
Vaccine Hesitancy and Anti-Vaccination Attitudes during the Start of COVID-19 Vaccination Program: A Content Analysis on Twitter Data


Abstract
:1. Introduction
2. Materials and Methods
3. Results
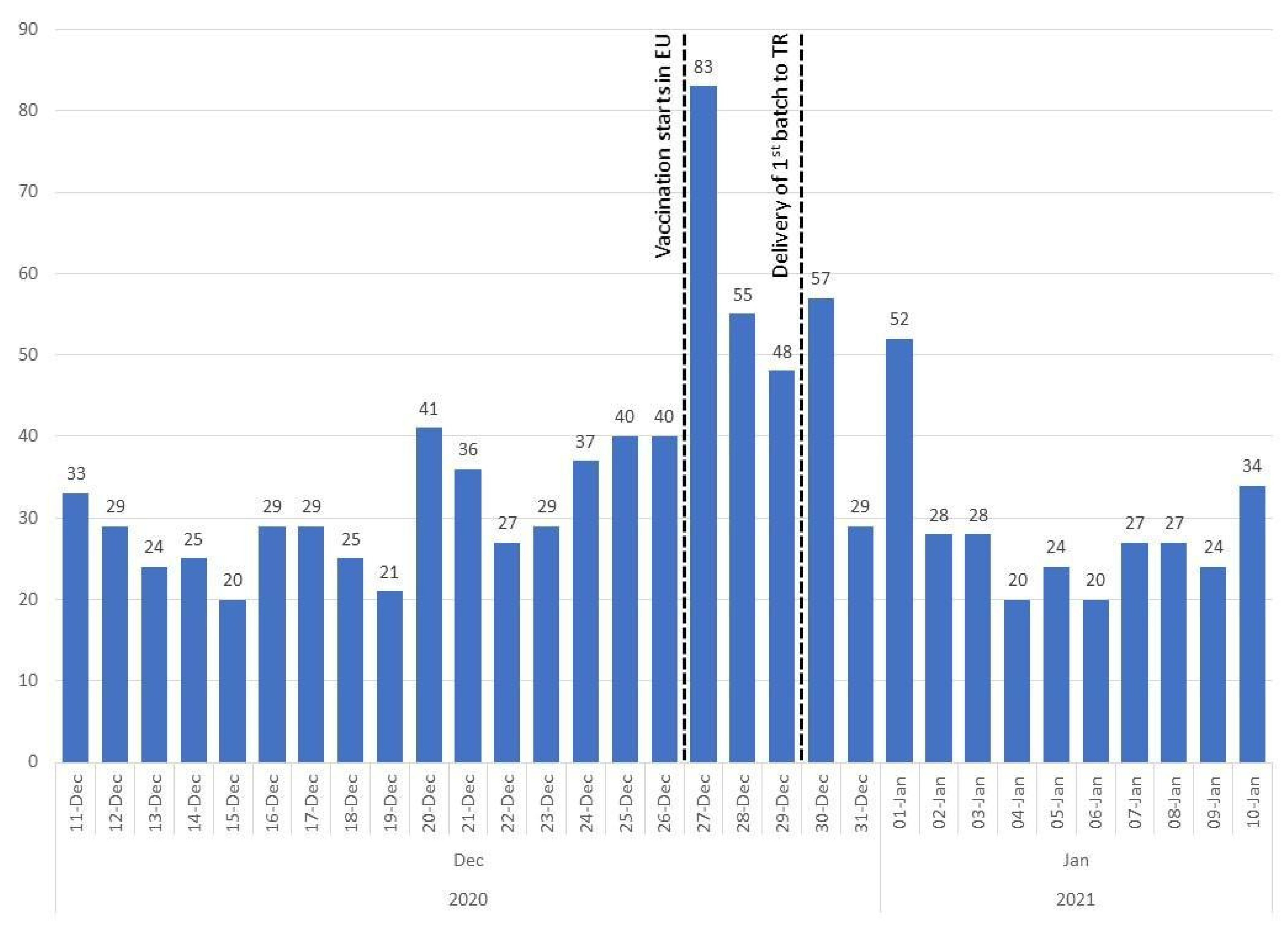
