
Canady Cold Helios Plasma Reduces Soft Tissue Sarcoma Viability by Inhibiting Proliferation, Disrupting Cell Cycle, and Inducing Apoptosis: A Preliminary Report

 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
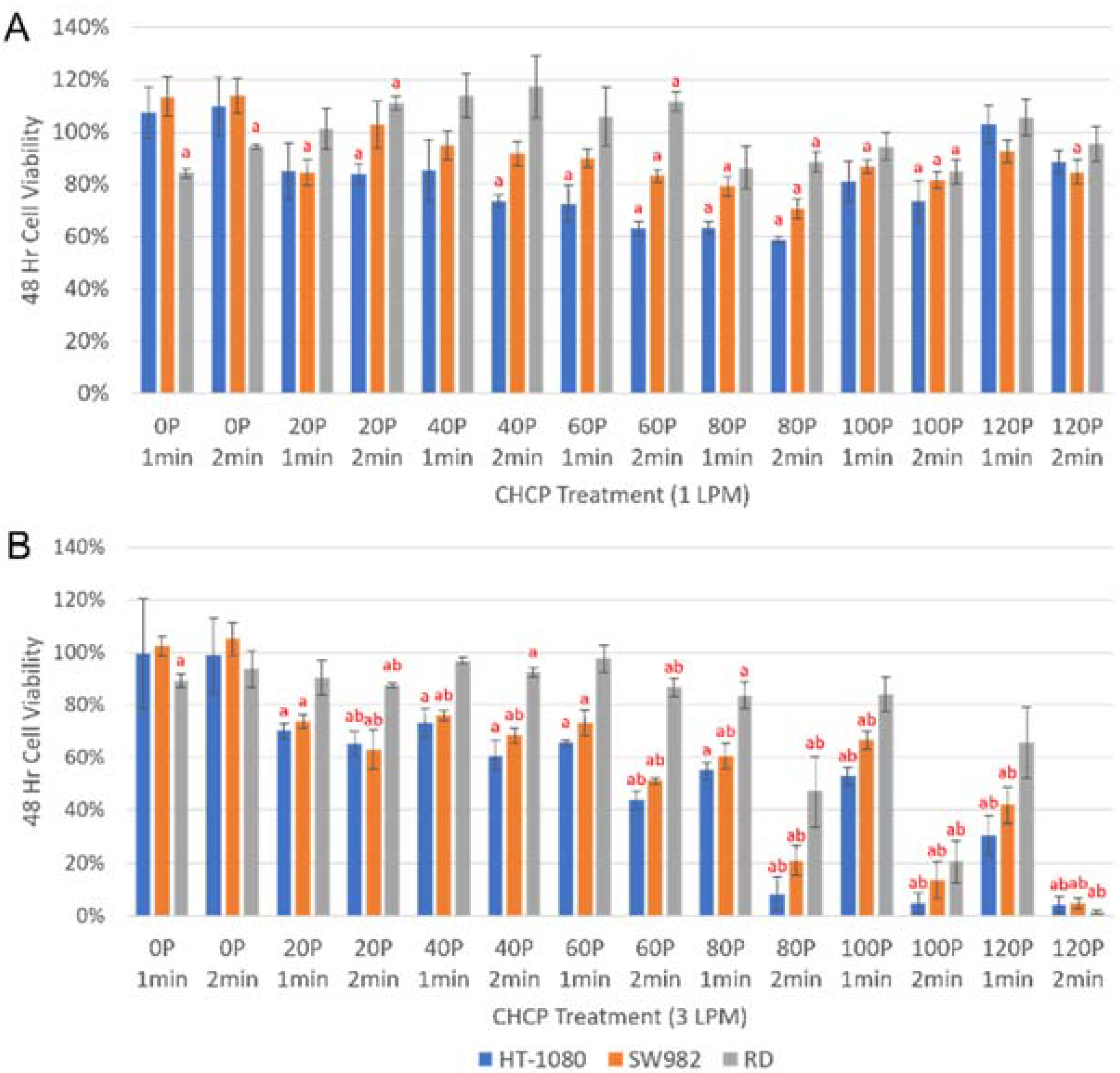
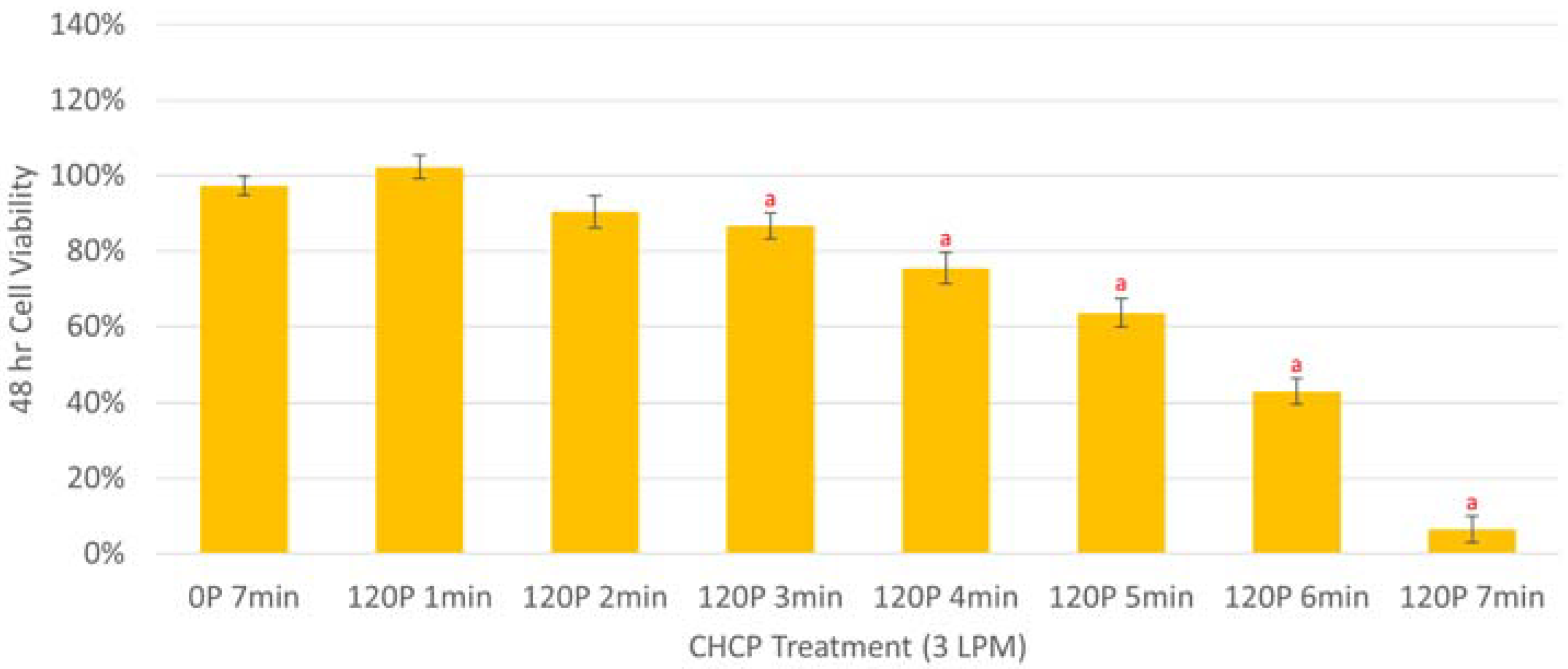
2.1. Cell Viability
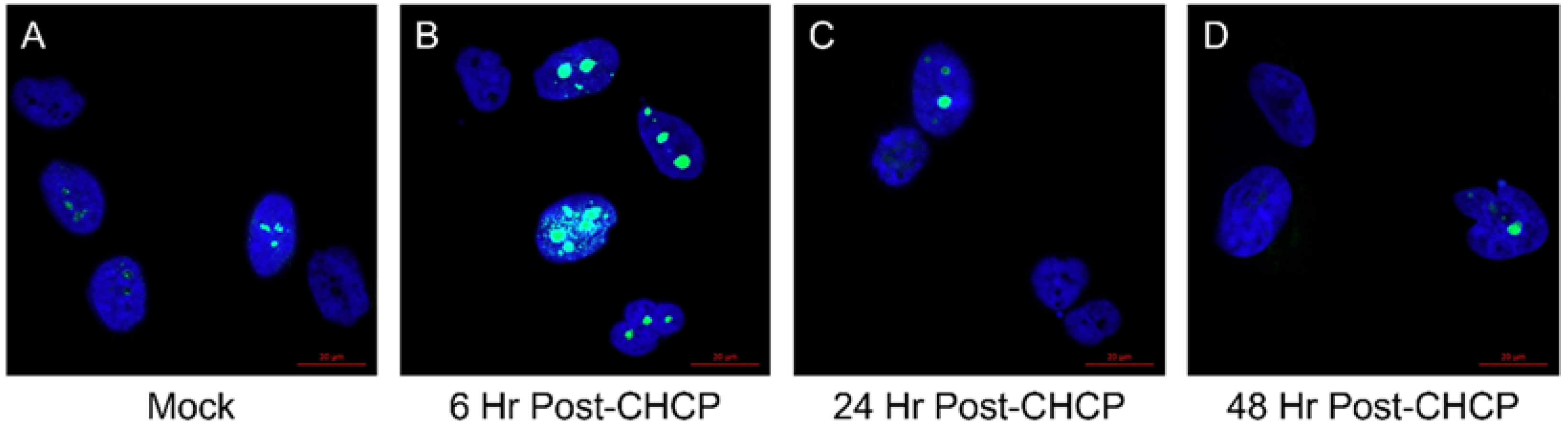
2.2. Cell Proliferation
2.3. Cell Cycle
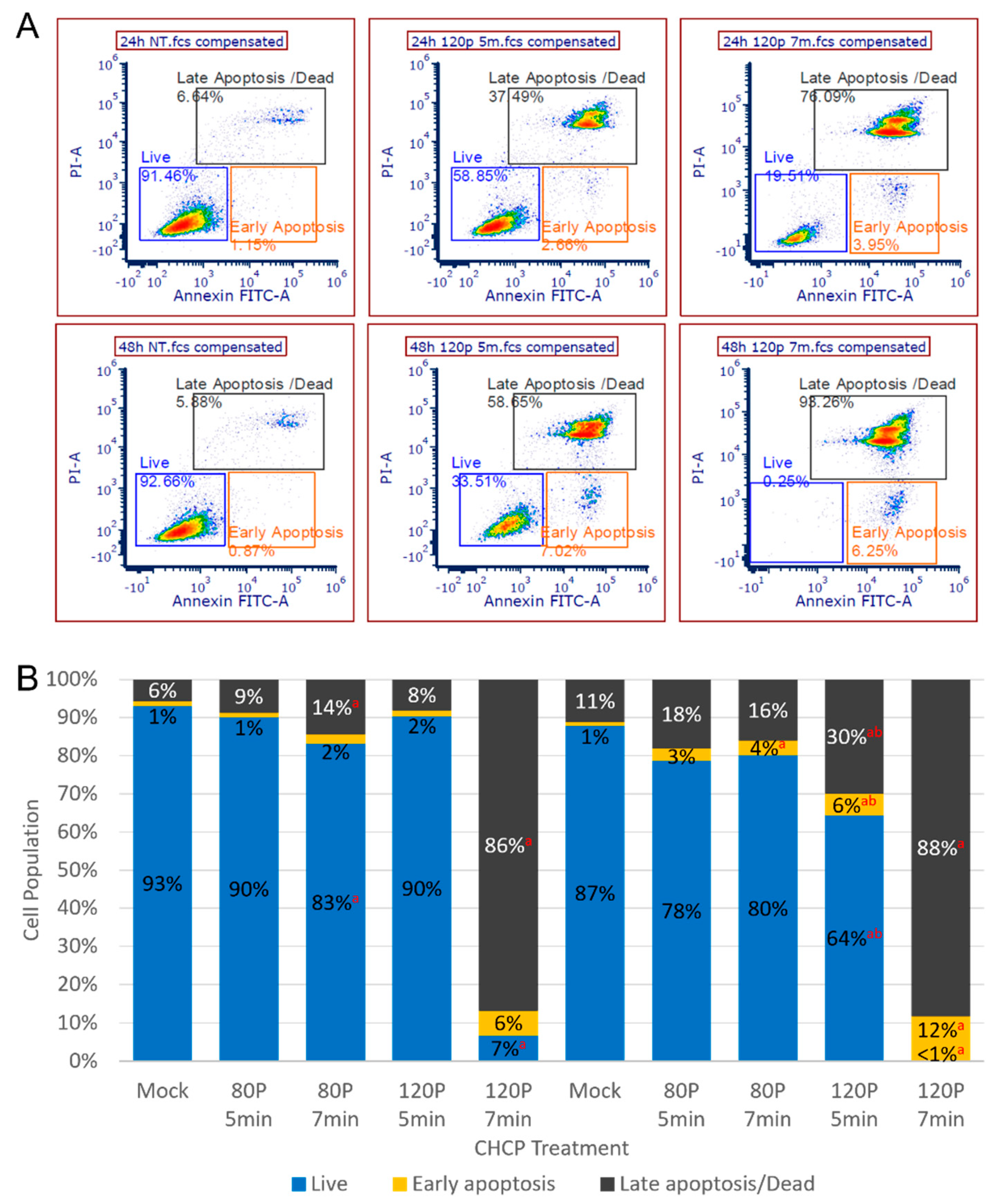
2.4. Apoptosis
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Henderson, S.R.; Guiliano, D.; Presneau, N.; McLean, S.; Frow, R.; Vujovic, S.; Anderson, J.; Sebire, N.; Whelan, J.; Athanasou, N.; et al. A molecular map of mesenchymal tumors. Genome Biol. 2005, 6, R76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, R.E. Sarcoma and metastatic carcinoma. J. Surg. Oncol. 2000, 73, 39–46. [Google Scholar] [CrossRef]
- Burningham, Z.; Hashibe, M.; Spector, L.; Schiffman, J.D. The epidemiology of sarcoma. Clin. Sarcoma Res. 2012, 2, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, L.A. Sarcoma classification: An update based on the 2013 World Health Organization classification of tumors of soft tissue and bone. Cancer 2014, 120, 1763–1774. [Google Scholar] [CrossRef] [PubMed]
- Ducimetière, F.; Lurkin, A.; Ranchère-Vince, D.; Decouvelaere, A.-V.; Peoc’h., M.; Istier, L.; Chalabreysse, P.; Muller, C.; Alberti, L.; Bringuier, P.-P.; et al. Incidence of sarcoma histotypes and molecular subtypes in a prospective epidemiological study with central pathology review and molecular testing. PLoS ONE 2011, 6, e20294. [Google Scholar] [CrossRef] [PubMed]
