Lixivaptan, a New Generation Diuretic, Counteracts Vasopressin-Induced Aquaporin-2 Trafficking and Function in Renal Collecting Duct Cells


 ,
, 

{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
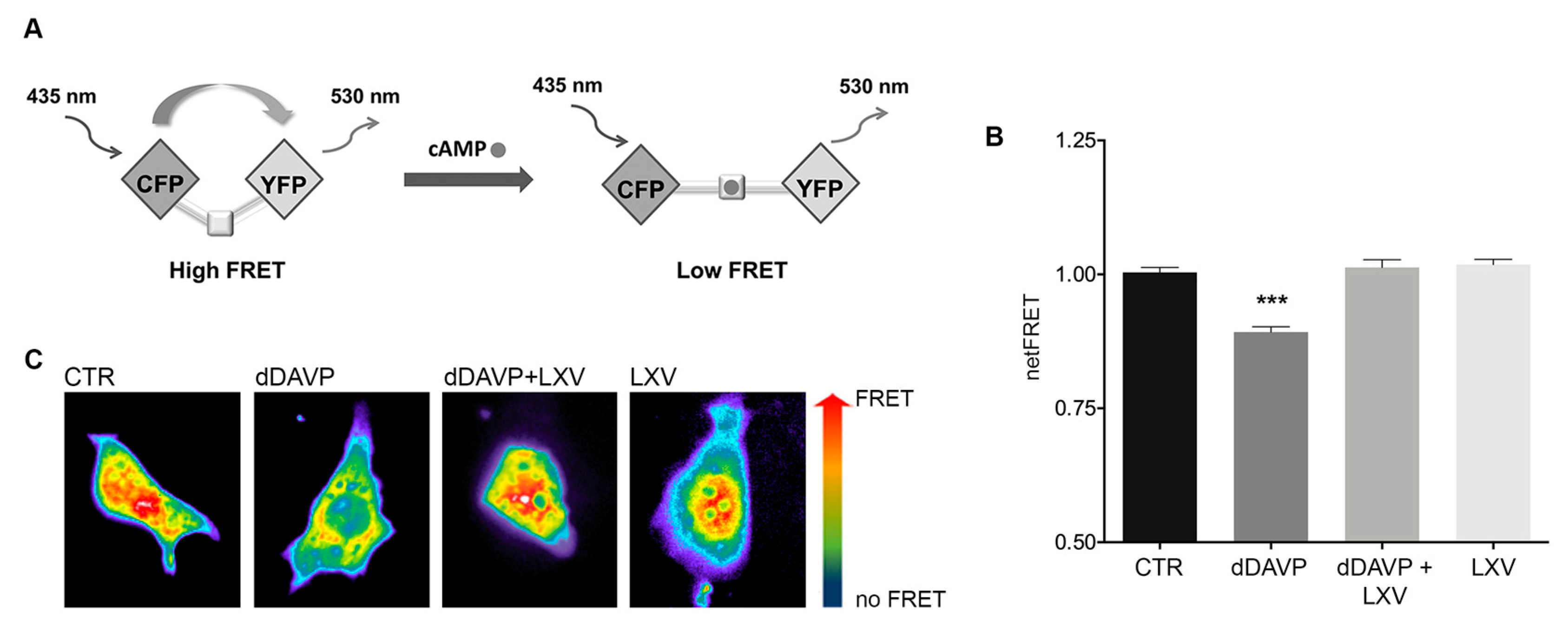
2.1. Effect of Lixivaptan on cAMP Levels in MCD4 Cells
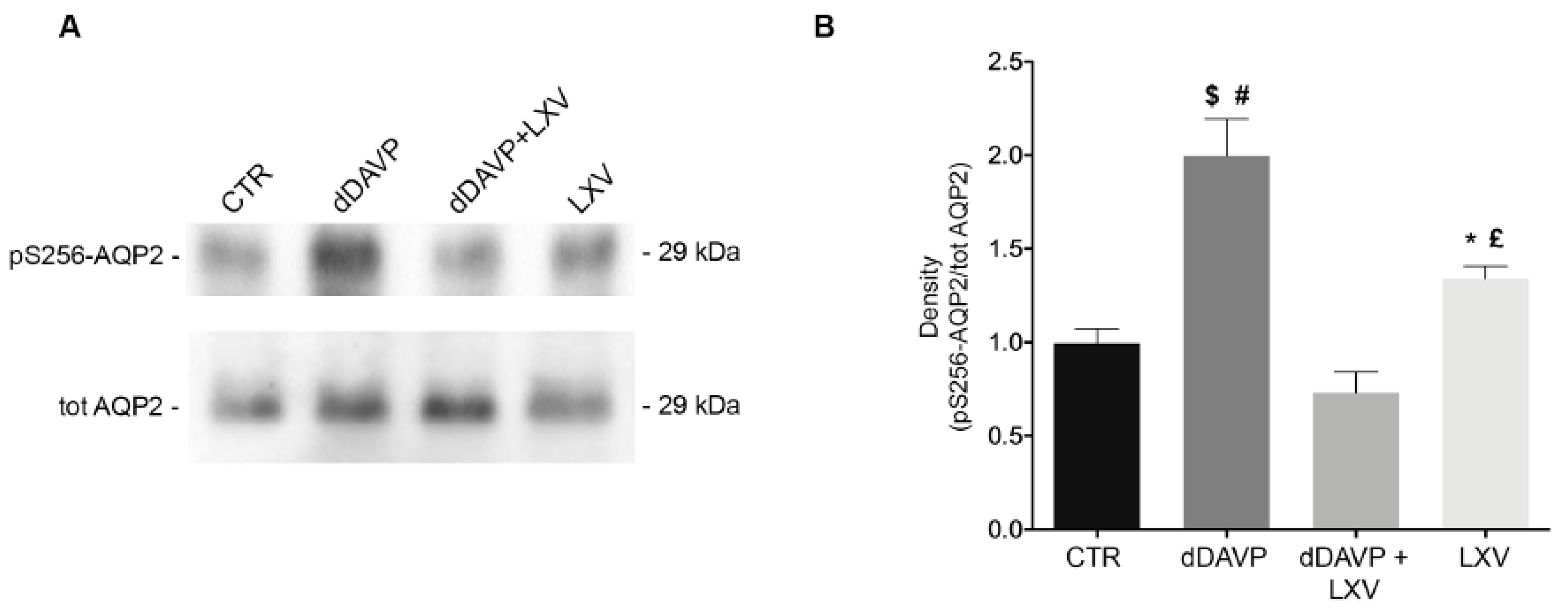
2.2. Lixivaptan Prevents the Increase in pS256-AQP2 and AQP2 Translocation to the Plasma Membrane in Response to dDAVP
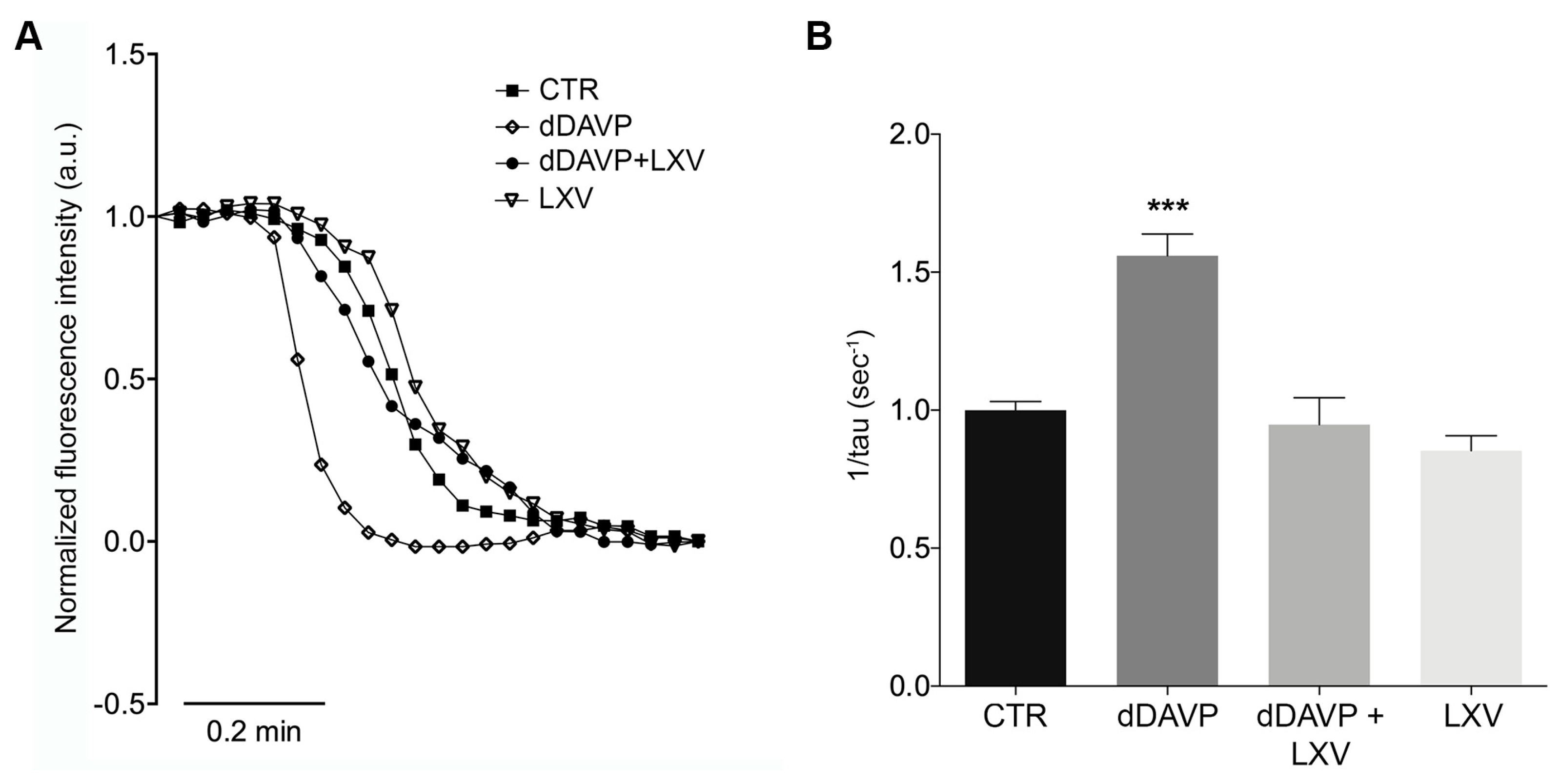
2.3. Lixivaptan Abolishes the Increase in Osmotic Water Permeability in Response to dDAVP
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Antibodies
4.3. Cell Culture and Treatments
4.4. Cell Preparations
4.5. Fluorescence Resonance Energy Transfer Measurements
4.6. Gel Electrophoresis and Immunoblotting
4.7. Water Permeability Assay
4.8. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Fenton, R.A.; Pedersen, C.N.; Moeller, H.B. New insights into regulated aquaporin-2 function. Curr. Opin. Nephrol. Hypertens. 2013, 22, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.J.; Kwon, T.H. Molecular mechanisms regulating aquaporin-2 in kidney collecting duct. Am. J. Physiol. Ren. Physiol. 2016, 311, F1318–F1328. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, M.; Di Mise, A.; Tamma, G.; Valenti, G. Vasopressin-aquaporin-2 pathway: Recent advances in understanding water balance disorders. F1000Research 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Fushimi, K.; Sasaki, S.; Marumo, F. Phosphorylation of serine 256 is required for cAMP-dependent regulatory exocytosis of the aquaporin-2 water channel. J. Biol. Chem. 1997, 272, 14800–14804. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.; DiGiovanni, S.R.; Christensen, E.I.; Knepper, M.A.; Harris, H.W. Cellular and subcellular immunolocalization of vasopressin-regulated water channel in rat kidney. Proc. Natl. Acad. Sci. USA 1993, 90, 11663–11667. [Google Scholar] [CrossRef]
