
Simultaneous Determination of Orelabrutinib, Zanubrutinib, Ibrutinib and Its Active Metabolite in Human Plasma Using LC-MS/MS

Abstract
1. Introduction
2. Results and Discussion
2.1. Method Development
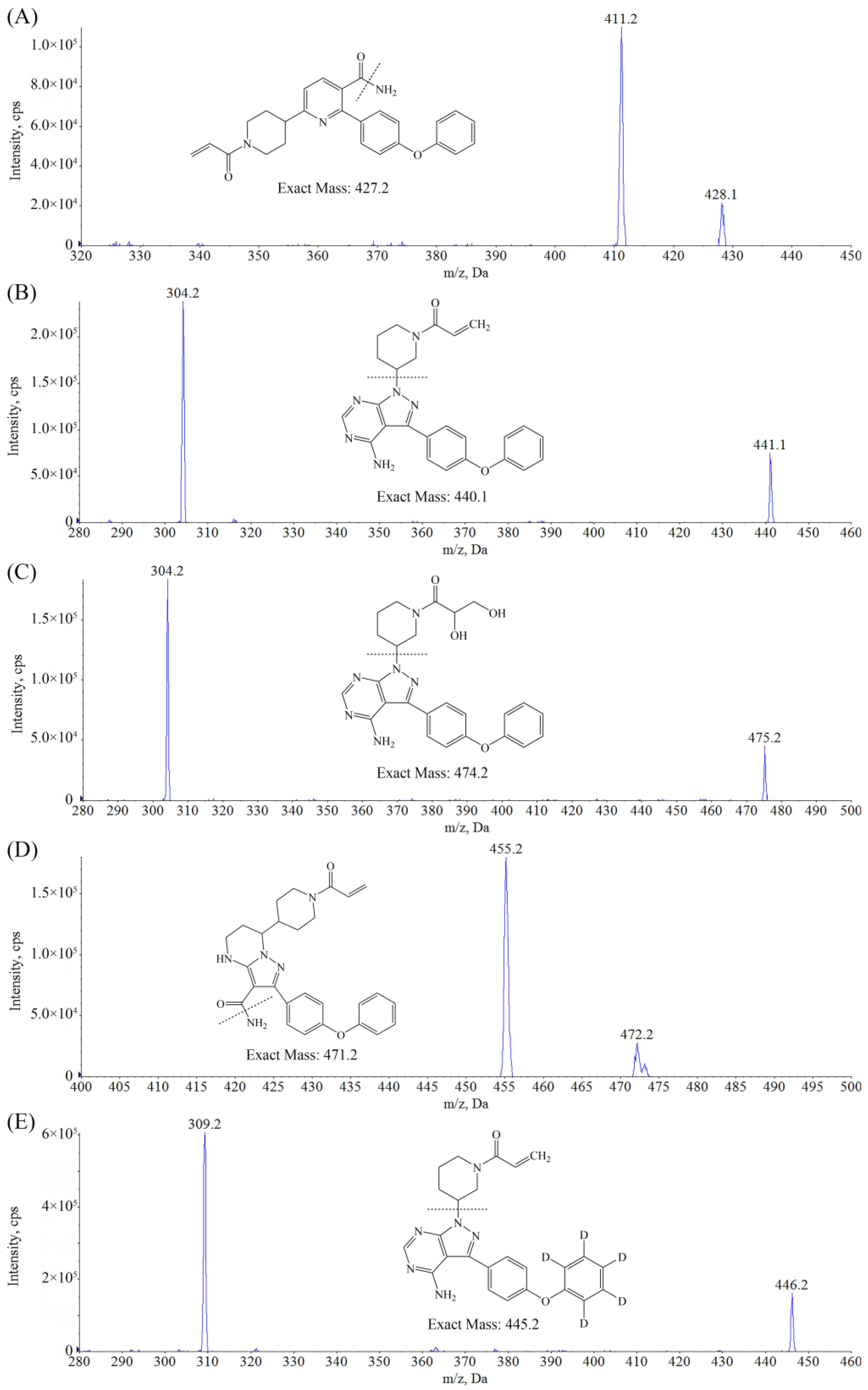
2.1.1. Optimization of Mass Spectrometry Conditions
2.1.2. Optimization of Chromatography Conditions
2.1.3. Sample Preparation
2.2. Method Validation
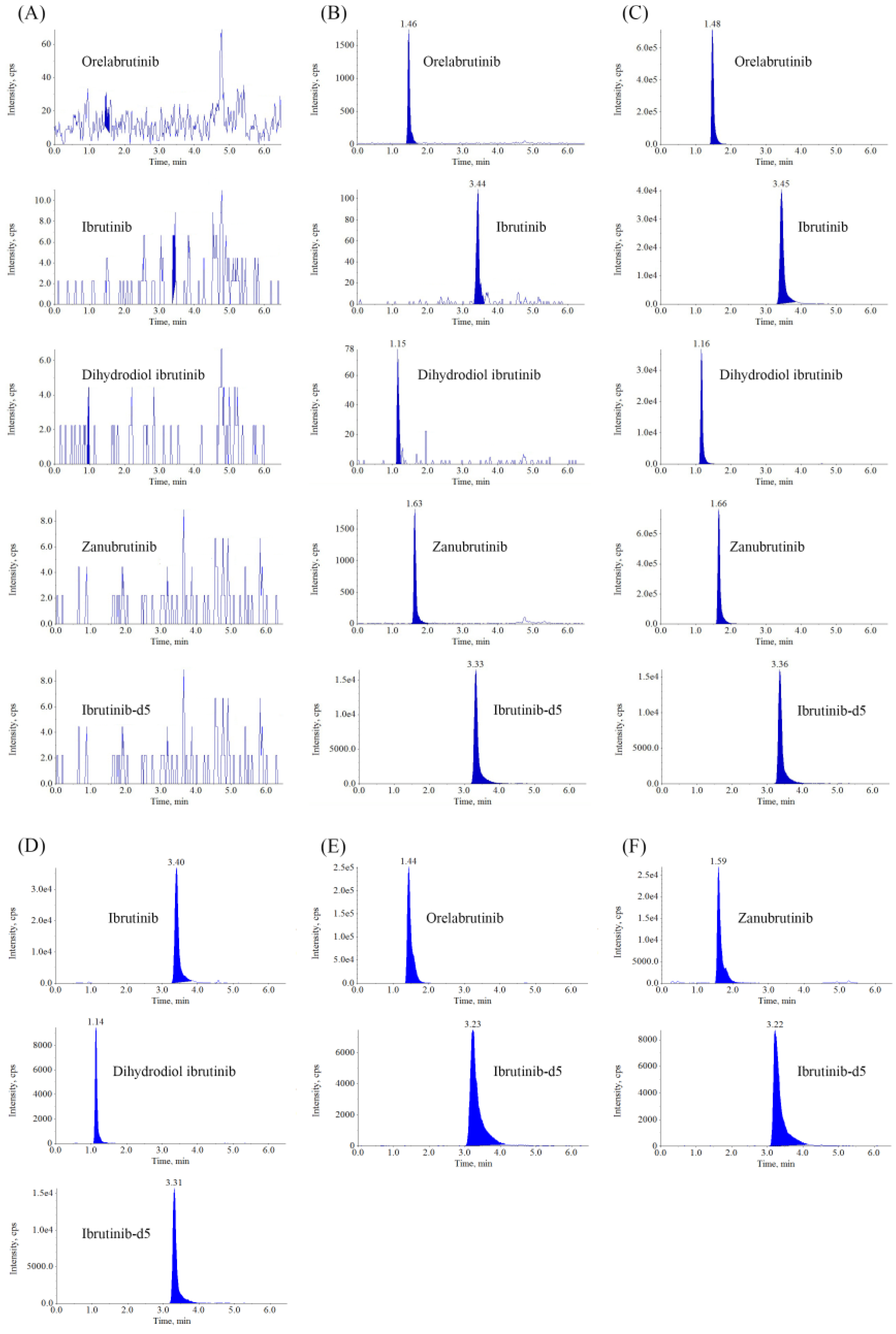
2.2.1. Selectivity
2.2.2. Matrix Effect and Recovery
2.2.3. Linearity, Lower Limit of Quantitation, Precision and Accuracy
2.2.4. Carryover
2.2.5. Stability
2.2.6. Dilution Integrity
2.3. Application
3. Materials and Methods
3.1. Chemicals and Reagents
3.2. Analytical Equipment
3.3. Chromatographic and Mass Spectrometric Conditions
3.4. Stock Solutions and Working Solutions Preparation
3.5. Calibration Standards and QC Samples Preparation
3.6. Plasma Sample Preparation
3.7. Validation of the Method
3.7.1. Selectivity
3.7.2. Linearity and Lower Limit of Quantitation
3.7.3. Precision and Accuracy
3.7.4. Extraction Recovery and Matrix Effect
3.7.5. Carryover
3.7.6. Stability
3.7.7. Dilution Integrity
3.8. Application
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moore, D.C.; Thompson, D. A Review of the Bruton Tyrosine Kinase Inhibitors in B-Cell Malignancies. J. Adv. Pract. Oncol. 2021, 12, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Shirley, M. Bruton Tyrosine Kinase Inhibitors in B-Cell Malignancies: Their Use and Differential Features. Targ. Oncol. 2022, 17, 69–84. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Tang, H.; Wu, J.; Li, J.; Miao, Y. Targeting Bruton Tyrosine Kinase Using Non-Covalent Inhibitors in B Cell Malignancies. J. Hematol. Oncol. 2021, 14, 40. [Google Scholar] [CrossRef]
