

Phytocannabinoids in the Pharmacotherapy of Psoriasis


Abstract
1. Introduction
2. Search Strategy
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Literature Screening
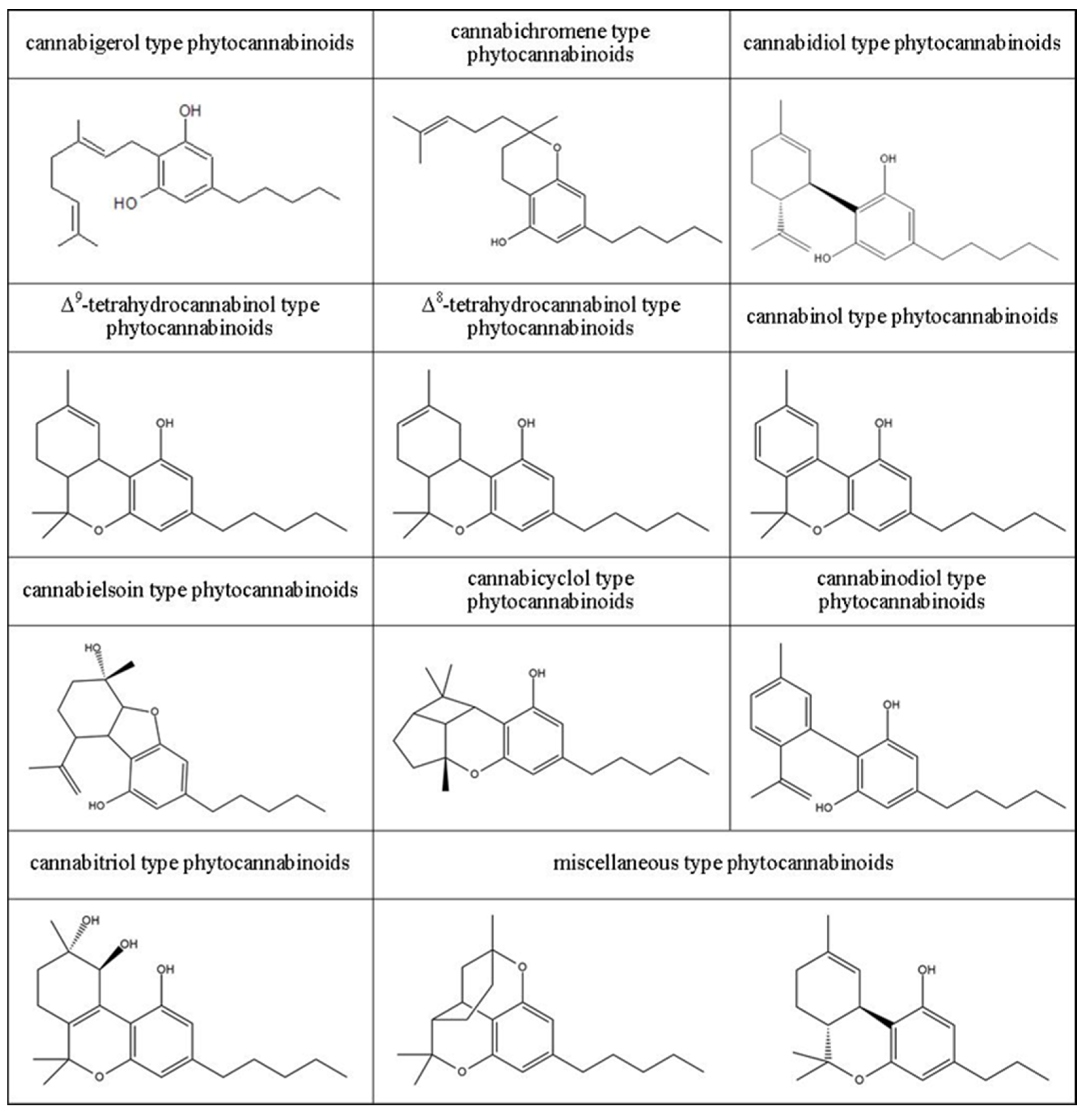
3. Classification of Phytocannabinoids
4. Biological Activity of Phytocannabinoids
5. Effect of Phytocannabinoids on Skin
5.1. Effect of Phytocannabinoids on the Metabolism of Healthy Skin Cells as Well as Healthy Skin Exposed to Physicochemical and Biological Factors—In Vitro Examinations
5.2. Effect of Phytocannabinoids on the Metabolism of Healthy Skin Cells as Well as Healthy Skin Exposed to Physicochemical and Biological Factors–In Vivo Examinations
6. The Use of Phytocannabinoids in Counteracting Metabolic Changes Accompanying Skin Diseases
6.1. Metabolic Changes in Psoriatic Skin Cells
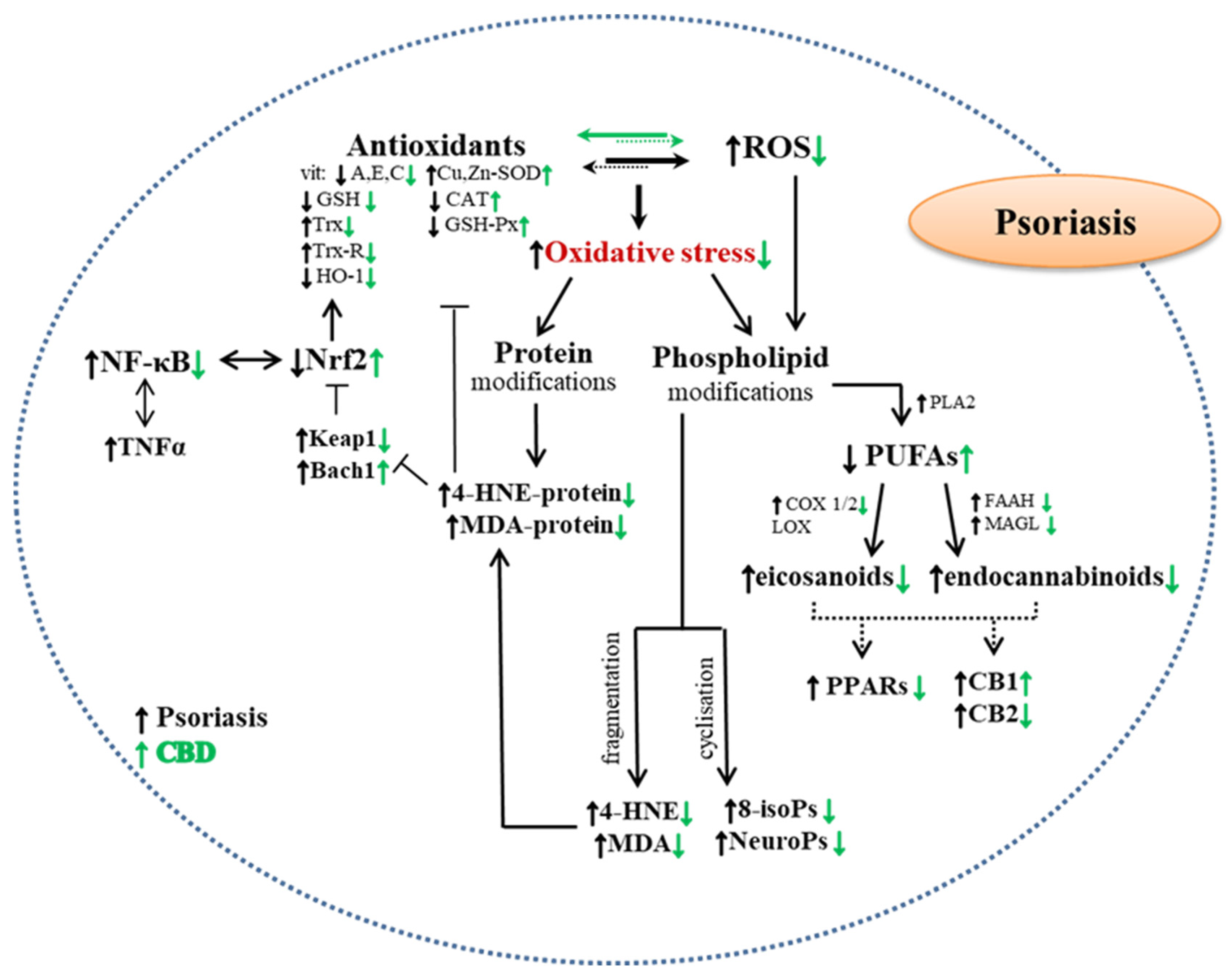
6.2. Influence of Phytocannabinoids on Redox Balance and Inflammation in Cells from Psoriatic Skin

{kind=link}
{kind=link}
| Phyto- Cannabinoids | Phyto- Cannabinoid Concentration | Tested Cells/ Method of Application (Skin/Skin Cells) | Effects of Action | Ref. |
|---|---|---|---|---|
| Psoriasis | ||||
| in vivo examinations | ||||
| CBD | Ointment with CBD oil [retrospective studies] | Applied to the skin of patients with psoriasis | Increasing skin hydration, TEWL and elasticity level | [23] |
| ex vivo examinations | ||||
| CBD | 4 μM | Keratinocytes from skin of psoriatic patients | Weakening the effects of UVB radiation
| [77] |
| CBD | 4 μM | Keratinocytes from skin of psoriatic patients |
| [63] |
| in vitro examinations | ||||
| CBG/CBN/Δ9-THC | 100–200 mM | Human keratinocytes (HPV-16 E6/E7) | Inhibition of keratinocytes proliferation | [110] |
| Acne | ||||
| in vitro examinations | ||||
| CBC | 0–10 μM | Human sebocytes (SZ95) |
synthesis, | [111] |
| THCV | 0.1–10 μM | Human sebocytes (SZ95) |
| [111] |
| CBGV | 0.1–10 μM | Human sebocytes (SZ95) |
| [111] |
| Seborrhea | ||||
| in vitro examinations | ||||
| CBD | 1–10 μM | Human sebocytes (SZ95) | Lipostatic effect
| [112] |
| Allergic contact dermatitis | ||||
| in vitro examinations | ||||
| CBC | 1–20 μM | Keratinocytes (HaCaT) stimulated with poly-(I:C) | Reduction of MCP-2, IL-6 and IL-8 levels | [113] |
| Atopic dermatitis | ||||
| in vivo examinations | ||||
| CBD | Ointment with CBD oil [retrospective studies] | Applied to the skin of patients |
| [23] |
7. Clinical Studies on the Effect of Phytocannabinoids on Skin Diseases
