
Perineural Epinephrine for Brachial Plexus Block Increases the Incidence of Hypotension during Dexmedetomidine Infusion: A Single-Center, Randomized, Controlled Trial

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
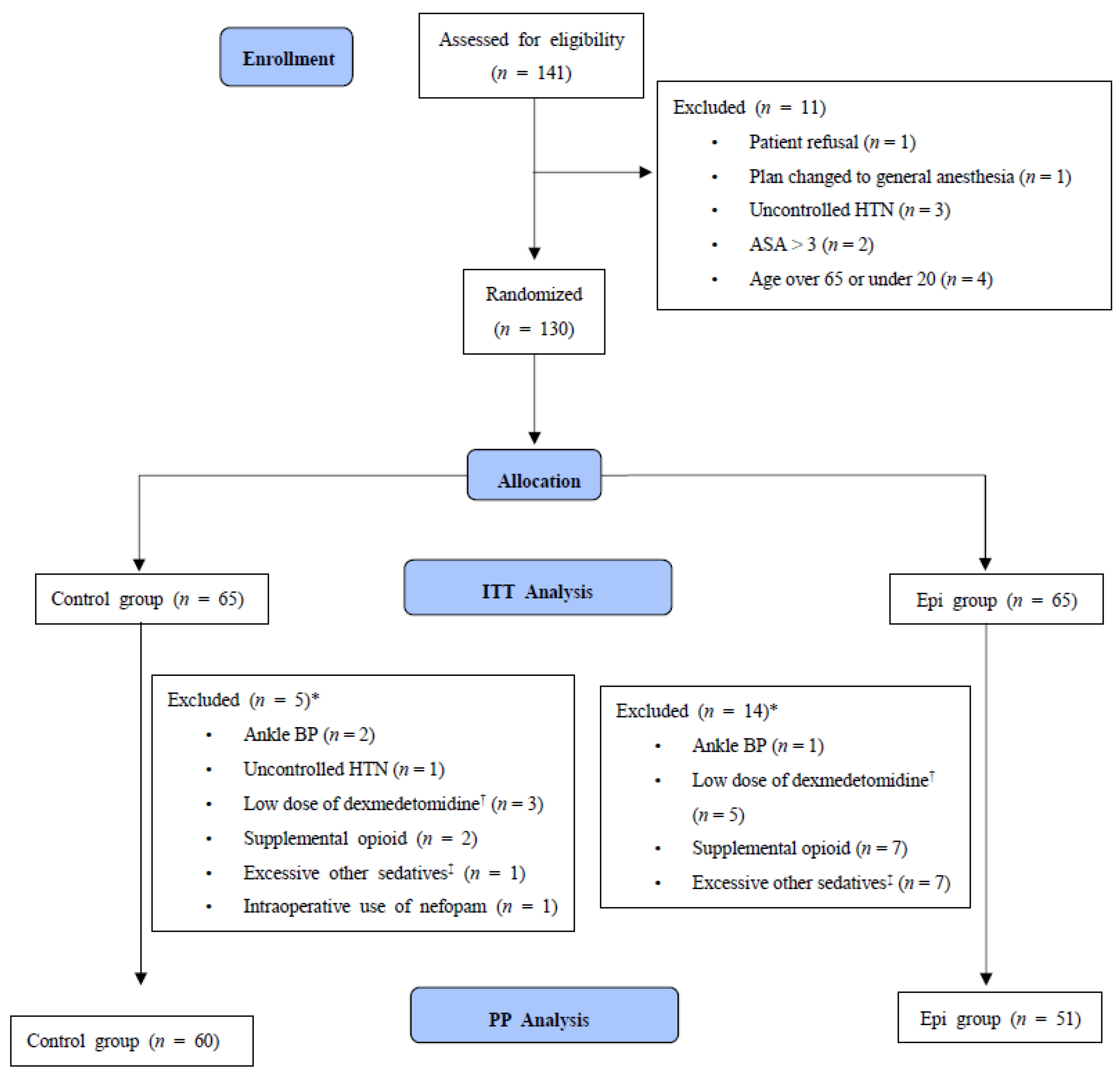
2.1. Study Participants
2.2. Randomization and Minimization of Bias
2.3. Anesthetic Procedures
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.H. Safe Sedation and Hypnosis using Dexmedetomidine for Minimally Invasive Spine Surgery in a Prone Position. Korean J. Pain 2014, 27, 313–320. [Google Scholar] [CrossRef]
- Lee, S. Dexmedetomidine: Present and future directions. Korean J. Anesthesiol. 2019, 72, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Hong, B.; Jung, C.; Jo, Y.; Kang, H.; Chung, W.; Kim, Y.H. Sedation with dexmedetomidine prolongs the analgesic duration of brachial plexus block: A randomised controlled trial. Anaesth. Crit. Care Pain Med. 2019, 38, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, F.W.; Dwyer, T.; Chan, V.W.; Niazi, A.U.; Ogilvie-Harris, D.J.; Oldfield, S. IV and Perineural Dexmedetomidine Similarly Prolong the Duration of Analgesia after Interscalene Brachial Plexus Block: A Randomized, Three-arm, Triple-masked, Placebo-controlled Trial. Anesthesiology 2016, 124, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Gurbet, A.; Basagan-Mogol, E.; Turker, G.; Ugun, F.; Kaya, F.N.; Ozcan, B. Intraoperative infusion of dexmedetomidine reduces perioperative analgesic requirements. Can. J. Anaesth 2006, 53, 646–652. [Google Scholar] [CrossRef] [Green Version]
- Young Hoon, J. The use of adjuvants to local anesthetics: Benefit and risk. Korean J. Pain 2018, 31, 233–234. [Google Scholar]
- Mulroy, M.F.; Hejtmanek, M.R. Prevention of Local Anesthetic Systemic Toxicity. Reg Anesth. Pain Med. 2010, 35, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inf. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [Green Version]
- Wesselink, E.M.; Kappen, T.H.; Torn, H.M.; Slooter, A.J.C.; van Klei, W.A. Intraoperative hypotension and the risk of postoperative adverse outcomes: A systematic review. Br. J. Anaesth. 2018, 121, 706–721. [Google Scholar] [CrossRef] [Green Version]