- Robak, T.; Witkowska, M.; Smolewski, P. The Role of Bruton’s Kinase Inhibitors in Chronic Lymphocytic Leukemia: Current Status and Future Directions. Cancers 2022, 14, 771. [Google Scholar] [CrossRef]
- Liu, J.; Chen, C.; Wang, D.; Zhang, J.; Zhang, T. Emerging small-molecule inhibitors of the Bruton’s tyrosine kinase (BTK): Current development. Eur. J. Med. Chem. 2021, 217, 113329. [Google Scholar] [CrossRef] [PubMed]
- Gaballa, S.; Pinilla-Ibarz, J. BTK Inhibitors in Chronic Lymphocytic Leukemia. Curr. Hematol. Malig. Rep. 2021, 16, 422–432. [Google Scholar] [CrossRef]
- Shaw, M.L. Second-Generation BTK Inhibitors Hit the Treatment Bullseye with Fewer off-Target Effects. Am. J. Manag. Care 2020, 26, SP226–SP227. [Google Scholar] [CrossRef]
- Ahn, I.E.; Brown, J.R. Targeting Bruton’s Tyrosine Kinase in CLL. Front. Immunol. 2021, 12, 687458. [Google Scholar] [CrossRef]
- Dhillon, S. Orelabrutinib: First Approval. Drugs 2021, 81, 503–507. [Google Scholar] [CrossRef]
- Estupiñán, H.Y.; Berglöf, A.; Zain, R.; Smith, C.I.E. Comparative Analysis of BTK Inhibitors and Mechanisms Underlying Adverse Effects. Front. Cell Dev. Biol. 2021, 9, 630942. [Google Scholar] [CrossRef]
- Cho, H.J.; Baek, D.W.; Kim, J.; Lee, J.M.; Moon, J.H.; Sohn, S.K. Keeping a balance in chronic lymphocytic leukemia (CLL) patients taking ibrutinib: Ibrutinib-associated adverse events and their management based on drug interactions. Expert Rev. Hematol. 2021, 14, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.X.; Jin, J.; Fu, C.C.; Yi, S.H.; Zhao, W.L.; Sun, Z.M.; Yang, W.; Li, D.J.; Cui, G.H.; Hu, J.D.; et al. Evaluation of orelabrutinib monotherapy in patients with relapsed or refractory Waldenström’s macroglobulinemia in a single-arm, multicenter, open-label, phase 2 study. EClinicalMedicine 2022, 52, 101682. [Google Scholar] [CrossRef]
