Salidroside Improves Bone Histomorphology and Prevents Bone Loss in Ovariectomized Diabetic Rats by Upregulating the OPG/RANKL Ratio

Abstract
1. Introduction
2. Results
2.1. Body Weight
2.2. Bone Mineral Density Evaluation of Lumbar Vertebrae and Femur
2.3. Serum Glucose, Ca, P, OPG, RANKL, and Bone Turnover Markers
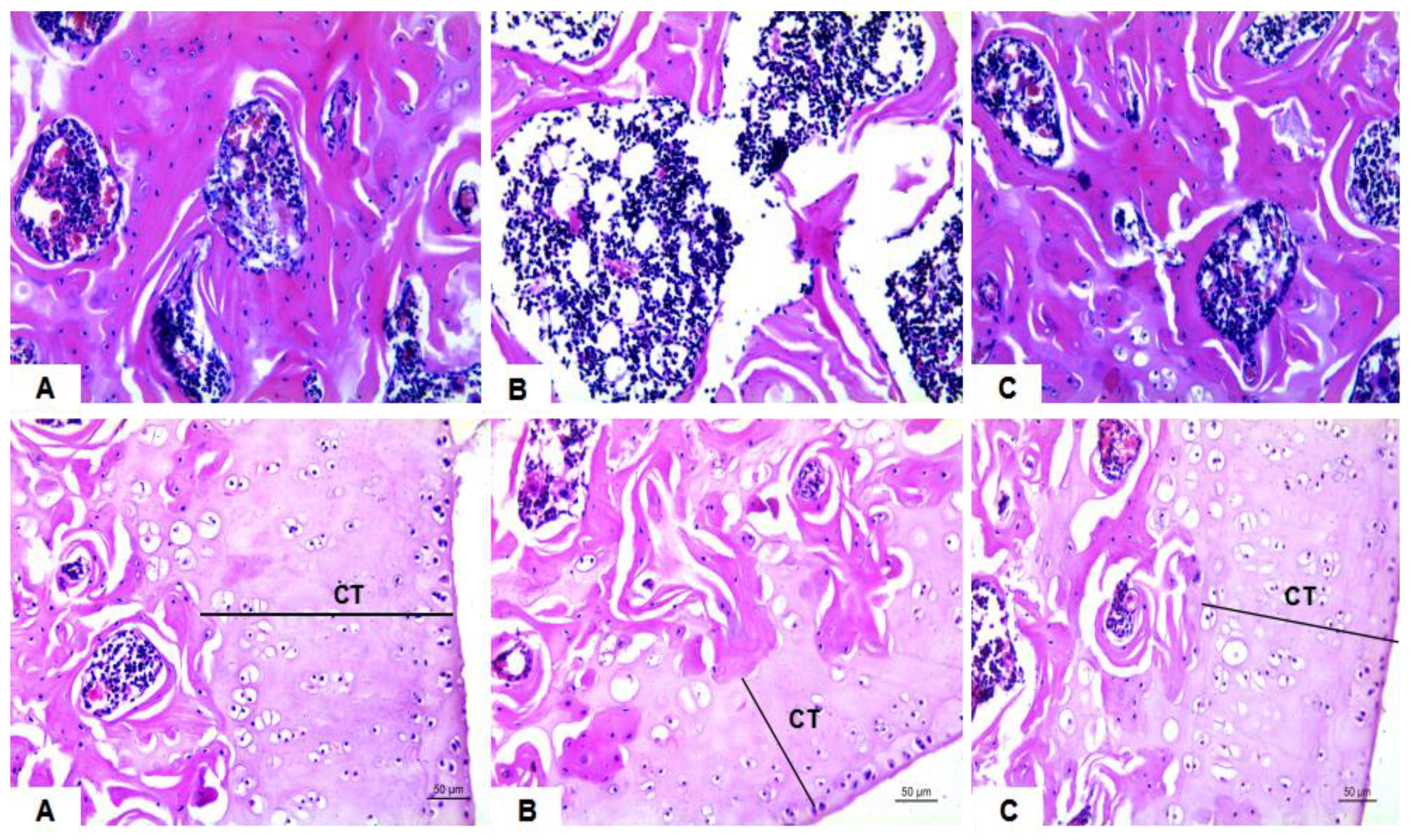
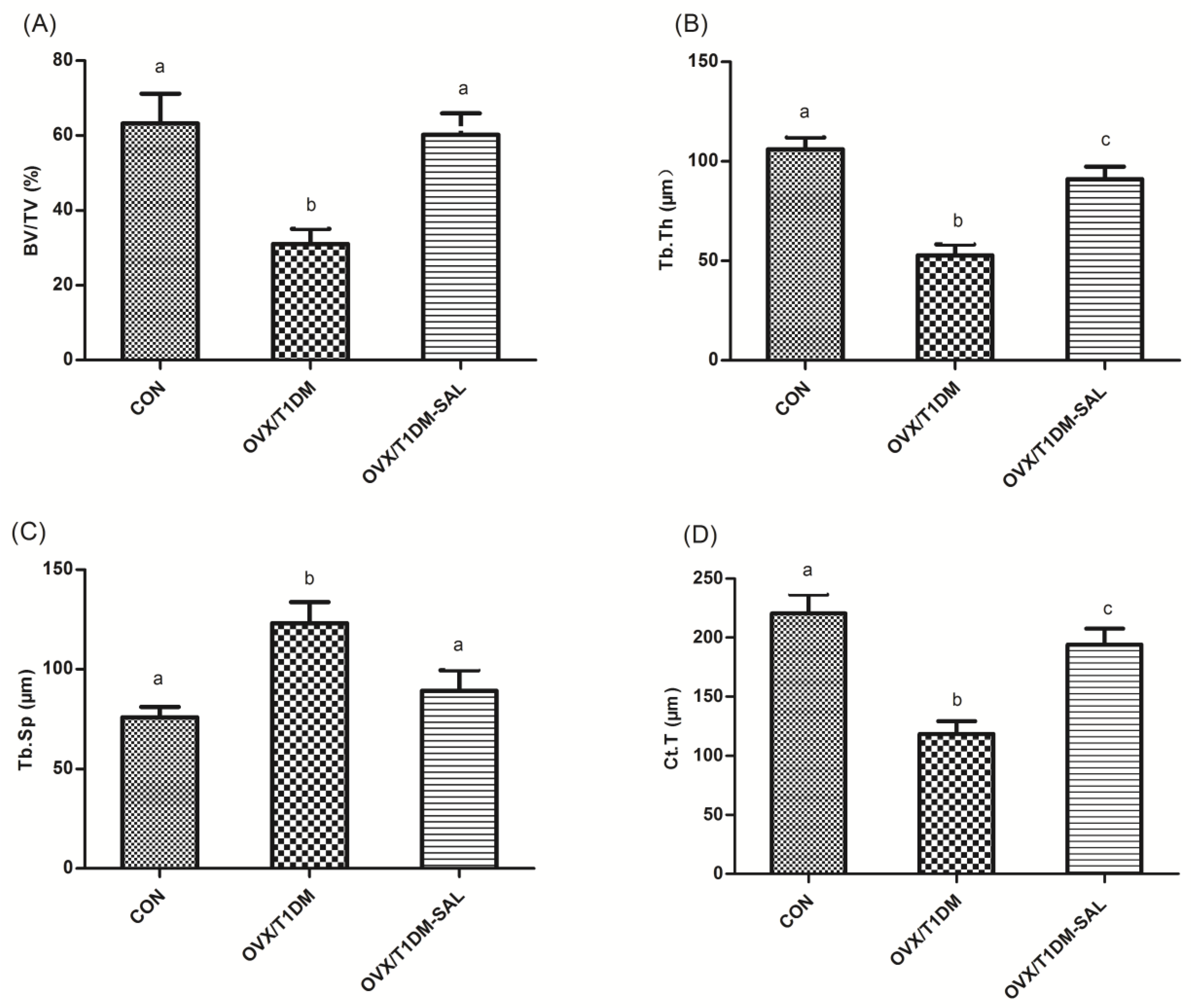
2.4. Morphological and Histomorphometrical Analysis of Femoral Trabecula
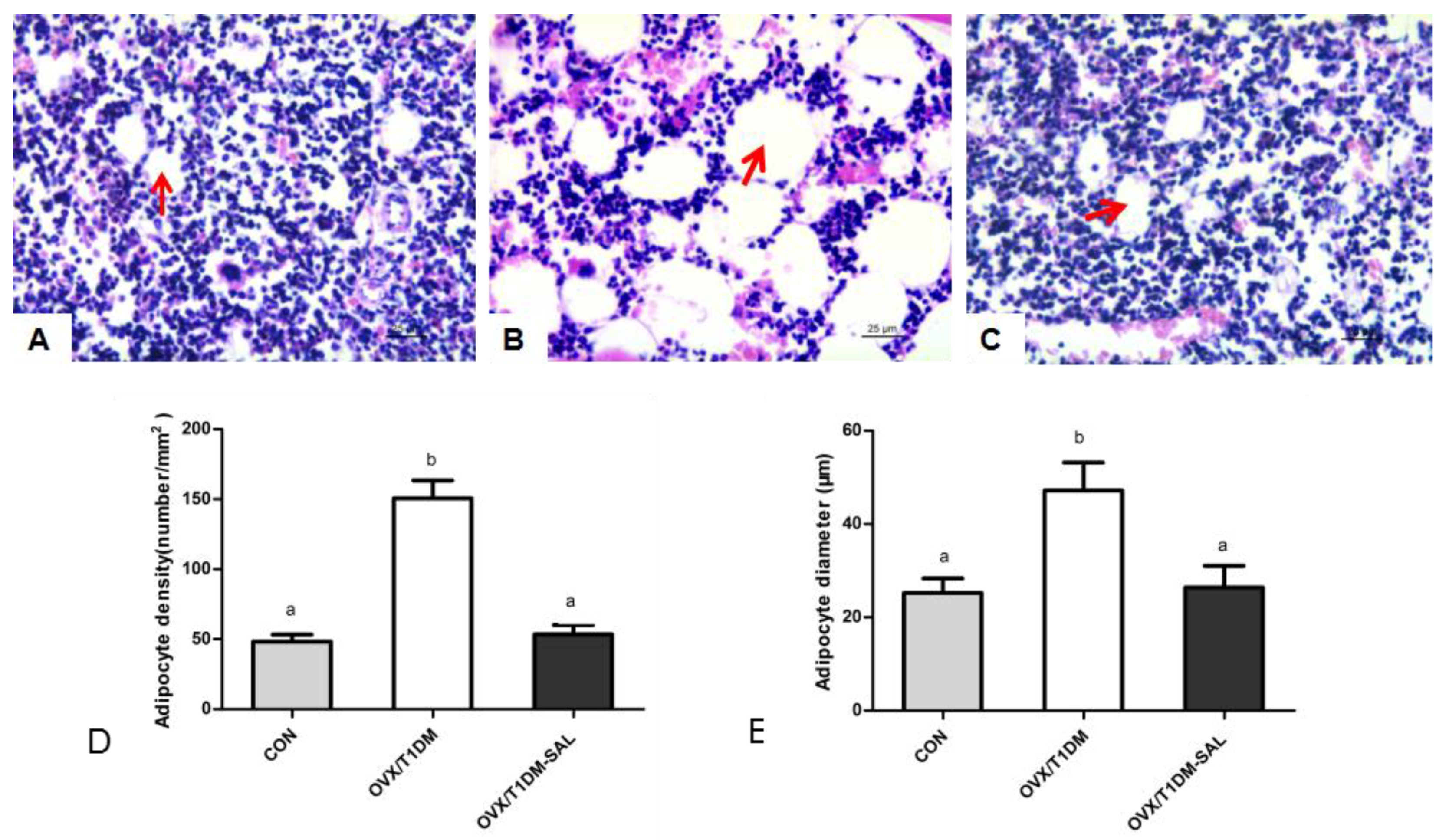
2.5. Adipocyte Density and Mean Adipocyte Diameter in the Femur Bone Marrow
2.6. The OPG and RANKL mRNA Expression in Bone Tissues, and OPG/RANKL mRNA Ratio in Bone Tissues
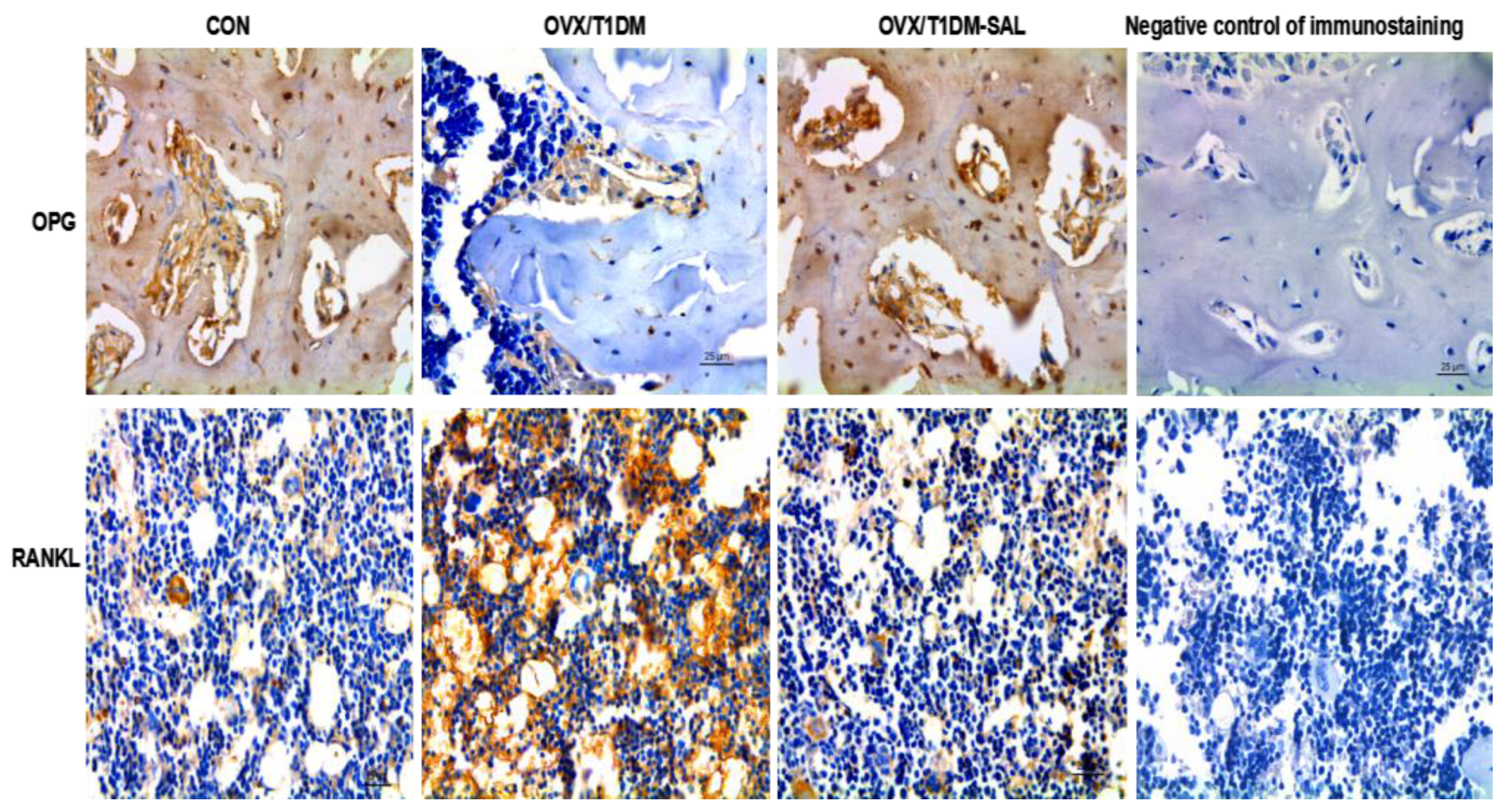
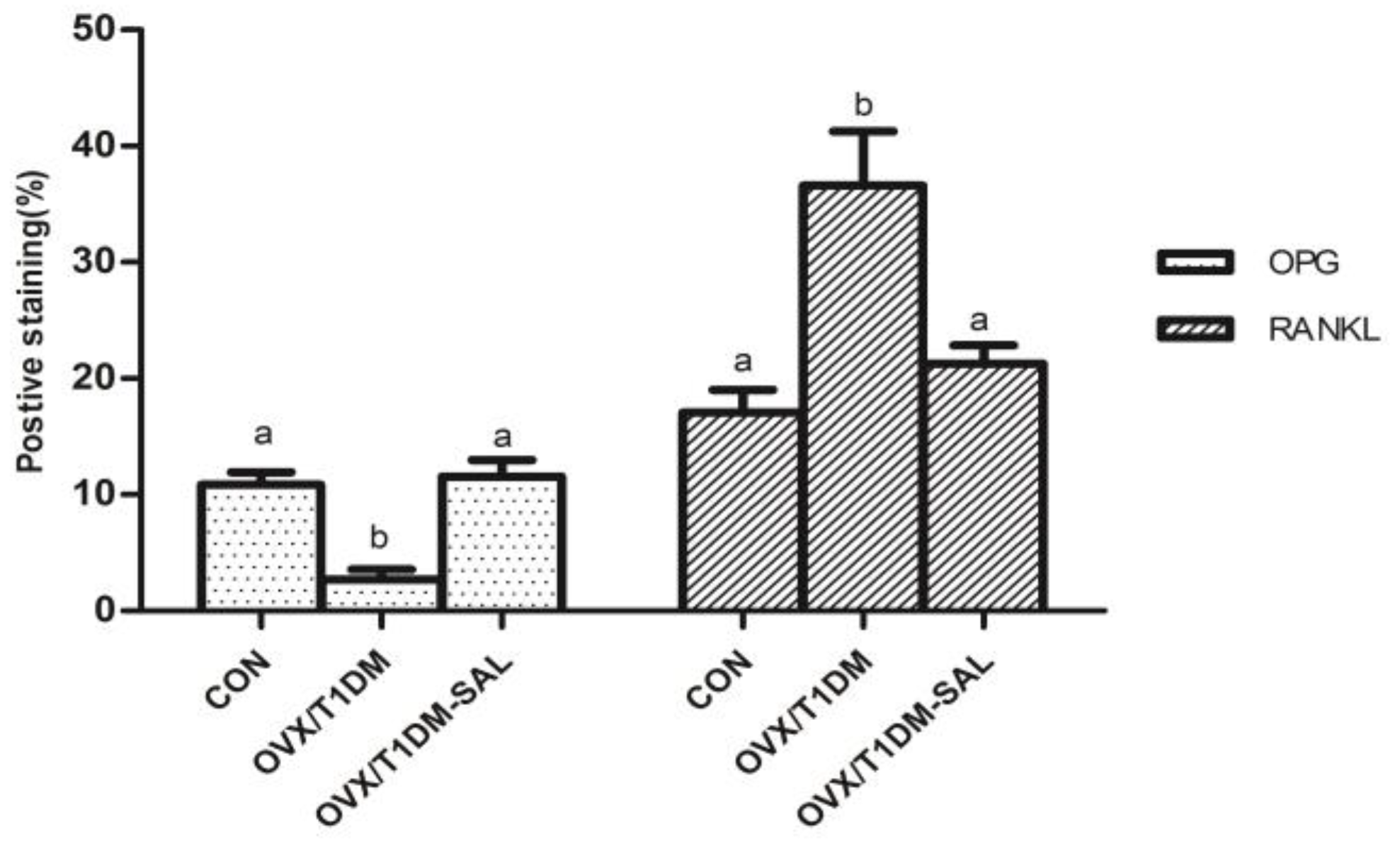
2.7. The OPG and RANKL Protein Expression in the Bone Tissues of Rats in Each Group
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Animals and Treatments
4.3. Assay of Ca, P, OPG, RANKL, and Bone Turnover Markers in Serum
4.4. Bone Mineral Density (BMD) Detection
4.5. Bone Histopathology and Histomorphometric Analysis
4.6. Bone Marrow Adipocyte Parameters Analysis
4.7. Immunohistochemistry for OPG and RANKL Detection
4.8. RT-PCR Analysis of OPG and RANKL mRNA Expression in Bone Tissues
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lane, N.E. Epidemiology, etiology, and diagnosis of osteoporosis. Am. J. Obstet. Gynecol. 2006, 194, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; McCloskey, E.V.; Harvey, N.C.; Johansson, H.; Leslie, W.D. Intervention thresholds and the diagnosis of osteoporosis. J. Bone Miner. Res. 2015, 30, 1747–1753. [Google Scholar] [CrossRef] [PubMed]
- Barzel, U.S. Estrogens in the prevention and treatment of postmenopausal osteoporosis: A. review. Am. J. Med. 1988, 85, 847–850. [Google Scholar] [CrossRef]
- Jackson, R.D.; Mysiw, W.J. Insights into the epidemiology of postmenopausal osteoporosis: The Women’s Health Initiative. Semin. Reprod. Med. 2014, 32, 454–462. [Google Scholar] [PubMed]
