Neurofilament Heavy Chain and Tau Protein Are Not Elevated in Cerebrospinal Fluid of Adult Patients with Spinal Muscular Atrophy during Loading with Nusinersen


Abstract
1. Introduction
2. Results
2.1. Clinical Characterization
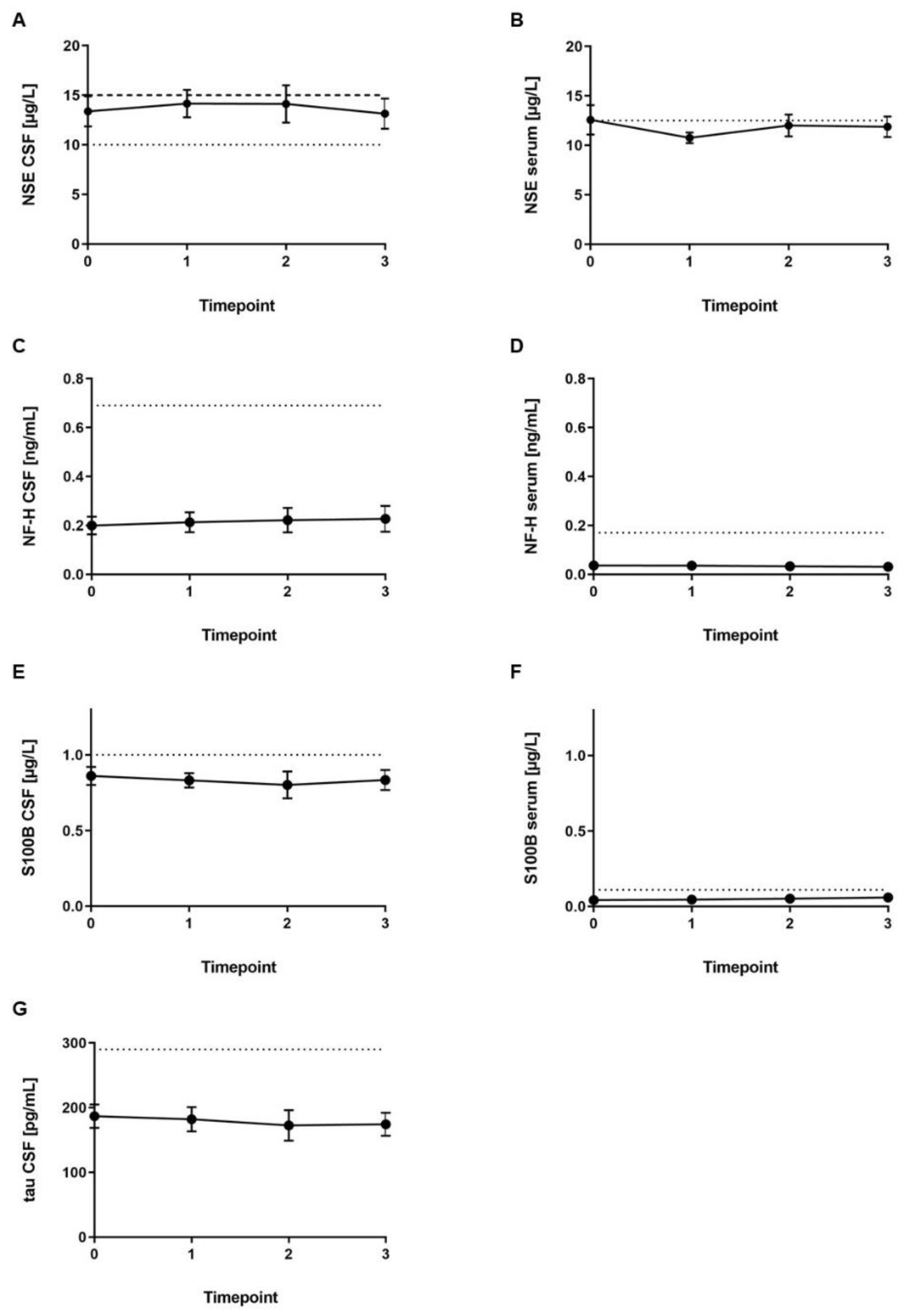
2.2. Laboratory Results
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Laboratory Analysis
4.3. Statistics
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ALS | amyotrophic lateral sclerosis |
| CSF | cerebrospinal fluid |
| HFMSE | Hammersmith Functional Motor Scale Expanded |
| NF | neurofilament |
| RBC | red blood cell count |
| SEM | standard error of mean |
| SMA | spinal muscular atrophy |
| SMN | survival motor neuron |
| WBC | white blood cell count |
References
- Clermont, O.; Burlet, P.; Lefebvre, S.; Burglen, L.; Munnich, A.; Melki, J. SMN gene deletions in adult-onset spinal muscular atrophy. Lancet 1995, 346, 1712–1713. [Google Scholar] [CrossRef]
- Lefebvre, S.; Burglen, L.; Reboullet, S.; Clermont, O.; Burlet, P.; Viollet, L.; Benichou, B.; Cruaud, C.; Millasseau, P.; Zeviani, M.; et al. Identification and characterization of a spinal muscular atrophy-determining gene. Cell 1995, 80, 155–165. [Google Scholar] [CrossRef]
- Talbot, K.; Davies, K.E. Spinal muscular atrophy. Semin. Neurol. 2001, 21, 189–197. [Google Scholar] [CrossRef]
- Burghes, A.H.; Beattie, C.E. Spinal muscular atrophy: Why do low levels of survival motor neuron protein make motor neurons sick? Nature reviews. Neuroscience 2009, 10, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, J.A.; Singh, P.; Darras, B.T. Spinal muscular atrophy: A clinical and research update. Pediatric Neurol. 2012, 46, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Munsat, T.L.; Davies, K.E. International SMA consortium meeting. (26–28 June 1992, Bonn, Germany). Neuromuscul. Disord. 1992, 2, 423–428. [Google Scholar] [CrossRef]
- Rudnik-Schoneborn, S.; Hausmanowa-Petrusewicz, I.; Borkowska, J.; Zerres, K. The predictive value of achieved motor milestones assessed in 441 patients with infantile spinal muscular atrophy types II and III. Eur. Neurol. 2001, 45, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Finkel, R.S.; Mercuri, E.; Darras, B.T.; Connolly, A.M.; Kuntz, N.L.; Kirschner, J.; Chiriboga, C.A.; Saito, K.; Servais, L.; Tizzano, E.; et al. Nusinersen versus Sham Control in Infantile-Onset Spinal Muscular Atrophy. N. Engl. J. Med. 2017, 377, 1723–1732. [Google Scholar] [CrossRef]
- Mercuri, E.; Darras, B.T.; Chiriboga, C.A.; Day, J.W.; Campbell, C.; Connolly, A.M.; Iannaccone, S.T.; Kirschner, J.; Kuntz, N.L.; Saito, K.; et al. Nusinersen versus Sham Control in Later-Onset Spinal Muscular Atrophy. N. Engl. J. Med. 2018, 378, 625–635. [Google Scholar] [CrossRef]
