
Transcranial Magnetic Stimulation for the Treatment of Cocaine Addiction: A Systematic Review


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.2.1. Design
2.2.2. Population
2.2.3. Intervention
2.2.4. Comparator
2.2.5. Outcomes
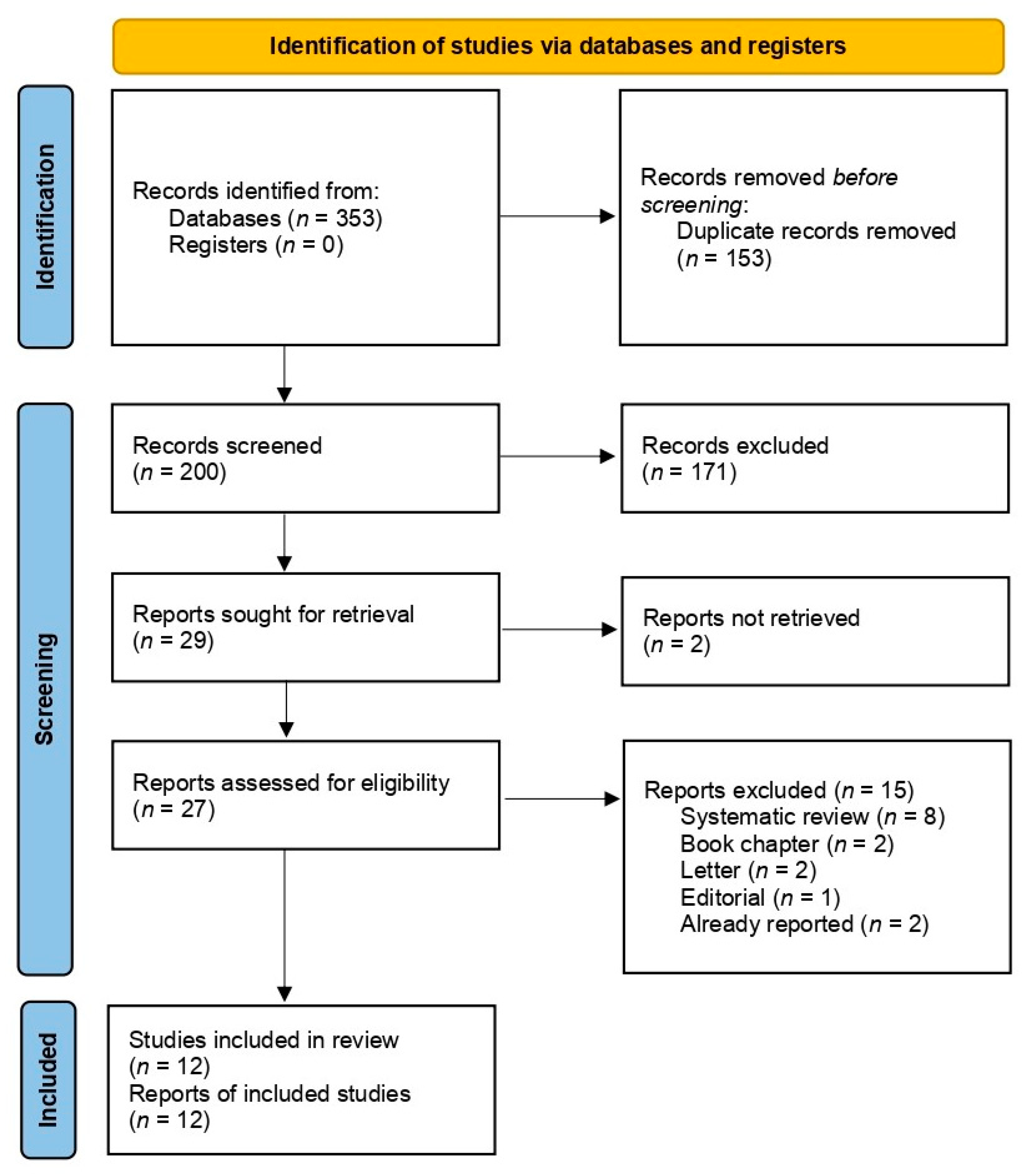
2.3. Study Selection
2.4. Data Extarction and Analysis
2.5. Quality Assessment
3. Results
3.1. Study Characteristics
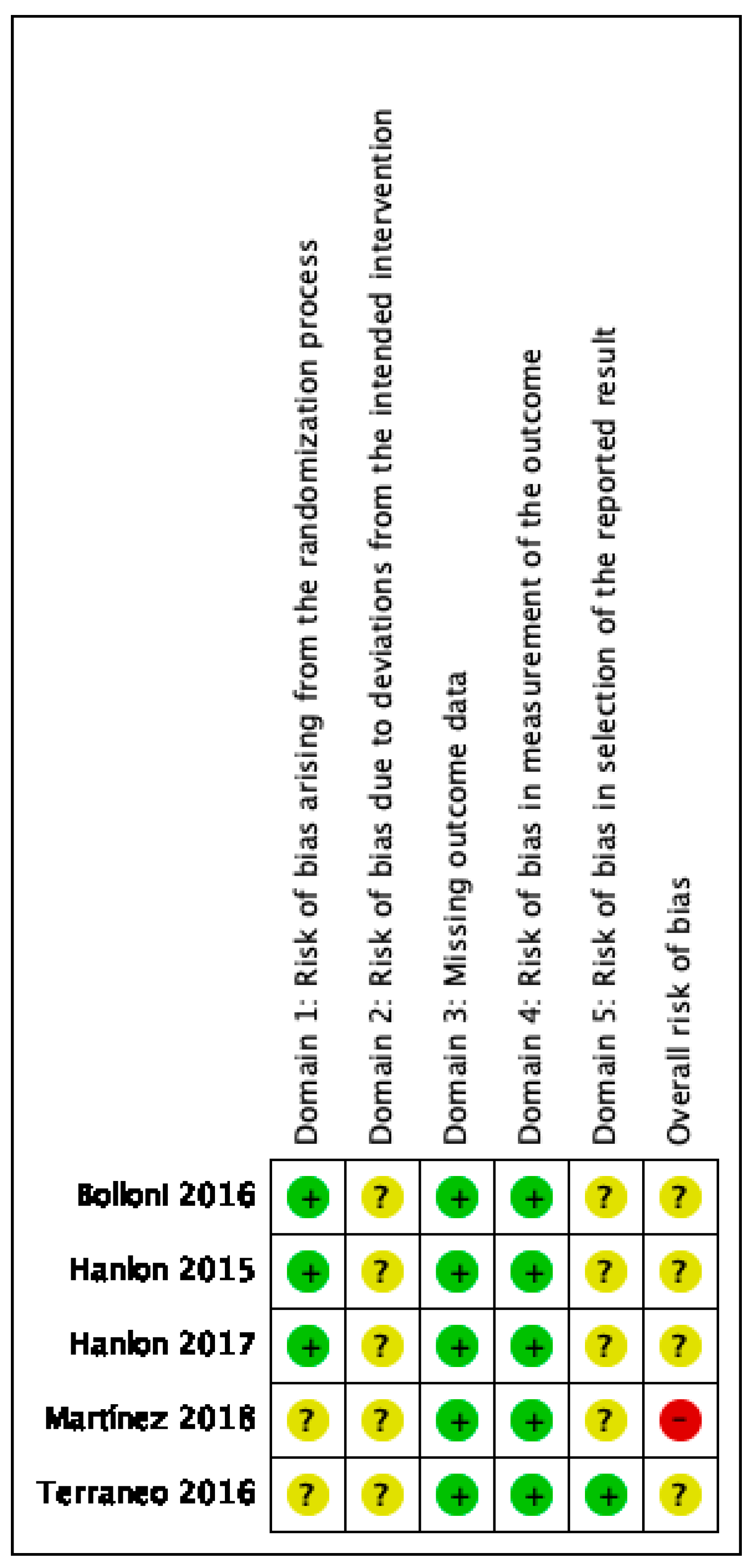
3.2. Quality Assessment
3.2.1. RCTs
3.2.2. nRCTs
3.2.3. Case-Series
3.3. Effectiveness of TMS
3.3.1. Dorsolateral Prefrontal Cortex Stimulation
3.3.2. Medial Prefrontal Cortex (MPFC) Stimulation
3.3.3. Comparison between Bilateral Deep Stimulation Protocols: iTBS vs. High Frequency rTMS
3.4. Evidence on the Safety of TMS for the Treatment of Cocaine Addiction
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Monitoring Centre for Drugs and Drug addiction Annual Overview of the European Drug Situation on 27 May in a Multilingual, Multimedia Information Package Focusing on Today’s Rapidly Shifting Drug Phenomenon, EMCDDA: 2014. Available online: https://www.emcdda.europa.eu/publications/edr/trends-developments/2014_en (accessed on 20 November 2020).
- United Nations, G.A. World Drug Report 2020. Report 2. Drug Use and Health Consequences; 2020. Available online: https://wdr.unodc.org/wdr2020/field/WDR20_Booklet_2.pdf (accessed on 23 November 2020).