3.1. Descriptive Statistics
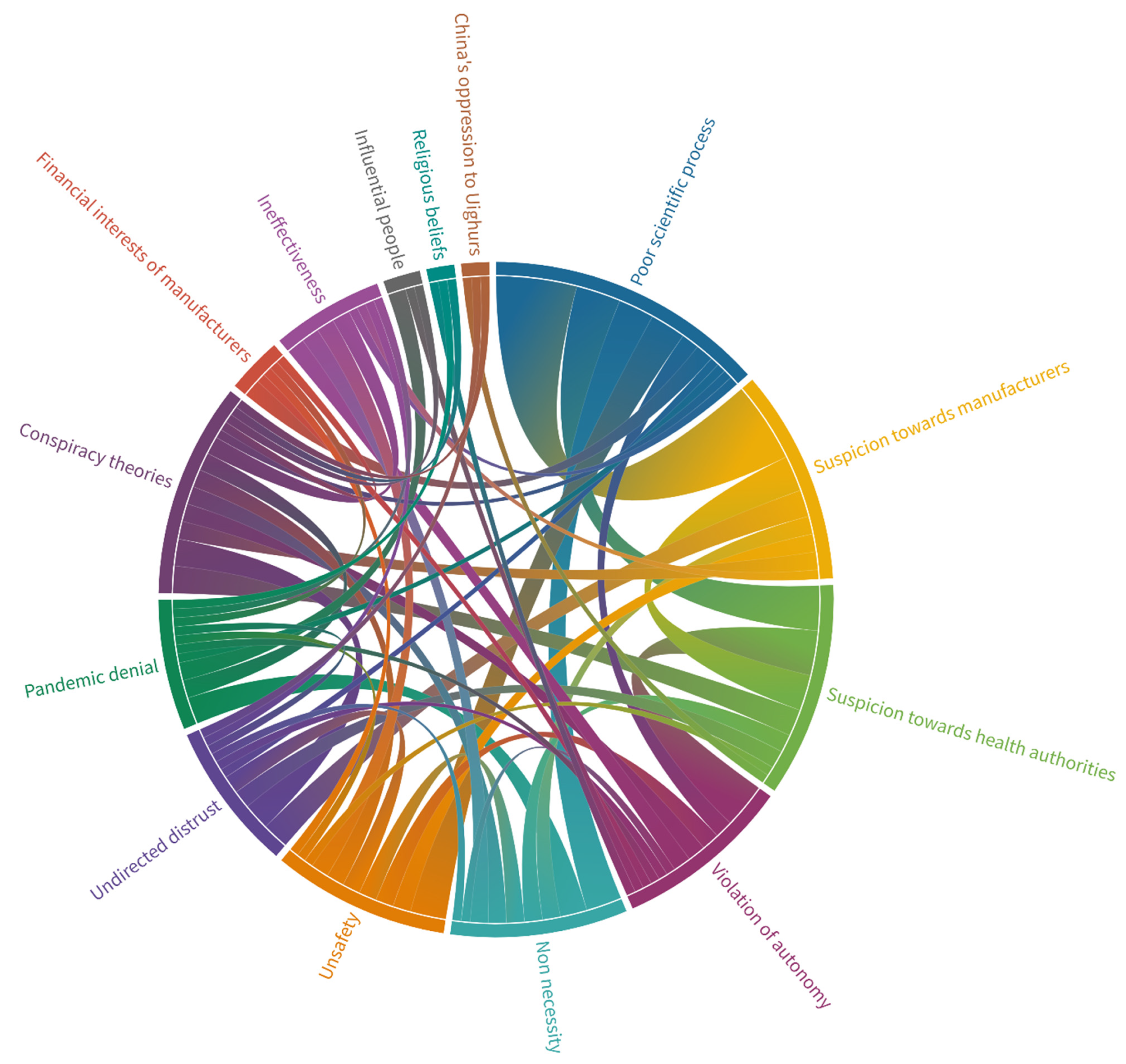
3.2. Emerging Themes
3.2.1. Poor Scientific Process
Example 1: Why do we get the vaccine that even [nation name] government does not use it for its own people? We are not experimental subjects.