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sheriff, T.; Lin, M.J.; Dubin, D.; Khorasani, H. The Potential Role of Cannabinoids in Dermatology. J. Dermatol. Treat. 2020, 31, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V.; Piscitelli, F. The Endocannabinoid System and Its Modulation by Phytocannabinoids. Neurotherapeutics 2015, 12, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Le Boisselier, R.; Alexandre, J.; Lelong-Boulouard, V.; Debruyne, D. Focus on Cannabinoids and Synthetic Cannabinoids. Clin. Pharmacol. Ther. 2017, 101, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Gülck, T.; Møller, B.L. Phytocannabinoids: Origins and Biosynthesis. Trends Plant Sci. 2020, 25, 985–1004. [Google Scholar] [CrossRef]
- Nigro, E.; Formato, M.; Crescente, G.; Daniele, A. Cancer Initiation, Progression and Resistance: Are Phytocannabinoids from Cannabis Sativa L. Promising Compounds? Molecules 2021, 26, 2668. [Google Scholar] [CrossRef]
- Hill, A.J.; Williams, C.M.; Whalley, B.J.; Stephens, G.J. Phytocannabinoids as Novel Therapeutic Agents in CNS Disorders. Pharmacol. Ther. 2012, 133, 79–97. [Google Scholar] [CrossRef]
- Brenneisen, R. Chemistry and Analysis of Phytocannabinoids and Other Cannabis Constituents. In Marijuana and the Cannabinoids; Forensic Science and Medicine; ElSohly, M.A., Ed.; Humana Press: Totowa, NJ, USA, 2007; pp. 17–49. ISBN 978-1-59259-947-9. [Google Scholar]
- Caprioglio, D.; Mattoteia, D.; Pollastro, F.; Negri, R.; Lopatriello, A.; Chianese, G.; Minassi, A.; Collado, J.A.; Munoz, E.; Taglialatela-Scafati, O.; et al. The Oxidation of Phytocannabinoids to Cannabinoquinoids. J. Nat. Prod. 2020, 83, 1711–1715. [Google Scholar] [CrossRef]
- Prandi, C.; Blangetti, M.; Namdar, D.; Koltai, H. Structure-Activity Relationship of Cannabis Derived Compounds for the Treatment of Neuronal Activity-Related Diseases. Molecules 2018, 23, 1526. [Google Scholar] [CrossRef]
- Stone, N.L.; Murphy, A.J.; England, T.J.; O’Sullivan, S.E. A Systematic Review of Minor Phytocannabinoids with Promising Neuroprotective Potential. Br. J. Pharmacol. 2020, 177, 4330–4352. [Google Scholar] [CrossRef]
- Amin, M.R.; Ali, D.W. Pharmacology of Medical Cannabis. In Recent Advances in Cannabinoid Physiology and Pathology; Advances in Experimental Medicine and, Biology; Bukiya, A.N., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 151–165. ISBN 978-3-030-21737-2. [Google Scholar]
- European Monitoring Centra for Drugs and Drug Addiction. Cannabis Legislation in Europe: An Overview. Available online: https://www.emcdda.europa.eu/system/files/publications/4135/TD0217210ENN.pdf (accessed on 13 January 2023).
