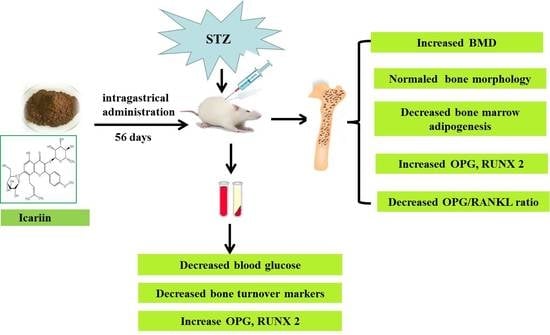
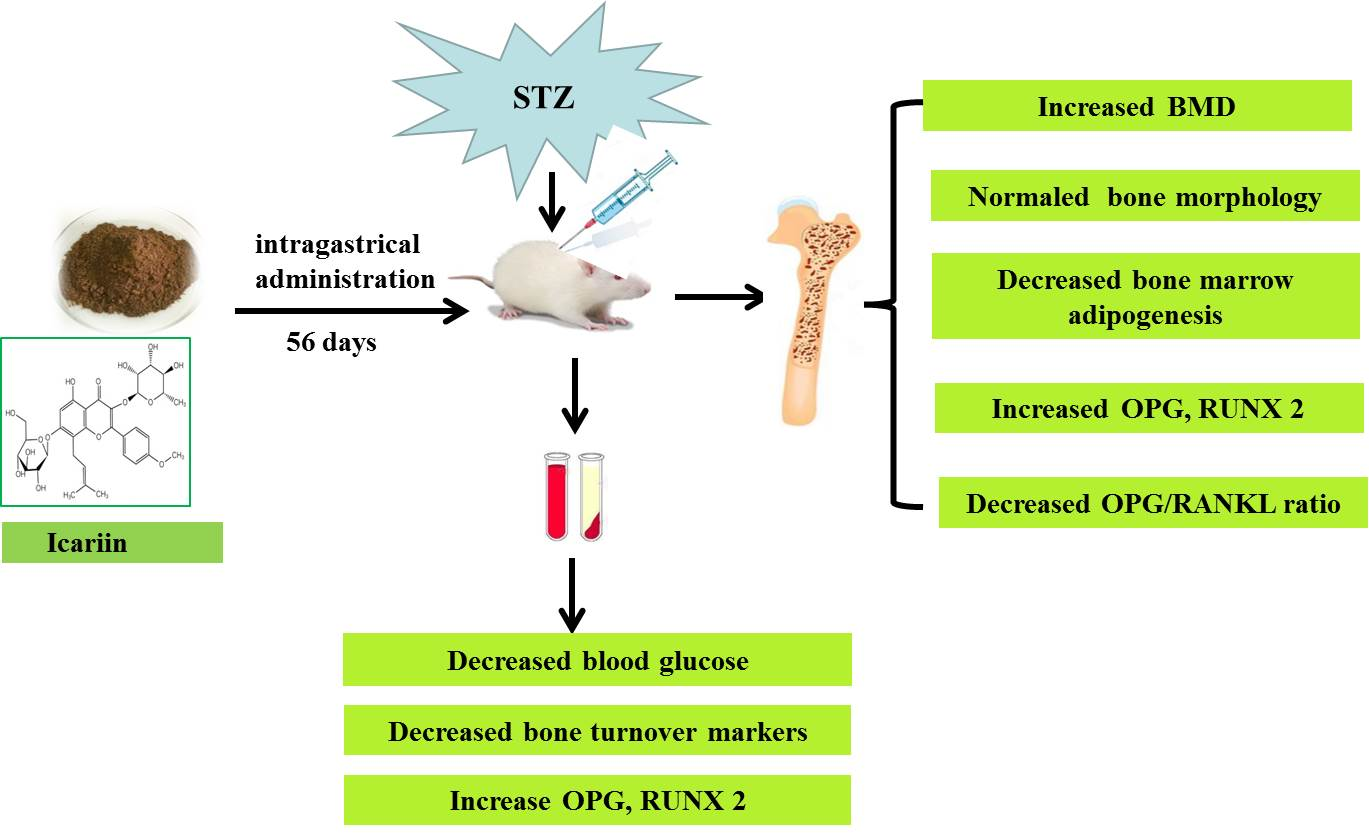
Icariin Prevents Diabetes-Induced Bone Loss in Rats by Reducing Blood Glucose and Suppressing Bone Turnover


Abstract
1. Introduction
2. Results
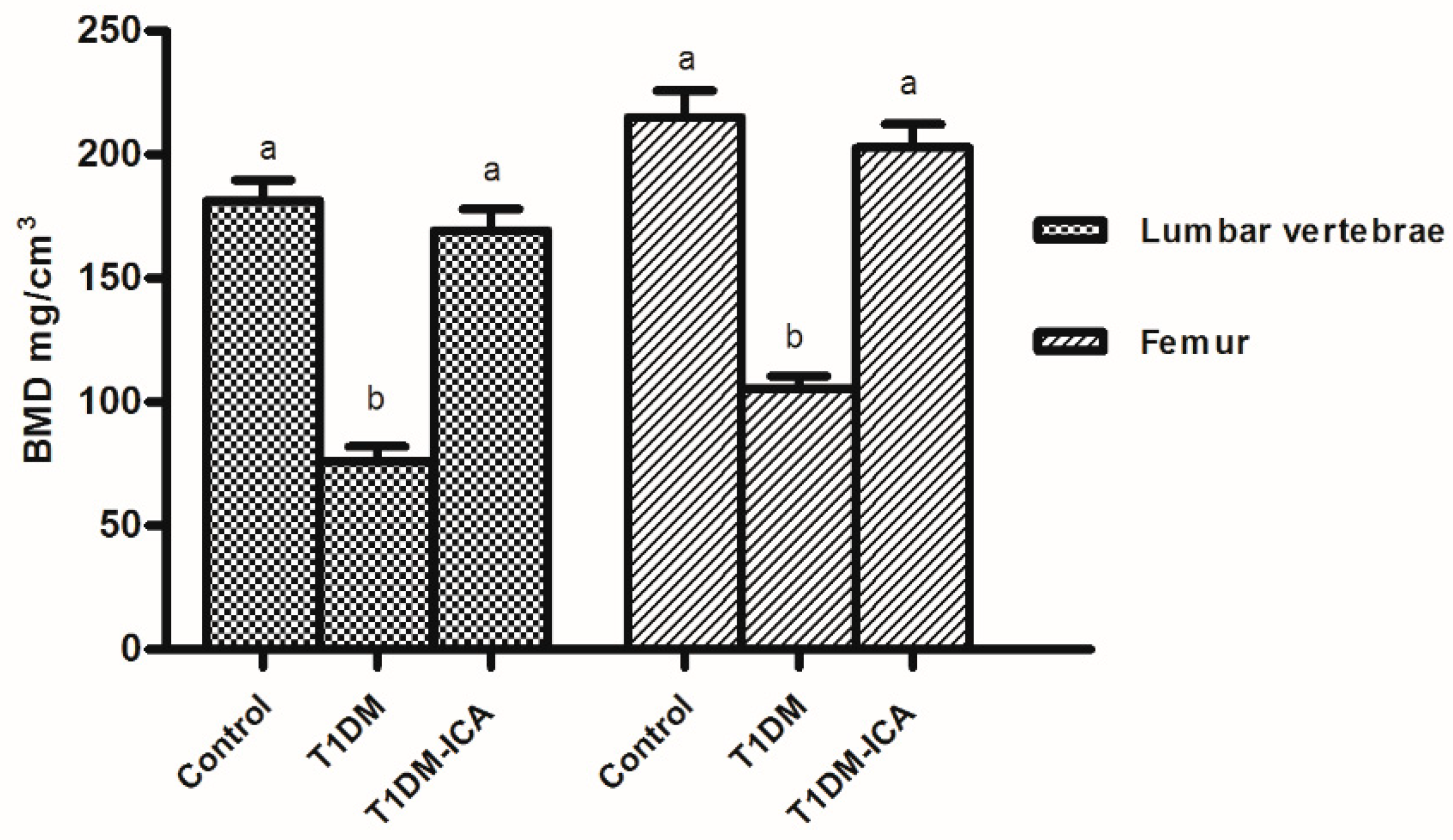
2.1. Icariin (ICA) Increased Bone Mineral Density of Diabetic Rats
2.2. ICA Decreased Blood Glucose and Serum Bone Turnover Markers
2.3. ICA Increased Serum Ca, P, OPG, and RUNX 2 and Decreased Serum RANKL
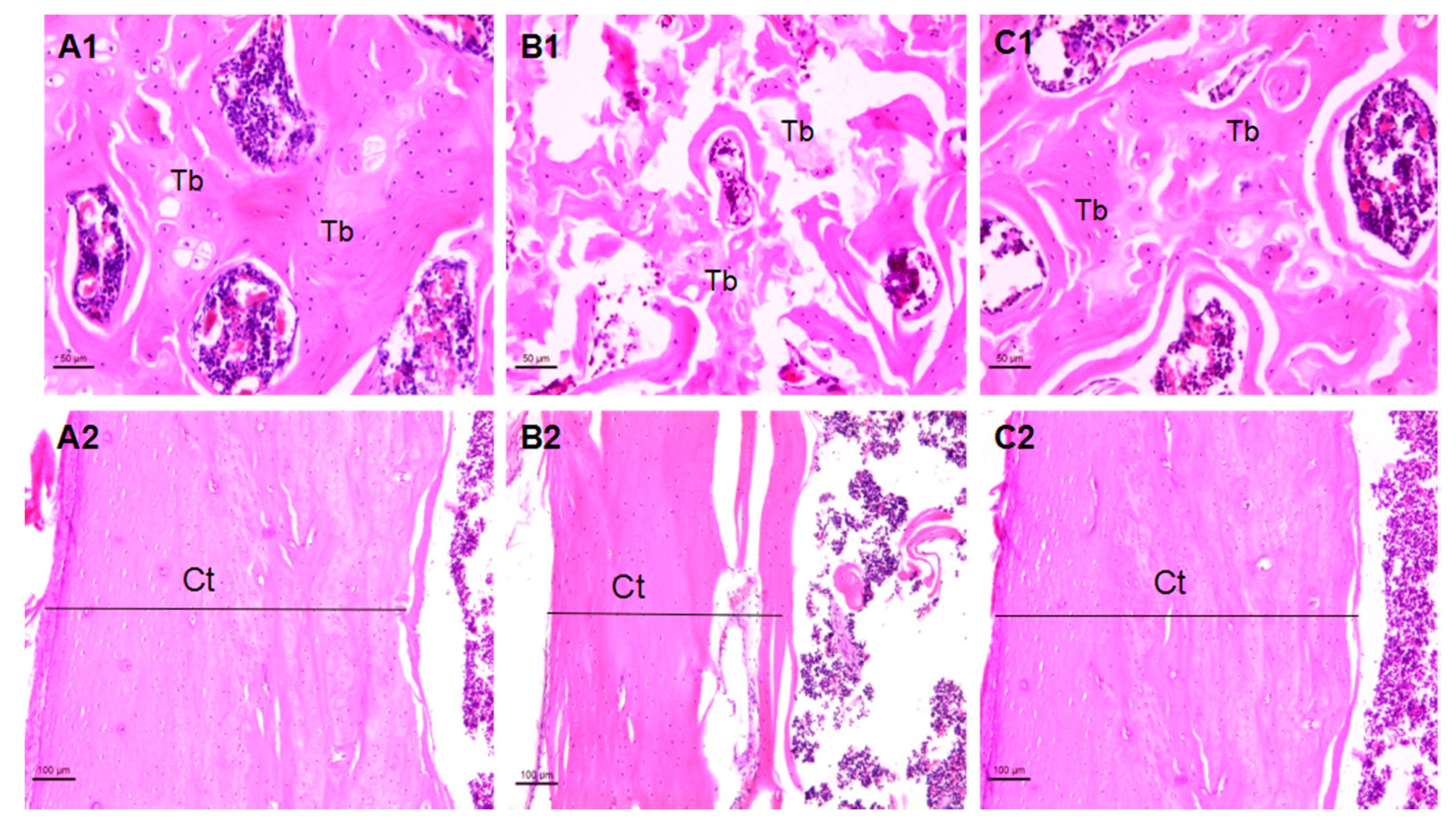
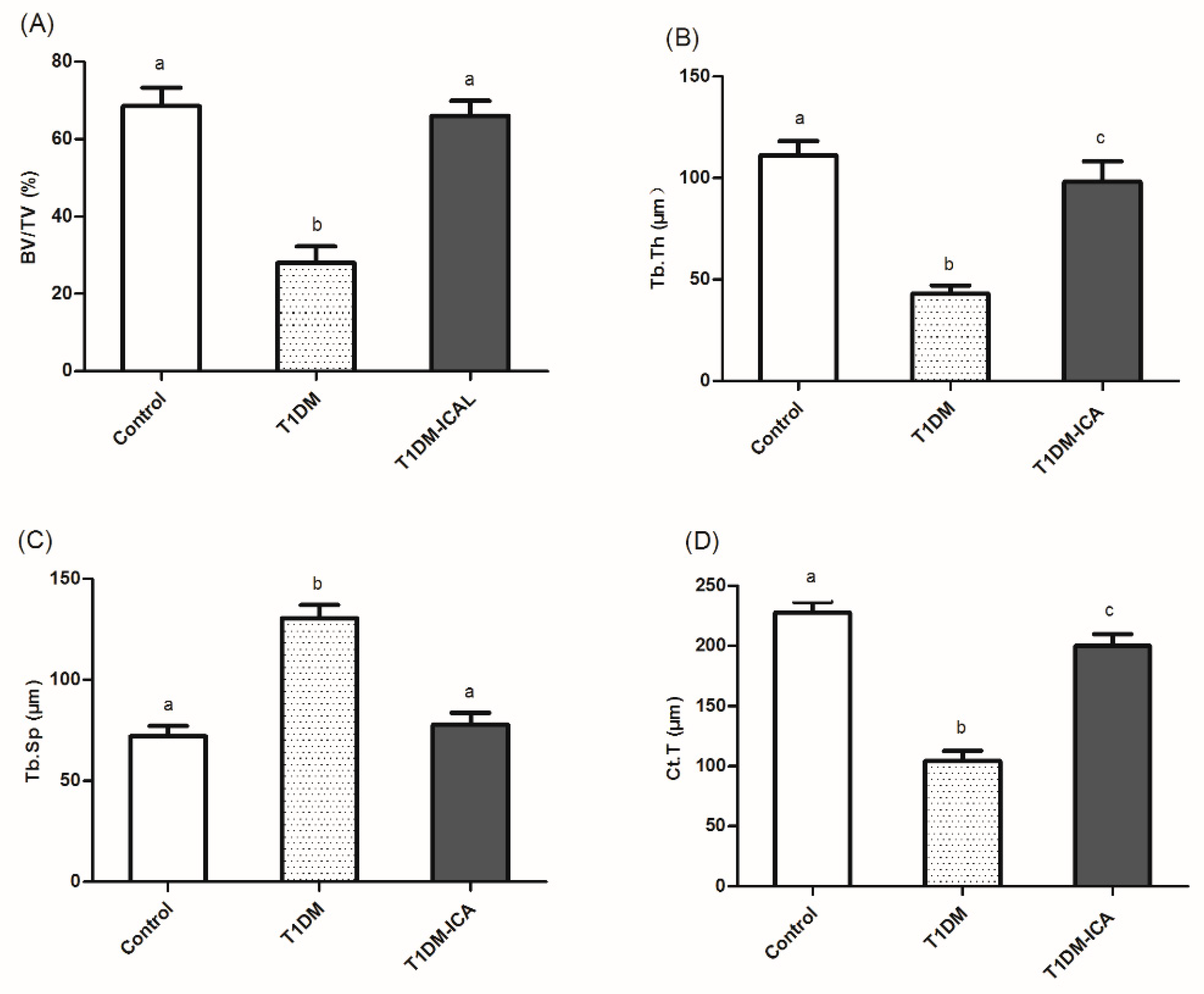
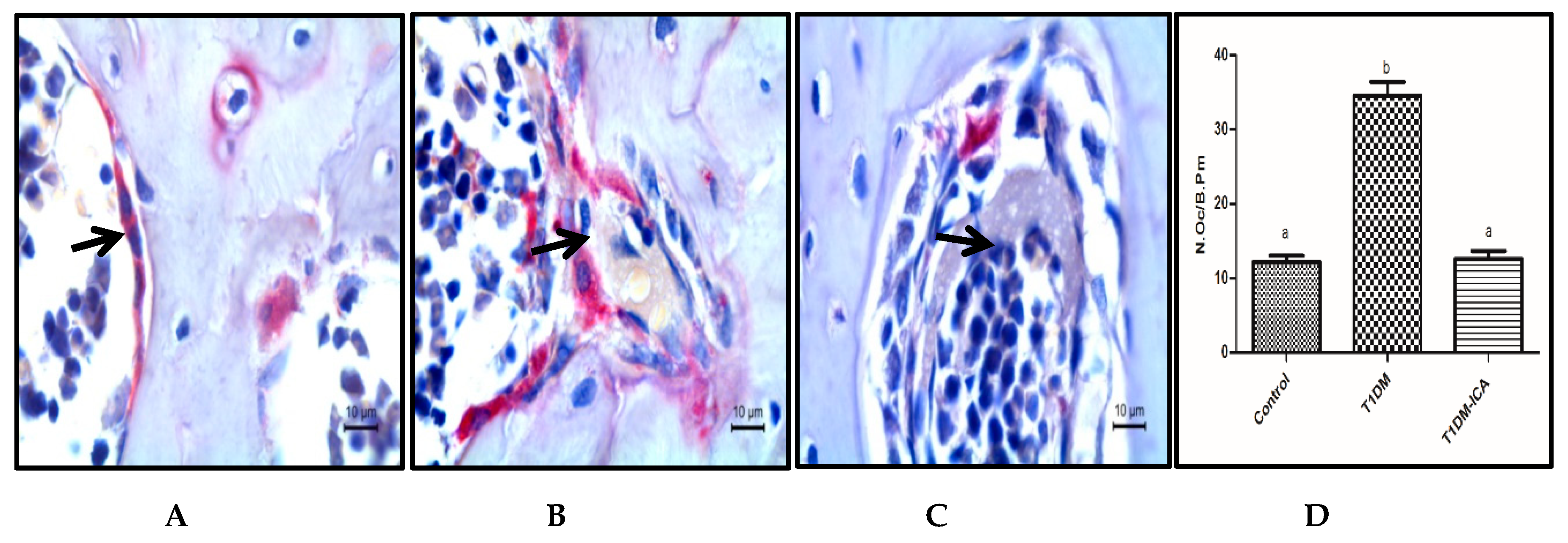
2.4. Effects of ICA on Bone Morphology and Bone Histomorphometry Parameters
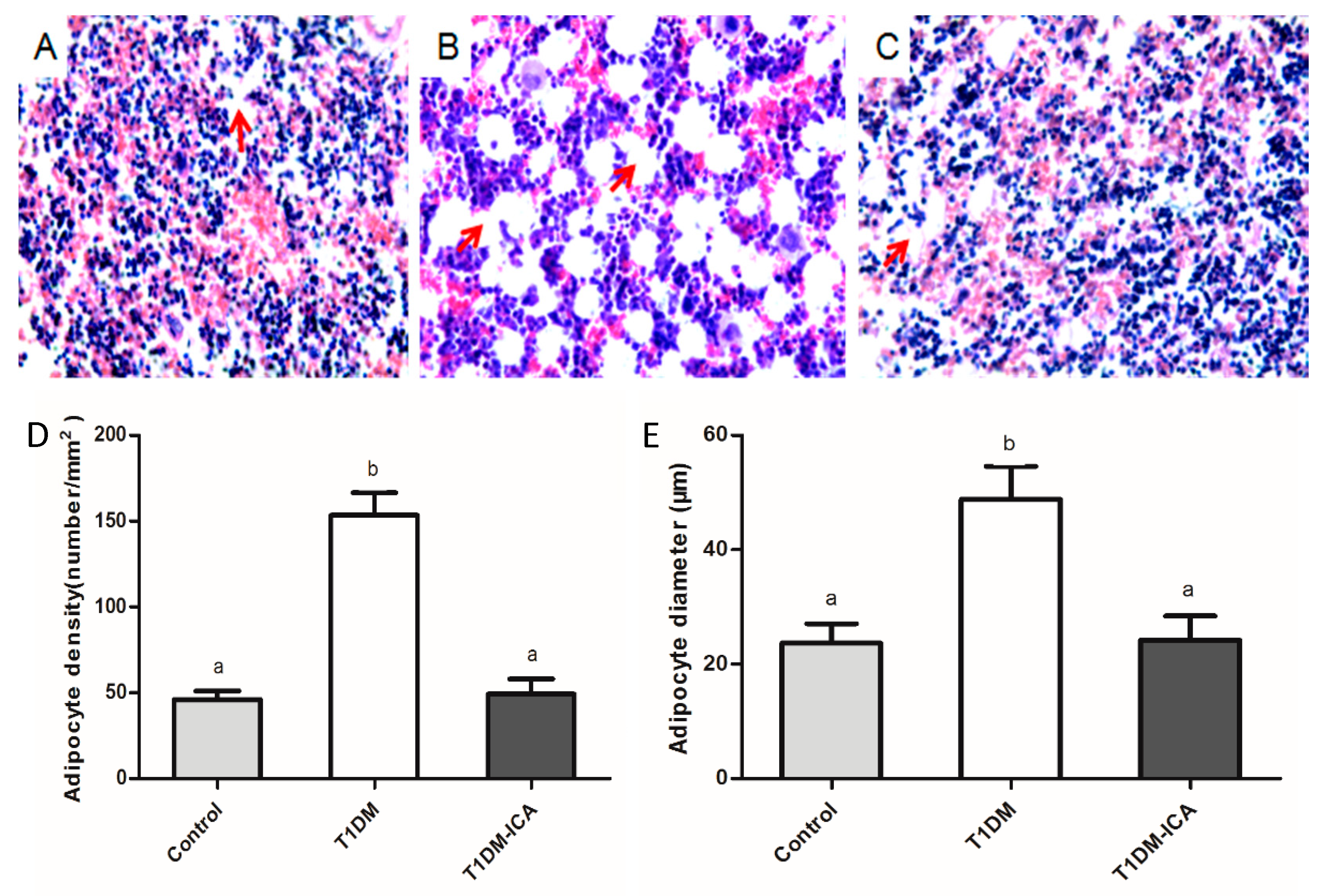
2.5. ICA Decreased Bone Marrow Adipocyte Density and Adipocyte Diameter
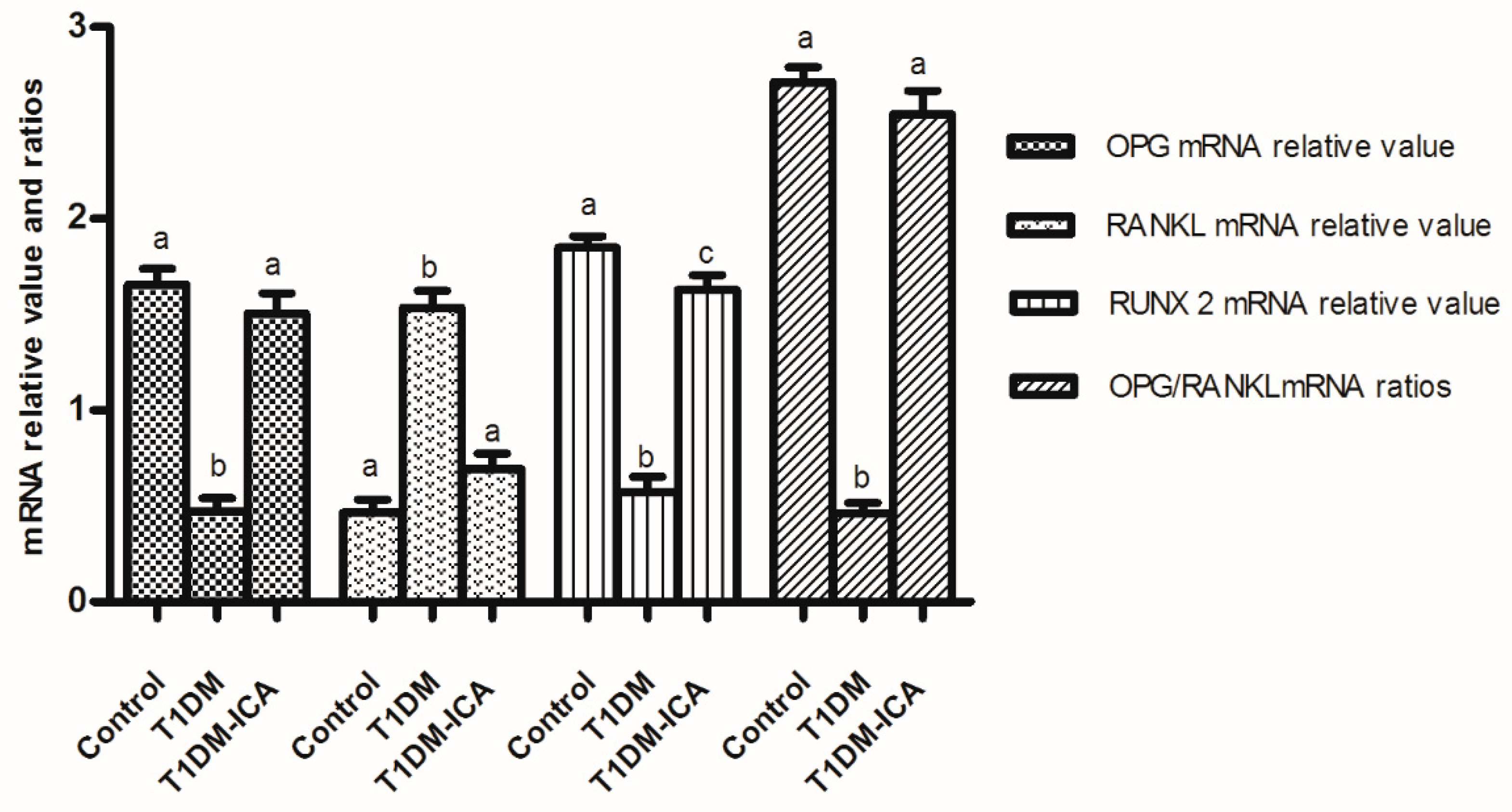
2.6. ICA Increased RUNX 2, OPG mRNA Expression, and OPG/RANKL mRNA Ratio in Bone Tissues of Diabetic Rats
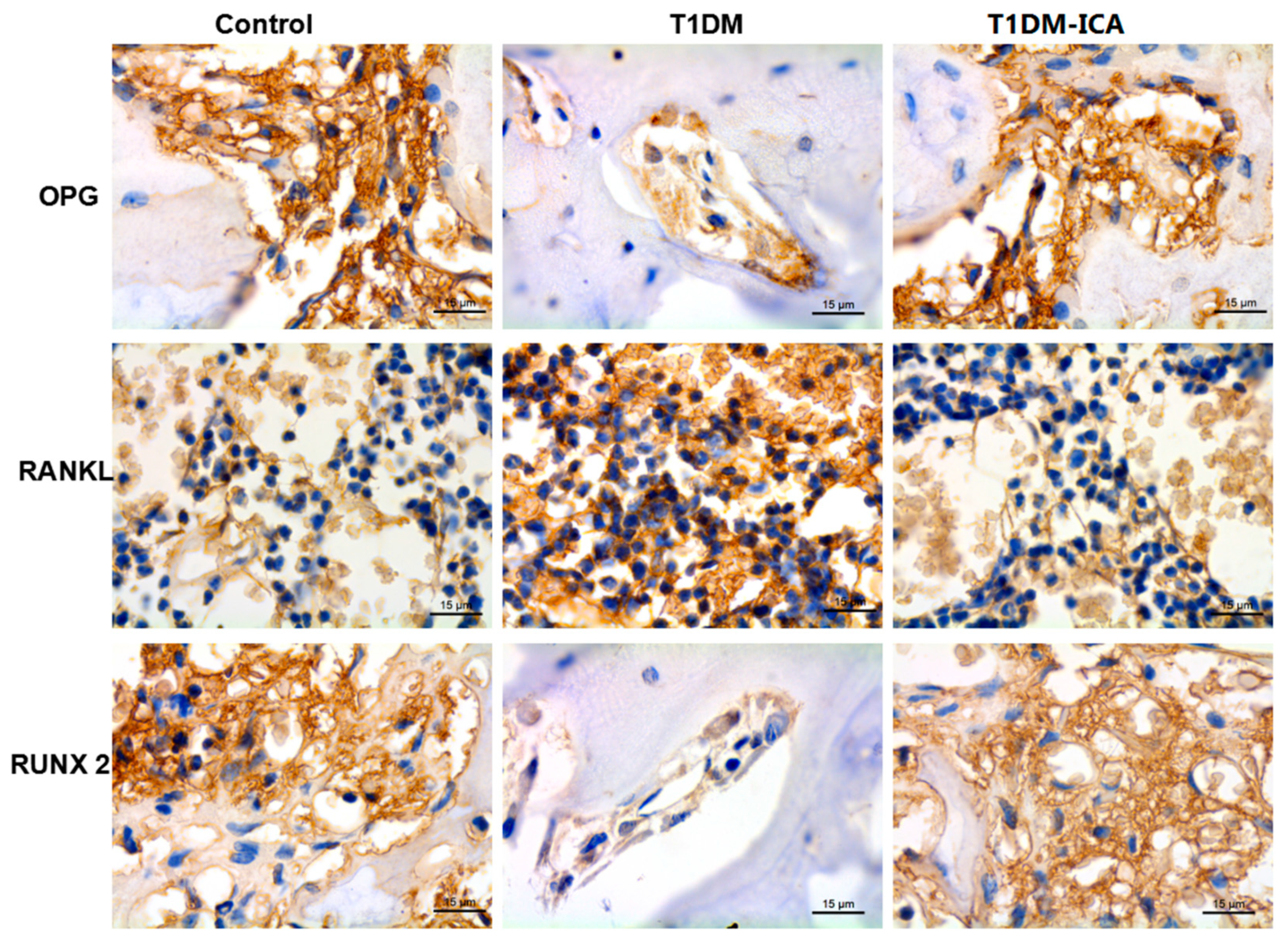
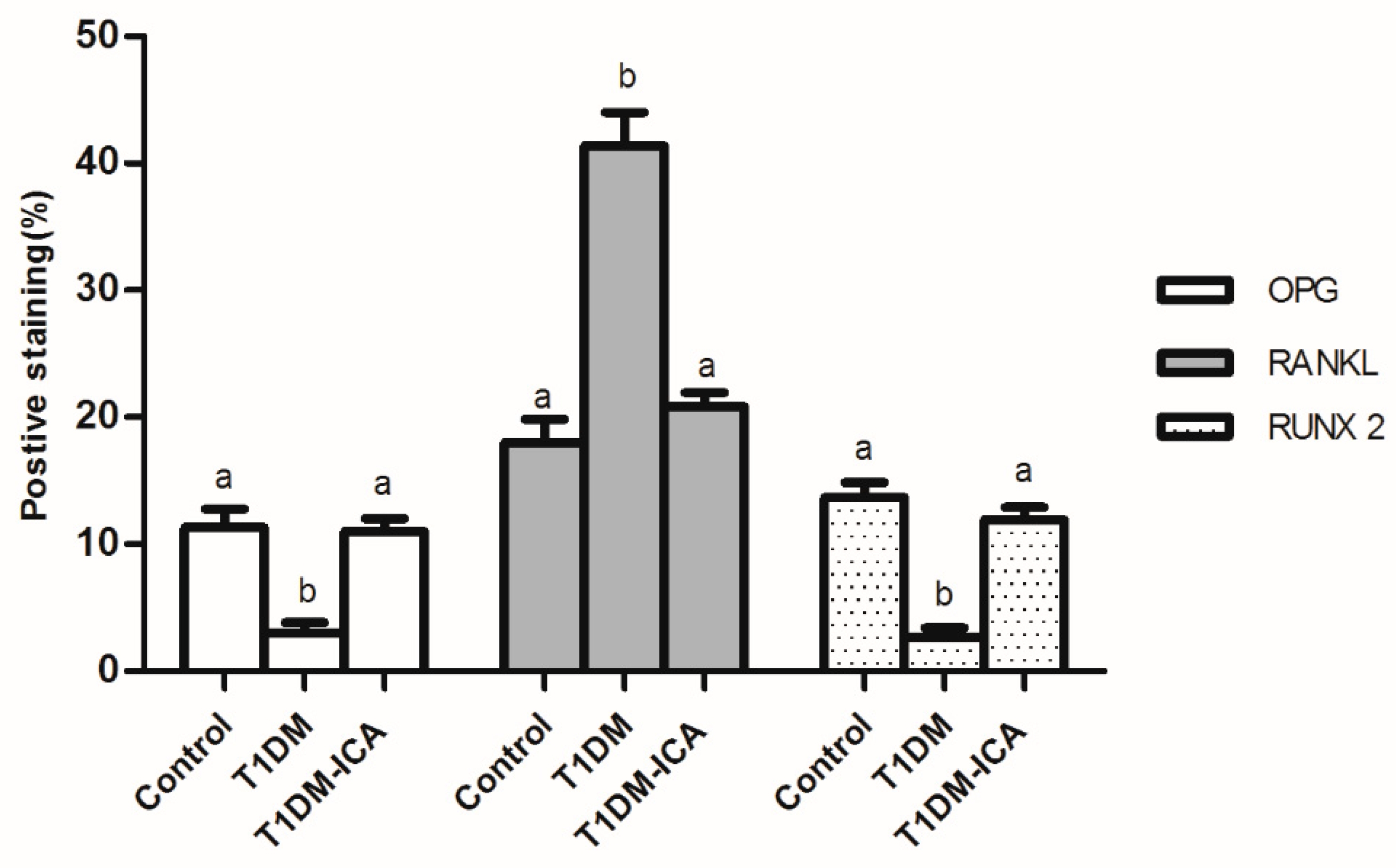
2.7. ICA Increased RUNX 2, OPG and Decreased RANKL Protein Expression in Bone Tissues of Diabetic Rats
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Establishment of Rat Model of Diabetes and ICA Administration
4.3. Serum Bone Turnover Markers, Ca, P, OPG, RANKL, and RUNX 2 Detection
4.4. Bone Mineral Density Measurement
4.5. Bone Histomorphometric Analysis
4.6. Bone Marrow Adipocyte Parameters Analysis
4.7. Immunohistochemistry
4.8. Quantitative Real-Time PCR
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ishtaya, G.A.; Anabtawi, Y.M.; Zyoud, S.H.; Sweileh, W.M. Osteoporosis knowledge and beliefs in diabetic patients: A cross sectional study from Palestine. BMC Musculoskel. Dis. 2018, 19, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chu, S.; Zhao, H. Effect of Zishen Jiangtang pill, a Chinese herbal product, on rats with diabetic osteoporosis. Evid-Based Compl. Alt. Med. 2018, 3, 1–10. [Google Scholar] [CrossRef]