- Schacter, G.I.; Leslie, W.D. Diabetes and bone disease. Endocrinol. Metab. Clin. N. Am. 2017, 46, 63–85. [Google Scholar] [CrossRef] [PubMed]
- Neglia, C.; Argentiero, A.; Chitano, G.; Agnello, N.; Ciccarese, R.; Vigilanza, A.; Pantile, V.; Argentiero, D.; Quarta, R.; Rivezzi, M.; et al. Diabetes and obesity as independent risk factors for osteoporosis: Updated results from the ROIS/EMEROS registry in a population of five thousand post-menopausal women living in a region characterized by heavy environmental pressure. Int. J. Environ. Res. Public. Health 2016, 13, 1067. [Google Scholar] [CrossRef] [PubMed]
- Al-Hariri, M. Sweet bones: The pathogenesis of bone alteration in diabetes. J. Diabetes Res. 2016, 1, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.B.; Christensen, J.O.; Svendsen, O.L. Bone Loss in Women with Type 1 Diabetes. J. Diabetes Mellit. 2015, 5, 252–257. [Google Scholar] [CrossRef]
- Piscitelli, P.; Neglia, C.; Vigilanza, A. Diabetes and bone: Biological and environmental factors. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Raehtz, S.; Bierhalter, H.; Schoenherr, D. Estrogen deficiency exacerbates type 1 diabetes-induced bone TNF-α expression and osteoporosis in female mice. Endocrinology 2017, 158, 2086–2101. [Google Scholar] [CrossRef] [PubMed]
- Fukuharu, M.; Sato, J.; Ohsawa, I. Additive effects of estrogen deficiency and diabetes on bone mineral density in rats. Diabetes Res. Clin. Pract. 2000, 48, 1–8. [Google Scholar]
- Fuhrman, B.J.; Schairer, C.; Gail, M.H. Estrogen metabolism and risk of breast cancer in postmenopausal women. J. Natl. Cancer Inst. 2012, 104, 326–339. [Google Scholar] [CrossRef] [PubMed]
