
Training Physicians in Motivational Communication to Address Influenza Vaccine Hesitation: A Proof-of-Concept Study

 , and
, and 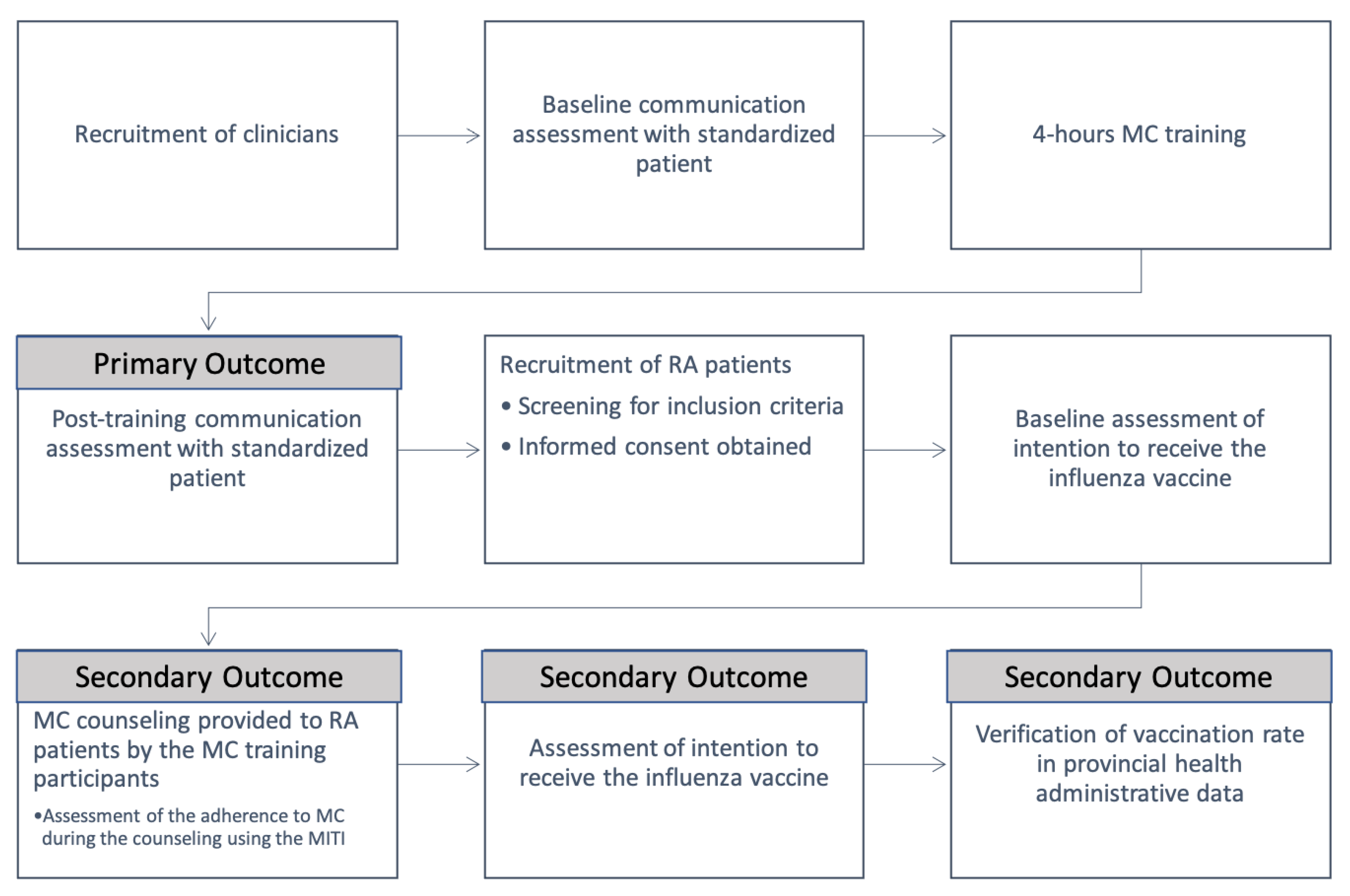{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
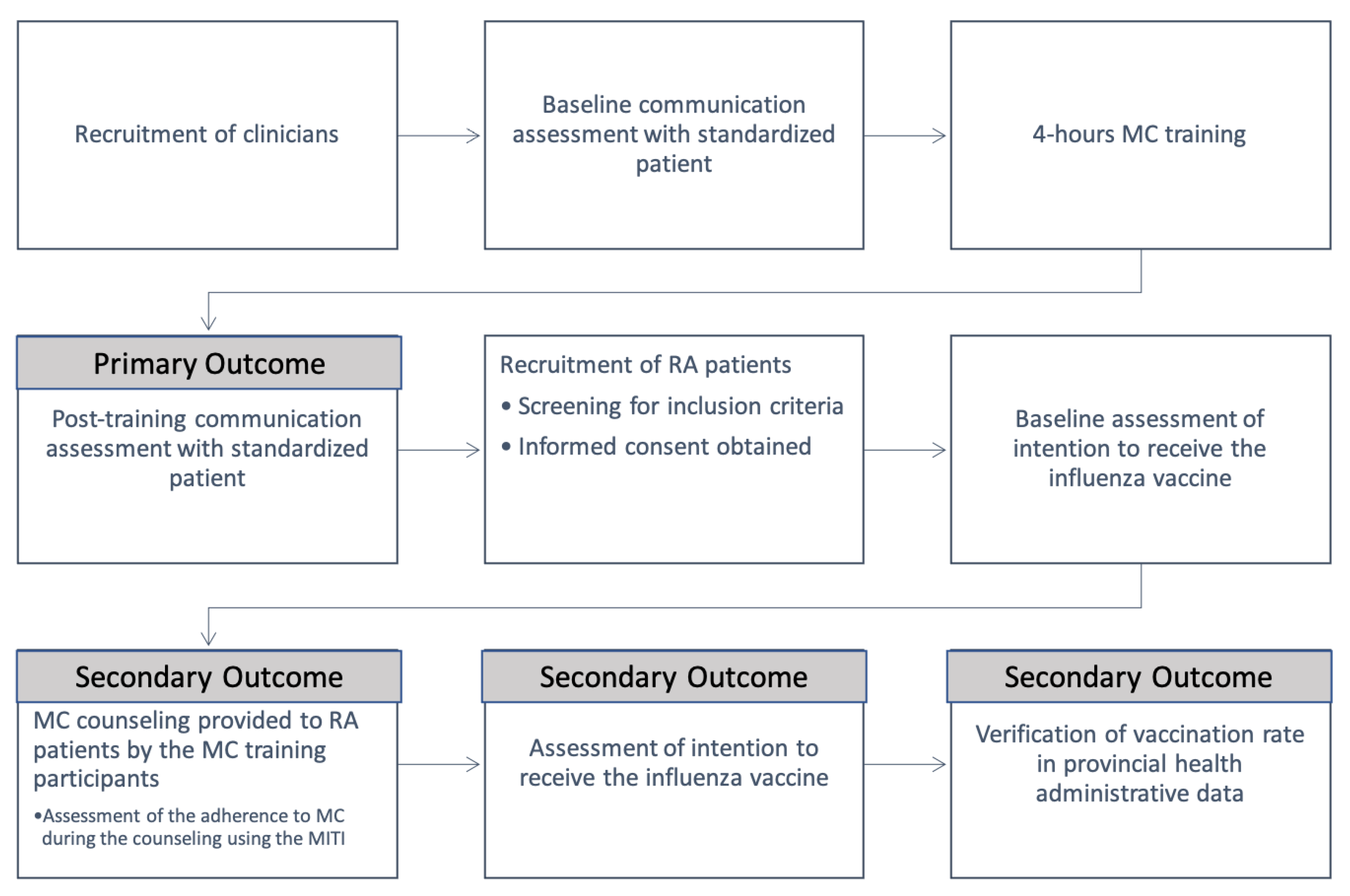
2.1. Study Design
2.2. Participants, Rheumatology Physicians
2.3. Patients with RA
2.4. Interventions and Measures: Clinicians
2.4.1. MC Competency with a Standardized Patient
2.4.2. MC Competency in Practice
2.5. Patients
2.5.1. Vaccine Hesitancy/Intention
2.5.2. Vaccination Rates
2.6. Motivational Communication Training Program
2.7. Outcomes
2.8. Data Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Fidelity of Training Delivery
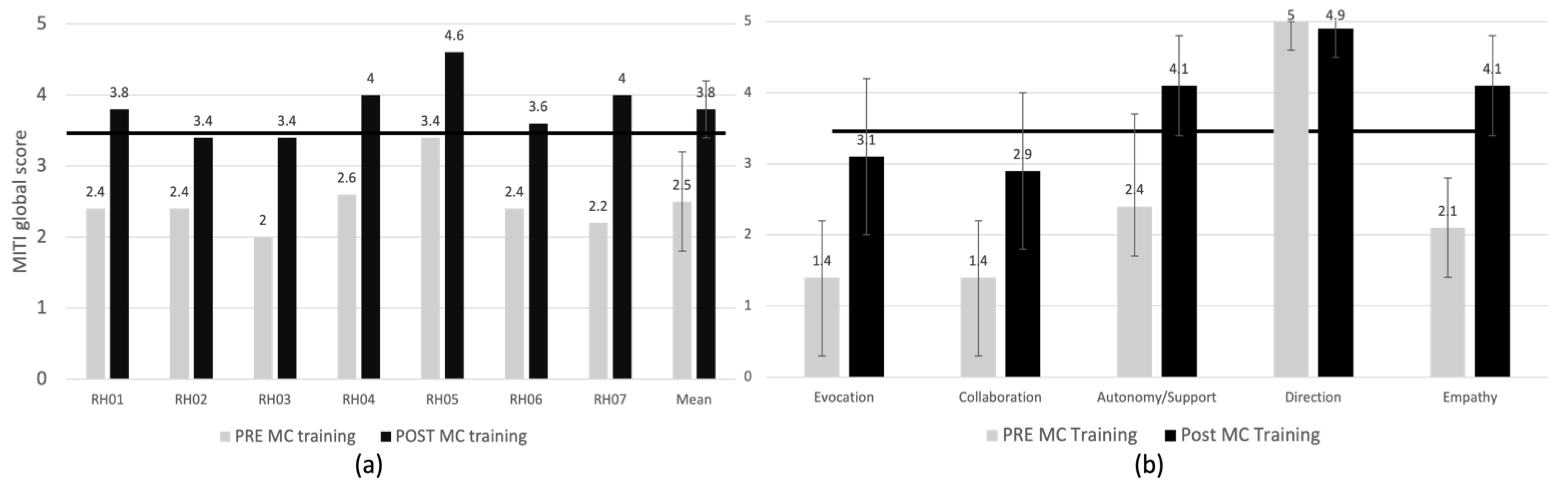
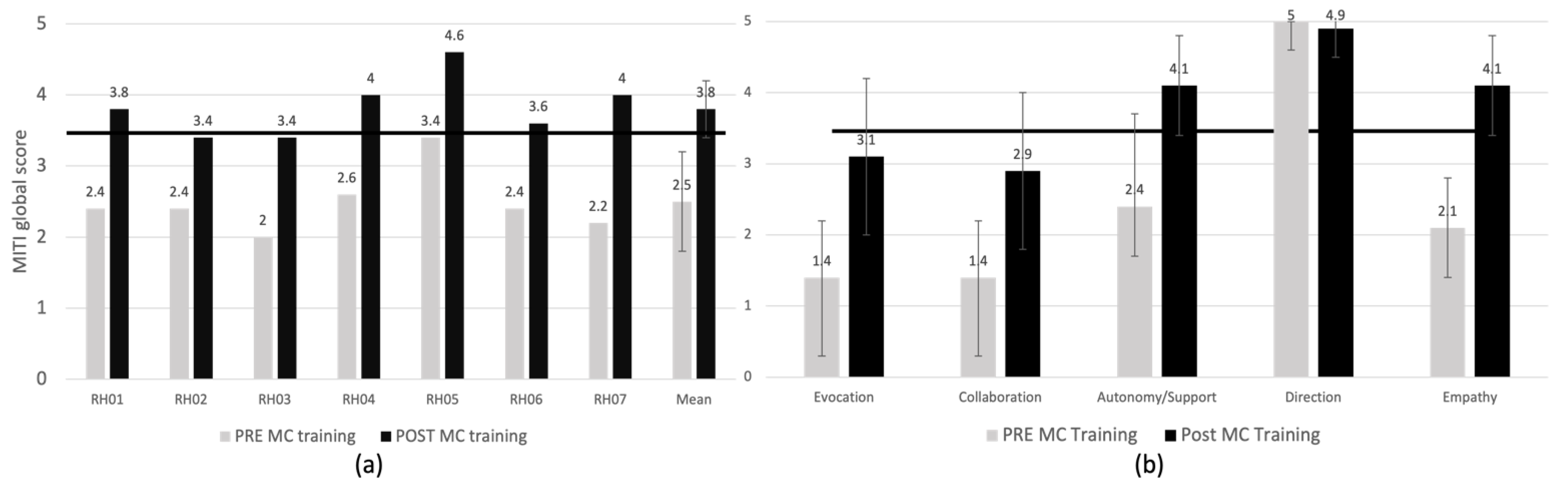
3.3. Primary Outcome
3.4. Secondary Outcomes
3.4.1. Change in MITI Global Score and Subscales
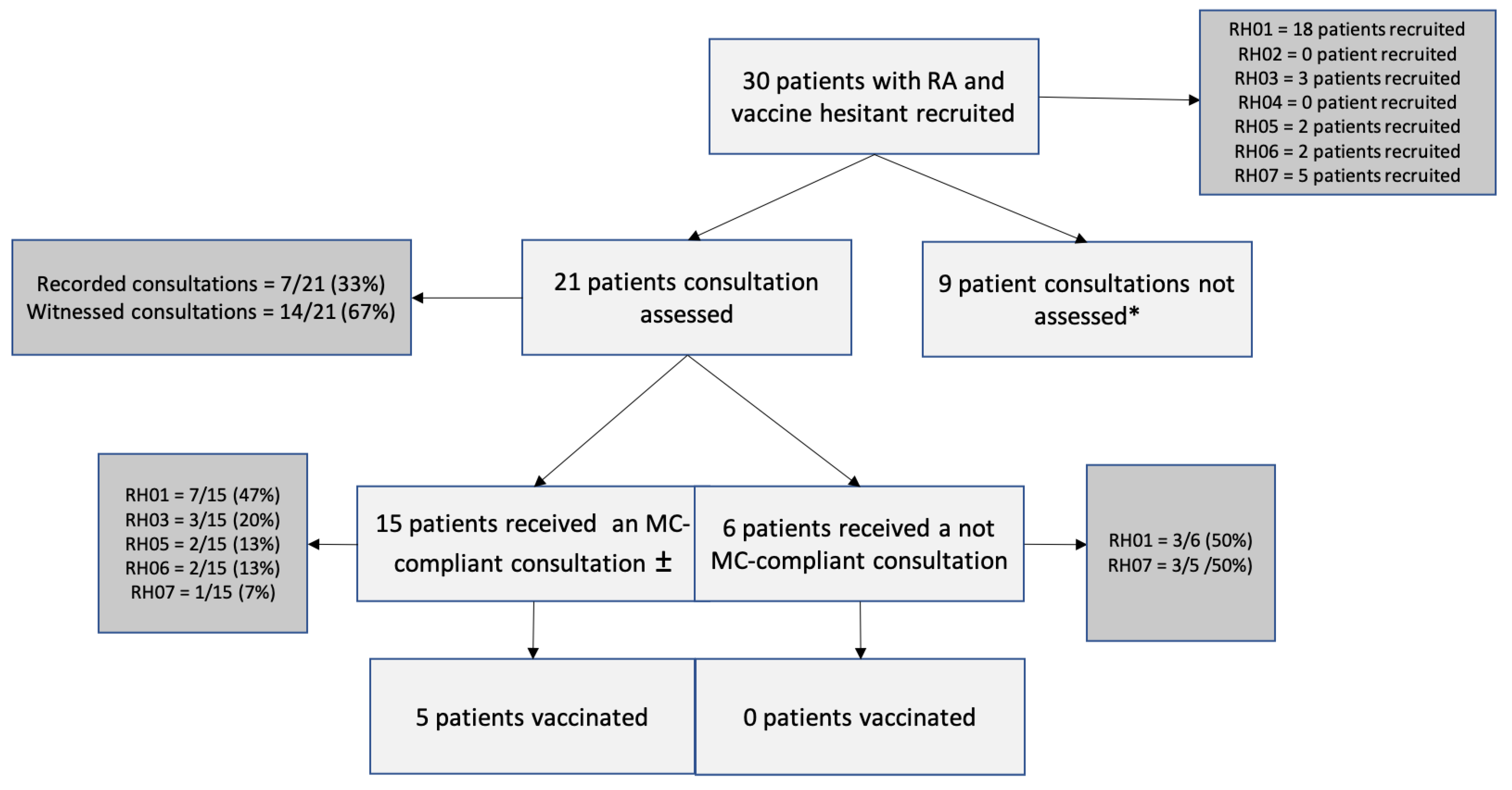
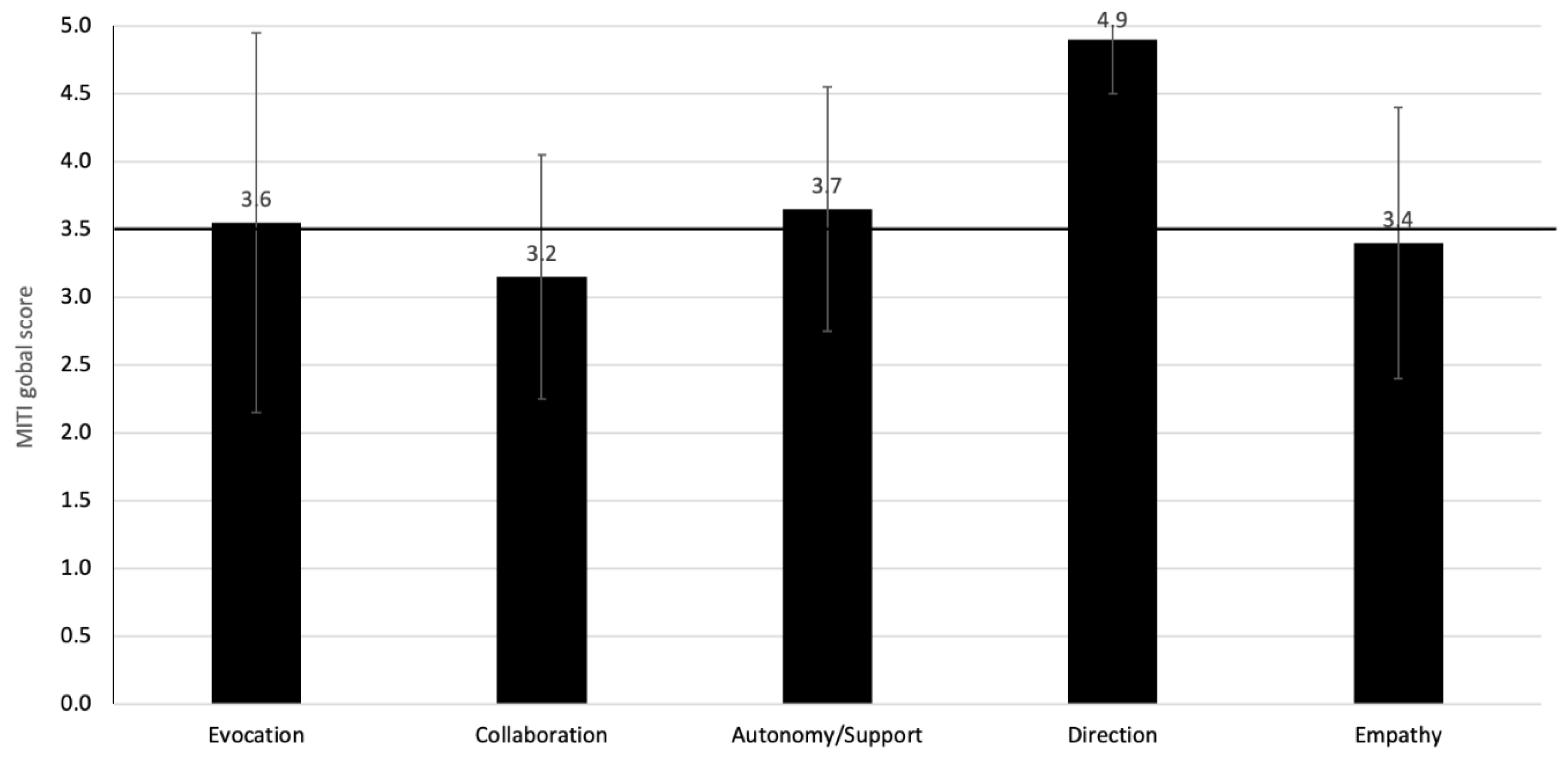
3.4.2. MC Compliance in Clinical Practice
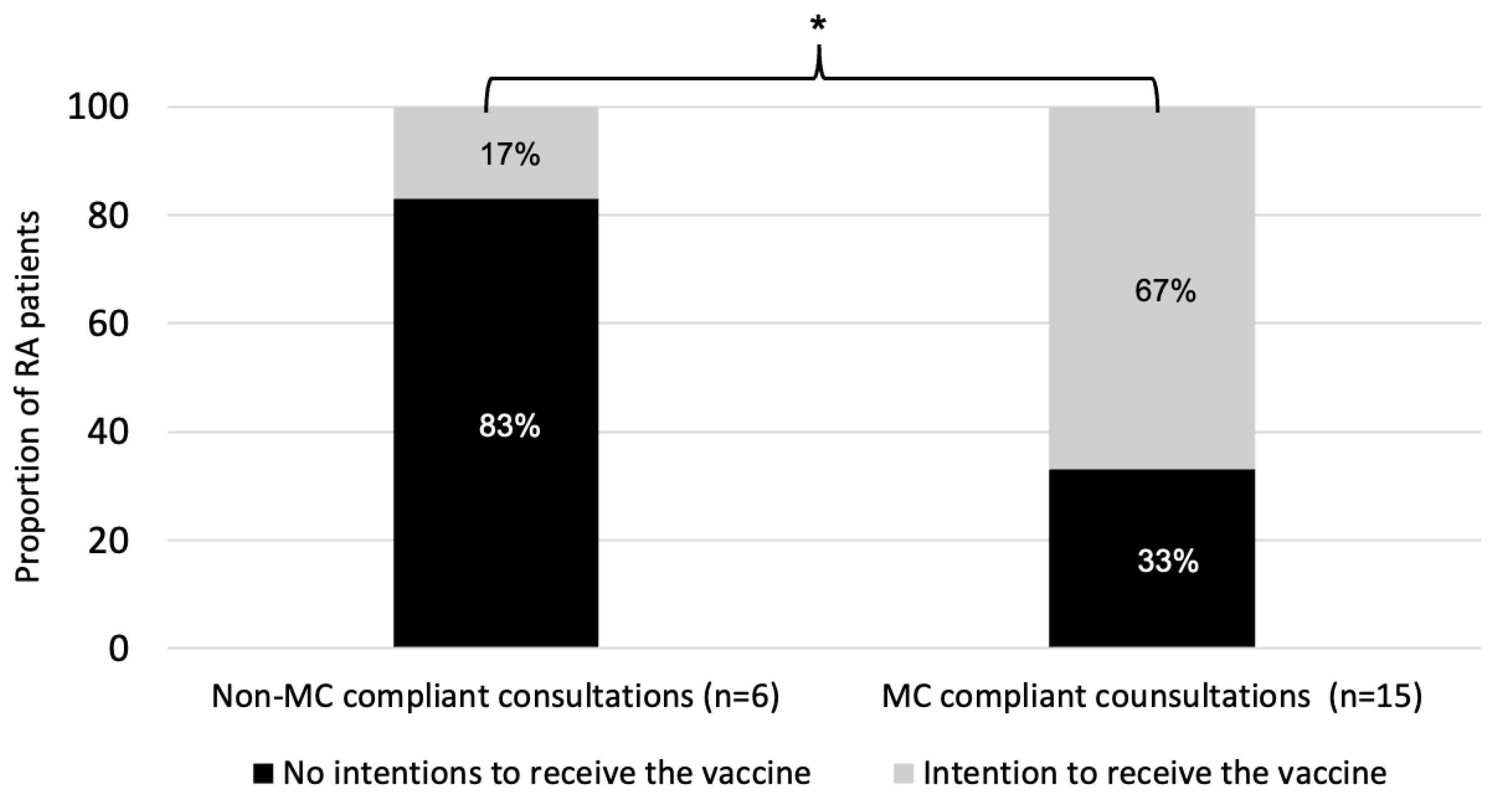
3.4.3. Change in Influenza Vaccine Intentions and Vaccination Rates among Patients with RA
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coyne, P.; Hamilton, J.; Heycock, C.; Saravanan, V.; Coulson, E.; Kelly, C.A. Acute lower respiratory tract infections in patients with rheumatoid arthritis. J. Rheumatol. 2007, 34, 1832–1836. [Google Scholar]
- Naz, S.M.; Symmons, D.P. Mortality in established rheumatoid arthritis. Best Pract. Res. Clin. Rheumatol. 2007, 21, 871–883. [Google Scholar] [CrossRef] [PubMed]
