
The Antimicrobial Activity of Origanum vulgare L. Correlated with the Gastrointestinal Perturbation in Patients with Metabolic Syndrome

 , , and
, , and
Abstract
1. Introduction
Phase Angle
2. Results
2.1. Antibacterial Activity of EOO
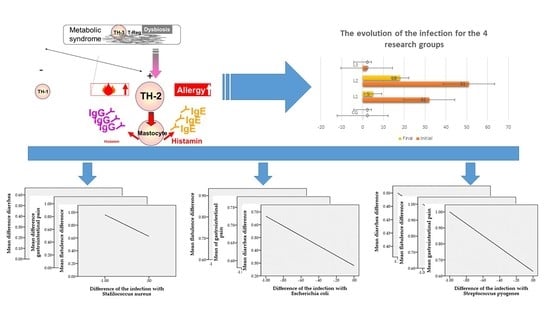
2.2. Study of Bacterial Infection Incidents in Patients with MS
2.3. The Status of the Evolution of Gastrointestinal Parameters in Correlation with EOO Therapy
2.4. Changes in the Phase Angle
- -
- No changes were recorded for the control group (t = 1000, p = 0.330);
- -
- For L1 an improvement t = −10.020, p < 0.01 is recorded;
- -
- For group L2 a significant improvement reflected from the value t = −8.099, p < 0.01 can be observed;
- -
- For group L3 t = −6.205, p < 0.01, indicating a statistically significant change.
3. Discussion
4. Materials and Methods
4.1. Ethics
4.2. The EOO Obtaining
- RI = retention indices of “i”;
- i = constituent of essential oil that is being analyzed;
- n = carbon number of the alkane which elutes before “i”;
- m = number of carbons of the alkane which elutes after “i”;
- tri = retention time of “i”;
- trn = retention time of the alkane which elutes before “i”;
- trm = retention time of the alkane which elutes after “i”.
4.3. Antimicrobial Activity
- The culture medium is a solid Mueller–Hinton agar medium in a uniform layer of 4 mm (stored at 4 °C, for a maximum of 7 days) sown with a bacterial culture;
- The discs with AB are placed on the surface of the medium;
- AB will diffuse into the environment, showing a constant decrease in the concentration gradient from the edge of the disc to the periphery;
- After incubation, two distinct areas are delimited: an area where bacterial growth is inhibited by AB concentration and a growth area where AB concentration is too low to inhibit growth;
- The larger the diameter of the inhibition zone, the more sensitive the bacteria (MIC is smaller).
4.4. Clinical Trials
- -
- CG = patients in control group without infection (n = 20);
- -
- L1 = patients with Staphylococcus infection (n = 32);
- -
- L2 = patients with Escherichia coli infection (n = 51);
- -
- L3 = patients with Streptococcus infection (n = 2).
4.5. Enrolled Patients and Anthropometry
4.6. Tracking Metabolic Parameters, Phase Angle
4.7. Tracking the Status of the Evolution of Gastrointestinal Parameters
4.7.1. Tracking Diarrhea Status
4.7.2. Tracking the Flatulence
4.7.3. Tracking Gastrointestinal Pain
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Sample Availability
References
- Sommer, P.; Sweeney, G. Functional and Mechanistic Integration of Infection and the Metabolic Syndrome. Korean Diabetes J. 2010, 34, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, S.P.; McCann, D.; Desai, M.; Rosenbaum, M.; Leibel, R.L.; Ferrante, A.W., Jr. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Investig. 2003, 112, 1796–1808. [Google Scholar] [CrossRef] [PubMed]
- Caffarelli, C.; Di Mauro, D.; Mastrorilli, C.; Bottau, P.; Cipriani, F.; Ricci, G. Solid Food Introduction and the Development of Food Allergies. Nutrients 2018, 10, 1790. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.M.; Ryu, O.; Lee, K.; Kim, H.; Seo, J.; Kim, S.G.; Kim, N.; Choi, D.; Baik, S. Serum adiponectin, interleukin-10 levels and inflammatory markers in the metabolic syndrome. Diabetes Res. Clin. Pr. 2007, 75, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Surendar, J.; Mohan, V.; Rao, M.M.; Babu, S.; Aravindhan, V. Increased Levels of Both Th1 and Th2 Cytokines in Subjects with Metabolic Syndrome (CURES-103). Diabetes Technol. Ther. 2011, 13, 477–482. [Google Scholar] [CrossRef]