- Sun, L.Y.; Wijeysundera, D.N.; Tait, G.A.; Beattie, W.S. Association of intraoperative hypotension with acute kidney injury after elective noncardiac surgery. Anesthesiology 2015, 123, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Roshanov, P.S.; Sheth, T.; Duceppe, E.; Tandon, V.; Bessissow, A.; Chan, M.T.V. Relationship between Perioperative Hypotension and Perioperative Cardiovascular Events in Patients with Coronary Artery Disease Undergoing Major Noncardiac Surgery. Anesthesiology 2019, 130, 756–766. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, K.; Ahuja, S.; Khanna, A.K.; Mao, G.; Perez-Protto, S.; Farag, E. Association Between Perioperative Hypotension and Delirium in Postoperative Critically Ill Patients: A Retrospective Cohort Analysis. Anesth. Analg. 2020, 130, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Dogru, K.; Duygulu, F.; Yildiz, K.; Kotanoglu, M.S.; Madenoglu, H.; Boyaci, A. Hemodynamic and blockade effects of high/low epinephrine doses during axillary brachial plexus blockade with lidocaine 1.5%: A randomized, double-blinded study. Reg. Anesth. Pain Med. 2003, 28, 401–405. [Google Scholar] [CrossRef]
- Yang, J.J.; Cheng, H.L.; Shang, R.J.; Shen, J.C.; Shi, J.X.; Wang, H.D. Hemodynamic changes due to infiltration of the scalp with epinephrine-containing lidocaine solution: A hypotensive episode before craniotomy. J. Neurosurg. Anesth. 2007, 19, 31–37. [Google Scholar] [CrossRef]
- Wu, J.; Ji, M.H.; Wang, Z.Y.; Zhu, W.; Yang, J.J.; Peng, Y.G. Blood pressure reduction induced by low dose of epinephrine via different routes in rats. J. Cardiovasc. Pharm. 2013, 62, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Phillips, S.; Hutchinson, S.E.; Bayly, P.; Hollway, T.E. Adrenaline-induced hypotension in neurosurgery. Br. J. Anaesth. 1993, 70, 687–688. [Google Scholar] [CrossRef]
- Kjeldsen, S.E.; Petrin, J.; Weder, A.B.; Julius, S. Contrasting effects of epinephrine on forearm hemodynamics and arterial plasma norepinephrine. Am. J. Hypertens. 1993, 6, 369–375. [Google Scholar] [CrossRef]
