
Serum Levels of Substance P and Mortality in Patients with a Severe Acute Ischemic Stroke

 , , and
, , and
Abstract
:
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Ethical Adherence
4.2. Design and Subjects
4.3. Variables Recorded
4.4. Blood Sample Collection
4.5. Substance P (SP) Assay
4.6. Tumor Necrosis Factor (TNF)-Alpha Assay
4.7. Statistical Methods
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Adams, H.P., Jr.; del Zoppo, G.; Alberts, M.J.; Bhatt, D.L.; Brass, L.; Furlan, A.; American Heart Association; American Stroke Association Stroke Council; Clinical Cardiology Council; Cardiovascular Radiology and Intervention Council; et al. Guidelines for the early management of adults with ischemic stroke: A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007, 38, 1655–1711. [Google Scholar] [PubMed]
- Turner, R.J.; Vink, R. The role of substance P in ischaemic brain injury. Brain Sci. 2013, 3, 123–142. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.M.; Turner, R.J.; Vink, R. Blocking neurogenic inflammation for the treatment of acute disorders of the central nervous system. Int. J. Inflamm. 2013, 2013, 578480. [Google Scholar] [CrossRef] [PubMed]
- Thornton, E.; Ziebell, J.M.; Leonard, A.V.; Vink, R. Kinin receptor antagonists as potential neuroprotective agents in central nervous system injury. Molecules 2010, 15, 6598–6618. [Google Scholar] [CrossRef] [PubMed]
- Vink, R.; van den Heuvel, C. Substance P antagonists as a therapeutic approach to improving outcome following traumatic brain injury. Neurotherapeutics 2010, 7, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Walsh, D.A.; McWilliams, D.F. Tachykinins and the cardiovascular system. Curr. Drug Targets 2006, 7, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- Almeida, T.A.; Rojo, J.; Nieto, P.M.; Pinto, F.M.; Hernandez, M.; Martín, J.D.; Candenas, M.L. Tachykinins and tachykinin receptors: Structure and activity relationships. Curr. Med. Chem. 2004, 11, 2045–2081. [Google Scholar] [CrossRef] [PubMed]
- Satake, H.; Kawada, T. Overview of the primary structure, tissue-distribution, and functions of tachykinins and their receptors. Curr. Drug Targets 2006, 7, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Klassert, T.E.; Pinto, F.; Hernández, M.; Candenas, M.L.; Hernández, M.C.; Abreu, J.; Almeida, T.A. Differential expression of neurokinin B and hemokinin-1 in human immune cells. J. Neuroimmunol. 