- Brandt, E.B. Th2 Cytokines and Atopic Dermatitis. J. Clin. Cell. Immunol. 2011, 2, 110. [Google Scholar] [CrossRef]
- Halmos, T.; Suba, I. A bélbakterióta élettani jellemzői és a dysbacteriosis szerepe az elhízásban, inzulinrezisztenciában, diabetesben és metabolikus szindrómában. Orvosi Hetil. 2016, 157, 13–22. [Google Scholar] [CrossRef]
- Simirgiotis, M.; Burton, D.; Parra, F.; López, J.; Muñoz, P.; Araya, H.E.; Parra, C. Antioxidant and Antibacterial Capacities of Origanum vulgare L. Essential Oil from the Arid Andean Region of Chile and its Chemical Characterization by GC-MS. Metabolites 2020, 10, 414. [Google Scholar] [CrossRef]
- Jurca, T.; Baldea, I.; Filip, G.A.; Olteanu, D.; Clichici, S.; Pallag, A.; Vicaș, L.; Marian, E.; Micle, O.; Crivii, C.B.; et al. A Phytocomplex Consisting of Tropaeolum majus L. and Salvia officinalis L. Extracts Alleviates the Inflammatory Response of Dermal Fibroblasts to Bacterial Lipopolysaccharides. Oxidative Med. Cell. Longev. 2020, 2020, 8516153. [Google Scholar] [CrossRef]
- Jurca, T.; Pallag, A.; Marian, E.; Mureșan, M.E.; Stan, R.L.; Vicaș, L.G. The histo-anatomical investigation and the polyphenolic profile of antioxidant complex active ingredients from three Viola species. Farm. J. 2019, 67, 634–640. [Google Scholar] [CrossRef]
- Dittmar, M.; Reber, H.; Kahaly, G.J. Bioimpedance phase angle indicates catabolism in Type 2 diabetes. Diabet. Med. 2015, 32, 1177–1185. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Danielzik, S.; Dörhöfer, R.-P.; Later, W.; Wiese, S.; Müller, M.J. Phase Angle from Bioelectrical Impedance Analysis: Population Reference Values by Age, Sex, and Body Mass Index. J. Parenter. Enter. Nutr. 2006, 30, 309–316. [Google Scholar] [CrossRef]
- Coelho, M.P.P.; Diniz, K.G.D.; Bering, T.; Ferreira, L.D.S.A.; Vieira, D.A.; Castro, M.R.C.; Correia, M.I.T.; Rocha, G.A.; Teixeira, R.; Garcia, F.D.; et al. Skeletal muscle mass index and phase angle are decreased in individuals with dependence on alcohol and other substances. Nutrition 2020, 71, 110614. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.-M.; Chen, C.-C.; Chang, C.-M.; Fang, Y.-J.; Bair, M.-J.; Chen, P.-Y.; Chang, C.-Y.; Hsu, Y.-C.; Chen, M.-J.; Chen, C.-C.; et al. Long-term changes of gut microbiota, antibiotic resistance, and metabolic parameters after Helicobacter pylori eradication: A multicentre, open-label, randomised trial. Lancet Infect. Dis. 2019, 19, 1109–1120. [Google Scholar] [CrossRef]
- Mendrick, D.L.; Diehl, A.M.; Topor, L.S.; Dietert, R.R.; Will, Y.; La Merrill, M.A.; Bouret, S.; Varma, V.; Hastings, K.L.; Schug, T.T.; et al. Metabolic Syndrome and Associated Diseases: From the Bench to the Clinic. Toxicol. Sci. 2018, 162, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Després, J.-P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nat. Cell Biol. 2006, 444, 881–887. [Google Scholar] [CrossRef]
- Hoza, A.; Moldovan, C.; Fărcaș, D.M.; Pallag, A.; Nemeth, S.; Felicia, M. Comparative study of oral antidiabetic therapy and insulin therapy on hepatic steatosis in patients with type 2 diabetes mellitus. Farm. J. 2018, 4, 652–657. [Google Scholar] [CrossRef]