- Eugene, A.R. The influences of nitric oxide, epinephrine, and dopamine on vascular tone: Dose-response modeling and simulations. Hosp. Chron. 2016, 11, 1–8. [Google Scholar]
- Belfrage, E. Comparison of β-adrenoceptors mediating vasodilatation in canine subcutaneous adipose tissue and skeletal muscle. Acta Physiol. Scand. 1978, 102, 469–476. [Google Scholar] [CrossRef]
- Hilal-Dandan, R.; Knollmann, B.; Brunton, L. Goodman and Gilman’s the Pharmacological Basis of Therapeutics, 13th ed.; McGraw-Hill Education: New York, NY, USA, 2017. [Google Scholar]
- Byon, H.J.; Ok, S.H.; Lee, S.H.; Kang, S.; Cho, Y.; Han, J.Y. Dexmedetomidine Inhibits Phenylephrine-induced Contractions via Alpha-1 Adrenoceptor Blockade and Nitric Oxide Release in Isolated Rat Aortae. Int. J. Med. Sci. 2017, 14, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, L.; Yu, W.; Wang, T.; Zhang, L.; Heerdt, P.M.; Gelb, A.W. Blood pressure targets in perioperative care: Provisional considerations based on a comprehensive literature review. Hypertension 2018, 72, 806–817. [Google Scholar] [CrossRef]
- Futier, E.; Lefrant, J.Y.; Guinot, P.G.; Godet, T.; Lorne, E.; Cuvillon, P. Effect of Individualized vs Standard Blood Pressure Management Strategies on Postoperative Organ Dysfunction Among High-Risk Patients Undergoing Major Surgery: A Randomized Clinical Trial. JAMA 2017, 318, 1346–1357. [Google Scholar] [CrossRef] [PubMed]
- Sessler, D.I.; Bloomstone, J.A.; Aronson, S.; Berry, C.; Gan, T.J.; Kellum, J.A. Perioperative Quality Initiative consensus statement on intraoperative blood pressure, risk and outcomes for elective surgery. Br. J. Anaesth. 2019, 122, 563–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Control | Epinephrine | |
|---|---|---|
| (n = 65) | (n = 65) | |
| Age (yr), median (IQR) | 46.0 (31.0–57.0) | 50.0 (38.0–57.0) |
| Sex (M/F) | 26/39 | 25/40 |
| Height (cm), median (IQR) | 164.0 (160.0–173.0) | 167.0 (158.0–174.4) |
| Weight (kg), mean ± SD | 68.2 ± 11.6 | 69.4 ± 13.9 |
| BMI (kg/m2), mean ± SD | 24.7 ± 2.8 | 24.9 ± 3.5 |
| ASA (1/2) | 14/51 | 4/61 |
