
COVID-19 mRNA Vaccine Tolerance and Immunogenicity in Hematopoietic Stem Cell Transplantation Recipients Aged 5–11 Years Old–Non-Randomized Clinical Trial
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recording of Adverse Events
2.2. Immunological Assays
2.3. Statistical Methods
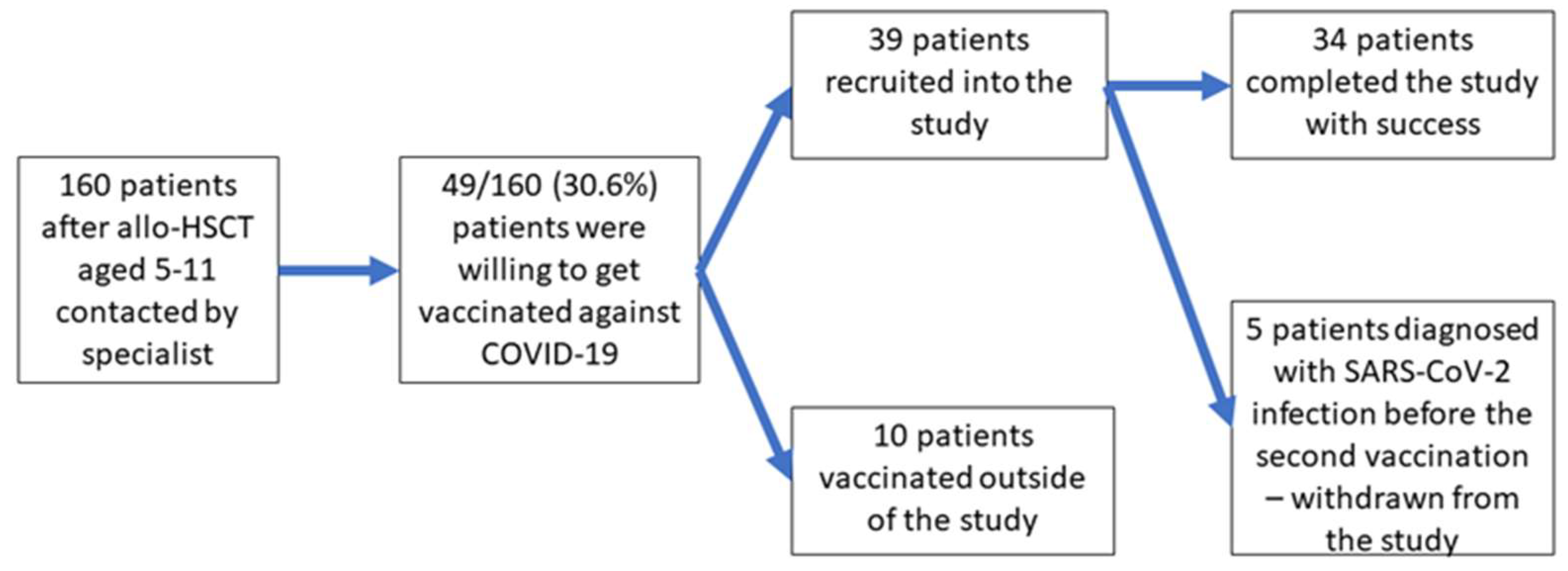
3. Results
4. Discussion
4.1. Immunogenicity of the Two-Dose Vaccine Schedule
4.2. Indications for the Third Vaccine Dose in Allo-HSCT Patients
4.3. Adverse Events after Vaccination
4.4. SARS-CoV-2 Infection after Inclusion in the Study
4.5. Parents’ Willingness to Vaccinate Their Children
4.6. Limitations of the Study
5. Conclusions
- COVID-19 vaccine hesitancy among parents of children after allo-HSCT poses a significant problem that complicates the prevention of SARS-CoV-2 infection in this high-risk group.
- The COVID-19 mRNA BNT162b vaccine is safe and very well tolerated in 5–11-year-old children following allo-HSCT and in healthy children.