- Wang, T.; Cai, L.; Wang, Y.; Lu, D.; Chen, H. The protective effects of silibinin in the treatment of streptozotocin-induced diabetic osteoporosis in rats. Biomed. Pharmacother. 2017, 89, 681–688. [Google Scholar] [CrossRef]
- Chandran, M.; Tay, D.; Huang, X.F.; Hao, Y. The burden of inpatient care for diabetic and non-diabetic patients with osteoporotic hip fractures—does it differ? An analysis of patients recruited into a fracture liaison service in Southeast Asia. Arch. Osteoporos. 2018, 13, 27–37. [Google Scholar] [CrossRef]
- Hygum, K.; Langdahl, B.L.; Staruplinde, J. Disentangling the association between diabetes and bone disease. Lancet Diabetes endocrinol. 2017, 5, 769–775. [Google Scholar] [CrossRef]
- Staruplinde, J.; Vestergaard, P. Management of endocrine disease: Diabetes and osteoporosis: Cause for concern? Eur. J. Endocrinol. 2015, 173, 93–99. [Google Scholar] [CrossRef]
- Gunter, M.J.; Hoover, D.R.; Yu, H. Insulin, insulin-like growth factor-I, and risk of breast cancer in postmenopausal women. J. Nat. Cancer Inst. 2009, 101, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.D.; Dixon, A.N.; Bain, S.C. Safety and side effects of the insulin analogues. Expert. Opin. Drug Saf. 2006, 5, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Sahasrabudhe, R.A.; Limaye, T.Y.; Gokhale, V.S. Insulin injection site adverse effect in a type 1 diabetes patient: An unusual presentation. J. Clin. Diagn. Res. 2017, 11, 10–19. [Google Scholar] [CrossRef]
- Both, T.; Zillikens, M.C.; Koedam, M. Hydroxychloroquine affects bone resorption both in vitro and in vivo. J. Cell Physiol. 2018, 233, 1424–1433. [Google Scholar] [CrossRef]
- Xue, L. Comparative effects of er-xian decoction, epimedium herbs, and icariin with estrogen on bone and reproductive tissue in ovariectomized rats. Evid-Based Compl. Alt. Med. 2012, 7, 24–33. [Google Scholar]