- van Assen, S.; Agmon-Levin, N.; Elkayam, O.; Cervera, R.; Doran, M.F.; Dougados, M.; Emery, P.; Geborek, P.; Ioannidis, J.P.; Jayne, D.R.; et al. EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 2011, 70, 414–422. [Google Scholar] [CrossRef] [Green Version]
- Riise, T.; Jacobsen, B.K.; Gran, J.T.; Haga, H.J.; Arnesen, E. Total mortality is increased in rheumatoid arthritis. A 17-year prospective study. Clin. Rheumatol. 2001, 20, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Blumentals, W.A.; Arreglado, A.; Napalkov, P.; Toovey, S. Rheumatoid arthritis and the incidence of influenza and influenza-related complications: A retrospective cohort study. BMC Musculoskelet. Disord. 2012, 13, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qendro, T.; de la Torre, M.L.; Panopalis, P.; Hazel, E.; Ward, B.J.; Colmegna, I.; Hudson, M. Suboptimal Immunization Coverage among Canadian Rheumatology Patients in Routine Clinical Care. J. Rheumatol. 2020, 47, 770–778. [Google Scholar] [CrossRef]
- Hmamouchi, I.; Winthrop, K.; Launay, O.; Dougados, M. Low rate of influenza and pneumococcal vaccine coverage in rheumatoid arthritis: Data from the international COMORA cohort. Vaccine 2015, 33, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, J.; Boucher, V.G.; Gagne, M.; Gupta, S.; Joyal-Desmarais, K.; Paduano, S.; Aburub, A.S.; Gorin, S.N.S.; Kassianos, A.P.; Ribeiro, P.A.B.; et al. Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study. Vaccines 2021, 9, 661. [Google Scholar] [CrossRef] [PubMed]
- WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/emergencies/ten-threats-to-global-health-in-2019 (accessed on 8 July 2019).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Thomas, R.E.; Lorenzetti, D.L. Interventions to increase influenza vaccination rates of those 60 years and older in the community. Cochrane Database Syst. Rev. 2018, 5, CD005188. [Google Scholar] [CrossRef]
- Corace, K.; Garber, G. When knowledge is not enough: Changing behavior to change vaccination results. Hum. Vaccines Immunother. 2014, 10, 2623–2624. [Google Scholar] [CrossRef] [Green Version]
- Sowden, E.; Mitchell, W.S. An audit of influenza and pneumococcal vaccination in rheumatology outpatients. BMC Musculoskelet. Disord. 2007, 8, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, S.; MacDonald, N.E.; Guirguis, S. Health communication and vaccine hesitancy. Vaccine 2015, 33, 4212–4214. [Google Scholar] [CrossRef] [Green Version]
- Rollnick, S.; Heather, N.; Bell, A. Negotiating behaviour change in medical settings: The development of brief motivational interviewing. J. Ment. Health 1992, 1, 25–37. [Google Scholar] [CrossRef]
- Burke, B.L.; Arkowitz, H.; Menchola, M. The efficacy of motivational interviewing: A meta-analysis of controlled clinical trials. J. Consult. Clin. Psychol. 2003, 71, 843–861. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.; Campbell, P.; Maxwell, M.; O’Carroll, R.E.; Dombrowski, S.U.; Williams, B.; Cheyne, H.; Coles, E.; Pollock, A. Effectiveness of Motivational Interviewing on adult behaviour change in health and social care settings: A systematic review of reviews. PLoS ONE 2018, 13, e0204890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, K.; Beauchamp, M.; Prothero, A.; Joyce, L.; Saunders, L.; Spencer-Bowdage, S.; Dancy, B.; Pedlar, C. The effectiveness of motivational interviewing for health behaviour change in primary care settings: A systematic review. Health Psychol. Rev. 2015, 9, 205–223. [Google Scholar] [CrossRef] [PubMed]
- Vasilaki, E.I.; Hosier, S.G.; Cox, W.M. The efficacy of motivational interviewing as a brief intervention for excessive drinking: A meta-analytic review. Alcohol Alcohol. 2006, 41, 328–335. [Google Scholar] [CrossRef] [Green Version]
- Gagneur, A.; Lemaitre, T.; Gosselin, V.; Farrands, A.; Carrier, N.; Petit, G.; Valiquette, L.; De Wals, P. A postpartum vaccination promotion intervention using motivational interviewing techniques improves short-term vaccine coverage: PromoVac study. BMC Public Health 2018, 18, 811. [Google Scholar] [CrossRef] [PubMed]
- Gagneur, A.; Battista, M.C.; Boucher, F.D.; Tapiero, B.; Quach, C.; De Wals, P.; Lemaitre, T.; Farrands, A.; Boulianne, N.; Sauvageau, C.; et al. Promoting vaccination in maternity wards horizontal line motivational interview technique reduces hesitancy and enhances intention to vaccinate, results from a multicentre non-controlled pre- and post-intervention RCT-nested study, Quebec, March 2014 to February 2015. Eurosurveillance 2019, 24, 1800641. [Google Scholar] [CrossRef] [Green Version]
