A Systematic Review of Neuroprotective Strategies during Hypovolemia and Hemorrhagic Shock


Abstract
1. Introduction
2. Results
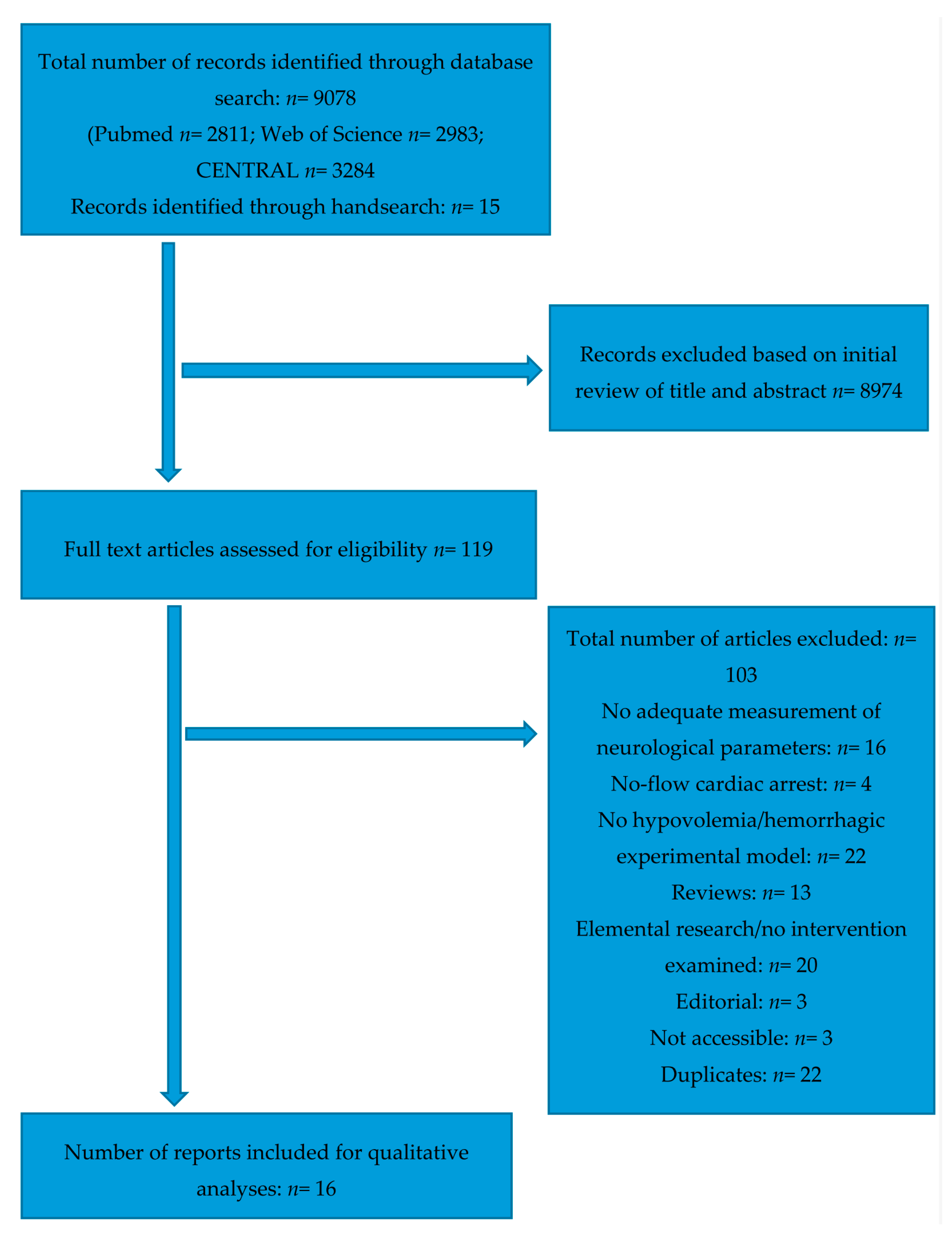
2.1. Study Selection
2.2. Study Characteristics
2.3. Results of Individual Studies
2.3.1. Hypothermia
2.3.2. Varying Fluid Resuscitation Protocols and Hypertonic-Hyperoncotic Solutions, Partly in Combination with Epinephrine and Vasopressin
2.3.3. Other Neuroprotective Strategies
NHE1-Inhibition
Aprotinin
Piracetam
Sevoflurane
Human Mesenchymal Stem Cells
Remote Ischemic Preconditioning
2.4. Risk of Bias within Studies
3. Discussion
3.1. Reviewed Interventions
3.2. Study Quality and Translational Value
3.3. Limitations
4. Materials and Methods
4.1. Review Protocol
4.2. Eligibility Criteria
- -
- Types of participants: Experimental animal models of haemorrhagic shock and hypovolemia, as well as studies considering human participants suffering from the same conditions.