- Honoré, C.; Méeus, P.; Stoeckle, E.; Bonvalot, S. Soft tissue sarcoma in France in 2015: Epidemiology, classification and organization of clinical care. J. Visc. Surg. 2015, 152, 223–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thway, K.; Fisher, C. Histopathological diagnostic discrepancies in soft tissue tumours referred to a specialist centre. Sarcoma 2009, 2009, 741975. [Google Scholar] [CrossRef] [Green Version]
- Clark, M.; Thomas, J. Delay in referral to a specialist soft-tissue sarcoma unit. Eur. J. Surg. Oncol. 2005, 31, 443–448. [Google Scholar] [CrossRef]
- Skapek, S.X.; Ferrari, A.; Gupta, A.A.; Lupo, P.J.; Butler, E.; Shipley, J.; Barr, F.G.; Hawkins, D.S. Rhabdomyosarcoma. Nat. Rev. Dis. Primers 2019, 5, 1. [Google Scholar] [CrossRef]
- Simon, J.H.; Paulino, A.C.; Ritchie, J.M.; Mayr, N.A.; Buatti, J.M. Presentation, prognostic factors and patterns of failure in adult rhabdomyosarcoma. Sarcoma 2003, 7, 150381. [Google Scholar] [CrossRef] [Green Version]
- Little, D.J.; Ballo, M.T.; Zagars, G.K.; Pisters, P.W.T.; Patel, S.R.; El-Naggar, A.K.; Garden, A.S.; Benjamin, R.S. Adult rhabdomyosarcoma: Outcome following multimodality treatment. Cancer 2002, 95, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Thway, K.; Fisher, C. Synovial sarcoma: Defining features and diagnostic evolution. Ann. Diagn. Pathol. 2014, 18, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Sultan, I.; Rodriguez-Galindo, C.; Saab, R.; Yasir, S.; Casanova, M.; Fetrrari, A. Comparing children and adults with synovial sarcoma in the surveillance, epidemiology, and end results program, 1983 to 2005: An analysis of 1268 patients. Cancer 2009, 115, 3537–3547. [Google Scholar] [CrossRef]
- Augsburger, D.; Nelson, P.J.; Kalinski, T.; Udelnow, A.; Knösel, T.; Hofstetter, M.; Qin, J.W.; Wang, Y.; Gupta, A.S.; Bonifatius, S.; et al. Current diagnostics and treatment of fibrosarcoma -perspectives for future therapeutic targets and strategies. Oncotarget 2017, 8, 104638–104653. [Google Scholar] [CrossRef] [Green Version]
