
Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go?



Abstract
1. Introduction
2. Methods for Study Selection
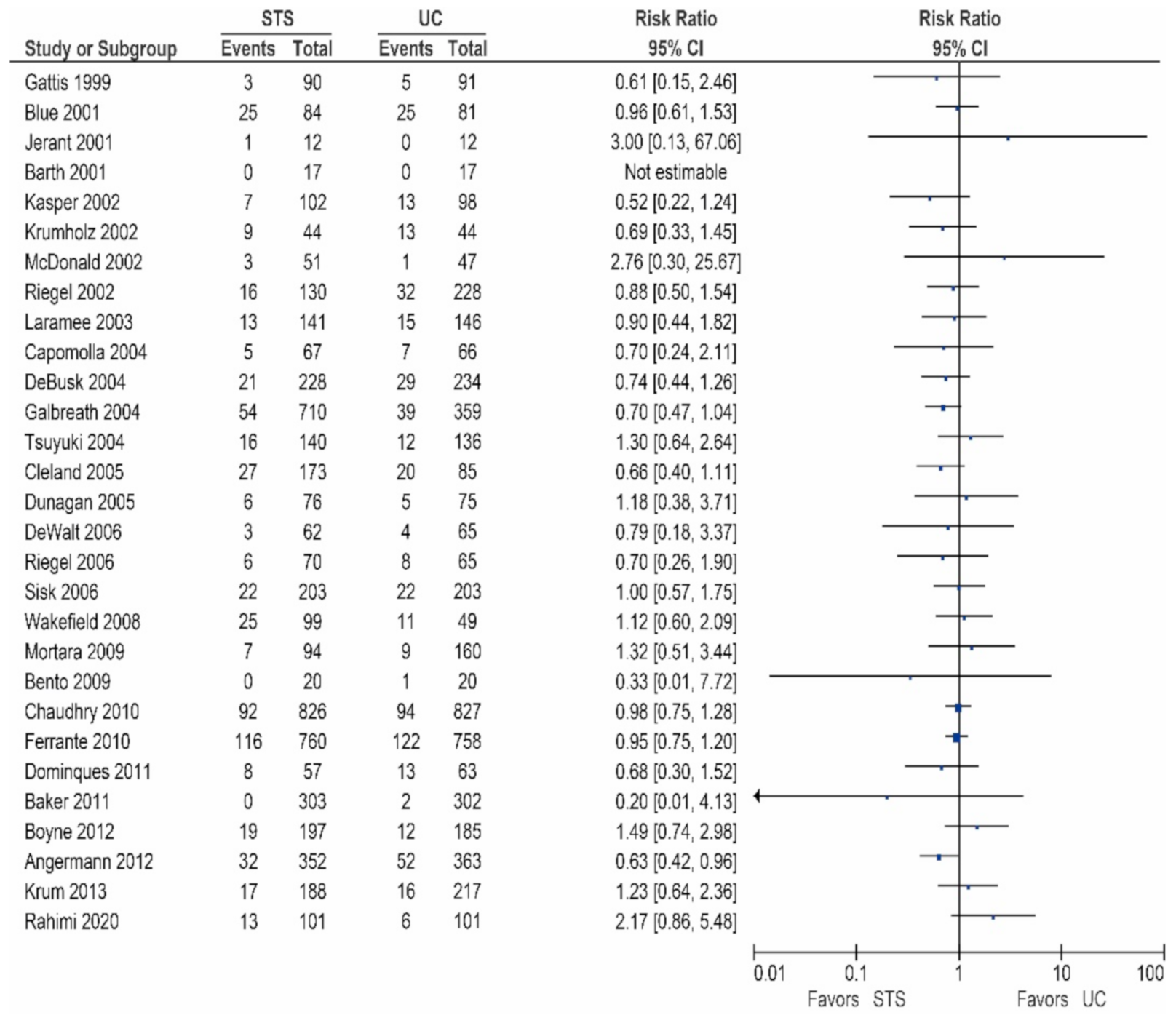
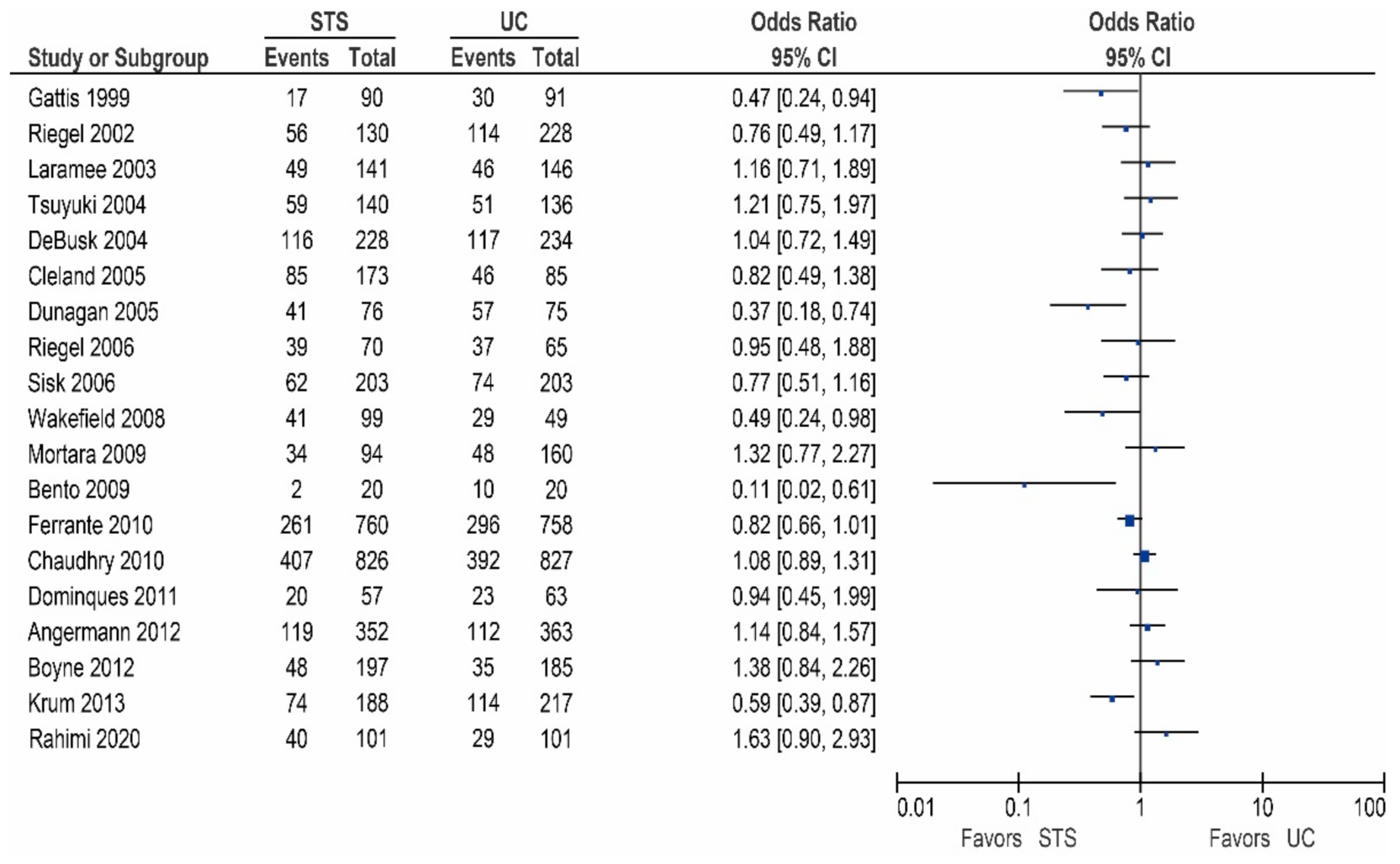
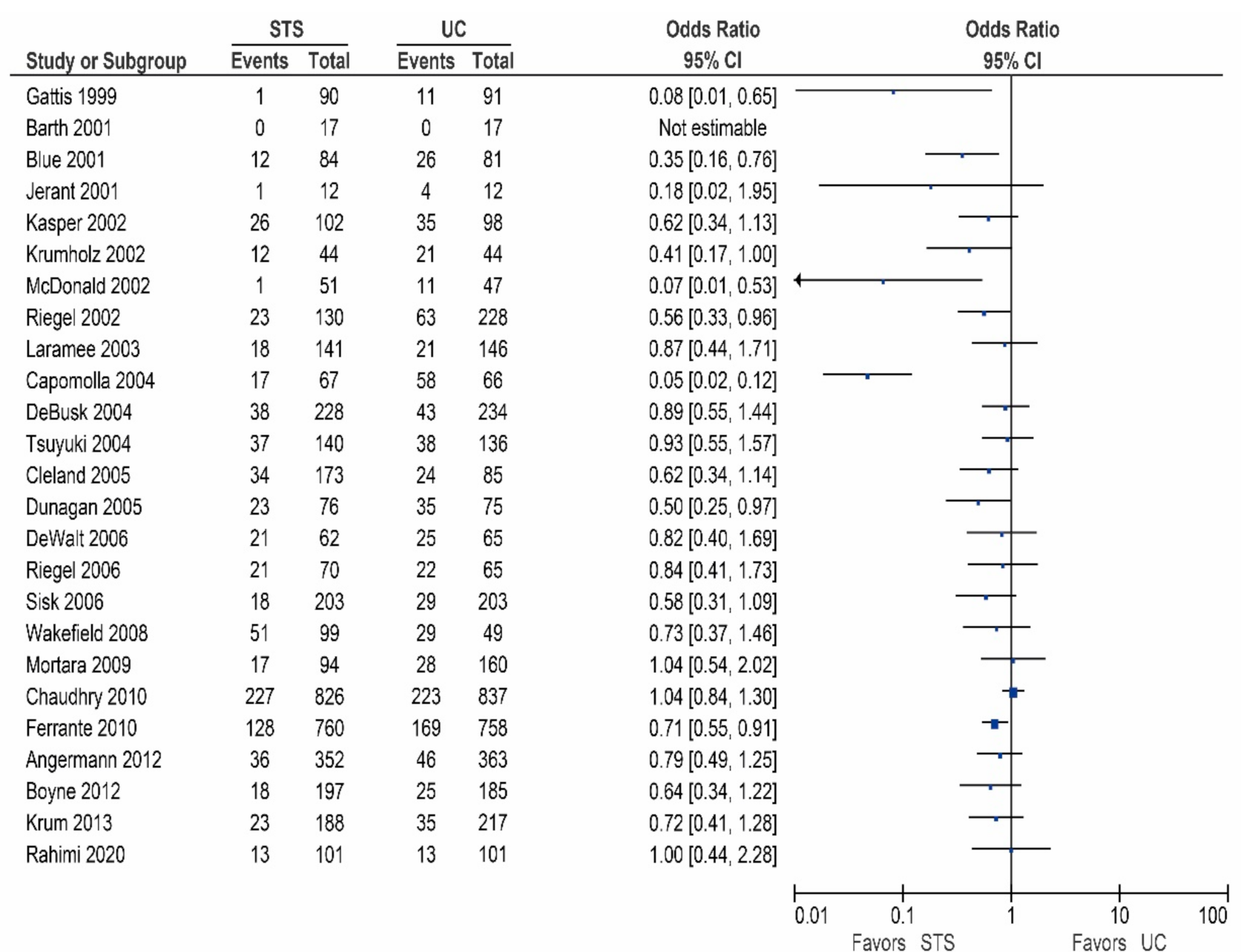
3. Structured Telephone Support versus Usual Care
3.1. Chaudhry et al. (Tele-HF Trial)
3.2. Ferrante et al. (DIAL Trial)
3.3. Galbreath et al.
3.4. Angermann et al. (INH Study)
3.5. Baker et al.
3.6. Other Studies
3.7. Quality of Life, Symptoms, and Functional Performance
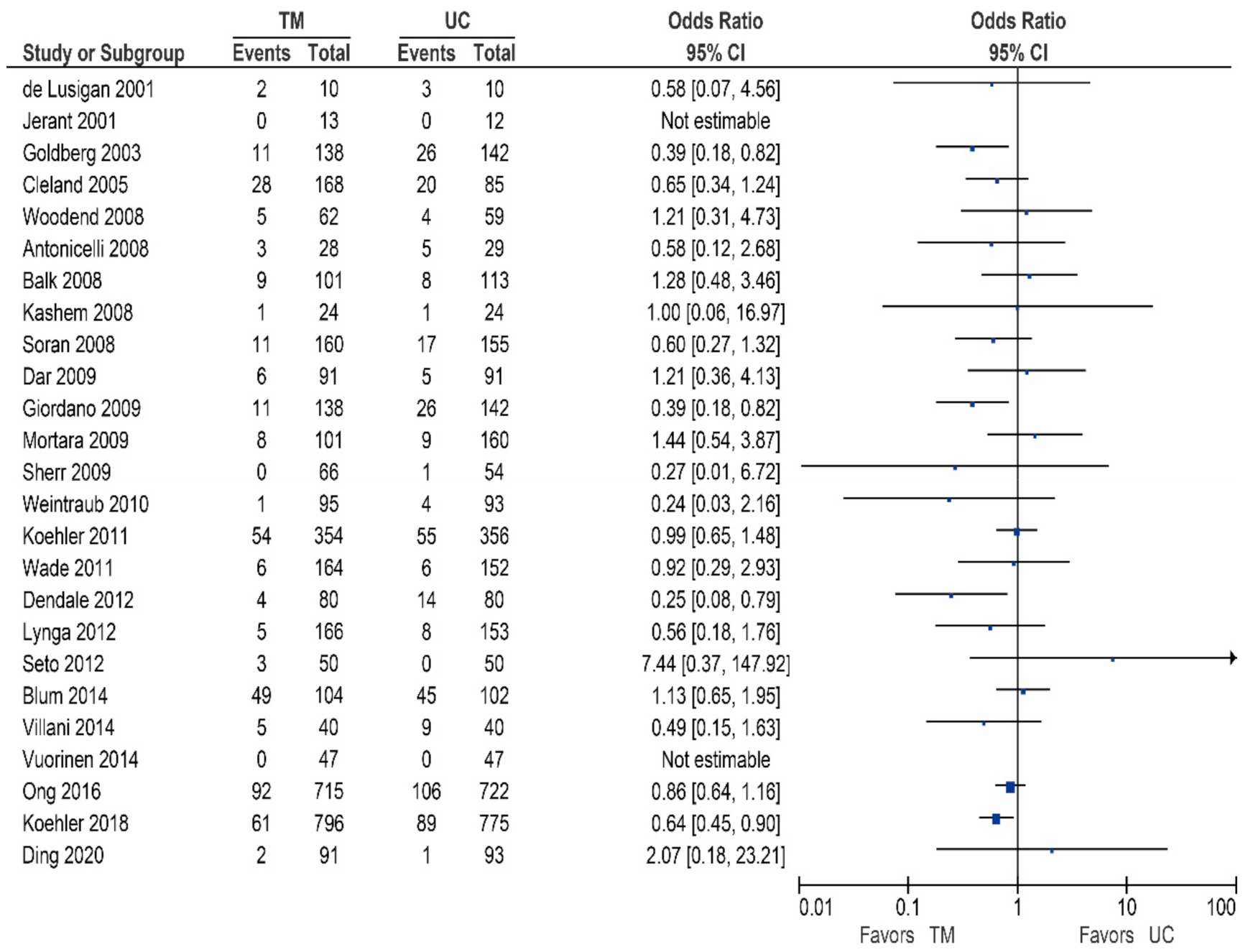
4. Non-Invasive Telemonitoring versus Usual Care
4.1. Koehler et al. (TIM-HF2 Trial)
4.2. Ong et al. (BEAT-HF Trial)
4.3. Koehler et al. (TIM-HF Study)
4.4. Mortara et al. (HHH Study)
4.5. Giordano et al.
4.6. Other Studies
4.7. Quality of Life, Symptoms, and Functional Performance
5. Overview of Available Studies for Non-Invasive Remote Monitoring in Heart Failure Management: Clinical Interpretations
5.1. Structured Telephone Support
5.2. Non-Invasive Telemonitoring
6. Reasons for Inconsistent Results
7. Future Perspectives
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponikowski, P.; Anker, S.D.; AlHabib, K.F.; Cowie, M.R.; Force, T.L.; Hu, S.; Jaarsma, T.; Krum, H.; Rastogi, V.; Rohde, L.E.; et al. Heart failure: Preventing disease and death worldwide. ESC Heart Fail. 2014, 1, 4–25. [Google Scholar] [CrossRef] [PubMed]
- Najafi, F.; Jamrozik, K.; Dobson, A.J. Understanding the ’epidemic of heart failure’: A systematic review of trends in deter-minants of heart failure. Eur. J. Heart Fail. 2009, 11, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.L.; Tong, X.; King, R.J.; Loustalot, F.; Hong, Y.; Ritchey, M.D. National Burden of Heart Failure Events in the United States, 2006 to 2014. Circ. Hear. Fail. 2018, 11, e004873. [Google Scholar] [CrossRef] [PubMed]
- Farré, N.; Vela, E.; Clèries, M.; Bustins, M.; Cainzos-Achirica, M.; Enjuanes, C.; Moliner, P.; Ruiz, S.; Verdú-Rotellar, J.M.; Comín-Colet, J. Real world heart failure epidemiology and outcome: A population-based analysis of 88,195 patients. PLoS ONE 2017, 12, e0172745. [Google Scholar] [CrossRef] [PubMed]
- Buddeke, J.; Valstar, G.B.; Van Dis, I.; Visseren, F.L.J.; Rutten, F.H.; Ruijter, H.M.D.; Vaartjes, I.; Bots, M.L. On behalf of the Queen of Hearts and RECONNECT investigators Mortality after hospital admission for heart failure: Improvement over time, equally strong in women as in men. BMC Public Health 2020, 20, 36. [Google Scholar] [CrossRef]
- Abraham, W.T. The Role of Implantable Hemodynamic Monitors to Manage Heart Failure. Cardiol. Clin. 2017, 35, 273–279. [Google Scholar] [CrossRef]
- Brugts, J.J.; Linssen, G.C.M.; Hoes, A.W.; Brunner-La Rocca, H.P. CHECK-HF investigators. Real-world heart failure manage-ment in 10,910 patients with chronic heart failure in the Netherlands: Design and rationale of the Chronic Heart failure ESC guideline-based Cardiology practice Quality project (CHECK-HF) registry. Neth Heart J. 2018, 26, 272–279. [Google Scholar] [CrossRef]
- Brunner-La Rocca, H.P.; Linssen, G.C.; Smeele, F.J.; van Drimmelen, A.A.; Schaafsma, H.J.; Westendorp, P.H.; Rademaker, P.C.; van de Kamp, H.J.; Hoes, A.W.; Brugts, J.J. Contemporary Drug Treatment of Chronic Heart Failure With Reduced Ejection Fraction: The CHECK-HF Registry. JACC Heart Fail. 2019, 7, 13–21. [Google Scholar] [CrossRef]
- Veenis, J.F.; Rocca, H.-P.B.-L.; Linssen, G.C.; Geerlings, P.R.; Van Gent, M.W.; Aksoy, I.; Oosterom, L.; Moons, A.H.; Hoes, A.W.; Brugts, J.J.; et al. Age differences in contemporary treatment of patients with chronic heart failure and reduced ejection fraction. Eur. J. Prev. Cardiol. 2019, 26, 1399–1407. [Google Scholar] [CrossRef]
- Greene, S.J.; Butler, J.; Albert, N.M.; DeVore, A.D.; Sharma, P.P.; Duffy, C.I.; Hill, C.L.; McCague, K.; Mi, X.; Patterson, J.H.; et al. Medical Therapy for Heart Failure With Reduced Ejection Fraction: The CHAMP-HF Registry. J. Am. Coll. Cardiol. 2018, 72, 351–366. [Google Scholar] [CrossRef]
- Smeets, C.J.; Storms, V.; Vandervoort, P.M.; Dreesen, P.; Vranken, J.; Houbrechts, M.; Goris, H.; Grieten, L.; Dendale, P. A Novel Intelligent Two-Way Communication System for Remote Heart Failure Medication Uptitration (the CardioCoach Study): Randomized Controlled Feasibility Trial. JMIR Cardio 2018, 2, e8. [Google Scholar] [CrossRef] [PubMed]
- Inglis, S.C.; Clark, R.A.; Dierckx, R.; Prieto-Merino, D.; Cleland, J.G. Structured telephone support or non-invasive telemonitor-ing for patients with heart failure. Cochrane Database Syst. Rev. 2015, 10, CD007228. [Google Scholar]
