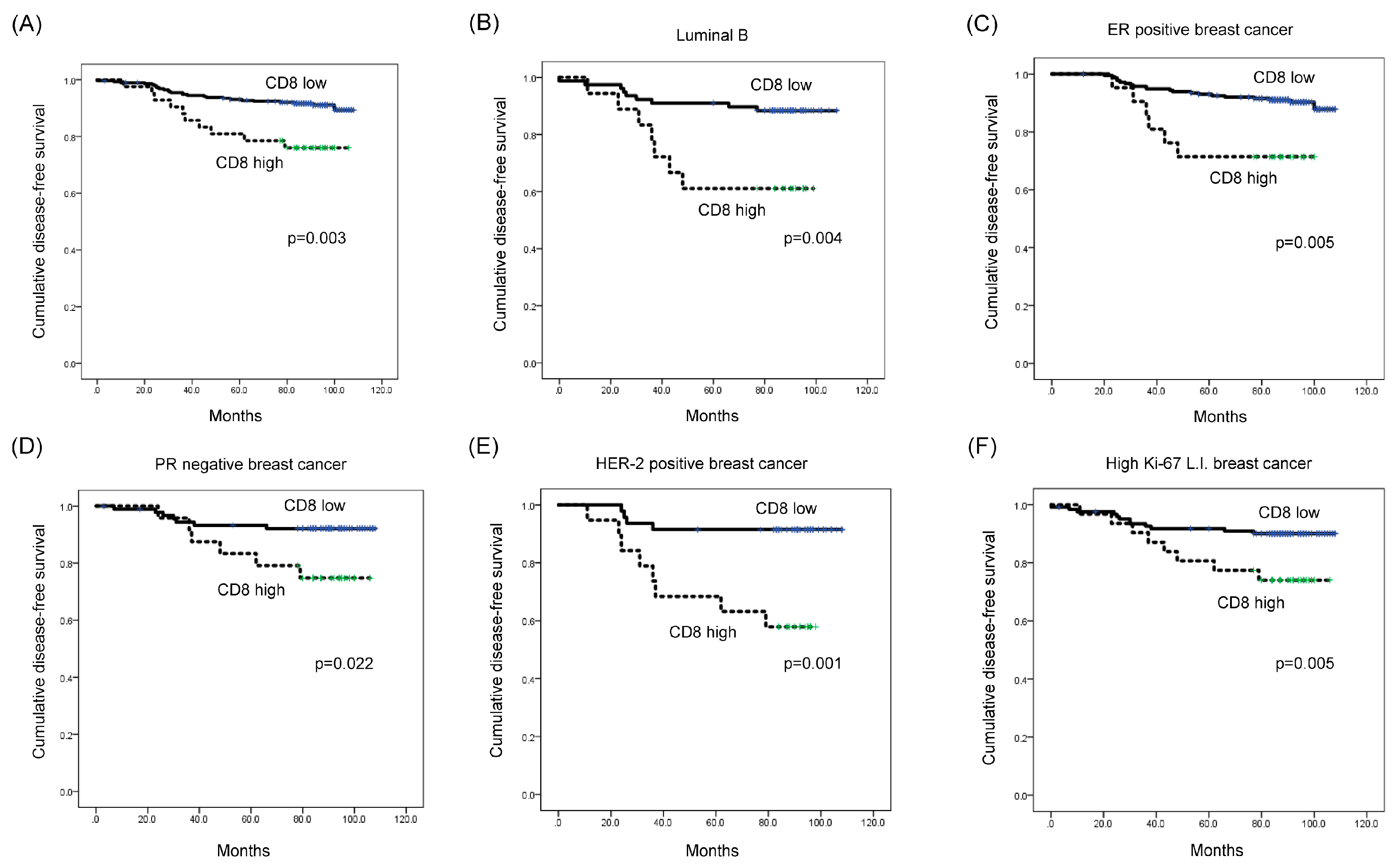
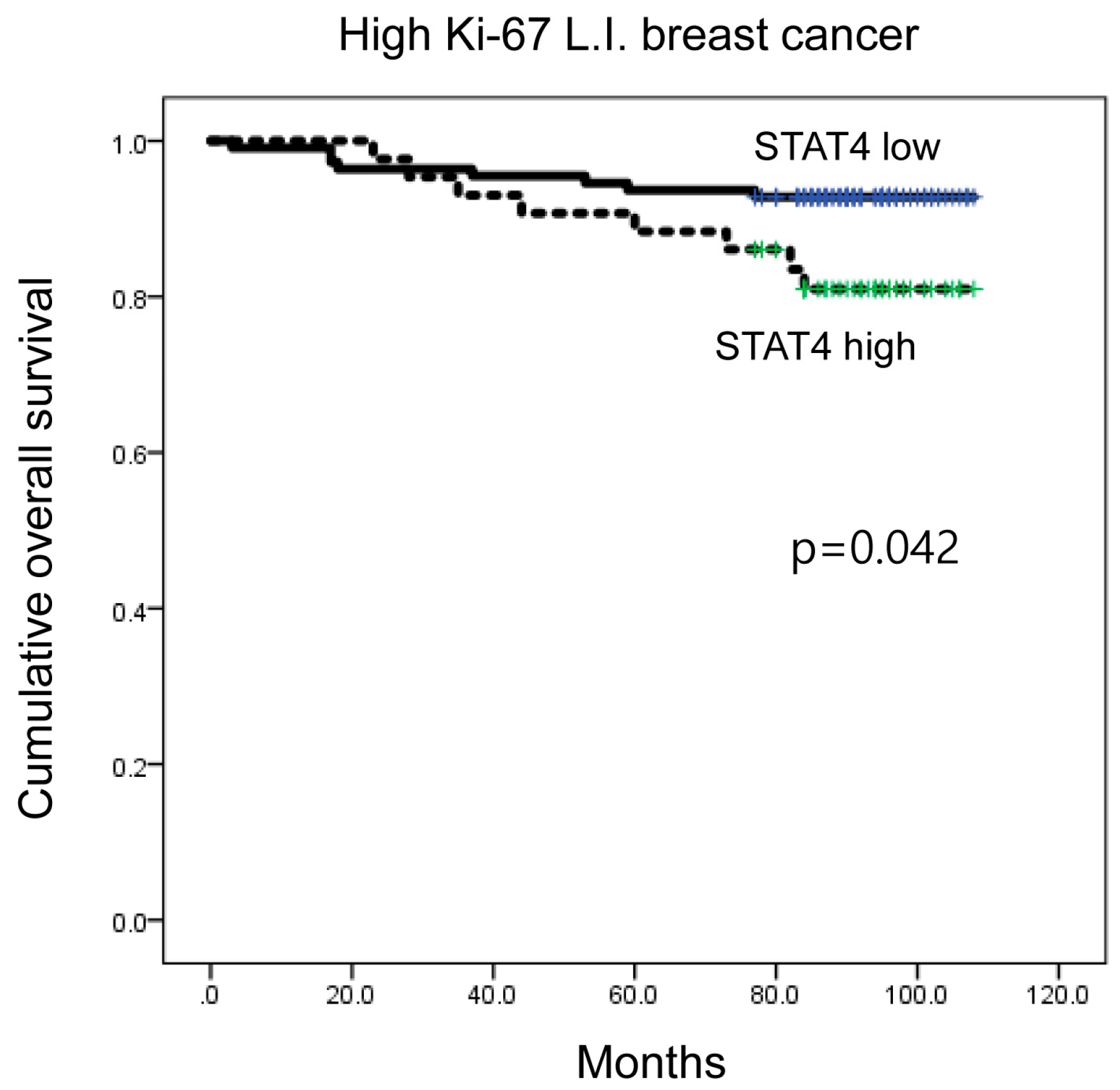
2.5. Impact of Immune Cell Subtype-Related Protein Expression on Patient Prognosis
3. Discussion
4. Materials and Methods
4.1. Patient Selection and Histologic Evaluation
4.2. Tissue Microarray
4.3. Immunohistochemistry
4.4. Immunohistochemistry Interpretation
4.5. Breast Cancer Molecular Classification
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Criscitiello, C.; Esposito, A.; Curigliano, G. Tumor-stroma crosstalk: Targeting stroma in breast cancer. Curr. Opin. Oncol. 2014, 26, 551–555. [Google Scholar] [CrossRef]
- Hanahan, D.; Coussens, L.M. Accessories to the crime: Functions of cells recruited to the tumor microenvironment. Cancer Cell 2012, 21, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Ravelli, A.; Roviello, G.; Cretella, D.; Cavazzoni, A.; Biondi, A.; Cappelletti, M.R.; Zanotti, L.; Ferrero, G.; Ungari, M.; Zanconati, F.; et al. Tumor-infiltrating lymphocytes and breast cancer: Beyond the prognostic and predictive utility. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2017, 39. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.Q.; Waaijer, S.J.H.; Zwager, M.C.; de Vries, E.G.E.; van der Vegt, B.; Schröder, C.P. Tumor-associated macrophages in breast cancer: Innocent bystander or important player? Cancer Treat. Rev. 2018, 70, 178–189. [Google Scholar] [CrossRef]
- Speiser, D.E.; Ho, P.C.; Verdeil, G. Regulatory circuits of T cell function in cancer. Nat. Rev. Immunol. 2016, 16, 599–611. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, Y.; Gu, W.; Sun, B. TH1/TH2 cell differentiation and molecular signals. Adv. Exp. Med. Biol. 2014, 841, 15–44. [Google Scholar] [PubMed]
- Rao, A.; Avni, O. Molecular aspects of T-cell differentiation. Br. Med. Bull. 2000, 56, 969–984. [Google Scholar] [CrossRef]
- Najafi, M.; Farhood, B.; Mortezaee, K. Contribution of regulatory T cells to cancer: A review. J. Cell. Physiol. 2019, 234, 7983–7993. [Google Scholar] [CrossRef]
- Taniuchi, I. CD4 Helper and CD8 Cytotoxic T Cell Differentiation. Annu. Rev. Immunol. 2018, 36, 579–601. [Google Scholar] [CrossRef]
- Troiano, G.; Caponio, V.C.A.; Adipietro, I.; Tepedino, M.; Santoro, R.; Laino, L.; Lo Russo, L.; Cirillo, N.; Lo Muzio, L. Prognostic significance of CD68(+) and CD163(+) tumor associated macrophages in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol. 2019, 93, 66–75. [Google Scholar] [CrossRef]
- Lakhani, S.R.; International Agency for Research on Cancer; World Health Organization. WHO Classification of Tumours of the Breast; International Agency for Research on Cancer: Lyon, France, 2012. [Google Scholar]