- Nian, H.; Ma, M.H.; Nian, S.S. Antiosteoporotic activity of icariin in ovariectomized rats. Phytomedicine 2009, 16, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Li, G.W.; Xu, Z.; Chang, S.X. Icariin prevents ovariectomy-induced bone loss and lowers marrow adipogenesis. Menopause 2014, 21, 1007–1016. [Google Scholar] [CrossRef]
- Wu, J.Z.; Liu, P.C.; Liu, R. Icariin restores bone structure and strength in a rat model of chronic high-dose alcohol-induced osteopenia. Cell Physiolo. Biochem. 2018, 4, 1727–1736. [Google Scholar] [CrossRef]
- He, J.P.; Feng, X.; Wang, J.F.; Shi, W.G.; Li, H.; Danilchenko, S.; Kalinkevich, A.; Zhovner, M. Icariin prevents bone loss by inhibiting bone resorption and stabilizing bone biological apatite in a hindlimb suspension rodent model. Acta Pharmacol. Sinica 2018, 39, 1760–1767. [Google Scholar] [CrossRef]
- Hye, K.D.; Ah, J.H.; Sook, S.H. Potential of icariin metabolites from epimedium koreanum nakai as antidiabetic therapeutic agents. Molecules 2017, 22, 986. [Google Scholar]
- Han, Y.; Jung, H.W.; Park, Y.K. Effects of Icariin on insulin resistance via the activation of AMPK pathway in C2C12 mouse muscle cells. Eur. J. Pharmacol. 2015, 758, 60–63. [Google Scholar] [CrossRef]
- Qia, M.Y.; Kai, C.; Liub, H.R.; Sua, Y.H.; Yua, S.Q. Protective effect of Icariin on the early stage of experimental diabetic nephropathy induced by streptozotocin via modulating transforming growth factor β 1, and type IV collagen expression in rats. J. Ethnopharmacol. 2011, 138, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Zhou, F.; Liu, T.; Li, G.Y. Icariin ameliorates streptozotocin-induced diabetic retinopathy in vitro and in vivo. Int. J. Mol. Sci. 2012, 13, 866–878. [Google Scholar]
- Schwartz, A.V. Clinical aspects of diabetic bone disease: An update. Clin. Rev. Bone Min. Metab. 2013, 11, 17–27. [Google Scholar] [CrossRef]
- Dhaon, P.; Shah, V.N. Type 1 diabetes and osteoporosis: A review of literature. Indian J. Endocrinol. Metab. 2014, 18, 159–165. [Google Scholar] [CrossRef]