- Alotaibi, S.; Hernandez-Montfort, J.; Ali, O.E.; El-Chilali, K.; Perez, B.A. Remote monitoring of implantable cardiac devices in heart failure patients: A systematic review and meta-analysis of randomized controlled trials. Hear. Fail. Rev. 2020, 25, 469–479. [Google Scholar] [CrossRef]
- Abraham, W.T.; Stevenson, L.W.; Bourge, R.C.; Lindenfeld, J.A.; Bauman, J.G.; Adamson, P.B. Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: Complete follow-up results from the CHAMPION randomised trial. Lancet 2016, 387, 453–461. [Google Scholar] [CrossRef]
- Rahimi, K.; Nazarzadeh, M.; Pinho-Gomes, A.-C.; Woodward, M.; Salimi-Khorshidi, G.; Ohkuma, T.; Fitzpatrick, R.; Tarassenko, L.; Denis, M.; Cleland, J.; et al. Home monitoring with technology-supported management in chronic heart failure: A randomised trial. Heart 2020, 106, 1573–1578. [Google Scholar] [PubMed]
- Gingele, A.J.; Ramaekers, B.; Rocca, H.P.B.-L.; De Weerd, G.; Kragten, J.; Van Empel, V.; Van Der Weg, K.; Vrijhoef, H.J.M.; Gorgels, A.; Cleuren, G.; et al. Effects of tailored telemonitoring on functional status and health-related quality of life in patients with heart failure. Neth. Hear. J. 2019, 27, 565–574. [Google Scholar] [CrossRef]
- Krum, H.; Forbes, A.; Yallop, J.; Driscoll, A.; Croucher, J.; Chan, B.; Clark, R.; Davidson, P.M.; Huynh, L.; Kasper, E.K.; et al. Telephone Support to Rural and Remote Patients with Heart Failure: The Chronic Heart Failure Assessment by Telephone (CHAT) study. Cardiovasc. Ther. 2013, 31, 230–237. [Google Scholar] [CrossRef]
- Boyne, J.J.; Vrijhoef, H.J.; Crijns, H.J.; De Weerd, G.; Kragten, J.; Gorgels, A.P. TEHAF investigators. Tailored telemonitoring in patients with heart failure: Results of a multicentre ran-domized controlled trial. Eur. J. Heart Fail. 2012, 14, 791–801. [Google Scholar] [CrossRef]
- Angermann, C.E.; Störk, S.; Gelbrich, G.; Faller, H.; Jahns, R.; Frantz, S.; Loeffler, M.; Ertl, G. Mode of action and effects of standardized collaborative disease management on mortality and morbidity in patients with systolic heart failure: The Interdisciplinary Network for Heart Failure (INH) study. Circ. Heart Fail. 2012, 5, 25–35. [Google Scholar] [CrossRef]
- Domingues, F.B.; Clausell, N.; Aliti, G.B.; Dominguez, D.R.; Rabelo, E.R. Education and telephone monitoring by nurses of patients with heart failure: Randomized clinical trial. Arq. Bras. de Cardiol. 2011, 96, 233–239. [Google Scholar] [CrossRef]
- Baker, D.W.; DeWalt, D.A.; Schillinger, D.; Hawk, V.; Ruo, B.; Bibbins-Domingo, K.; Weinberger, M.; Macabasco-O’Connell, A.; Grady, K.L.; Holmes, G.M.; et al. The Effect of Progressive, Reinforcing Telephone Education and Counseling Versus Brief Educational Intervention on Knowledge, Self-Care Behaviors and Heart Failure Symptoms. J. Card. Fail. 2011, 17, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, D.; Varini, S.; Macchia, A.; Soifer, S.; Badra, R.; Nul, D.; Grancelli, H.; Doval, H. GESICA Investigators. Long-term results after a telephone intervention in chronic heart failure: DIAL (Ran-domized Trial of Phone Intervention in Chronic Heart Failure) follow-up. J. Am. Coll. Cardiol. 2010, 56, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, S.I.; Mattera, J.A.; Curtis, J.P.; Spertus, J.A.; Herrin, J.; Lin, Z.; Phillips, C.O.; Hodshon, B.V.; Cooper, L.S.; Krumholz, H.M. Telemonitoring in Patients with Heart Failure. New Engl. J. Med. 2010, 363, 2301–2309. [Google Scholar] [CrossRef] [PubMed]
- Mortara, A.; Pinna, G.D.; Johnson, P.; Maestri, R.; Capomolla, S.; La Rovere, M.T.; Ponikowski, P.; Tavazzi, L.; Sleight, P. On behalf of the HHH Investigators Home telemonitoring in heart failure patients: The HHH study (Home or Hospital in Heart Failure). Eur. J. Hear. Fail. 2009, 11, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Bento, V.F.; Brofman, P.R. Impact of the nursing consultation on the frequency of hospitalizations in patients with heart failure in Curitiba, Parana State. Arq. Bras Cardiol. 2009, 92, 454–460. [Google Scholar]
- Brandon, A.F.; Schuessler, J.B.; Ellison, K.J.; Lazenby, R.B. The effects of an advanced practice nurse led telephone intervention on outcomes of patients with heart failure. Appl. Nurs. Res. 2009, 22, e1–e7. [Google Scholar] [CrossRef]
- Wakefield, B.J.; Ward, M.M.; Holman, J.E.; Ray, A.; Scherubel, M.; Burns, T.L.; Kienzle, M.G.; Rosenthal, G.E. Evaluation of home telehealth following hospitalization for heart failure: A ran-domized trial. Telemed. J. E Health. 2008, 14, 753–761. [Google Scholar] [CrossRef]
- Sisk, J.E.; Hebert, P.L.; Horowitz, C.R.; McLaughlin, M.A.; Wang, J.J.; Chassin, M.R. Effects of nurse management on the quality of heart failure care in minority communities: A randomized trial. Ann. Intern. Med. 2006, 145, 273–283. [Google Scholar] [CrossRef]