- Volkow, N.D.; Fowler, J.S.; Wang, G.J.; Swanson, J.M. Dopamine in drug abuse and addiction: Results from imaging studies and treatment implications. Mol. Psychiatry 2004, 9, 557–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-López, L.; Catena, A.; Fernández-Serrano, M.J.; Delgado-Rico, E.; Stamatakis, E.A.; Pérez-García, M.; Verdejo-García, A. Trait impulsivity and prefrontal gray matter reductions in cocaine dependent individuals. Drug Alcohol Depend. 2012, 125, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Matochik, J.A.; London, E.D.; Eldreth, D.A.; Cadet, J.L.; Bolla, K.I. Frontal cortical tissue composition in abstinent cocaine abusers: A magnetic resonance imaging study. Neuroimage 2003, 19, 1095–1102. [Google Scholar] [CrossRef]
- Goldstein, R.Z.; Volkow, N.D. Dysfunction of the prefrontal cortex in addiction: Neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 2011, 12, 652–669. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.N.; Ross, T.J.; Stein, E.A.; Garavan, H. Cingulate hypoactivity in cocaine users during a GO-NOGO task as revealed by event-related functional magnetic resonance imaging. J. Neurosci. 2003, 23, 7839–7843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkow, N.D.; Fowler, J.S.; Wang, G.J. The addicted human brain: Insights from imaging studies. J. Clin. Invest. 2003, 111, 1444–1451. [Google Scholar] [CrossRef]
- Licata, S.C.; Renshaw, P.F. Neurochemistry of drug action: Insights from proton magnetic resonance spectroscopic imaging and their relevance to addiction. Ann. N. Y. Acad. Sci. 2010, 1187, 148–171. [Google Scholar] [CrossRef] [Green Version]
- Ke, Y.; Streeter, C.C.; Nassar, L.E.; Sarid-Segal, O.; Hennen, J.; Yurgelun-Todd, D.A.; Awad, L.A.; Rendall, M.J.; Gruber, S.A.; Nason, A.; et al. Frontal lobe GABA levels in cocaine dependence: A two-dimensional, J-resolved magnetic resonance spectroscopy study. Psychiatry Res.-Neuroimaging 2004, 130, 283–293. [Google Scholar] [CrossRef]
- Jasinska, A.J.; Chen, B.T.; Bonci, A.; Stein, E.A. Dorsal medial prefrontal cortex (MPFC) circuitry in rodent models of cocaine use: Implications for drug addiction therapies. Addict. Biol. 2015, 20, 215–226. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.T.; Yau, H.J.; Hatch, C.; Kusumoto-Yoshida, I.; Cho, S.L.; Hopf, F.W.; Bonci, A. Rescuing cocaine-induced prefrontal cortex hypoactivity prevents compulsive cocaine seeking. Nature 2013, 496, 359–362. [Google Scholar] [CrossRef]
- Terraneo, A.; Leggio, L.; Saladini, M.; Ermani, M.; Bonci, A.; Gallimberti, L. Transcranial magnetic stimulation of dorsolateral prefrontal cortex reduces cocaine use: A pilot study. Eur. Neuropsychopharmacol. 2016, 26, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Nutt, D.J.; Lingford-Hughes, A.; Erritzoe, D.; Stokes, P.R.A. The dopamine theory of addiction: 40 years of highs and lows. Nat. Rev. Neurosci. 2015, 16, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, C.A.; Dowdle, L.T.; Austelle, C.W.; Devries, W.; Mithoefer, O.; Badran, B.W.; George, M.S. What goes up, can come down: Novel brain stimulation paradigms may attenuate craving and craving-related neural circuitry in substance dependent individuals. Brain Res. 2015, 1628, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.J.; Sayette, M.A.; Fiez, J.A. Prefrontal responses to drug cues: A neurocognitive analysis. Nat. Neurosci. 2004, 7, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Rapinesi, C.; Del Casale, A.; Di Pietro, S.; Ferri, V.R.; Piacentino, D.; Sani, G.; Raccah, R.N.; Zangen, A.; Ferracuti, S.; Vento, A.E.; et al. Add-on high frequency deep transcranial magnetic stimulation (dTMS) to bilateral prefrontal cortex reduces cocaine craving in patients with cocaine use disorder. Neurosci. Lett. 2016, 629, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Bolloni, C.; Badas, P.; Corona, G.; Diana, M. Transcranial magnetic stimulation for the treatment of cocaine addiction: Evidence to date. Subst. Abuse Rehabil. 2018, Volume 9, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Ferenczi, E.; Deisseroth, K. Illuminating next-generation brain therapies. Nat. Neurosci. 2016, 19, 414–416. [Google Scholar] [CrossRef] [Green Version]