- Pagano, L.; Akova, M.; Dimopoulos, G.; Herbrecht, R.; Drgona, L.; Blijlevens, N. Risk Assessment and Prognostic Factors for Mould-Related Diseases in Immunocompromised Patients. J. Antimicrob. Chemother. 2011, 66, i5–i14. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.Y.; Lee, D.G.; Yeh, S.P.; Bhurani, D.; Khanh, B.Q.; Low, C.Y.; Norasetthada, L.; Chan, T.; Kwong, Y.L.; Vaid, A.K.; et al. Epidemiology of Invasive Fungal Diseases among Patients with Haematological Disorders in the Asia-Pacific: A Prospective Observational Study. Clin. Microbiol. Infect. 2015, 21, 594.e7–594.e11. [Google Scholar] [CrossRef] [PubMed]
- de Jong, J.; Skee, D.; Murphy, J.; Sukbuntherng, J.; Hellemans, P.; Smit, J.; de Vries, R.; Jiao, J.J.; Snoeys, J.; Mannaert, E. Effect of CYP3A Perpetrators on Ibrutinib Exposure in Healthy Participants. Pharmacol. Res. Perspect. 2015, 3, e00156. [Google Scholar] [CrossRef]
- Mukai, Y.; Yoshida, Y.; Yoshida, T.; Kondo, T.; Inotsume, N.; Toda, T. Simultaneous Quantification of BCR-ABL and Bruton Tyrosine Kinase Inhibitors in Dried Plasma Spots and Its Application to Clinical Sample Analysis. Ther. Drug Monit. 2021, 43, 386–393. [Google Scholar] [CrossRef]
- Hirasawa, T.; Kikuchi, M.; Shigeta, K.; Takasaki, S.; Sato, Y.; Sato, T.; Ogura, J.; Onodera, K.; Fukuhara, N.; Onishi, Y.; et al. High-Throughput Liquid Chromatography/Electrospray Ionization-Tandem Mass Spectrometry Method Using in-Source Collision-Induced Dissociation for Simultaneous Quantification of Imatinib, Dasatinib, Bosutinib, Nilotinib, and Ibrutinib in Human Plasma. Biomed. Chromatogr. 2021, 35, e5124. [Google Scholar] [CrossRef]
