
The Pertinent Literature of Enhanced Recovery after Surgery Programs: A Bibliometric Approach



1
Center for Musculoskeletal Surgery (CMSC), Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, 10117 Berlin, Germany
2
Department of Respiratory and Critical Care Medicine, The Fourth Medical College of Peking University, Beijing 100035, China
*
Author to whom correspondence should be addressed.
Medicina 2021, 57(2), 172; https://doi.org/10.3390/medicina57020172
Submission received: 31 December 2020
/
Revised: 6 February 2021
/
Accepted: 9 February 2021
/
Published: 17 February 2021
(This article belongs to the Special Issue Nursing and Allied Health Professional Focused Research on Enhanced Recovery after Surgery (ERAS))
Abstract
:Background and Objectives: The programs of enhanced recovery after surgery are the new revolution in surgical departments; however, features of this concept have not been systematically explored. Therefore, the purpose of this study was to explore Enhanced recovery after surgery (ERAS)-related research using bibliometric analysis. Materials and Methods: The search strategy of ERAS programs was conducted in the Web of Science database. Bibliometric analysis was further performed by Excel and Bibliometrix software. The relationship between citation counts and Mendeley readers was assessed by linear regression analysis. Results: 8539 studies from 1994–2019 were included in the present research, with reporting studies originating from 91 countries using 18 languages. The United States (US) published the greatest number of articles. International cooperation was discovered in 82 countries, with the most cooperative country being the United Kingdom. Henrik Kehlet was found to have published the highest number of studies. The journal Anesthesia and Analgesia had the largest number of articles. Linear regression analysis presented a strong positive correlation between citations and Mendeley readers. Most research was related to gastrointestinal surgery in this field. Conclusion: This bibliometric analysis shows the current status of ERAS programs from multiple perspectives, and it provides reference and guidance to scholars for further research.
1. Introduction
Enhanced recovery after surgery (ERAS) is a series of effective perioperative interventions under the instruction of a multidisciplinary team, thus improving the surgical patients’ experiences both psychologically and physiologically [1,2]. Compared with the traditional perspective, the ERAS pathway is the new revolution for surgery, as it significantly decreases surgical complications, hospital stay, overall medical charges, and patient discomfort [3,4,5]. ERAS has a broad prospect of perioperative application, and an increasing number of surgery-related guidelines have been published in recent years. Meanwhile, ERAS management is complex and involves multiple measures, with controversy remaining in its clinical application. Therefore, ERAS programs still need to be continually refined and optimized in practice [6,7]. To improve and guide further research, it is necessary to investigate the current developmental status and research hotspots of ERAS programs in different surgical specialties.
Scientific publication is the core of discipline development and scholarly communication, and the creation of clinical practice guidelines also depends on the strong evidence from the literature [8,9,10]. Bibliometric analysis is a method for discovering the characteristics of a research subject to understand the current status and trend through the literature, and it is commonly used in the medical field [11,12,13,14,15]. Unfortunately, as one of the hot topics in the surgical field, ERAS has not been assessed.
Citations are a significant indicator for the assessment of literature quality in bibliometric studies [16]. However, with the development of internet technology, alternative indicators have also become a promising literature measurement. Mendeley is one of the most frequently used reference management softwares for scholars that is available locally or online. Mendeley readers were recorded by the number of users who saved the publication in their Mendeley library. This is a commonly used indicator to analyze the relationship with citations in bibliometric studies [17,18,19]. Previous studies found a strong positive correlation between Mendeley readers and citations [20,21]. The investigation of the relationship between citation counts and alternative indicators could make up for the deficiency from fewer citations in the early stage and provide another means of helping scholars to assess the value of the literature. However, no literature has assessed the relationship between Mendeley readers and citations in ERAS studies.
The aim of the present study was: (1) to find the study characteristics in ERAS programs from the country, author, journal, type of surgery, and research topic applied by bibliometric analysis; (2) to identify the relationship between citation counts and Mendeley readers in ERAS-related research.
2. Materials and Methods
2.1. Data Sources and Search Strategy
The online database of Web of Science was systematically searched using the following search terms: (Enhanced recovery after surgery OR Enhanced recovery program OR Enhanced recovery pathways OR Accelerated rehabilitation OR Fast track surgery).
2.2. Data Acquisition
Total records from the Web of Science were exported to plain text and Excel format. Excel (Microsoft, Redmond, WA, USA) and Bibliometrix (University of Naples Federico II, Naples, Italy) softwares were used to analyze the results, which included author, document type, number of citations, country, journal quality, digital object identifier, journal impact factor, publication source, institution, abstract, keywords, article title, language, type of surgery, and publication year [22]. The data of Mendeley reader counts were identified from the official website of Mendeley using the article title or digital object identifier.
2.3. Statistical Analysis
Linear regression analysis was performed using the R language (R Core Team, Newark, NJ, USA) to examine the relationship between citations and Mendeley readers and determine the correlation coefficient.
3. Results
3.1. Publication Output
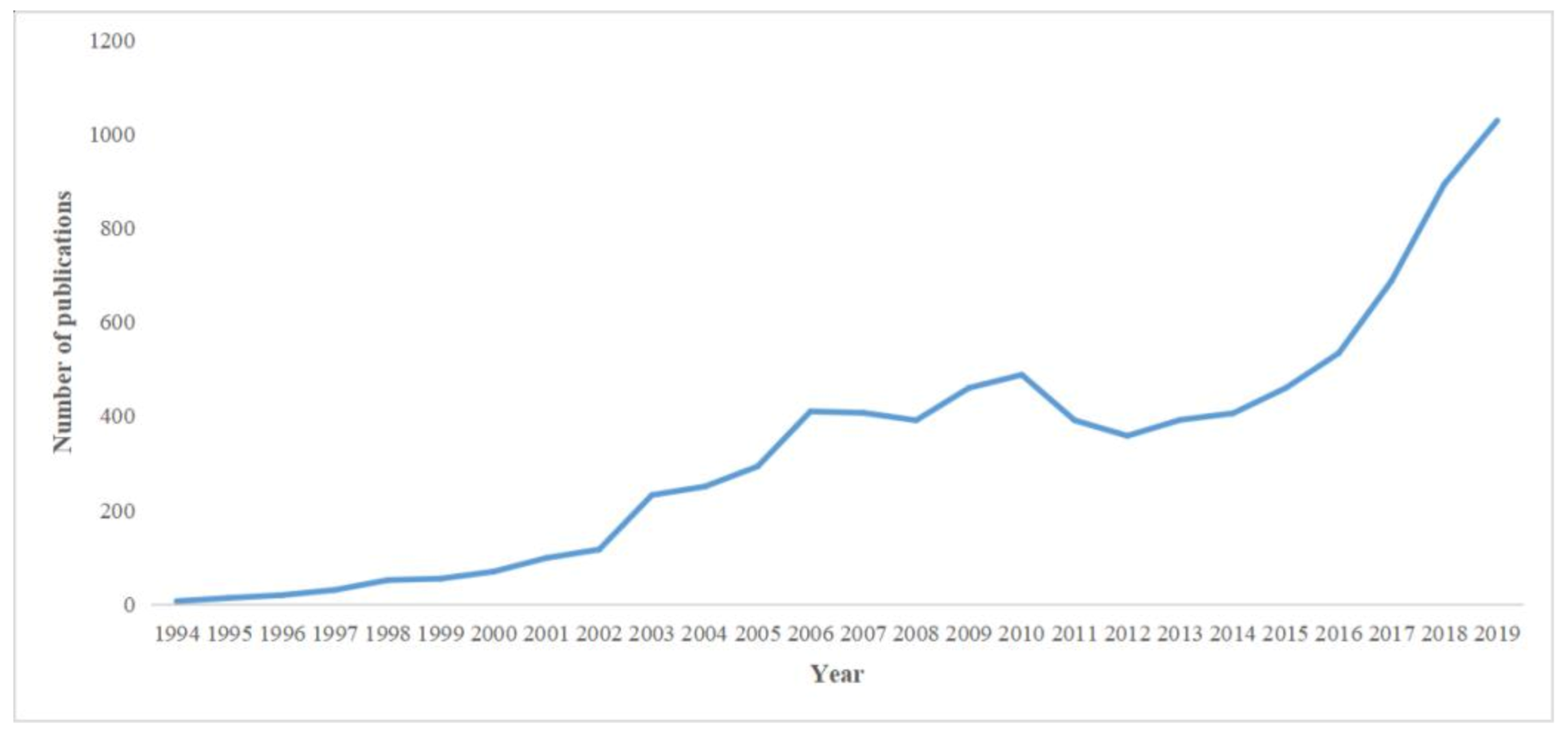
A total of 8539 papers were associated with ERAS programs between 1994 and 2019. Figure 1 shows the annual number of publications and demonstrates an upward trend in recent years, with a large percentage of publications presented during 2014–2019 (4011; 46.9%). The overall publications included 7263 (85.1%) original articles, 968 (11.3%) systematic reviews, and 308 (3.6%) proceedings papers. All included studies were published in 18 languages, with most in English (8156; 95.5%), followed by 233 (2.7%) in German, and 71 (0.8%) in French (Table 1).