- Gómez Pérez, L.J.; Cardullo, S.; Cellini, N.; Sarlo, M.; Monteanni, T.; Bonci, A.; Terraneo, A.; Gallimberti, L.; Madeo, G. Sleep quality improves during treatment with repetitive transcranial magnetic stimulation (rTMS) in patients with cocaine use disorder: A retrospective observational study. BMC Psychiatry 2020, 20, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Dakwar, E.; Nunes, E.V.; Hart, C.L.; Foltin, R.W.; Mathew, S.J.; Carpenter, K.M.; Choi, C.J.; Basaraba, C.N.; Pavlicova, M.; Levin, F.R. A single ketamine infusion combined with mindfulness-based behavioral modification to treat cocaine dependence: A randomized clinical trial. Am. J. Psychiatry 2019, 176, 923–930. [Google Scholar] [CrossRef]
- Coles, A.S.; Kozak, K.; George, T.P. A review of brain stimulation methods to treat substance use disorders. Am. J. Addict. 2018, 27, 71–91. [Google Scholar] [CrossRef]
- Lefaucheur, J.P.; André-Obadia, N.; Antal, A.; Ayache, S.S.; Baeken, C.; Benninger, D.H.; Cantello, R.M.; Cincotta, M.; de Carvalho, M.; De Ridder, D.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin. Neurophysiol. 2014, 125, 2150–2206. [Google Scholar] [CrossRef]
- Barker, A.T.; Jalinous, R.; Freeston, I.L. Non-invasive magnetic stimulation of human motor cortex. Lancet 1985, 11, 1106–1107. [Google Scholar] [CrossRef]
- Terao, Y.; Ugawa, Y. Basic mechanisms of TMS. J. Clin. Neurophysiol. 2002, 19, 322–343. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.D.; Lisanby, S.H.; Peterchev, A.V. Coil design considerations for deep transcranial magnetic stimulation. Clin. Neurophysiol. 2014, 125, 1202–1212. [Google Scholar] [CrossRef] [Green Version]
- Roth, Y.; Amir, A.; Levkovitz, Y.; Zangen, A. Three-dimensional distribution of the electric field induced in the brain by transcranial magnetic stimulation using figure-8 and deep H-coils. J. Clin. Neurophysiol. 2007, 24, 31–38. [Google Scholar] [CrossRef]
- Cohen, L.G.; Roth, B.J.; Nilsson, J.; Dang, N.; Panizza, M.; Bandinelli, S.; Friauf, W.; Hallett, M. Effects of coil design on delivery of focal magnetic stimulation. Technical considerations. Electroencephalogr. Clin. Neurophysiol. 1990, 75, 350–357. [Google Scholar] [CrossRef]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef]
- Pascual-leone, A.; Valls-solé, J.; Wassermann, E.M.; Hallett, M. Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain 1994, 117, 847–858. [Google Scholar] [CrossRef]
- Daskalakis, Z.J.; Möller, B.; Christensen, B.K.; Fitzgerald, P.B.; Gunraj, C.; Chen, R. The effects of repetitive transcranial magnetic stimulation on cortical inhibition in healthy human subjects. Exp. Brain Res. 2006, 174, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, P.B.; Brown, T.L.; Daskalakis, Z.J. The application of transcranial magnetic stimulation in psychiatry and neurosciences research. Acta Psychiatr. Scand. 2002, 105, 324–340. [Google Scholar] [CrossRef]
- Huang, Y.Z.; Edwards, M.J.; Rounis, E.; Bhatia, K.P.; Rothwell, J.C. Theta burst stimulation of the human motor cortex. Neuron 2005, 45, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Bulteau, S.; Sébille, V.; Fayet, G.; Thomas-Ollivier, V.; Deschamps, T.; Bonnin-Rivalland, A.; Laforgue, E.; Pichot, A.; Valrivière, P.; Auffray-Calvier, E.; et al. Efficacy of intermittent Theta Burst Stimulation (iTBS) and 10-Hz high-frequency repetitive transcranial magnetic stimulation (rTMS) in treatment-resistant unipolar depression: Study protocol for a randomised controlled trial. Trials 2017, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A.; Avanzini, G.; Bestmann, S.; Berardelli, A.; Brewer, C.; Canli, T.; Cantello, R.; et al. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef] [Green Version]
- Rossi, S.; Antal, A.; Bestmann, S.; Bikson, M.; Brewer, C.; Brockmöller, J.; Carpenter, L.L.; Cincotta, M.; Chen, R.; Daskalakis, J.D.; et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert Guidelines. Clin. Neurophysiol. 2020, 132. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366. [Google Scholar] [CrossRef] [Green Version]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.H.L. Chapter 3: Systematic reviews of effectiveness. In Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Institute of Health Economics (IHE). Quality Appraisal of Case Series Studies Checklist. 2014. Available online: https://cdn-links.lww.com/permalink/jbjsrev/a/jbjsrev_2018_03_28_greysdc_17-00129_sdc2.pdf (accessed on 20 November 2020).