- -
- Types of interventions: All neuroprotective interventions.
- -
- Types of Comparators: Trials comparing the interventions either with a control group/no intervention, standard care or other neuroprotective interventions (if the study design featured multiple interventions).
- -
- Types of outcome measures: A neuroprotective effect, either measured through neurological parameters, cognitive tests or imaging techniques (brain imaging, staining, etc.).
- -
- Types of study design: Randomised controlled trials.
4.3. Information Sources
4.4. Study Selection
4.5. Data Collection Process
4.6. Data Items
- General data of the respective trials (animal model, number of animals, and general vital parameters);
- The specific hypovolemia model that the respective study used (i.e., blood loss/heart rate/blood pressure values the studies’ authors defined as an established hypovolemia);
- The type of intervention (including dosage and duration);
- The outcome measures of the neuroprotective interventions (brain specific parameters, cerebral histopathological values, cognitive tests, and further brain tissue markers).
4.7. Risk of Bias in Individual Studies
4.8. Summary Measures and Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A
Pubmed Search Strategy
- cerebrovascular circulation [MeSH terms]
- neuroprotection [tw]
- neuro* [tw]
- brain
- brain protection
- brain damage
- cerebral blood flow
- autoregulation
- cogni* [tw]
- 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9
- shock, hemorrhagic [MeSH terms]
- hypovol* [tw]
- hemorrha* [tw]
- haemorrha* [tw]
- 11 OR 12 OR 13 OR 14
- randomized trial
- randomized trial
- random*
- 16 OR 17 OR 18
- 10 AND 15 AND 19
CENTRAL Search Strategy
- MeSH descriptor: [Shock, Hemorrhagic] explode all trees
- MeSH descriptor: [Hypovolemia] explode all trees
- hypovol*:ti,ab,kw (Word variations have been searched)
- hemorrha*:ti,ab,kw (Word variations have been searched)
- haemorrha*:ti,ab,kw (Word variations have been searched)
- blood loss:ti,ab,kw (Word variations have been searched)
- #1 or #2 or #3 or #4 or #5 or #6
- MeSH descriptor: [Neuroprotective Agents] explode all trees
- MeSH descriptor: [Cerebrovascular Circulation] explode all trees
- neuro*:ti,ab,kw (Word variations have been searched)
- cogniti*:ti,ab,kw (Word variations have been searched)
- brain damage:ti,ab,kw (Word variations have been searched)
- #8 or #9 or #10 or #11 or #12
- #7 and #13
Web of Science Search Strategy
- “h*morrhagic shock”
- “hypovol*mic shock”
- h*morrhag*
- hypovol*
- #1 OR #2 OR #3 OR #4
- neuroprotect*
- “cerebr* circulation”
- “cerebral blood flow”
- “brain damage”
- cogniti*
- #6 OR #7 OR #8 OR #9 OR #10
- #5 AND #11
- random*
- rct
- trial
- #13 OR #14 OR #15
- #12 AND #16
References
- Kauvar, D.S.; Lefering, R.; Wade, C.E. Impact of hemorrhage on trauma outcome: An overview of epidemiology, clinical presentations, and therapeutic considerations. J. Trauma 2006, 60, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Peden, M.; Mcgee, K.S.; Sharma, G. The Injury Chartbook: A Graphical Overview of the Global Burden of Injuries; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Gutierrez, G.; Reines, H.D.; Wulf-Gutierrez, M.E. Clinical review: Hemorrhagic shock. Crit. Care (Lond. Engl.) 2004, 8, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Shevell, T.; Malone, F.D. Management of obstetric hemorrhage. Semin. Perinatol. 2003, 27, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (dalys) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet (Lond. Engl.) 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Chouchani, E.T.; Pell, V.R.; James, A.M.; Work, L.M.; Saeb-Parsy, K.; Frezza, C.; Krieg, T.; Murphy, M.P. A unifying mechanism for mitochondrial superoxide production during ischemia-reperfusion injury. Cell Metab. 2016, 23, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Osterbur, K.; Mann, F.A.; Kuroki, K.; DeClue, A. Multiple organ dysfunction syndrome in humans and animals. J. Vet. Intern. Med. 2014, 28, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- Fantini, S.; Sassaroli, A.; Tgavalekos, K.T.; Kornbluth, J. Cerebral blood flow and autoregulation: Current measurement techniques and prospects for noninvasive optical methods. Neurophotonics 2016, 3, 031411. [Google Scholar] [CrossRef] [PubMed]