- Riegel, B.; Carlson, B.; Glaser, D.; Romero, T. Randomized Controlled Trial of Telephone Case Management in Hispanics of Mexican Origin with Heart Failure. J. Card. Fail. 2006, 12, 211–219. [Google Scholar] [CrossRef]
- DeWalt, D.A.; Malone, R.M.; Bryant, M.; Kosnar, M.C.; Corr, K.; Rothman, R.L.; Sueta, C.; Pignone, M.P. A heart failure self-management program for patients of all literacy levels: A randomized, controlled trial [ISRCTN11535170]. BMC Health Serv. Res. 2006, 6, 30. [Google Scholar] [CrossRef]
- Dunagan, W.C.; Littenberg, B.; Ewald, G.A.; Jones, C.A.; Emery, V.B.; Waterman, B.M.; Silverman, D.C.; Rogers, J.G. Randomized trial of a nurse-administered, telephone-based disease manage-ment program for patients with heart failure. J. Card Fail. 2005, 11, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Louis, A.; Rigby, A.; Janssens, U.; Balk, A. Noninvasive Home Telemonitoring for Patients With Heart Failure at High Risk of Recurrent Admission and Death: The Trans-European Network–Home-Care Management System (TEN-HMS) Study. ACC Curr. J. Rev. 2005, 14, 37. [Google Scholar] [CrossRef]
- Tsuyuki, R.T.; Fradette, M.; Johnson, J.A.; Bungard, T.J.; Eurich, D.T.; Ashton, T.; Gordon, W.; Ikuta, R.; Kornder, J.; Mackay, E.; et al. A multicenter disease management program for hospitalized patients with heart failure. J. Card. Fail. 2004, 10, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Galbreath, A.D.; Krasuski, R.A.; Smith, B.; Stajduhar, K.; Kwan, M.D.; Ellis, R.; Freeman, G.L. Long-Term Healthcare and Cost Outcomes of Disease Management in a Large, Randomized, Community-Based Population With Heart Failure. Circulation 2004, 110, 3518–3526. [Google Scholar] [CrossRef] [PubMed]
- De Busk, R.; Miller, N.; Parker, K. Care management for low-risk patients with heart failure: A randomized, controlled trial. ACC Curr. J. Rev. 2005, 14, 34–35. [Google Scholar] [CrossRef]
- Capomolla, S.; Pinna, G.; La Rovere, M.T.; Maestri, R.; Ceresa, M.; Ferrari, M.; Febo, O.; Caporotondi, A.; Guazzotti, G.; Lenta, F.; et al. Heart failure case disease management program: A pilot study of home tele-monitoring versus usual care. Eur. Heart J. Suppl. 2004, 6, F91–F98. [Google Scholar] [CrossRef]
- Laramee, A.S.; Levinsky, S.K.; Sargent, J.; Ross, R.; Callas, P. Case management in a heterogeneous congestive heart failure population: A randomized controlled trial. Arch. Intern. Med. 2003, 163, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Carlson, B.; Kopp, Z.; LePetri, B.; Glaser, D.; Unger, A. Effect of a Standardized Nurse Case-Management Telephone Intervention on Resource Use in Patients With Chronic Heart Failure. Arch. Intern. Med. 2002, 162, 705–712. [Google Scholar] [CrossRef]
- McDonald, K.; Ledwidge, M.; Cahill, J.; Quigley, P.; Maurer, B.; Travers, B.; Ryder, M.; Kieran, E.; Timmons, L.; Ryan, E. Heart failure management: Multidisciplinary care has intrinsic benefit above the optimization of medical care. J. Card. Fail. 2002, 8, 142–148. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Amatruda, J.; Smith, G.L.; Mattera, J.A.; Roumanis, S.A.; Radford, M.J.; Crombie, P.; Vaccarino, V. Randomized trial of an education and support intervention to prevent read-mission of patients with heart failure. J. Am. Coll. Cardiol. 2002, 39, 83–89. [Google Scholar] [CrossRef]
- Kasper, E.K.; Gerstenblith, G.; Hefter, G.; Van Anden, E.; Brinker, J.A.; Thiemann, D.R.; Terrin, M.; Forman, S.; Gottlieb, S.H. A randomized trial of the efficacy of multidisciplinary care in heart failure out-patients at high risk of hospital readmission. J. Am. Coll. Cardiol. 2002, 39, 471–480. [Google Scholar] [CrossRef]
- Jerant, A.F.; Azari, R.; Nesbitt, T.S. Reducing the cost of frequent hospital admissions for congestive heart failure: A random-ized trial of a home telecare intervention. Med. Care 2001, 39, 1234–1245. [Google Scholar] [CrossRef] [PubMed]
- Blue, L.; Lang, E.; McMurray, J.J.; Davie, A.P.; McDonagh, T.A.; Murdoch, D.R.; Petrie, M.C.; Connolly, E.; Norrie, J.; Round, C.E.; et al. Randomised controlled trial of specialist nurse intervention in heart failure. BMJ 2001, 323, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Barth, V. A Nurse-Managed Discharge Program for Congestive Heart Failure Patients: Outcomes and Costs. Home Health Care Manag. Pr. 2001, 13, 436–443. [Google Scholar] [CrossRef]
- Gattis, W.A.; Hasselblad, V.; Whellan, D.J.; O’Connor, C.M. Reduction in heart failure events by the addition of a clinical pharmacist to the heart failure management team: Results of the Pharmacist in Heart Failure Assessment Recommendation and Monitoring (PHARM) Study. Arch Intern Med. 1999, 159, 1939–1945. [Google Scholar] [CrossRef]
