
Body Composition Assessment and Mediterranean Diet Adherence in U12 Spanish Male Professional Soccer Players: Cross-Sectional Study

 ,
,  ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.2.1. Anthropometric Measurements
2.2.2. Evaluation of the Mediterranean Diet Quality Index
2.2.3. Supplementation and Beverages Survey
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Anthropometric Characteristics and Body Composition of Different Field Positions
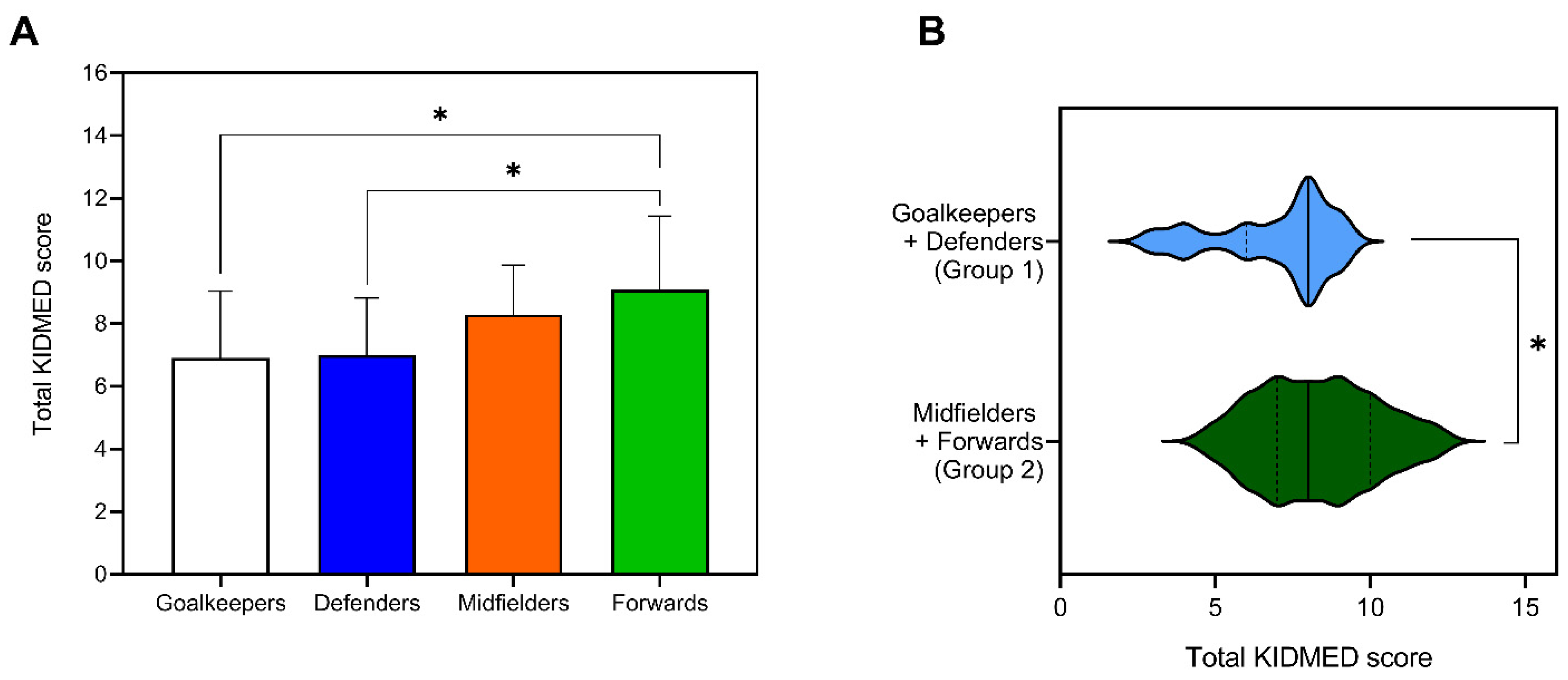
3.3. Adherence to the Mediterranean Diet
3.4. Body Composition and Nutritional Behaviors
3.5. Supplements and Beverage Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kunz, M. FIFA magazine: Big count. Retrieved Dec. 2007, 16, 2015. [Google Scholar]
- Di Salvo, V.; Baron, R.; Tschan, H.; Montero, F.C.; Bachl, N.; Pigozzi, F. Performance characteristics according to playing position in elite soccer. Int. J. Sports Med. 2007, 28, 222–227. [Google Scholar] [CrossRef]
- Faude, O.; Rößler, R.; Junge, A. Football injuries in children and adolescent players: Are there clues for prevention? Sports Med. 2013, 43, 819–837. [Google Scholar] [CrossRef]
- Stølen, T.; Chamari, K.; Castagna, C.; Wisløff, U. Physiology of soccer. Sports Med. 2005, 35, 501–536. [Google Scholar] [CrossRef] [PubMed]
- Castagna, C.; D’Ottavio, S.; Abt, G. Activity profile of young soccer players during actual match play. J. Strength Cond. Res. 2003, 17, 775–780. [Google Scholar] [PubMed]
- Meyer, T. The Importance of Nutrition in Football: Perspective of a National Team’s Doctor; BMJ Publishing Group Ltd and British Association of Sport and Exercise Medicine: London, UK, 2021. [Google Scholar]
- Manore, M.; Barr, S.; Butterfield, G. Position of dietitians of Canada, the American Dietetic Association, and the American College of Sports Medicine: Nutrition and athletic performance. Can. J. Diet. Pract. Res. 2000, 61, 176–192. [Google Scholar]
- Collins, J.; Maughan, R.J.; Gleeson, M.; Bilsborough, J.; Jeukendrup, A.; Morton, J.P.; Phillips, S.; Armstrong, L.; Burke, L.M.; Close, G.L. UEFA expert group statement on nutrition in elite football. Current evidence to inform practical recommendations and guide future research. Br. J. Sports Med. 2021, 55, 416. [Google Scholar]
- Kerksick, C.M.; Wilborn, C.D.; Roberts, M.D.; Smith-Ryan, A.; Kleiner, S.M.; Jäger, R.; Collins, R.; Cooke, M.; Davis, J.N.; Galvan, E. ISSN exercise & sports nutrition review update: Research & recommendations. J. Int. Soc. Sports Nutr. 2018, 15, 1–57. [Google Scholar]
- Galan-Lopez, P.; Ries, F.; Gisladottir, T.; Domínguez, R.; Sánchez-Oliver, A.J. Healthy lifestyle: Relationship between Mediterranean diet, body composition and physical fitness in 13 to 16-years old Icelandic students. Int. J. Environ. Res. Public Health 2018, 15, 2632. [Google Scholar] [CrossRef] [Green Version]