- Jørgensen, M.B.; Christensen, J.O.; Svendsen, O.L. Bone loss in women with type 1 diabetes. J. Diabetes Mellit. 2015, 12, 252–257. [Google Scholar] [CrossRef]
- Hamann, C.; Kirschner, S.; KlausPeter, G. Bone, sweet bone osteoporotic fractures in diabetes mellitus. Nat. Rev. Endocrinol. 2012, 8, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Piscitelli, P.; Neglia, C.; Vigilanza, A.; Colao, A. Diabetes and bone: Biological and environmental factors. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 439–445. [Google Scholar] [CrossRef]
- Roy, B. Biomolecular basis of the role of diabetes mellitus in osteoporosis and bone fractures. World J. Diabetes 2013, 4, 101–113. [Google Scholar] [CrossRef]
- Carvalho, A.L.; Demambro, V.E.; Guntur, A.R. High fat diet attenuates hyperglycemia, body composition changes, and bone loss in male streptozotocin-induced type 1 diabetic mice. J. Cell Physiol. 2018, 233, 1585–1596. [Google Scholar] [CrossRef] [PubMed]
- Jiao, H.; Xiao, E.; Graves, D.T. Diabetes and its effect on bone and fracture healing. Curr. Osteoporos Rep. 2015, 13, 327–335. [Google Scholar] [CrossRef]
- Liu, Y.; Zuo, H.; Liu, X. The antiosteoporosis effect of icariin in ovariectomized rats: A systematic review and meta-analysis. Cell Mol. Biol. 2017, 63, 124–134. [Google Scholar] [CrossRef]
- Mok, S.K.; Chen, W.F.; Lai, W.P. Icariin protects against bone loss induced by oestrogen deficiency and activates oestrogen receptor-dependent osteoblastic functions in UMR 106 cells. Briti. J. Pharmacol. 2010, 159, 934–949. [Google Scholar] [CrossRef]
- Rufeng, M.; Ruyuan, Z.; Lili, W. Diabetic osteoporosis: A review of its traditional Chinese medicinal use and clinical and preclinical research. Evid-Based Compl. Alt. Med. 2016, 2016, 1–13. [Google Scholar]
- Schwartz, A.V. Efficacy of osteoporosis therapies in diabetic patients. Calcif. Tissue Int. 2017, 100, 165–173. [Google Scholar] [CrossRef]