- Gunter, M.J.; Hoover, D.R.; Yu, H. Insulin, insulin-like growth factor-I., and risk of breast cancer in postmenopausal women. J. Natl. Cancer Inst. 2009, 101, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Si, X.P.; Huang, J.; Han, J.; Liang, X.; Xu, X.B.; Wang, Y.T.; Li, G.Y.; Wang, H.Y.; Wang, J.H. Preventive effects of Rhodiola rosea L. on bleomycin-induced pulmonary fibrosis in rats. Int. J. Mol. Sci. 2016, 17, 89. [Google Scholar] [CrossRef] [PubMed]
- Fan, X.J.; Wang, Y.; Wang, L.; Zhu, M. Salidroside induces apoptosis and autophagy in human colorectal cancer cells through inhibition of PI3K/Akt/mTORpathway. Oncol. Rep. 2016, 36, 3559–3567. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.T.; Wu, Z.H.; Wei, Y.; Dai, J.J.; Yu, G.F.; Yuan, F.; Ye, L.C. Induction of autophagy by salidroside through the AMPK-mTOR pathway protects vascular endothelial cells from oxidative stress-induced apoptosis. Mol. Cell. Biochem. 2017, 425, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Qu, Y.; Jin, X.; Guo, X.Q.; Wang, Y.; Qi, L.; Yang, J.; Zhang, P.; Li, L.Z. Protective effect of salidroside against bone loss via hypoxia-inducible factor-1α pathway-induced angiogenesis. Sci. Rep. 2016, 6, 32131. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Tang, H.; Xiao, F.; Gong, J.; Peng, Y.; Meng, X. Protective effect of salidroside from Rhodiolae Radix on diabetes-induced oxidative stress in mice. Molecules 2011, 16, 9912–9924. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Li, Q.; Liu, Z.; Feng, J.; Li, J.; Han, Z.; Duan, Y. Antidiabetic potential of Rhodiola sachalinensis root extract in streptozotocin-induced diabetic rats. Methods Find. Exp. Clin. Pharmacol. 2009, 31, 375–381. [Google Scholar] [PubMed]
- Boyce, B.F.; Xing, L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res. Ther. 2007, 9 (Suppl. S1). [Google Scholar] [CrossRef] [PubMed]
