
Effects of Anesthetic Techniques on the Risk of Postoperative Complications Following Lower Extremity Amputation in Diabetes Patients with Coagulation Abnormalities: A Retrospective Cohort Study Using Propensity Score Analysis


Abstract
:1. Introduction
2. Materials and Methods
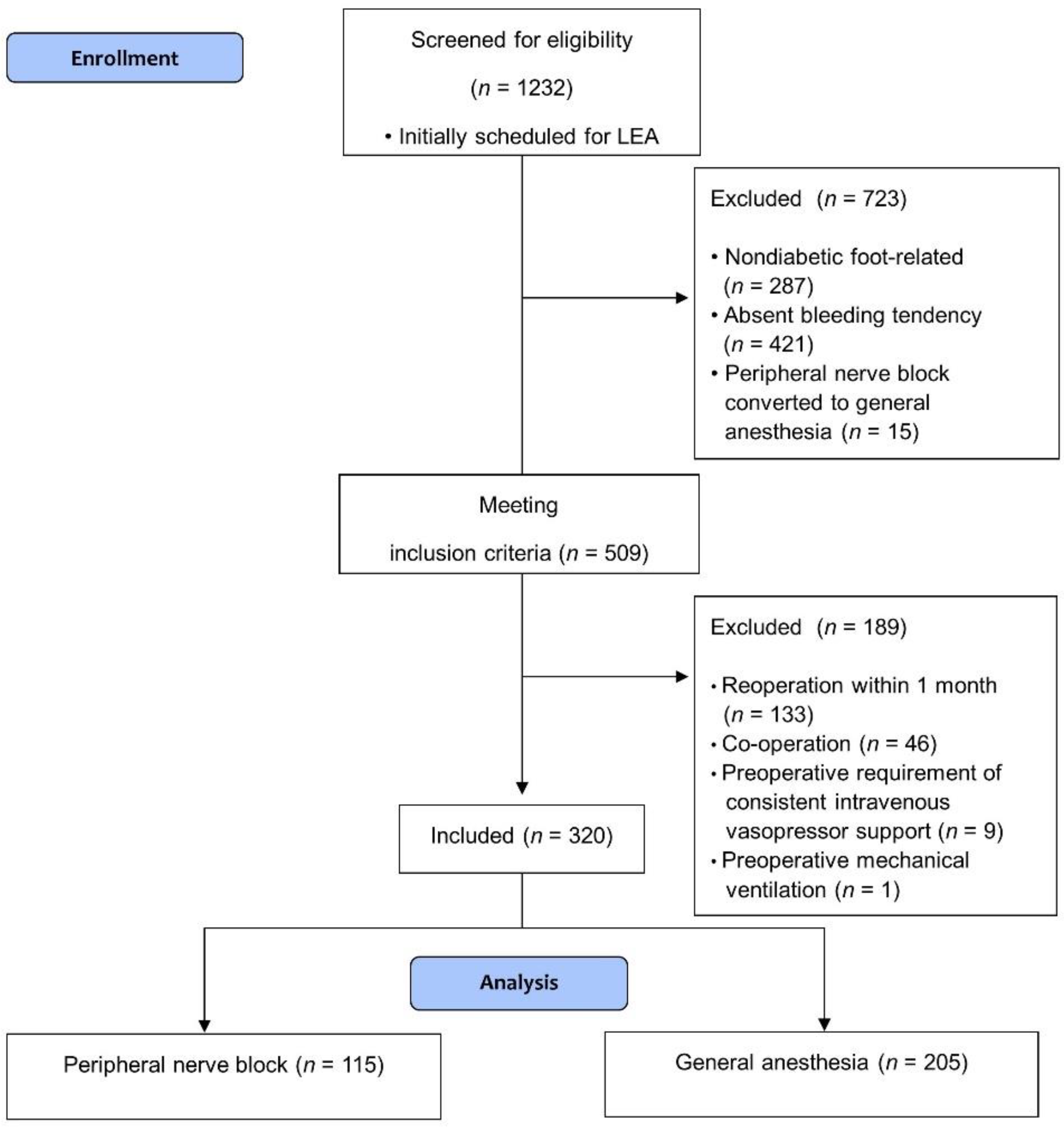
2.1. Study Design and Population
2.2. Data Collection
2.3. Study Endpoint
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Yazdanpanah, L.; Shahbazian, H.; Nazari, I.; Arti, H.R.; Ahmadi, F.; Mohammadianinejad, S.E.; Cheraghian, B.; Hesam, S. Incidence and Risk Factors of Diabetic Foot Ulcer: A Population-Based Diabetic Foot Cohort (ADFC Study)-Two-Year Follow-Up Study. Int. J. Endocrinol. 2018, 2018, 7631659. [Google Scholar] [CrossRef]
- Lin, C.; Liu, J.; Sun, H. Risk factors for lower extremity amputation in patients with diabetic foot ulcers: A meta-analysis. PLoS ONE 2020, 15, e0239236. [Google Scholar] [CrossRef] [PubMed]
- Belmont, P.J., Jr.; Davey, S.; Orr, J.D.; Ochoa, L.M.; Bader, J.O.; Schoenfeld, A.J. Risk factors for 30-day postoperative complications and mortality after below-knee amputation: A study of 2911 patients from the national surgical quality improvement program. J. Am. Coll. Surg. 2011, 213, 370–378. [Google Scholar] [CrossRef]
- Ploeg, A.J.; Lardenoye, J.W.; Vrancken Peeters, M.P.F.M.; Breslau, P.J. Contemporary Series of Morbidity and Mortality after Lower Limb Amputation. Eur. J. Vasc. Endovasc. Surg. 2005, 29, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Van Netten, J.J.; Fortington, L.V.; Hinchliffe, R.J.; Hijmans, J.M. Early Post-operative Mortality after Major Lower Limb Amputation: A Systematic Review of Population and Regional Based Studies. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 248–257. [Google Scholar] [CrossRef]
- Khan, S.A.; Qianyi, R.L.; Liu, C.; Ng, E.L.; Fook-Chong, S.; Tan, M.G. Effect of anaesthetic technique on mortality following major lower extremity amputation: A propensity score-matched observational study. Anaesthesia 2013, 68, 612–620. [Google Scholar] [CrossRef]
- Moreira, C.C.; Farber, A.; Kalish, J.A.; Eslami, M.H.; Didato, S.; Rybin, D.; Doros, G.; Siracuse, J.J. The effect of anesthesia type on major lower extremity amputation in functionally impaired elderly patients. J. Vasc. Surg. 2016, 63, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.A.M.; Bisset, W.I.K. Anaesthesia for lower limb amputation. Anaesthesia 1983, 38, 1185–1191. [Google Scholar] [CrossRef]