- Darras, B.T.; Crawford, T.O.; Finkel, R.S.; Mercuri, E.; De Vivo, D.C.; Oskoui, M.; Tizzano, E.F.; Ryan, M.M.; Muntoni, F.; Zhao, G.; et al. Neurofilament as a potential biomarker for spinal muscular atrophy. Ann. Clin. Transl. Neurol. 2019, 6, 932–944. [Google Scholar] [CrossRef]
- Olsson, B.; Alberg, L.; Cullen, N.C.; Michael, E.; Wahlgren, L.; Kroksmark, A.K.; Rostasy, K.; Blennow, K.; Zetterberg, H.; Tulinius, M. NFL is a marker of treatment response in children with SMA treated with nusinersen. J. Neurol. 2019, 266, 2129–2136. [Google Scholar] [CrossRef] [PubMed]
- Boylan, K.B.; Glass, J.D.; Crook, J.E.; Yang, C.; Thomas, C.S.; Desaro, P.; Johnston, A.; Overstreet, K.; Kelly, C.; Polak, M.; et al. Phosphorylated neurofilament heavy subunit (pNF-H) in peripheral blood and CSF as a potential prognostic biomarker in amyotrophic lateral sclerosis. J. Neurol. Neurosurg Psychiatry 2013, 84, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Brettschneider, J.; Petzold, A.; Sussmuth, S.D.; Ludolph, A.C.; Tumani, H. Axonal damage markers in cerebrospinal fluid are increased in ALS. Neurology 2006, 66, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Ganesalingam, J.; An, J.; Bowser, R.; Andersen, P.M.; Shaw, C.E. pNfH is a promising biomarker for ALS. Amyotroph. Lateral Scler. Front. Degener. 2013, 14, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Mendonca, D.M.; Martins, S.C.; Higashi, R.; Muscara, M.N.; Neto, V.M.; Chimelli, L.; Martinez, A.M. Neurofilament heavy subunit in cerebrospinal fluid: A biomarker of amyotrophic lateral sclerosis? Amyotroph. Lateral Scler. 2011, 12, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Reijn, T.S.; Abdo, W.F.; Schelhaas, H.J.; Verbeek, M.M. CSF neurofilament protein analysis in the differential diagnosis of ALS. J. Neurol. 2009, 256, 615–619. [Google Scholar] [CrossRef]
- Sobue, G.; Hashizume, Y.; Yasuda, T.; Mukai, E.; Kumagai, T.; Mitsuma, T.; Trojanowski, J.Q. Phosphorylated high molecular weight neurofilament protein in lower motor neurons in amyotrophic lateral sclerosis and other neurodegenerative diseases involving ventral horn cells. Acta Neuropathol. 1990, 79, 402–408. [Google Scholar] [CrossRef]
- Michetti, F.; D’Ambrosi, N.; Toesca, A.; Puglisi, M.A.; Serrano, A.; Marchese, E.; Corvino, V.; Geloso, M.C. The S100B story: From biomarker to active factor in neural injury. J. Neurochem. 2018, 148, 168–187. [Google Scholar] [CrossRef]
- Olsson, B.; Lautner, R.; Andreasson, U.; Ohrfelt, A.; Portelius, E.; Bjerke, M.; Holtta, M.; Rosen, C.; Olsson, C.; Strobel, G.; et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: A systematic review and meta-analysis. Lancet Neurol. 2016, 15, 673–684. [Google Scholar] [CrossRef]