- Bolloni, C.; Panella, R.; Pedetti, M.; Frascella, A.G.; Gambelunghe, C.; Piccoli, T.; Maniaci, G.; Brancato, A.; Cannizzaro, C.; Diana, M. Bilateral Transcranial Magnetic Stimulation of the Prefrontal Cortex Reduces Cocaine Intake: A Pilot Study. Front. Psychiatry 2016, 7, 1. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, C.A.; Dowdle, L.T.; Correia, B.; Mithoefer, O.; Kearney-Ramos, T.; Lench, D.; Griffin, M.; Anton, R.F.; George, M.S. Left frontal pole theta burst stimulation decreases orbitofrontal and insula activity in cocaine users and alcohol users. Drug Alcohol Depend. 2017, 178, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Madeo, G.; Terraneo, A.; Cardullo, S.; Gómez Pérez, L.J.; Cellini, N.; Sarlo, M.; Bonci, A.; Gallimberti, L. Long-Term Outcome of Repetitive Transcranial Magnetic Stimulation in a Large Cohort of Patients With Cocaine-Use Disorder: An Observational Study. Front. Psychiatry 2020, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Martinez, D.; Urban, N.; Grassetti, A.; Chang, D.; Hu, M.C.; Zangen, A.; Levin, F.R.; Foltin, R.; Nunes, E.V. Transcranial magnetic stimulation of medial prefrontal and cingulate cortices reduces cocaine self-administration: A pilot study. Front. Psychiatry 2018, 9, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Pettorruso, M.; Martinotti, G.; Santacroce, R.; Montemitro, C.; Fanella, F.; di Giannantonio, M. rTMS Reduces Psychopathological Burden and Cocaine Consumption in Treatment-Seeking Subjects With Cocaine Use Disorder: An Open Label, Feasibility Study. Front. Psychiatry 2019, 10, 1–9. [Google Scholar] [CrossRef]
- Politi, E.; Fauci, E.; Santoro, A.; Smeraldi, E. Daily sessions of transcranial magnetic stimulation to the left prefrontal cortex gradually reduce cocaine craving. Am. J. Addict. 2008, 17, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Sanna, A.; Fattore, L.; Badas, P.; Corona, G.; Cocco, V.; Diana, M. Intermittent Theta Burst Stimulation of the Prefrontal Cortex in Cocaine Use Disorder: A Pilot Study. Front. Neurosci. 2019, 13, 765. [Google Scholar] [CrossRef] [PubMed]
- Steele, V.R.; Maxwell, A.M.; Ross, T.J.; Stein, E.A.; Salmeron, B.J. Accelerated intermittent theta-burst stimulation as a treatment for cocaine use disorder: A proof-of-concept study. Front. Neurosci. 2019, 13, 1–13. [Google Scholar] [CrossRef]
- Strafella, A.P.; Paus, T.; Barrett, J.; Dagher, A. Repetitive transcranial magnetic stimulation of the human prefrontal cortex induces dopamine release in the caudate nucleus. J. Neurosci. 2001, 21. [Google Scholar] [CrossRef]
- Keck, M.E.; Welt, T.; Müller, M.B.; Erhardt, A.; Ohl, F.; Toschi, N.; Holsboer, F.; Sillaber, I. Repetitive transcranial magnetic stimulation increases the release of dopamine in the mesolimbic and mesostriatal system. Neuropharmacology 2002, 43, 101–109. [Google Scholar] [CrossRef]
- Kanno, M.; Matsumoto, M.; Togashi, H.; Yoshioka, M.; Mano, Y. Effects of acute repetitive transcranial magnetic stimulation on dopamine release in the rat dorsolateral striatum. J. Neurol. Sci. 2004, 217, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Zangen, A.; Hyodo, K. Transcranial magnetic stimulation induces increases in extracellular levels of dopamine and glutamate in the nucleus accumbens. Neuroreport 2002, 13, 2401–2405. [Google Scholar] [CrossRef]
- Creed, M.; Pascoli, V.J.; Lüscher, C. Addiction therapy. Refining deep brain stimulation to emulate optogenetic treatment of synaptic pathology. Science 2015, 347, 659–664. [Google Scholar] [CrossRef]
- Enokibara, M.; Trevizol, A.; Shiozawa, P.; Cordeiro, Q. Establishing an Effective TMS Protocol for Craving in Substance Addiction: Is It Possible? Am. J. Addict. 2016, 25, 28–30. [Google Scholar] [CrossRef]
- Dinur-Klein, L.; Dannon, P.; Hadar, A.; Rosenberg, O.; Roth, Y.; Kotler, M.; Zangen, A. Smoking cessation induced by deep repetitive transcranial magnetic stimulation of the prefrontal and insular cortices: A prospective, randomized controlled trial. Biol. Psychiatry 2014, 76, 742–749. [Google Scholar] [CrossRef]
- Camprodon, J.A.; Martínez-Raga, J.; Alonso-Alonso, M.; Shih, M.C.; Pascual-Leone, A. One session of high frequency repetitive transcranial magnetic stimulation (rTMS) to the right prefrontal cortex transiently reduces cocaine craving. Drug Alcohol Depend. 2007, 86, 91–94. [Google Scholar] [CrossRef]
- Rapinesi, C.; Kotzalidis, G.D.; Serata, D.; Del Casale, A.; Bersani, F.S.; Solfanelli, A.; Scatena, P.; Raccah, R.N.; Brugnoli, R.; Digiacomantonio, V.; et al. Efficacy of add-on deep transcranial magnetic stimulation in comorbid alcohol dependence and dysthymic disorder: Three case reports. Prim. Care Companion J. Clin. Psychiatry 2013, 15. [Google Scholar] [CrossRef] [PubMed]