- Smith, B.; Forkner, E.; Zaslow, B.; Krasuski, R.A.; Stajduhar, K.; Kwan, M.; Ellis, R.; Galbreath, A.D.; Freeman, G.L. Disease management produces limited quality-of-life improvements in patients with congestive heart failure: Evidence from a randomized trial in community-dwelling patients. Am. J. Manag. Care 2005, 11, 701–713. [Google Scholar]
- Haynes, S.C.; Tancredi, D.J.; Tong, K.; Hoch, J.S.; Ong, M.K.; Ganiats, T.G.; Evangelista, L.S.; Black, J.T.; Auerbach, A.; Romano, P.S. The Effect of Rehospitalization and Emergency Department Visits on Subsequent Adherence to Weight Telemonitoring. J. Cardiovasc. Nurs. 2020. [Google Scholar] [CrossRef]
- Ding, H.; Jayasena, R.; Chen, S.H.; Maiorana, A.; Dowling, A.; Layland, J.; Good, N.; Karunanithi, M.; Edwards, I. The Effects of Telemonitoring on Patient Compliance With Self-Management Recom-mendations and Outcomes of the Innovative Telemonitoring Enhanced Care Program for Chronic Heart Failure: Random-ized Controlled Trial. J. Med. Internet Res. 2020, 22, e17559. [Google Scholar] [CrossRef]
- Pekmezaris, R.; Nouryan, C.N.; Schwartz, R.; Castillo, S.; Makaryus, A.N.; Ahern, D.; Akerman, M.B.; Lesser, M.L.; Bauer, L.; Murray, L.; et al. A Randomized Controlled Trial Comparing Telehealth Self-Management to Standard Outpatient Management in Underserved Black and Hispanic Patients Living with Heart Failure. Telemed. e-Health 2019, 25, 917–925. [Google Scholar] [CrossRef]
- Park, C.; Otobo, E.; Ullman, J.; Rogers, J.; Fasihuddin, F.; Garg, S.; Kakkar, S.; Goldstein, M.; Chandrasekhar, S.V.; Pinney, S.; et al. Impact on Readmission Reduction Among Heart Failure Patients Using Digital Health Monitoring: Feasibility and Adoptability Study. JMIR Med. Informatics 2019, 7, e13353. [Google Scholar] [CrossRef]
- Koehler, F.; Koehler, K.; Deckwart, O.; Prescher, S.; Wegscheider, K.; Kirwan, B.-A.; Winkler, S.; Vettorazzi, E.; Bruch, L.; Oeff, M.; et al. Efficacy of telemedical interventional management in patients with heart failure (TIM-HF2): A randomised, controlled, parallel-group, unmasked trial. Lancet 2018, 392, 1047–1057. [Google Scholar] [CrossRef]
- Ong, M.K.; Romano, P.S.; Edgington, S.; Aronow, H.U.; Auerbach, A.D.; Black, J.T.; De Marco, T.; Escarce, J.J.; Evangelista, L.S.; Hanna, B.; et al. Effectiveness of Remote Patient Monitoring After Discharge of Hospitalized Pa-tients With Heart Failure: The Better Effectiveness After Transition—Heart Failure (BEAT-HF) Randomized Clinical Trial. JAMA Intern Med. 2016, 176, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Vuorinen, A.L.; Leppänen, J.; Kaijanranta, H.; Kulju, M.; Heliö, T.; van Gils, M.; Lähteenmäki, J. Use of home telemonitoring to support multidisciplinary care of heart fail-ure patients in Finland: Randomized controlled trial. J. Med. Internet Res. 2014, 16, e282. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Malfatto, G.; Compare, A.; Della Rosa, F.; Bellardita, L.; Branzi, G.; Molinari, E.; Parati, G. Clinical and psychological telemonitoring and telecare of high risk heart failure patients. J. Telemed. Telecare 2014, 20, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Gottlieb, S.S. The effect of a randomized trial of home telemonitoring on medical costs, 30-day readmissions, mortality, and health-related quality of life in a cohort of community-dwelling heart failure patients. J. Card Fail. 2014, 20, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Seto, E.; Leonard, K.J.; Cafazzo, J.A.; Barnsley, J.; Masino, C.; Ross, H.J. Mobile Phone-Based Telemonitoring for Heart Failure Management: A Randomized Controlled Trial. J. Med. Internet Res. 2012, 14, e31. [Google Scholar] [CrossRef]
- Pekmezaris, R.; Mitzner, I.; Pecinka, K.R.; Nouryan, C.N.; Lesser, M.L.; Siegel, M.; Swiderski, J.W.; Moise, G.; Younker Sr, R.; Smolich, K. The impact of remote patient monitoring (telehealth) upon Medicare beneficiar-ies with heart failure. Telemed. J. E Health. 2012, 18, 101–108. [Google Scholar] [CrossRef]
- Lynga, P.; Persson, H.; Hägg-Martinell, A.; Hägglund, E.; Hagerman, I.; Langius-Eklöf, A.; Rosenqvist, M. Weight monitoring in patients with severe heart failure (WISH). A randomized controlled trial. Eur. J. Hear. Fail. 2012, 14, 438–444. [Google Scholar] [CrossRef]
- Dendale, P.; De Keulenaer, G.; Troisfontaines, P.; Weytjens, C.; Mullens, W.; Elegeert, I.; Ector, B.; Houbrechts, M.; Willekens, K.; Hansen, D. Effect of a telemonitoring-facilitated collaboration between general practitioner and heart failure clinic on mortality and rehospitalization rates in severe heart failure: The TEMA-HF 1 (TEle-monitoring in the MAnagement of Heart Failure) study. Eur. J. Heart Fail. 2012, 14, 333–340. [Google Scholar] [CrossRef]