- Park, D.W.; Park, S.H.; Hwang, S.K. Serial measurement of S100B and NSE in pediatric traumatic brain injury. Childs Nerv. Syst. 2018, 35, 343–348. [Google Scholar] [CrossRef]
- Scarafino, A.; D’Errico, E.; Introna, A.; Fraddosio, A.; Distaso, E.; Tempesta, I.; Morea, A.; Mastronardi, A.; Leante, R.; Ruggieri, M.; et al. Diagnostic and prognostic power of CSF Tau in amyotrophic lateral sclerosis. J. Neurol. 2018, 265, 2353–2362. [Google Scholar] [CrossRef] [PubMed]
- Spreca, A.; Rambotti, M.G.; Rende, M.; Saccardi, C.; Aisa, M.C.; Giambanco, I.; Donato, R. Immunocytochemical localization of S-100b protein in degenerating and regenerating rat sciatic nerves. J. Histochem. Cytochem. 1989, 37, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Bowman, G.L.; Dayon, L.; Kirkland, R.; Wojcik, J.; Peyratout, G.; Severin, I.C.; Henry, H.; Oikonomidi, A.; Migliavacca, E.; Bacher, M.; et al. Blood-brain barrier breakdown, neuroinflammation, and cognitive decline in older adults. Alzheimers Dement. 2018, 14, 1640–1650. [Google Scholar] [CrossRef] [PubMed]
- Lamoureux, G.; Jolicoeur, R.; Giard, N.; St-Hilaire, M.; Duplantis, F. Cerebrospinal fluid proteins in multiple sclerosis. Neurology 1975, 25, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, M.; Mokuno, K.; Sugimura, K.; Kiyosawa, K.; Aoki, S.; Takahashi, A.; Kato, K. Cerebrospinal fluid levels of S-100b protein and neuron-specific enolase in chronic inflammatory demyelinating polyneuropathy. Acta Neurol. Scand. 1995, 91, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.H.; Macdonald-Wallis, C.; Gray, E.; Pearce, N.; Petzold, A.; Norgren, N.; Giovannoni, G.; Fratta, P.; Sidle, K.; Fish, M.; et al. Neurofilament light chain: A prognostic biomarker in amyotrophic lateral sclerosis. Neurology 2015, 84, 2247–2257. [Google Scholar] [CrossRef] [PubMed]
- Menke, R.A.; Gray, E.; Lu, C.H.; Kuhle, J.; Talbot, K.; Malaspina, A.; Turner, M.R. CSF neurofilament light chain reflects corticospinal tract degeneration in ALS. Ann. Clin. Transl. Neurol. 2015, 2, 748–755. [Google Scholar] [CrossRef]
- Wurster, C.D.; Gunther, R.; Steinacker, P.; Dreyhaupt, J.; Wollinsky, K.; Uzelac, Z.; Witzel, S.; Kocak, T.; Winter, B.; Koch, J.C.; et al. Neurochemical markers in CSF of adolescent and adult SMA patients undergoing nusinersen treatment. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419846058. [Google Scholar] [CrossRef]
- Wurster, C.D.; Steinacker, P.; Gunther, R.; Koch, J.C.; Lingor, P.; Uzelac, Z.; Witzel, S.; Wollinsky, K.; Winter, B.; Osmanovic, A.; et al. Neurofilament light chain in serum of adolescent and adult SMA patients under treatment with nusinersen. J. Neurol. 2019, 1–9. [Google Scholar] [CrossRef]