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 15, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.G.; Zhang, X.; Zhou, Y.P.; Lu, C.; Thu, P.M.; Qian, C. Anhydroicaritin: A srebps inhibitor, inhibits rankl-induced osteoclastic differentiation and improves diabetic osteoporosis in STZ-induced mice. Eur. J. Pharmacol. 2017, 809, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Gao, R.; Lu, B.; Ran, Y.; Yang, Z.; Liu, J.; Li, R. Ghrelin protects against depleted uranium-induced bone damage by increasing osteoprotegerin/RANKL ratio. Toxicol. Appl. Pharm. 2018, 343, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Ejiri, S.; Tanaka, M.; Watanabe, N.; Anwar, R.B.; Yamashita, E. Estrogen deficiency and its effect on the jaw bones. J. Bone Miner. Metab. 2008, 26, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Cyran, W. Estrogen deficiency causing osteoporosis in older women. Fortschritte Der Medizin 1973, 91, 425. [Google Scholar] [PubMed]
- Hamann, C.; Kirschner, S.; Günther, K.P.; Hofbauer, L.C. Bone, sweet bone—Osteoporotic fractures in diabetes mellitus. Nat. Rev. Endocrinol. 2012, 8, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Weitzmann, M.N.; Pacifici, R. Estrogen deficiency and bone loss: An inflammatory tale. J. Clin. Investig. 2006, 116, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Danielson, K.K.; Elliott, M.E.; Lecaire, T.; Binkley, N.; Palta, M. Poor glycemic control is associated with low bmd detected in premenopausal women with type 1 diabetes. Osteoporos. Int. 2009, 20, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.S.; Fraser, L.A. Type 1 diabetes and osteoporosis: From molecular pathways to bone phenotype. J. Osteoporos. 2015, 2015, 174186. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Z.; Han, J.; Zhang, J.; Xiao, Q.; Hu, J.; Chen, L. Pharmacological activities, mechanisms of action, and safety of salidroside in the central nervous system. Drug Des. Dev. Ther. 2018, 12, 1479–1489. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wan, X.; Zhu, Y.; Ma, X.; Zheng, Y.; Zhang, T. Evaluation of salidroside in vitro and in vivo genotoxicity. Drug Chem. Toxicol. 2010, 33, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.P.; Zhang, T.B.; Wan, X. Genetic toxicity of rhodioside injection. Pharm. Care Res. 2009, 9, 279–282. [Google Scholar]