- Government of Canada. Cannabis Legalization and Regulation. Available online: https://www.justice.gc.ca/eng/cj-jp/cannabis/ (accessed on 13 January 2023).
- National Conference of State Legislatures. Cannabis Overview. Available online: https://www.ncsl.org/civil-and-criminal-justice/cannabis-overview/maptype/tile#undefined (accessed on 13 January 2023).
- Unated Nations Commission on Narcotic Drugs. Press Statement ‘CND Votes on Recommendation for Cannabis and Cannabis-related Substances’. Available online: https://www.unodc.org/documents/commissions/CND/CND_Sessions/CND_63Reconvened/Press_statement_CND_2_December.pdf (accessed on 13 January 2023).
- Maroon, J.; Bost, J. Review of the Neurological Benefits of Phytocannabinoids. Surg. Neurol. Int. 2018, 9, 91. [Google Scholar] [CrossRef]
- Martínez, V.; Iriondo De-Hond, A.; Borrelli, F.; Capasso, R.; Del Castillo, M.D.; Abalo, R. Cannabidiol and Other Non-Psychoactive Cannabinoids for Prevention and Treatment of Gastrointestinal Disorders: Useful Nutraceuticals? Int. J. Mol. Sci. 2020, 21, 3067. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, F.; Fasolino, I.; Romano, B.; Capasso, R.; Maiello, F.; Coppola, D.; Orlando, P.; Battista, G.; Pagano, E.; Di Marzo, V.; et al. Beneficial Effect of the Non-Psychotropic Plant Cannabinoid Cannabigerol on Experimental Inflammatory Bowel Disease. Biochem. Pharmacol. 2013, 85, 1306–1316. [Google Scholar] [CrossRef] [PubMed]
- Tomko, A.M.; Whynot, E.G.; Ellis, L.D.; Dupré, D.J. Anti-Cancer Potential of Cannabinoids, Terpenes, and Flavonoids Present in Cannabis. Cancers 2020, 12, 1985. [Google Scholar] [CrossRef]
- Kudish, A.I.; Evseev, E.G.; Cohen, G.; Harari, M. Ultraviolet Measurements and Photoclimatotherapy for Psoriasis at the Dead Sea: 25 Years of Experience. Int. J. Environ. Res. Public Health 2022, 19, 12364. [Google Scholar] [CrossRef]
- Heath, M.S.; Kolli, S.S.; Dowling, J.R.; Cline, A.; Feldman, S.R. Pharmacotherapeutic Strategies for Standard Treatment-Resistant Psoriasis. Expert Opin. Pharmacother. 2019, 20, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Bakshi, H.; Nagpal, M.; Singh, M.; Dhingra, G.A.; Aggarwal, G. Treatment of Psoriasis: A Comprehensive Review of Entire Therapies. Curr. Drug Saf. 2020, 15, 82–104. [Google Scholar] [CrossRef]
- Palmieri, B.; Laurino, C.; Vadalà, M. A Therapeutic Effect of Cbd-Enriched Ointment in Inflammatory Skin Diseases and Cutaneous Scars. Clin. Ter. 2019, 170, e93–e99. [Google Scholar] [CrossRef]
- Changoer, L.; Anastassov, G. Method to Treat Psoriasis. U.S. Patent 20190060250A1, 28 February 2019. [Google Scholar]
- ElSohly, M.A.; Radwan, M.M.; Gul, W.; Chandra, S.; Galal, A. Phytochemistry of Cannabis Sativa L. Prog. Chem. Org. Nat. Prod. 2017, 103, 1–36. [Google Scholar] [CrossRef]
- ElSohly, M.A.; Slade, D. Chemical Constituents of Marijuana: The Complex Mixture of Natural Cannabinoids. Life Sci. 2005, 78, 539–548. [Google Scholar] [CrossRef]
- Stella, N. Cannabinoid and Cannabinoid-like Receptors in Microglia, Astrocytes, and Astrocytomas. Glia 2010, 58, 1017–1030. [Google Scholar] [CrossRef]
- Tagen, M.; Klumpers, L.E. Review of Delta-8-Tetrahydrocannabinol (Δ8-THC): Comparative Pharmacology with Δ9-THC. Br. J. Pharmacol. 2022, 179, 3915–3933. [Google Scholar] [CrossRef]
- De Petrocellis, L.; Di Marzo, V. Non-CB1, Non-CB2 Receptors for Endocannabinoids, Plant Cannabinoids, and Synthetic Cannabimimetics: Focus on G-Protein-Coupled Receptors and Transient Receptor Potential Channels. J. Neuroimmune Pharmacol. 2010, 5, 103–121. [Google Scholar] [CrossRef]
- Morales, P.; Hurst, D.P.; Reggio, P.H. Molecular Targets of the Phytocannabinoids: A Complex Picture. Prog. Chem. Org. Nat. Prod. 2017, 103, 103–131. [Google Scholar] [CrossRef] [PubMed]
- Bossong, M.G.; van Berckel, B.N.; Boellaard, R.; Zuurman, L.; Schuit, R.C.; Windhorst, A.D.; van Gerven, J.M.A.; Ramsey, N.F.; Lammertsma, A.A.; Kahn, R.S. Δ9-Tetrahydrocannabinol Induces Dopamine Release in the Human Striatum. Neuropsychopharmacology 2009, 34, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Maccarrone, M. Phytocannabinoids and Endocannabinoids: Different in Nature. Rend. Fis. Acc. Lincei 2020, 31, 931–938. [Google Scholar] [CrossRef]
- Lu, D.; Potter, D.E. Chapter 58—Cannabinoids and the Cannabinoid Receptors: An Overview. In Handbook of Cannabis and Related Pathologies; Preedy, V.R., Ed.; Academic Press: San Diego, CA, USA, 2017; pp. 553–563. ISBN 978-0-12-800756-3. [Google Scholar]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants 2020, 9, 21. [Google Scholar] [CrossRef]
- Atalay, S.; Gęgotek, A.; Skrzydlewska, E. Membrane Proteins of Keratinocyte Protection by Cannabidiol Applied before and after UVB Irradiation. Med. Sci. Forum 2020, 2, 4. [Google Scholar] [CrossRef]
- Callén, L.; Moreno, E.; Barroso-Chinea, P.; Moreno-Delgado, D.; Cortés, A.; Mallol, J.; Casadó, V.; Lanciego, J.L.; Franco, R.; Lluis, C.; et al. Cannabinoid Receptors CB1 and CB2 Form Functional Heteromers in Brain. J. Biol. Chem. 2012, 287, 20851–20865. [Google Scholar] [CrossRef]