| Diabetes mellitus | 5 (7.7%) | 4 (6.2%) |
| Hypertension | 13 (20.0%) | 13 (20.0%) |
| Cardiovascular disease | 1 (1.5%) | 0 (0.0%) |
| Anesthesia time (min), median (IQR) | 85.0 (64.0–112.0) | 75.0 (58.0–104.0) |
| Type of procedure | ||
| - Elbow | 10 (15.4%) | 8 (12.3%) |
| - Forearm | 26 (40.0%) | 24 (36.9%) |
| - Hand | 19 (29.2%) | 25 (38.5%) |
| - Wrist | 10 (15.4%) | 8 (12.3%) |
| Type of blockade | ||
| - Axillary | 1 (1.5%) | 2 (3.1%) |
| - Costoclavicular | 5 (7.7%) | 8 (12.3%) |
| - Supraclavicular | 59 (90.8%) | 55 (84.6%) |
| Dexmedetomidine (µg/kg), median (IQR) | 1.3 (1.1–1.5) | 1.2 (1.1–1.4) |
| Baseline sBP (mmHg), mean ± SD | 126.5 ± 12.8 | 127.8 ± 11.4 |
| Baseline mBP (mmHg), mean ± SD | 92.7 ± 9.9 | 93.9 ± 8.1 |
| Baseline dBP (mmHg), mean ± SD | 75.7 ± 9.7 | 76.9 ± 8.1 |
| Baseline heart rate (beats/min), mean ± SD | 73.9 ± 9.9 | 74.1 ± 8.7 |
| ITT | p | PP | p | |||
|---|---|---|---|---|---|---|
| Control | Epinephrine | Control | Epinephrine | |||
| (n = 65) | (n = 65) | (n = 60) | (n = 51) | |||
| Hypotension | 33 (56.9%) | 50 (80.6%) | 0.009 | 31 (57.4%) | 38 (77.6%) | 0.05 |
| Intraoperative | 15 (23.1%) | 35 (53.8%) | 0.001 | 14 (23.3%) | 28 (54.9%) | 0.001 |
| Postoperative | 30 (52.6%) | 42 (71.2%) | 0.062 | 29 (54.7%) | 32 (69.6%) | 0.191 |
| Control | Epinephrine | p | |
|---|---|---|---|
| (n = 65) | (n = 65) | ||
| Hypotension duration (min), median (IQR) | 5.0 (0.0–35.0) | 20.0 (5.0–55.0) | 0.003 |
| Bradycardia, n (%) | 11 (18.6%) | 7 (11.9%) | 0.442 |
| - Intraoperative | 10 (15.4%) | 7 (11.9%) | 0.603 |
| - Postoperative | 7 (12.3%) | 3 (5.1%) | 0.294 |
| Maximum change, mean ± SD | |||
| - sBP, mmHg | 26.1 ± 12.5 | 30.6 ± 12.3 | 0.039 |
| - mBP, mmHg | 23.4 ± 10.3 | 27.0 ± 10.5 | 0.047 |
| - dBP, mmHg | 16.8 ± 10.2 | 20.8 ± 10.1 | 0.027 |
| Heart rate, beats/min | 19.3 ± 7.0 | 15.8 ± 9.0 | 0.014 |
| Drug use *, n (%) | 4 (6.2) | 1 (1.5) | 0.362 |
| LOS in PACU (hr), median (IQR) | 36.0 (34.0–43.0) | 36.0 (33.0–41.0) | 0.754 |
| Time to first rescue analgesic ** (min), mean ± SD | 714.8 ± 195.0 | 654.3 ± 210.0 | 0.292 |