- Zhang, J.K.; Yang, L.; Meng, G.L.; Yuan, Z.; Fan, J.; Li, D.; Chen, J.Z.; Shi, T.Y.; Hu, H.M.; Wei, B.Y.; et al. Protection by salidroside against bone loss via inhibition of oxidative stress and bone-resorbing mediators. PLoS ONE 2013, 8, e57251. [Google Scholar] [CrossRef] [PubMed]
- Devogelaer, J.P.; Boutsen, Y.; Gruson, D.; Manicourt, D. Is there a place for bone turnover markers in the assessment of osteoporosis and its treatment? Rheum. Dis. Clin. N. Am. 2011, 37, 365–386. [Google Scholar] [CrossRef] [PubMed]
- Delmas, P.D.; Eastell, R.; Garnero, P.; Seibel, M.J.; Stepan, J. The use of biochemical markers of bone turnover in osteoporosis. Osteoporos. Int. 2000, 11, 2–17. [Google Scholar] [CrossRef]
- Garnero, P.; Sornay-Rendu, E.; Chapuy, M.C.; Delmas, P.D. Increased bone turnover in late postmenopausal women is a major determinant of osteoporosis. J. Bone Miner. Res. 1996, 11, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Lumachi, F.; Ermani, M.; Camozzi, V.; Tombolan, V.; Luisetto, G. Changes of bone formation markers osteocalcin and bone-specific alkaline phosphatase in postmenopausal women with osteoporosis. Ann. N. Y. Acad. Sci. 2009, 1173, E60–E63. [Google Scholar] [CrossRef] [PubMed]
- Szulc, P.; Naylor, K.; Hoyle, N.R.; Eastell, R.; Leary, E.T. Use of CTX-1 and PIPN as bone turnover markers: National bone health alliance recommendations to standardize sample handling and patient preparation to reduce pre-analytical variability. Osteoporos. Int. 2017, 28, 2541–2556. [Google Scholar] [CrossRef] [PubMed]
- Halleen, J.M.; Tiitinen, S.L.; Ylipahkala, H. Tartrate-resistant acid phosphatase 5b (TRACP 5b) as a marker of bone resorption. Clin. Lab. 2006, 52, 499–509. [Google Scholar] [PubMed]