- Giacoppo, S.; Galuppo, M.; Pollastro, F.; Grassi, G.; Bramanti, P.; Mazzon, E. A New Formulation of Cannabidiol in Cream Shows Therapeutic Effects in a Mouse Model of Experimental Autoimmune Encephalomyelitis. DARU J. Pharm. Sci. 2015, 23, 48. [Google Scholar] [CrossRef]
- Muller, C.; Morales, P.; Reggio, P.H. Cannabinoid Ligands Targeting TRP Channels. Front. Mol. Neurosci. 2019, 11, 487. [Google Scholar] [CrossRef]
- Jastrząb, A.; Jarocka-Karpowicz, I.; Skrzydlewska, E. The Origin and Biomedical Relevance of Cannabigerol. Int. J. Mol. Sci. 2022, 23, 7929. [Google Scholar] [CrossRef] [PubMed]
- Filipiuc, L.E.; Ababei, D.C.; Alexa-Stratulat, T.; Pricope, C.V.; Bild, V.; Stefanescu, R.; Stanciu, G.D.; Tamba, B.-I. Major Phytocannabinoids and Their Related Compounds: Should We Only Search for Drugs That Act on Cannabinoid Receptors? Pharmaceutics 2021, 13, 1823. [Google Scholar] [CrossRef] [PubMed]
- Su, T.; Zhang, L.; Peng, M.; Wu, C.; Pan, W.; Tian, B.; Shi, J.; Pan, H.; Li, M. Cannabinoid CB2 Receptors Contribute to Upregulation of β-Endorphin in Inflamed Skin Tissues by Electroacupuncture. Mol. Pain 2011, 7, 98. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Porreca, F.; Lai, J.; Albrecht, P.J.; Rice, F.L.; Khodorova, A.; Davar, G.; Makriyannis, A.; Vanderah, T.W.; Mata, H.P.; et al. CB2 Cannabinoid Receptor Activation Produces Antinociception by Stimulating Peripheral Release of Endogenous Opioids. Proc. Natl. Acad. Sci. USA 2005, 102, 3093–3098. [Google Scholar] [CrossRef]
- De Almeida, D.L.; Devi, L.A. Diversity of Molecular Targets and Signaling Pathways for CBD. Pharmacol. Res. Perspect. 2020, 8, e00682. [Google Scholar] [CrossRef]
- Cascio, M.; Gauson, L.; Stevenson, L.; Ross, R.; Pertwee, R. Evidence That the Plant Cannabinoid Cannabigerol Is a Highly Potent A2-Adrenoceptor Agonist and Moderately Potent 5HT1A Receptor Antagonist. Br. J. Pharmacol. 2010, 159, 129–141. [Google Scholar] [CrossRef]
- Nachnani, R.; Raup-Konsavage, W.M.; Vrana, K.E. The Pharmacological Case for Cannabigerol. J. Pharmacol. Exp. Ther. 2021, 376, 204–212. [Google Scholar] [CrossRef]
- Lone, A.M.; Taskén, K. Proinflammatory and Immunoregulatory Roles of Eicosanoids in T Cells. Front. Immunol. 2013, 4, 130. [Google Scholar] [CrossRef]
- Kendall, A.C.; Nicolaou, A. Bioactive Lipid Mediators in Skin Inflammation and Immunity. Prog. Lipid Res. 2013, 52, 141–164. [Google Scholar] [CrossRef]
- Wójcik, P.; Žarković, N.; Gęgotek, A.; Skrzydlewska, E. Involvement of Metabolic Lipid Mediators in the Regulation of Apoptosis. Biomolecules 2020, 10, 402. [Google Scholar] [CrossRef]
- Cintosun, A.; Lara-Corrales, I.; Pope, E. Mechanisms of Cannabinoids and Potential Applicability to Skin Diseases. Clin. Drug Investig. 2020, 40, 293–304. [Google Scholar] [CrossRef]
- Hönigsmann, H. History of Phototherapy in Dermatology. Photochem. Photobiol. Sci. 2012, 12, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wu, M.X. A Clinical Review of Phototherapy for Psoriasis. Lasers Med. Sci. 2018, 33, 173–180. [Google Scholar] [CrossRef]
- Perez, E.; Fernandez, J.R.; Fitzgerald, C.; Rouzard, K.; Tamura, M.; Savile, C. In Vitro and Clinical Evaluation of Cannabigerol (CBG) Produced via Yeast Biosynthesis: A Cannabinoid with a Broad Range of Anti-Inflammatory and Skin Health-Boosting Properties. Molecules 2022, 27, 491. [Google Scholar] [CrossRef] [PubMed]
- Gęgotek, A.; Atalay, S.; Domingues, P.; Skrzydlewska, E. The Differences in the Proteome Profile of Cannabidiol-Treated Skin Fibroblasts Following UVA or UVB Irradiation in 2D and 3D Cell Cultures. Cells 2019, 8, 995. [Google Scholar] [CrossRef]
- Jastrząb, A.; Gęgotek, A.; Skrzydlewska, E. Cannabidiol Regulates the Expression of Keratinocyte Proteins Involved in the Inflammation Process through Transcriptional Regulation. Cells 2019, 8, 827. [Google Scholar] [CrossRef]
- Casares, L.; García, V.; Garrido-Rodríguez, M.; Millán, E.; Collado, J.A.; García-Martín, A.; Peñarando, J.; Calzado, M.A.; de la Vega, L.; Muñoz, E. Cannabidiol Induces Antioxidant Pathways in Keratinocytes by Targeting BACH1. Redox Biol. 2020, 28, 101321. [Google Scholar] [CrossRef]
- Atalay, S.; Gęgotek, A.; Domingues, P.; Skrzydlewska, E. Protective Effects of Cannabidiol on the Membrane Proteins of Skin Keratinocytes Exposed to Hydrogen Peroxide via Participation in the Proteostasis Network. Redox Biol. 2021, 46, 102074. [Google Scholar] [CrossRef] [PubMed]
- Boxberger, M.; Cenizo, V.; Cassir, N.; La Scola, B. Challenges in Exploring and Manipulating the Human Skin Microbiome. Microbiome 2021, 9, 125. [Google Scholar] [CrossRef]
- Gęgotek, A.; Biernacki, M.; Ambrożewicz, E.; Surażyński, A.; Wroński, A.; Skrzydlewska, E. The Cross-Talk between Electrophiles, Antioxidant Defence and the Endocannabinoid System in Fibroblasts and Keratinocytes after UVA and UVB Irradiation. J. Dermatol. Sci. 2016, 81, 107–117. [Google Scholar] [CrossRef]
- Gęgotek, A.; Domingues, P.; Wroński, A.; Skrzydlewska, E. Changes in Proteome of Fibroblasts Isolated from Psoriatic Skin Lesions. Int J Mol Sci 2020, 21, 5363. [Google Scholar] [CrossRef] [PubMed]