- Galan-Lopez, P.; Sánchez-Oliver, A.J.; Ries, F.; González-Jurado, J.A. Mediterranean diet, physical fitness and body composition in sevillian adolescents: A healthy lifestyle. Nutrients 2019, 11, 2009. [Google Scholar]
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Weight status, adherence to the Mediterranean diet, and physical fitness in Spanish children and adolescents: The Active Health Study. Nutrients 2020, 12, 1680. [Google Scholar] [CrossRef] [PubMed]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health benefits of the Mediterranean diet: Metabolic and molecular mechanisms. J. Gerontol. Ser. A 2018, 73, 318–326. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.E.; DeCesare, K.N.; Johnson, A.; Kress, K.S.; Inman, C.L.; Weiss, E.P. Short-Term Mediterranean Diet Improves Endurance Exercise Performance: A Randomized-Sequence Crossover Trial. J. Am. Coll. Nutr. 2019, 38, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, S.G.; Fernández, N.H.; Hernández, C.R.; Nissensohn, M.; Román-Viñas, B.; Serra-Majem, L. KIDMED test; prevalence of low adherence to the Mediterranean Diet in children and young; a systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- Valadés Cerrato, D.; Chena Sinovas, M.; Pérez López, A.; Álvarez Valverde, I.; Rubio Arias, J.Á.; Ramos Campo, D.J.; Bores Cerezal, A. Influence of body composition on vertical jump performance according with the age and the playing position in football players. Nutr. Hosp. 2015, 32, 299–307. [Google Scholar]
- Alvarado, M.U. Nutrition for young soccer players. Int. J. Soccer Sci. 2005, 3, 12–20. [Google Scholar]
- Spehnjak, M.; Gušić, M.; Molnar, S.; Baić, M.; Andrašić, S.; Selimi, M.; Mačak, D.; Madić, D.M.; Fišer, S.Ž.; Sporiš, G. Body Composition in Elite Soccer Players from Youth to Senior Squad. Int. J. Environ. Res. Public Health 2021, 18, 4982. [Google Scholar] [CrossRef]
- Cárdenas-Fernández, V.; Chinchilla-Minguet, J.L.; Castillo-Rodríguez, A. Somatotype and body composition in young soccer players according to the playing position and sport success. J. Strength Cond. Res. 2019, 33, 1904–1911. [Google Scholar] [CrossRef]
- Arroyo, M.; González-de-Suso, J.M.; Sanchez, C.; Ansotegui, L.; Rocandio, A.M. Body image and body composition: Comparisons of young male elite soccer players and controls. Int. J. Sport Nutr. Exerc. Metab. 2008, 18, 628–638. [Google Scholar] [CrossRef] [Green Version]
- Bernal-Orozco, M.F.; Posada-Falomir, M.; Quiñónez-Gastélum, C.M.; Plascencia-Aguilera, L.P.; Arana-Nuño, J.R.; Badillo-Camacho, N.; Márquez-Sandoval, F.; Holway, F.E.; Vizmanos-Lamotte, B. Anthropometric and body composition profile of young professional soccer players. J. Strength Cond. Res. 2020, 34, 1911. [Google Scholar] [CrossRef]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.; Horswill, C.; Stillman, R.; Van Loan, M.; Bemben, D. Skinfold equations for estimation of body fatness in children and youth. Hum. Biol. 1988, 60, 709–723. [Google Scholar]