- Girardi, P.; Rapinesi, C.; Chiarotti, F.; Kotzalidis, G.D.; Piacentino, D.; Serata, D.; Del Casale, A.; Scatena, P.; Mascioli, F.; Raccah, R.N.; et al. Add-on deep transcranial magnetic stimulation (dTMS) in patients with dysthymic disorder comorbid with alcohol use disorder: A comparison with standard treatment. World J. Biol. Psychiatry 2015, 16, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Kearney-Ramos, T.E.; Dowdle, L.T.; Mithoefer, O.J.; Devries, W.; George, M.S.; Hanlon, C.A. State-dependent effects of ventromedial prefrontal cortex continuous thetaburst stimulation on cocaine cue reactivity in chronic cocaine users. Front. Psychiatry 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| 1 | Transcranial Magnetic Stimulation | 11,631 |
| 2 | (Transcranial adj1 magnetic stimulation$).tw. | 14,512 |
| 3 | ((transcranial magnetic stimulation or tms) adj5 repetitive).tw. | 4917 |
| 4 | ((transcranial magnetic stimulation or tms) adj5 rhythmic).tw. | 41 |
| 5 | (rtms or tms).tw. | 15,423 |
| 6 | ((Repetitive or “single pulse” or “paired pulse”) adj1 “transcranial magnetic stimulation”).tw. | 5260 |
| 7 | 1 or 2 or 3 or 4 or 5 or 6 | 21,895 |
| 8 | Cocaine-Related Disorders | 8278 |
| 9 | (cocaine * adj2 (abuse* or addict * or dependent * or disorder *)). ti,ab. | 7622 |
| 10 | 8 or 9 | 12,519 |
| 11 | 7 and 10 | 46 |
| Author (Year), Country | Study Design | Population | No. of Participants | Intervention | Stimulation Area | Stimulation Protocol | Frequency (Hz) and Intensity (% RMT) | Comparator | Outcomes | Measures |
|---|---|---|---|---|---|---|---|---|---|---|
| Bolloni (2016) [41], Italy, USA and Israel | RCT | CUD (DSM-5) Male: n=16 Female: n = 2 Mean age: 27–48 years | n = 18 | Deep rTMS | Bilateral PFC | 12 rTMS sessions were administered three times a week for 4 weeks | 10 Hz 100–120% | Sham | Cocaine intake (hair analysis) | Baseline, after 1 month and 3 and 6 months later |
| Gómez (2020) [20], Italy | CS | CUD (DSM-5) Male: n = 85 Female: n = 2 Mean age: 37.67 years | n = 87 | rTMS | Left-DLPFC | 2 sessions per day for the first 5 consecutive days of treatment (10 sessions), and 2 sessions per week for the following 12 weeks. | 15 Hz 100% | NA | Cocaine use (self-report and urine screens) Craving (CCQ) Sleep Quality (PSQI) Depression (BDI-II) Anxiety (SAS) Symptoms (SCL-90) | Baseline, and after 5, 30, 60, and 90 days of rTMS treatment. |
| Hanlon (2015) [15], USA | RCT | Cocaine users Male: n = 9 Female: n = 2 Mean age: 39 years | n = 11 | cTBS | MPFC | 2 stimulation visits (occurring within 7–14 days of each other). | 5 Hz 110% | Sham | Craving (VAS) | Before and after the cTBS session |
| Hanlon (2017) [42], USA | RCT | Cocaine users Male: n = 12 Female: n = 3 Mean age: 42 years | n = 25 | cTBS | MPFC | 2 stimulation visits (occurring within 7–14 days of each other) with exposure to 6 trains of cBTS. | 5 Hz 110% | Sham | Craving (VAS) | Before and after the cTBS session |
| Madeo (2020) [43], Italy and USA | CS | CUD (DSM-5) Male: n = 139 Female: n = 8 Mean age: 36.6 years | n = 147 | rTMS | Left-DLPFC | 2 rTMS sessions per day for the first 5 days, then weekly, twice per day on each session day for 11 consecutive weeks. | 15 Hz 100% | NA | Cocaine use (urine screening, self-report and reports by collateral informants) | Baseline, after 3 months of rTMS and up to 2 years. |
| Martínez (2018) [44], USA and Israel | RCT | CUD (DSM-5) Male: n = 17 Female: n = 1 Mean age: 43.3 years | n = 18 | rTMS | MPFC | The rTMS was delivered on weekdays, over the course of 3 weeks. | HF: 10 Hz LF: 1 Hz 90–110% | Sham | Number of doses chosen during self-administration Craving (VAS) | Baseline, after 4 days and after 13 days of rTMS. |
| Pettorruso (2019) [45], Italy and UK | CS | CUD (DSM-5) Male: n = 4 Female: n = 2 Mean age: 36.63 years | n = 16 | rTMS | Left-DLPFC | 20 stimulation sessions (2 daily, 5 d/week) for 2 weeks and 2 consecutive maintenance rTMS sessions once a week for 2 weeks. | 15 Hz 100% | NA | Cocaine use (urine test) Cocaine withdrawal signs and symptoms (CSSA) Craving (CSSA) Depression (BDI) Anxiety (SAS) Global Psychopathology (SCL-90) Insomnia (ISI) | Baseline, after 2 and after 4 weeks of rTMS treatment. |
| Politi (2008) [46], Italy | CS | CUD (DSM-IV) Male: n = 31 Female: n = 5 Mean age: NI | n = 36 | rTMS | Left-DLPFC | 10 daily sessions of rTMS. | 15 Hz 100% | NA | Craving (VAS) | During sessions of rTMS. |
| Rapinesi (2016) [17] Italy | CS | CUD (DSM-IV) Male: n = 7 Female: n = 0 Mean age: 48.71 years | n = 7 | Deep TMS | Bilateral PFC | 3 weekly sessions on alternate days for 4 consecutive weeks, for a total of 12 sessions. | 20 Hz 100% | NA | Craving (VAS) | Baseline and after 2, 4 and 8 weeks of treatment. |