- Parida, L.; Fernandez-Pineda, I.; Uffman, J.K.; Davidoff, A.M.; Krasin, M.J.; Pappo, A.; Rao, B.N. Clinical management of infantile fibrosarcoma: A retrospective single-institution review. Pediatr. Surg. Int. 2013, 29, 703–708. [Google Scholar] [CrossRef] [Green Version]
- Bahrami, A.; Folpe, A.L. Adult-type Fibrosarcoma: A reevaluation of 163 putative cases diagnosed at a single institution over a 48-year period. Am. J. Surg. Pathol. 2010, 34, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Hoang, N.T.; Acevedo, L.; Mann, M.J.; Tolani, B. A review of soft-tissue sarcomas: Translation of biological advances into treatment measures. Cancer Manag. Res. 2018, 10, 1089–1114. [Google Scholar] [CrossRef] [Green Version]
- Clark, M.A.; Fisher, C.; Judson, I.; Thomas, J.M. Soft-tissue sarcomas in adults. N. Engl. J. Med. 2005, 353, 701–711. [Google Scholar] [CrossRef] [Green Version]
- Ballo, M.T.; Zagars, G.K.; Pollock, R.; Benjamin, R.S.; Feig, B.W.; Cormier, J.N.; Hunt, K.K.; Patel, S.R.; Trent, J.C.; Beddar, S.; et al. Retroperitoneal soft tissue sarcoma: An analysis of radiation and surgical treatment. Int. J. Radiat. Oncol. 2007, 67, 158–163. [Google Scholar] [CrossRef]
- Singer, S.; Antonescu, C.R.; Riedel, E.; Brennan, M.F. Histologic subtype and margin of resection predict pattern of recurrence and survival for retroperitoneal liposarcoma. Ann. Surg. 2003, 238, 358–371. [Google Scholar] [CrossRef]
- Stojadinovic, A.; Leung, D.H.Y.; Hoos, A.; Jaques, D.P.; Lewis, J.J.; Brennan, M. Analysis of the prognostic significance of microscopic margins in 2084 localized primary adult soft tissue sarcomas. Ann. Surg. 2002, 235, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Fabiano, S.; Contiero, P.; Barigelletti, G.; D’Agostino, A.; Tittarelli, A.; Mangone, L.; Bisceglia, I.; Bongiorno, S.; De Lorenzis, L.E.; Mazzoleni, G.; et al. Epidemiology of soft tissue sarcoma and bone sarcoma in Italy: Analysis of data from 15 population-based cancer registries. Sarcoma 2020, 2020, 6142613. [Google Scholar] [CrossRef]
- Crago, A.M.; Singer, S. Clinical and molecular approaches to well differentiated and dedifferentiated liposarcoma. Curr. Opin. Oncol. 2011, 23, 373–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zagars, G.K.; Ballo, M.T.; Pisters, P.W.; Pollock, R.E.; Patel, S.R.; Benjamin, R.S. Surgical margins and reresection in the management of patients with soft tissue sarcoma using conservative surgery and radiation therapy. Cancer 2003, 97, 2544–2553. [Google Scholar] [CrossRef] [PubMed]
- Lorigan, P.; Verweij, J.; Papai, Z.; Rodenhuis, S.; Le Cesne, A.; Leahy, M.; Radford, J.; Van Glabbeke, M.M.; Kirkpatrick, A.; Hogendoorn, P.; et al. Phase III trial of two investigational schedules of ifosfamide compared with standard-dose doxorubicin in advanced or metastatic soft tissue sarcoma: A European Organisation for Research and Treatment of cancer soft tissue and bone sarcoma group study. J. Clin. Oncol. 2007, 25, 3144–3150. [Google Scholar] [CrossRef]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.-Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- Martin-Broto, J.; Pousa, A.L.; Peñas, R.D.L.; Del Muro, X.G.; Gutierrez, A.; Martinez-Trufero, J.; Cruz, J.; Alvarez, R.; Cubedo, R.; Redondo, A.; et al. Randomized phase II study of trabectedin and doxorubicin compared with doxorubicin alone as first-line treatment in patients with advanced soft tissue sarcomas: A Spanish group for research on sarcoma study. J. Clin. Oncol. 2016, 34, 2294–2302. [Google Scholar] [CrossRef]