- National Center for Health Statistics. Growth Charts. Available online: https://www.cdc.gov/growthcharts/percentile_data_files.htm (accessed on 6 October 2021).
- Rei, M.; Severo, M.; Rodrigues, S. Reproducibility and validity of the Mediterranean Diet Quality Index (KIDMED Index) in a sample of Portuguese adolescents. Br. J. Nutr. 2021, 1–12. [Google Scholar] [CrossRef]
- Gledhill, A.; Harwood, C.; Forsdyke, D. Psychosocial factors associated with talent development in football: A systematic review. Psychol. Sport Exerc. 2017, 31, 93–112. [Google Scholar] [CrossRef]
- Saward, C.; Morris, J.G.; Nevill, M.E.; Minniti, A.M.; Sunderland, C. Psychological characteristics of developing excellence in elite youth football players in English professional academies. J. Sports Sci. 2020, 38, 1380–1386. [Google Scholar] [CrossRef] [PubMed]
- Vicente-Rodriguez, G.; Jimenez-Ramirez, J.; Ara, I.; Serrano-Sanchez, J.; Dorado, C.; Calbet, J. Enhanced bone mass and physical fitness in prepubescent footballers. Bone 2003, 33, 853–859. [Google Scholar] [CrossRef]
- Randers, M.B.; Petersen, J.; Andersen, L.J.; Krustrup, B.R.; Hornstrup, T.; Nielsen, J.J.; Nordentoft, M.; Krustrup, P. Short-term street soccer improves fitness and cardiovascular health status of homeless men. Eur. J. Appl. Physiol. 2012, 112, 2097–2106. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Martin, A.; Garcia-Unanue, J.; Martínez-Rodríguez, A.; Manzano-Carrasco, S.; Felipe, J.L.; Carvalho, M.J.; Gallardo, L.; Sanchez-Sanchez, J. The Effects of Football Practice on Nutritional Status and Body Composition in Children: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2562. [Google Scholar] [CrossRef] [PubMed]
- Carl, R.L.; Johnson, M.D.; Martin, T.J. Promotion of healthy weight-control practices in young athletes. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ørntoft, C.; Larsen, M.N.; Madsen, M.; Sandager, L.; Lundager, I.; Møller, A.; Hansen, L.; Madsen, E.E.; Elbe, A.-M.; Ottesen, L. Physical Fitness and Body Composition in 10–12-Year-Old Danish Children in Relation to Leisure-Time Club-Based Sporting Activities. BioMed Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chanavat, N.; Desbordes, M.; Lorgnier, N. Routledge Handbook of Football Marketing; Taylor & Francis: Oxfordshire, UK, 2017. [Google Scholar]
- Hammami, M.A.; Ben Abderrahmane, A.; Nebigh, A.; Le Moal, E.; Ben Ounis, O.; Tabka, Z.; Zouhal, H. Effects of a soccer season on anthropometric characteristics and physical fitness in elite young soccer players. J. Sports Sci. 2013, 31, 589–596. [Google Scholar] [CrossRef]