- Real, F.J.; DeBlasio, D.; Beck, A.F.; Ollberding, N.J.; Davis, D.; Cruse, B.; Samaan, Z.; McLinden, D.; Klein, M.D. A Virtual Reality Curriculum for Pediatric Residents Decreases Rates of Influenza Vaccine Refusal. Acad. Pediatrics 2017, 17, 431–435. [Google Scholar] [CrossRef]
- Wermers, R.; Ostroski, T.; Hagler, D. Health care provider use of motivational interviewing to address vaccine hesitancy in college students. J. Am. Assoc. Nurse Pract. 2021, 33, 86–93. [Google Scholar] [CrossRef]
- Gagneur, A.; Bergeron, J.; Gosselin, V.; Farrands, A.; Baron, G. A complementary approach to the vaccination promotion continuum: An immunization-specific motivational-interview training for nurses. Vaccine 2019, 37, 2748–2756. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.W.; Rollnick, S. Motivational Interviewing: Preparing People for Change, 2nd ed.; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Dragomir, A.I.; Boucher, V.G.; Bacon, S.L.; Gemme, C.; Szczepanik, G.; Corace, K.; Campbell, T.S.; Vallis, M.T.; Garber, G.; Rouleau, C.; et al. An international Delphi consensus study to define motivational communication in the context of developing a training program for physicians. Transl. Behav. Med. 2020, 11, 642–652. [Google Scholar] [CrossRef]