- Solinas, C.; Carbognin, L.; De Silva, P.; Criscitiello, C.; Lambertini, M. Tumor-infiltrating lymphocytes in breast cancer according to tumor subtype: Current state of the art. Breast (Edinb. Scotl.) 2017, 35, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Denkert, C.; Campbell, C.; Savas, P.; Nuciforo, P.; Aura, C.; de Azambuja, E.; Eidtmann, H.; Ellis, C.E.; Baselga, J.; et al. Tumor-infiltrating lymphocytes and associations with pathological complete response and event-free survival in HER2-positive early-stage breast cancer treated with lapatinib and trastuzumab: A secondary analysis of the NeoALTTO trial. JAMA Oncol. 2015, 1, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.M.; Al-Foheidi, M.E.; Al-Mansour, M.M.; Kazkaz, G.A. The prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancer: A meta-analysis. Breast Cancer Res. Treat. 2014, 148, 467–476. [Google Scholar] [CrossRef]
- Liu, S.; Lachapelle, J.; Leung, S.; Gao, D.; Foulkes, W.D.; Nielsen, T.O. CD8+ lymphocyte infiltration is an independent favorable prognostic indicator in basal-like breast cancer. Breast Cancer Res. BCR 2012, 14, R48. [Google Scholar] [CrossRef]
- Kim, S.T.; Jeong, H.; Woo, O.H.; Seo, J.H.; Kim, A.; Lee, E.S.; Shin, S.W.; Kim, Y.H.; Kim, J.S.; Park, K.H. Tumor-infiltrating lymphocytes, tumor characteristics, and recurrence in patients with early breast cancer. Am. J. Clin. Oncol. 2013, 36, 224–231. [Google Scholar] [CrossRef]
- Wang, K.; Shen, T.; Siegal, G.P.; Wei, S. The CD4/CD8 ratio of tumor-infiltrating lymphocytes at the tumor-host interface has prognostic value in triple-negative breast cancer. Hum. Pathol. 2017, 69, 110–117. [Google Scholar] [CrossRef]
- Sharma, M.; Beck, A.H.; Webster, J.A.; Espinosa, I.; Montgomery, K.; Varma, S.; van de Rijn, M.; Jensen, K.C.; West, R.B. Analysis of stromal signatures in the tumor microenvironment of ductal carcinoma in situ. Breast Cancer Res. Treat. 2010, 123, 397–404. [Google Scholar] [CrossRef]
- Campbell, M.J.; Baehner, F.; O’Meara, T.; Ojukwu, E.; Han, B.; Mukhtar, R.; Tandon, V.; Endicott, M.; Zhu, Z.; Wong, J.; et al. Characterizing the immune microenvironment in high-risk ductal carcinoma in situ of the breast. Breast Cancer Res. Treat. 2017, 161, 17–28. [Google Scholar] [CrossRef]
- Thompson, E.; Taube, J.M.; Elwood, H.; Sharma, R.; Meeker, A.; Warzecha, H.N.; Argani, P.; Cimino-Mathews, A.; Emens, L.A. The immune microenvironment of breast ductal carcinoma in situ. Mod. Pathol. 2016, 29, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Dieci, M.V.; Griguolo, G.; Miglietta, F.; Guarneri, V. The immune system and hormone-receptor positive breast cancer: Is it really a dead end? Cancer Treat. Rev. 2016, 46, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Sirtaine, N.; Piette, F.; Salgado, R.; Viale, G.; Van Eenoo, F.; Rouas, G.; Francis, P.; Crown, J.P.; Hitre, E.; et al. Prognostic and predictive value of tumor-infiltrating lymphocytes in a phase III randomized adjuvant breast cancer trial in node-positive breast cancer comparing the addition of docetaxel to doxorubicin with doxorubicin-based chemotherapy: BIG 02-98. J. Clin. Oncol. 2013, 31, 860–867. [Google Scholar] [CrossRef]