- Sánchez-Díaz, S.; Yanci, J.; Castillo, D.; Scanlan, A.T.; Raya-González, J. Effects of Nutrition Education Interventions in Team Sport Players. A Systematic Review. Nutrients 2020, 12, 3664. [Google Scholar] [CrossRef]
- McCarthy, H.; Cole, T.; Fry, T.; Jebb, S.; Prentice, A. Body fat reference curves for children. Int. J. Obes. 2006, 30, 598–602. [Google Scholar] [CrossRef] [Green Version]
- López, A.L.; Vélez, J.D.; García, A.M.; Arango, E.F. Concurrent validity of five prediction equations to evaluate fat percentage in a sports group expected to yield high performance from Medellín, Colombia. Biomédica 2021, 41, 131–144. [Google Scholar] [CrossRef]
- Nikolaidis, P.T. Elevated body mass index and body fat percentage are associated with decreased physical fitness in soccer players aged 12–14 years. Asian J. Sports Med. 2012, 3, 168. [Google Scholar] [CrossRef]
- Martinez-Vizcaino, V.; Martínez, M.S.; Pacheco, B.N.; López, M.S.; García-Prieto, J.C.; Nino, C.T.; Palencia, N.A.; Aguilar, F.S.; Rodríguez-Artalejo, F. Trends in excess of weight, underweight and adiposity among Spanish children from 2004 to 2010: The Cuenca Study. Public Health Nutr. 2012, 15, 2170–2174. [Google Scholar] [CrossRef] [Green Version]
- Aranceta-Bartrina, J.; Gianzo-Citores, M.; Pérez-Rodrigo, C. Prevalencia de sobrepeso, obesidad y obesidad abdominal en población española entre 3 y 24 años. Estudio ENPE. Rev. Esp. Cardiol. 2020, 73, 290–299. [Google Scholar] [CrossRef]
- Campa, F.; Silva, A.M.; Iannuzzi, V.; Mascherini, G.; Benedetti, L.; Toselli, S. The role of somatic maturation on bioimpedance patterns and body composition in male elite youth soccer players. Int. J. Environ. Res. Public Health 2019, 16, 4711. [Google Scholar] [CrossRef] [Green Version]
- Gryko, K.; Stastny, P.; Kopiczko, A.; Mikołajec, K.; Pecha, O.; Perkowski, K. Can Anthropometric Variables and Maturation Predict the Playing Position in Youth Basketball Players? J. Hum. Kinet. 2019, 69, 109. [Google Scholar] [CrossRef] [Green Version]
- Moreno, L.A.; Leon, J.F.; Seron, R.; Mesana, M.I.; Fleta, J. Body composition in young male football (soccer) players. Nutr. Res. 2004, 24, 235–242. [Google Scholar] [CrossRef]
- Leão, C.; Camões, M.; Clemente, F.M.; Nikolaidis, P.T.; Lima, R.; Bezerra, P.; Rosemann, T.; Knechtle, B. Anthropometric profile of soccer players as a determinant of position specificity and methodological issues of body composition estimation. Int. J. Environ. Res. Public Health 2019, 16, 2386. [Google Scholar] [CrossRef] [Green Version]
- Espada, M.; Figueiredo, T.; Ferreira, C.; Santos, F. Body composition and physical fitness analysis in different field position U-15 soccer players. J. Phys. Educ. Sport 2020, 20, 1917–1924. [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Gerritsen, S.; Renker-Darby, A.; Harré, S.; Rees, D.; Raroa, D.A.; Eickstaedt, M.; Sushil, Z.; Allan, K.; Bartos, A.E.; Waterlander, W.E. Improving low fruit and vegetable intake in children: Findings from a system dynamics, community group model building study. PLoS ONE 2019, 14, e0221107. [Google Scholar] [CrossRef] [Green Version]