- Dai, Z.; Wang, R.; Ang, L.W.; Yuan, J.M.; Koh, W.P. Bone turnover biomarkers and risk of osteoporotic hip fracture in an asian population. Bone 2016, 83, 171–177. [Google Scholar] [CrossRef]
- Delmas, P.D.; Eastell, R.; Garnero, P.; Seibel, M.J.; Stepan, J. The use of biochemical markers of bone turnover in osteoporosis. Osteoporos Int. 2000, 11, 2–17. [Google Scholar] [CrossRef]
- Garnero, P.; Sornay-Rendu, E.; Chapuy, M.C.; Delmas, P.D. Increased bone turnover in late postmenopausal women is a major determinant of osteoporosis. J. Bone Miner Res. 1996, 11, 337–349. [Google Scholar] [CrossRef]
- Lumachi, F.; Ermani, M.; Camozzi, V.; Tombolan, V.; Luisetto, G. Changes of bone formation markers osteocalcin and bone-specific alkaline phosphatase in postmenopausal women with osteoporosis. Ann. N. Y. Acad. Sci. 2009, 1173, E60–E63. [Google Scholar] [CrossRef] [PubMed]
- Halleen, J.M.; Tiitinen, S.L.; Ylipahkala, H. Tartrate-resistant acid phosphatase 5b (TRACP 5b) as a marker of bone resorption. Clin. Lab. 2006, 52, 499–509. [Google Scholar] [PubMed]
- Rosen, H.N.; Moses, A.C.; Garber, J.; Iloputaife, I.D.; Ross, D.S. Serum CTX: A new marker of bone resorption that shows treatment effect more often than other markers because of low coefficient of variability and large changes with bisphosphonate therapy. Calcif. Tissue Int. 2000, 66, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Halleen, J.M.; Ylipahkala, H.; Alatalo, S.L.; Janckila, A.J.; Heikkinen, J.E. Serum tartrate-resistant acid phosphatase 5b, but not 5a, correlates with other markers of bone turnover and bone mineral density. Calcif. Tissue Int. 2002, 71, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Kasai, H.; Ose, A.; Serada, M.; Ishiguro, M. Modeling and simulation of bone mineral density in Japanese osteoporosis patients treated with zoledronic acid using tartrate-resistant acid phosphatase 5b, a bone resorption marker. Osteoporos. Int. 2018, 29, 1155–1168. [Google Scholar] [CrossRef]