- Wade, M.J.; Desai, A.S.; Spettell, C.; Snyder, A.D.; McGowan-Stackewicz, V.; Kummer, P.J.; MacCoy, M.C.; Krakauer, R.S. Telemonitoring with case management for seniors with heart failure. Am. J. Manag. Care 2011, 17, 71–79. [Google Scholar]
- Koehler, F.; Winkler, S.; Schieber, M.; Sechtem, U.; Stangl, K.; Böhm, M.; Boll, H.; Baumann, G.; Honold, M.; Koehler, K.; et al. Impact of remote telemedical management on mortality and hospitalizations in ambulatory patients with chronic heart failure: The telemedical interventional monitoring in heart failure study. Circulation 2011, 123, 1873–1880. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, A.; Gregory, D.; Patel, A.R.; Levine, D.; Venesy, D.; Perry, K.; Delano, C.; Konstam, M.A. A Multicenter Randomized Controlled Evaluation of Automated Home Monitoring and Telephonic Disease Management in Patients Recently Hospitalized for Congestive Heart Failure: The SPAN-CHF II Trial. J. Card. Fail. 2010, 16, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Scherr, D.; Kastner, P.; Kollmann, A.; Hallas, A.; Auer, J.; Krappinger, H.; Schuchlenz, H.; Stark, G.; Grander, W.; Jakl, G.; et al. Effect of home-based telemonitoring using mobile phone technology on the out-come of heart failure patients after an episode of acute decompensation: Randomized controlled trial. J. Med. Internet Res. 2009, 11, e34. [Google Scholar] [CrossRef] [PubMed]
- Giordano, A.; Scalvini, S.; Zanelli, E.; Corrà, U.; Longobardi, G.L.; Ricci, V.; Baiardi, P.; Glisenti, F. Multicenter randomised trial on home-based telemanagement to prevent hospital readmission of patients with chronic heart failure. Int. J. Cardiol. 2009, 131, 192–199. [Google Scholar] [CrossRef]
- Dar, O.; Riley, J.; Chapman, C.; Dubrey, S.W.; Morris, S.; Rosen, S.D.; Roughton, M.; Cowie, M.R. A randomized trial of home telemonitoring in a typical elderly heart failure population in North West London: Results of the Home-HF study. Eur. J. Hear. Fail. 2009, 11, 319–325. [Google Scholar] [CrossRef]
- Woodend, A.K.; Sherrard, H.; Fraser, M.; Stuewe, L.; Cheung, T.; Struthers, C. Telehome monitoring in patients with cardiac disease who are at high risk of readmission. Hear. Lung 2008, 37, 36–45. [Google Scholar] [CrossRef]
- Soran, O.Z.; Piña, I.L.; Lamas, G.A.; Kelsey, S.F.; Selzer, F.; Pilotte, J.; Lave, J.R.; Feldman, A.M. A Randomized Clinical Trial of the Clinical Effects of Enhanced Heart Failure Monitoring Using a Computer-Based Telephonic Monitoring System in Older Minorities and Women. J. Card. Fail. 2008, 14, 711–717. [Google Scholar] [CrossRef]
- Kashem, A.; Droogan, M.T.; Santamore, W.P.; Wald, J.W.; Bove, A.A. Managing heart failure care using an internet-based tele-medicine system. J. Card. Fail. 2008, 14, 121–126. [Google Scholar] [CrossRef]
- Balk, A.H.; Davidse, W.; Van Dommelen, P.; Klaassen, E.; Caliskan, K.; Van Der Burgh, P.; Leenders, C.M. Tele-guidance of chronic heart failure patients enhances knowledge about the disease. A multi-centre, randomised controlled study. Eur. J. Hear. Fail. 2008, 10, 1136–1142. [Google Scholar] [CrossRef]
- Antonicelli, R.; Testarmata, P.; Spazzafumo, L.; Gagliardi, C.; Valentini, M.; Olivieri, F.; Bilo, G.; Parati, G. Impact of telemonitoring at home on the management of elderly patients with congestive heart failure. J. Telemed. Telecare 2008, 14, 300–305. [Google Scholar] [CrossRef]
- Goldberg, L.R.; Piette, J.D.; Walsh, M.N.; Frank, T.; Jaski, B.; Smith, A.L.; Rodriguez, R.; Mancini, D.M.; Hopton, L.; Orav, E.; et al. Randomized trial of a daily electronic home monitoring system in patients with advanced heart failure: The Weight Monitoring in Heart Failure (WHARF) trial. Am. Hear. J. 2003, 146, 705–712. [Google Scholar] [CrossRef]
- Benatar, D.; Bondmass, M.; Ghitelman, J.; Avitall, B. Outcomes of chronic heart failure. Arch. Intern. Med. 2003, 163, 347–352. [Google Scholar] [CrossRef] [PubMed]
- De Lusignan, S.; Wells, S.; Johnson, P.; Meredith, K.; Leatham, E. Compliance and effectiveness of 1 year’s home telemonitor-ing. The report of a pilot study of patients with chronic heart failure. Eur. J. Heart Fail. 2001, 3, 723–730. [Google Scholar] [CrossRef]
- Goldgrab, D.; Balakumaran, K.; Kim, M.J.; Tabtabai, S.R. Updates in heart failure 30-day readmission prevention. Hear. Fail. Rev. 2018, 24, 177–187. [Google Scholar] [CrossRef]
- Choi, H.-M.; Park, M.-S.; Youn, J.-C. Update on heart failure management and future directions. Korean J. Intern. Med. 2019, 34, 11–43. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardi-ology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013, 128, 1810–1852. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef]