Example 2: The only way to end the pandemic is to get vaccinated. However, no scientific evidence has been presented regarding the efficacy and the safety of the current vaccines. Without safety, no vaccine should be given to large populations.
3.2.2. Conspiracy Theories
Example 1: Do you really believe all of these? They all tell you what globalists order them. First, it was supposed to end in 2021 summer, but now we are in 2021 winter, and they already extend it for the next ten years. I think it will end in 2071! My final call. What about those saying that vaccine is the light at the end of the tunnel? Vaccines are useless apparently.
Example 2: This is only the beginning. If we ain’t gonna stop all these today, their next steps might be even more dangerous. Don’t you get that the real matter is not COVID, vaccine, 5G, nor mask!
3.2.3. Suspicion towards Manufacturers
Example 1: While [nation name] gets the vaccines from [another nation name] for its citizens, they sell us their illegal vaccine that does not even complete phase 3.
Example 2: Today, I’ve heard rumors about, “[company name] and [nation name] vaccines are produced with active and passive viruses, respectively. And those who’ve gotten the [company name] are miserable right now.” I don’t know about their accuracy and I could not see any news about them. But, as I said, it’s all getting chaotic because they do not have any kind of safety mechanism.
3.2.4. Suspicion towards Health Authorities
Example 1: [scientist name] [company name] [vaccine brand] etc. You can show the dirty past of all vaccine producers and medical companies. You can countin all the doctors and their institutions as well. And all the governments that took side… Media, don’t be afraid. #GLOBALDECEPTION
Example 2: Dear minister, we don’t believe in you anymore. You’ve ruined the lives of all people and artisans. They are all #GLOBALDECEPTION We all are sick of your lies and do not trust in your vaccines. And, we are not gonna get any of them. [URL]
3.2.5. Undirected Distrust
Example 1: Lies about pandemic and institutions that fuel the fear among society… COVID might be a game or more of a trailer for a bigger game. Even the vaccination is a huge mystery.
Example 2: It should be all followed to see where this mutation stuff will be related to. I feel like it’s gonna be a reason for the mandatory vaccination instead of the second wave. Almost all of the vaccination companies have already stated that the vaccines are effective even when the virus has mutated.
3.2.6. Violation of Autonomy
Example 1: It is not obligated yet we are not happy with this vaccination imposition. #CitizensAreTheState
Example 2: So they all are gonna make debates through my body about the mandatory vaccination, but I am gonna shut up, not look it up and come into the line like a sheep. Is that so?
3.2.7. Unsafety
Example 1: Nobody knows the side effects of that vaccine on me. I prefer not having a vaccine that may harm or kill me, just for the sake of protecting others. And we all have a right to do this, do you get that? The vaccine or the experiment that’s gonna happen to me, I’ll make the call for that. What do you expect?
Example 2: If the vaccine will result in malformed births for the next generations. I am pretty sure it will be. (There are tons of examples for the malformed births in Africa and India because of the mRNA vaccines). In order to avoid its damages, the unvaccinated generation should not marry with the vaccinated generation. You can’t see the extent of its damages.
3.2.8. Non-Necessity
Example 1: Did you even end the flu with vaccine? You cannot vaccinate a virus that’s mutated. All we need is to have a strong immune system. That’s it.
Example 2: We do not wanna get vaccination or something like that. Does anybody hear our voice??? I’ve survived from corona at home without any medicine. My relative that had a hard time during their recoveries also survived from it at thome. The half of my country people have survived it. I don’t wanna get a vaccination for something that I’ve already gotten the immunity for.