- Meena, P.D.; Khatkhatay, M.I.; Prakash, K.V.B.; Savardekar, L.S.; Shah, R.S.; Ansari, Z. Hormonal profiles and biochemical indices of bone turnover in indian women. Osteoporos. Int. 2007, 18, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Halleen, J.M.; Ylipahkala, H.; Alatalo, S.L.; Janckila, A.J.; Heikkinen, J.E.; Suominen, H. Serum tartrate-resistant acid phosphatase 5b, but not 5a, correlates with other markers of bone turnover and bone mineral density. Calcif. Tissue Int. 2002, 71, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Justesen, J.; Stenderup, K.; Ebbesen, E.N.; Mosekilde, L.; Steiniche, T.; Kassem, M. Adipocyte tissue volume in bone marrow is increased with aging and in patients with osteoporosis. Biogerontology 2001, 2, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Dempster, D.W.; Stein, E.M.; Nickolas, T.L.; Zhou, H.; McMahon, D.J.; Müller, R.; Kohler, T.; Zwahlen, A.; Lappe, J.M.; et al. Increased marrow adiposity in premenopausal women with idiopathic osteoporosis. J. Clin. Endocrinol. Metab. 2012, 97, 2782–2791. [Google Scholar] [CrossRef] [PubMed]
- Paccou, J.; Hardouin, P.; Cotten, A.; Penel, G.; Cortet, B. The role of bone marrow fat in skeletal health: Usefulness and perspectives for clinicians. J. Clin. Endocrinol. Metab. 2015, 100, 3613–3621. [Google Scholar] [CrossRef] [PubMed]
- Cornish, J.L.; Wang, T.; Lin, J.M. Role of marrow adipocytes in regulation of energy metabolism and bone homeostasis. Curr. Osteoporos. Rep. 2018, 16, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Ando, K.; Mori, K.; Rédini, F. RANKL/RANK/OPG: Key therapeutic target in bone oncology. Curr. Drug Discov. Technol. 2008, 5, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Wolski, H.; Drews, K.; Bogacz, A.; Kamiński, A.; Barlik, M.; BartkowiakWieczorek, J.; Klejewski, A.; Ożarowski, M.; Majchrzycki, M.; Seremak-Mrozikiewicz, A. The RANKL/RANK/OPG signal trail: Significance of genetic polymorphisms in the etiology of