- Dayrit, J.F.; Sugiharto, A.; Coates, S.J.; Lucero-Prisno III, D.E.; Davis, M.D.D.; Andersen, L.K. Climate Change, Human Migration, and Skin Disease: Is There a Link? Int. J. Dermatol. 2022, 61, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.Q.; Agha, M.V.; Sheikhan, K.S.A.M.; Younis, S.M.; Tamimi, M.A.; Alam, M.; Ahmad, A.; Uddin, S.; Buddenkotte, J.; Steinhoff, M. Targeting Deregulated Oxidative Stress in Skin Inflammatory Diseases: An Update on Clinical Importance. Biomed. Pharmacother. 2022, 154, 113601. [Google Scholar] [CrossRef]
- Rapalli, V.K.; Waghule, T.; Gorantla, S.; Dubey, S.K.; Saha, R.N.; Singhvi, G. Psoriasis: Pathological Mechanisms, Current Pharmacological Therapies, and Emerging Drug Delivery Systems. Drug Discov. Today 2020, 25, 2212–2226. [Google Scholar] [CrossRef] [PubMed]
- Jarocka-Karpowicz, I.; Biernacki, M.; Wroński, A.; Gęgotek, A.; Skrzydlewska, E. Cannabidiol Effects on Phospholipid Metabolism in Keratinocytes from Patients with Psoriasis Vulgaris. Biomolecules 2020, 10, 367. [Google Scholar] [CrossRef]
- Baswan, S.M.; Klosner, A.E.; Glynn, K.; Rajgopal, A.; Malik, K.; Yim, S.; Stern, N. Therapeutic Potential of Cannabidiol (CBD) for Skin Health and Disorders. Clin. Cosmet. Investig. Dermatol. 2020, 13, 927–942. [Google Scholar] [CrossRef]
- Gęgotek, A.; Skrzydlewska, E. Biological Effect of Protein Modifications by Lipid Peroxidation Products. Chem. Phys. Lipids 2019, 221, 46–52. [Google Scholar] [CrossRef]
- Wójcik, P.; Biernacki, M.; Domian, N.; Žarković, N.; Skrzydlewska, E. Influence of Inhibition of COX-2-Dependent Lipid Metabolism on Regulation of UVB-Induced Keratinocytes Apoptosis by Cannabinoids. Biomolecules 2022, 12, 842. [Google Scholar] [CrossRef]
- Łuczaj, W.; Dobrzyńska, I.; Wroński, A.; Domingues, M.R.; Domingues, P.; Skrzydlewska, E. Cannabidiol-Mediated Changes to the Phospholipid Profile of UVB-Irradiated Keratinocytes from Psoriatic Patients. Int. J. Mol. Sci. 2020, 21, 6592. [Google Scholar] [CrossRef]
- Atalay, S.; Gęgotek, A.; Skrzydlewska, E. Protective Effects of Cannabidiol on the Membrane Proteome of UVB-Irradiated Keratinocytes. Antioxidants 2021, 10, 402. [Google Scholar] [CrossRef]
- Atalay, S.; Gęgotek, A.; Wroński, A.; Domigues, P.; Skrzydlewska, E. Therapeutic Application of Cannabidiol on UVA and UVB Irradiated Rat Skin. A Proteomic Study. J. Pharm. Biomed. Anal. 2021, 192, 113656. [Google Scholar] [CrossRef] [PubMed]
- Jastrząb, A.; Jarocka-Karpowicz, I.; Markowska, A.; Wroński, A.; Gęgotek, A.; Skrzydlewska, E. Antioxidant and Anti-Inflammatory Effect of Cannabidiol Contributes to the Decreased Lipid Peroxidation of Keratinocytes of Rat Skin Exposed to UV Radiation. Oxidative Med. Cell. Longev. 2021, 2021, 6647222. [Google Scholar] [CrossRef]
- Łuczaj, W.; Gęgotek, A.; Skrzydlewska, E. Analytical Approaches to Assess Metabolic Changes in Psoriasis. J. Pharm. Biomed. Anal. 2021, 205, 114359. [Google Scholar] [CrossRef]
- Ganguly, B.; Hota, M.; Pradhan, J.; Ganguly, B.; Hota, M.; Pradhan, J. Skin Aging: Implications of UV Radiation, Reactive Oxygen Species and Natural Antioxidants; IntechOpen: London, UK, 2021; ISBN 978-1-83968-282-7. [Google Scholar]
- Nakai, K.; Tsuruta, D. What Are Reactive Oxygen Species, Free Radicals, and Oxidative Stress in Skin Diseases? Int. J. Mol. Sci. 2021, 22, 10799. [Google Scholar] [CrossRef]
- Hebert, A.A. Oxidative Stress as a Treatment Target in Atopic Dermatitis: The Role of Furfuryl Palmitate in Mild-to-Moderate Atopic Dermatitis. Int. J. Womens Dermatol. 2020, 6, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Masutin, V.; Kersch, C.; Schmitz-Spanke, S. A Systematic Review: Metabolomics-Based Identification of Altered Metabolites and Pathways in the Skin Caused by Internal and External Factors. Exp. Dermatol. 2022, 31, 700–714. [Google Scholar] [CrossRef] [PubMed]
- Frederick, U.O.; Samson, H.A. Chapter 13—Bioactive Lead Compounds Effective against Skin Diseases. In Phytochemicals as Lead Compounds for New Drug Discovery; Egbuna, C., Kumar, S., Ifemeje, J.C., Ezzat, S.M., Kaliyaperumal, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 211–220. ISBN 978-0-12-817890-4. [Google Scholar]
- Wójcik, P.; Gęgotek, A.; Žarković, N.; Skrzydlewska, E. Disease-Dependent Antiapoptotic Effects of Cannabidiol for Keratinocytes Observed upon UV Irradiation. Int. J. Mol. Sci. 2021, 22, 9956. [Google Scholar] [CrossRef]
- Zhang, J.; Duan, D.; Osama, A.; Fang, J. Natural Molecules Targeting Thioredoxin System and Their Therapeutic Potential. Antioxid. Redox Signal. 2021, 34, 1083–1107. [Google Scholar] [CrossRef]
- Chovatiya, R.; Silverberg, J.I. Pathophysiology of Atopic Dermatitis and Psoriasis: Implications for Management in Children. Children 2019, 6, 108. [Google Scholar] [CrossRef]
- Friedland, R.; Kridin, K.; Cohen, A.D.; Landau, D.; Ben-Amitai, D. Psoriasis and Renal Disorders: A Large-Scale Population-Based Study in Children and Adults. Dermatology 2022, 238, 904–909. [Google Scholar] [CrossRef]
- Griffiths, C.E.M.; van de Kerkhof, P.; Czarnecka-Operacz, M. Psoriasis and Atopic Dermatitis. Dermatol. Ther. 2017, 7, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Kantor, R.; Silverberg, J.I. Environmental Risk Factors and Their Role in the Management of Atopic Dermatitis. Expert Rev. Clin. Immunol. 2017, 13, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Schäkel, K. Psoriasis Pathogenesis and Treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef]