3.2.9. Ineffectiveness
Example 1: I think the vaccination is not the way to end the disease. Whats’ important is that we need to develop medicines that can lead people to survive from this disease easily. The flu vaccinations are not%100 protective and they’re never gonna be. Everybody gets caught a flu and gets well with a medicine. That’s the only solution that we should focus.
Example 2: Does the COVID-19 vaccine not working well? A doctor who got the vaccine 6 days ago just caught the corona virus again.
3.2.10. Influential People
Example 1: [Controversial celebrity name] praised the [nation name] vaccine and said that those who discredit it create negative perception. I hope you understand why we should question this vaccine.
Example 2: Don’t fool yourself, none of them have gotten the vaccine because there is no such a thing as COVID. You don’t wanna get this. Do you really think that they all get the vaccine?
3.2.11. Pandemic Denial
Example 1: Although it might be a regular vaccine, there is no need for it because there is no such a disease. But, how are you really gonna believe whether those people in the media saying that they got vaccinated? Also, its effects should last 4–5 years at least.
Example 2: Look at these photos that were just taken. Also in Wuhan… Look, how China is messing with you al. Even there is a virus for those tribe countries that have almost no people living in them, China with 2 billion people is joking with the world. No vaccine, no treatment, yet we are done with virus, they says. WAKE UP PEOPLE THERE IS NO VIRUS
3.2.12. Financial Interests of Manufacturers
Example 1: Those people used to say that vaccines will be free but now trying to make profit out of them. They’ll even get taxes.
Example 2: They all are really trying to make profit out of it. At the beginning, they all said that vaccines will be free, and now there are rumors saying that one dose will be 10 dollars.
3.2.13. China’s Oppression of Uighurs
Example 1: Things have done to our Uighur Turkish brothers are never ending. Also, we are contributing to the Chinese economy by taking the vaccination from them although the Chinese government is the responsible for all pressures and tortures. These vaccinations are betrayal to our Uighurian brothers #UighursCannotBeRepatriated
Example 2: Let’s stop all the fuss and I am not gonna get a vaccine or not even let them into my apartment who gathers Uighurians into more than 500 different camps under the so-called a training program
3.2.14. Religious Beliefs
Example 1: We are not against the vaccine. We are against the vaccines that contain haram stuff. We wanna get halal drug and halal vaccine. #Vaccine #Drug #Halal #Local #National
Example 2: How’s it gonna be permissable both for them and for muslims? Whats the difference if we all gonna get that piggy foetus mRNA vaccine that gonna change our genetic codes? But, see the Pope does not even wear a mask. But of course it should be an exception because mask is a symbol of slavery and not gonna work out for them.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 20 May 2021).
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 7 May 2021).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.D.; Paterson, P. Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G.; Wyatt, J. Using the Internet for Surveys and Health Research. J. Med. Internet Res. 2002, 4, e13. [Google Scholar] [CrossRef] [PubMed]
- Sinnenberg, L.; Buttenheim, A.M.; Padrez, K.; Mancheno, C.; Ungar, L.; Merchant, R.M. Twitter as a Tool for Health Research: A Systematic Review. Am. J. Public Health 2017, 107, e1–e8. [Google Scholar] [CrossRef]
- Shoup, J.A.; Narwaney, K.J.; Wagner, N.M.; Kraus, C.R.; Gleason, K.S.; Albright, K.; Glanz, J.M. Social Media Vaccine Websites: A Comparative Analysis of Public and Moderated Websites. Health Educ. Behav. 2019, 46, 454–462. [Google Scholar] [CrossRef]