- Dieci, M.V.; Mathieu, M.C.; Guarneri, V.; Conte, P.; Delaloge, S.; Andre, F.; Goubar, A. Prognostic and predictive value of tumor-infiltrating lymphocytes in two phase III randomized adjuvant breast cancer trials. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Michiels, S.; Salgado, R.; Sirtaine, N.; Jose, V.; Fumagalli, D.; Kellokumpu-Lehtinen, P.L.; Bono, P.; Kataja, V.; Desmedt, C.; et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: Results from the FinHER trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25, 1544–1550. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Ballman, K.V.; Tenner, K.S.; Thompson, E.A.; Badve, S.S.; Bailey, H.; Baehner, F.L. Association of stromal tumor-infiltrating lymphocytes with recurrence-free survival in the N9831 adjuvant trial in patients with early-stage HER2-positive breast cancer. JAMA Oncol. 2016, 2, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Pruneri, G.; Vingiani, A.; Bagnardi, V.; Rotmensz, N.; De Rose, A.; Palazzo, A.; Colleoni, A.M.; Goldhirsch, A.; Viale, G. Clinical validity of tumor-infiltrating lymphocytes analysis in patients with triple-negative breast cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2016, 27, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Stanton, S.E.; Adams, S.; Disis, M.L. Variation in the incidence and magnitude of tumor-infiltrating lymphocytes in breast cancer subtypes: A systematic review. JAMA Oncol. 2016, 2, 1354–1360. [Google Scholar] [CrossRef]
- Glajcar, A.; Szpor, J.; Hodorowicz-Zaniewska, D.; Tyrak, K.E.; Okon, K. The composition of T cell infiltrates varies in primary invasive breast cancer of different molecular subtypes as well as according to tumor size and nodal status. Virchows Arch. 2019, 475, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, E.; Sakellakis, M.; Melachrinou, M.; Tzoracoleftherakis, E.; Kalofonos, H.; Kourea, E. A standardized evaluation method for FOXP3+ Tregs and CD8+ T-cells in breast carcinoma: Association with breast carcinoma subtypes, stage and prognosis. Anticancer Res. 2019, 39, 1217–1232. [Google Scholar] [CrossRef]