3.2. The Status of Global Contributions and Collaborations
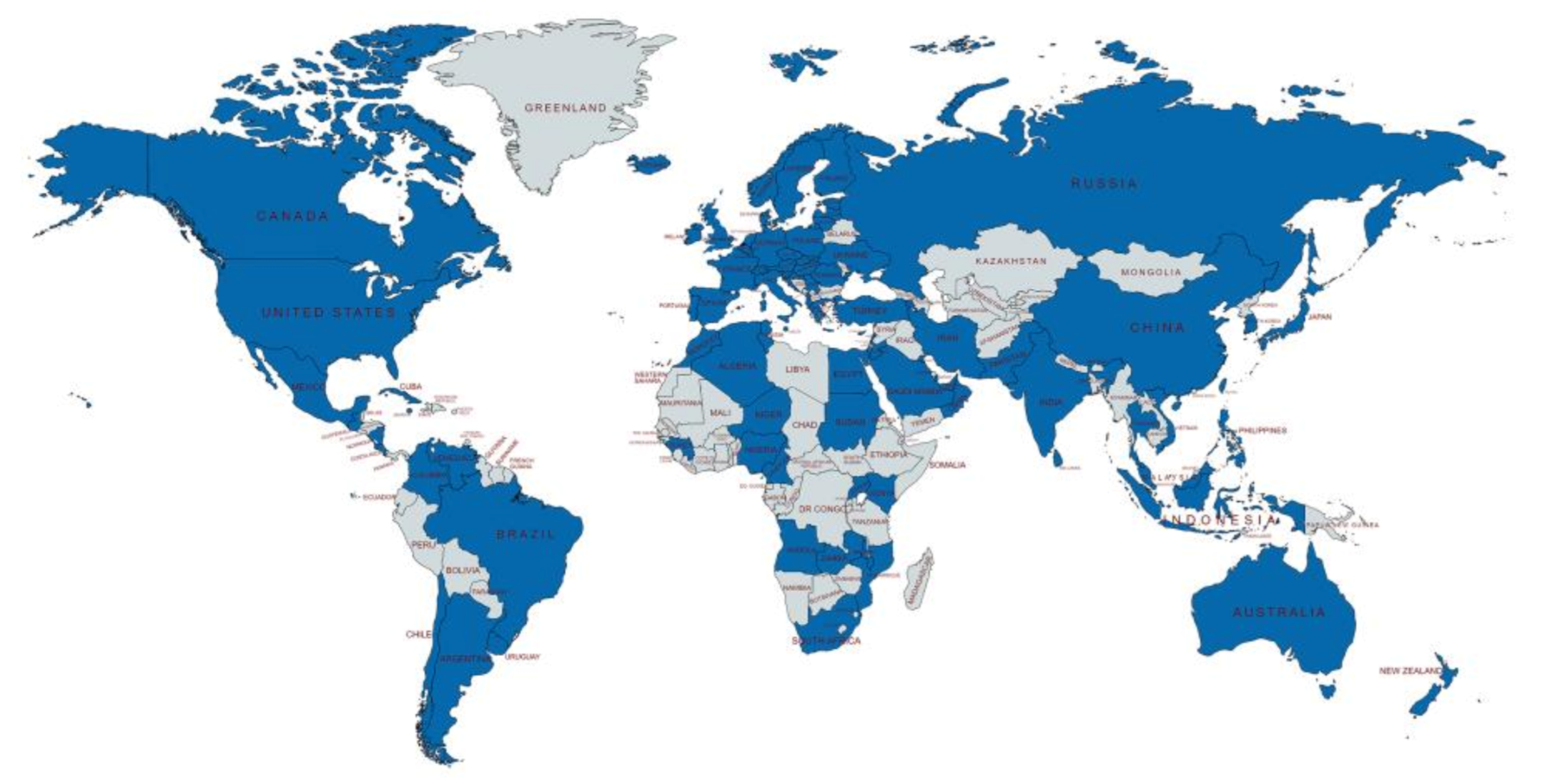
Globally, 91 countries participated in the relevant research of the ERAS program (Figure 2). The United States (US) contributed the most in this field with 2717 (31.8%) papers and also had the highest total citation count (107,682). The United Kingdom (UK) ranked second (818; 9.6%) and China third (663, 7.8%) in the number of publications (Table 2).
Eighty-two countries participated in the collaboration. The UK had the largest number of cooperations with other countries (52), followed by the US (50) and The Netherlands (44). The most frequent collaborations were between the US and Canada (132), followed by the US and the UK (98), and the US and Germany (71). Table 3 shows the number of collaborations between countries, which occurred on more than 30 occasions. Approximately 71.9% (22) of collaborations were from the top 10 most contributing countries.
3.3. Author Contributions
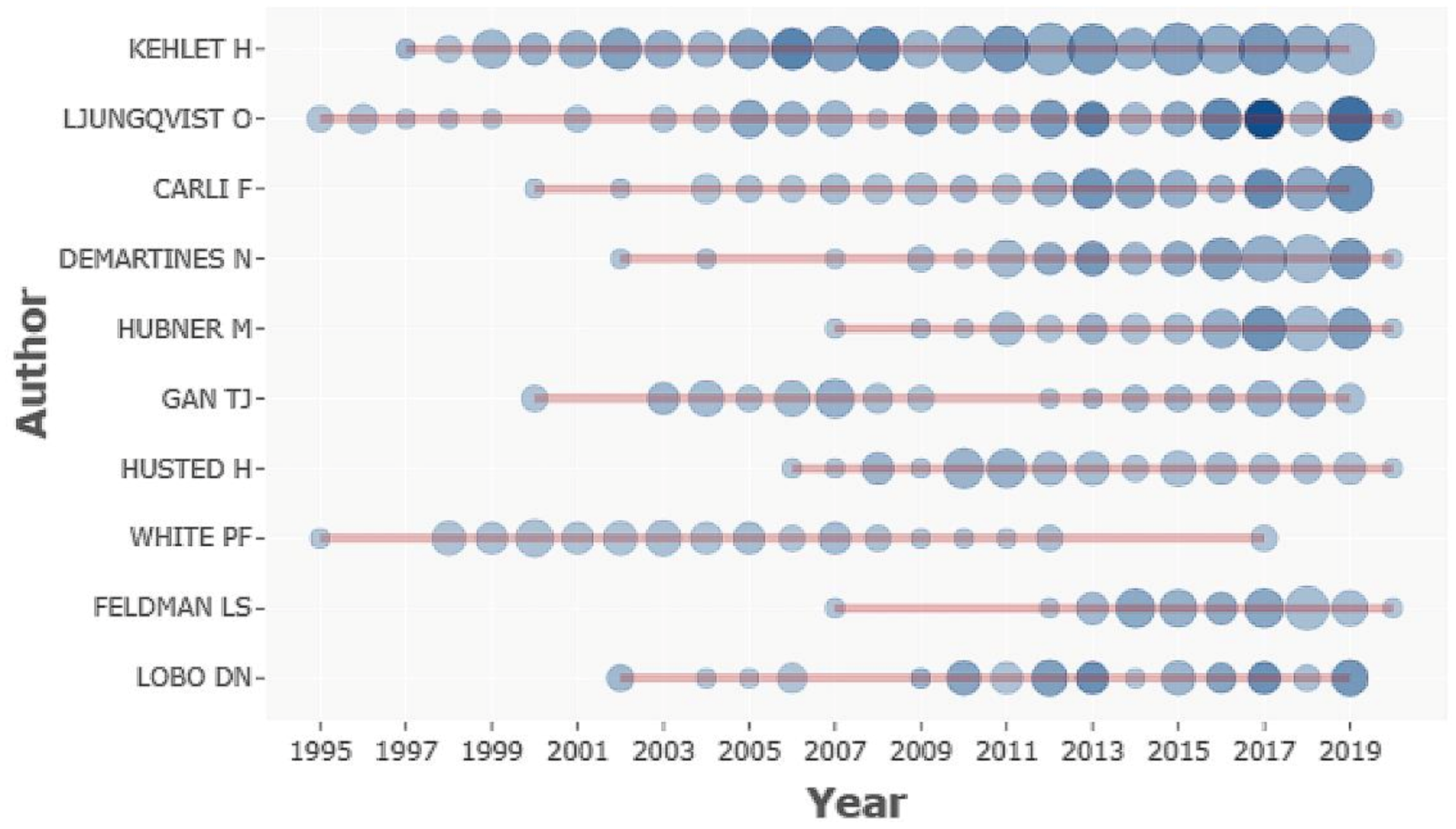
A total of 33,762 authors contributed to ERAS-related research. The percentage of single-authored documents was 3.1% (265). In the top 10 most contributing author list, Henrik Kehlet, from the Department of Surgical Pathophysiology, had the highest number of publications (261), citations (21,497), and h-index (74). The second and third most productive authors in this field are Olle Ljungqvist and Francesco Carli (99 and 88, respectively). The top 10 most productive authors come from seven different institutions, with more than half of the authors being from European countries (Table 4). Figure 3 presented the top 10 authors’ average outputs between 1994 and 2019.