- Piedrahita-Valdés, H.; Piedrahita-Castillo, D.; Bermejo-Higuera, J.; Guillem-Saiz, P.; Bermejo-Higuera, J.R.; Guillem-Saiz, J.; Sicilia-Montalvo, J.A.; Machío-Regidor, F. Vaccine Hesitancy on Social Media: Sentiment Analysis from June 2011 to April 2019. Vaccines 2021, 9, 28. [Google Scholar] [CrossRef]
- Ortiz-Sánchez, E.; Velando-Soriano, A.; Pradas-Hernández, L.; Vargas-Román, K.; Gómez-Urquiza, J.L.; La Fuente, G.A.C.-D.; Albendín-García, L. Analysis of the Anti-Vaccine Movement in Social Networks: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5394. [Google Scholar] [CrossRef]
- Bonnevie, E.; Goldbarg, J.; Gallegos-Jeffrey, A.K.; Rosenberg, S.D.; Wartella, E.; Smyser, J. Content Themes and Influential Voices within Vaccine Opposition on Twitter, 2019. Am. J. Public Health 2020, 110, S326–S330. [Google Scholar] [CrossRef]
- Başara, B.B.; Çağlar, İ.S.; Aygün, A.; Kulali, B. The Ministry of Health of Turkey Health Statistics Yearbook 2019; General Directorate of Health Information Systems, Ministry of Health: Ankara, Turkey, 2021; pp. 81–84. [Google Scholar]
- Akar, B.; Akar, N. Vaccine hesitancy in turkey. J. Paediatr. Child Health 2020, 56, 180. [Google Scholar] [CrossRef]
- Filiz, M.; Kaya, M. Systematic review of studies to determine factors affecting vaccine rejection/instability/contrast. Turk. Res. J. Acad. Soc. Sci. 2019, 2, 1–7. [Google Scholar]
- Tılıç, L.D.; Özcan, H.U. An analysis on the anti-vaccination movement in Turkish digital platforms: Ekşisözlük and Facebook. Eskişehir Türk Dünyası Uygul. Araştırma Merk. Halk Sağlığı Derg. 2021, 6, 1–10. [Google Scholar]
- Uzun, S.U.; Mut, A.N.U. Youtube’daki Aşılarla İlgili Türkçe Videolar Neler Söylüyor? Bir İçerik Analizi. In Proceedings of the 3. International 21, National Public Health Congress, Antalya, Turkey, 26–30 November 2019. [Google Scholar]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Digital 2021: Turkey. Available online: https://datareportal.com/reports/digital-2021-turkey (accessed on 2 November 2021).
- Standard v1.1. Available online: https://developer.twitter.com/en/docs/twitter-api/v1 (accessed on 12 December 2020).
- Francis, J.J.; Johnston, M.; Robertson, C.; Glidewell, L.; Entwistle, V.; Eccles, M.P.; Grimshaw, J.M. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol. Health 2010, 25, 1229–1245. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; Namey, E.; Chen, M. A simple method to assess and report thematic saturation in qualitative research. PLoS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.D.; Johnson, K.S.; Myles, L.; Herndon, L.; Montoya, A.; Fashaw, S.; Gifford, D. Lessons learned from frontline skilled nursing facility staff regarding COVID-19 vaccine hesitancy. J. Am. Geriatr. Soc. 2021, 69, 1140–1146. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Salali, G.D.; Uysal, M.S. COVID-19 vaccine hesitancy is associated with beliefs on the origin of the novel coronavirus in the UK and Turkey. Psychol. Med. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Nuzhath, T.; Tasnim, S.; Sanjwal, R.K.; Trisha, N.F.; Rahman, M.; Mahmud, S.M.F.; Arman, A.; Chakraborty, S.; Hossain, M.M. COVID-19 vaccination hesitancy, misinformation and conspiracy theories on social media: A content analysis of Twitter data. SocArXiv 2020. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Rapid Literature Review on Motivating Hesitant Population Groups in Europe to Vaccinate; ECDC Technical Report; European Centre for Disease Prevention and Control: Stockholm, Sweden, October 2015. [Google Scholar]
- Griffith, J.; Marani, H.; Monkman, H. COVID-19 Vaccine Hesitancy in Canada: Content Analysis of Tweets Using the Theoretical Domains Framework. J. Med. Internet Res. 2021, 23, e26874. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- Jeffrey, D.I. Relational ethical approaches to the COVID-19 pandemic. J. Med. Ethics 2020, 46, 495–498. [Google Scholar] [CrossRef] [PubMed]
- TRT Haber. Diyanet: Salgında Aşı Yaptırmamak Kul Hakkına Girer. Available online: https://www.trthaber.com/haber/koronavirus/diyanet-salginda-asi-yaptirmamak-kul-hakkina-girer-584487.html (accessed on 2 November 2021).