- Kessler, J.; Marhofer, P.; Hopkins, P.M.; Hollmann, M.W. Peripheral regional anaesthesia and outcome: Lessons learned from the last 10 years. Br. J. Anaesth. 2015, 114, 728–745. [Google Scholar] [CrossRef]
- Dal Canto, E.; Ceriello, A.; Rydén, L.; Ferrini, M.; Hansen, T.B.; Schnell, O.; Standl, E.; Beulens, J.W. Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Eur. J. Prev. Cardiol. 2019, 26, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Horlocker, T.T.; Vandermeuelen, E.; Kopp, S.L.; Gogarten, W.; Leffert, L.R.; Benzon, H.T. Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition). Reg. Anesth. Pain Med. 2018, 43, 263–309. [Google Scholar] [CrossRef]
- Li, J.; Halaszynski, T. Neuraxial and peripheral nerve blocks in patients taking anticoagulant or thromboprophylactic drugs: Challenges and solutions. Local Reg. Anesth. 2015, 8, 21–32. [Google Scholar] [PubMed]
- Di Giovanni, P.; Scampoli, P.; Meo, F.; Cedrone, F.; D’Addezio, M.; Di Martino, G.; Valente, A.; Romano, F.; Staniscia, T. The impact of gender on diabetes-related lower extremity amputations: An Italian regional analysis on trends and predictors. Foot Ankle Surg. 2021, 27, 25–29. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, N.; Kim, E.H.; Roh, Y.H.; Song, J.; Park, K.H.; Choi, Y.S. Use of Regional Anesthesia for Lower Extremity Amputation May Reduce the Need for Perioperative Vasopressors: A Propensity Score-Matched Observational Study. Ther. Clin. Risk. Manag. 2019, 15, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Takemura, H.; Fujita, D.; Matsuda, M.; Fujita, K.; Sakaguchi, M.; Amaya, F. Peripheral nerve block combined with general anesthesia for lower extremity amputation in hemodialysis patients: Case series. JA Clin. Rep. 2018, 4, 77. [Google Scholar] [CrossRef]
- Matsuzaki, K.; Hayashi, R.; Okabe, K.; Aramaki-Hattori, N.; Kishi, K. Prognosis of critical limb ischemia: Major vs. minor amputation comparison. Wound Repair Regen. 2015, 23, 759–764. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef]
- Miskovic, A.; Lumb, A.B. Postoperative pulmonary complications. Br. J. Anaesth. 2017, 118, 317–334. [Google Scholar] [CrossRef]
- Mendis, S.; Thygesen, K.; Kuulasmaa, K.; Giampaoli, S.; Mähönen, M.; Ngu Blackett, K.; Lisheng, L. World Health Organization definition of myocardial infarction: 2008–2009 revision. Int. J. Epidemiol. 2011, 40, 139–146. [Google Scholar] [CrossRef]