- Badale, A.; Pallag, A.; Kozma, M.; Hegedus, C.; Kovacs, D.; Gulyas, H.; Zdrinca, M.; Magyar, I.; Marc, F.; Nemeth, S.; et al. Fenugreek seed and its active agent diosgenin treatment effects on different metabolic parameters in rats. Farm. J. 2019, 67, 92–98. [Google Scholar] [CrossRef]
- Thaiss, C.A.; Zmora, N.; Levy, M.; Elinav, E. The microbiome and innate immunity. Nat. Cell Biol. 2016, 535, 65–74. [Google Scholar] [CrossRef]
- Hegedűs, C.; Mureșan, M.; Badale, A.; Juhász, B.; Varga, B.; Szilágyi, A.; Sinka, D.; Bácskay, I.; Popoviciu, M.; Magyar, I.; et al. SIRT1 Activation by Equisetum arvense L. (Horsetail) Modulates Insulin Sensitivity in Streptozotocin Induced Diabetic Rats. Molecules 2020, 25, 2541. [Google Scholar] [CrossRef]
- Andersen, C.J.; Murphy, K.E.; Fernandez, M.L. Impact of Obesity and Metabolic Syndrome on Immunity. Adv. Nutr. 2016, 7, 66–75. [Google Scholar] [CrossRef]
- Scully, I.L.; McNeil, L.K.; Pathirana, S.; Singer, C.L.; Liu, Y.; Mullen, S.; Girgenti, D.; Gurtman, A.; Pride, M.W.; Jansen, K.U.; et al. Neutrophil killing of Staphylococcus aureus in diabetes, obesity and metabolic syndrome: A prospective cellular surveillance study. Diabetol. Metab. Syndr. 2017, 9, 76. [Google Scholar] [CrossRef] [PubMed]
- Ghitea, T.C.; Bungau, S.; Tit, D.M.; Purza, L.; Otrisal, P.; Aleya, L.; Cioca, G.; Pantis, C.; Lazar, L. The Effects of Oregano Oil on Fungal Infections Associated with Metabolic Syndrome. Rev. Chim. 2020, 71, 335–341. [Google Scholar] [CrossRef]
- Proestos, C.; Lytoudi, K.; Mavromelanidou, O.K.; Zoumpoulakis, P.; Sinanoglou, V.J. Antioxidant Capacity of Selected Plant Extracts and Their Essential Oils. Antioxidants 2013, 2, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Loof, T.G.; Edeicke, C.; Medina, E. The role of coagulation/fibrinolysis during Streptococcus pyogenes infection. Front. Cell. Infect. Microbiol. 2014, 4, 128. [Google Scholar] [CrossRef]
- Biran, D.; Ron, E. Extraintestinal Pathogenic Escherichia coli. Curr. Top. Microbiol. Immunol. 2018, 416, 149–161. [Google Scholar] [CrossRef]
- Bauer, B.W.; Radovanovic, A.; Willson, N.-L.; Bajagai, Y.S.; Van, T.T.H.; Moore, R.J.; Stanley, D. Oregano: A potential prophylactic treatment for the intestinal microbiota. Heliyon 2019, 5, e02625. [Google Scholar] [CrossRef]
- Earley, S.; Gonzales, A.L.; Garcia, Z.I. A Dietary Agonist of Transient Receptor Potential Cation Channel V3 Elicits Endothelium-Dependent Vasodilation. Mol. Pharmacol. 2010, 77, 612–620. [Google Scholar] [CrossRef]
- Wijesundara, N.M.; Rupasinghe, H.P.V. Essential oils from Origanum vulgare and Salvia officinalis exhibit antibacterial and anti-biofilm activities against Streptococcus pyogenes. Microb. Pathog. 2018, 117, 118–127. [Google Scholar] [CrossRef]
- Man, A.; Santacroce, L.; Iacob, R.; Mare, A.; Man, L. Antimicrobial Activity of Six Essential Oils Against a Group of Human Pathogens: A Comparative Study. Pathogens 2019, 8, 15. [Google Scholar] [CrossRef]
- Paitan, Y. Current Trends in Antimicrobial Resistance of Escherichia coli. Curr. Top. Microbiol. Immunol. 2018, 416, 181–211. [Google Scholar] [CrossRef]
- Doesschate, T.T.; Van Mens, S.P.; Van Nieuwkoop, C.; Geerlings, S.; Hoepelman, A.I.M.; Bonten, M.J.M. Oral fosfomycin versus ciprofloxacin in women with E.coli febrile urinary tract infection, a double-blind placebo-controlled randomized controlled non-inferiority trial (FORECAST). BMC Infect. Dis. 2018, 18, 626. [Google Scholar] [CrossRef] [PubMed]