- Sotiropoulou, P.A.; Perez, S.A.; Iliopoulou, E.G.; Missitzis, I.; Voelter, V.; Echner, H.; Baxevanis, C.N.; Papamichail, M. Cytotoxic T-cell precursor frequencies to HER-2 (369–377) in patients with HER-2/neu-positive epithelial tumours. Br. J. Cancer 2003, 89, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Sotiropoulou, P.A.; Perez, S.A.; Voelter, V.; Echner, H.; Missitzis, I.; Tsavaris, N.B.; Papamichail, M.; Baxevanis, C.N. Natural CD8+ T-cell responses against MHC class I epitopes of the HER-2/ neu oncoprotein in patients with epithelial tumors. Cancer Immunol. Immunother. 2003, 52, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, S.M.; Lee, A.H.; Paish, E.C.; Macmillan, R.D.; Ellis, I.O.; Green, A.R. Tumour-infiltrating macrophages and clinical outcome in breast cancer. J. Clin. Pathol. 2012, 65, 159–163. [Google Scholar] [CrossRef]
- Gwak, J.M.; Jang, M.H.; Kim, D.I.; Seo, A.N.; Park, S.Y. Prognostic value of tumor-associated macrophages according to histologic locations and hormone receptor status in breast cancer. PLoS ONE 2015, 10, e0125728. [Google Scholar] [CrossRef] [PubMed]
- Medrek, C.; Ponten, F.; Jirstrom, K.; Leandersson, K. The presence of tumor associated macrophages in tumor stroma as a prognostic marker for breast cancer patients. BMC Cancer 2012, 12, 306. [Google Scholar] [CrossRef] [PubMed]
- Lindsten, T.; Hedbrant, A.; Ramberg, A.; Wijkander, J.; Solterbeck, A.; Eriksson, M.; Delbro, D.; Erlandsson, A. Effect of macrophages on breast cancer cell proliferation, and on expression of hormone receptors, uPAR and HER-2. Int. J. Oncol. 2017, 51, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.; Hwang, I.; Kang, S.H.; Shin, H.C.; Kwon, S.Y. Tumor-associated macrophages as potential prognostic biomarkers of invasive breast cancer. J. Breast Cancer 2019, 22, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Linde, N.; Casanova-Acebes, M.; Sosa, M.S.; Mortha, A.; Rahman, A.; Farias, E.; Harper, K.; Tardio, E.; Reyes Torres, I.; Jones, J.; et al. Macrophages orchestrate breast cancer early dissemination and metastasis. Nat. Commun. 2018, 9, 21. [Google Scholar] [CrossRef]
- Van Nguyen, A.; Pollard, J.W. Colony stimulating factor-1 is required to recruit macrophages into the mammary gland to facilitate mammary ductal outgrowth. Dev. Biol. 2002, 247, 11–25. [Google Scholar] [CrossRef]
- Gouon-Evans, V.; Rothenberg, M.E.; Pollard, J.W. Postnatal mammary gland development requires macrophages and eosinophils. Development 2000, 127, 2269–2282. [Google Scholar]
- Gouon-Evans, V.; Lin, E.Y.; Pollard, J.W. Requirement of macrophages and eosinophils and their cytokines/chemokines for mammary gland development. Breast Cancer Res. BCR 2002, 4, 155–164. [Google Scholar] [CrossRef]
- Catacchio, I.; Silvestris, N.; Scarpi, E.; Schirosi, L.; Scattone, A.; Mangia, A. Intratumoral, rather than stromal, CD8+ T cells could be a potential negative prognostic marker in invasive breast cancer patients. Transl. Oncol. 2019, 12, 585–595. [Google Scholar] [CrossRef]