- Tap, W.D.; Wagner, A.J.; Schöffski, P.; Martin-Broto, J.; Krarup-Hansen, A.; Ganjoo, K.N.; Yen, C.C.; Abdul Razak, A.R.; Spira, A.; Kawai, A. Effect of doxorubicin plus olaratumab vs doxorubicin plus placebo on survival in patients with advanced soft tissue sarcomas: The announce randomized clinical trial. J. Am. Med. Assoc. 2020, 323, 1266–1276. [Google Scholar] [CrossRef]
- Sleijfer, S.; Ouali, M.; Van Glabbeke, M.; Krarup-Hansen, A.; Rodenhuis, S.; Le Cesne, A.; Hogendoorn, P.; Verweij, J.; Blay, J.-Y. Prognostic and predictive factors for outcome to first-line ifosfamide-containing chemotherapy for adult patients with advanced soft tissue sarcomas: An exploratory, retrospective analysis on large series from the European Organization for Research and Treatment of Cancer-Soft Tissue and Bone Sarcoma Group (EORTC-STBSG). Eur. J. Cancer 2010, 46, 72–83. [Google Scholar]
- Van Oosterom, A.; Mouridsen, H.; Nielsen, O.; Dombernowsky, P.; Krzemieniecki, K.; Judson, I.; Svancarova, L.; Spooner, D.; Hermans, C.; Van Glabbeke, M.; et al. Results of randomised studies of the EORTC soft tissue and bone sarcoma group (STBSG) with two different ifosfamide regimens in first- and second-line chemotherapy in advanced soft tissue sarcoma patients. Eur. J. Cancer 2002, 38, 2397–2406. [Google Scholar] [CrossRef]
- Demetri, G.D.; Chawla, S.P.; Von Mehren, M.; Ritch, P.; Baker, L.H.; Blay, J.Y.; Hande, K.R.; Keohan, M.L.; Samuels, B.L.; Schuetze, S.; et al. Efficacy and safety of trabectedin in patients with advanced or metastatic liposarcoma or leiomyosarcoma after failure of prior anthracyclines and ifosfamide: Results of a randomized phase ii study of two different schedules. J. Clin. Oncol. 2009, 27, 4188–4196. [Google Scholar] [CrossRef]