- Alacid, F.; Vaquero-Cristóbal, R.; Sánchez-Pato, A.; Muyor, J.M.; López-Miñarro, P.Á. Adhesión a la dieta mediterránea y relación con los parámetros antropométricos de mujeres jóvenes kayakistas. Nutr. Hosp. 2014, 29, 121–127. [Google Scholar]
- Kelly, S.; Melnyk, B.M.; Belyea, M. Predicting physical activity and fruit and vegetable intake in adolescents: A test of the information, motivation, behavioral skills model. Res. Nurs. Health 2012, 35, 146–163. [Google Scholar] [CrossRef]
- Silva, D.A.S.; Silva, R.J.d.S. Association between physical activity level and consumption of fruit and vegetables among adolescents in northeast Brazil. Rev. Paul. Pediatr. 2015, 33, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Rani, R.; Dharaiya, C.N.; Singh, B. Importance of not skipping breakfast: A review. Int. J. Food Sci. Technol. 2021, 56, 28–38. [Google Scholar] [CrossRef]
- Watanabe, Y.; Saito, I.; Henmi, I.; Yoshimura, K.; Maruyama, H.; Yamauchi, K.; Matsuo, T.; Kato, T.; Tanigawa, T.; Kishida, T. Skipping breakfast is correlated with obesity. J. Rural Med. 2014, 2887. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, E.; Hatamoto, Y.; Yonekura, S.; Tanaka, H. Skipping breakfast reduces energy intake and physical activity in healthy women who are habitual breakfast eaters: A randomized crossover trial. Physiol. Behav. 2017, 174, 89–94. [Google Scholar] [CrossRef]
- Philippou, E.; Middleton, N.; Pistos, C.; Andreou, E.; Petrou, M. The impact of nutrition education on nutrition knowledge and adherence to the Mediterranean Diet in adolescent competitive swimmers. J. Sci. Med. Sport 2017, 20, 328–332. [Google Scholar] [CrossRef]
- Johnson, L.; Toumpakari, Z.; Papadaki, A. Social gradients and physical activity trends in an obesogenic dietary pattern: Cross-sectional analysis of the UK National Diet and Nutrition Survey 2008–2014. Nutrients 2018, 10, 388. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Rodríguez, A.; Martínez-Olcina, M.; Hernández-García, M.; Rubio-Arias, J.Á.; Sánchez-Sánchez, J.; Lara-Cobos, D.; Vicente-Martínez, M.; Carvalho, M.J.; Sánchez-Sáez, J.A. Mediterranean diet adherence, body composition and performance in beach handball players: A cross sectional study. Int. J. Environ. Res. Public Health 2021, 18, 2837. [Google Scholar] [CrossRef]