- Jayusman, P.A.; Mohame, I.N. The effects of quassinoid-rich eurycoma longifolia extract on bone turnover and histomorphometry indices in the androgen-deficient osteoporosis rat model. Nutrients 2018, 10, 799. [Google Scholar] [CrossRef]
- Stenström, M.; Olander, B.; Lehtoaxtelius, D. Bone mineral density and bone structure parameters as predictors of bone strength: An analysis using computerized microtomography and gastrectomy-induced osteopenia in the rat. J. Biomech. 2000, 33, 289–297. [Google Scholar] [CrossRef]
- Justesen, J.; Stenderup, K.; Ebbesen, E.N.; Li, M.; Steiniche, T. Adipocyte tissue volume in bone marrow is increased with aging and in patients with osteoporosis. Biogerontology 2001, 2, 165–171. [Google Scholar] [CrossRef]
- Pino, A.M.; Miranda, M.; Figueroa, C.; Rodríguez, J.P.; Rosen, C.J. Qualitative aspects of bone marrow adiposity in osteoporosis. Front Endocrinol. 2016, 7, 139–149. [Google Scholar] [CrossRef]
- Paccou, J.; Hardouin, P.; Cotten, A.; Penel, G.; Cortet, B. The role of bone marrow fat in skeletal health: Usefulness and perspectives for clinicians. J. Clin. Endocrinol. Metab. 2015, 100, 3613–3621. [Google Scholar] [CrossRef]
- Li, J.; Liu, X.; Zuo, B.; Zhang, L. The role of bone marrow microenvironment in governing the balance between osteoblastogenesis and adipogenesis. Aging Dis. 2015, 7, 514–525. [Google Scholar] [CrossRef]
- Komori, T. Runx2, an inducer of osteoblast and chondrocyte differentiation. Histochem. Cell Biol. 2018, 149, 313–323. [Google Scholar] [CrossRef]
- Fan, F.; Shi, P.; Liu, M. Lactoferrin preserves bone homeostasis by regulating the RANKL/RANK/OPG pathway of osteoimmunology. Food Funct. 2018, 9, 2653–2660. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef]
- Alfaqih, M.A.; Bashir, N.; Saadeh, R.; Khader, Y.; Barqawi, M.; Alqudah, S. Dysregulation of the RANKL/RANK/OPG axis in thalassemia intermedia patients. BMC Res. Not. 2018, 11, 534–545. [Google Scholar] [CrossRef]