3.4. Journal Information and Type of Surgery
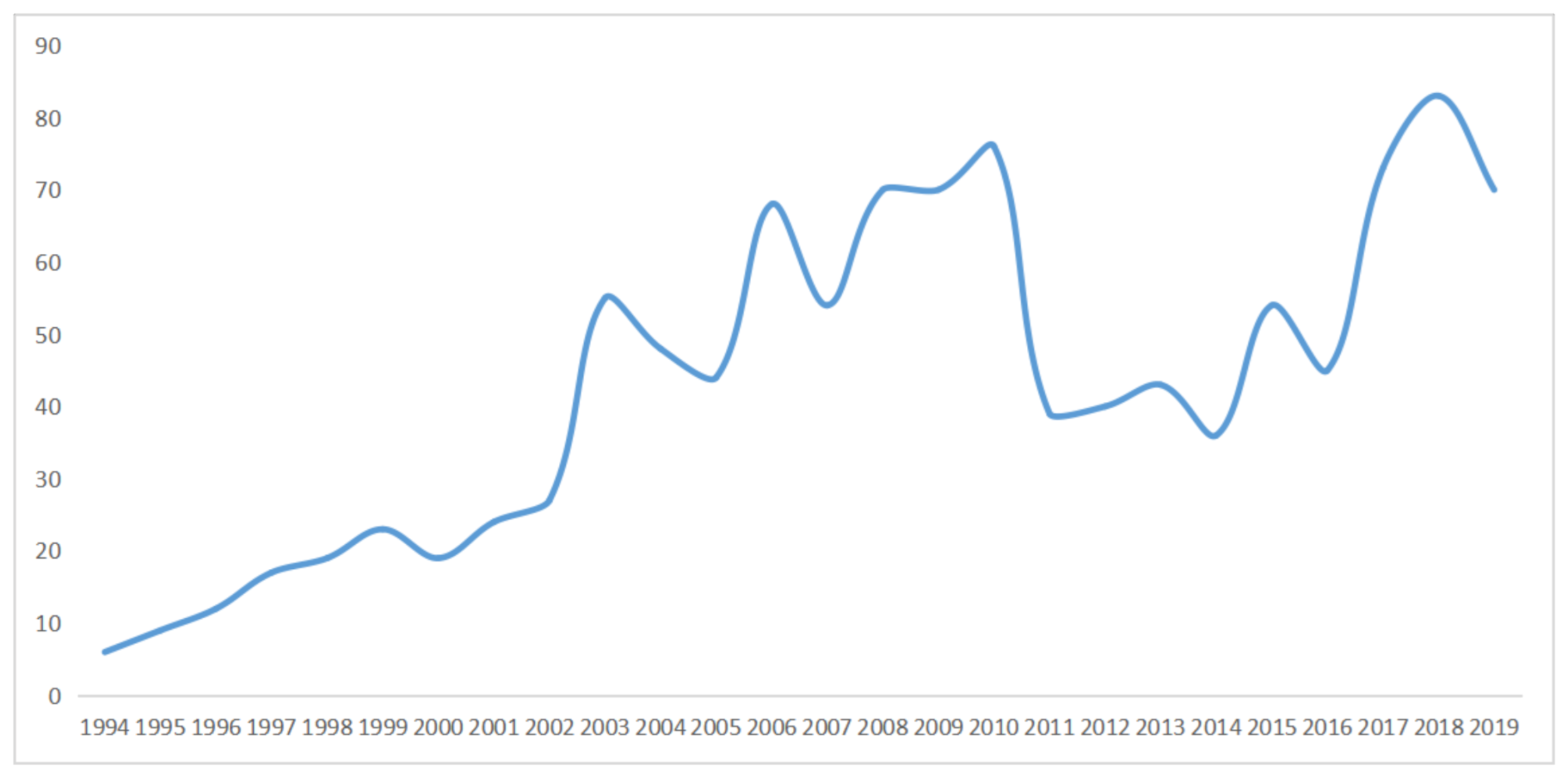
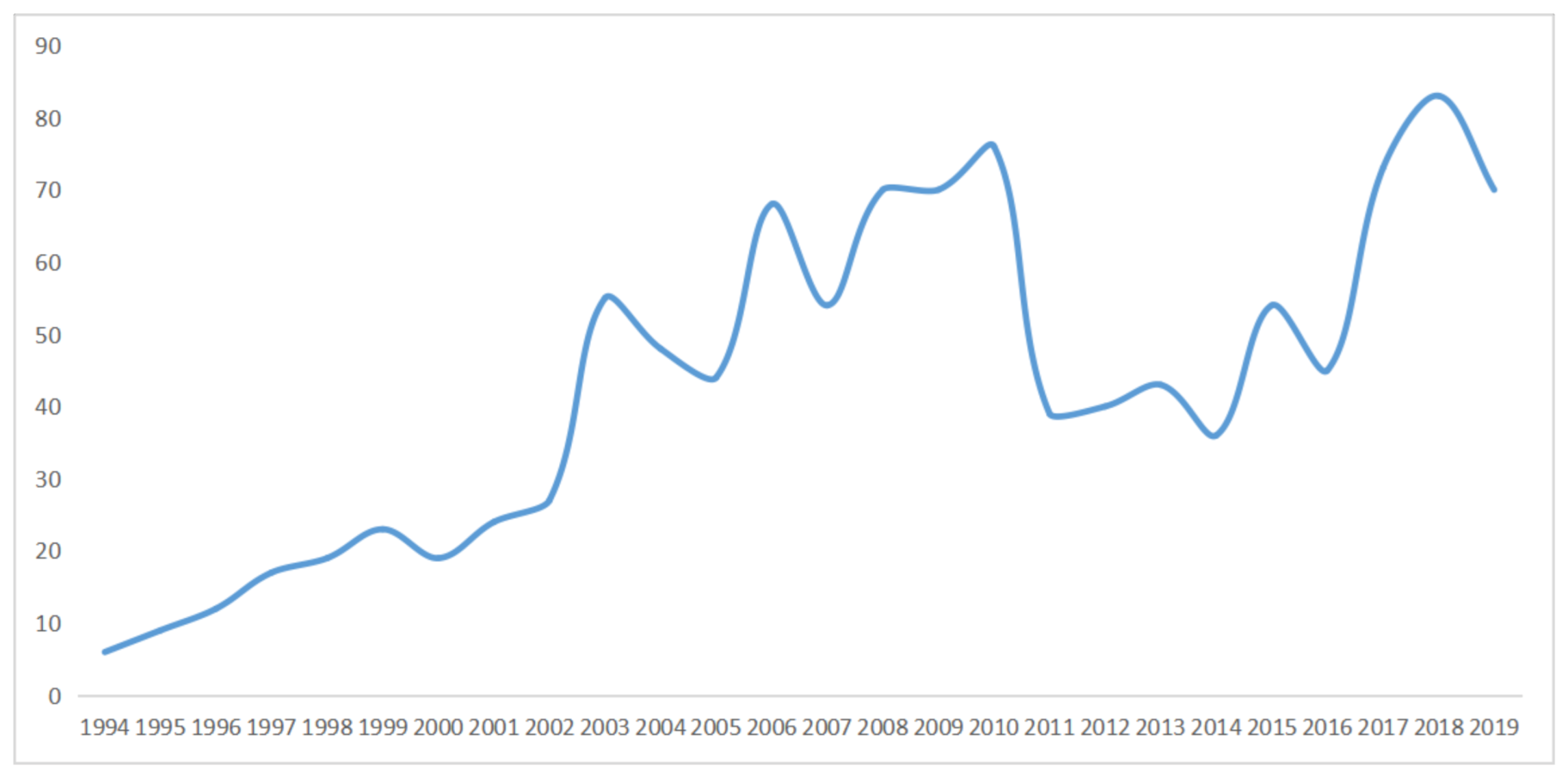
ERAS-related research was published in 1121 journals, and 1014 journals had an impact factor in 2019. Around 27.7% of journals (281) were ranked in the first quartile, 25.4% (258) in the second quartile, 23.9% (243) in the third quartile, and 22.8% (232) in the fourth quartile. Anesthesia and Analgesia had the greatest number of papers (358), followed by the British Journal of Anaesthesia (189), and Acta Anaesthesiologica Scandinavica (147). The rank list of the top 10 journals shows The New England Journal of Medicine has the highest impact factor (74.699), followed by Lancet (60.392), and The Journal of the American Medical Association (45.54; Table 5). Figure 4 presents the year of the journal’s first publication in ERAS, with most journals appearing in 2018 (83), followed by 2010 (76) and 2017 (73).
The surgical information was identified from 6920 papers with 11 clinical departments. Gastrointestinal surgery had the greatest number of papers with ERAS programs (2162), followed by orthopedic surgery (1740), and cardiac surgery (608). In these 11 clinical departments, most journals were from the first quartile (8; Table 6).
3.5. Citations and Mendeley Readers
Of the articles, 8104 had at least one citation. Table 7 shows the top five most cited papers in ERAS, with a range of citations between 970 and 1923 and all publications ranked in the first quartile of the medical journal. In the Mendeley database, Mendeley readers of 8079 publications could be found. Linear regression analysis revealed a significant positive correlation (Pearson r: r = 0.7008; p < 0.001) between citations and Mendeley readers.
3.6. Research Topic
The research topic was identified by thematic maps in Bibliometrix. Ninety-three author keywords occur more than 40 times and were automatically classified into five clusters. Following selection, 72 keywords were further analyzed. Cluster 2 had the largest number of keywords (26), followed by cluster 4 (23), and cluster 1 (11). Cluster 1 was the topic of ERAS programs in orthopedic surgery, with the top three most frequent keywords being “rehabilitation”, “total knee arthroplasty”, and “hip fracture”. Cluster 2 was related to the ERAS protocol in gastrointestinal surgery, with the most popular keywords “enhanced recovery after surgery”, “colorectal surgery”, and “complications”. Cluster 3 was associated with clinical nutrition in surgery, with the most frequent keywords being “surgery”, “outcome”, and “nutrition”. Cluster 4 correlated to ERAS programs of pain management, with the most commonly occurring keywords being “pain”, “postoperative”, and “analgesia”. Cluster 5 correlates with ERAS programs of cardiac surgery, with the most used keywords being “fast-track”, “cardiac surgery”, and “recovery” (Table S1, Supplementary Materials).
4. Discussion
In the present study, bibliometric analysis was used to find ERAS characteristics from multiple perspectives and further identified the relationship between citations and Mendeley readers in this area.
4.1. Principal Findings and Explanation
In this bibliometric analysis, 8539 ERAS-related studies were identified for the period 1994−2019, with the annual global publication showing significant growth since 2014. This condition might be affected by various guidelines published by the ERAS Society in recent years [1,9,10,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44]. Eighteen languages were published in ERAS-related studies. With the exception of Korean and Japanese, other languages are typically used in European countries. English is the dominant language for academic communication, accounting for the largest proportion (95.5%).
Ninety-one countries contributed to the ERAS programs. The list of the top 10 largest contributing countries reported that 70% originated in European countries, with others from Northern America (2) and Asia (1). The US is the most influential country with the highest number of publications. Eighty-two countries were involved in international collaborations. The UK had the highest number of international collaborations (52), followed by the US (50), and The Netherlands (44). The list of the top 31 most frequent collaborations between countries shows 13 countries with more than 30 international cooperations. The most frequent collaborative countries were between the US and Canada (132). Approximately 51.6% of international collaborations were between European countries. These phenomena most likely indicate that geographical location is the potential advantage of fostering intercountry collaborations, which were closer between European countries.