| Sanna (2019) [47], Italy | nRCT | CUD (DSM-5) Male: n = 45 Female: n = 2 Mean age: 37.40 years | n = 47 | iTBS | PFC | 20 stimulations over 4 weeks: 10 stimulations during the 1st week, 4 stimulations during the 2nd week, 3 stimulations during the 3rd and 4th week. | HF rTMS: 15 Hz; 100% iTBS: 5 Hz; 80% | HF rTMS | Cocaine use (urine test) Craving (CCQ-brief) Risk for developing problems due to the use of cocaine (ASSIST) | Baseline, weekly during treatment and at the end of treatment. |
| Steele (2019) [48], USA | CS | CUD (DSM-5) Male: n = 13 Female: n = 6 Mean age: 47.4 years | n = 19 | iTBS | Left-DLPFC | 3 iTBS sessions per day, with an interval of approximately 60-min between sessions, for 10 days over a 2-week period (30 total iTBS sessions). | 5 Hz 90–120% | NA | Amount of money spent on cocaine consumption Craving (CCS and CCQ) iTBS side effects Depression (MADRS) | Baseline, during, and after the intervention and at 1-and 4-week follow-up visits. |
| Terraneo (2016) [13], Italy | RCT | CUD Male: n = 30 Female: n = 2 Mean age: 40.28 years | n = 32 | rTMS | Left-DLPFC | 1 rTMS session per day during the first 5 days of treatment, and then once a week for the following 3 weeks, for a total of 8 rTMS sessions. | 15 Hz 100% | Pharmacological agents | Cocaine use (urine test) Craving (VAS) Adverse events Depression (SCL-90) | Baseline, after 29-day treatment and after 63-day follow-up. |
| Cocaine Use | Craving | Anxiety | Depression | Psychopathology | Insomnia | |
|---|---|---|---|---|---|---|
| rTMS over the left-DLPFC | ||||||
| Terraneo et al., 2016 [13] (n = 36) RCT | Negative urine test during treatment: rTMS: 11(69%) PT: 3 (19%) OR = 6.47 (IC95%: 1.14, 36.6). | VAS 0–10: Significantly lower craving with rTMS ANOVA RM: F (1,27) = 4.74, p = 0.038 | - | - | - | - |
| Madeo et al., 2020 [43] (n = 147) CS | Days until relapse (median): rTMS: 91 (70–109) TAU: 51 (39–78) 147 patients followed for 84–974 days: Mean use <1.0 day/month (median 0). | - | - | - | - | - |
| Gómez et al., 2020 [20] (n = 87) CS | Days of cocaine use (mean): reduction at 30 days: −18.7 (97.3%) p < 0.001 reduction at 90 days: −18.3 (95.6%) p < 0.001 | CCQ reduction at 30 days: −11.32 (89.3%) p < 0.001 reduction at 90 days: −8.86 (69.9%) p < 0.001 | SAS reduction at 30 days: −11.96 (24.9%) p < 0.001 reduction at 90 days: −9.83 (20.5%) p < 0.001 | BDI-II reduction at 30 days: −13.89 (73.1%) p < 0.001 reduction at 90 days: −12.26 (64.5%) p < 0.001 | SCL-90-R reduction at 30 days: −18.24 (27.7%) p < 0.001 reduction at 90 days: −19.45 (29.5%) p < 0.001 | PSQI reduction at 30 days: −4.24 (45.6%) p < 0.001 reduction at 90 days: −3.12 (33.8%) |
| Pettorruso et al., 2019 [47] (n = 20) CS | Negative urine test at the end of treatment: 9 of 16 (56.25%) (Z = −3.00; p = 0.003). | CSSA (craving) reduction at 4 weeks: −1.5 (33.9%) p = 0.020 | SAS reduction at 4 weeks: −8.4 (23.0%) p = 0.001 | BDI-II reduction at 4 weeks: −9.8 (57.1%) p = 0.008 | SCL-90-R reduction at 4 weeks: −0.51 (52.0%) p < 0.001 | ISI reduction at 4 weeks: −5.2 (59.7%) p = 0.077 |
| Politi et al., 2008 [48] (n = 36) CS | - | Greater reduction with TMS ANOVA RM (time effect) F (30,270) = 4.96 p < 0.001 | - | - | - | - |
| Steele et al., 2019 [42] (n = 19) CS | Mean use (days/week): Reduction at 7 weeks: −3 (70.0%) p < 0.001 Money spent on consumption at 4 weeks: −167$ (78.0%) p < 0.001 | Reduction at 7 weeks: CCQ: 37% CCS: 26% | BAI Increase at 3 weeks: 33% | MADRS Reduction at 3 weeks: 18% | - | - |
| High frequency deep rTMS over the bilateral PFC | ||||||
| Bolloni et al., 2016 [41] (n = 18) RCT | Amount of cocaine in hair analysis ANOVA RM (interaction) F = 0.35; p = 0.87 | - | - | - | - | - |
| Rapinesi et al., 2016 [17] (n = 20) CS | - | VAS 0–10 Craving reduction at the end of treatment: −6.3 (64.7%) p < 0.001 Craving reduction at one month follow-up: −3.8 (39.6%) p = 0.003 | - | - | - | - |
| Medial prefrontal cortex (MPFC) stimulation | ||||||
| Martínez et al., 2018 [46] (n = 18) RCT | Choice of cocaine vs. receiving money: lower with rTMS ANOVA RM (interaction) F = 5.36, p = 0.02 | Negative binominal distribution with random effects F (2, 14) = 0.77, p = 0.48 | - | - | - | - |
| Hanlon et al., 2015 [15] (n = 11) Crossover | - | VAS 0–10 No significant different on mean change. Fewer patients getting worse and more patients remaining stables with TMS. χ2 = 19.14, p <0.001 | - | - | - | - |
| Hanlon et al., 2017 [44] (n = 25) Crossover | - | VAS 0–10 Post-treatment result not significant (p-value not reported): rTMS: 2.93 (2.78) Control: 2.90 (2.25) | - | - | - | - |