- Demetri, G.D.; von Mehren, M.; Jones, R.L.; Hensley, M.L.; Schuetze, S.M.; Staddon, A.; Milhem, M.; Elias, A.; Ganjoo, K.; Tawbi, H.; et al. Efficacy and safety of trabectedin or dacarbazine for metastatic liposarcoma or leiomyosarcoma after failure of conventional chemotherapy: Results of a phase III randomized multicenter clinical trial. J. Clin. Oncol. 2016, 34, 786–793. [Google Scholar] [CrossRef]
- Keidar, M.; Robert, E. Preface to Special Topic: Plasmas for Medical Applications. Phys. Plasmas 2015, 22, 121901. [Google Scholar] [CrossRef]
- Keidar, M.; Shashurin, A.; Volotskova, O.; Stepp, M.A.; Srinivasan, P.; Sandler, A.; Trink, B. Cold atmospheric plasma in cancer therapy. Phys. Plasmas 2013, 20, 57101. [Google Scholar] [CrossRef]
- Babington, P.; Rajjoub, K.; Canady, J.; Siu, A.; Keidar, M.; Sherman, J.H. Use of cold atmospheric plasma in the treatment of cancer. Biointerphases 2015, 10, 29403. [Google Scholar] [CrossRef] [Green Version]
- Cheng, X.; Rowe, W.; Ly, L.; Shashurin, A.; Zhuang, T.; Wigh, S.; Basadonna, G.; Trink, B.; Keidar, M.; Canady, J. Treatment of triple-negative breast cancer cells with the canady cold plasma conversion system: Preliminary results. Plasma 2018, 1, 218–228. [Google Scholar] [CrossRef] [Green Version]
- Ly, L.; Cheng, X.; Murthy, S.R.K.; Zhuang, T.; Jones, O.Z.; Basadonna, G.; Keidar, M.; Canady, J. Canady cold plasma conversion system treatment: An effective inhibitor of cell viability in breast cancer molecular subtypes. Clin. Plasma Med. 2020, 19, 100109. [Google Scholar] [CrossRef]
- Cheng, X.; Murthy, S.R.K.; Zhuang, T.; Ly, L.; Jones, O.; Basadonna, G.; Keidar, M.; Kanaan, Y.; Canady, J. Canady helios cold plasma induces breast cancer cell death by oxidation of histone mRNA. Int. J. Mol. Sci. 2021, 22, 9578. [Google Scholar] [CrossRef]