The result from the top 10 most productive authors shows anesthesiologists and surgeons to be predominant in ERAS programs [45,46,47,48]. Increasing attention should be paid to the role of nurses and physiotherapists in multidisciplinary work in the future to improve patient outcomes [49,50,51]. Henrik Kehlet is the most relevant and academic influential author in ERAS. Olle Ljungqvist, the chairman of the ERAS society, ranked second. In addition, Henrik Kehlet was also the top active author in this area, contributing research papers commencing annually in 1997 (Figure 3).
Of the top 10 journals with the greatest number of publications, Anesthesia and Analgesia ranked first place. Most ERAS-related studies were published in anesthesiology journals, with more than half of the top 10 journals being anesthesia-related journals. The list of the top 10 highest impact factor journals shows that a high impact and quality medical journal was interested in the ERAS. All journals were in the first quartile, with impact factors above 20. The year of the journal’s first publication in ERAS indicated that ERAS-related research developed rapidly and popularly, with an increasing amount of new journals producing ERAS-related research, with the highest number of new journals being reached in 2018 (Figure 4). ERAS programs were identified in 11 clinical departments from 6920 papers, with 72.7% (eight) of the most relevant journals being in the first quartile. Gastrointestinal, orthopedic, and cardiac surgeries ranked as the top three most popular departments in ERAS.
Citations are a valuable indicator for assessing the quality of literature. The current study discovered the top five articles with the highest academic influence based on the number of citations. As the main disadvantage of citations could not reflect the value of the literature in the early stages, we further analyzed whether the alternative indicator (Mendeley readers) helps readers determine its academic impact. Simple linear regression analysis of 8079 papers presented a significant positive correlation between citations and Mendeley readers, with the latter being able to be potentially put to use as a reference indicator for research quality assessment in ERAS.
The hot topic was determined according to the frequency of the author’s keywords. Five research themes were identified in the present study. Cluster 1 relates to the ERAS programs in orthopedic surgery. Total knee arthroplasty, total hip arthroplasty, and anterior cruciate ligament reconstruction were the most often performed orthopedic surgeries in ERAS programs. Hip fracture was the most frequently occuring orthopedic disease in ERAS pathways. Functional exercise is one of the most critical components in the perioperative management of orthopedics, improving patient outcomes. Based on the guidelines of the ERAS society perioperative care on total hip replacement and total knee replacement surgery, the evidence level and recommendation grade of early mobilization were strong [32]. Cluster 2 is associated with the ERAS programs in gastrointestinal surgery. Surgeries most related to the ERAS programs were bariatric surgery, gastrectomy, colectomy, and pancreaticoduodenectomy, with the laparoscopic instrument being the most frequently applied. Several studies supported laparoscopic use to achieve a better prognosis than open surgery, with laparoscopic use in gastrointestinal surgery appearing to be more consistent with the concept of ERAS [24,52,53,54]. The National Surgical Quality Improvement Program data are commonly used to assess the outcome of ERAS programs [55,56]. Gastrointestinal surgeons, who utilized ERAS programs for their patients, are more focused on readmission, morbidity, mortality, length of stay, and surgery-related intestinal obstruction. Cluster 3 was associated with clinical nutrition in surgery. Malnutrition was associated with increased postoperative complications and mortality, and effective interventions reduce the risk of complications [57,58,59]. Perioperative nutritional support is one of the most important aspects of ERAS programs. As patients with cancer were more likely to have perioperative malnutrition, ERAS programs placed increasing focus on the nutritional status in cancer patients [37,41,60,61,62]. Early oral nutrition is advocated by ERAS programs in postsurgical recovery, with some studies supporting an early oral diet to safe, feasible, and shorter hospital stays than noninterventional groups. However, whether oral nutrition can reduce postoperative complications requires further investigation [63,64,65]. Cluster 4 correlates to perioperative pain management. Multimodal analgesia is the core of pain control in ERAS programs. A combination of various analgesics and anesthesia techniques will help reduce opioid-related side effects [66]. Currently, epidural analgesia is the most frequently researched anesthesia technique in multimodal analgesia, with the most concerning adverse effects being analgesics postoperative nausea and vomiting. Cluster 5 correlates with ERAS programs in cardiac surgery. The first cardiac surgery report dates back to 1994 and was termed “fast-track recovery” to treat coronary artery bypass grafting patients [67]. The development of ERAS-related cardiac surgery matured over the years, and clinical guidelines in cardiac surgery were published by the ERAS society [31].
4.2. Implications for Research and Practices
In the present study, bibliometric analysis was used to characterize ERAS research from multiple perspectives. These findings will likely help scholars in their further investigations. First, country information could help provide the researcher with information on the current global contribution of countries, as well as providing a reference for further improve and enhance international cooperation. Second, institution lists provide value information to practitioners who want to accept advanced research training in experienced organizations. Third, author information may improve scholarly communication, as it provides a reference to participation in the ERAS meeting or manuscript review. Fourth, journal information likely aids scholars to further subscribe, trace the most related journal in the future, or submit an ERAS-related manuscript as a reference. Fifth, citations and Mendeley readers could assist scholars in quickly finding high-impact articles in the area of ERAS. Finally, the type of surgery and research topic help physicians discover the mainstream discipline, research hotspot, and inadequate research areas. Hence, it may contribute to improving variations across disciplines and provide reference direction for further studies.
4.3. Limitations
The present study has several limitations. First, only a single database was used in this study. Web of Science is the most frequently used database in bibliometric studies, and most of the bibliometric softwares could identify the format from Web of Science [68,69,70,71]. However, the drawback is that some valuable literature from other database sources are most likely missed [13]. Second, the research topic of ERAS contains multiple medical disciplines. Although we selected multiple search terms to identify more relevant research, some potential papers might still be missed. Third, conference proceedings were included in the bibliometric analysis. Therefore, identical content may exist in the literature, as results may be published as a conference abstract as well as a complete journal article [72].
5. Conclusions
In summary, our bibliometric study indicates that the overall global contribution shows an increase in ERAS-related research. The US is the most influential country, whereas the UK is the most cooperative country. Henrik Kehlet is the most relevant, academically influential and active author in this field. Anesthesiologists and surgeons were predominant in the ERAS program. The journal Anesthesia and Analgesia had the most related articles, with anesthesiology-related and high-impact medical journals being the most interested in ERAS. Mendeley readers could be used in ERAS research to assess literature quality. ERAS programs were more likely to be utilized for gastrointestinal, orthopedic, and cardiac surgeries. Pain management and perioperative nutrition were more concerned with ERAS programs.
Supplementary Materials
The following are available online at https://www.mdpi.com/1648-9144/57/2/172/s1, Table S1: Research topic of ERAS.
Author Contributions
Project conceptualization: C.L.; methodology: C.L., Y.C., Z.L. and D.M.; software: C.L.; validation: C.P. and A.T.; formal analysis: C.L.; investigation: C.L.; resources: C.L., Y.C.; data curation: C.L.; writing—original draft preparation: C.L.; writing—review and editing: C.L., Y.C., Z.L., D.M., C.P. and A.T.; supervision: C.P. and A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the PRO-IMPLANT Foundation, Berlin, Germany (https://www.pro-implant-foundation.org).