postmenopausal osteoporosis. Ginekol. Pol. 2016, 87, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Indridason, O.S.; Franzson, L.; Sigurdsson, G. Serum osteoprotegerin and its relationship with bone mineral density and markers of bone turnover. Osteoporos. Int. 2005, 16, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Kostenuik, P.J. Osteoprotegerin and rankl regulate bone resorption, density, geometry and strength. Curr. Opin. Pharmacol. 2005, 5, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zheng, H.; Qi, S. Genistein and silicon synergistically protects against ovariectomy-induced bone loss through upregulating OPG/RANKL ratio. Biol. Trace Elem. Res. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lee, Y.J.; Kim, H.Y.; Tan, R.; Park, M.C.; Kang, D.G.; Lee, H.S. Beneficial effects of scutellaria baicalensis on penile erection in streptozotocin-induced diabetic rats. Am. J. Chin. Med. 2016, 44, 305–320. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.S. Synergistic effects of genistein and zinc on bone metabolism and the femoral metaphyseal histomorphology in the ovariectomized rats. Biol. Trace Elem. Res. 2017, 183, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.S.; Zheng, H.X. Combined effects of phytoestrogen genistein and silicon on ovariectomy-induced bone loss in rat. Biol. Trace Elem. Res. 2017, 177, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Kurabayashi, T.; Tomita, M.; Matsushita, H.; Honda, A.; Takakuwa, K.; Tanaka, K. Effects of a beta 3 a drenergic receptor agonist on bone and bone marrow adipocytes in the tibia and lumbar spine of the ovariectomized rat. Calcif. Tissue Int. 2001, 68, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Li, G.W.; Xu, Z.; Chang, S.X. Influence of early zoledronic acid administration on bone marrow fat in ovariectomized rats. Endocrinology 2014, 155, 4731–4738. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: Samples of the compounds are available from the authors. |