- Rickards, C.A.; Sprick, J.D.; Colby, H.B.; Kay, V.L.; Tzeng, Y.C. Coupling between arterial pressure, cerebral blood velocity, and cerebral tissue oxygenation with spontaneous and forced oscillations. Physiol. Meas. 2015, 36, 785–801. [Google Scholar] [CrossRef] [PubMed]
- Rickards, C.A. Cerebral blood-flow regulation during hemorrhage. Compr. Physiol. 2015, 5, 1585–1621. [Google Scholar] [PubMed]
- Kudo, Y.; Ohtaki, H.; Dohi, K.; Yin, L.; Nakamachi, T.; Endo, S.; Yofu, S.; Hiraizumi, Y.; Miyaoka, H.; Shioda, S. Neuronal damage in rat brain and spinal cord after cardiac arrest and massive hemorrhagic shock. Crit. Care Med. 2006, 34, 2820–2826. [Google Scholar] [CrossRef] [PubMed]
- Heckbert, S.R.; Vedder, N.B.; Hoffman, W.; Winn, R.K.; Hudson, L.D.; Jurkovich, G.J.; Copass, M.K.; Harlan, J.M.; Rice, C.L.; Maier, R.V. Outcome after hemorrhagic shock in trauma patients. J. Trauma 1998, 45, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Schiffner, R.; Bischoff, S.J.; Lehmann, T.; Rakers, F.; Rupprecht, S.; Reiche, J.; Matziolis, G.; Schubert, H.; Schwab, M.; Huber, O.; et al. Redistribution of cerebral blood flow during severe hypovolemia and reperfusion in a sheep model: Critical role of α1-adrenergic signaling. Int. J. Mol. Sci. 2017, 18, 1031. [Google Scholar] [CrossRef] [PubMed]
- Thomas Yeo, B.T.; Krienen, F.M.; Sepulcre, J.; Sabuncu, M.R.; Lashkari, D.; Hollinshead, M.; Roffman, J.L.; Smoller, J.W.; Zöllei, L.; Polimeni, J.R.; et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 2011, 106, 1125–1165. [Google Scholar] [CrossRef] [PubMed]
- Frey, C.B.; Osborne, M.A. The future of employment: How susceptible are jobs to computerisation? Technol. Forecast. Soc. Chang. 2017, 114, 254–280. [Google Scholar] [CrossRef]
- Cavus, E.; Meybohm, P.; Dorges, V.; Stadlbauer, K.H.; Wenzel, V.; Weiss, H.; Scholz, J.; Bein, B. Regional and local brain oxygenation during hemorrhagic shock: A prospective experimental study on the effects of small-volume resuscitation with norepinephrine. J. Trauma 2008, 64, 641–648; discussion 648–649. [Google Scholar] [CrossRef] [PubMed]
- Cavus, E.; Meybohm, P.; Doerges, V.; Hugo, H.H.; Steinfath, M.; Nordstroem, J.; Scholz, J.; Bein, B. Cerebral effects of three resuscitation protocols in uncontrolled haemorrhagic shock: A randomised controlled experimental study. Resuscitation 2009, 80, 567–572. [Google Scholar] [CrossRef] [PubMed]
- Chien, J.C.; Jeng, M.J.; Soong, W.J.; Hwang, B. Effects of fluid resuscitation on cerebral tissue oxygenation changes in a piglet model of hemorrhagic shock. J. Chin. Med. Assoc. JCMA 2011, 74, 448–454. [Google Scholar] [CrossRef] [PubMed]
- Ida, K.K.; Otsuki, D.A.; Sasaki, A.T.C.; Borges, E.S.; Castro, L.U.C.; Sanches, T.R.; Shimizu, M.H.M.; Andrade, L.C.; Auler, J.O.C.; Dyson, A.; et al. Effects of terlipressin as early treatment for protection of brain in a model of haemorrhagic shock. Crit. Care 2015, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Meybohm, P.; Cavus, E.; Bein, B.; Steinfath, M.; Brand, P.A.; Scholz, J.; Dorges, V. Cerebral metabolism assessed with microdialysis in uncontrolled hemorrhagic shock after penetrating liver trauma. Anesth. Analg. 2006, 103, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Meybohm, P.; Cavus, E.; Dorges, V.; Weber, B.; Stadlbauer, K.H.; Wenzel, V.; Scholz, J.; Steffen, M.; Bein, B. Release of protein s100b in haemorrhagic shock: Effects of small volume resuscitation combined with arginine vasopressin. Resuscitation 2008, 76, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Meybohm, P.; Cavus, E.; Bein, B.; Steinfath, M.; Weber, B.; Hamann, C.; Scholz, J.; Dorges, V. Small volume resuscitation: A randomized controlled trial with either norepinephrine or vasopressin during severe hemorrhage. J. Trauma 2007, 62, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Vogt, N.; Herden, C.; Roeb, E.; Roderfeld, M.; Eschbach, D.; Steinfeldt, T.; Wulf, H.; Ruchholtz, S.; Uhl, E.; Scholler, K. Cerebral alterations following experimental multiple trauma and hemorrhagic shock. Shock (Augusta Ga.) 2017. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Russano, K.; Kouz, I.; Abraham, W.M. Nhe1 inhibition improves tissue perfusion and resuscitation outcome after severe hemorrhage. J. Surg. Res. 2013, 181, e75–e81. [Google Scholar] [CrossRef] [PubMed]