Institutional Review Board Statement
This study did not involve humans or animals.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery after Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H. Accelerated Recovery after Surgery: A Continuous Multidisciplinary Challenge. Anesthesiology 2015, 123, 1219–1220. [Google Scholar] [CrossRef] [PubMed]
- Büttner, M.; Mayer, A.M.; Büchler, B.; Betz, U.; Drees, P.; Susanne, S. Economic analyses of fast-track total hip and knee arthroplasty: A systematic review. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Gu, H.-Y.; Huang, Z.-D.; Wu, Y.-P.; Zhang, Q.; Luo, J.; Zhang, C.; Fu, Y. Impact of Enhanced Recovery after Surgery on Postoperative Recovery for Pancreaticoduodenectomy: Pooled Analysis of Observational Study. Front. Oncol. 2019, 9, 687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, J.K.; Singh, K.; Dumitru, R.; Chan, E.; Kim, M.P. The Benefits of Enhanced Recovery after Surgery Programs and Their Application in Cardiothoracic Surgery. Methodist Debakey Cardiovasc. J. 2018, 14, 77–88. [Google Scholar] [PubMed]
- Kehlet, H.; Joshi, G.P. Enhanced Recovery after Surgery: Current Controversies and Concerns. Anesth. Analg. 2017, 125, 2154–2155. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H. Enhanced postoperative recovery: Good from afar, but far from good? Anaesthesia 2020, 75 (Suppl. S1), e54–e61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Practice Guidelines for Central Venous Access 2020: An Updated Report by the American Society of Anesthesiologists Task Force on Central Venous Access. Anesthesiology 2020, 132, 8–43. [CrossRef] [PubMed] [Green Version]
- Brindle, M.E.; McDiarmid, C.; Short, K.; Miller, K.; MacRobie, A.; Lam, J.Y.K.; Brockel, M.; Raval, M.V.; Howlett, A.; Lee, K.-S.; et al. Consensus Guidelines for Perioperative Care in Neonatal Intestinal Surgery: Enhanced Recovery after Surgery (ERAS®) Society Recommendations. World J. Surg. 2020, 44, 2482–2492. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery after Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardiothorac. Surg. 2019, 55, 91–115. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Ojeda-Thies, C.; Renz, N.; Margaryan, D.; Perka, C.; Trampuz, A. The global state of clinical research and trends in periprosthetic joint infection: A bibliometric analysis. Int. J. Infect. Dis. 2020, 96, 696–709. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Zhou, Z.; Zhang, H.; Gu, X.; Gu, G.; Guan, X.; Fan, Y.; He, S. Global scientific production of robotic surgery in medicine: A 20-year survey of research activities. Int. J. Surg. 2016, 30, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Ojeda-Thies, C.; Xu, C.; Trampuz, A. Meta-analysis in periprosthetic joint infection: A global bibliometric analysis. J. Orthop. Surg. Res. 2020, 15, 251. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Lee, I.-S.; Lee, H.; Chae, Y. Bibliometric Analysis of Moxibustion Research Trends over the Past 20 Years. J. Clin. Med. Res. 2020, 9, 1254. [Google Scholar] [CrossRef] [PubMed]
- Simopoulou, M.; Sfakianoudis, K.; Maziotis, E.; Rapani, A.; Giannelou, P.; Pantou, A.; Anifandis, G.; Bakas, P.; Vlahos, N.; Pantos, K.; et al. Assessing Clinical Embryology Research: A Global Bibliometric Analysis. Medicina 2020, 56, 210. [Google Scholar] [CrossRef] [PubMed]
- Loomes, D.E.; van Zanten, S.V. Bibliometrics of the top 100 clinical articles in digestive disease. Gastroenterology 2013, 144, 673–676.e5. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, R.; Mahajan, P. Relationship between citation counts and Mendeley readership metrics: A case of top 100 cited papers in Physics. New Libr. World 2016, 117, 229–238. [Google Scholar] [CrossRef]
- Zahedi, Z.; Costas, R.; Wouters, P. Mendeley readership as a filtering tool to identify highly cited publications. J. Assoc. Inf. Sci. Technol. 2017, 68, 2511–2521. [Google Scholar] [CrossRef] [Green Version]
- Naudé, F. Comparing downloads, mendeley readership and Google scholar citations as indicators of article performance. Electron. J. Inf. Syst. Dev. Ctries. 2017, 78, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Thelwall, M. Early Mendeley readers correlate with later citation counts. Scientometrics 2018, 115, 1231–1240. [Google Scholar] [CrossRef]
- Maflahi, N.; Thelwall, M. How quickly do publications get read? The evolution of mendeley reader counts for new articles. J. Assoc. Inf. Sci. Technol. 2018, 69, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Aria, M.; Cuccurullo, C. Bibliometrix: An R-tool for comprehensive science mapping analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Mortensen, K.; Nilsson, M.; Slim, K.; Schäfer, M.; Mariette, C.; Braga, M.; Carli, F.; Demartines, N.; Griffin, S.M.; Lassen, K.; et al. Consensus guidelines for enhanced recovery after gastrectomy. Br. J. Surg. 2014, 101, 1209–1229. [Google Scholar] [CrossRef] [PubMed]
- Thorell, A.; MacCormick, A.D.; Awad, S.; Reynolds, N.; Roulin, D.; Demartines, N.; Vignaud, M.; Alvarez, A.; Singh, P.M.; Lobo, D.N. Guidelines for Perioperative Care in Bariatric Surgery: Enhanced Recovery after Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2065–2083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melloul, E.; Hübner, M.; Scott, M.; Snowden, C.; Prentis, J.; Dejong, C.H.C.; Garden, O.J.; Farges, O.; Kokudo, N.; Vauthey, J.-N.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery after Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2425–2440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temple-Oberle, C.; Shea-Budgell, M.A.; Tan, M.; Semple, J.L.; Schrag, C.; Barreto, M.; Blondeel, P.; Hamming, J.; Dayan, J.; Ljungqvist, O.; et al. Consensus Review of Optimal Perioperative Care in Breast Reconstruction: Enhanced Recovery after Surgery (ERAS) Society Recommendations. Plast. Reconstr. Surg. 2017, 139, 1056e–1071e. [Google Scholar] [CrossRef] [PubMed]
- Hübner, M.; Kusamura, S.; Villeneuve, L.; Al-Niaimi, A.; Alyami, M.; Balonov, K.; Bell, J.; Bristow, R.; Guiral, D.C.; Fagotti, A.; et al. Guidelines for Perioperative Care in Cytoreductive Surgery (CRS) with or without hyperthermic IntraPEritoneal chemotherapy (HIPEC): Enhanced Recovery after Surgery (ERAS®) Society Recommendations—Part II: Postoperative management and special considerations. Eur. J. Surg. Oncol. 2020, 46, 2311–2323. [Google Scholar] [CrossRef] [PubMed]
- Melloul, E.; Lassen, K.; Roulin, D.; Grass, F.; Perinel, J.; Adham, M.; Wellge, E.B.; Kunzler, F.; Besselink, M.G.; Asbun, H.; et al. Guidelines for Perioperative Care for Pancreatoduodenectomy: Enhanced Recovery after Surgery (ERAS) Recommendations 2019. World J. Surg. 2020, 44, 2056–2084. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.D.; Caughey, A.B.; Wood, S.L.; Macones, G.A.; Wrench, I.J.; Huang, J.; Norman, M.; Pettersson, K.; Fawcett, W.J.; Shalabi, M.M.; et al. Guidelines for Antenatal and Preoperative care in Cesarean Delivery: Enhanced Recovery after Surgery Society Recommendations (Part 1). Am. J. Obstet. Gynecol. 2018, 219, 523.e1–523.e15. [Google Scholar] [CrossRef] [PubMed]
- Caughey, A.B.; Wood, S.L.; Macones, G.A.; Wrench, I.J.; Huang, J.; Norman, M.; Pettersson, K.; Fawcett, W.J.; Shalabi, M.M.; Metcalfe, A.; et al. Guidelines for intraoperative care in cesarean delivery: Enhanced Recovery after Surgery Society Recommendations (Part 2). Am. J. Obstet. Gynecol. 2018, 219, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelman, D.T.; Ali, W.B.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery after Surgery Society Recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, T.W.; Gill, M.; McDonald, D.A.; Middleton, R.G.; Reed, M.; Sahota, O.; Yates, P.; Ljungqvist, O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery after Surgery (ERAS®) Society recommendations. Acta Orthop. 2020, 91, 3–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debono, B.; Wainwright, T.W.; Wang, M.Y.; Sigmundsson, F.G.; Yang, M.M.H.; Smid-Nanninga, H.; Bonnal, A.; Le Huec, J.-C.; Fawcett, W.J.; Ljungqvist, O.; et al. Consensus statement for perioperative care in lumbar spinal fusion: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Spine J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G.; Bakkum-Gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; Lasala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery after Surgery (ERAS) Society recommendations-2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for Perioperative Care in Elective Colorectal Surgery: Enhanced Recovery after Surgery (ERAS®) Society Recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, D.E.; Allum, W.; De Manzoni, G.; Ferri, L.; Immanuel, A.; Kuppusamy, M.; Law, S.; Lindblad, M.; Maynard, N.; Neal, J.; et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery after Surgery (ERAS®) Society Recommendations. World J. Surg. 2019, 43, 299–330. [Google Scholar] [CrossRef] [PubMed]