- Kellum, J.A.; Lameire, N.; Aspelin, P.; Barsoum, R.S.; Burdmann, E.A.; Goldstein, S.L.; Herzog, C.A.; Joannidis, M.; Kribben, A.; Levey, A.S.; et al. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Naja, Z.; El Hassan, M.J.; Khatib, H.; Ziade, M.F.; Lönnqvist, P.A. Combined sciatic-paravertebral nerve block vs. general anaesthesia for fractured hip of the elderly. Middle East J. Anaesthesiol. 2000, 15, 559–568. [Google Scholar]
- Levy, N.; Lirk, P. Regional anaesthesia in patients with diabetes. Anaesthesia 2021, 76 (Suppl. 1), 127–135. [Google Scholar] [CrossRef]
- Lin, R.; Hingorani, A.; Marks, N.; Ascher, E.; Jimenez, R.; McIntyre, T.; Jacob, T. Effects of anesthesia versus regional nerve block on major leg amputation mortality rate. Vascular 2013, 21, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Hausman, M.S., Jr.; Jewell, E.S.; Engoren, M. Regional Versus General Anesthesia in Surgical Patients with Chronic Obstructive Pulmonary Disease: Does Avoiding General Anesthesia Reduce the Risk of Postoperative Complications? Anesth. Analg. 2015, 120, 1405–1412. [Google Scholar] [CrossRef] [PubMed]
- Saraswat, V. Effects of anaesthesia techniques and drugs on pulmonary function. Indian J. Anaesth. 2015, 59, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Guay, J.; Parker, M.J.; Griffiths, R.; Kopp, S. Peripheral nerve blocks for hip fractures. Cochrane Database Syst. Rev. 2017, 5, CD001159. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.Y.; Lee, K.-Y.; Bai, S.J.; Hong, J.H.; Lee, J.; Park, J.M.; Kim, S.H. Comparison of the effects of remifentanil-based general anesthesia and popliteal nerve block on postoperative pain and hemodynamic stability in diabetic patients undergoing distal foot amputation: A retrospective observational study. Medicine (Baltimore) 2016, 95, e4302. [Google Scholar] [CrossRef]
- Brienza, N.; Giglio, M.T.; Marucci, M.; Fiore, T. Does perioperative hemodynamic optimization protect renal function in surgical patients? A meta-analytic study. Crit. Care Med. 2009, 37, 2079–2090. [Google Scholar] [CrossRef]
- Jor, O.; Maca, J.; Koutna, J.; Gemrotova, M.; Vymazal, T.; Litschmannova, M.; Sevcik, P.; Reimer, P.; Mikulova, V.; Trlicova, M.; et al. Hypotension after induction of general anesthesia: Occurrence, risk factors, and therapy. A prospective multicentre observational study. J. Anesth. 2018, 32, 673–680. [Google Scholar] [CrossRef]