- Eser, O.; Kalkan, E.; Cosar, M.; Buyukbas, S.; Avunduk, M.C.; Aslan, A.; Kocabas, V. The effect of aprotinin on brain ischemic-reperfusion injury after hemorrhagic shock in rats: An experimental study. J. Trauma 2007, 63, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Guven, H.; Amanvermez, R.; Malazgirt, Z.; Kaya, E.; Doganay, Z.; Celik, C.; Ozkan, K. Moderate hypothermia prevents brain stem oxidative stress injury after hemorrhagic shock. J. Trauma 2002, 53, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.W.; Wang, J.X.; Zhang, Q.Q.; Duan, X.W.; Chen, Z.W.; Zhang, Y. Postconditioning with sevoflurane ameliorates spatial learning and memory deficit after hemorrhage shock and resuscitation in rats. J. Surg. Res. 2016, 206, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Yang, Z.; Yang, M.; Qian, J.; Cahoon, J.; Xu, J.; Sun, S.; Tang, W. Remote ischemic preconditioning mitigates myocardial and neurological dysfunction via k(atp) channel activation in a rat model of hemorrhagic shock. Shock (Augusta Ga.) 2014, 42, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Plaschke, K. Human adult mesenchymal stem cells improve rat spatial cognitive function after systemic hemorrhagic shock. Behav. Brain Res. 2009, 201, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, S.; Ikizceli, I.; Sozuer, E.M.; Avsarogullari, L.; Ozturk, F.; Muhtaroglu, S.; Akdur, O.; Kucuk, C.; Durukan, P. The effect of piracetam on brain damage and serum nitric oxide levels in dogs submitted to hemorrhagic shock. Ulus. Travma Acil Cerrahi Derg. Turk. J. Trauma Emerg. Surg. TJTES 2008, 14, 277–283. [Google Scholar]
- Kishi, K.; Kawaguchi, M.; Kurehara, K.; Inoue, S.; Sakamoto, T.; Einaga, T.; Kitaguchi, K.; Furuya, H. Hypothermia attenuates the vasodilatory response of pial arterioles to hemorrhagic hypotension in the cat. Anesth. Analg. 2000, 91, 140–144. [Google Scholar] [PubMed]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. Syrcle’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [PubMed]
- Bulger, E.M.; Hoyt, D.B. Hypertonic resuscitation after severe injury: Is it of benefit? Adv. Surg. 2012, 46, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Bulger, E.M.; May, S.; Kerby, J.D.; Emerson, S.; Stiell, I.G.; Schreiber, M.A.; Brasel, K.J.; Tisherman, S.A.; Coimbra, R.; Rizoli, S.; et al. Out-of-hospital hypertonic resuscitation after traumatic hypovolemic shock: A randomized, placebo controlled trial. Ann. Surg. 2011, 253, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Roberts, I.; Alderson, P.; Bunn, F.; Chinnock, P.; Ker, K.; Schierhout, G. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database Syst. Rev. 2004, CD000567. [Google Scholar] [CrossRef] [PubMed]
- Rossaint, R.; Bouillon, B.; Cerny, V.; Coats, T.J.; Duranteau, J.; Fernandez-Mondejar, E.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Nardi, G.; et al. The european guideline on management of major bleeding and coagulopathy following trauma: Fourth edition. Crit. Care (Lond. Engl.) 2016, 20, 100. [Google Scholar] [CrossRef]
- Bulger, E.M.; Jurkovich, G.J.; Nathens, A.B.; Copass, M.K.; Hanson, S.; Cooper, C.; Liu, P.Y.; Neff, M.; Awan, A.B.; Warner, K.; et al. Hypertonic resuscitation of hypovolemic shock after blunt trauma: A randomized controlled trial. Arch. Surg. (Chicago IL. 1960) 2008, 143, 139–148; discussion 149. [Google Scholar] [CrossRef] [PubMed]