- Dort, J.C.; Farwell, D.G.; Findlay, M.; Huber, G.F.; Kerr, P.; Shea-Budgell, M.A.; Simon, C.; Uppington, J.; Zygun, D.; Ljungqvist, O.; et al. Optimal Perioperative Care in Major Head and Neck Cancer Surgery with Free Flap Reconstruction: A Consensus Review and Recommendations From the Enhanced Recovery after Surgery Society. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 292–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nygren, J.; Thacker, J.; Carli, F.; Fearon, K.C.H.; Norderval, S.; Lobo, D.N.; Ljungqvist, O.; Soop, M.; Ramirez, J. Enhanced Recovery after Surgery Society Guidelines for perioperative care in elective rectal/pelvic surgery: Enhanced Recovery after Surgery (ERAS®) Society recommendations. Clin. Nutr. 2012, 31, 801–816. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, U.O.; Scott, M.J.; Schwenk, W.; Demartines, N.; Roulin, D.; Francis, N.; McNaught, C.E.; MacFie, J.; Liberman, A.S.; Soop, M.; et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery after Surgery (ERAS®) Society recommendations. Clin. Nutr. 2012, 31, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Lassen, K.; Coolsen, M.M.E.; Slim, K.; Carli, F.; de Aguilar-Nascimento, J.E.; Schäfer, M.; Parks, R.W.; Fearon, K.C.H.; Lobo, D.N.; Demartines, N.; et al. Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced Recovery after Surgery (ERAS®) Society recommendations. Clin. Nutr. 2012, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Cerantola, Y.; Valerio, M.; Persson, B.; Jichlinski, P.; Ljungqvist, O.; Hubner, M.; Kassouf, W.; Muller, S.; Baldini, G.; Carli, F.; et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: Enhanced Recovery after Surgery (ERAS(®)) society recommendations. Clin. Nutr. 2013, 32, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Feldheiser, A.; Aziz, O.; Baldini, G.; Cox, B.P.B.W.; Fearon, K.C.H.; Feldman, L.S.; Gan, T.J.; Kennedy, R.H.; Ljungqvist, O.; Lobo, D.N.; et al. Enhanced Recovery after Surgery (ERAS) for gastrointestinal surgery, part 2: Consensus statement for anaesthesia practice. Acta Anaesthesiol. Scand. 2016, 60, 289–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, M.J.; Baldini, G.; Fearon, K.C.H.; Feldheiser, A.; Feldman, L.S.; Gan, T.J.; Ljungqvist, O.; Lobo, D.N.; Rockall, T.A.; Schricker, T.; et al. Enhanced Recovery after Surgery (ERAS) for gastrointestinal surgery, part 1: Pathophysiological considerations. Acta Anaesthesiol. Scand. 2015, 59, 1212–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, G.; Altman, A.D.; Nick, A.; Meyer, L.A.; Ramirez, P.T.; Achtari, C.; Antrobus, J.; Huang, J.; Scott, M.; Wijk, L.; et al. Guidelines for pre- and intra-operative care in gynecologic/oncology surgery: Enhanced Recovery after Surgery (ERAS®) Society recommendations—Part I. Gynecol. Oncol. 2016, 140, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kranke, P.; Redel, A.; Schuster, F.; Muellenbach, R.; Eberhart, L.H. Pharmacological interventions and concepts of fast-track perioperative medical care for enhanced recovery programs. Expert Opin. Pharmacother. 2008, 9, 1541–1564. [Google Scholar] [CrossRef] [PubMed]
- White, P.F.; Kehlet, H.; Neal, J.M.; Schricker, T.; Carr, D.B.; Carli, F. Fast-Track Surgery Study Group The role of the anesthesiologist in fast-track surgery: From multimodal analgesia to perioperative medical care. Anesth. Analg. 2007, 104, 1380–1396. [Google Scholar] [CrossRef] [PubMed]
- Yost, M.T.; Jolissaint, J.S.; Fields, A.C.; Fisichella, P.M. Enhanced Recovery Pathways for Minimally Invasive Esophageal Surgery. J. Laparoendosc. Adv. Surg. Tech. A 2018, 28, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Pache, B.; Hübner, M.; Jurt, J.; Demartines, N.; Grass, F. Minimally invasive surgery and enhanced recovery after surgery: The ideal combination? J. Surg. Oncol. 2017, 116, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.M.; Keller, D.S.; Delaney, C.P. Successful Implementation of an Enhanced Recovery Pathway: The Nurse’s Role. AORN J. 2015, 102, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Boden, I.; Skinner, E.H.; Browning, L.; Reeve, J.; Anderson, L.; Hill, C.; Robertson, I.K.; Story, D.; Denehy, L. Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: Pragmatic, double blinded, multicentre randomised controlled trial. BMJ 2018, 360, j5916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Yan, C.; Li, J.; Wang, Q.; Zhang, J.; Qiang, W.; Qi, D. A nurse-driven enhanced recovery after surgery (ERAS) nursing program for geriatric patients following lung surgery. Thorac. Cancer 2020, 11, 1105–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlug, M.S.; Wind, J.; Hollmann, M.W.; Ubbink, D.T.; Cense, H.A.; Engel, A.F.; Gerhards, M.F.; van Wagensveld, B.A.; van der Zaag, E.S.; van Geloven, A.A.W.; et al. Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: A randomized clinical trial (LAFA-study). Ann. Surg. 2011, 254, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Esteban, F.; Cerdan, F.J.; Garcia-Alonso, M.; Sanz-Lopez, R.; Arroyo, A.; Ramirez, J.M.; Moreno, C.; Morales, R.; Navarro, A.; Fuentes, M. A multicentre comparison of a fast track or conventional postoperative protocol following laparoscopic or open elective surgery for colorectal cancer surgery. Colorectal Dis. 2014, 16, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Pedrazzani, C.; Conti, C.; Mantovani, G.; Fernandes, E.; Turri, G.; Lazzarini, E.; Menestrina, N.; Ruzzenente, A.; Guglielmi, A. Laparoscopic colorectal surgery and Enhanced Recovery after Surgery (ERAS) program: Experience with 200 cases from a single Italian center. Medicine 2018, 97, e12137. [Google Scholar] [CrossRef] [PubMed]
- Gresham, L.M.; Sadiq, M.; Gresham, G.; McGrath, M.; Lacelle, K.; Szeto, M.; Trickett, J.; Schramm, D.; Pearsall, E.; McKenzie, M.; et al. Evaluation of the effectiveness of an enhanced recovery after surgery program using data from the National Surgical Quality Improvement Program. CJS 2019, 62, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Berian, J.R.; Ban, K.A.; Liu, J.B.; Sullivan, C.L.; Ko, C.Y.; Thacker, J.K.M.; Feldman, L.S. Association of an Enhanced Recovery Pilot with Length of Stay in the National Surgical Quality Improvement Program. JAMA Surg. 2018, 153, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banning, L.B.D.; Ter Beek, L.; El Moumni, M.; Visser, L.; Zeebregts, C.J.; Jager-Wittenaar, H.; Pol, R.A. Vascular Surgery Patients at Risk for Malnutrition Are at an Increased Risk of Developing Postoperative Complications. Ann. Vasc. Surg. 2020, 64, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, J.M.; Boissonneault, A.R.; Schwartz, A.M.; Staley, C.A.; Schenker, M.L. Frailty and Malnutrition Are Associated with Inpatient Postoperative Complications and Mortality in Hip Fracture Patients. J. Orthop. Trauma 2019, 33, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Ryan, E.; McNicholas, D.; Creavin, B.; Kelly, M.E.; Walsh, T.; Beddy, D. Sarcopenia and Inflammatory Bowel Disease: A Systematic Review. Inflamm. Bowel Dis. 2019, 25, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Bisch, S.; Nelson, G.; Altman, A. Impact of Nutrition on Enhanced Recovery after Surgery (ERAS) in Gynecologic Oncology. Nutrients 2019, 11, 1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Silva, F.R.M.; de Oliveira, M.G.O.A.; Souza, A.S.R.; Figueroa, J.N.; Santos, C.S. Factors associated with malnutrition in hospitalized cancer patients: A croos-sectional study. Nutr. J. 2015, 14, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pressoir, M.; Desné, S.; Berchery, D.; Rossignol, G.; Poiree, B.; Meslier, M.; Traversier, S.; Vittot, M.; Simon, M.; Gekiere, J.P.; et al. Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br. J. Cancer 2010, 102, 966–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tweed, T.; van Eijden, Y.; Tegels, J.; Brenkman, H.; Ruurda, J.; van Hillegersberg, R.; Sosef, M.; Stoot, J. Safety and efficacy of early oral feeding for enhanced recovery following gastrectomy for gastric cancer: A systematic review. Surg. Oncol. 2019, 28, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Berkelmans, G.H.K.; Fransen, L.F.C.; Dolmans-Zwartjes, A.C.P.; Kouwenhoven, E.A.; van Det, M.J.; Nilsson, M.; Nieuwenhuijzen, G.A.P.; Luyer, M.D.P. Direct Oral Feeding Following Minimally Invasive Esophagectomy (NUTRIENT II trial): An International, Multicenter, Open-label Randomized Controlled Trial. Ann. Surg. 2020, 271, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Herbert, G.; Perry, R.; Andersen, H.K.; Atkinson, C.; Penfold, C.; Lewis, S.J.; Ness, A.R.; Thomas, S. Early enteral nutrition within 24 hours of lower gastrointestinal surgery versus later commencement for length of hospital stay and postoperative complications. Cochrane Database Syst. Rev. 2019, 7, CD004080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, J.C.; Bao, X.; Agarwala, A. Pain Management in Enhanced Recovery after Surgery (ERAS) Protocols. Clin. Colon Rectal Surg. 2019, 32, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Engelman, R.M.; Rousou, J.A.; Flack, J.E., III; Deaton, D.W.; Humphrey, C.B.; Ellison, L.H.; Allmendinger, P.D.; Owen, S.G.; Pekow, P.S. Fast-track recovery of the coronary bypass patient. Ann. Thorac. Surg. 1994, 58, 1742–1746. [Google Scholar] [CrossRef]
- Aggarwal, A.; Lewison, G.; Idir, S.; Peters, M.; Aldige, C.; Boerckel, W.; Boyle, P.; Trimble, E.L.; Roe, P.; Sethi, T.; et al. The State of Lung Cancer Research: A Global Analysis. J. Thorac. Oncol. 2016, 11, 1040–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.; Hughes, T.; Lawson, K.; DeSilva, G. Citation analysis of the 100 most common articles regarding distal radius fractures. J. Clin. Orthop. Trauma 2017, 8, 73–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goerlandt, F.; Li, J.; Reniers, G. The Landscape of Risk Communication Research: A Scientometric Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3255. [Google Scholar] [CrossRef] [PubMed]
- Ke, L.; Lu, C.; Shen, R.; Lu, T.; Ma, B.; Hua, Y. Knowledge Mapping of Drug-Induced Liver Injury: A Scientometric Investigation (2010–2019). Front. Pharmacol. 2020, 11, 842. [Google Scholar] [CrossRef] [PubMed]
- Sweileh, W.M.; Al-Jabi, S.W.; AbuTaha, A.S.; Zyoud, S.H.; Anayah, F.M.A.; Sawalha, A.F. Bibliometric analysis of worldwide scientific literature in mobile-health: 2006–2016. BMC Med. Inform. Decis. Mak. 2017, 17, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Annual output between 1994 and 2019.