- Cannavò, S.P.; Riso, G.; Casciaro, M.; Di Salvo, E.; Gangemi, S. Oxidative Stress Involvement in Psoriasis: A Systematic Review. Free Radic. Res. 2019, 53, 829–840. [Google Scholar] [CrossRef]
- Felquer, M.L.A.; LoGiudice, L.; Galimberti, M.L.; Rosa, J.; Mazzuoccolo, L.; Soriano, E.R. Treating the Skin with Biologics in Patients with Psoriasis Decreases the Incidence of Psoriatic Arthritis. Ann. Rheum. Dis. 2022, 81, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Mease, P.J.; Gladman, D.D.; Helliwell, P.; Khraishi, M.M.; Fuiman, J.; Bananis, E.; Alvarez, D. Comparative Performance of Psoriatic Arthritis Screening Tools in Patients with Psoriasis in European/North American Dermatology Clinics. J. Am. Acad. Dermatol. 2014, 71, 649–655. [Google Scholar] [CrossRef]
- Zhou, X.; Chen, Y.; Cui, L.; Shi, Y.; Guo, C. Advances in the Pathogenesis of Psoriasis: From Keratinocyte Perspective. Cell Death Dis. 2022, 13, 1–13. [Google Scholar] [CrossRef]
- Blauvelt, A.; Chiricozzi, A. The Immunologic Role of IL-17 in Psoriasis and Psoriatic Arthritis Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 55, 379–390. [Google Scholar] [CrossRef]
- Becatti, M.; Barygina, V.; Mannucci, A.; Emmi, G.; Prisco, D.; Lotti, T.; Fiorillo, C.; Taddei, N. Sirt1 Protects against Oxidative Stress-Induced Apoptosis in Fibroblasts from Psoriatic Patients: A New Insight into the Pathogenetic Mechanisms of Psoriasis. Int. J. Mol. Sci. 2018, 19, 1572. [Google Scholar] [CrossRef] [PubMed]
- Barygina, V.; Becatti, M.; Lotti, T.; Taddei, N.; Fiorillo, C. Low Dose Cytokines Reduce Oxidative Stress in Primary Lesional Fibroblasts Obtained from Psoriatic Patients. J. Dermatol. Sci. 2016, 83, 242–244. [Google Scholar] [CrossRef]
- Medovic, M.V.; Jakovljevic, V.L.; Zivkovic, V.I.; Jeremic, N.S.; Jeremic, J.N.; Bolevich, S.B.; Ravic Nikolic, A.B.; Milicic, V.M.; Srejovic, I.M. Psoriasis between Autoimmunity and Oxidative Stress: Changes Induced by Different Therapeutic Approaches. Oxidative Med. Cell. Longev. 2022, 2022, e2249834. [Google Scholar] [CrossRef]
- Szachowicz-Petelska, B.; Łuczaj, W.; Wroński, A.; Jastrząb, A.; Dobrzyńska, I.; You, M. The Differential Effect of Cannabidiol on the Composition and Physicochemical Properties of Keratinocyte and Fibroblast Membranes from Psoriatic Patients and Healthy People. Membranes 2021, 11, 111. [Google Scholar] [CrossRef] [PubMed]
- Dobrzyńska, I.; Szachowicz-Petelska, B.; Wroński, A.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Changes in the Physicochemical Properties of Blood and Skin Cell Membranes as a Result of Psoriasis Vulgaris and Psoriatic Arthritis Development. Int. J. Mol. Sci. 2020, 21, 9129. [Google Scholar] [CrossRef] [PubMed]
- Gęgotek, A.; Domingues, P.; Wroński, A.; Ambrożewicz, E.; Skrzydlewska, E. The Proteomic Profile of Keratinocytes and Lymphocytes in Psoriatic Patients. Proteom.—Clin. Appl. 2019, 13, 1800119. [Google Scholar] [CrossRef]
- Łuczaj, W.; Gęgotek, A.; Skrzydlewska, E. Antioxidants and HNE in Redox Homeostasis. Free. Radic. Biol. Med. 2017, 111, 87–101. [Google Scholar] [CrossRef]
- Bakry, O.A.; Samaka, R.M.; Shoeib, M.A.M.; Abdel Aal, S.M. Nuclear Factor Kappa B and Cyclo-Oxygenase-2: Two Concordant Players in Psoriasis Pathogenesis. Ultrastruct. Pathol. 2015, 39, 49–61. [Google Scholar] [CrossRef] [PubMed]
- Atalay Ekiner, S.; Gęgotek, A.; Skrzydlewska, E. The Molecular Activity of Cannabidiol in the Regulation of Nrf2 System Interacting with NF-ΚB Pathway under Oxidative Stress. Redox Biol. 2022, 57, 102489. [Google Scholar] [CrossRef]
- Dimon-Gadal, S.; Gerbaud, P.; Guibourdenche, J.; Evain-Brion, D.; Raynaud, F.; Thérond, P.; Anderson, W.B. Increased Oxidative Damage to Fibroblasts in Skin with and Without Lesions in Psoriasis. J. Investig. Dermatol. 2000, 114, 984–989. [Google Scholar] [CrossRef]
- Zalewska, A.; Głowacka, E.; Wyczółkowska, J.; Tchórzewski, H.; Narbutt, J.; Sysa-Jȩdrzejowska, A. Interleukin 6 and 8 Levels in Plasma and Fibroblast Cultures in Psoriasis. Mediat. Inflamm. 2006, 2006, 1–6. [Google Scholar] [CrossRef]
- Yang, L.; Fan, X.; Cui, T.; Dang, E.; Wang, G. Nrf2 Promotes Keratinocyte Proliferation in Psoriasis through Up-Regulation of Keratin 6, Keratin 16, and Keratin 17. J. Investig. Dermatol. 2017, 137, 2168–2176. [Google Scholar] [CrossRef]
- Sorokin, A.V.; Domenichiello, A.F.; Dey, A.K.; Yuan, Z.-X.; Goyal, A.; Rose, S.M.; Playford, M.P.; Ramsden, C.E.; Mehta, N.N. Bioactive Lipid Mediator Profiles in Human Psoriasis Skin and Blood. J. Investig. Dermatol. 2018, 138, 1518–1528. [Google Scholar] [CrossRef] [PubMed]
- Tóth, K.F.; Ádám, D.; Bíró, T.; Oláh, A. Cannabinoid Signaling in the Skin: Therapeutic Potential of the “C(Ut)Annabinoid” System. Molecules 2019, 24, 918. [Google Scholar] [CrossRef]
- Romanowska, M.; Reilly, L.; Palmer, C.N.A.; Gustafsson, M.C.U.; Foerster, J. Activation of PPARbeta/Delta Causes a Psoriasis-like Skin Disease in Vivo. PLoS ONE 2010, 5, e9701. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.-Y.; Jan, T.-R. Cannabidiol Hydroxyquinone-Induced Apoptosis of Splenocytes Is Mediated Predominantly by Thiol Depletion. Toxicol. Lett. 2010, 195, 68–74. [Google Scholar] [CrossRef]