- Sperry, J.L.; Minei, J.P.; Frankel, H.L.; West, M.A.; Harbrecht, B.G.; Moore, E.E.; Maier, R.V.; Nirula, R. Early use of vasopressors after injury: Caution before constriction. J. Trauma 2008, 64, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Giraud, R.; Siegenthaler, N.; Arroyo, D.; Bendjelid, K. Impact of epinephrine and norepinephrine on two dynamic indices in a porcine hemorrhagic shock model. J. Trauma Acute Care Surg. 2014, 77, 564–569; quiz 650–561. [Google Scholar] [CrossRef] [PubMed]
- Anand, T.; Skinner, R. Arginine vasopressin: The future of pressure-support resuscitation in hemorrhagic shock. J. Surg. Res. 2012, 178, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Cossu, A.P.; Mura, P.; De Giudici, L.M.; Puddu, D.; Pasin, L.; Evangelista, M.; Xanthos, T.; Musu, M.; Finco, G. Vasopressin in hemorrhagic shock: A systematic review and meta-analysis of randomized animal trials. BioMed Res. Int. 2014, 2014, 421291. [Google Scholar] [CrossRef] [PubMed]
- Serpa Neto, A.; Nassar, A.P.; Cardoso, S.O.; Manetta, J.A.; Pereira, V.G.; Esposito, D.C.; Damasceno, M.C.; Russell, J.A. Vasopressin and terlipressin in adult vasodilatory shock: A systematic review and meta-analysis of nine randomized controlled trials. Crit. Care (Lond. Engl.) 2012, 16, R154. [Google Scholar] [CrossRef] [PubMed]
- Frank, F.; Broessner, G. Is there still a role for hypothermia in neurocritical care? Curr. Opin. Crit. Care 2017, 23, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Stocchetti, N.; Taccone, F.S.; Citerio, G.; Pepe, P.E.; Le Roux, P.D.; Oddo, M.; Polderman, K.H.; Stevens, R.D.; Barsan, W.; Maas, A.I.; et al. Neuroprotection in acute brain injury: An up-to-date review. Crit. Care (Lond. Engl.) 2015, 19, 186. [Google Scholar] [CrossRef] [PubMed]
- Lier, H.; Krep, H.; Schroeder, S.; Stuber, F. Preconditions of hemostasis in trauma: A review. The influence of acidosis, hypocalcemia, anemia, and hypothermia on functional hemostasis in trauma. J. Trauma 2008, 65, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Coats, T.J.; Duranteau, J.; Fernandez-Mondejar, E.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Nardi, G.; et al. Management of bleeding and coagulopathy following major trauma: An updated european guideline. Crit. Care (Lond. Engl.) 2013, 17, R76. [Google Scholar] [CrossRef] [PubMed]
- Krueger, A.; Frink, M.; Kiessling, A.; Ruchholtz, S.; Kuhne, C.A. [emergency room management: In the era of the white paper, s3 guidelines, advanced trauma life support(r) and traumanetwork dgu(r) of the german society of trauma surgery]. Chir. Z. Alle Geb. Oper. Medizen 2013, 84, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Celani, M.G.; Cantisani, T.A.; Righetti, E. Piracetam for acute ischaemic stroke. Cochrane Database Syst. Rev. 2012, CD000419. [Google Scholar] [CrossRef]
- Verma, D.K.; Joshi, N.; Raju, K.S.; Wahajuddin, M.; Singh, R.K.; Singh, S. Metabolic enhancer piracetam attenuates rotenone induced oxidative stress: A study in different rat brain regions. Acta Neurobiol. Exp. 2015, 75, 399–411. [Google Scholar]
- Hwang, I.K.; Yoo, K.Y.; An, S.J.; Li, H.; Lee, C.H.; Choi, J.H.; Lee, J.Y.; Lee, B.H.; Kim, Y.M.; Kwon, Y.G.; et al. Late expression of na+/h+ exchanger 1 (nhe1) and neuroprotective effects of nhe inhibitor in the gerbil hippocampal ca1 region induced by transient ischemia. Exp. Neurol. 2008, 212, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, P.; Kleman, N.; Uluc, K.; Kendigelen, P.; Hagemann, T.; Akture, E.; Messing, A.; Ferrazzano, P.; Sun, D. Inhibition of na+/h+ exchanger isoform 1 is neuroprotective in neonatal hypoxic ischemic brain injury. Antioxid. Redox Signal. 2011, 14, 1803–1813. [Google Scholar] [CrossRef] [PubMed]