- Okitsu, K.; Iritakenishi, T.; Iura, A.; Kuri, M.; Fujino, Y. Femoral nerve block with propofol sedation versus general anesthesia in patients with severe cardiac dysfunction undergoing autologous myoblast sheet transplantation. J. Anesth. 2017, 31, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Tevis, S.E.; Kennedy, G.D. Postoperative complications and implications on patient-centered outcomes. J. Surg. Res. 2013, 181, 106–113. [Google Scholar] [CrossRef]
- Ashken, T.; West, S. Regional anaesthesia in patients at risk of bleeding. BJA Educ. 2021, 21, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Tsui, B.C.H.; Kirkham, K.; Kwofie, M.K.; Tran, Q.; Wong, P.; Chin, K.J.; Sondekoppam, R.V. Practice advisory on the bleeding risks for peripheral nerve and interfascial plane blockade: Evidence review and expert consensus. Can. J. Anaesth. 2019, 66, 1356–1384. [Google Scholar] [CrossRef] [PubMed]
- Tsui, B.C.H.; Kirkham, K.; Kwofie, M.K.; Tran, D.Q.; Wong, P.; Chin, K.J.; Sondekoppam, R.V. Practice advisory on the bleeding risks for peripheral nerve and interfascial blockade: Rooted in evidence. Can. J. Anesth. /Journal canadien d’anesthésie 2020, 67, 379–380. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Before IPTW | After IPTW | ||||
|---|---|---|---|---|---|---|
| General Anesthesia Group (n = 205) | PNB Group (n = 115) | p-Value | General Anesthesia Group (n = 231.8) | PNB Group (n = 157.7) | p-Value | |
| Age (years) | 66.3 ± 10.8 | 68 ± 9.5 | 0.1470 | 67 ± 11.4 | 67.2 ± 10.6 | 0.9186 |
| Male sex | 163 (79.5) | 86 (74.8) | 0.3286 | 186.5 (80.5) | 130.3 (82.6) | 0.6389 |
| BMI (kg/m2) | 23.3 ± 3.5 | 23.1 ± 3.3 | 0.5138 | 23.2 ± 3.6 | 23 ± 3.5 | 0.5457 |
| Year of operation | 2015.6 ± 3.2 | 2016.8 ± 2.6 | 0.0001 | 2016 ± 3.3 | 2016.2 ± 3.1 | 0.5243 |
| Emergency | 57 (27.8) | 20 (17.4) | 0.0365 | 55.5 (23.9) | 33.4 (21.2) | 0.6370 |
| Level of amputation | 0.0609 * | 0.8435 * | ||||
| Major amputation (BKA) | 30 (14.6) | 6 (5.2) | 0.0105 † | 27.2 (11.7) | 16.7 (10.6) | 0.8313 † |
| Minor amputation | 175 (85.4) | 109 (94.8) | 204.1 (88.3) | 141.0 (89.4) | ||
| Fore-foot (toe, ray, transmetatarsal) | 162 (79.0) | 101 (87.8) | 187.3 (80.8) | 133.8 (84.8) | ||
| Mid-foot (Lisfranc, Chopart) | 9 (4.4) | 5 (4.3) | 12.1 (5.2) | 4.8 (3.0) | ||
| Hind-foot (Syme, Pirogoff) | 4 (2.0) | 3 (2.6) | 5.1 (2.2) | 2.5 (1.6) | ||
| ASA-PS > 3 | 33 (16.1) | 46 (40) | <.0001 | 56.3 (24.3) | 40.5 (25.7) | 0.8127 |
| Current smoker | 24 (11.7) | 8 (7) | 0.1741 | 23.8 (10.3) | 12.1 (7.7) | 0.4928 |