- Kilic, M.; Ocal, N.U.; Uslukilic, G. The relationship of COVID-19 vaccine attitude with life satisfaction, religious attitude and COVID-19 avoidance in Turkey. Hum. Vaccines Immunother. 2021, 17, 3384–3393. [Google Scholar] [CrossRef] [PubMed]
- Germani, F.; Biller-Andorno, N. The anti-vaccination infodemic on social media: A behavioral analysis. PLoS ONE 2021, 16, e0247642. [Google Scholar] [CrossRef] [PubMed]
- Republic of Turkey Ministry of Health. COVID-19 Vaccination Information Platform. Available online: https://covid19asi.saglik.gov.tr/?_Dil=2 (accessed on 2 November 2021).
- Ullah, I.; Khan, K.S.; Tahir, M.J.; Ahmed, A.; Harapan, H. Myths and conspiracy theories on vaccines and COVID-19: Potential effect on global vaccine refusals. Vacunas 2021, 22, 93–97. [Google Scholar] [CrossRef]
- Hyland, P.; Vallières, F.; Shevlin, M.; Bentall, R.P.; McKay, R.; Hartman, T.K.; McBride, O.; Murphy, J. Resistance to COVID-19 vaccination has increased in Ireland and the United Kingdom during the pandemic. Public Health 2021, 195, 54–56. [Google Scholar] [CrossRef]
- Cristea, D.; Ilie, D.-G.; Constantinescu, C.; Fîrțală, V. Vaccinating against COVID-19: The Correlation between Pro-Vaccination Attitudes and the Belief That Our Peers Want to Get Vaccinated. Vaccines 2021, 9, 1366. [Google Scholar] [CrossRef]
- Lutkenhaus, R.O.; Jansz, J.; Bouman, M.P.A. Mapping the Dutch vaccination debate on Twitter: Identifying communities, narratives, and interactions. Vaccine X 2019, 1, 100019. [Google Scholar] [CrossRef]
- Silva, C.J.; Cruz, C.; Torres, D.F.M.; Muñuzuri, A.P.; Carballosa, A.; Area, I.; Nieto, J.J.; Fonseca-Pinto, R.; Passadouro, R.; dos Santos, E.S.; et al. Optimal control of the COVID-19 pandemic: Controlled sanitary deconfinement in Portugal. Sci. Rep. 2021, 11, 3451. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Verification status | ||