- Cantoral, A.; Téllez-Rojo, M.M.; Ettinger, A.; Hu, H.; Hernández-Ávila, M.; Peterson, K. Early introduction and cumulative consumption of sugar-sweetened beverages during the pre-school period and risk of obesity at 8–14 years of age. Pediatr. Obes. 2016, 11, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ersoy, N.; Ersoy, G.; Kutlu, M. Assessment of hydration status of elite young male soccer players with different methods and new approach method of substitute urine strip. J. Int. Soc. Sports Nutr. 2016, 13, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aragón-Vargas, L.F.; Moncada-Jiménez, J.; Hernández-Elizondo, J.; Barrenechea, A.; Monge-Alvarado, M. Evaluation of pre-game hydration status, heat stress, and fluid balance during professional soccer competition in the heat. Eur. J. Sport Sci. 2009, 9, 269–276. [Google Scholar] [CrossRef] [Green Version]
- Australia, S.D.; Middleton, L.; Logan, R.; Garden, L. Fuelling Active Kids. Junior Soccer Player. A Guide for Parents, Coaches and Team Managers; Sports Dietitians Australia: Melbourne, VIC, Australia, 2013. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KIDMED Test | Scoring |
|---|---|
| 1. Consume natural fruit juice or fruit juice every day | +1 |
| 2. Have a second fruit every day | +1 |
| 3. Eat fresh or cooked vegetables once a day | +1 |
| 4. Eat fresh or cooked vegetables more than once a day | +1 |
| 5. Consume fish at least 2–3 times a week | +1 |
| 6. Go once or more times a week to a fast-food restaurant (burger joint, pizzeria, etc.) | −1 |
| 7. Eat legumes more than once a week (chickpeas, beans, lentils, peas, etc.) | +1 |
| 8. Consume pasta, rice, bread, and potato almost every day (5 or more per week) | +1 |
| 9. Have cereals or grains (bread, etc.) for breakfast | +1 |
| 10. Consume nuts at least 2 or 3 times a week (walnuts, hazelnuts, almonds) | +1 |
| 11. Use olive oil at home | +1 |
| 12. Skip breakfast | −1 |
| 13. Have a dairy product for breakfast (yogurt, milk, etc.) | +1 |
| 14. Have commercially baked goods or pastries for breakfast | −1 |
| 15. Consume two yogurts and/or some cheese daily | +1 |
| 16. Consume sweets and candy several times every day | −1 |
| Mean ± SD | |||
|---|---|---|---|
| Anthropometric Parameters | Total (n = 71) | 8–10 Years (n = 26) | 10–12 Years (n = 45) |
| Age (years) | 10.19 ± 1.17 | 8.95 ± 0.63 | 11.01 ± 0.53 *** |
| Weight (kg) | 34.51 ± 5.43 | 30.36 ± 3.98 | 37.27 ± 4.44 *** |
| Height (cm) | 141.42 ± 8.37 | 135.15 ± 6.25 | 145.60 ± 6.88 *** |
| BMI (kg/m2) | 17.17 ± 1.54 | 16.59 ± 1.54 | 17.55 ± 1.42 ** |
| Weight percentile | 58.36 ± 21.95 | 60.39 ± 24.89 | 57.02 ± 19.94 |
| Height percentile | 59.72 ± 27.41 | 59.20 ± 27.78 | 60.07 ± 27.48 |
| BMI percentile | 54.43 ± 22.21 | 55.07 ± 24.78 | 54.01 ± 20.60 |
| Triceps skinfold (mm) | 9.55 ± 3.23 | 8.81 ± 3.18 | 10.04 ± 3.20 |
| Calf skinfold (mm) | 8.74 ± 3.56 | 8.11 ± 3.77 | 9.16 ± 3.40 |
| Body fat (Slaughter equation) (%) | 14.44 ± 4.75 | 13.43 ± 4.91 | 15.11 ± 4.58 * |
| Body fat (kg) | 5.11 ± 2.28 | 4.19 ± 2.13 | 5.73 ± 2.18 *** |