- Fortis, S.P.; Sofopoulos, M.; Sotiriadou, N.N.; Haritos, C.; Vaxevanis, C.K.; Anastasopoulou, E.A.; Janssen, N.; Arnogiannaki, N.; Ardavanis, A.; Pawelec, G.; et al. Differential intratumoral distributions of CD8 and CD163 immune cells as prognostic biomarkers in breast cancer. J. Immunother. Cancer 2017, 5, 39. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Ponde, N.F.; Solinas, C.; de Azambuja, E. Adjuvant trastuzumab: A 10-year overview of its benefit. Expert Rev. Anticancer Ther. 2017, 17, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Wimberly, H.; Brown, J.R.; Schalper, K.; Haack, H.; Silver, M.R.; Nixon, C.; Bossuyt, V.; Pusztai, L.; Lannin, D.R.; Rimm, D.L. PD-L1 Expression correlates with tumor-infiltrating lymphocytes and response to neoadjuvant chemotherapy in breast cancer. Cancer Immunol. Res. 2015, 3, 326–332. [Google Scholar] [CrossRef]
- Schalper, K.A.; Velcheti, V.; Carvajal, D.; Wimberly, H.; Brown, J.; Pusztai, L.; Rimm, D.L. In situ tumor PD-L1 mRNA expression is associated with increased TILs and better outcome in breast carcinomas. Clin. Cancer Res. 2014, 20, 2773–2782. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Philips, A.V.; Meric-Bernstam, F.; Qiao, N.; Wu, Y.; Harrington, S.; Su, X.; Wang, Y.; Gonzalez-Angulo, A.M.; Akcakanat, A.; et al. PD-L1 expression in triple-negative breast cancer. Cancer Immunol. Res. 2014, 2, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cruz, C.; Braiteh, F.S.; Eder, J.P.; Tolaney, S.; Kuter, I.; Nanda, R.; Chung, C.; Cassier, P.; Delord, J.-P.; et al. Abstract 2986: Atezolizumab in metastatic TNBC (mTNBC): Long-term clinical outcomes and biomarker analyses. Cancer Res. 2017, 77 (Suppl. S13), 2986. [Google Scholar]
- Dirix, L.; Takacs, I.; Nikolinakos, P.; Jerusalem, G.; Arkenau, H.-T.; Hamilton, E.; von Heydebreck, A.; Grote, H.-J.; Chin, K.; Lippman, M. Abstract S1-04: Avelumab (MSB0010718C), an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: A phase Ib JAVELIN solid tumor trial. Cancer Res. 2016, 76 (Suppl. S4), S1-04. [Google Scholar]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Ohtani, H.; Mori-Shiraishi, K.; Nakajima, M.; Ueki, H. Defining lymphocyte-predominant breast cancer by the proportion of lymphocyte-rich stroma and its significance in routine histopathological diagnosis. Pathol. Int. 2015, 65, 644–651. [Google Scholar] [CrossRef]
- Salgado, R.; Denkert, C.; Demaria, S.; Sirtaine, N.; Klauschen, F.; Pruneri, G.; Wienert, S.; Van den Eynden, G.; Baehner, F.L.; Penault-Llorca, F.; et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: Recommendations by an International TILs Working Group 2014. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 259–271. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing tumor-infiltrating lymphocytes in solid tumors: A practical review for pathologists and proposal for a standardized method from the international immunooncology biomarkers working group: Part 1: Assessing the host immune response, TILs in invasive breast carcinoma and ductal carcinoma in situ, metastatic tumor deposits and areas for further research. Adv. Anat. Pathol. 2017, 24, 235–251. [Google Scholar] [PubMed]