- Chen, C.; Zheng, H.X.; Qi, S.S. Genistein and silicon synergistically protects against ovariectomy-induced bone loss through upregulating OPG/RANKL ratio. Biol. Trace Elem. Res. 2019, 188, 441–450. [Google Scholar] [CrossRef]
- Zheng, H.X.; Chen, C.; Qi, S.S. Salidroside improves bone histomorphology and prevents bone loss in ovariectomized diabetic rats by upregulating the OPG/RANKL ratio. Molecules 2018, 9, 2398. [Google Scholar] [CrossRef]
- Zhang, J.; Song, J.; Shao, J. Icariin attenuates glucocorticoid-induced bone deteriorations, hypocalcemia and hypercalciuria in mice. Int. J. Clin. Exp. Med. 2015, 8, 7306–7314. [Google Scholar]
- Qi, S.S. Synergistic effects of genistein and zinc on bone metabolism and the femoral metaphyseal histomorphology in the ovariectomized rats. Biol. Trace Elem. Res. 2017, 37, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.S.; Chen, C.; Zheng, H.X.; Jiang, H. Du-Zhong (Eucommia ulmoides Oliv.) cortex extract alleviates lead acetate-induced bone loss in rats. Biol. Trace Elem. Res. 2019, 187, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Lee, J.H.; Lee, G.S. Sophorae Flos extract inhibits RANKL-induced osteoclast differentiation by suppressing the NF-κB/NFATc1 pathway in mouse bone marrow cells. BMC Complem. Alter. Med. 2017, 17, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Li, G.W.; Xu, Z.; Chang, S.X. Influence of early zoledronic acid administration on bone marrow fat in ovariectomized rats. Endocrinology 2014, 155, 4731–4738. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the compounds are available from the authors. |










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | T1DM | T1DM-ICA |
|---|---|---|---|
| Glucose (mg/dL) | 88.56 ± 7.41 a | 417.34 ± 29.64 b | 98.45 ± 9.04 a |
| ALP (U/dL) | 104.31 ±10.91 a | 200.56 ± 18.59 b | 118.78 ± 11.78 a |
| CTX-1 (ng/mL) | 24.31 ± 4.07 a | 107.96 ± 13.67 b | 30.56 ± 4.16 a |
| Osteocalcin (ng/mL) | 17.39 ± 2.91 a | 43.16 ± 6.55 b | 25.76 ± 4.18 c |