- Greenberg, A.; Verbalis, J.G. Vasopressin receptor antagonists. Kidney Int. 2006, 69, 2124–2130. [Google Scholar] [CrossRef]
- Costello-Boerrigter, L.C.; Boerrigter, G.; Burnett, J.C. Pharmacology of vasopressin antagonists. Heart Fail. Rev. 2009, 14, 75–82. [Google Scholar] [CrossRef]
- Decaux, G.; Soupart, A.; Vassart, G. Non-peptide arginine-vasopressin antagonists: The vaptans. Lancet 2008, 371, 1624–1632. [Google Scholar] [CrossRef]
- Elhassan, E.A.; Schrier, R.W. The use of vasopressin receptor antagonists in hyponatremia. Expert Opin Investig. Drugs 2011, 20, 373–380. [Google Scholar] [CrossRef]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Grantham, J.J.; Higashihara, E.; Perrone, R.D.; Krasa, H.B.; Ouyang, J.; Czerwiec, F.S.; et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N. Engl. J. Med. 2012, 367, 2407–2418. [Google Scholar] [CrossRef]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Perrone, R.D.; Koch, G.; Ouyang, J.; McQuade, R.D.; Blais, J.D.; Czerwiec, F.S.; et al. Tolvaptan in later-stage autosomal dominant polycystic kidney disease. N. Engl. J. Med. 2017, 377, 1930–1942. [Google Scholar] [CrossRef] [PubMed]
- Shusterman, N.H.H.; Hogan, L.C.; Pellegrini, L. Effect of Lixivaptan on Pharmacokinetic (PK) and Pharmacodynamic (PD) End Points in Patients with Autosomal Dominant Polycystic Kidney Disease (ADPKD) in the ELiSA Study (PA-102); Kidney Week—American Society of Nephrology: Washington, DC, USA, 2019. [Google Scholar]