- Andreasen, N.; Sjogren, M.; Blennow, K. CSF markers for Alzheimer’s disease: Total tau, phospho-tau and Abeta42. World J. Biol. Psychiatry 2003, 4, 147–155. [Google Scholar] [CrossRef]
- Hesse, C.; Rosengren, L.; Andreasen, N.; Davidsson, P.; Vanderstichele, H.; Vanmechelen, E.; Blennow, K. Transient increase in total tau but not phospho-tau in human cerebrospinal fluid after acute stroke. Neurosci. Lett. 2001, 297, 187–190. [Google Scholar] [CrossRef]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; Mukherjee, P.; Valadka, A.B.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau-Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol. 2017, 74, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Thelin, E.P.; Zeiler, F.A.; Ercole, A.; Mondello, S.; Buki, A.; Bellander, B.M.; Helmy, A.; Menon, D.K.; Nelson, D.W. Serial Sampling of Serum Protein Biomarkers for Monitoring Human Traumatic Brain Injury Dynamics: A Systematic Review. Front. Neurol. 2017, 8, 300. [Google Scholar] [CrossRef] [PubMed]
- Nash, L.A.; Burns, J.K.; Chardon, J.W.; Kothary, R.; Parks, R.J. Spinal Muscular Atrophy: More than a Disease of Motor Neurons? Curr. Mol. Med. 2016, 16, 779–792. [Google Scholar] [CrossRef] [PubMed]
- Shababi, M.; Lorson, C.L.; Rudnik-Schoneborn, S.S. Spinal muscular atrophy: A motor neuron disorder or a multi-organ disease? J. Anat. 2014, 224, 15–28. [Google Scholar] [CrossRef]
- Christopherson, K.S.; Ullian, E.M.; Stokes, C.C.; Mullowney, C.E.; Hell, J.W.; Agah, A.; Lawler, J.; Mosher, D.F.; Bornstein, P.; Barres, B.A. Thrombospondins are astrocyte-secreted proteins that promote CNS synaptogenesis. Cell 2005, 120, 421–433. [Google Scholar] [CrossRef]
- Eroglu, C.; Allen, N.J.; Susman, M.W.; O’Rourke, N.A.; Park, C.Y.; Ozkan, E.; Chakraborty, C.; Mulinyawe, S.B.; Annis, D.S.; Huberman, A.D.; et al. Gabapentin receptor alpha2delta-1 is a neuronal thrombospondin receptor responsible for excitatory CNS synaptogenesis. Cell 2009, 139, 380–392. [Google Scholar] [CrossRef]
- Pera, M.C.; Coratti, G.; Forcina, N.; Mazzone, E.S.; Scoto, M.; Montes, J.; Pasternak, A.; Mayhew, A.; Messina, S.; Sframeli, M.; et al. Content validity and clinical meaningfulness of the HFMSE in spinal muscular atrophy. BMC Neurol. 2017, 17, 39. [Google Scholar] [CrossRef]
- Stern, P.; Bartos, V.; Uhrova, J.; Bezdickova, D.; Vanickova, Z.; Tichy, V.; Pelinkova, K.; Prusa, R.; Zima, T. Performance characteristics of seven neuron-specific enolase assays. Tumour. Biol. 2007, 28, 84–92. [Google Scholar] [CrossRef]