- Laroni, A.; de Rosbo, N.K.; Uccelli, A. Mesenchymal stem cells for the treatment of neurological diseases: Immunoregulation beyond neuroprotection. Immunol. Lett. 2015, 168, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, T.B.; Duarte, A.S.; Longhini, A.L.; Pradella, F.; Farias, A.S.; Luzo, A.C.; Oliveira, A.L.; Olalla Saad, S.T. Neuroprotection and immunomodulation by xenografted human mesenchymal stem cells following spinal cord ventral root avulsion. Sci. Rep. 2015, 5, 16167. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Nicole, O.; Okamura, T.; Zurakowski, D.; Jonas, R.A. Aprotinin confers neuroprotection by reducing apoptotic cell death. Asian Cardiovasc. Thorac. Ann. 2010, 18, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Okamura, T.; Ishibashi, N.; Zurakowski, D.; Lidov, H.G.; Jonas, R.A. Optimal dose of aprotinin for neuroprotection and renal function in a piglet survival model. J. Thorac. Cardiovasc. Surg. 2009, 137, 1521–1529; discussion 1529. [Google Scholar] [CrossRef] [PubMed]
- Schifilliti, D.; Grasso, G.; Conti, A.; Fodale, V. Anaesthetic-related neuroprotection intravenous or inhalational agents? CNS Drugs 2010, 24, 893–907. [Google Scholar] [PubMed]
- Ishida, K.; Berger, M.; Nadler, J.; Warner, D.S. Anesthetic neuroprotection: Antecedents and an appraisal of preclinical and clinical data quality. Curr. Pharm. Des. 2014, 20, 5751–5765. [Google Scholar] [CrossRef] [PubMed]
- Meller, R.; Simon, R.P. A critical review of mechanisms regulating remote preconditioning-induced brain protection. J. Appl. Physiol. 2015, 119, 1135–1142. [Google Scholar] [CrossRef] [PubMed]
- Tengfei, L.; Jiangning, W. Remote ischemic conditioning: A novel way to treat ischemia-related injury of limbs. Med. Hypotheses 2015, 84, 504–505. [Google Scholar] [CrossRef] [PubMed]
- Heusch, G. Molecular basis of cardioprotection: Signal transduction in ischemic pre-, post-, and remote conditioning. Circ. Res. 2015, 116, 674–699. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Li, X.; Peng, Y. Remote ischemic conditioning for acute ischemic stroke: Dawn in the darkness. Rev. Neurosci. 2016, 27, 501–510. [Google Scholar] [CrossRef] [PubMed]
- De Vries, R.B.; Wever, K.E.; Avey, M.T.; Stephens, M.L.; Sena, E.S.; Leenaars, M. The usefulness of systematic reviews of animal experiments for the design of preclinical and clinical studies. ILAR J. 2014, 55, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Russel, W.; Burch, R. The Principles of Humane Experimental Technique; as reprinted 1992; Universities Federation for Animal Welfare: Wheathampstead, UK, 1959. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Int. J. Surg. (Lond. Engl.) 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. JBI Data Extraction form for Experimental/Observational Studies. Available online: https://joannabriggs.org/assets/docs/jbc/operations/dataExtractionForms/JBC_Form_DataE_ExpObs.pdf (accessed on 2 August 2017).
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Clin. Res. Ed.) 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Table 1A. Study design. | |||||
| Author/Year | Animal Model | Intervention | Total Number of Animals n = x | Extent of Hypovolemia | Observation Period of Animals after Intervention (None = Direct Euthanasia) |
| Cavus et al., 2008 [16] | pigs | HHS vs. low-dose norepinephrine vs. high-dose epinephrine | 22 | MAP < 25 mmHg or −20% HR of baseline | None |
| Cavus et al., 2009 [17] | pigs | HHS vs. low-dose norepinephrine vs. high-dose epinephrine | 24 | MAP < 25 mmHg or −20% HR of baseline | None |
| Chien et al., 2011 [18] | pigs | normal saline vs. initial bolus saline and, respectively, whole blood, ringer lactat and normal saline | 30 | <45 mmHg MAP | None |
| Eser et al., 2007 [25] | rats | Isotonic solution vs. aprotinin | 18 | 40–50% systolic BP of baseline | None |
| Guven et al., 2002 [26] | rats | Normothermia vs. 32 °C hypothermia vs. 28 °C hypothermia | 40 | 40% of estimated total blood volume | None |
| Hu et al., 2014 [28] | rats | RICP vs. RICP and KATP-blocker | 21 | 50% estimated total blood volume | to 3 days |
| Hu et al., 2016 [27] | rats | low-dose sevoflurane vs. moderate-dose sevoflurane vs. high-dose sevoflurane | 35 | Unclear | 3 days |
| Ida et al., 2015 [19] | pigs | Ringer lactat vs. terlipressin | 46 | <40 mmHg MAP | None |
| Kishi et al., 2000 [31] | cats | Normothermia vs. hypothermia (in respect to vasodilatory response of pail arterioles | 20 | 50 mmHg MAP | None |
| Meybohm et al., 2006 [20] | pigs | Fluid vs. HHS and arginine vasopressine | 16 | <25 mmHg or −20% HR of baseline | None |