- Verougstraete, N.; Stove, V.; Verstraete, A.G.; Stove, C. Quantification of Eight Hematological Tyrosine Kinase Inhibitors in Both Plasma and Whole Blood by a Validated LC-MS/MS Method. Talanta 2021, 226, 122140. [Google Scholar] [CrossRef]
- Écsiová, D.; Šimkovič, M.; Uher, M.; Hroch, M. High-Throughput Salting-out Assisted Liquid-Liquid Extraction Using a 3D Printed Device and Its Application in the Quantification of Ibrutinib and Its Metabolite PCI-45227 in Human Serum. J. Pharm. Biomed. Anal. 2022, 219, 114923. [Google Scholar] [CrossRef]
- Mukai, Y.; Yoshida, T.; Kondo, T.; Inotsume, N.; Toda, T. Novel High-Performance Liquid Chromatography-Tandem Mass Spectrometry Method for Simultaneous Quantification of BCR-ABL and Bruton’s Tyrosine Kinase Inhibitors and Their Three Active Metabolites in Human Plasma. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2020, 1137, 121928. [Google Scholar] [CrossRef]
- Koller, D.; Vaitsekhovich, V.; Mba, C.; Steegmann, J.L.; Zubiaur, P.; Abad-Santos, F.; Wojnicz, A. Effective Quantification of 11 Tyrosine Kinase Inhibitors and Caffeine in Human Plasma by Validated LC-MS/MS Method with Potent Phospholipids Clean-up Procedure. Application to Therapeutic Drug Monitoring. Talanta 2020, 208, 120450. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration Bioanalytical Method Validation Guidance for Industry. Available online: https://www.fda.gov/downloads/drugs/guidances/ucm070107.pdf (accessed on 25 October 2022).