2008, 196, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Stumm, R.; Culmsee, C.; Schafer, M.K.; Krieglstein, J.; Weihe, E. Adaptive plasticity in tachykinin and tachykinin receptor expression after focal cerebral ischemia is differentially linked to gabaergic and glutamatergic cerebrocortical circuits and cerebrovenular endothelium. J. Neurosci. 2001, 21, 798–811. [Google Scholar] [PubMed]
- Turner, R.J.; Blumbergs, P.C.; Sims, N.R.; Helps, S.C.; Rodgers, K.M.; Vink, R. Increased substance P immunoreactivity and edema formation following reversible ischemic stroke. Acta Neurochir. Suppl. 2006, 96, 263–266. [Google Scholar] [PubMed]
- Van Bree, L.; Zhang, F.; Schiffmann, S.N.; Halleux, P.; Mailleux, P.; Vanderhaeghen, J.J. Homolateral cerebrocortical changes in neuropeptide and receptor expression after minimal cortical infarction. Neuroscience 1995, 69, 847–858. [Google Scholar] [CrossRef]
- Nishimura, A.; Takashima, S.; Mito, T.; Becker, L.E. Aberrant distribution of tyrosine hydroxylase and substance P in infants with brain-stem infarction. Acta Paediatr. Jpn. 1994, 36, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Bruno, G.; Tega, F.; Bruno, A.; Graf, U.; Corelli, F.; Molfetta, R.; Barucco, M. The role of substance P in cerebral ischemia. Int. J. Immunopathol. Pharmacol. 2003, 16, 67–72. [Google Scholar] [PubMed]
- Lorente, L.; Martín, M.M.; Almeida, T.; Hernández, M.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A. Serum substance P levels are associated with severity and mortality in patients with severe traumatic brain injury. Crit. Care 2015, 19, 192. [Google Scholar] [CrossRef] [PubMed]
- Marriott, D.R.; Wilkin, G.P.; Wood, J.N. Substance P-induced release of prostaglandins from astrocytes: Regional specialisation and correlation with phosphoinositol metabolism. J. Neurochem. 1991, 56, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Palma, C.; Minghetti, L.; Astolfi, M.; Ambrosini, E.; Silberstein, F.C.; Manzini, S.; Levi, G.; Aloisi, F. Functional characterization of substance P receptors on cultured human spinal cord astrocytes: Synergism of substance P with cytokines in inducing interleukin-6 and prostaglandin E2 production. Glia 1997, 21, 183–193. [Google Scholar] [CrossRef]
- Persson, M.G.; Hedqvist, P.; Gustafsson, L.E. Nerve-induced tachykinin-mediated vasodilation in skeletal muscle is dependent on nitric oxide formation. Eur. J. Pharmacol. 1991, 205, 295–301. [Google Scholar] [CrossRef]