- The 5–11-year-old patients who were more than 2 years removed from HSCT and who were not receiving immunosuppressive treatment presented excellent immunity after two doses of the mRNA BNT162b2 vaccine; thus, children in this group should be vaccinated according to the same schedule as the healthy population.
- Some of the 5–11-year-old children after HSCT who fulfill the official criteria for the three-dose primary vaccination schedule might not need the third dose, and anti-SARS-CoV-2 IgG can be incorporated into decision making about the best vaccination schedule for such patients.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, F.; Cattaneo, C.; Arcaini, L.; Bruna, R.; Cavo, M.; Merli, F.; Angelucci, E.; Krampera, M.; Cairoli, R.; Della Porta, M.G.; et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: A retrospective, multicentre, cohort study. Lancet Haematol. 2020, 7, e737–e745. [Google Scholar] [CrossRef] [PubMed]
- Goldman, J.D.; Robinson, P.C.; Uldrick, T.S.; Ljungman, P. COVID-19 in immunocompromised populations: Implications for prognosis and repurposing of immunotherapies. J. Immunother. Cancer 2021, 9, e002630. [Google Scholar] [CrossRef]
- Parker, E.P.K.; Desai, S.; Marti, M.; Nohynek, H.; Kaslow, D.C.; Kochhar, S.; O’Brien, K.L.; Hombach, J.; Wilder-Smith, A. Response to additional COVID-19 vaccine doses in people who are immunocompromised: A rapid review. Lancet Glob. Health 2022, 10, e326–e328. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus (COVID-19) Update: FDA Authorizes Additional Vaccine Dose for Certain Immunocompromised Individuals|FDA. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-vaccine-dose-certain-immunocompromised (accessed on 1 September 2022).
- Comirnaty COVID-19 Vaccine: EMA Recommends Approval for Children Aged 5 to 11|European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/comirnaty-covid-19-vaccine-ema-recommends-approval-children-aged-5-11 (accessed on 1 September 2022).
- Pfizer-BioNTech COVID-19 Vaccine (5 through 11 Years of Age)|CDC. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/index.html (accessed on 1 September 2022).
- Common Terminology Criteria for Adverse Events (CTCAE)|Protocol Development|CTEP. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 20 April 2022).
- Maneikis, K.; Šablauskas, K.; Ringelevičiūtė, U.; Vaitekėnaitė, V.; Čekauskienė, R.; Kryžauskaitė, L.; Naumovas, D.; Banys, V.; Pečeliūnas, V.; Beinortas, T.; et al. Immunogenicity of the BNT162b2 COVID-19 mRNA vaccine and early clinical outcomes in patients with haematological malignancies in Lithuania: A national prospective cohort study. Lancet Haematol. 2021, 8, e583–e592. [Google Scholar] [CrossRef]
- Negahdaripour, M.; Shafiekhani, M.; Moezzi, S.M.I.; Amiri, S.; Rasekh, S.; Bagheri, A.; Mosaddeghi, P.; Vazin, A. Administration of COVID-19 vaccines in immunocompromised patients. Int. Immunopharmacol. 2021, 99, 108021. [Google Scholar] [CrossRef]
- Ali, H.; Ngo, D.; Aribi, A.; Arslan, S.; Dadwal, S.; Marcucci, G.; Nakamura, R.; Forman, S.J.; Chen, J.; Al Malki, M.M. Safety and Tolerability of SARS-CoV2 Emergency-Use Authorized Vaccines for Allogeneic Hematopoietic Stem Cell Transplant Recipients. Transplant. Cell. Ther. 2021, 27, 938.e1. [Google Scholar] [CrossRef]