{kind=link}
{kind=link}
| Analytes | Precursor Ion (m/z) | Product Ion (m/z) | DP (V) | EP (V) | CE (V) | CXP (V) |
|---|---|---|---|---|---|---|
| IBR | 441.2 | 304.2 | 109 | 7 | 40 | 15 |
| DIH | 475.2 | 304.2 | 108 | 9 | 43 | 15 |
| ORE | 428.1 | 411.2 | 104 | 8 | 29 | 15 |
| ZAN | 472.2 | 455.2 | 110 | 10 | 28 | 15 |
| IBR-d5 | 446.2 | 309.2 | 109 | 7 | 40 | 15 |
| Compound | Conc. Spiked (ng/mL) | Matrix Effect | Recovery |
|---|---|---|---|
| Mean ± SD (%) | Mean ± SD (%) | ||
| IBR | 1.00 | 102.7 ± 4.3 | 92.1 ± 4.7 |
| 10.0 | — | 98.3 ± 3.4 | |
| 40.0 | — | 92.6 ± 2.6 | |
| 160 | 98.8 ± 2.2 | 92.8 ± 7.4 | |
| DIH | 1.00 | 107.4 ± 4.6 | 99.2 ± 18.2 |
| 10.0 | — | 94.9 ± 5.2 | |
| 40.0 | — | 96.4 ± 7.1 | |
| 160 | 106.8 ± 2.8 | 91.1 ± 5.3 | |
| ORE | 1.00 | 100.5 ± 3.3 | 92.9 ± 3.8 |
| 2.50 | — | 96.2 ± 2.3 | |
| 25.0 | — | 95.3 ± 5.3 | |
| 100 | 97.6 ± 2.7 | 94.8 ± 5.6 | |
| ZAN | 400 | 99.5 ± 1.6 | 94.5 ± 4.4 |
| 25.0 | — | 97.9 ± 2.8 | |
| 100 | — | 96.4 ± 5.6 | |
| 400 | 100.5 ± 2.7 | 94.8 ± 6.9 |
| Analytes | Linear Range (ng/mL) | Regression Equation | Correlation Coefficient (r2) |
|---|---|---|---|
| IBR | 0.400–200 | f = 0.0119 × C + 0.000401 | 0.9986 |
| DIH | 0.400–200 | f = 0.00611 × C + 0.0000178 | 0.9982 |
| ORE | 1.00–500 | f = 0.0556 × C + 0.000915 | 0.9982 |
| ZAN | 2.00–1000 | f = 0.0320 × C + 0.000852 | 0.9988 |
| Analytes | Conc. Spiked (ng/mL) | Conc. Found (ng/mL) | Intra-Run | Inter-Run | ||
|---|---|---|---|---|---|---|
| RSD (%) | RE (%) | RSD (%) | RE (%) | |||
| IBR | 0.400 | 0.401 | 12.2 | 0.2 | 13.0 | 1.7 |
| 1.00 | 1.02 | 6.4 | 1.6 | 5.0 | −1.2 | |
| 10.0 | 9.82 | 3.8 | −1.8 | 3.0 | −5.3 | |
| 40.0 | 39.7 | 2.5 | −0.7 | 2.6 | −1.0 | |
| 160 | 159 | 2.6 | −0.2 | 2.2 | −2.4 | |
| DIH | 0.400 | 0.393 | 12.2 | −1.4 | 8.6 | −2.3 |
| 1.00 | 1.01 | 6.9 | 1.2 | 6.5 | −1.1 | |
| 10.0 | 10.0 | 3.6 | 0.3 | 3.4 | 0.0 | |
| 40.0 | 39.9 | 4.0 | −0.2 | 4.1 | −1.0 | |
| 160 | 158 | 5.1 | −1.1 | 4.4 | −4.8 | |
| ORE | 1.00 | 0.987 | 5.3 | −1.3 | 4.2 | −1.9 |
| 2.50 | 2.62 | 3.1 | 4.6 | 2.7 | 2.6 | |
| 25.0 | 25.6 | 3.6 | 2.3 | 3.0 | −0.2 | |
| 100 | 102 | 2.8 | 1.9 | 2.8 | 2.0 | |
| 400 | 389 | 2.3 | −2.7 | 2.3 | −3.5 | |
| ZAN | 2.00 | 1.96 | 4.5 | −2.3 | 4.8 | −2.1 |
| 5.00 | 5.28 | 2.4 | 5.7 | 2.2 | 4.2 | |
| 50.0 | 50.9 | 2.9 | 1.3 | 3.0 | 0.1 | |
| 200 | 202 | 2.3 | 0.8 | 2.3 | 1.4 | |
| 800 | 773 | 2.8 | −3.4 | 2.8 | −4.6 | |
| Stability | Storage Condition | IBR | DIH | ORE | ZAN | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group (ng/mL) | RSD (%) | RE (%) | Group (ng/mL) | RSD (%) | RE (%) | Group (ng/mL) | RSD (%) | RE (%) | Group (ng/mL) | RSD (%) | RE (%) | ||