| Comparison between bilateral deep stimulation protocols: iTBS vs. high frequency rTMS | ||||||
| Sanna et al., 2019 [41] (n = 49) nRCT | Urine test and consumption statement ANOVA RM: Significant effect of time (F = 49.97; p <0.001) but not of treatment (F = 0.67) or interaction (F = 0.66). | brief modified CCQ ANOVA RM: Significant effect of time (F = 127.3; p <0.001 but not of treatment (F = 1.48) or interaction (F = 0.03). | - | - | - | - |
| Author (Year) | Drop-Outs | Adverse Events |
|---|---|---|
| Boloni (2016) [41] | 4/18 (22.2%) | Discomfort was not observed except for a patient who suffered from a mild headache after receiving active stimulation. |
| Gómez (2020) [20] | NR | Serious AEs were not reported. There were no seizures, syncopes, neurological complications or subjective complaints about memory or concentration impairment limiting the treatment. |
| Hanlon (2015) [15] | NA | NR |
| Hanlon (2017) [42] | NA | NR |
| Madeo (2020) [43] | 58/284 (20.4%) | AEs were reported by 41 of the 284 patients. AEs reported were headache (n = 23), hypomania (n = 4), anxiety (n = 2), irritability (n = 2), dental pain (n = 2), scalp discomfort during the first 2 (n = 1), angioedema and urticaria (n = 1), distractibility (n = 1), dizziness (n = 1), nausea (n = 1), nausea and numbness (n = 1), seizure (n = 1), and a hypomanic episode (n = 1). |
| Martínez (2018) [44] | NR | Participants had difficulty tolerating stimulation that increased from 100 to 120% of MT, and thus the protocol was amended by lowering the maximal stimulation. |
| Pettorruso (2019) [45] | 4/20 (20%) | The treated subjects reported no significant side effect. |
| Politi (2008) [46] | NR | NR |
| Rapinesi (2016) [17] | 0/7 (0%) | All patients tolerated the stimulation without complications or AEs. |
| Sanna (2019) [47] | 4/47 (8.5%) | A few participants in both the 15 Hz rTMS and the iTBS groups reported mild discomfort at the start of stimulation, especially during the first session. Both treatments were safe and there were no serious or unexpected AEs related to the treatments. There were no seizures or any other transient neurological event. |
| Steele (2019) [48] | 7/16 (43.7%) | There were no unexpected, serious AEs. Nine of the 14 participants experienced at least one headache. One participant experienced sudden pain around her eyes and one experienced muscle soreness in the right forearm. No negative side-effects in cognitive and affective assessments were reported. No participant experienced any signs of mania or suicidality. After completing 26 iTBS sessions, a participant reported right-hand supination/pronation and thus treatment was terminated. |
| Terraneo (2016) [13] | 3/32 (9.4%) | A few participants reported mild discomfort at the start of stimulation, especially during the first session, but overall, there were no significant differences in AEs across groups. There were no serious or unexpected AEs. |
| AEs: adverse events; NR: not reported; NA: not applicable. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres-Castaño, A.; Rivero-Santana, A.; Perestelo-Pérez, L.; Duarte-Díaz, A.; Toledo-Chávarri, A.; Ramos-García, V.; Álvarez-Pérez, Y.; Cudeiro-Mazaira, J.; Padrón-González, I.; Serrano-Pérez, P. Transcranial Magnetic Stimulation for the Treatment of Cocaine Addiction: A Systematic Review. J. Clin. Med. 2021, 10, 5595. https://doi.org/10.3390/jcm10235595
Torres-Castaño A, Rivero-Santana A, Perestelo-Pérez L, Duarte-Díaz A, Toledo-Chávarri A, Ramos-García V, Álvarez-Pérez Y, Cudeiro-Mazaira J, Padrón-González I, Serrano-Pérez P. Transcranial Magnetic Stimulation for the Treatment of Cocaine Addiction: A Systematic Review. Journal of Clinical Medicine. 2021; 10(23):5595. https://doi.org/10.3390/jcm10235595
Chicago/Turabian StyleTorres-Castaño, Alezandra, Amado Rivero-Santana, Lilisbeth Perestelo-Pérez, Andrea Duarte-Díaz, Ana Toledo-Chávarri, Vanesa Ramos-García, Yolanda Álvarez-Pérez, Javier Cudeiro-Mazaira, Iván Padrón-González, and Pedro Serrano-Pérez. 2021. "Transcranial Magnetic Stimulation for the Treatment of Cocaine Addiction: A Systematic Review" Journal of Clinical Medicine 10, no. 23: 5595. https://doi.org/10.3390/jcm10235595
APA StyleTorres-Castaño, A., Rivero-Santana, A., Perestelo-Pérez, L., Duarte-Díaz, A., Toledo-Chávarri, A., Ramos-García, V., Álvarez-Pérez, Y., Cudeiro-Mazaira, J., Padrón-González, I., & Serrano-Pérez, P. (2021). Transcranial Magnetic Stimulation for the Treatment of Cocaine Addiction: A Systematic Review. Journal of Clinical Medicine, 10(23), 5595. https://doi.org/10.3390/jcm10235595