- Lotz, M.; Vaughan, J.H.; Carson, D.A. Effect of neuropeptides on production of inflammatory cytokines by human monocytes. Science 1988, 241, 1218–1221. [Google Scholar] [CrossRef] [PubMed]
- Laurenzi, M.A.; Persson, M.A.; Dalsgaard, C.J.; Haegerstrand, A. The neuropeptide substance P stimulates production of interleukin 1 in human blood monocytes: Activated cells are preferentially influenced by the neuropeptide. Scand. J. Immunol. 1990, 31, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Ansel, J.C.; Brown, J.R.; Payan, D.G.; Brown, M.A. Substance P selectively activates TNF-alpha gene expression in murine mast cells. J. Immunol. 1993, 150, 4478–4485. [Google Scholar] [PubMed]
- Yamaguchi, M.; Kojima, T.; Kanekawa, M.; Aihara, N.; Nogimura, A.; Kasai, K. Neuropeptides stimulate production of interleukin-1β, interleukin-6, and tumor necrosis factor-α in human dental pulp cells. Inflamm. Res. 2004, 53, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Donkin, J.J.; Nimmo, A.J.; Cernak, I.; Blumbergs, P.C.; Vink, R. Substance P is associated with the development of brain edema and functional deficits after traumatic braininjury. J. Cereb. Blood Flow Metab. 2009, 29, 1388–1398. [Google Scholar] [CrossRef] [PubMed]
- Gabrielian, L.; Helps, S.C.; Thornton, E.; Turner, R.J.; Leonard, A.V.; Vink, R. Substance P antagonists as a novel intervention for brain edema and raised intracranial pressure. Acta Neurochir. Suppl. 2013, 118, 201–204. [Google Scholar] [PubMed]
- Cyrino, L.A.; Cardoso, R.C.; Hackl, L.P.; Nicolau, M. Effect of quercetin on plasma extravasation in rat CNS and dura mater by ACE and NEP inhibition. Phytother. Res. 2002, 16, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Nimmo, A.J.; Cernak, I.; Heath, D.L.; Hu, X.; Bennett, C.J.; Vink, R. Neurogenic inflammation is associated with development of edema and functional deficits following traumatic brain injury in rats. Neuropeptides 2004, 38, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Vink, R.; Young, A.; Bennett, C.J.; Hu, X.; Connor, C.O.; Cernak, I.; Nimmo, A.J. Neuropeptide release influences brain edema formation after diffuse traumatic brain injury. Acta Neurochir. Suppl. 2003, 86, 257–260. [Google Scholar] [PubMed]