- Lagha, R.; Ben Abdallah, F.; Al-Sarhan, B.O.; Al-Sodany, Y.M. Antibacterial and Biofilm Inhibitory Activity of Medicinal Plant Essential Oils Against Escherichia coli Isolated from UTI Patients. Molecules 2019, 24, 1161. [Google Scholar] [CrossRef]
- Veenstra, J.P.; Johnson, J.J. Oregano (Origanium Vulgare) Extract for Food Preservation and Improving Gastrointestinal Health. Int. J. Nutr. 2019, 3, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Selberg, O.; Selberg, D. Norms and correlates of bioimpedance phase angle in healthy human subjects, hospitalized patients, and patients with liver cirrhosis. Graefe’s Arch. Clin. Exp. Ophthalmol. 2002, 86, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Goossens, G.H. The role of adipose tissue dysfunction in the pathogenesis of obesity-related insulin resistance. Physiol. Behav. 2008, 94, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, R.V.; Alves, M.D.S.; Pinto, T.D.O.; Menezes, R.D.S.; Junior, P.C.D.; Chaves, D.S.; De Sousa, M.A.A. Hydrodistillation Extraction Kinetics of Volatile Oils from Varronia curassavica and Laurus nobilis. Rev. Bras. Farm. 2020, 30, 503–509. [Google Scholar] [CrossRef]
- Olmedo, R.; Ribotta, P.; Grosso, N.R. Decrease of chemical and volatile oxidation indicators using oregano essential oil combined with BHT in sunflower oil under accelerated storage conditions. J. Food Sci. Technol. 2019, 56, 2522–2535. [Google Scholar] [CrossRef]
- Patel, J.B.; Weinstein, M.P.; Eliopoulos, G.M.; Jenkins, S.G.; Lewis, J.S.; Limbago, B.; Mathers, A.J.; Mazzulli, T.; Patel, R.; Richter, S.S.; et al. Performance Standards for Antimicrobial Susceptibility Testing; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017; Volume 37. [Google Scholar]
- Lambert, R.; Skandamis, P.; Coote, P.; Nychas, G.-J. A study of the minimum inhibitory concentration and mode of action of oregano essential oil, thymol and carvacrol. J. Appl. Microbiol. 2001, 91, 453–462. [Google Scholar] [CrossRef]
- Jabłonowska-Lietz, B.; Wrzosek, M.; Włodarczyk, M.; Nowicka, G. New indexes of body fat distribution, visceral adiposity index, body adiposity index, waist-to-height ratio, and metabolic disturbances in the obese. Kardiol. Pol. 2017, 75, 1185–1191. [Google Scholar] [CrossRef]
- Ferreira-Valente, A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef] [PubMed]
- Hickey, G.L.; Grant, S.W.; Dunning, J.; Siepe, M. Statistical primer: Sample size and power calculations—Why, when and how? Eur. J. Cardiothorac. Surg. 2018, 54, 4–9. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Staphylococcus aureus | Escherichia coli | Streptococcus pyogenes | |||
|---|---|---|---|---|---|
| Antibiotics | Diameter (mm) | Antibiotics | Diameter (mm) | Antibiotics | Diameter (mm) |
| Azithromycin | 25 | Azithromycin | 23 | Ampicillin | 27 |
| Erythromycin | 32 | Ampicillin | 24 | Erythromycin | 30 |
| Levofloxacin | 29 | Levofloxacin | 33 | Levofloxacin | 30 |
| Tetracycline | 30 | Tetracycline | 29 | Tetracycline | 31 |
| EOO 0.2 μL | 33 | EOO 0.2 μL | 34 | EOO 0.2 μL | 32 |
| EOO 0.4 μL | 35 | EOO 0.4 μL | 35 | EOO 0.4 μL | 33 |
| EOO 0.6 μL | 36 | EOO 0.6 μL | 36 | EOO 0.6 μL | 34 |
| Research Variables | Difference in Infection with Staphylococcus aureus | Difference in Infection with Escherichia coli | Difference in Infection with Streptococcus pyogenes | |