| Meybohm et al., 2008 [21] | pigs | Crystalloid and colloidal fluids vs. HHS and NS vs. HHS and arginine vasopressine | 30 | <25 mmHg or −30% HR of baseline | None |
| Meybohm et al., 2007 [22] | pigs | HHS and norepinephrine vs. HHS and arginine vasopressin | 14 | <25 mmHg MAP or −20% HR of baseline | None |
| Özkan et al., 2008 [30] | dogs | Blood and saline vs., blood and piracetam | 40 | 40 mmHg MAP | None |
| Plaschke 2009 [29] | rats | hMSC | 32 | 30–40 mmHg MAP | 6 days |
| Vogt et al., 2017 [23] | pigs | Hypothermia after 90 min vs. 120 min | 60 | 40–50% of estimated total blood volume | None |
| Wu et al., 2012 [24] | pigs | NHE1 inhibtion | 22 | Removal of 40 mL/kg blood | 3 days |
| Table 1B. Outcome parameters. | |||||
| Author/Year | Detected Vital Parameters (e.g., Blood Gases, Hemodynamics, Blood Pressure, Heart Rate, Temperature) | Detected Brain Specific Parameters (e.g., ICP, CPP, CBF, Diameters of Brain Resistant Vessels, rScO2) | Detected Brain Specific Histo-Pathological Treatmens (Neuronal Cell Damage) | Detected Log Term Results, Cognitive Function | Other Specific Parameters in Brain Tissues |
| Cavus et al., 2008 [16] | + | + | − | − | − |
| Cavus et al., 2009 [17] | + | + | − | − | − |
| Chien et al., 2011 [18] | + | + | − | − | − |
| Eser et al., 2007 [25] | + | − | + | − | SOD, MDA, MPO |
| Guven et al., 2002 [26] | + | − | − | − | GSH, TBARS |
| Hu et al., 2014 [28] | + | − | - | + | − |
| Hu et al., 2016 [27] | + | − | + | + | CHAT, ACHE |
| Ida et al., 2015 [19] | + | + | − | − | AQP4, NKCC1, SOD, TBARS, Bax, Bcl-x |
| Kishi et al., 2000 [31] | + | + | − | − | − |
| Meybohm et al., 2006 [20] | + | + | − | − | Glu, La, Py, Gly |
| Meybohm et al., 2008 [21] | + | + | − | − | S100B |
| Meybohm et al., 2007 [22] | + | + | − | − | Glu, La, Py, Gly |
| Özkan et al., 2008 [30] | + | − | + | − | − |
| Plaschke 2009 [29] | + | − | + | + | − |
| Vogt et al., 2017 [23] | + | + | + | − | S100B, NSE, Iba1 |
| Wu et al., 2012 [24] | + | + | − | + | − |
| Author | Start of Hypothermia Respective to Hypovolemia | Depth of Hypovolemia | Length of Hypovolemia (Total Length/Time after which Desired Depth was Achieved) | Rewarming Period |
|---|---|---|---|---|
| Guven et al. [26] | 0 min | 32 °C vs. 28 °C | 1.5 h/0.5 h | None |
| Kishi et al. [31] | −60 min | 32 °C | 1.4 h/? | None |
| Vogt et al. [23] | +90 vs. +120 min | 33 °C | 12 h/3 h | 10 h |
| Author/Year | Interventions | Dosage | Start of Intervention Respective to Hypovolemia | Length of Intervention/Length of Subsequent Observation Period | |
|---|---|---|---|---|---|
| Cavus et al., 2009 [17] | Fluid resuscitation | 6% HES 130/0.4, 20 mL/kg, and Ringer 40 mL/kg | Immediately after predefined hypovolemia criteria were met | 30 min/30 min | |
| NE + HS | Bolus 20 µg/kg and continuously 1 µ/kg/min + HS 4 mL/kg | ||||
| AVP + HS | Bolus 0.2 U/kg and continuously 0.04 U/kg/min + HS 4 mL/kg | ||||
| Cavus et al., 2008 [16] | HHS | 4 mL/kg | Immediately after predefined hypovolemia criteria were met | 30 min/30 min | |
| HHS + low-dose NE | 4 mL/kg + 500 µg and 1/kg/min | ||||
| HHS+ high-dose NE | 4 mL + 1000 µg and 1 µg/kg/min | ||||
| Chien et al., 2011 [18] | NS | NS (all groups: 10 mL/kg | / | Immediately after induction of haemorrhagic shock | 240 min/0 min |
| NS + WB | 15 mL/kg (+additional 15 mL/kg every 15 min if MAP > 45 | ||||
| NS + LR | 15 mL/kg (+additional 15 mL/kg every 15 min if MAP > 45 | ||||
| NS + NS | 15 mL/kg (+additional 15 mL/kg every 15 min if MAP > 45 | ||||
| Ida et al.,2015 [19] | LR | Three-times of bled volume | 30 min after predefined hypovolemia criteria were met | Instantenous/120 min | |
| Terlipressin | 2 mg bolus | ||||
| Meybohm et al., 2006 [20] | Fluid resuscitation | Ringer’s solution (40 mL/kg) and hydroxyethyl starch 130/0.4 (20 mL/kg) | Immediately after predefined hypovolemia criteria were met | 30 min/30 min | |
| HHS + AVP | 4 mL/kg + bolus 10 U and continuously 2 U/kg/h | ||||