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | OVX/T1DM | OVX/T1DM-SAL |
|---|---|---|---|
| Glucose (mg/dL) | 90.46 ± 8.14 a | 444.92 ± 29.16 b | 102.39 ± 11.82 a |
| ALP (U/dL) | 102.23 ± 9.71 a | 189.56 ± 17.33 b | 121.67 ± 12.13 a |
| Ca (mg/dL) | 9.41 ± 0.98 a | 4.78 ± 0.57 b | 8.87 ± 0.91 a |
| P (mg/dL) | 6.54 ± 0.79 a | 3.76 ± 0.43 b | 5.01 ± 0.91 c |
| CTX-1 (ng/mL) | 21.43 ± 3.78 a | 104.32 ± 13.45 b | 30.78 ± 4.91 a |
| Osteocalcin (ng/mL) | 19.56 ± 3.59 a | 37.42 ± 4.89 b | 27.31 ± 3.18 c |
| TRACP 5b (U/L) | 1.74 ± 0.20 a | 3.02 ± 0.67 b | 1.97 ± 0.43 a |
| PINP (μg/L) | 40.35 ± 7.56 a | 51.21 ± 8.54 b | 42.67 ± 6.89 a |
| OPG (ng/mL) | 6.78 ± 1.90 a | 2.45 ± 0.56 b | 5.74 ± 0.69 a |
| RANKL (ng/mL) | 1.89 ± 0.56 a | 4.17 ± 0.98 b | 1.99 ± 0.51 a |
| OPG/RANKL ratio | 4.21 ± 0.54 a | 0.62 ± 0.11 b | 3.78 ± 0.37 a |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, H.; Qi, S.; Chen, C. Salidroside Improves Bone Histomorphology and Prevents Bone Loss in Ovariectomized Diabetic Rats by Upregulating the OPG/RANKL Ratio. Molecules 2018, 23, 2398. https://doi.org/10.3390/molecules23092398
Zheng H, Qi S, Chen C. Salidroside Improves Bone Histomorphology and Prevents Bone Loss in Ovariectomized Diabetic Rats by Upregulating the OPG/RANKL Ratio. Molecules. 2018; 23(9):2398. https://doi.org/10.3390/molecules23092398
Chicago/Turabian StyleZheng, Hongxing, Shanshan Qi, and Chen Chen. 2018. "Salidroside Improves Bone Histomorphology and Prevents Bone Loss in Ovariectomized Diabetic Rats by Upregulating the OPG/RANKL Ratio" Molecules 23, no. 9: 2398. https://doi.org/10.3390/molecules23092398
APA StyleZheng, H., Qi, S., & Chen, C. (2018). Salidroside Improves Bone Histomorphology and Prevents Bone Loss in Ovariectomized Diabetic Rats by Upregulating the OPG/RANKL Ratio. Molecules, 23(9), 2398. https://doi.org/10.3390/molecules23092398