- Graham, G.J.; Stevens, J.M.; Page, N.M.; Grant, A.D.; Brain, S.D.; Lowry, P.J.; Gibbins, J.M. Tachykinins regulate the function of platelets. Blood 2004, 104, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Tucker, K.L.; Sage, T.; Kaiser, W.J.; Barrett, N.E.; Lowry, P.J.; Zimmer, A.; Hunt, S.P.; Emerson, M.; Gibbins, J.M. Peripheral tachykinins and the neurokinin receptor NK1 are required for platelet thrombus formation. Blood 2008, 111, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.J.; Helps, S.C.; Thornton, E.; Vink, R. A substance P antagonist improves outcome when administered 4 h after onset of ischaemic stroke. Brain Res. 2011, 1393, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.J.; Vink, R. NK1 tachykinin receptor treatment is superior to capsaicin pre-treatment in improving functional outcome following acute ischemic stroke. Neuropeptides 2014, 48, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Cheng, G.; Huang, X.; Li, K.; Cao, X. Neurokinin-1 receptor antagonist SR140333: A novel type of drug to treat cerebral ischemia. Neuroreport 1997, 8, 2117–2119. [Google Scholar] [CrossRef] [PubMed]
- Khatibi, N.H.; Jadhav, V.; Charles, S.; Chiu, J.; Buchholz, J.; Tang, J.; Zhang, J.H. Capsaicin pre-treatment provides neurovascular protection against neonatal hypoxic-ischemic brain injury in rats. Acta Neurochir. Suppl. 2011, 11, 225–230. [Google Scholar]
- Lorente, L.; Martín, M.M.; Almeida, T.; Hernández, M.; Ferreres, J.; Solé-Violán, J.; Labarta, L.; Díaz, C.; Jiménez, A. Association between serum substance P levels and mortality in patients with severe sepsis. J. Crit. Care 2015, 3, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Kincy-Cain, T.; Bost, K.L. Increased susceptibility of mice to Salmonella infection following in vivo treatment with the substance P antagonist, spantide II. J. Immunol. 1996, 157, 255–264. [Google Scholar] [PubMed]
- Lighvani, S.; Huang, X.; Trivedi, P.P.; Swanborg, R.H.; Hazlett, L.D. Substance P regulates natural killer cell interferon-γ production and resistance to Pseudomonas aeruginosa infection. Eur. J. Immunol. 2005, 35, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Verdrengh, M.; Tarkowski, A. The impact of substance P signalling on the development of experimental staphylococcal sepsis and arthritis. Scand. J. Immunol. 2008, 67, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessement of coma and impaired conciousness. A practical scale. Lancet 1974, 2, 1–84. [Google Scholar]