- Goldhirsch, A.; Wood, W.C.; Coates, A.S.; Gelber, R.D.; Thurlimann, B.; Senn, H.J. Strategies for subtypes--dealing with the diversity of breast cancer: Highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2011, 22, 1736–1747. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 334) (%) | Luminal A (n = 162) (%) | Luminal B (n = 96) (%) | HER-2 (n = 21) (%) | TNBC (n = 55) (%) | p-Value |
|---|---|---|---|---|---|---|
| STAT4 | 0.809 | |||||
| Low | 237 (71.0) | 115 (71.0) | 71 (74.0) | 14 (66.7) | 37 (67.3) | |
| High | 97 (29.0) | 47 (29.0) | 25 (26.0) | 7 (33.3) | 18 (32.7) | |
| STAT6 | 0.047 | |||||
| Low | 252 (75.4) | 131 (80.9) | 65 (67.7) | 13 (61.9) | 43 (78.2) | |
| High | 82 (24.6) | 31 (19.1) | 31 (32.3) | 8 (38.1) | 12 (21.8) | |
| FOXP3 | 0.006 | |||||
| Low | 300 (89.8) | 151 (93.2) | 88 (91.7) | 15 (71.4) | 46 (83.6) | |
| High | 34 (10.2) | 11 (6.8) | 8 (8.3) | 6 (28.6) | 9 (16.4) | |
| CD8 | <0.001 | |||||
| Low | 292 (87.4) | 155 (95.7) | 78 (81.3) | 12 (57.1) | 47 (85.5) | |
| High | 42 (12.6) | 7 (4.3) | 18 (18.8) | 9 (42.9) | 8 (14.5) | |
| CD68 | 0.026 | |||||
| Low | 183 (54.8) | 101 (62.3) | 48 (50.0) | 7 (33.3) | 27 (49.1) | |
| High | 151 (45.2) | 61 (37.7) | 48 (50.0) | 14 (66.7) | 28 (50.9) | |
| CD163 | <0.001 | |||||
| Low | 223 (66.8) | 131 (80.9) | 57 (59.4) | 8 (38.1) | 27 (49.1) | |
| High | 111 (33.2) | 31 (19.1) | 39 (40.6) | 13 (61.9) | 28 (50.9) |
| Parameter | Total (n = 334) (Mean ± SD) | Luminal A (n = 162) (Mean ± SD) | Luminal B (n = 96) (Mean ± SD) | HER-2 (n = 21) (Mean ± SD) | TNBC (n = 55) (Mean ± SD) | p-Value |
|---|---|---|---|---|---|---|
| STAT4 H-score | 87.7 ± 56.6 | 87.8 ± 53.6 | 81.8 ± 55.3 | 102.8 ± 65.0 | 92.0 ± 64.0 | 0.417 |
| STAT6 H-score | 2.6 ± 7.3 | 1.5 ± 3.9 | 3.5 ± 8.1 | 7.1 ± 16.3 | 2.7 ± 7.9 | 0.005 |
| FOXP3 (%) | 0.5 ± 1.5 | 0.3 ± 1.2 | 0.4 ± 1.3 | 1.6 ± 2.8 | 0.8 ± 1.8 | 0.001 |
| CD8 (%) | 6.3 ± 7.9 | 5.2 ± 5.3 | 7.6 ± 9.6 | 10.2 ± 8.1 | 6.1 ± 10.1 | 0.012 |
| CD68 (%) | 1.0 ± 1.9 | 0.7 ± 1.6 | 1.0 ± 1.7 | 1.4 ± 2.4 | 1.7 ± 2.7 | 0.011 |
| CD163 (%) | 14.6 ± 15.6 | 9.7 ± 11.7 | 17.4 ± 17.1 | 22.1 ± 17.4 | 21.4 ± 17.9 | <0.001 |
| Parameter | Total breast cancer | Luminal A | Luminal B | HER-2 | TNBC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
No LPBC n = 292 (%) |
LPBC n = 42 (%) | p-Value |
No LPBC n = 154 (%) |
LPBC n = 8 (%) | p-Value |
No LPBC n = 81 (%) |
LPBC n = 15 (%) | p-Value |
No LPBC n = 13 (%) |
LPBC n = 8 (%) | p-Value |
No LPBC n = 44 (%) |