- Zeltzer, P.M.; Marangos, P.J.; Evans, A.E.; Schneider, S.L. Serum neuron-specific enolase in children with neuroblastoma. Relationship to stage and disease course. Cancer 1986, 57, 1230–1234. [Google Scholar]
- Sieber, M.; Dressler, J.; Franke, H.; Pohlers, D.; Ondruschka, B. Post-mortem biochemistry of NSE and S100B: A supplemental tool for detecting a lethal traumatic brain injury? J. Forensic Leg. Med. 2018, 55, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Spinella, P.C.; Dominguez, T.; Drott, H.R.; Huh, J.; McCormick, L.; Rajendra, A.; Argon, J.; McIntosh, T.; Helfaer, M. S-100beta protein-serum levels in healthy children and its association with outcome in pediatric traumatic brain injury. Crit. Care Med. 2003, 31, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Sutphen, C.L.; Jasielec, M.S.; Shah, A.R.; Macy, E.M.; Xiong, C.; Vlassenko, A.G.; Benzinger, T.L.; Stoops, E.E.; Vanderstichele, H.M.; Brix, B.; et al. Longitudinal Cerebrospinal Fluid Biomarker Changes in Preclinical Alzheimer Disease During Middle Age. JAMA Neurol. 2015, 72, 1029–1042. [Google Scholar] [CrossRef] [PubMed]
- De Schaepdryver, M.; Jeromin, A.; Gille, B.; Claeys, K.G.; Herbst, V.; Brix, B.; Van Damme, P.; Poesen, K. Comparison of elevated phosphorylated neurofilament heavy chains in serum and cerebrospinal fluid of patients with amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 367–373. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | Patient 9 | Patient 10 | Patient 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age [y] | 39 | 29 | 48 | 19 | 38 | 28 | 44 | 29 | 51 | 27 | 71 |
| Gender | male | male | male | female | male | female | female | male | male | female | male |
| SMN2 gene copy number [n] | 4 | 4 | 3 | 3 | 4 | 4 | 4 | 4 | 7 | 3 | 4 |
| Age when diagnosed [y] | 28 | 15 | 36 | 9 | 15 | 11 | 2 | 13 | 16 | 19 | 4 |
| Working | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | no |
| Able to walk | yes | yes | no | yes | yes | yes | yes | yes | yes | yes | no |
| HFMSE [n of 66] timepoint 0 | 51 | 54 | 16 | 53 | 44 | 57 | 51 | 57 | 38 | 38 | 2 |
| HFMSE [n of 66] before fifth dose | 53 | 59 | 36 | 60 | 45 | 59 | 52 | 57 | 41 | 45 | 1 |
| Timepoint | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | Patient 9 | Patient 10 | Patient 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CSF WBC (/µL) | 0 | 5 | 2 | 3 | 1 | 5 | 3 | 3 | 4 | 6 | 1 | 1 |
| Reference range: <5/µL | 1 | 0 | 0 | 3 | 3 | 9 | 5 | 3 | 3 | 4 | 2 | 5 |
| 2 | 1 | 3 | 6 | 5 | 6 | 3 | 3 | 6 | 6 | 2 | 1 | |
| 3 | 1 | 3 | 3 | 2 | 4 | 3 | 1 | 4 | 3 | 3 | 0 | |
| CSF RBC (/µL) | 0 | <100 | <100 | <100 | <100 | <500 | <500 | <500 | <500 | <500 | <500 | <500 |
| 1 | <100 | <100 | <100 | 200 | <500 | <500 | <500 | <500 | <500 | <500 | <500 | |