- Lorente, L.; Martín, M.M.; Abreu-González, P.; Ramos, L.; Argueso, M.; Solé-Violán, J.; Riaño-Ruiz, M.; Jiménez, A. Serum malondialdehyde levels in patients with malignant middle cerebral artery infarction are associated with mortality. PLoS ONE 2015, 10, e0125893. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; González-Rivero, A.F.; Ramos, L.; Argueso, A.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A.; Borreguero-León, J.M. Association between Serum Soluble CD154 Levels and Mortality in Patients with Malignant Middle Cerebral Artery Infarction. Int. J. Mol. Sci. 2015, 16, 12147–12158. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Ramos, L.; Cáceres, J.J.; Solé-Violán, J.; Argueso, M.; Jiménez, A.; Borreguero-León, J.M.; Orbe, J.; Rodríguez, J.A.; et al. Serum tissue inhibitor of matrix metalloproteinase-1 levels are associated with mortality in patients with malignant middle cerebral artery infarction. BMC Neurol. 2015, 15, 111. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Pérez-Cejas, A.; Abreu-González, P.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A. Association between total antioxidant capacity and mortality in ischemic stroke patients. Ann. Intensive Care 2016, 6, 39. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P. Advantages to transforming the receiver operating characteristic (ROC) curve into likelihood ratio co-ordinates. Stat. Med. 2004, 23, 2257–2266. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Survivors (n = 30) | Non-Survivors (n = 31) | p Value |
|---|---|---|---|
| TNF-alpha (pg/mL)—median (p. 25–75) | 9.5 (9.1–12.1) | 13.0 (10.7–14.4) | 0.01 |
| Temperature (°C)—median (p. 25–75) | 36.4 (35.6–37.0) | 37.0 (36.0–37.4) | 0.15 |
| Temperature (°C)—median (p. 25–75) | 36.4 (35.6–37.0) | 37.0 (36.0–37.4) | 0.15 |
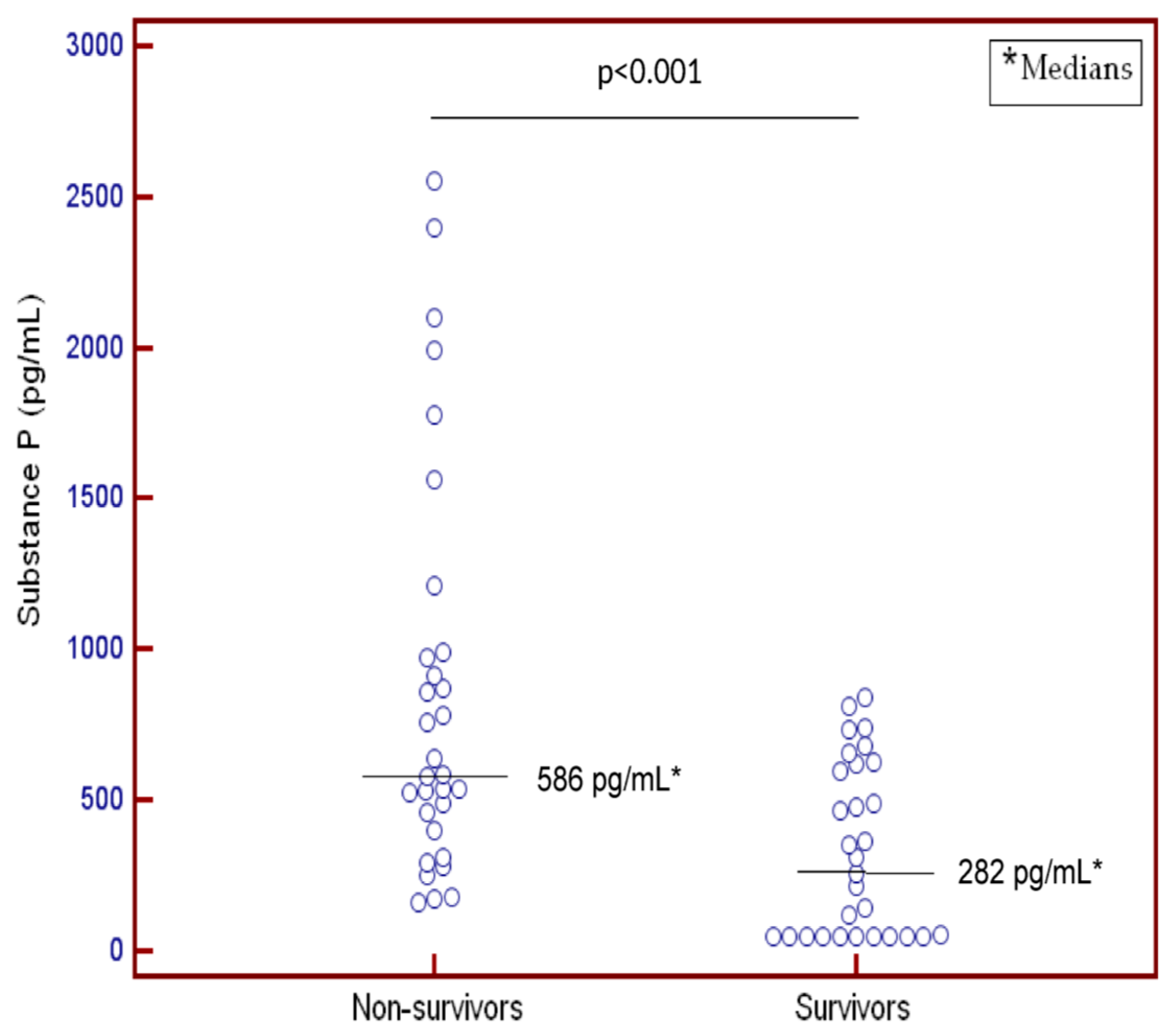
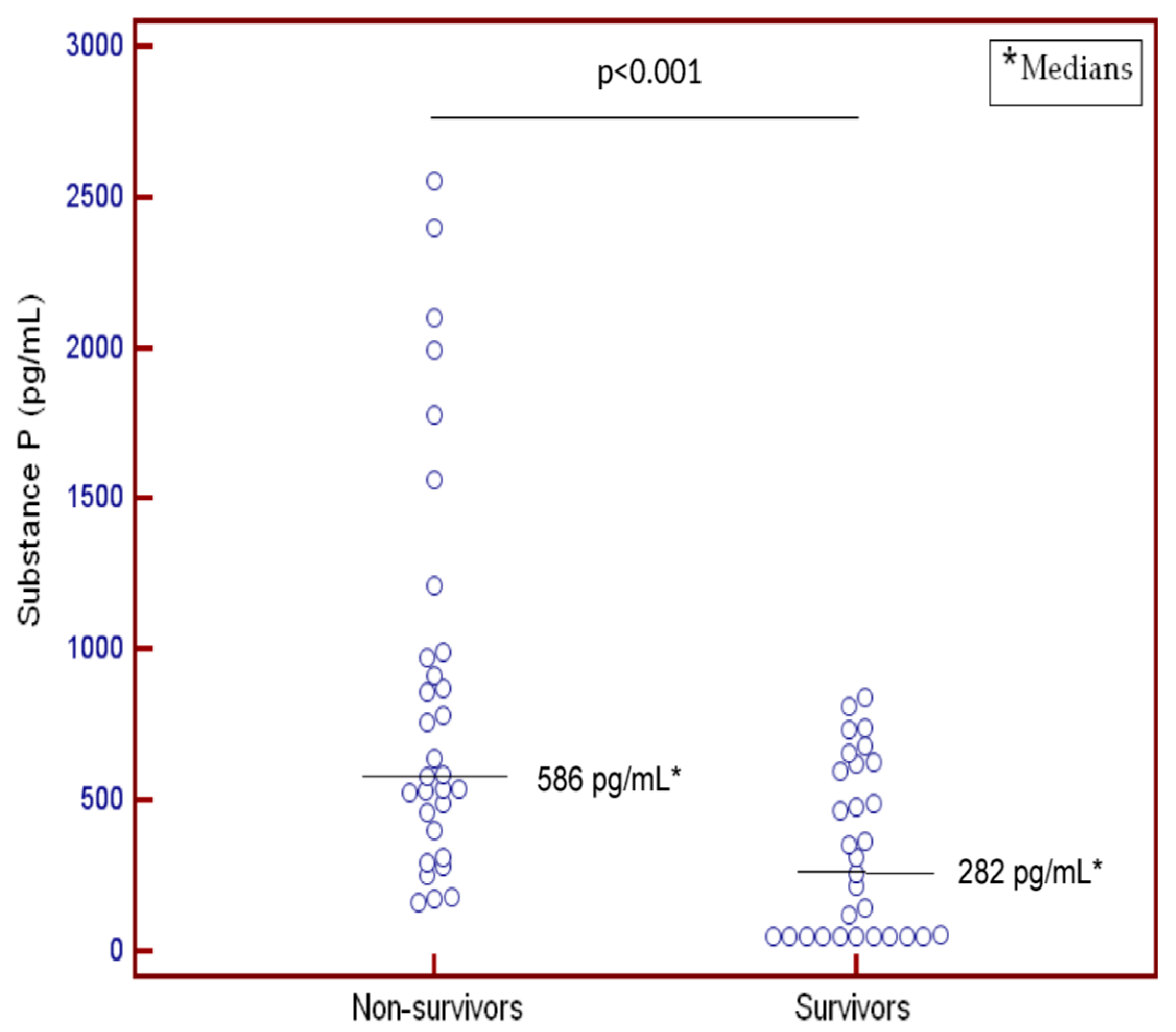
| Substance P (pg/mL)—median (p. 25–75) | 282 (50–620) | 586 (397–990) | <0.001 |
| Sodium (mEq/L)—median (p. 25–75) | 139 (136–145) | 140 (139–144) | 0.42 |
| Platelets—median × 103/mm3 (p. 25–75) | 218 (171–283) | 165 (128–209) | 0.003 |
| PaO2 (mmHg)—median (p. 25–75) | 130 (101–194) | 114 (86–153) | 0.38 |
| PaO2/FiO2 ratio—median (p. 25–75) | 282 (198–369) | 242 (181–325) | 0.17 |
| Leukocytes—median × 103/mm3 (p. 25–75) | 12.8 (9.6–17.1) | 13.8 (9.3–18.9) | 0.67 |
| Lactic acid (mmol/L)—median (p. 25–75) | 1.30 (0.90–1.70) | 1.45 (1.00–2.63) | 0.18 |
| INR—median (p. 25–75) | 1.09 (1.01–1.20) | 1.20 (1.04–1.31) | 0.11 |