- Dhakal, B.; Abedin, S.; Fenske, T.; Chhabra, S.; Ledeboer, N.; Hari, P.; Hamadani, M. Response to SARS-CoV-2 vaccination in patients after hematopoietic cell transplantation and CAR T-cell therapy. Blood 2021, 138, 1278–1281. [Google Scholar] [CrossRef] [PubMed]
- Chiarucci, M.; Paolasini, S.; Isidori, A.; Guiducci, B.; Loscocco, F.; Capalbo, M.; Visani, G. Immunological Response against SARS-COV-2 After BNT162b2 Vaccine Administration Is Impaired in Allogeneic but Not in Autologous Stem Cell Transplant Recipients. Front. Oncol. 2021, 11, 3501. [Google Scholar] [CrossRef]
- Matkowska-Kocjan, A.; Owoc-Lempach, J.; Chruszcz, J.; Kuźnik, E.; Szenborn, F.; Jurczenko, L.; Wójcik, M.; Banyś, D.; Szenborn, L.; Ussowicz, M. The COVID-19 mRNA BNT163b2 Vaccine Was Well Tolerated and Highly Immunogenic in Young Adults in Long Follow-Up after Haematopoietic Stem Cell Transplantation. Vaccines 2021, 9, 1209. [Google Scholar] [CrossRef]
- Majcherek, M.; Matkowska-Kocjan, A.; Szymczak, D.; Karasek, M.; Szeremet, A.; Kiraga, A.; Milanowska, A.; Kuznik, E.; Kujawa, K.; Wrobel, T.; et al. Two Doses of BNT162b2 mRNA Vaccine in Patients after Hematopoietic Stem Cell Transplantation: Humoral Response and Serological Conversion Predictors. Cancers 2022, 14, 325. [Google Scholar] [CrossRef]
- Krammer, F. Correlates of protection from SARS-CoV-2 infection. Lancet 2021, 397, 1421–1423. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Perry, J.; Osman, S.; Wright, J.; Richard-Greenblatt, M.; Buchan, S.A.; Sadarangani, M.; Bolotinid, S. Does a humoral correlate of protection exist for SARS-CoV-2? A systematic review. PLoS ONE 2022, 17, e0266852. [Google Scholar] [CrossRef]
- Wei, J.; Pouwels, K.B.; Stoesser, N.; Matthews, P.C.; Diamond, I.; Studley, R.; Rourke, E.; Cook, D.; Bell, J.I.; Newton, J.N.; et al. Antibody responses and correlates of protection in the general population after two doses of the ChAdOx1 or BNT162b2 vaccines. Nat. Med. 2022, 28, 1072–1082. [Google Scholar] [CrossRef]
- Goldblatt, D.; Fiore-Gartland, A.; Johnson, M.; Hunt, A.; Bengt, C.; Zavadska, D.; Snipe, H.D.; Brown, J.S.; Workman, L.; Zar, H.J.; et al. Towards a population-based threshold of protection for COVID-19 vaccines. Vaccine 2022, 40, 306–315. [Google Scholar] [CrossRef]
- Dimeglio, C.; Herin, F.; Martin-Blondel, G.; Miedougé, M.; Izopet, J. Antibody titers and protection against a SARS-CoV-2 infection. J. Infect. 2022, 84, 248. [Google Scholar] [CrossRef]
- Prevention of SARS-CoV-2|COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/prevention-of-sars-cov-2/ (accessed on 1 April 2022).
- Duni, A.; Markopoulos, G.S.; Mallioras, I.; Pappas, H.; Pappas, E.; Koutlas, V.; Tzalavra, E.; Baxevanos, G.; Priska, S.; Gartzonika, K.; et al. The Humoral Immune Response to BNT162b2 Vaccine Is Associated With Circulating CD19+ B Lymphocytes and the Naïve CD45RA to Memory CD45RO CD4+ T Helper Cells Ratio in Hemodialysis Patients and Kidney Transplant Recipients. Front. Immunol. 2021, 12, 760249. [Google Scholar] [CrossRef]