| Hypertension | 178 (86.8) | 107 (93) | 0.0875 | 203.1 (87.6) | 141 (89.4) | 0.7130 |
| Congestive heart failure | 14 (6.8) | 22 (19.1) | 0.0008 | 25.3 (10.9) | 18.6 (11.8) | 0.8368 |
| CAOD | 89 (43.4) | 82 (71.3) | <.0001 | 123.1 (53.1) | 86 (54.5) | 0.8453 |
| PAOD | 169 (82.4) | 103 (89.6) | 0.0867 | 197.2 (85.1) | 139.1 (88.2) | 0.4963 |
| COPD | 7 (3.4) | 5 (4.3) | 0.7616 | 8.3 (3.6) | 6.3 (4) | 0.8614 |
| CVA | 52 (25.4) | 39 (33.9) | 0.1039 | 58.7 (25.3) | 40 (25.3) | 0.9982 |
| CKD | 119 (58) | 74 (64.3) | 0.2691 | 143.3 (61.8) | 99.8 (63.2) | 0.8348 |
| Sepsis | 6 (2.9) | 6 (5.2) | 0.3613 | 6.1 (2.6) | 5.4 (3.4) | 0.6911 |
| Preoperative amputation history | 63 (30.7) | 56 (48.7) | 0.0014 | 86.5 (37.3) | 68.1 (43.1) | 0.4085 |
| Variables | Before IPTW | After IPTW | ||||
|---|---|---|---|---|---|---|
| General Anesthesia Group (n = 205) | PNB Group (n = 115) | p-Value | General Anesthesia Group (n = 231.8) | PNB Group (n = 157.7) | p-Value | |
| Duration of operation (mins) | 62.9 ± 36.6 | 50.8 ± 21.4 | 0.0002 | 58.1 ± 36.7 | 53 ± 26.2 | 0.1708 |
| Duration of anesthesia (mins) | 107.3 ± 44.8 | 92.9 ± 29.1 | 0.0006 | 102.6 ± 44.5 | 95.5 ± 36.7 | 0.1416 |
| Crystalloids (mL) | 451 ± 311.7 | 260.7 ± 163.5 | <0.0001 | 415.7 ± 307.1 | 287.3 ± 202.9 | <0.0001 |
| Colloids (mL) | 38.1 ± 126.4 | 9.9 ± 55 | 0.0061 | 29.8 ± 117.4 | 18.7 ± 83.4 | 0.3399 |
| Transfused red blood cell (mL) | 28.5 ± 103 | 7.8 ± 39.5 | 0.0109 | 24.8 ± 97.5 | 11.6 ± 49.4 | 0.1076 |
| Blood loss (mL) | 78.1 ± 143.5 | 46.4 ± 113 | 0.0300 | 67.7 ± 137.2 | 73.8 ± 149.5 | 0.7557 |
| Urine output (mL) | 15.6 ± 76.5 | 17 ± 76.4 | 0.8748 | 12.3 ± 71.3 | 14.1 ± 80.4 | 0.8162 |
| Number of patients requiring vasopressor support * | 153 (74.6) | 13 (11.3) | <0.0001 | 177.5 (76.6) | 17.3 (11) | <0.0001 |
| Variables | Before IPTW | After IPTW | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Pneumonia | 0.141 (0.018–1.099) | 0.0615 | 0.091 (0.010–0.850) | 0.0355 |
| Myocardial infarction | 0.587 (0.117–2.957) | 0.5185 | 0.337 (0.065–1.752) | 0.1961 |
| Stroke | 5.384 (0.216–134.505) | 0.3052 | 5.010 (0.211–119.098) | 0.3189 |
| Venous thromboembolism * | Not applicable | Not applicable | 0.3399 | |
| Delirium | 0.459 (0.211–0.999) | 0.0498 | 0.543 (0.283–1.041) | 0.0659 |
| Acute kidney injury | 0.155 (0.020–1.214) | 0.0758 | 0.078 (0.007–0.871) | 0.0382 |
| New requirement for dialysis | 0.441 (0.049–3.991) | 0.4662 | 0.269 (0.021–3.441) | 0.3127 |