| Hemoglobin (g/dL)—median (p. 25–75) | 12.2 (11.4–14.8) | 13.7 (11.0–15.0) | 0.95 |
| Glycemia (g/dL)—median (p. 25–75) | 128 (101–170) | 135 (100–159) | 0.93 |
| GCS score—median (p. 25–75) | 7 (6–8) | 6 (3–8) | 0.04 |
| Gender female—n (%) | 13 (43.3) | 11 (35.5) | 0.61 |
| Fibrinogen (mg/dL)—median (p. 25–75) | 443 (355–518) | 417 (323–622) | 0.86 |
| Decompressive craniectomy—n (%) | 8 (26.7) | 5 (16.1) | 0.36 |
| Creatinine (mg/dL)—median (p. 25–75) | 0.80 (0.60–1.13) | 1.00 (0.79–1.23) | 0.09 |
| Bilirubin (mg/dL)—median (p. 25–75) | 0.65 (0.40–0.93) | 0.70 (0.35–1.13) | 0.94 |
| aPTT (seconds)—median (p. 25–75) | 28 (26–30) | 27 (26–33) | 0.75 |
| APACHE-II score—median (p. 25–75) | 20 (16–25) | 22 (19–27) | 0.20 |
| Age (years)—median (p. 25–75) | 58 (47–67) | 64 (53–70) | 0.07 |
| Variable | Odds Ratio | 95% Confidence Interval | p |
|---|---|---|---|
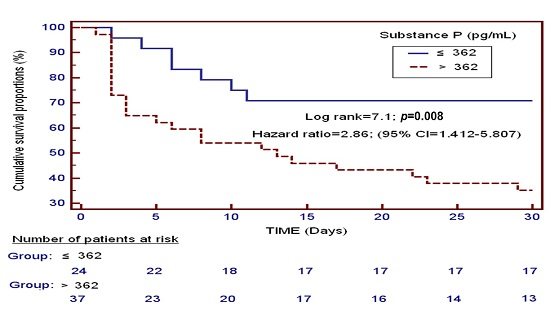
| Serum levels of substance P > 362 pg/mL | 5.33 | 1.541–18.470 | 0.008 |
| Glasgow Coma Scale | 0.72 | 0.529–0.990 | 0.04 |
| Age (years) | 1.03 | 0.986–1.082 | 0.17 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorente, L.; Martín, M.M.; Almeida, T.; Pérez-Cejas, A.; Ramos, L.; Argueso, M.; Riaño-Ruiz, M.; Solé-Violán, J.; Hernández, M. Serum Levels of Substance P and Mortality in Patients with a Severe Acute Ischemic Stroke. Int. J. Mol. Sci. 2016, 17, 991. https://doi.org/10.3390/ijms17060991
Lorente L, Martín MM, Almeida T, Pérez-Cejas A, Ramos L, Argueso M, Riaño-Ruiz M, Solé-Violán J, Hernández M. Serum Levels of Substance P and Mortality in Patients with a Severe Acute Ischemic Stroke. International Journal of Molecular Sciences. 2016; 17(6):991. https://doi.org/10.3390/ijms17060991
Chicago/Turabian StyleLorente, Leonardo, María M. Martín, Teresa Almeida, Antonia Pérez-Cejas, Luis Ramos, Mónica Argueso, Marta Riaño-Ruiz, Jordi Solé-Violán, and Mariano Hernández. 2016. "Serum Levels of Substance P and Mortality in Patients with a Severe Acute Ischemic Stroke" International Journal of Molecular Sciences 17, no. 6: 991. https://doi.org/10.3390/ijms17060991
APA StyleLorente, L., Martín, M. M., Almeida, T., Pérez-Cejas, A., Ramos, L., Argueso, M., Riaño-Ruiz, M., Solé-Violán, J., & Hernández, M. (2016). Serum Levels of Substance P and Mortality in Patients with a Severe Acute Ischemic Stroke. International Journal of Molecular Sciences, 17(6), 991. https://doi.org/10.3390/ijms17060991