- Fouad, A.A.; Albuali, W.H.; Al-Mulhim, A.S.; Jresat, I. Cardioprotective Effect of Cannabidiol in Rats Exposed to Doxorubicin Toxicity. Environ. Toxicol. Pharmacol. 2013, 36, 347–357. [Google Scholar] [CrossRef]
- Lee, Y.J.; Bae, J.H.; Kang, S.-G.; Cho, S.W.; Chun, D.-I.; Nam, S.M.; Kim, C.H.; Nam, H.S.; Lee, S.H.; Lee, S.H.; et al. Pro-Oxidant Status and Nrf2 Levels in Psoriasis Vulgaris Skin Tissues and Dimethyl Fumarate-Treated HaCaT Cells. Arch. Pharm. Res. 2017, 40, 1105–1116. [Google Scholar] [CrossRef]
- Kastelan, M.; Prpić-Massari, L.; Brajac, I. Apoptosis in Psoriasis. Acta Dermatovenerol. Croat. 2009, 17, 182–186. [Google Scholar]
- Wójcik, P.; Biernacki, M.; Wroński, A.; Łuczaj, W.; Waeg, G.; Žarković, N.; Skrzydlewska, E. Altered Lipid Metabolism in Blood Mononuclear Cells of Psoriatic Patients Indicates Differential Changes in Psoriasis Vulgaris and Psoriatic Arthritis. Int. J. Mol. Sci. 2019, 20, 4249. [Google Scholar] [CrossRef] [PubMed]
- Sangiovanni, E.; Fumagalli, M.; Pacchetti, B.; Piazza, S.; Magnavacca, A.; Khalilpour, S.; Melzi, G.; Martinelli, G.; Dell’Agli, M. Cannabis Sativa L. Extract and Cannabidiol Inhibit in Vitro Mediators of Skin Inflammation and Wound Injury. Phytother. Res. 2019, 33, 2083–2093. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, J.D.; Williamson, E.M. Cannabinoids Inhibit Human Keratinocyte Proliferation through a Non-CB1/CB2 Mechanism and Have a Potential Therapeutic Value in the Treatment of Psoriasis. J. Dermatol. Sci. 2007, 45, 87–92. [Google Scholar] [CrossRef]
- Oláh, A.; Markovics, A.; Szabó-Papp, J.; Szabó, P.T.; Stott, C.; Zouboulis, C.C.; Bíró, T. Differential Effectiveness of Selected Non-Psychotropic Phytocannabinoids on Human Sebocyte Functions Implicates Their Introduction in Dry/Seborrhoeic Skin and Acne Treatment. Exp. Dermatol. 2016, 25, 701–707. [Google Scholar] [CrossRef]
- Oláh, A.; Tóth, B.I.; Borbíró, I.; Sugawara, K.; Szöllõsi, A.G.; Czifra, G.; Pál, B.; Ambrus, L.; Kloepper, J.; Camera, E.; et al. Cannabidiol Exerts Sebostatic and Antiinflammatory Effects on Human Sebocytes. J. Clin. Investig. 2014, 124, 3713–3724. [Google Scholar] [CrossRef] [PubMed]
- Petrosino, S.; Verde, R.; Vaia, M.; Allarà, M.; Iuvone, T.; Di Marzo, V. Anti-Inflammatory Properties of Cannabidiol, a Nonpsychotropic Cannabinoid, in Experimental Allergic Contact Dermatitis. J. Pharmacol. Exp. Ther. 2018, 365, 652–663. [Google Scholar] [CrossRef]
- Kaczocha, M.; Glaser, S.T.; Deutsch, D.G. Identification of Intracellular Carriers for the Endocannabinoid Anandamide. Proc. Natl. Acad. Sci. USA 2009, 106, 6375–6380. [Google Scholar] [CrossRef]
- Briganti, S.; Picardo, M. Antioxidant Activity, Lipid Peroxidation and Skin Diseases. What’s New. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 663–669. [Google Scholar] [CrossRef]
- Lee, Y.; Je, Y.-J.; Lee, S.-S.; Li, Z.J.; Choi, D.-K.; Kwon, Y.-B.; Sohn, K.-C.; Im, M.; Seo, Y.J.; Lee, J.H. Changes in Transepidermal Water Loss and Skin Hydration According to Expression of Aquaporin-3 in Psoriasis. Ann. Dermatol. 2012, 24, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Ikarashi, N.; Shiseki, M.; Yoshida, R.; Tabata, K.; Kimura, R.; Watanabe, T.; Kon, R.; Sakai, H.; Kamei, J. Cannabidiol Application Increases Cutaneous Aquaporin-3 and Exerts a Skin Moisturizing Effect. Pharmaceuticals 2021, 14, 879. [Google Scholar] [CrossRef]
- Ambrożewicz, E.; Wójcik, P.; Wroński, A.; Łuczaj, W.; Jastrząb, A.; Žarković, N.; Skrzydlewska, E. Pathophysiological Alterations of Redox Signaling and Endocannabinoid System in Granulocytes and Plasma of Psoriatic Patients. Cells 2018, 7, 159. [Google Scholar] [CrossRef] [PubMed]
- Biernacki, M.; Jastrząb, A.; Skrzydlewska, E. Changes in Hepatic Phospholipid Metabolism in Rats under UV Irradiation and Topically Treated with Cannabidiol. Antioxidants 2021, 10, 1157. [Google Scholar] [CrossRef]
- Norooznezhad, A.H.; Norooznezhad, F. Cannabinoids: Possible Agents for Treatment of Psoriasis via Suppression of Angiogenesis and Inflammation. Med. Hypotheses 2017, 99, 15–18. [Google Scholar] [CrossRef]
- Ali, A.; Akhtar, N. The Safety and Efficacy of 3% Cannabis Seeds Extract Cream for Reduction of Human Cheek Skin Sebum and Erythema Content. Pak. J. Pharm. Sci. 2015, 28, 1389–1395. [Google Scholar]
- Spleman, L.; Sinclair, R.; Freeman, M.; Davis, M.; Gebauer, K. 1061 The Safety of Topical Cannabidiol (CBD) for the Treatment of Acne. J. Investig. Dermatol. 2018, 138, S180. [Google Scholar] [CrossRef]
- Schräder, N.H.B.; Duipmans, J.C.; Molenbuur, B.; Wolff, A.P.; Jonkman, M.F. Combined Tetrahydrocannabinol and Cannabidiol to Treat Pain in Epidermolysis Bullosa: A Report of Three Cases. Br. J. Dermatol. 2019, 180, 922–924. [Google Scholar] [CrossRef] [PubMed]
- Maghfour, J.; Rietcheck, H.; Szeto, M.D.; Rundle, C.W.; Sivesind, T.E.; Dellavalle, R.P.; Lio, P.; Dunnick, C.A.; Fernandez, J.; Yardley, H. Tolerability Profile of Topical Cannabidiol and Palmitoylethanolamide: A Compilation of Single-Centre Randomized Evaluator-Blinded Clinical and in Vitro Studies in Normal Skin. Clin. Exp. Dermatol. 2021, 46, 1518–1529. [Google Scholar] [CrossRef] [PubMed]