| TRACP 5b (U/L) | 1.79 ± 0.33 a | 3.90 ± 0.72 b | 2.21 ± 0.43 a |
| PINP (μg/L) | 44.78 ± 6.01 a | 70.84 ± 7.89 b | 46.90 ± 6.01 a |
| Parameter | Control | T1DM | T1DM-ICA |
|---|---|---|---|
| Ca (mg/dL) | 9.49 ± 0.82 a | 4.74 ± 0.63 b | 9.45 ± 0.70 a |
| P (mg/dL) | 7.69 ± 0.45 a | 3.89 ± 0.65 b | 5.89 ± 0.56 c |
| RUNX 2 (ng/mL) | 10.96 ± 2.18 a | 3.18 ± 0.54 b | 9.64 ± 1.96 a |
| OPG (ng/mL) | 8.79 ± 2.54 a | 2.17 ± 0.61 b | 8.42 ± 1.35 a |
| RANKL (ng/mL) | 2.33 ± 0.46 a | 7.49 ± 1.21 b | 2.49 ± 0.38 a |
| OPG/RANKL ratio | 4.21 ± 0.51 a | 0.54 ± 0.10 b | 3.78 ± 0.46 a |
| Primer Name | Primer Sequence (5–3′) |
|---|---|
| β-actin-F | GAG ACC TTC AAC ACC CCA GCC |
| β-actin-R | GGC CAT CTC TTG CTC GAA GTC |
| RUNX 2-F | CGA AAT GCC TCT GCT GTT AT |
| RUNX 2-R | TTC TGT CTG TGC CTT CTT GG |
| OPG-F | ATG TAC GCA CTC AAG CAC TT |
| OPG-R | AAA GAG TTT CTG ATA CAA TCG GTA C |
| RANKL-F | TTT CAA GGG GCC GTG CAA AG |
| RANKL-R | AGC CAC GAA CCT TCC ATC ATA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, S.; He, J.; Zheng, H.; Chen, C.; Lan, S. Icariin Prevents Diabetes-Induced Bone Loss in Rats by Reducing Blood Glucose and Suppressing Bone Turnover. Molecules 2019, 24, 1871. https://doi.org/10.3390/molecules24101871
Qi S, He J, Zheng H, Chen C, Lan S. Icariin Prevents Diabetes-Induced Bone Loss in Rats by Reducing Blood Glucose and Suppressing Bone Turnover. Molecules. 2019; 24(10):1871. https://doi.org/10.3390/molecules24101871
Chicago/Turabian StyleQi, Shanshan, Jia He, Hongxing Zheng, Chen Chen, and Shiqiang Lan. 2019. "Icariin Prevents Diabetes-Induced Bone Loss in Rats by Reducing Blood Glucose and Suppressing Bone Turnover" Molecules 24, no. 10: 1871. https://doi.org/10.3390/molecules24101871
APA StyleQi, S., He, J., Zheng, H., Chen, C., & Lan, S. (2019). Icariin Prevents Diabetes-Induced Bone Loss in Rats by Reducing Blood Glucose and Suppressing Bone Turnover. Molecules, 24(10), 1871. https://doi.org/10.3390/molecules24101871