- Pellicori, P.; Cleland, J.G.F.; Zhang, J.; Kallvikbacka-Bennett, A.; Urbinati, A.; Shah, P.; Kazmi, S.; Clark, A.L. Cardiac Dysfunction, Congestion and Loop Diuretics: Their Relationship to Prognosis in Heart Failure. Cardiovasc. Drugs Ther. 2016, 30, 599–609. [Google Scholar] [CrossRef]
- Cleland, J.; Clark, R.A.; Pellicori, P.; Inglis, S.C.; Rn, S.C.I. Caring for people with heart failure and many other medical problems through and beyond the COVID -19 pandemic: The advantages of universal access to home telemonitoring. Eur. J. Hear. Fail. 2020, 22, 995–998. [Google Scholar] [CrossRef]
- Shavelle, D.M.; Desai, A.S.; Abraham, W.T.; Bourge, R.C.; Raval, N.; Rathman, L.D.; Heywood, J.T.; Jermyn, R.A.; Pelzel, J.; Jonsson, O.T.; et al. Lower Rates of Heart Failure and All-Cause Hospitalizations During Pulmo-nary Artery Pressure-Guided Therapy for Ambulatory Heart Failure: One-Year Outcomes From the CardioMEMS Post-Approval Study. Circ. Heart Fail. 2020, 13, e006863. [Google Scholar] [CrossRef] [PubMed]
- Givertz, M.M.; Stevenson, L.W.; Costanzo, M.R.; Bourge, R.C.; Bauman, J.G.; Ginn, G.; Abraham, W.T. Pulmonary Artery Pressure-Guided Management of Patients With Heart Failure and Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2017, 70, 1875–1886. [Google Scholar] [CrossRef] [PubMed]
- Heywood, J.T.; Jermyn, R.; Shavelle, D.; Abraham, W.T.; Bhimaraj, A.; Bhatt, K.; Sheikh, F.; Eichorn, E.; Lamba, S.; Bharmi, R.; et al. Impact of Practice-Based Management of Pulmonary Artery Pressures in 2000 Patients Implanted With the CardioMEMS Sensor. Circulation 2017, 135, 1509–1517. [Google Scholar] [CrossRef] [PubMed]
- Angermann, C.E.; Assmus, B.; Anker, S.D.; Asselbergs, F.W.; Brachmann, J.; Brett, M.E.; Brugts, J.J.; Ertl, G.; Ginn, G.; Hilker, L.; et al. Pulmonary artery pressure-guided therapy in ambulatory patients with symp-tomatic heart failure: The CardioMEMS European Monitoring Study for Heart Failure (MEMS-HF). Eur. J. Heart Fail. 2020, 22, 1891–1901. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Acronym | Number of Patients | Age | Male (%) | NYHA III/IV (%) | Duration of Follow-Up | Background HF Therapy | ||
|---|---|---|---|---|---|---|---|---|---|
| Beta-Blockers | RAS-Inhibitors | MRAs | |||||||
| Rahimi et al. (2020) [15] | SUPPORT-HF 2 | 202 | 71.3 ± 11.1 | 71.3 | 40.5 | 6 months | NA | NA | NA |
| Gingele et al. (2019) [16] | TEHAF | 382 | 71.4 ± 11.2 | 59.2 | 42.7 | 12 months | 82.0 | 89.9 | NA |
| Krum et al. (2013) [17] | CHAT | 405 | 73.0 ± 10.5 | 63.1 | 41.4 | 12 months | 61.4 | 84.2 | 26.1 |
| Boyne et al. (2012) [18] | TEHAF | 382 | 71.4 ± 11.2 | 59.2 | 42.7 | 12 months | 81.1 | 89.0 | NA |
| Angermann et al. (2012) [19] | INH | 715 | 68.6 ± 12.2 | 70.6 | 39.9 | 6 months | 79.9 | 88.1 | 41.8 |
| Domingues et al. (2011) [20] | 111 | 63 ± 13 | 57.7 | 97.3 | 3 months | NA | NA | NA | |
| Baker et al. (2011) [21] | 605 | 60.7 ± 13.1 | 51.9 | 30.9 | 1 month | 81.3 | 82.1 | 27.4 | |
| Ferrante et al. (2010) [22] | DIAL | 1518 | 65.0 ± 13.3 | 70.8 | 49.4 | 12 months | 61.6 | 92.9 | 32.2 |
| Chaudhry et al. (2010) [23] | Tele-HF | 1653 | 61 (51–73) | 58.0 | 57.3 | 6 months | 79.2 | 66.9 | 32.8 |
| Mortara et al. (2009) [24] | HHH | 461 | 60 ± 12 | 85.0 | 39.9 | 12 months | 87 | 87 | NA |
| Bento and Brofman (2009) [25] | 40 | 57.5 ± 9.4 | 70.0 | 37.5 | 6 months | 85.0 | 75.0 | 62.5 | |
| Brandon et al. (2009) [26] | 20 | 60 (49–69) | 45.0 | 25.0 | 3 months | NA | NA | NA | |
| Wakefield et al. (2008) [27] | 148 | 69.3 ± 9.6 | 98.6 | 71.6 | 12 months | NA | NA | NA | |
| Sisk et al. (2006) [28] | 406 | 59.4 ± 13.7 | 53.7 | 59.1 | 12 months | 52.0 | NA | NA | |
| Riegel et al. (2006) [29] | 134 | 72.1 ± 11.0 | 46.3 | 81.3 | 6 months | 54.0 | 74.6 | 11.1 | |
| DeWalt et al. (2006) [30] | 123 | 62.5 ± 10.0 | 49.2 | 50.1 | 12 months | 63.3 | 73.3 | NA | |
| Dunagan et al. (2005) [31] | 151 | 70.0 ± 13.3 | 43.7 | 80.1 | 12 months | NA | 70.2 | NA | |
| Cleland et al. (2005) [32] | TEN-HMS | 426 | 67.2 ± 11.6 | 77.2 | 34.0 | 8 months | 80.9 | 81.0 | 49.1 |
| Tsuyuki et al. (2004) [33] | 276 | 71.5 ± 12 | 58.0 | 26.4 | 6 months | 42.8 | 84.8 | 13.4 | |
| Galbreath et al. (2004) [34] | 1069 | 70.9 ± 10.3 | 71 | 24 | 18 months | 47 | 73 | NA | |
| DeBusk et al. (2004) [35] | 462 | 72 ± 11 | 51.1 | 50.1 | 12 months | NA | NA | NA | |
| Capomolla et al. (2004) [36] | 133 | 57 ± 10 | 88.0 | 33.1 | 12 months | NA | 84.2 | 21.1 | |
| Laramee et al. (2003) [37] | 287 | 70.7 ± 11.8 | 54.4 | 35.9 | 3 months | NA | NA | NA | |
| Riegel et al. (2002) [38] | 358 | 73.9 ± 12.4 | 48.9 | 96.9 | 6 months | 16.9 | 53.6 | NA | |
| McDonald et al. (2002) [39] | 98 | 70.8 ± 10.5 | 66.3 | 2.3 ± 0.6 | 3 months | NA | 61.2 | NA | |