LPBC n = 11 (%) | p-Value | |
| STAT4 | <0.001 | 0.171 | 0.060 | 0.041 | 0.021 | ||||||||||
| Low | 218 (74.7) | 19 (45.2) | 111 (72.1) | 4 (50.0) | 63 (77.8) | 8 (53.3) | 11 (84.6) | 3 (37.5) | 33 (75.0) | 4 (36.4) | |||||
| High | 74 (25.3) | 23 (54.8) | 43 (27.9) | 4 (50.0) | 18 (22.2) | 7 (46.7) | 2 (15.4) | 5 (62.5) | 11 (25.0) | 7 (63.6) | |||||
| STAT6 | <0.001 | 0.180 | 0.016 | 0.310 | 0.182 | ||||||||||
| Low | 228 (78.1) | 24 (57.1) | 126 (81.8) | 5 (62.5) | 59 (72.8) | 6 (40.0) | 7 (53.8) | 6 (75.0) | 36 (81.8) | 7 (63.6) | |||||
| High | 64 (21.9) | 18 (42.9) | 28 (18.2) | 3 (37.5) | 22 (27.2) | 9 (60.0) | 6 (46.2) | 2 (25.0) | 8 (18.2) | 4 (36.4) | |||||
| FOXP3 | 0.010 | 0.510 | 0.107 | 0.410 | 0.582 | ||||||||||
| Low | 267 (91.4) | 33 (78.6) | 144 (93.5) | 7 (87.5) | 76 (93.8) | 12 (80.0) | 10 (76.9) | 5 (62.5) | 37 (84.1) | 9 (81.8) | |||||
| High | 25 (8.6) | 9 (21.4) | 10 (6.5) | 1 (12.5) | 5 (6.2) | 3 (20.0) | 3 (23.1) | 3 (37.5) | 7 (15.9) | 2 (18.2) | |||||
| CD8 | <0.001 | <0.001 | <0.001 | 0.002 | 0.005 | ||||||||||
| Low | 279 (95.5) | 13 (31.0) | 152 (98.7) | 3 (37.5) | 75 (92.6) | 3 (20.0) | 11 (84.6) | 1 (12.5) | 41 (93.2) | 6 (54.5) | |||||
| High | 13 (4.5) | 29 (69.0) | 2 (1.3) | 5 (62.5) | 6 (7.4) | 12 (80.0) | 2 (15.4) | 7 (87.5) | 3 (6.8) | 5 (45.5) | |||||
| CD68 | <0.001 | 0.003 | 0.002 | 0.112 | 0.023 | ||||||||||
| Low | 177 (60.6) | 6 (14.3) | 100 (64.9) | 1 (12.5) | 46 (56.8) | 2 (13.3) | 6 (46.2) | 1 (12.5) | 25 (56.8) | 2 (18.2) | |||||
| High | 115 (39.4) | 36 (85.7) | 54 (35.1) | 7 (87.5) | 35 (43.2) | 13 (86.7) | 7 (53.8) | 7 (87.5) | 19 (43.2) | 9 (81.8) | |||||
| CD163 | <0.001 | <0.001 | 0.001 | 0.310 | 0.023 | ||||||||||
| Low | 215 (73.6) | 8 (19.0) | 130 (84.4) | 1 (12.5) | 54 (66.7) | 3 (20.0) | 6 (46.2) | 2 (25.0) | 25 (56.8) | 2 (18.2) | |||||
| High | 77 (26.4) | 34 (81.0) | 24 (15.6) | 7 (87.5) | 27 (33.3) | 12 (80.0) | 7 (53.8) | 6 (75.0) | 19 (43.2) | 9 (81.8) | |||||
| Parameters | STAT4 H-Score | STAT6 H-Score | FOXP3 | CD8 | CD68 | CD163 |
|---|---|---|---|---|---|---|
| ER | ||||||
| r-coefficient | −0.086 | −0.148 | −0.197 | −0.046 | −0.131 | −0.298 |
| p-value | 0.117 | 0.007 | <0.001 | 0.399 | 0.017 | <0.001 |
| PR | ||||||
| r-coefficient | −0.051 | −0.083 | −0.156 | −0.105 | −0.149 | −0.204 |
| p-value | 0.357 | 0.131 | 0.004 | 0.055 | 0.006 | <0.001 |
| Stromal TIL | ||||||
| r-coefficient | 0.313 | 0.316 | 0.175 | 0.665 | 0.465 | 0.525 |
| p-value | <0.001 | <0.001 | 0.001 | <0.001 | <0.001 | <0.001 |
| Parameter | Number of Patients /Recurrence/Death | Disease-Free Survival | Overall Survival | ||
|---|---|---|---|---|---|
| Mean Survival (95% CI) Months | p-Value | Mean Survival (95% CI) Months | p-Value | ||
| STAT4 | 0.346 | 0.074 | |||