- Abraham, W.T.; Hensen, J.; Gross, P.A.; Bichet, D.G.; Josiassen, R.C.; Chafekar, D.S.; Orlandi, C.; LIBRA Study Group. Lixivaptan safely and effectively corrects serum sodium concentrations in hospitalized patients with euvolemic hyponatremia. Kidney Int. 2012, 82, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Constans, M.M.; Chebib, F.T.; Torres, V.E.; Pellegrini, L. Effect of a vasopressin V2 receptor antagonist on polycystic kidney disease development in a rat model. Am. J. Nephrol. 2019, 49, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Tamma, G.; Ranieri, M.; Dossena, S.; Di Mise, A.; Nofziger, C.; Svelto, M.; Paulmichl, M.; Valenti, G. A FRET-based approach for quantitative evaluation of forskolin-induced pendrin trafficking at the plasma membrane in bronchial NCI H292 cells. Cell Physiol. Biochem. 2013, 32, 200–209. [Google Scholar] [CrossRef]
- Ranieri, M.; Tamma, G.; Pellegrino, T.; Vezzi, V.; Ambrosio, C.; Gro, C.; Di Mise, A.; Costa, T.; Valenti, G.; Cotecchia, S. Gain-of-function mutations of the V2 vasopressin receptor in nephrogenic syndrome of inappropriate antidiuresis (NSIAD): A cell-based assay to assess constitutive water reabsorption. Pflug. Arch. 2019, 471, 1291–1304. [Google Scholar] [CrossRef]
- Abraham, W.T.; Decaux, G.; Josiassen, R.C.; Yagil, Y.; Kopyt, N.; Thacker, H.P.; Mannelli, M.; Bichet, D.G.; Orlandi, C.; Group, H.S. Oral lixivaptan effectively increases serum sodium concentrations in outpatients with euvolemic hyponatremia. Kidney Int. 2012, 82, 1215–1222. [Google Scholar] [CrossRef]
- Woodhead, J.L.; Brock, W.J.; Roth, S.E.; Shoaf, S.E.; Brouwer, K.L.; Church, R.; Grammatopoulos, T.N.; Stiles, L.; Siler, S.Q.; Howell, B.A.; et al. Application of a mechanistic model to evaluate putative mechanisms of tolvaptan drug-Induced liver injury and identify patient susceptibility factors. Toxicol. Sci. 2017, 155, 61–74. [Google Scholar] [CrossRef]