- Dragomir, A.I.; Bacon, S.; Boucher, V.G.; Szczepanik, G.; Lavoie, K.L. Development of a Behavior Change Counselling Training Program for Physicians Using an Integrated Knowledge Translation Approach. In Annals of Behavioral Medicine; Oxford University Press: Oxford, UK, 2019; p. 299. [Google Scholar]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Peterson, J.C.; et al. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. 2015, 34, 971–982. [Google Scholar] [CrossRef]
- Moyers, T.B.; Martin, T.; Manuel, J.K.; Hendrickson, S.M.; Miller, W.R. Assessing competence in the use of motivational interviewing. J. Subst. Abus. Treat. 2005, 28, 19–26. [Google Scholar] [CrossRef]
- Boucher, V.G.; Pelaez, S.; Gemme, C.; Labbe, S.; Lavoie, K.L. Understanding factors associated with vaccine uptake and vaccine hesitancy in patients with rheumatoid arthritis: A scoping literature review. Clin. Rheumatol. 2020, 20, 244–489. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better Reporting of Interventions: Template for Intervention Description and Replication (TIDieR) Checklist and Guide. Gesundheitswesen 2016, 78, e174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, K.; Bourbeau, J.; MacDonald, R.; Wilt, T.J. Collaborative self-management and behavioral change. Clin. Chest Med. 2014, 35, 337–351. [Google Scholar] [CrossRef]