| Surgical site infection | 0.650 (0.390–1.083) | 0.0985 | 0.759 (0.490–1.175) | 0.2162 |
| Re-operation | 0.710 (0.425–1.186) | 0.1909 | 0.775 (0.495–1.207) | 0.2597 |
| Mortality | 0.248 (0.030–2.042) | 0.1905 | 0.176 (0.026–1.195) | 0.0754 |
| Total major complications † | 0.508 (0.317–0.816) | 0.0051 | 0.603 (0.400–0.910) | 0.0161 |
| Intensive care unit admission | 0.532 (0.294–0.962) | 0.0369 | 0.447 (0.262–0.760) | 0.0030 |
| Variables | Before IPTW | After IPTW | ||
|---|---|---|---|---|
| Estimates (95% CI) | p-Value | Estimates (95% CI) | p-Value | |
| Length of ICU stay (days) | ||||
| General anesthesia | Reference | Reference | ||
| PNB | −0.2723 (−1.1250–0.5804) | 0.5302 | −0.40931 (−1.23981–0.42119) | 0.3330 |
| Length of hospital stay (days) | ||||
| General anesthesia | Reference | Reference | ||
| PNB | −1.9413 (−6.7215–2.8390) | 0.4249 | −2.70379 (−7.10752–1.69994) | 0.2280 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Park, C.-G.; Choi, Y.S.; Lee, Y.S.; Kwak, H.-J. Effects of Anesthetic Techniques on the Risk of Postoperative Complications Following Lower Extremity Amputation in Diabetes Patients with Coagulation Abnormalities: A Retrospective Cohort Study Using Propensity Score Analysis. J. Clin. Med. 2021, 10, 5598. https://doi.org/10.3390/jcm10235598
Kim HJ, Park C-G, Choi YS, Lee YS, Kwak H-J. Effects of Anesthetic Techniques on the Risk of Postoperative Complications Following Lower Extremity Amputation in Diabetes Patients with Coagulation Abnormalities: A Retrospective Cohort Study Using Propensity Score Analysis. Journal of Clinical Medicine. 2021; 10(23):5598. https://doi.org/10.3390/jcm10235598
Chicago/Turabian StyleKim, Hye Jin, Chun-Gon Park, Yong Seon Choi, Yong Suk Lee, and Hyun-Jeong Kwak. 2021. "Effects of Anesthetic Techniques on the Risk of Postoperative Complications Following Lower Extremity Amputation in Diabetes Patients with Coagulation Abnormalities: A Retrospective Cohort Study Using Propensity Score Analysis" Journal of Clinical Medicine 10, no. 23: 5598. https://doi.org/10.3390/jcm10235598
APA StyleKim, H. J., Park, C.-G., Choi, Y. S., Lee, Y. S., & Kwak, H.-J. (2021). Effects of Anesthetic Techniques on the Risk of Postoperative Complications Following Lower Extremity Amputation in Diabetes Patients with Coagulation Abnormalities: A Retrospective Cohort Study Using Propensity Score Analysis. Journal of Clinical Medicine, 10(23), 5598. https://doi.org/10.3390/jcm10235598