| Meybohm et al., 2008 [21] | Fluid resuscitation | Crystalloid (40 mL/kg) and colloid (20 mL/kg) | Immediately after predefined hypovolemia criteria were met | 30 min/30 min | |
| HHS + NS | 4 mL/kg + 10 mL bolus and continuously 1 mL/kg/h | ||||
| HHS + AVP | 4 mL/kg + 0.2 U/kg bolus and continuously 2 U/kg/h | ||||
| Meybohm et al., 2007 [22] | HHS + NE | 4 mL/kg + 1000 µg bolus and continuously 60 µg/kg/h | Immediately after predefined hypovolemia criteria were met | 30 min/30 min | |
| HHS + AVP | 4 mL/kg + 10 U bolus and continuously 2 U/kg/h | ||||
| Author/Year | Intervention | Dosage | Start of Intervention Respective to Hypovolemia | Length of Intervention/Length of Subsequent Observation Period |
|---|---|---|---|---|
| Eser, et al., 2007 [25] | Aprotinin | 30,000 KIU/kg/h/0.7 mL bolus + 10,000 KIU/kg/h/0.2 mL during reperfusion | +15 min (5 min before reperfusion) | 20 min/? |
| Hu et al., 2014 [28] | Remote ischemic preconditioning (RIPC) | 4 cycles of 5 min limb ischemia and 5 min reperfusion vs. 4 cycles of limb ischemia and 5 min reperfusion with addition of KATP-blockade | Immediately before the start of the hypovolemia protocol | 120 min/72 h |
| Hu et al., 2016 [27] | Sevoflurane | 1.2% vs. 2.2% vs. 3.6% | +60 min | 120 min/72 h |
| Özkan et al., 2008 [30] | Piracetam | 800 mg/kg | +60 min | 120 min/0 min |
| Plaschke 2009 [29] | Human mesenchymal stem cells | 1 × 106 hMSC | +30 min | 30 min/6 days |
| Wu et al., 2012 [24] | NHE1-Inhibition | 3 mg/kg BIIB513 (both for neurological outcome experimental group and organ blood flow experimental group) | Immediately after predefined hypovolemia criteria were met | 90 min/72 h |
| Author/Year | Baseline Characteristics | Allocation Concealment | Random Housing | Blinding (Performance) | Random Outcome Assessment | Blinding (Detection) | Incomplete Outcome Data | Selective Outcome Reporting | Sequence Generation | Other Sources of Bias |
|---|---|---|---|---|---|---|---|---|---|---|
| Cavus et al., 2008 [16] | + | + | N.A. | + | − | + | + | + | + | + |
| Cavus et al., 2009 [17] | + | + | N.A. | − | − | + | + | + | + | + |
| Chien et al., 2011 [18] | + | ? | N.A. | − | ? | + | + | + | + | ? |
| Eser et al., 2007 [25] | + | − | ? | − | − | − | ? | ? | − | ? |
| Guven et al., 2002 [26] | + | − | N.A. | − | − | − | + | + | − | + |
| Hu et al., 2014 [28] | + | + | N.A. | + | ? | + | + | + | + | + |
| Hu et al., 2016 [27] | + | − | N.A. | − | − | ? | + | + | + | + |
| Ida et al., 2015 [19] | + | + | N.A. | − | − | + | + | + | + | + |
| Kishi et al., 2000 [31] | + | − | − | − | − | − | ? | ? | + | ? |
| Meybohm et al., 2006 [20] | + | ? | N.A. | − | ? | + | + | + | + | + |
| Meybohm et al., 2008 [21] | + | − | N.A | − | − | + | + | + | + | + |
| Meybohm et al., 2007 [22] | + | + | N.A | + | ? | + | + | + | + | + |
| Özkan et al., 2008 [30] | + | − | N.A | − | − | − | + | ? | + | + |
| Plaschke 2009 [29] | + | − | ? | ? | ? | ? | − | − | + | − |
| Vogt et al., 2017 [23] | + | ? | N.A | − | ? | + | − | + | − | + |
| Wu et al., 2012 [24] | + | + | ? | + | − | + | + | + | + | + |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nistor, M.; Behringer, W.; Schmidt, M.; Schiffner, R. A Systematic Review of Neuroprotective Strategies during Hypovolemia and Hemorrhagic Shock. Int. J. Mol. Sci. 2017, 18, 2247. https://doi.org/10.3390/ijms18112247
Nistor M, Behringer W, Schmidt M, Schiffner R. A Systematic Review of Neuroprotective Strategies during Hypovolemia and Hemorrhagic Shock. International Journal of Molecular Sciences. 2017; 18(11):2247. https://doi.org/10.3390/ijms18112247
Chicago/Turabian StyleNistor, Marius, Wilhelm Behringer, Martin Schmidt, and René Schiffner. 2017. "A Systematic Review of Neuroprotective Strategies during Hypovolemia and Hemorrhagic Shock" International Journal of Molecular Sciences 18, no. 11: 2247. https://doi.org/10.3390/ijms18112247
APA StyleNistor, M., Behringer, W., Schmidt, M., & Schiffner, R. (2017). A Systematic Review of Neuroprotective Strategies during Hypovolemia and Hemorrhagic Shock. International Journal of Molecular Sciences, 18(11), 2247. https://doi.org/10.3390/ijms18112247