|---|---|---|---|---|
| Pearson coefficient | Group 106 patients | |||
| Diarrhea | −0.277 ** | −0.366 ** | 0.132 | |
| Gastrointestinal pain | −0.292 ** | −0.174 * | −0.224 ** | |
| Flatulence | −0.302 ** | −0.224 ** | 0.021 | |
| Compound Name | Retention Time | Relative Area % | Kovats Retention Indices (RI) |
|---|---|---|---|
| α-Pinene | 6.074 | 0.23 | 713 |
| 1-Octen-3-ol | 6.710 | 0.77 | 966 |
| Bicyclo[2.2.1]heptan, 2,2-dimethyl-3-methylene-, (1S)- | 6.323 | 0.16 | 1055 |
| endo-Borneol | 9.737 | 3.39 | 1214 |
| 2-Furanmethanol, 5-eteniltetrahydro- α,α,5-trimethyl-, cis- | 8.248 | 0.23 | 1239 |
| 2-Methyl-5-(propan-2-yliden)cyclohexan-1,4-diol | 11.877 | 0.98 | 1244 |
| o-Cymene | 7.489 | 0.44 | 1251 |
| p-Cymene-2-ol-methyl-ether | 10.790 | 0.18 | 1256 |
| cis-Linalool oxide | 8.496 | 0.16 | 1265 |
| Thymol | 11.445 | 3.62 | 1268 |
| Carvacrol | 11.670 | 29.22 | 1292 |
| Carvone | 11.118 | 0.61 | 1299 |
| (R)-lavandulyl acetate | 12.414 | 0.17 | 1341 |
| 4,4-Dimethylpent-2-enal | 11.969 | 0.19 | 1369 |
| Terpineol | 10.210 | 1.06 | 1381 |
| R-(-)-p-Menth-l-en-4-ol | 9.890 | 2.89 | 1409 |
| α-Cadinol | 15.997 | 0.02 | 1500 |
| 3-Octanol | 6.969 | 0.19 | 1601 |
| Eucaliptol | 7.622 | 0.40 | 1670 |
| .tau.-Cadinol | 15.989 | 0.57 | 1804 |
| (-)-Spatulenol | 15.302 | 0.46 | 1829 |
| Linalool | 8.659 | 11.18 | 1861 |
| o-lzopropilphenethol | 12.033 | 0.27 | 1895 |
| Phenol, 2-methil-5-(1-methyletil)-, acetate | 12.574 | 0.32 | 1953 |
| Caryophyllene | 13.356 | 1.44 | 1962 |
| β-Bisabolene | 14.349 | 2.65 | 2264 |
| 2,7-Dimethyloctadiin-3,5-diol-2,7 | 13.734 | 0.52 | 2288 |
| S-lndacen-l-(2H)-ona, 3,5,6,7-tetrahydro-3,3,5,5-tetramethyl-8-(3-methilbutil) | 21.508 | 0.20 | 3101 |
| 3-Trifluoroacetate ester pregnenolone | 21.107 | 0.46 | 3162 |
| Caryophyllene oxide | 15.397 | 1.01 | 3669 |
| Geranyl acetate | 12.656 | 0.23 | 4360 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghitea, T.C.; El-Kharoubi, A.; Ganea, M.; Bimbo-Szuhai, E.; Nemeth, T.S.; Ciavoi, G.; Foghis, M.; Dobjanschi, L.; Pallag, A.; Micle, O. The Antimicrobial Activity of Origanum vulgare L. Correlated with the Gastrointestinal Perturbation in Patients with Metabolic Syndrome. Molecules 2021, 26, 283. https://doi.org/10.3390/molecules26020283
Ghitea TC, El-Kharoubi A, Ganea M, Bimbo-Szuhai E, Nemeth TS, Ciavoi G, Foghis M, Dobjanschi L, Pallag A, Micle O. The Antimicrobial Activity of Origanum vulgare L. Correlated with the Gastrointestinal Perturbation in Patients with Metabolic Syndrome. Molecules. 2021; 26(2):283. https://doi.org/10.3390/molecules26020283
Chicago/Turabian StyleGhitea, Timea Claudia, Amina El-Kharoubi, Mariana Ganea, Erika Bimbo-Szuhai, Tiberiu Sebastian Nemeth, Gabriela Ciavoi, Monica Foghis, Luciana Dobjanschi, Annamaria Pallag, and Otilia Micle. 2021. "The Antimicrobial Activity of Origanum vulgare L. Correlated with the Gastrointestinal Perturbation in Patients with Metabolic Syndrome" Molecules 26, no. 2: 283. https://doi.org/10.3390/molecules26020283
APA StyleGhitea, T. C., El-Kharoubi, A., Ganea, M., Bimbo-Szuhai, E., Nemeth, T. S., Ciavoi, G., Foghis, M., Dobjanschi, L., Pallag, A., & Micle, O. (2021). The Antimicrobial Activity of Origanum vulgare L. Correlated with the Gastrointestinal Perturbation in Patients with Metabolic Syndrome. Molecules, 26(2), 283. https://doi.org/10.3390/molecules26020283