- Nelli, F.; Fabbri, A.; Panichi, V.; Giannarelli, D.; Topini, G.; Giron Berrios, J.R.; Virtuoso, A.; Marrucci, E.; Mazzotta, M.; Schirripa, M.; et al. Peripheral lymphocyte subset counts predict antibody response after SARS-CoV-2 mRNA-BNT162b2 vaccine in cancer patients: Results from the Vax-On-Profile study. Int. Immunopharmacol. 2022, 108, 108774. [Google Scholar] [CrossRef]
- DiPiazza, A.T.; Graham, B.S.; Ruckwardt, T.J. T cell immunity to SARS-CoV-2 following natural infection and vaccination. Biochem. Biophys. Res. Commun. 2021, 538, 211–217. [Google Scholar] [CrossRef]
- Oyaert, M.; De Scheerder, M.-A.; Van Herrewege, S.; Laureys, G.; Van Assche, S.; Cambron, M.; Naesens, L.; Hoste, L.; Claes, K.; Haerynck, F.; et al. Evaluation of Humoral and Cellular Responses in SARS-CoV-2 mRNA Vaccinated Immunocompromised Patients. Front. Immunol. 2022, 13, 1151. [Google Scholar] [CrossRef]
- Bacova, B.; Kohutova, Z.; Zubata, I.; Gaherova, L.; Kucera, P.; Heizer, T.; Mikesova, M.; Karel, T.; Novak, J. Cellular and humoral immune response to SARS-CoV-2 mRNA vaccines in patients treated with either Ibrutinib or Rituximab. Clin. Exp. Med. 2022. [Google Scholar] [CrossRef]
- Mamez, A.C.; Pradier, A.; Giannotti, F.; Petitpas, A.; Urdiola, M.F.; Vu, D.L.; Masouridi-Levrat, S.; Morin, S.; Dantin, C.; Clerc-Renaud, D.; et al. Antibody responses to SARS-CoV2 vaccination in allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 2021, 56, 3094–3096. [Google Scholar] [CrossRef]
- Maillard, A.; Redjoul, R.; Klemencie, M.; Labussière Wallet, H.; Le Bourgeois, A.; D’Aveni, M.; Huynh, A.; Berceanu, A.; Marchand, T.; Chantepie, S.; et al. Antibody response after 2 and 3 doses of SARS-CoV-2 mRNA vaccine in allogeneic hematopoietic cell transplant recipients. Blood 2022, 139, 134. [Google Scholar] [CrossRef]
- Redjoul, R.; Le Bouter, A.; Beckerich, F.; Fourati, S.; Maury, S. Antibody response after second BNT162b2 dose in allogeneic HSCT recipients. Lancet 2021, 398, 298–299. [Google Scholar] [CrossRef]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef]
- Gao, P.; Cai, S.; Liu, Q.; Du, M.; Liu, J.; Liu, M. Effectiveness and Safety of SARS-CoV-2 Vaccines among Children and Adolescents: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 421. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Pfizer-BioNTech COVID-19 Vaccine Reactions & Adverse Events | CDC. Available online: https://www.cdc.gov/vaccines/covid-19/info-by-product/pfizer/reactogenicity.html (accessed on 1 September 2022).
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Chen, F.; He, Y.; Shi, Y. Parents’ and Guardians’ Willingness to Vaccinate Their Children against COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 179. [Google Scholar] [CrossRef]
- Giudice, G.M.D.; Napoli, A.; Corea, F.; Folcarelli, L.; Angelillo, I.F. Evaluating COVID-19 Vaccine Willingness and Hesitancy among Parents of Children Aged 5–11 Years with Chronic Conditions in Italy. Vaccines 2022, 10, 396. [Google Scholar] [CrossRef]
- Skeens, M.; Guttoo, P.; Stanek, J.R.; Taylor, K.; Stratz, E.; Ardura, M.I.; Rangarajan, H.G. An Exploration of COVID-19 Impact and Vaccine Hesitancy in Parents of Pediatric Hematopoietic Stem Cell Transplant (HCT) Recipients. Bone Marrow Transplant. 2022, 57, 547–553. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HSCT Group | Control Group |