| Krumholz et al. (2002) [40] | 88 | 73.8 ± 9.5 | 56.8 | NA | 12 months | 40.9 | 59.1 | NA | |
| Kasper et al. (2002) [41] | 200 | 61.9 ± 14.3 | 60.5 | 58.5 | 6 months | 39.0 | 94.5 | NA | |
| Jerant et al. (2001) [42] | 37 | 70.1 ± 12.1 | 45.9 | 35.1 | 12 months | 37.8 | 67.6 | 27.0 | |
| Blue et al. (2001) [43] | 165 | 75.5 ± 8.3 | 57.6 | 77.0 | 12 months | 4.2 | 71.5 | 5.5 | |
| Barth (2001) [44] | 34 | 75.2 ± 8.4 | 47.1 | NA | 6 months | NA | NA | NA | |
| Gattis et al. (1999) [45] | PHARMA | 181 | 67.2 (55.0–74.5) | 68.0 | 33.1 | 6 months | NA | 77.9 | NA |
| Author (Year) | Number of Patients | All-Cause Mortality | All-Cause Hospitalization | HF-Related Hospitalization | Quality of Life | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Events | OR (95% CI) | Number of Events | OR (95% CI) | Number of Events | OR (95% CI) | |||||||
| STS | UC | STS | UC | STS | UC | STS | UC | |||||
| Rahimi et al. (2020) [15] | 101 | 101 | 13 | 6 | 2.17 (0.86–5.48) | 40 | 29 | 1.63 (0.90–2.93) | 13 | 13 | 1.00 (0.44–2.28) | MLWHFQ STS −0.30; UC −0.66 p = 0.63 |
| Gingele et al. (2019) [16] | 197 | 185 | NA | NA | NA | NA | NA | NA | NA | NA | NA | EQ-5D STS +0.01; UC +0.02 p = 0.83 |
| Krum et al. (2013) [17] | 188 | 217 | 17 | 16 | 1.23 (0.64–2.36) | 74 | 114 | 0.59 (0.39–0.87) | 23 | 35 | 0.72 (0.41–1.28) | NA |
| Boyne et al. (2012) [18] | 197 | 185 | 19 | 12 | 1.49 (0.74–2.98) | 48 | 35 | 1.38 (0.84–1.57) | 18 | 25 | 0.64 (0.34–1.22) | NA |
| Angermann et al. (2012) [19] | 352 | 363 | 32 | 52 | 0.63 (0.42–0.96) | 119 | 112 | 1.14 (0.84–1.57) | 36 | 46 | 0.79 (0.49–1.25) | SF-36—physical health STS +2.8; UC +1.3 p = 0.03 SF-36—physical functioning STS +5.9; UC +1.8 p = 0.03 |
| Domingues et al. (2011) [20] | 57 | 63 | 8 | 13 | 0.68 (0.30–1.52) | 20 | 23 | 0.94 (0.45–1.99) | NA | NA | NA | |
| Baker et al. (2011) [21] | 303 | 302 | 0 | 2 | 0.20 (0.01–4.13) | NA | NA | NA | NA | NA | NA | ICICE HFSS STS +6.7; UC −0.1 p < 0.01 |
| Ferrante et al. (2010) [22] | 760 | 758 | 116 | 122 | 0.95 (0.75–1.20) | 261 | 296 | 0.85 (0.66–1.01) | 128 | 169 | 0.71 (0.55–0.91) | MLWHFQ STS −35.0; UC −30.6 p < 0.01 |
| Chaudhry et al. (2010) [23] | 826 | 827 | 92 | 94 | 0.98 (0.75–1.28) | 407 | 392 | 1.08 (0.89–1.31) | 227 | 223 | 1.04 (0.84–1.30) | NA |
| Mortara et al. (2009) [24] | 94 | 160 | 7 | 9 | 1.32 (0.51–3.44) | NA | NA | NA | 17 | 28 | 1.04 (0.54–2.02) | NA |
| Bento and Brofman (2009) [25] | 20 | 20 | 0 | 1 | 0.33 (0.01–7.72) | NA | NA | NA | NA | NA | NA | NA |
| Brandon et al. (2009) [26] | 10 | 10 | NA | NA | NA | NA | NA | NA | NA | NA | NA | MLWHFQ STS −18.7; UC +6.6 p = 0.03 |
| Wakefield et al. (2008) [27] | 99 | 49 | 25 | 11 | 1.12 (0.60–2.09) | 41 | 29 | 0.49 (0.24–0.98) | 51 | 29 | 0.73 (0.37–1.46) | MLWHFQ STS −16.9; UC −4.0 p = NS |
| Sisk et al. (2006) [28] | 203 | 203 | 22 | 22 | 1.00 (0.57–1.75) | 62 | 74 | 0.77 (0.51–1.16) | 18 | 29 | 0.58 (0.31–1.09) | MLWHFQ STS 38.6; UC 47.3 Difference −7.3 (−12.1–−2.6) SF-36 physical health STS 39.9; UC 36.3 Difference 3.2 (1.0–5.3) |
| Riegel et al. (2006) [29] | 70 | 65 | 6 | 8 | 0.70 (0.26–1.90) | 39 | 37 | 0.95 (0.48–1.88) | 21 | 22 | 0.84 (0.41–1.73) | MLWHFQ STS −40.6; UC −43.2 EQ-5D STS +0.13; UC +0.12 PHQ-9 STS −7.3; UC −6.6 |
| DeWalt et al. (2006) [30] | 62 | 65 | 3 | 4 | 0.79 (0.18–3.37) | NA | NA | NA | 21 | 25 | 0.82 (0.40–1.69) | MLWHFQ STS −1; UC −5 p = 0.59 |
| Dunagan et al. (2005) [31] | 76 | 75 | 6 | 5 | 1.18 (0.38–3.71) | 41 | 57 | 0.37 (0.18–0.74) | 23 | 35 | 0.50 (0.25–0.97) | NA |
| Cleland et al. (2005) [32] | 173 | 85 | 27 | 20 | 0.66 (0.40–1.11) | 85 | 46 | 0.82 (0.49–1.38) | 34 | 24 | 0.62 (0.34–1.14) | NA |
| Tsuyuki et al. (2004) [33] | 140 | 136 | 16 | 12 | 1.30 (0.64–2.64) | 59 | 51 | 1.21 (0.75–1.97) | 37 | 38 | 0.93 (0.55–1.57) | NA |
| Galbreath et al. (2004) [34] | 710 | 359 | 54 | 39 | 0.70 (0.47–1.04) | NA | NA | NA | NA | NA | NA | SF-36—general health STS −0.4; UC +0.2 p = 0.87 |
| DeBusk et al. (2004) [35] | 228 | 234 | 21 | 29 | 0.74 (0.44–1.26) | 116 | 117 | 1.04 (0.72–1.49) | 38 | 43 | 0.89 (0.55–1.57) | NA |
| Capomolla et al. (2004) [36] | 67 | 66 | 5 | 7 | 0.70 (0.24–2.11) | 17 | 58 | 0.05 (0.02–0.12) | NA | |||
| Laramee et al. (2003) [37] | 141 | 146 | 13 | 15 | 0.90 (0.44–1.82) | 49 | 46 | 1.16 (0.71–1.89) | 18 | 21 | 0.87 (0.44–1.71) | NA |
| Riegel et al. (2002) [38] | 130 | 228 | 16 | 32 | 0.88 (0.50–1.54) | 56 | 114 | 0.76 (0.49–1.17) | 23 | 63 | 0.56 (0.33–0.96) | NA |
| McDonald et al. (2002) [39] | 51 | 47 | 3 | 1 | 2.76 (0.30–25.67) | NA | NA | NA | 1 | 11 | 0.07 (0.01–0.53) | NA |
| Krumholz et al. (2002) [40] | 44 | 44 | 9 | 13 | 0.69 (0.33–1.45) | NA | NA | NA | 12 | 21 | 0.41 (0.17–1.00) | NA |