- Rowe, W.; Cheng, X.; Ly, L.; Zhuang, T.; Basadonna, G.; Trink, B.; Keidar, M.; Canady, J. The Canady helios cold plasma scalpel significantly decreases viability in malignant solid tumor cells in a dose-dependent manner. Plasma 2018, 1, 177–188. [Google Scholar] [CrossRef] [Green Version]
- Yamazaki, T.; Yokoyama, T.; Akatsu, H.; Tukiyama, T.; Tokiwa, T. Phenotypic characterization of a human synovial sarcoma cell line, SW982, and its response to dexamethasone. Vitr. Cell. Dev. Biol. Anim. 2003, 39, 337–339. [Google Scholar] [CrossRef]
- Hinson, A.R.P.; Jones, R.; Crose, L.E.S.; Belyea, B.C.; Barr, F.G.; Linardic, C.M. Human rhabdomyosarcoma cell lines for rhabdomyosarcoma research: Utility and pitfalls. Front. Oncol. 2013, 3, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macchia, G.; Severgnini, M.; Purgato, S.; Tolomeo, D.; Casciaro, H.; Cifola, I.; L’Abbate, A.; Loverro, A.; Palumbo, O.; Carella, M.; et al. The hidden genomic and transcriptomic plasticity of giant marker chromosomes in cancer. Genetics 2018, 208, 951–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, O.; Cheng, X.; Murthy, S.R.K.; Ly, L.; Zhuang, T.; Basadonna, G.; Keidar, M.; Canady, J. The synergistic effect of Canady Helios cold atmospheric plasma and a FOLFIRINOX regimen for the treatment of cholangiocarcinoma in vitro. Sci. Rep. 2021, 11, 8967. [Google Scholar] [CrossRef] [PubMed]
- Murthy, S.R.K.; Cheng, X.; Zhuang, T.; Ly, L.; Jones, O.; Basadonna, G.; Keidar, M.; Canady, J. BCL2A1 regulates Canady helios cold plasma-induced cell death in triple-negative breast cancer. Sci. Rep. 2022, 12, 4038. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Human Cell Line | STS Subtypes | Tissue of Origin | References |
|---|---|---|---|