- Woodhead, J.L.E.A. Comparison of the Hepatotoxic Potential of Two Treatments for Autosomal-Dominant Polycystic Kidney Disease Using Quantitative Systems Toxicology Modeling. Pharm. Res. Press 2019, in press. [Google Scholar]
- Yan, L.; Xie, F.; Lu, J.; Ni, Q.; Shi, C.; Tang, C.; Yang, J. The treatment of vasopressin V2-receptor antagonists in cirrhosis patients with ascites: A meta-analysis of randomized controlled trials. BMC Gastroenterol. 2015, 15, 65. [Google Scholar] [CrossRef]
- Tamma, G.; Di Mise, A.; Ranieri, M.; Geller, A.; Tamma, R.; Zallone, A.; Valenti, G. The V2 receptor antagonist tolvaptan raises cytosolic calcium and prevents AQP2 trafficking and function: An in vitro and in vivo assessment. J. Cell Mol. Med. 2017, 21, 1767–1780. [Google Scholar] [CrossRef]
- Procino, G.; Mastrofrancesco, L.; Mira, A.; Tamma, G.; Carmosino, M.; Emma, F.; Svelto, M.; Valenti, G. Aquaporin 2 and apical calcium-sensing receptor: New players in polyuric disorders associated with hypercalciuria. Semin. Nephrol. 2008, 28, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Rodighiero, S.; Bazzini, C.; Ritter, M.; Furst, J.; Botta, G.; Meyer, G.; Paulmichl, M. Fixation, mounting and sealing with nail polish of cell specimens lead to incorrect FRET measurements using acceptor photobleaching. Cell Physiol. Biochem. 2008, 21, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Ranieri, M.; Di Mise, A.; Dossena, S.; Pellegrino, T.; Furia, E.; Nofziger, C.; Debellis, L.; Paulmichl, M.; Valenti, G.; et al. Interleukin-13 increases pendrin abundance to the cell surface in bronchial NCI-H292 cells via Rho/actin signaling. Pflug. Arch. 2017, 469, 1163–1176. [Google Scholar] [CrossRef] [PubMed]