|---|---|---|
| Sex | male 28, female 6 | male 17, female 18 |
| Age | 5–11 years (median 7) | 5–11 years (median 7) |
| Diagnosis | severe aplastic anemia-10 acute lymphoblastic leukemia-6 juvenile myelomonycytic leukemia-4 acute myeloblastic leukemia-2 Wiskott–Aldrich syndrome-2 lymphoma-2 chronic myeloid leukemia-1 hemophagocytic syndrome-1 severe combined immunodeficiency-1 adrenoleukodystrophy-1 Diamond–Blackfan anemia-1 X-linked agammaglobulinemia-1 mucopolysaccharidosis-1 | n/a |
| Time from allo-HSCT | 5–120 months (median 36) | n/a |
| Symptoms of cGvHD at vaccination | present in 9 patients | n/a |
| Immunosupressive treatment at vaccination | 9 patients receiving immunosuppressive treatment | n/a |
| Parameter | HSCT Group | Control Group | p Value |
|---|---|---|---|
| The number of patients with positive anti-SARS-CoV-2 IgG detected before vaccination | 23/34 | 25/35 | p = ns |
| The number of patients with anti-SARS-CoV-2 IgG detected after the second dose of the vaccine | 34/34 | 35/35 | p = ns |
| Anti-SARS-CoV-2 IgG concentration before one dose of the vaccine | 0.1–1448 BAU/mL (median 75.4 BAU/mL) | 0–1247 BAU/mL (median 81) | p = ns |
| Anti-SARS-CoV-2 IgG concentration after two doses of the vaccine | 11.5–>5680 BAU/mL (median 3596) | 1481–>5680 BAU/mL (median 3868) | p = ns |
| The number of patients who declared SARS-CoV-2 infection before the vaccination | 8/34 | 10/35 | p = ns |
| Value | SARS-CoV-2 Ab before Vaccination | SARS-CoV-2 Ab after 2nd Dose | ||
|---|---|---|---|---|
| Spearman r | p Value | Spearman r | p Value | |
| T CD4+ lymphocytes (CD3 + 4+ cells/µL) | 0.0092 | 0.96 | 0.1917 | 0.29 |
| T CD8+ lymphocytes (CD3 + 8+ cells/µL) | −0.1274 | 0.48 | −0.0035 | 0.98 |
| NK cells (CD56+ cells/µL) | −0.0114 | 0.95 | 0.1387 | 0.44 |
| B lymphocytes (CD19+ cells/µL) | 0.3288 | 0.06 | 0.2236 | 0.21 |
| IgG g/dL | −0.0836 | 0.64 | 0.1622 | 0.37 |
| The Reason Why the Patients Fulfilled the Criteria for the 3rd Dose of the Vaccine | Less than 2 Years from HSCT | Still Receiving Immunosuppressive Treatment | Both Criteria Fulfilled |
| 12/15 | 9/15 | 5/15 | |
| Anti-SARS-CoV-2 IgG concentration before the vaccination | 1–1448 BAU/mL (3 patients negative, 12 patients >7 BAU/mL; median 66.8 BAU/mL) | ||
| Anti-SARS-CoV-2 IgG concentration after the 2nd dose of the vaccine | 11.5–>5680 BAU/mL (median 5574 BAU/mL) | ||
| 7–999 BAU/mL | 1000–4999 BAU/mL | >5000 BAU/mL | |
| 7 patients | 0 patients | 8 patients | |
| Anti-SARS-CoV-2 IgG after the 3rd dose of the vaccine | 158–5680 BAU/mL (median 1240) | n/a | The 3rd vaccine dose was not given in the primary schedule due to excellent immunologic response to the 2nd dose |