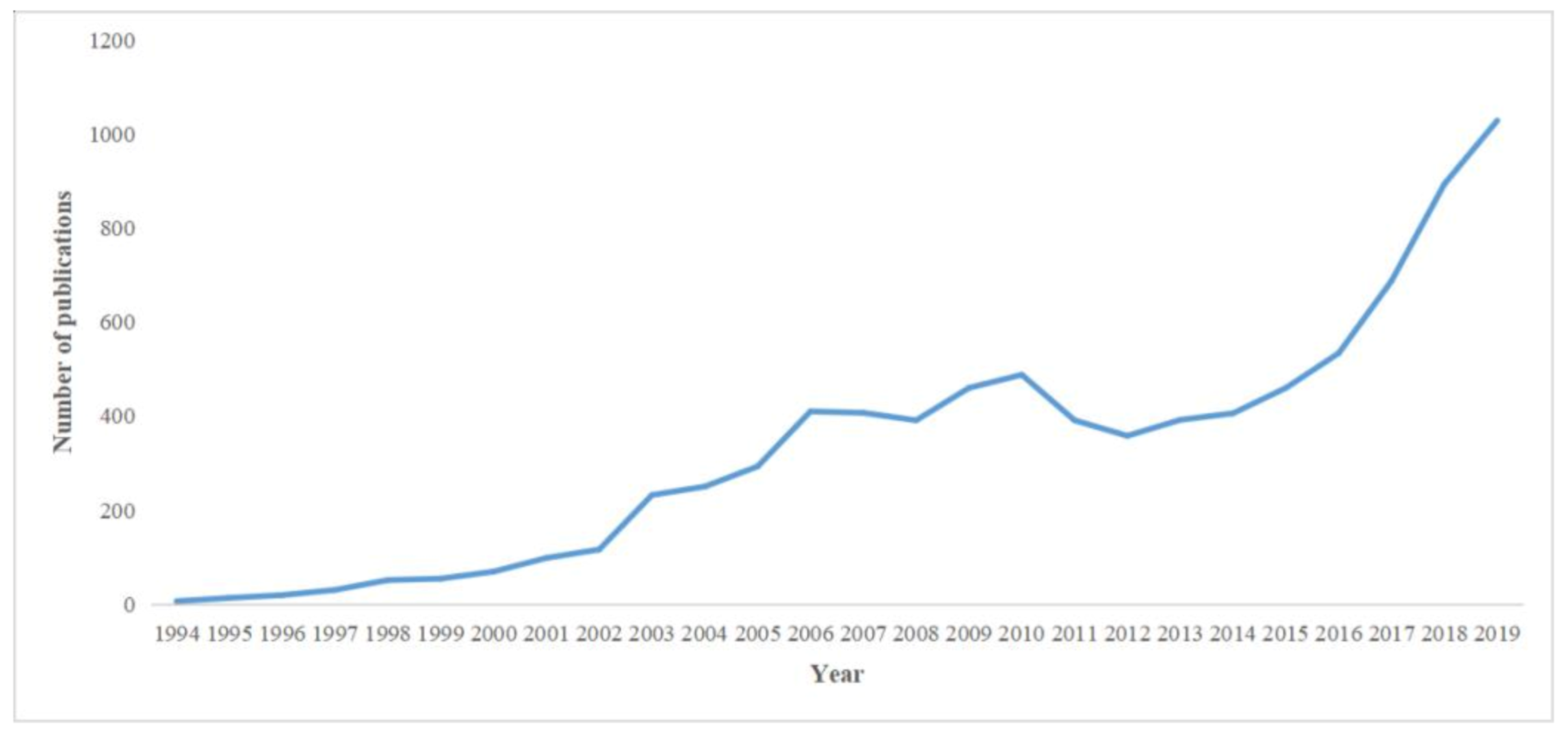
Figure 2.
Global distribution of Enhanced recovery after surgery (ERAS)-relevant studies.
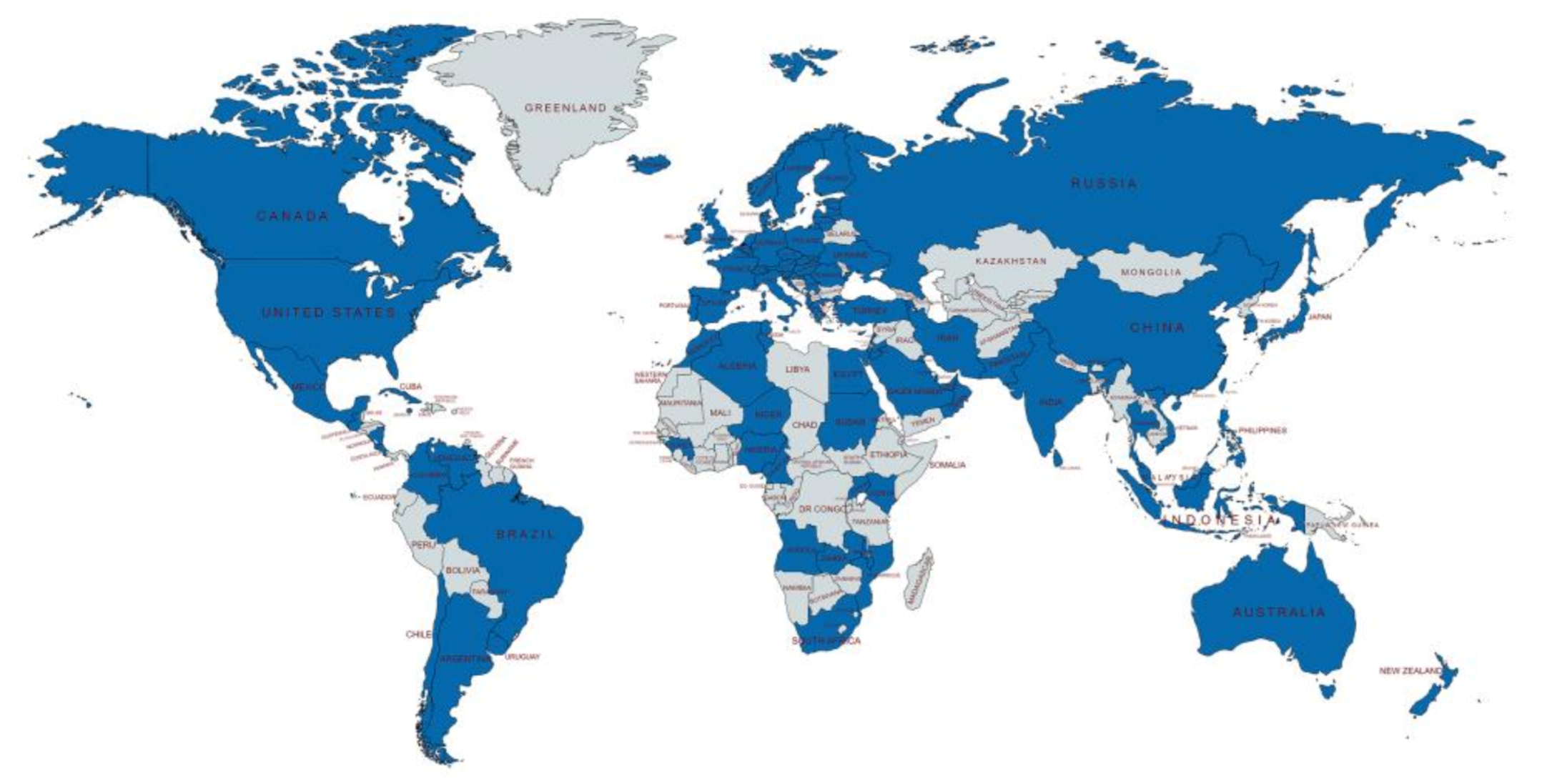
Figure 3.
Top 10 authors’ productions over time.
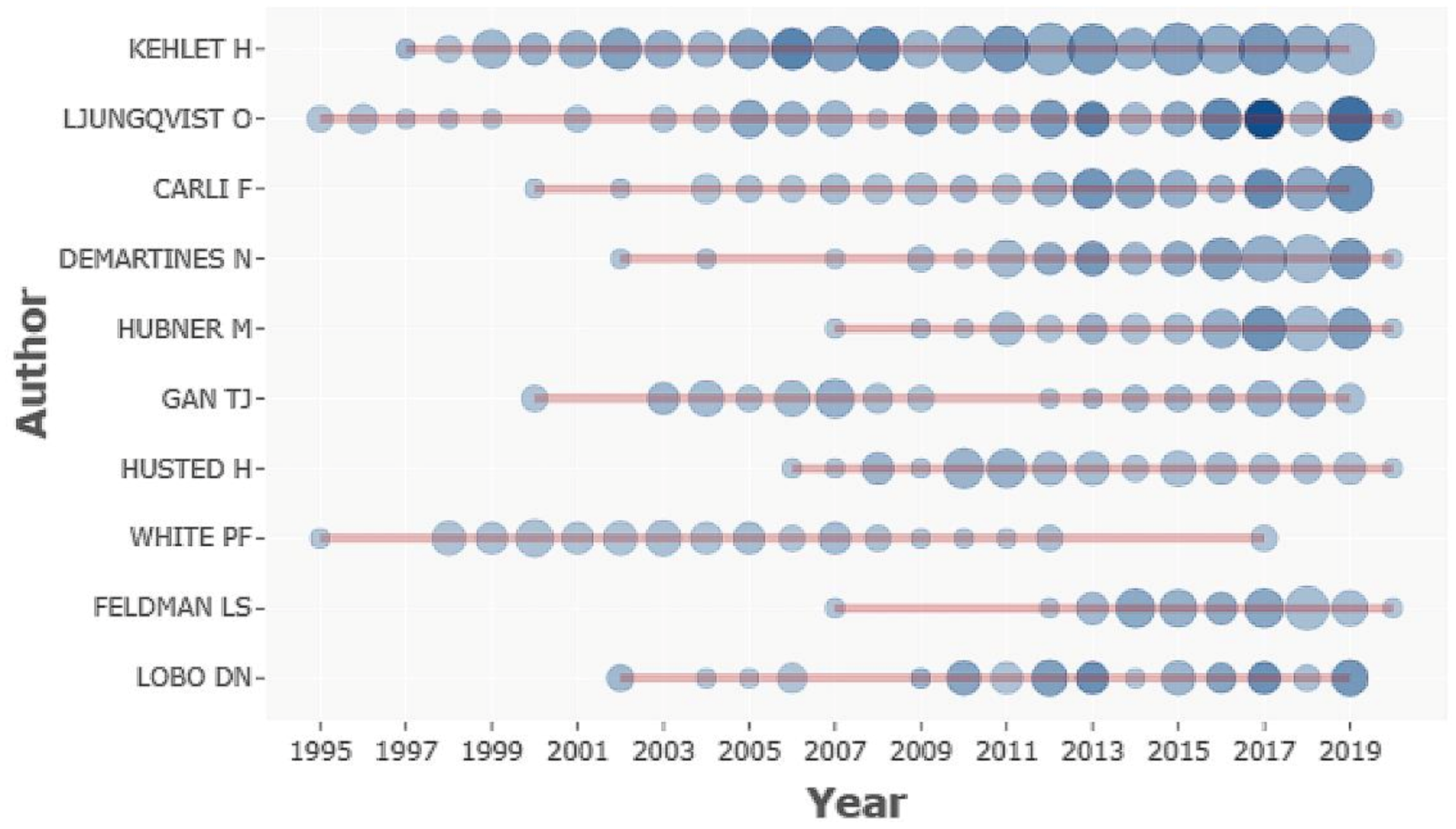
Figure 4.