| HT-1080 1 | Fibrosarcoma | Connective | [14] |
| SW-982 1 | Synovial Sarcoma | Joint; Synovium | [40] |
| RD 1 | Rhabdomyosarcoma | Muscle | [41] |
| 94T778 1,2 | Liposarcoma | Adipose | [42] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ly, L.; Cheng, X.; Murthy, S.R.K.; Jones, O.Z.; Zhuang, T.; Gitelis, S.; Blank, A.T.; Nissan, A.; Adileh, M.; Colman, M.; et al. Canady Cold Helios Plasma Reduces Soft Tissue Sarcoma Viability by Inhibiting Proliferation, Disrupting Cell Cycle, and Inducing Apoptosis: A Preliminary Report. Molecules 2022, 27, 4168. https://doi.org/10.3390/molecules27134168
Ly L, Cheng X, Murthy SRK, Jones OZ, Zhuang T, Gitelis S, Blank AT, Nissan A, Adileh M, Colman M, et al. Canady Cold Helios Plasma Reduces Soft Tissue Sarcoma Viability by Inhibiting Proliferation, Disrupting Cell Cycle, and Inducing Apoptosis: A Preliminary Report. Molecules. 2022; 27(13):4168. https://doi.org/10.3390/molecules27134168
Chicago/Turabian StyleLy, Lawan, Xiaoqian Cheng, Saravana R. K. Murthy, Olivia Z. Jones, Taisen Zhuang, Steven Gitelis, Alan T. Blank, Aviram Nissan, Mohammad Adileh, Matthew Colman, and et al. 2022. "Canady Cold Helios Plasma Reduces Soft Tissue Sarcoma Viability by Inhibiting Proliferation, Disrupting Cell Cycle, and Inducing Apoptosis: A Preliminary Report" Molecules 27, no. 13: 4168. https://doi.org/10.3390/molecules27134168
APA StyleLy, L., Cheng, X., Murthy, S. R. K., Jones, O. Z., Zhuang, T., Gitelis, S., Blank, A. T., Nissan, A., Adileh, M., Colman, M., Keidar, M., Basadonna, G., & Canady, J. (2022). Canady Cold Helios Plasma Reduces Soft Tissue Sarcoma Viability by Inhibiting Proliferation, Disrupting Cell Cycle, and Inducing Apoptosis: A Preliminary Report. Molecules, 27(13), 4168. https://doi.org/10.3390/molecules27134168