| Autosampler stability | (10 °C, 24 h) | 1.00 160 | 8.0 2.4 | −4.5 −1.7 | 1.00 160 | 12.1 5.5 | 1.0 −3.3 | 2.50 400 | 3.5 3.3 | 4.7 −7.5 | 5.00 800 | 2.3 2.0 | 0.1 −6.9 |
| Ice bath stability | (0 °C, 2 h) | 1.00 160 | 4.1 1.7 | −5.8 −1.9 | 1.00 160 | 11.2 3.3 | 1.5 −2.7 | 2.50 400 | 7.6 2.6 | 4.1 −3.2 | 5.00 800 | 5.0 3.1 | 5.5 1.5 |
| Benchtop stability | (20 °C, 6 h) | 1.00 160 | 5.3 4.0 | −5.8 −1.3 | 1.00 160 | 2.8 2.8 | 8.7 6.0 | 2.50 400 | 5.4 3.6 | −2.8 1.1 | 5.00 800 | 1.5 4.2 | 1.8 0.6 |
| Freeze-thaw stability | (−40 °C, 3 cycles) | 1.00 160 | 6.5 3.7 | −0.9 −2.9 | 1.00 160 | 4.1 4.8 | 4.2 4.4 | 2.50 400 | 6.8 6.6 | 3.9 −3.0 | 5.00 800 | 6.9 4.9 | −1.4 −2.3 |
| Freeze-thaw stability | (−80 °C, 3 cycles) | 1.00 160 | 7.3 4.4 | 1.6 0.0 | 1.00 160 | 3.0 6.7 | 7.7 −1.0 | 2.50 400 | 5.8 1.7 | 5.7 −5.8 | 5.00 800 | 5.6 4.5 | 1.5 −2.5 |
| Long-term | (−40 °C, 30 d) | 1.00 | −8.5 | 3.9 | 1.00 | 8.0 | 3.3 | 2.50 | 1.1 | 7.9 | 5.00 | 5.2 | 4.7 |
| stability | 160 | −10.2 | 2.6 | 160 | 0.6 | 1.1 | 400 | −7.7 | 6.0 | 800 | −8.1 | 5.1 | |
| Long-term stability | (−80 °C, 30 d) | 1.00 | −3.4 | 5.0 | 1.00 | 0.0 | 8.0 | 2.50 | 6.1 | 4.7 | 5.00 | 7.5 | 7.7 |
| 160 | −7.3 | 2.7 | 160 | −1.0 | 4.3 | 400 | −2.0 | 5.1 | 800 | −3.9 | 5.5 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, L.-N.; Zhao, Y.; Qian, Z.-Y.; Chen, X.-L.; Ma, H.; Guo, Y.-J.; Shen, H.; Wang, Y.-Q. Simultaneous Determination of Orelabrutinib, Zanubrutinib, Ibrutinib and Its Active Metabolite in Human Plasma Using LC-MS/MS. Molecules 2023, 28, 1205. https://doi.org/10.3390/molecules28031205
Sun L-N, Zhao Y, Qian Z-Y, Chen X-L, Ma H, Guo Y-J, Shen H, Wang Y-Q. Simultaneous Determination of Orelabrutinib, Zanubrutinib, Ibrutinib and Its Active Metabolite in Human Plasma Using LC-MS/MS. Molecules. 2023; 28(3):1205. https://doi.org/10.3390/molecules28031205
Chicago/Turabian StyleSun, Lu-Ning, Yang Zhao, Zhou-Yi Qian, Xiang-Long Chen, Hong Ma, Yu-Jiao Guo, Hao Shen, and Yong-Qing Wang. 2023. "Simultaneous Determination of Orelabrutinib, Zanubrutinib, Ibrutinib and Its Active Metabolite in Human Plasma Using LC-MS/MS" Molecules 28, no. 3: 1205. https://doi.org/10.3390/molecules28031205
APA StyleSun, L.-N., Zhao, Y., Qian, Z.-Y., Chen, X.-L., Ma, H., Guo, Y.-J., Shen, H., & Wang, Y.-Q. (2023). Simultaneous Determination of Orelabrutinib, Zanubrutinib, Ibrutinib and Its Active Metabolite in Human Plasma Using LC-MS/MS. Molecules, 28(3), 1205. https://doi.org/10.3390/molecules28031205