| 2 | <100 | 100 | <100 | <500 | <500 | <500 | <500 | <500 | <500 | <500 | 700 | |
| 3 | 100 | <500 | 100 | <500 | <500 | <500 | <500 | <500 | <500 | <500 | <500 | |
| CSF lactate (mM) | 0 | 1.6 | 1.7 | 1.6 | 1.7 | 1.7 | 1.4 | 1.7 | 1.7 | 1.8 | 1.7 | 2.5 |
| Reference range: 0.5–2.2 mM, | 1 | 1.3 | 1.3 | 1.7 | 1.5 | 1.8 | 1.6 | 1.6 | 1.5 | 1.6 | 1.8 | 2.3 |
| >60 years: 1.7–2.6 mM | 2 | 1.4 | 1.4 | 1.4 | 1.5 | 1.6 | 1.7 | 1.9 | 1.5 | 1.9 | 1.7 | 2.1 |
| 3 | 1.4 | 1.5 | 1.8 | 1.5 | 1.6 | 1.7 | 1.7 | 1.3 | 2.0 | 1.9 | 2.1 | |
| CSF glucose (mg/dL) | 0 | 64 | 70 | 64 | 59 | 63 | 60 | 60 | 66 | 69 | 60 | 60 |
| Reference range: 49–75 mg/dL | 1 | 61 | 63 | 65 | 58 | 59 | 61 | 56 | 66 | 66 | 59 | 61 |
| 2 | 58 | 67 | 60 | 57 | 63 | 58 | 60 | 61 | 70 | 61 | 55 | |
| 3 | 63 | 68 | 70 | 59 | 65 | 62 | 58 | 61 | 63 | 61 | 60 | |
| CSF total protein (mg/dL) | 0 | 63 | 34 | 63 | 27 | 56 | 36 | 40 | 29 | 54 | 36 | 68 |
| Reference range: 15–45 mg/dL | 1 | 60 | 24 | 62 | 33 | 56 | 35 | 43 | 31 | 55 | 32 | 70 |
| 2 | 66 | 36 | 63 | 31 | 50 | 36 | 40 | 29 | 55 | 25 | 80 | |
| 3 | 69 | 34 | 58 | 27 | 50 | 30 | 41 | 31 | 57 | 31 | 57 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Totzeck, A.; Stolte, B.; Kizina, K.; Bolz, S.; Schlag, M.; Thimm, A.; Kleinschnitz, C.; Hagenacker, T. Neurofilament Heavy Chain and Tau Protein Are Not Elevated in Cerebrospinal Fluid of Adult Patients with Spinal Muscular Atrophy during Loading with Nusinersen. Int. J. Mol. Sci. 2019, 20, 5397. https://doi.org/10.3390/ijms20215397
Totzeck A, Stolte B, Kizina K, Bolz S, Schlag M, Thimm A, Kleinschnitz C, Hagenacker T. Neurofilament Heavy Chain and Tau Protein Are Not Elevated in Cerebrospinal Fluid of Adult Patients with Spinal Muscular Atrophy during Loading with Nusinersen. International Journal of Molecular Sciences. 2019; 20(21):5397. https://doi.org/10.3390/ijms20215397
Chicago/Turabian StyleTotzeck, Andreas, Benjamin Stolte, Kathrin Kizina, Saskia Bolz, Melina Schlag, Andreas Thimm, Christoph Kleinschnitz, and Tim Hagenacker. 2019. "Neurofilament Heavy Chain and Tau Protein Are Not Elevated in Cerebrospinal Fluid of Adult Patients with Spinal Muscular Atrophy during Loading with Nusinersen" International Journal of Molecular Sciences 20, no. 21: 5397. https://doi.org/10.3390/ijms20215397
APA StyleTotzeck, A., Stolte, B., Kizina, K., Bolz, S., Schlag, M., Thimm, A., Kleinschnitz, C., & Hagenacker, T. (2019). Neurofilament Heavy Chain and Tau Protein Are Not Elevated in Cerebrospinal Fluid of Adult Patients with Spinal Muscular Atrophy during Loading with Nusinersen. International Journal of Molecular Sciences, 20(21), 5397. https://doi.org/10.3390/ijms20215397