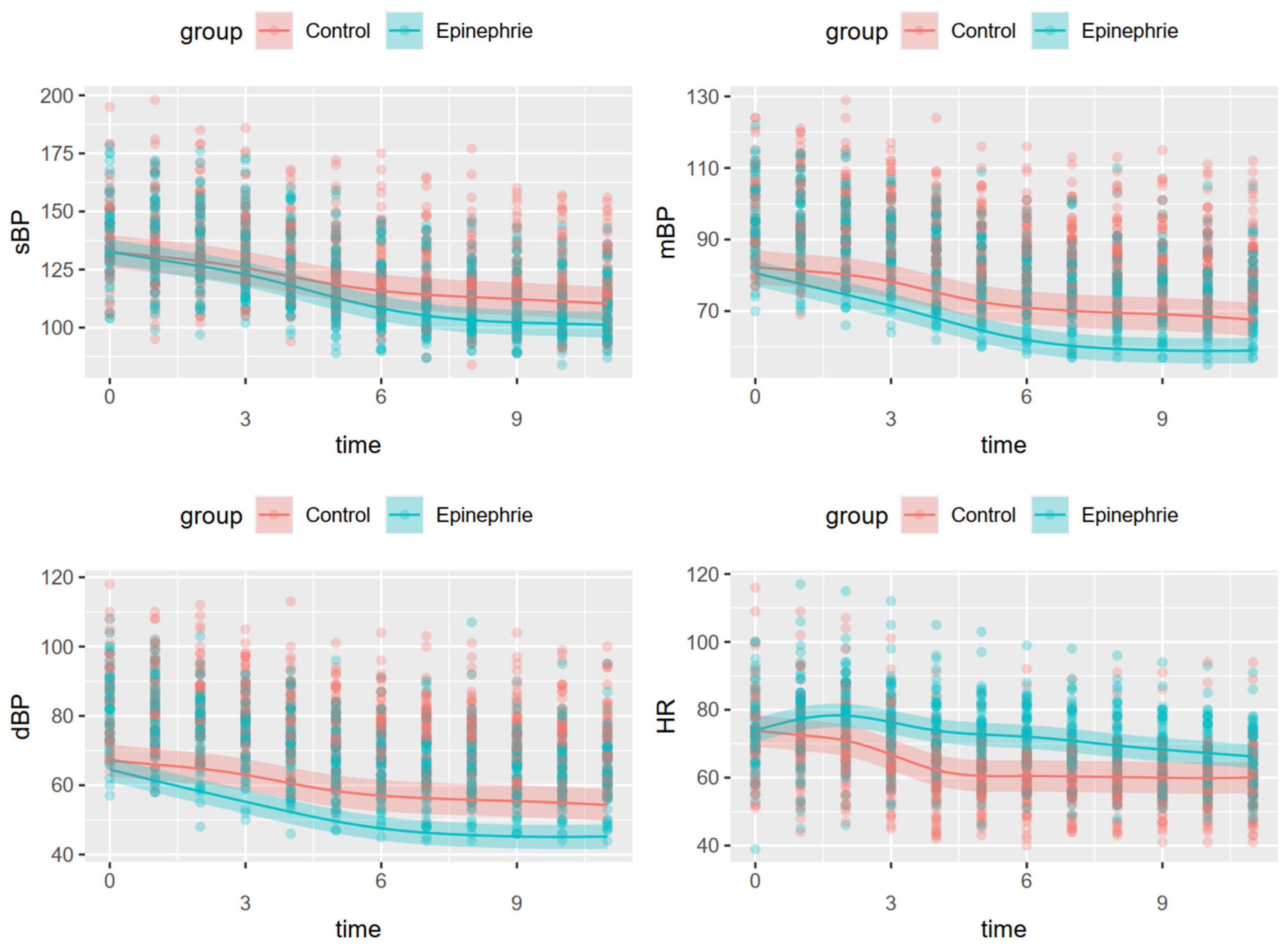
| Dependent Variable | Systolic Blood Pressure | Mean Blood Pressure | Diastolic Blood Pressure | Heart Rate | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted R2 | 0.752 | 0.776 | 0.763 | 0.775 | ||||||||
| Parametric Coefficient | Estimate | SE | p | Estimate | SE | p | Estimate | SE | p | Estimate | SE | p |
| Intercept | 127.294 | 1.697 | <0.001 | 88.883 | 1.116 | <0.001 | 77.401 | 1.087 | <0.001 | 63.327 | 1.113 | <0.001 |
| Group (epinephrine) | –6.019 | 2.400 | 0.012 | –7.596 | 1.578 | <0.001 | –8.188 | 1.538 | <0.001 | 8.286 | 1.575 | <0.001 |
| Smooth Terms | EDF | F | p | EDF | F | p | EDF | F | p | EDF | F | p |
| Time by Control G | 3.991 | 97.87 | <0.001 | 4.797 | 88.77 | <0.001 | 4.321 | 73.97 | <0.001 | 6.411 | 82.45 | <0.001 |
| Time by Epinephrine G | 4.523 | 191.01 | <0.001 | 4.435 | 212.17 | <0.001 | 4.087 | 176.08 | <0.001 | 6.308 | 44.71 | <0.001 |
| Individual | 122.756 | 23.30 | <0.001 | 122.903 | 23.82 | <0.001 | 122.749 | 23.28 | <0.001 | 123.259 | 27.66 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, C.; Hong, B.; Jo, Y.; Jeon, S.; Park, S.; Chung, W.; Ko, Y.; Lee, S.Y.; Lim, C. Perineural Epinephrine for Brachial Plexus Block Increases the Incidence of Hypotension during Dexmedetomidine Infusion: A Single-Center, Randomized, Controlled Trial. J. Clin. Med. 2021, 10, 2579. https://doi.org/10.3390/jcm10122579
Oh C, Hong B, Jo Y, Jeon S, Park S, Chung W, Ko Y, Lee SY, Lim C. Perineural Epinephrine for Brachial Plexus Block Increases the Incidence of Hypotension during Dexmedetomidine Infusion: A Single-Center, Randomized, Controlled Trial. Journal of Clinical Medicine. 2021; 10(12):2579. https://doi.org/10.3390/jcm10122579
Chicago/Turabian StyleOh, Chahyun, Boohwi Hong, Yumin Jo, Seungbin Jeon, Sooyong Park, Woosuk Chung, Youngkwon Ko, Sun Yeul Lee, and Chaeseong Lim. 2021. "Perineural Epinephrine for Brachial Plexus Block Increases the Incidence of Hypotension during Dexmedetomidine Infusion: A Single-Center, Randomized, Controlled Trial" Journal of Clinical Medicine 10, no. 12: 2579. https://doi.org/10.3390/jcm10122579