| Anthropometric Parameters | Goalkeeper (n = 12) | Defender (n = 19) | Midfielder (n = 24) | Forward (n = 16) |
|---|---|---|---|---|
| Age (years) | 10.19 ± 1.32 | 10.16 ± 0.97 | 10.34 ± 1.34 | 10.21 ± 1.13 |
| Weight (kg) | 37.53 ± 4.91 | 33.88 ± 3.69 ** | 33.79 ± 5.16 ** | 32.86 ± 5.57 * |
| Height (cm) | 143.92 ± 7.04 | 139.88 ± 6.39 | 142.27 ± 8.30 | 141.57 ± 11.31 |
| BMI (kg/m2) | 18.13 ± 2.08 | 17.28 ± 1.02 | 17.01 ± 1.21 | 16.65 ± 1.16 * |
| Weight percentile | 74.26 ± 14.24 | 57.75 ± 16.67 ** | 55.81 ± 22.27 ** | 52.94 ± 24.33 * |
| Height percentile | 71.18 ± 26.81 | 54.31 ± 24.80 | 60.88 ± 25.46 | 57.46 ± 32.80 |
| BMI percentile | 64.69 ± 25.15 | 58.52 ± 16.01 | 51.46 ± 19.51 | 44.73 ± 23.41 * |
| Triceps skinfold (mm) | 11.44 ± 3.88 | 9.37 ± 3.19 | 9.37 ± 2.57 | 8.05 ± 2.05 * |
| Calf skinfold (mm) | 10.45 ± 3.15 | 8.65 ± 3.11 | 8.19 ± 2.99 * | 7.55 ± 2.69 ** |
| Body fat (Slaughter equation) (%) | 17.09 ± 4.86 | 14.25 ± 4.34 | 13.91 ± 3.88 * | 12.47 ± 3.26 * |
| Body fat (kg) | 6.51 ± 2.28 | 4.87 ± 1.77 | 4.97 ± 2.19 * | 4.28 ± 1.66 ** |
| Total KIDMED Score | 7.83 ± 2.03 | ||
|---|---|---|---|
| ITEMS | Yes (%) | No (%) | p-Value |
| 1 | 81.69 | 18.31 | <0.001 |
| 2 | 50.70 | 49.30 | 1.000 |
| 3 | 54.93 | 45.07 | 0.477 |
| 4 | 19.72 | 80.28 | <0.001 |
| 5 | 70.42 | 29.58 | 0.001 |
| 6 | 15.49 | 84.51 | <0.001 |
| 7 | 98.59 | 1.41 | <0.001 |
| 8 | 90.14 | 9.86 | <0.001 |
| 9 | 85.92 | 14.08 | <0.001 |
| 10 | 28.17 | 71.83 | <0.001 |
| 11 | 100.00 | 0.00 | <0.001 |
| 12 | 21.13 | 78.87 | <0.001 |
| 13 | 91.55 | 8.45 | <0.001 |
| 14 | 23.94 | 76.06 | <0.001 |
| 15 | 70.42 | 29.58 | 0.001 |
| 16 | 18.31 | 81.69 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos-Sánchez, G.; Cruz-Chamorro, I.; Perza-Castillo, J.L.; Vicente-Salar, N. Body Composition Assessment and Mediterranean Diet Adherence in U12 Spanish Male Professional Soccer Players: Cross-Sectional Study. Nutrients 2021, 13, 4045. https://doi.org/10.3390/nu13114045
Santos-Sánchez G, Cruz-Chamorro I, Perza-Castillo JL, Vicente-Salar N. Body Composition Assessment and Mediterranean Diet Adherence in U12 Spanish Male Professional Soccer Players: Cross-Sectional Study. Nutrients. 2021; 13(11):4045. https://doi.org/10.3390/nu13114045
Chicago/Turabian StyleSantos-Sánchez, Guillermo, Ivan Cruz-Chamorro, José Luis Perza-Castillo, and Néstor Vicente-Salar. 2021. "Body Composition Assessment and Mediterranean Diet Adherence in U12 Spanish Male Professional Soccer Players: Cross-Sectional Study" Nutrients 13, no. 11: 4045. https://doi.org/10.3390/nu13114045
APA StyleSantos-Sánchez, G., Cruz-Chamorro, I., Perza-Castillo, J. L., & Vicente-Salar, N. (2021). Body Composition Assessment and Mediterranean Diet Adherence in U12 Spanish Male Professional Soccer Players: Cross-Sectional Study. Nutrients, 13(11), 4045. https://doi.org/10.3390/nu13114045