Year of first publication from the journals.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Language distribution of publications.
| Languages | Records |
|---|---|
| English | 8156 |
| German | 233 |
| French | 71 |
| Spanish | 38 |
| Portuguese | 11 |
| Korean | 6 |
| Turkish | 6 |
| Czech | 3 |
| Romanian | 3 |
| Hungarian | 2 |
| Lithuanian | 2 |
| Serbian | 2 |
| Icelandic | 1 |
| Italian | 1 |
| Japanese | 1 |
| Polish | 1 |
| Russian | 1 |
| Slovene | 1 |
Table 2.
Top 10 largest contributing countries in ERAS.
| Countries | Records | h-Index | Sum of Times Cited | Average Citations per Item |
|---|---|---|---|---|
| US | 2717 | 146 | 107,682 | 39.59 |
| UK | 818 | 101 | 41,177 | 50.22 |
| China | 663 | 51 | 10,431 | 16.15 |
| Germany | 626 | 76 | 25,574 | 40.79 |
| Canada | 599 | 87 | 29,740 | 49.57 |
| Denmark | 477 | 89 | 31,092 | 65.05 |
| Italy | 432 | 65 | 20,225 | 46.71 |
| The Netherlands | 360 | 71 | 21,898 | 60.66 |
| Sweden | 357 | 76 | 21,619 | 60.39 |
| France | 335 | 57 | 12,792 | 38.19 |
Table 3.
Top 31 most frequent collaborating countries.
| From | To | Frequency |
|---|---|---|
| US | Canada | 132 |
| US | UK | 98 |
| US | Germany | 71 |
| UK | Canada | 66 |
| UK | Sweden | 62 |
| UK | Germany | 58 |
| US | China | 57 |
| US | Italy | 57 |
| The Netherlands | UK | 55 |
| US | Switzerland | 53 |
| UK | Italy | 50 |
| Italy | Germany | 49 |
| UK | Switzerland | 47 |
| The Netherlands | Germany | 42 |
| Sweden | Canada | 42 |
| Switzerland | Germany | 41 |
| US | Sweden | 41 |
| UK | Australia | 39 |
| US | The Netherlands | 39 |
| US | Denmark | 37 |
| Switzerland | France | 36 |
| UK | Norway | 36 |
| UK | France | 35 |
| US | France | 34 |
| Sweden | Switzerland | 33 |
| The Netherlands | Italy | 32 |
| US | Australia | 32 |
| Canada | Germany | 31 |
| France | Germany | 31 |
| Italy | Switzerland | 31 |
| UK | Denmark | 31 |
Table 4.
Top 10 authors with the greatest number of publications in ERAS.
| Authors | Articles | Sum of Times Cited | h-Index | Specialized Subject | Institution | Country |
|---|---|---|---|---|---|---|
| Kehlet, H. | 261 | 21,497 | 74 | Surgical Pathophysiology | Copenhagen Univ Hosp | Denmark |
| Ljungqvist, O. | 99 | 11,877 | 52 | Department of Surgery | Orebro University | Sweden |
| Carli, F. | 88 | 5607 | 41 | Department of Anesthesiology | McGill University | Canada |
| Demartines, N. | 81 | 4413 | 27 | Department of Visceral Surgery | Centre Hospitalier Universitaire Vaudois | Switzerland |
| Hubner, M. | 63 | 2346 | 23 | Department of Visceral Surgery | Centre Hospitalier Universitaire Vaudois | Switzerland |
| Gan, T.J. | 57 | 4494 | 33 | Department of Anesthesiology | Stony Brook University | US |
| Husted, H. | 57 | 2717 | 29 | Department of Orthopedic Surgery | Copenhagen Univ Hosp | Denmark |
| White, P.F. | 55 | 2952 | 32 | Department of Anesthesiology | Cedars Sinai Medical Center | US |
| Feldman, L.S. | 52 | 2045 | 23 | Department of Surgery | McGill University | Canada |
| Lobo, D.N. | 48 | 6078 | 30 | Department of Gastrointestinal Surgery | University of Nottingham | UK |
Table 5.
Top 10 journals ranked by the number of publications and impact factor, respectively.
| Source | Journal Impact Factor | Journal Quartile | Number of Publications | Total Citations | h-Index |
|---|---|---|---|---|---|
| Anesthesia and Analgesia | 4.305 | Q1 | 358 | 21,494 | 79 |
| British Journal of Anaesthesia | 6.880 | Q1 | 189 | 14,386 | 65 |
| Acta Anaesthesiologica Scandinavica | 2.050 | Q3 | 147 | 5060 | 40 |
| Surgical Endoscopy | 3.149 | Q1 | 147 | 4213 | 37 |
| Anesthesiology | 7.067 | Q1 | 135 | 12,697 | 65 |
| World Journal of Surgery | 2.234 | Q2 | 128 | 4817 | 36 |
| European Journal of Anaesthesiology | 4.500 | Q1 | 127 | 3564 | 29 |
| Journal of Cardiothoracic and Vascular Anesthesia | 2.258 | Q3 | 125 | 3101 | 31 |
| Annals of Surgery | 10.130 | Q1 | 117 | 11,928 | 59 |
| Colorectal Disease | 2.769 | Q2 | 111 | 3328 | 32 |
| The New England Journal of Medicine | 74.699 | Q1 | 2 | 839 | 2 |
| Lancet | 60.392 | Q1 | 10 | 5118 | 10 |
| The Journal of the American Medical Association | 45.540 | Q1 | 8 | 2637 | 8 |
| Lancet Oncology | 33.752 | Q1 | 2 | 267 | 2 |
| Journal of Clinical Oncology | 32.956 | Q1 | 3 | 289 | 3 |
| British Medical Journal | 30.223 | Q1 | 8 | 1451 | 8 |
| Nature Reviews Gastroenterology and Hepatology | 29.848 | Q1 | 2 | 66 | 2 |
| Lancet Infectious Diseases | 24.446 | Q1 | 1 | 24 | 1 |
| Circulation | 23.603 | Q1 | 7 | 764 | 7 |
| European Heart Journal | 22.673 | Q1 | 3 | 222 | 3 |
Table 6.
Type of surgery and most relevant journals.
| Subject | Articles | Journal Title | Articles | Impact Factor | Journal Quartile |
|---|---|---|---|---|---|
| Gastrointestinal surgery | 2162 | Surgical Endoscopy | 110 | 3.149 | Q1 |
| Orthopedic surgery | 1740 | Journal of Arthroplasty | 85 | 3.709 | Q1 |
| Cardiac surgery | 608 | Journal of Cardiothoracic and Vascular Anesthesia | 99 | 2.258 | Q3 |
| Thoracic surgery | 462 | Journal of Thoracic Disease | 55 | 2.046 | Q3 |
| Head and neck surgery | 438 | Anesthesia and Analgesia | 22 | 4.305 | Q1 |
| Obstetrics and gynecology surgery | 419 | Anesthesia and Analgesia | 40 | 4.305 | Q1 |
| Urologic surgery | 385 | Urology | 35 | 1.924 | Q3 |
| Hepatobiliary surgery | 359 | Surgical Endoscopy | 25 | 3.149 | Q1 |
| Pancreatic surgery | 180 | HPB | 18 | 3.401 | Q1 |
| Breast surgery | 143 | Plastic and Reconstructive Surgery | 22 | 4.209 | Q1 |
| Vascular surgery | 24 | Journal of Vascular Surgery | 3 | 3.405 | Q1 |
Table 7.
Top 5 highest number of citations publication in ERAS.
| First Author | Article Title | Source Title | Times Cited | Publication Year |
|---|---|---|---|---|
| Kehlet, H. | Persistent postsurgical pain: risk factors and prevention | Lancet | 1923 | 2006 |
| Kehlet, H. | Multimodal approach to control postoperative pathophysiology and rehabilitation | British Journal of Anaesthesia | 1121 | 1997 |
| Heran, B.S. | Exercise-based cardiac rehabilitation for coronary heart disease | Cochrane Database of Systematic Reviews | 1105 | 2011 |
| Falck-Ytter, Y. | Prevention of VTE in Orthopedic Surgery Patients Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines | Chest | 970 | 2012 |
| Brandstrup, B. | Effects of intravenous fluid restriction on postoperative complications: Comparison of two perioperative fluid regimens—A randomized assessor-blinded multicenter trial | Annals of Surgery | 970 | 2003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Li, C.; Cheng, Y.; Li, Z.; Margaryan, D.; Perka, C.; Trampuz, A. The Pertinent Literature of Enhanced Recovery after Surgery Programs: A Bibliometric Approach. Medicina 2021, 57, 172. https://doi.org/10.3390/medicina57020172
AMA Style
Li C, Cheng Y, Li Z, Margaryan D, Perka C, Trampuz A. The Pertinent Literature of Enhanced Recovery after Surgery Programs: A Bibliometric Approach. Medicina. 2021; 57(2):172. https://doi.org/10.3390/medicina57020172
Chicago/Turabian StyleLi, Cheng, Yang Cheng, Zhao Li, Donara Margaryan, Carsten Perka, and Andrej Trampuz. 2021. "The Pertinent Literature of Enhanced Recovery after Surgery Programs: A Bibliometric Approach" Medicina 57, no. 2: 172. https://doi.org/10.3390/medicina57020172