- van Rheenen, J.; Langeslag, M.; Jalink, K. Correcting confocal acquisition to optimize imaging of fluorescence resonance energy transfer by sensitized emission. Biophys. J. 2004, 86, 2517–2529. [Google Scholar] [CrossRef]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Mise, A.; Venneri, M.; Ranieri, M.; Centrone, M.; Pellegrini, L.; Tamma, G.; Valenti, G. Lixivaptan, a New Generation Diuretic, Counteracts Vasopressin-Induced Aquaporin-2 Trafficking and Function in Renal Collecting Duct Cells. Int. J. Mol. Sci. 2020, 21, 183. https://doi.org/10.3390/ijms21010183
Di Mise A, Venneri M, Ranieri M, Centrone M, Pellegrini L, Tamma G, Valenti G. Lixivaptan, a New Generation Diuretic, Counteracts Vasopressin-Induced Aquaporin-2 Trafficking and Function in Renal Collecting Duct Cells. International Journal of Molecular Sciences. 2020; 21(1):183. https://doi.org/10.3390/ijms21010183
Chicago/Turabian StyleDi Mise, Annarita, Maria Venneri, Marianna Ranieri, Mariangela Centrone, Lorenzo Pellegrini, Grazia Tamma, and Giovanna Valenti. 2020. "Lixivaptan, a New Generation Diuretic, Counteracts Vasopressin-Induced Aquaporin-2 Trafficking and Function in Renal Collecting Duct Cells" International Journal of Molecular Sciences 21, no. 1: 183. https://doi.org/10.3390/ijms21010183
APA StyleDi Mise, A., Venneri, M., Ranieri, M., Centrone, M., Pellegrini, L., Tamma, G., & Valenti, G. (2020). Lixivaptan, a New Generation Diuretic, Counteracts Vasopressin-Induced Aquaporin-2 Trafficking and Function in Renal Collecting Duct Cells. International Journal of Molecular Sciences, 21(1), 183. https://doi.org/10.3390/ijms21010183