| Not verified | 973 | 97.3 |
| Verified | 27 | 2.7 |
| User type | ||
| Personal or others | 887 | 88.7 |
| Organizational | 113 | 11.3 |
| Total | 1000 | 100.0 |
| Median (IQR) | ||
| Duration of Twitter use (year) | 4.0 (1.0–8.0) | |
| Number of followers | 276.5 (55.0–603.8) | |
| Number of tweets published | 3163.5 (1561.5–13,951.0) | |
| n | % | |
|---|---|---|
| Presence of a visual | ||
| Yes | 116 | 11.1 |
| No | 925 | 88.9 |
| Presence of an URL | ||
| Yes | 219 | 21.0 |
| No | 822 | 79.0 |
| Presence of a hashtag | ||
| Yes | 123 | 11.8 |
| No | 918 | 88.2 |
| Relevancy with the vaccine | ||
| Irrelevant | 99 | 9.5 |
| Relevant | 942 | 90.5 |
| Total | 1041 | 100.0 |
| Median (IQR) | ||
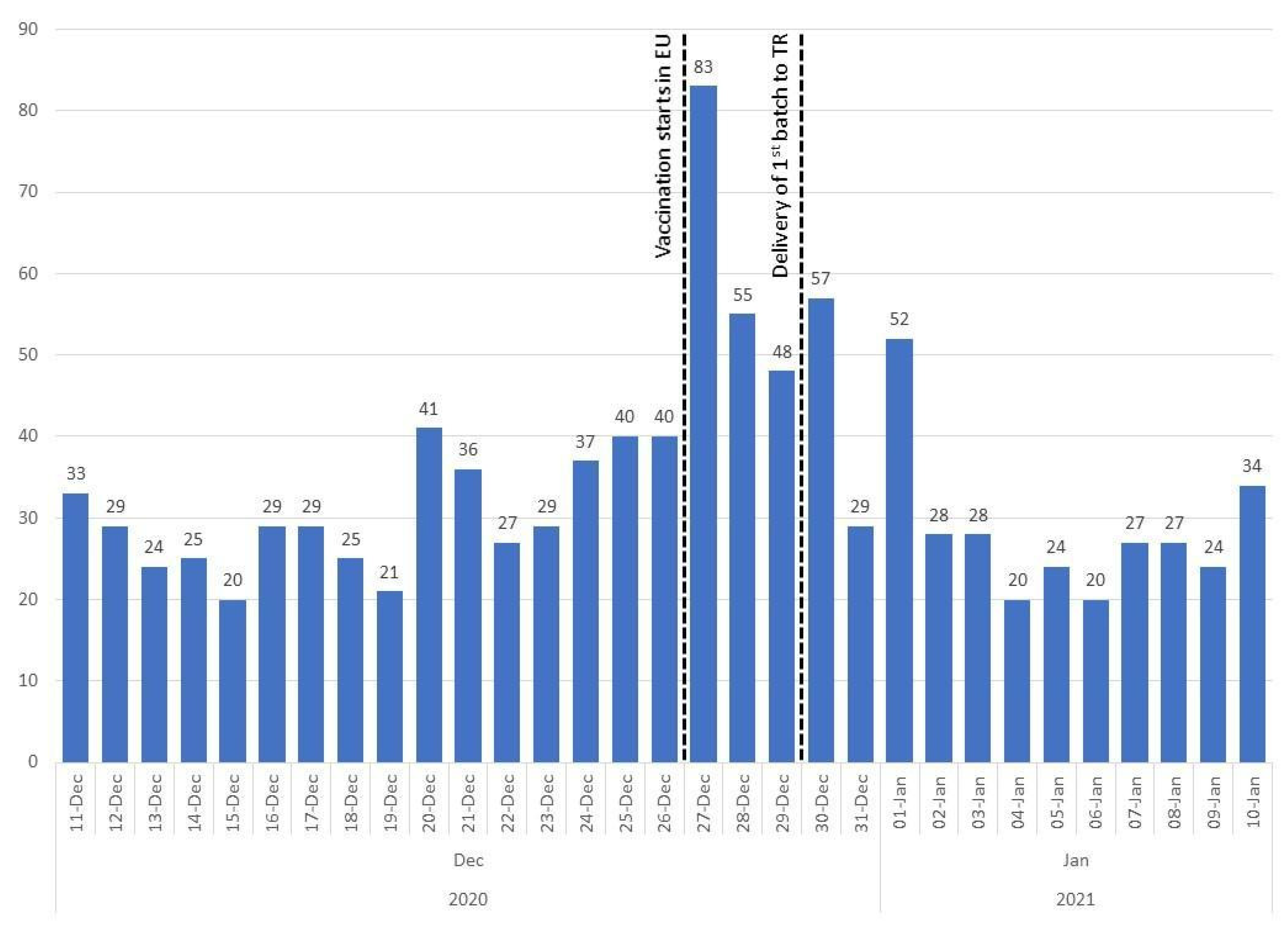
| Number of tweets per day | ||
| Before arrival of vaccines (11 Dec–29 Dec) | 29.0 (25.0–40.0) | |
| After arrival of vaccines (30 Dec–10 Jan) | 27.0 (24.0–29.0) | |
| Total | 29.0 (24.5–38.5) | |
| Contents | n | % |
|---|---|---|
| Vaccine names | ||
| Name of a COVID-19 vaccine | 213 | 22.6 |
| Name of other vaccines * | 25 | 2.7 |
| No vaccine name | 705 | 74.8 |
| Total | 942 | 100.0 |
| Anti-vaccination themes | ||
| Present in tweets | 207 | 22.0 |
| Not present in tweets | 735 | 78.0 |
| Total | 942 | 100.0 |
| Names of the Vaccines | n * | % |
|---|---|---|
| CoronaVac mentions | 109 | 51.2 |
| Chinese vaccine | 90 | 42.3 |
| Sinovac | 19 | 8.9 |
| CoronaVac | 4 | 1.9 |
| Comirnaty mentions | 57 | 26.7 |
| Pfizer-Biontech | 54 | 25.4 |
| German vaccine | 5 | 2.3 |
| Comirnaty | 1 | 0.5 |
| Moderna mentions | 14 | 6.6 |
| Moderna | 12 | 5.6 |
| American vaccine | 4 | 1.9 |
| National (Turkish) vaccine mentions | 12 | 5.6 |
| mRNA vaccine mentions | 8 | 3.8 |
| AstraZeneca mentions | 7 | 3.3 |
| Oxford | 4 | 1.9 |
| AstraZeneca | 3 | 1.4 |
| Sputnik V mentions | 5 | 2.3 |