- Shao, K.; Stewart, C.; Grant-Kels, J.M. Cannabis and the Skin. Clin. Dermatol. 2021, 39, 784–795. [Google Scholar] [CrossRef] [PubMed]
- Botanix Pharmaceuticals. A Randomized, Double-Blind, Vehicle-Controlled Study to Evaluate the Safety and Efficacy of BTX 1503 in Patients with Moderate to Severe Acne Vulgaris; Botanix Pharmaceuticals: Philadelphia, PA, USA, 2022. [Google Scholar]
- Schuetz, M.; Savile, C.; Webb, C.; Rouzard, K.; Fernandez, J.R.; Perez, E. 480 Cannabigerol: The Mother of Cannabinoids Demonstrates a Broad Spectrum of Anti-Inflammatory and Anti-Microbial Properties Important for Skin. J. Investig. Dermatol. 2021, 141, S83. [Google Scholar] [CrossRef]
- Fölster-Holst, R. The Role of the Skin Microbiome in Atopic Dermatitis—Correlations and Consequences. J. Dtsch. Dermatol. Ges. 2022, 20, 571–577. [Google Scholar] [CrossRef]
- Heineman, J.T.; Forster, G.L.; Stephens, K.L.; Cottler, P.S.; Timko, M.P.; DeGeorge, B.R. A Randomized Controlled Trial of Topical Cannabidiol for the Treatment of Thumb Basal Joint Arthritis. J. Hand Surg. Am. 2022, 47, 611–620. [Google Scholar] [CrossRef] [PubMed]


| Receptors | Phytocannabinoids | |||||
|---|---|---|---|---|---|---|
| CBG | CBC | CBD | Δ9-THC | Δ8-THC | CBN | |
| CB1 | wa | pa | wa | a | pa | wa |
| CB2 | a | pa | want | pa | pa | a/ra |
| GPR18 | NDF | NDF | ant | a | NDF | NDF |
| GPR55 | NDF | NDF | ant | wa | NDF | NDF |
| TRPV1 | a | a | a | a | NDF | a |
| TRPV2 | a | a | a | a | NDF | a |
| TRPM8 | ant | ant | ant | ant | NDF | ant |
| TRPA1 | a | a | a | a | NDF | a |
| 5-HT1A | ant | NDF | a | ant | NDF | NDF |
| α2-AR | a | NDF | a | NDF | NDF | NDF |
| PPARγ | a | NDF | a | a | NDF | NDF |
|
Cannabis
sativa/Phyto- cannabinoids |
Test Products/ Time of Application | Method of Application | Skin Problems |
Total Participants | The Effects of the Preparation |
Suggestion
for Treatment | Ref. |
|---|---|---|---|---|---|---|---|
| CBD + CBG oil |
3–20% 3 and 15% CBD/CBG oil (2:1—ratio of compounds) twice a day for 6 weeks |
Topically on psoriatic lesions on the arms | Psoriasis vulgaris | 2 patients |
Reduction of psoriatic lession |
Psoriasis vulgaris | [24] |
| CBD |
5% CBD solution twice a day for 84 days |
Topically on face with acne changes |
Acne vulgaris | 368 patients |
Reduction of acne lession | Acne vulgaris | [126] |
| Cannabis seeds extract |
3% extract cream [12 weeks extract + base and base twice a day] |
Topically (on the cheeks) |
Sebum and erythema (human cheek) | 11 healthy volunteers |
Reduction of skin sebum and erythema |
Acne vulgaris, seborrhea, papules | [121] |
|
Synthetic CBD (BTX1503) PermetrexTM Patent |
5% CBD [14 and 28 days -twice a day] | Topically |
Acne vulgaris |
20 healthy volunteers + 23 people with moderate to severe acne |
Safe and well tolerated; anti-acne effect | Acne vulgaris | [122] |
|
CBM oil (CBD + THC) |
CBD (20 mg/mL) + THC (13 mg/mL) [from several months up to 2 years] | Sublingually | Epidermolysis bullosa |
3 patients with EB; without control | Reducing pain/itching and taking painkillers |
Epidermolysis bullosa | [123] |
| CBG |
0,1% CBG serum/placebo [2-weeks after irritation] | Topically on the skin after sodium lauryl sulfate (SLS)-induced irritation |
Skin irritation | 20 healthy volunteers |
Reduced inflammation, Redness, improved the skin barrier (TEWL) |
Skin problems after inflammatory inducers (physical/chemical) | [52] |
| CBD + PEA |
1% CBD + PEA (gel, balm); (0,1–10% CBD); hemp seed oil- without CBD; 0.9% NaCl and 0.1% w/v SLS as control [21-days cumulative test] |
Topically (skin of the back) | Normal skin | 20 healthy volunteers with exclusion criteria |
No increase in skin irritation or sensitization |
Possibility: long-term use of medicinal/cosmetic preparations containing CBD and PEA | [124] |
| CBD + PEA |
balm (0.1% CBD and PEA) cream (hemp seed oil, no CBD) + UVA irradiation [24 h after] |
Topically (skin of the back) |
Skin irradiated | 22 healthy volunteers with exclusion criteria |
No differences in phototoxicity vs. negative control |
Possibility: using preparations on skin exposed to solar radiation | [124] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wroński, A.; Jarocka-Karpowicz, I.; Stasiewicz, A.; Skrzydlewska, E. Phytocannabinoids in the Pharmacotherapy of Psoriasis. Molecules 2023, 28, 1192. https://doi.org/10.3390/molecules28031192
Wroński A, Jarocka-Karpowicz I, Stasiewicz A, Skrzydlewska E. Phytocannabinoids in the Pharmacotherapy of Psoriasis. Molecules. 2023; 28(3):1192. https://doi.org/10.3390/molecules28031192
Chicago/Turabian StyleWroński, Adam, Iwona Jarocka-Karpowicz, Anna Stasiewicz, and Elżbieta Skrzydlewska. 2023. "Phytocannabinoids in the Pharmacotherapy of Psoriasis" Molecules 28, no. 3: 1192. https://doi.org/10.3390/molecules28031192
APA StyleWroński, A., Jarocka-Karpowicz, I., Stasiewicz, A., & Skrzydlewska, E. (2023). Phytocannabinoids in the Pharmacotherapy of Psoriasis. Molecules, 28(3), 1192. https://doi.org/10.3390/molecules28031192