- Bacon, S.L.; Lavoie, K.L.; Boyle, J.; Stojanovic, J.; Joyal-Desmarais, K. International assessment of the link between COVID-19 related attitudes, concerns and behaviours in relation to public health policies: Optimising policy strategies to improve health, economic and quality of life outcomes (the iCARE Study). BMJ Open 2021, 11, e046127. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.; Staiger, P.K.; Simpson, A.; Best, D.; Lubman, D.I. After 30 years of dissemination, have we achieved sustained practice change in motivational interviewing? Addiction 2016, 111, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Schwalbe, C.S.; Oh, H.Y.; Zweben, A. Sustaining motivational interviewing: A meta-analysis of training studies. Addiction 2014, 109, 1287–1294. [Google Scholar] [CrossRef]
- Hardavella, G.; Aamli-Gaagnat, A.; Saad, N.; Rousalova, I.; Sreter, K.B. How to give and receive feedback effectively. Breathe 2017, 13, 327–333. [Google Scholar] [CrossRef]
- Hills, L. Giving and receiving constructive feedback: A staff training tool. J. Med. Pract. Manag. MPM 2010, 25, 356–359. [Google Scholar]
- Schechter, N.; Butt, L.; Jacocks, C.; Staguhn, E.; Castillo, R.; Wegener, S.T. Evaluation of an online motivational interviewing training program for rehabilitation professionals: A pilot study. Clin. Rehabil. 2021, 35, 1266–1276. [Google Scholar] [CrossRef] [PubMed]
- Sng, J.H.; Pei, Y.; Toh, Y.P.; Peh, T.Y.; Neo, S.H.; Krishna, L.K.R. Mentoring relationships between senior physicians and junior doctors and/or medical students: A thematic review. Med. Teach. 2017, 39, 866–875. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, D.T.; Varkey, P.; Cook, D.A. Mentoring programs for physicians in academic medicine: A systematic review. Acad. Med. 2013, 88, 1029–1037. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labbé, S.; Colmegna, I.; Valerio, V.; Boucher, V.G.; Peláez, S.; Dragomir, A.I.; Laurin, C.; Hazel, E.M.; Bacon, S.L.; Lavoie, K.L. Training Physicians in Motivational Communication to Address Influenza Vaccine Hesitation: A Proof-of-Concept Study. Vaccines 2022, 10, 143. https://doi.org/10.3390/vaccines10020143
Labbé S, Colmegna I, Valerio V, Boucher VG, Peláez S, Dragomir AI, Laurin C, Hazel EM, Bacon SL, Lavoie KL. Training Physicians in Motivational Communication to Address Influenza Vaccine Hesitation: A Proof-of-Concept Study. Vaccines. 2022; 10(2):143. https://doi.org/10.3390/vaccines10020143
Chicago/Turabian StyleLabbé, Sara, Inés Colmegna, Valeria Valerio, Vincent Gosselin Boucher, Sandra Peláez, Anda I. Dragomir, Catherine Laurin, Elizabeth M. Hazel, Simon L. Bacon, and Kim L. Lavoie. 2022. "Training Physicians in Motivational Communication to Address Influenza Vaccine Hesitation: A Proof-of-Concept Study" Vaccines 10, no. 2: 143. https://doi.org/10.3390/vaccines10020143
APA StyleLabbé, S., Colmegna, I., Valerio, V., Boucher, V. G., Peláez, S., Dragomir, A. I., Laurin, C., Hazel, E. M., Bacon, S. L., & Lavoie, K. L. (2022). Training Physicians in Motivational Communication to Address Influenza Vaccine Hesitation: A Proof-of-Concept Study. Vaccines, 10(2), 143. https://doi.org/10.3390/vaccines10020143