| Russian vaccine | 4 | 1.9 |
| Sputnik V | 1 | 0.5 |
| Other COVID-19 vaccine mentions | 14 | 6.6 |
| Total | 213 | 100.0 |
| Themes | n | % |
|---|---|---|
| Poor scientific process | 45 | 21.7 |
| Conspiracy theories | 34 | 16.4 |
| Suspicion towards manufacturers | 32 | 15.5 |
| Suspicion towards health authorities | 27 | 13.0 |
| Undirected distrust | 26 | 12.6 |
| Violation of autonomy | 25 | 12.1 |
| Unsafety | 23 | 11.1 |
| Non necessity | 21 | 10.1 |
| Ineffectiveness | 17 | 8.2 |
| Influential people | 14 | 6.8 |
| Pandemic denial | 11 | 5.3 |
| Financial interests of manufacturers | 9 | 4.3 |
| China’s oppression of Uighurs | 8 | 3.9 |
| Religious beliefs | 3 | 1.4 |
| Total * | 207 | 100.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Küçükali, H.; Ataç, Ö.; Palteki, A.S.; Tokaç, A.Z.; Hayran, O. Vaccine Hesitancy and Anti-Vaccination Attitudes during the Start of COVID-19 Vaccination Program: A Content Analysis on Twitter Data. Vaccines 2022, 10, 161. https://doi.org/10.3390/vaccines10020161
Küçükali H, Ataç Ö, Palteki AS, Tokaç AZ, Hayran O. Vaccine Hesitancy and Anti-Vaccination Attitudes during the Start of COVID-19 Vaccination Program: A Content Analysis on Twitter Data. Vaccines. 2022; 10(2):161. https://doi.org/10.3390/vaccines10020161
Chicago/Turabian StyleKüçükali, Hüseyin, Ömer Ataç, Ayşe Seval Palteki, Ayşe Zülal Tokaç, and Osman Hayran. 2022. "Vaccine Hesitancy and Anti-Vaccination Attitudes during the Start of COVID-19 Vaccination Program: A Content Analysis on Twitter Data" Vaccines 10, no. 2: 161. https://doi.org/10.3390/vaccines10020161
APA StyleKüçükali, H., Ataç, Ö., Palteki, A. S., Tokaç, A. Z., & Hayran, O. (2022). Vaccine Hesitancy and Anti-Vaccination Attitudes during the Start of COVID-19 Vaccination Program: A Content Analysis on Twitter Data. Vaccines, 10(2), 161. https://doi.org/10.3390/vaccines10020161