| Low | 237/23/17 | 101 (98–104) | 103 (101–105) | ||
| High | 97/13/13 | 98 (93–103) | 100 (97–104) | ||
| STAT6 | 0.995 | 0.054 | |||
| Low | 252/27/27 | 100 (97–103) | 102 (99–104) | ||
| High | 82/9/3 | 100 (95–105) | 105 (102–108) | ||
| FOXP3 | 0.672 | 0.957 | |||
| Low | 300/33/27 | 100 (97–102) | 102 (100–104) | ||
| High | 34/3/3 | 101 (94–108) | 103 (99–108) | ||
| CD8 | 0.003 | 0.475 | |||
| Low | 292/26/25 | 101 (99–104) | 103 (101–105) | ||
| High | 42/10/5 | 90 (81–99) | 99 (94–105) | ||
| CD68 | 0.136 | 0.629 | |||
| Low | 183/15/15 | 100 (97–103) | 101 (99–104) | ||
| High | 151/21/15 | 99 (95–102) | 103 (100–105) | ||
| CD163 | 0.714 | 0.681 | |||
| Low | 223/23/19 | 100 (97–103) | 103 (101–105) | ||
| High | 111/13/11 | 100 (95–104) | 102 (99–105) | ||
| Parameters | Disease-Free Survival | Overall Survival | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age | 0.627 | 0.021 | ||||
| ≤50 versus >50 | 1.185 | 0.597–2.353 | 2.418 | 1.145–5.108 | ||
| Histologic grade | 0.220 | 0.201 | ||||
| I/II versus III | 1.674 | 0.735–3.814 | 1.784 | 0.734–4.338 | ||
| T stage | 0.765 | 0.816 | ||||
| T1 versus T2/3 | 0.900 | 0.451–1.797 | 0.915 | 0.436–1.923 | ||
| Lymph node metastasis | 0.022 | 0.163 | ||||
| No versus Yes | 2.247 | 1.125–4.488 | 1.708 | 0.805–3.626 | ||
| ER status | 0.162 | 0.453 | ||||
| Negative versus Positive | 0.481 | 0.173–1.342 | 1.490 | 0.526–4.218 | ||
| PR status | 0.893 | 0.840 | ||||
| Negative versus Positive | 0.943 | 0.404–2.203 | 1.096 | 0.452–2.656 | ||
| HER-2 status | 0.216 | 0.450 | ||||
| Negative versus Positive | 1.628 | 0.752–3.525 | 1.400 | 0.585–3.348 | ||
| Ki-67 L.I. | 0.539 | 0.489 | ||||
| ≤14 versus >14 | 1.258 | 0.542–2.917 | 0.705 | 0.262–1.897 | ||
| CD8 | 0.026 | 0.975 | ||||
| Low versus High | 2.435 | 1.110–5.344 | 0.984 | 0.355–2.728 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.M.; Koo, J.S. Clinicopathologic Characteristics of Breast Cancer According to the Infiltrating Immune Cell Subtypes. Int. J. Mol. Sci. 2020, 21, 4438. https://doi.org/10.3390/ijms21124438
Kim HM, Koo JS. Clinicopathologic Characteristics of Breast Cancer According to the Infiltrating Immune Cell Subtypes. International Journal of Molecular Sciences. 2020; 21(12):4438. https://doi.org/10.3390/ijms21124438
Chicago/Turabian StyleKim, Hye Min, and Ja Seung Koo. 2020. "Clinicopathologic Characteristics of Breast Cancer According to the Infiltrating Immune Cell Subtypes" International Journal of Molecular Sciences 21, no. 12: 4438. https://doi.org/10.3390/ijms21124438
APA StyleKim, H. M., & Koo, J. S. (2020). Clinicopathologic Characteristics of Breast Cancer According to the Infiltrating Immune Cell Subtypes. International Journal of Molecular Sciences, 21(12), 4438. https://doi.org/10.3390/ijms21124438