| Symptom | HSCT Patients Presenting the Symptom after the 1st Dose of the Vaccine (n = 34) | CONTROL Patients Presenting the Symptom after the 1st Dose of the Vaccine (n = 35) | HSCT Duration of the Symptom–Days after Vaccination–Median (Range) | CONTROL Duration of the Symptom–Days after Vaccination–Median (Range) | HSCT Patients Presenting the Symptom after the 2nd Dose of the Vaccine (n = 34) | CONTROL Patients Presenting the Symptom after the 2nd Dose of the Vaccine (n = 35) | HSCT Duration of the Symptom–Days after Vaccination–Median (Range) | CONTROL Duration of the Symptom–Days after Vaccination–Median (Range) | HSCT Patients in Whom the Symptom Was Present after both Doses (n = 34) | CONTROL Patients in Whom the Symptom Was Present After both Doses (n = 35) |
|---|---|---|---|---|---|---|---|---|---|---|
| Temp. 37.2–37.9 C | 3 (8.8%) | 1 (2.8%) | 3 (1–4) | 1 (1) | 0 | 2 (5.7%) | - | 3 (2–3) | 1 (2.9%) | 0 |
| Temp. 38.0–38.4 C | 0 | 0 | - | - | 0 | 1 (2.8%) | - | (3) | - | - |
| Fatigue | 0 | 0 | - | - | 0 | 0 | - | - | - | - |
| Headache | 1 | 3 (8.5%) | (4) | 2 (1–4) | 2 (5.9%) | 5 (14.2%) | (1–3) | 2 (2–3) | 1 (2.9%) | 0 |
| Chills | 0 | 0 | - | - | 2 (5.9%) | 3 (8.5%) | (1–3) | 2 (1–3) | - | - |
| New or worsening muscle pain | 2 (5.9%) | 0 | (2–4) | - | 0 | 1 (2.8%) | - | (2) | - | - |
| New or worsening joint pain | 0 | 0 | - | - | 0 | 0 | - | - | - | - |
| Vomiting/nausea | 0 | 0 | - | - | 1 (2.9%) | 0 | On 5th day | - | - | - |
| Pain at injection site | 6 (17.6%) | 7 (20.0%) | 3 (1–4) | 2 (1–4) | 6 (17.6%) | 13 (37.1%) | 2 (1–2) | 2 (1–5) | 2 (5.9%) | 4 (11.4%) |
| Swelling at the injection site | 0 | 0 | - | - | 0 | 3 (8.5%) | - | 5 (3–5) | - | - |
| Induration at the injection site | 0 | 0 | - | - | 0 | 3 (8.5%) | - | 5 (3–5) | - | - |
| Redness at the injection site | 0 | 2 (5.7%) | - | (2–4) | 1 (2.9%) | 3 (8.5%) | (2) | 3 (2–3) | 0 | 0 |
| Pruritus at the injection site | 0 | 0 | - | - | 0 | 1 (2.8%) | - | (3) | - | |
| Axillary lymphadenopathy | 0 | 0 | - | - | 0 | 0 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matkowska-Kocjan, A.; Owoc-Lempach, J.; Ludwikowska, K.; Szenborn, F.; Moskwa, N.; Kurek, K.; Kałwak, K.; Szenborn, L.; Ussowicz, M. COVID-19 mRNA Vaccine Tolerance and Immunogenicity in Hematopoietic Stem Cell Transplantation Recipients Aged 5–11 Years Old–Non-Randomized Clinical Trial. Vaccines 2023, 11, 195. https://doi.org/10.3390/vaccines11010195
Matkowska-Kocjan A, Owoc-Lempach J, Ludwikowska K, Szenborn F, Moskwa N, Kurek K, Kałwak K, Szenborn L, Ussowicz M. COVID-19 mRNA Vaccine Tolerance and Immunogenicity in Hematopoietic Stem Cell Transplantation Recipients Aged 5–11 Years Old–Non-Randomized Clinical Trial. Vaccines. 2023; 11(1):195. https://doi.org/10.3390/vaccines11010195
Chicago/Turabian StyleMatkowska-Kocjan, Agnieszka, Joanna Owoc-Lempach, Kamila Ludwikowska, Filip Szenborn, Natalia Moskwa, Katarzyna Kurek, Krzysztof Kałwak, Leszek Szenborn, and Marek Ussowicz. 2023. "COVID-19 mRNA Vaccine Tolerance and Immunogenicity in Hematopoietic Stem Cell Transplantation Recipients Aged 5–11 Years Old–Non-Randomized Clinical Trial" Vaccines 11, no. 1: 195. https://doi.org/10.3390/vaccines11010195
APA StyleMatkowska-Kocjan, A., Owoc-Lempach, J., Ludwikowska, K., Szenborn, F., Moskwa, N., Kurek, K., Kałwak, K., Szenborn, L., & Ussowicz, M. (2023). COVID-19 mRNA Vaccine Tolerance and Immunogenicity in Hematopoietic Stem Cell Transplantation Recipients Aged 5–11 Years Old–Non-Randomized Clinical Trial. Vaccines, 11(1), 195. https://doi.org/10.3390/vaccines11010195