| Kasper et al. (2002) [41] | 102 | 98 | 7 | 13 | 0.52 (0.22–1.24) | NA | NA | NA | 26 | 35 | 0.62 (0.34–1.13) | MLWHFQ STS −28.3; UC −25.7 p < 0.01 |
| Jerant et al. (2001) [42] | 12 | 12 | 1 | 0 | 3.00 (0.13–67.06) | NA | NA | NA | 1 | 4 | 0.18 (0.02–1.95) | NA |
| Blue et al. (2001) [43] | 84 | 81 | 25 | 25 | 0.96 (0.61–1.53) | NA | NA | NA | 12 | 26 | 0.35 (0.16–0.76) | NA |
| Barth (2001) [44] | 17 | 17 | 0 | 0 | Not estimable | NA | NA | NA | 0 | 0 | Not estimable | MLWHFQ STS −8.2; UC +0.0 p < 0.01 |
| Gattis et al. (1999) [45] | 90 | 91 | 3 | 5 | 0.61 (0.15–2.46) | 17 | 30 | 0.47 (0.24–0.94) | 1 | 11 | 0.08 (0.01–0.65) | NA |
| Author (Year) | Study Acronym | Intervention | Number of Patients | Age | Male (%) | NYHA III/IV (%) | Duration of Follow-Up | Background HF Therapy | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Beta-Blockers | RAS-Inhibitors | MRAs | ||||||||
| Haynes et al. (2020) [47] | BEAT-HF | BP, BW, HR, S and S | 288 | 72 (61–83) | 52.7 | NA | 6 months | NA | NA | NA |
| Ding et al. (2020) [48] | ITEC-CHF | BW | 184 | 70.1 ± 12.3 | 76.6 | 2.1 ± 0.6 | 6 months | 87.5 | 77.1 | 57.6 |
| Pekmezaris et al. (2019) [49] | BP, BW, HR, SpO2 | 104 | 59.9 ± 15.1 | 58.7 | 70.2 | 3 months | NA | NA | NA | |
| Park et al. (2019) [50] | BP, BW | 58 | 59.1 ± 13.6 | 67.2 | NA | 1 month | NA | NA | NA | |
| Koehler et al. (2018) [51] | TIM-HF2 | BP, BW, ECG, HR, HS, SpO2 | 1538 | 70.0 ± 10.5 | 69.6 | 47.5 | 12 months | 91.9 | 82.5 | 55.0 |
| Ong et al. (2016) [52] | BEAT-HF | BP, BW, HR, S and S | 1437 | 73.5 (62.5–83.0) | 53.8 | 74.9 | 6 months | 74.7 | 55.6 | 19.3 |
| Vuorinen et al. (2014) [53] | BP, BW, S and S | 94 | 58.1 ± 11.8 | 83.0 | 61.7 | 6 months | NA | NA | NA | |
| Villani (2014) et al. [54] | ICARLOS | BP, BW, HR | 80 | 72 ± 3 | 73.8 | 3.0 ± 0.5 | 12 months | NA | NA | NA |
| Blum and Gotlieb (2014) [55] | MCCD | BP, BW, HR | 203 | 72.5 ± 9.0 | 71.0 | 85.5 | 48 months | 68.0 | 66.0 | NA |
| Seto et al. (2012) [56] | BP, BW, ECG | 100 | 53.7 ± 13.7 | 79.0 | 46.0 | 6 months | 98.0 | 97.0 | 52.0 | |
| Pekmezaris et al. (2012) [57] | BP, Stethoscope | 168 | 82.0 ± 7.0 | 38.1 | 20.2 | 3 months | NA | NA | NA | |
| Lyngå et al. (2012) [58] | WISH | BW | 319 | 73.6 ± 10.1 | 74.9 | 100.0 | 12 months | 92.5 | 96.2 | 42.6 |
| Dendale et al. (2012) [59] | TEMA-HF 1 | BP, BW, HR | 160 | 75.8 ± 9.7 | 65.0 | 3.0 ± 0.5 | 6 months | NA | NA | NA |
| Wade et al. (2011) [60] | BP, BW | 316 | 76.7 ± 7.0 | 52.2 | NA | 6 months | 81.6 | 72.0 | NA | |
| Koehler et al. (2011) [61] | TIM-HF | BP, BW, ECG | 710 | 66.9 ± 10.6 | 81.3 | 49.9 | 24 months | 92.5 | 95.4 | 64.2 |
| Weintraub et al. (2010) [62] | SPAN-CHF II | BP, BW, HR | 188 | 69.0 ± 13.5 | 66.0 | 52.7 | 3 months | 88.3 | 85.6 | 20.7 |
| Scherr et al. (2009) [63] | BP, BW, HR | 108 | 66 (62–72) | 70.8 | 87.0 | 6 months | 82.4 | 100.0 | 40.7 | |
| Mortara et al. (2009) [24] | HHH | BP, BW, HR, S and S | 461 | 60 ± 12 | 85.0 | 39.9 | 12 months | 87 | 87 | NA |
| Giordano et al. (2009) [64] | ECG | 460 | 57.0 ± 10.0 | 85.0 | 40.4 | 12 months | 72.4 | 94.3 | 62.0 | |
| Dar et al. (2009) [65] | Home-HF | BP, BW, SpO2, S and S | 182 | 71.0 ± 11,6 | 66.5 | NA | 6 months | 56.0 | 87.9 | 40.7 |
| Woodend et al. (2008) [66] | BP, BW, ECG | 121 | 66.5 ± 12.0 | 72.0 | 62.1 | 12 months | NA | NA | NA | |
| Soran et al. (2008) [67] | BW, S and S | 315 | 76.5 ± 7.0 | 35.3 | 41.6 | 6 months | 80.3 | 97.4 | NA | |
| Kashem et al. (2008) [68] | BP, BW, HR, S and S | 48 | 53.5 ± 10.5 | 74.0 | 57.5 | 12 months | NA | NA | NA | |
| Balk et al. (2008) [69] | BP, BW | 214 | 66 (33–87) | 70.1 | 51.9 | 8 months | 80.0 | 95.3 | 47.2 | |
| Antonicelli et al. (2008) [70] | BP, BW, ECG, HR, UO | 57 | 78.0 ± 7.0 | 61.4 | 42.1 | 12 months | NA | NA | NA | |
| Cleland et al. (2005) [32] | TEN-HMS | BP, BW, ECG, HR | 426 | 67.2 ± 11.6 | 77.2 | 34.0 | 8 months | 80.9 | 81.0 | 49.1 |
| Goldberg et al. (2003) [71] | WHARF | BW | 280 | 59.1 ± 15.3 | 67.5 | 100.0 | 6 months | 37.5 | 89.6 | NA |
| Benatar et al. (2003) [72] | BP, BW, HR, SpO2 | 216 | 63.1 ± 12.9 | 37.0 | 3.1 ± 0.3 | 12 months | 53.2 | 83.8 | NA | |
| Jerant et al. (2001) [42] | BW, Stethoscope, S and S | 37 | 70.1 ± 12.1 | 45.9 | 35.1 | 12 months | 37.8 | 67.6 | 27.0 | |
| de Lusignan et al. (2001) [73] | BP, BW, HR | 20 | 75.2 | NA | 1.8 (1–4) | 12 months | NA | NA | NA | |
| Author (Year) | Number of Patients | All-Cause Mortality | All-Cause Hospitalization | HF-Related Hospitalization | Quality of Life | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Events | OR (95% CI) | Number of Events | OR (95% CI) | Number of Events | OR (95% CI) | |||||||
| TM | UC | TM | UC | TM | UC | TM | UC | |||||
| Haynes et al. (2020) [47] | 292 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
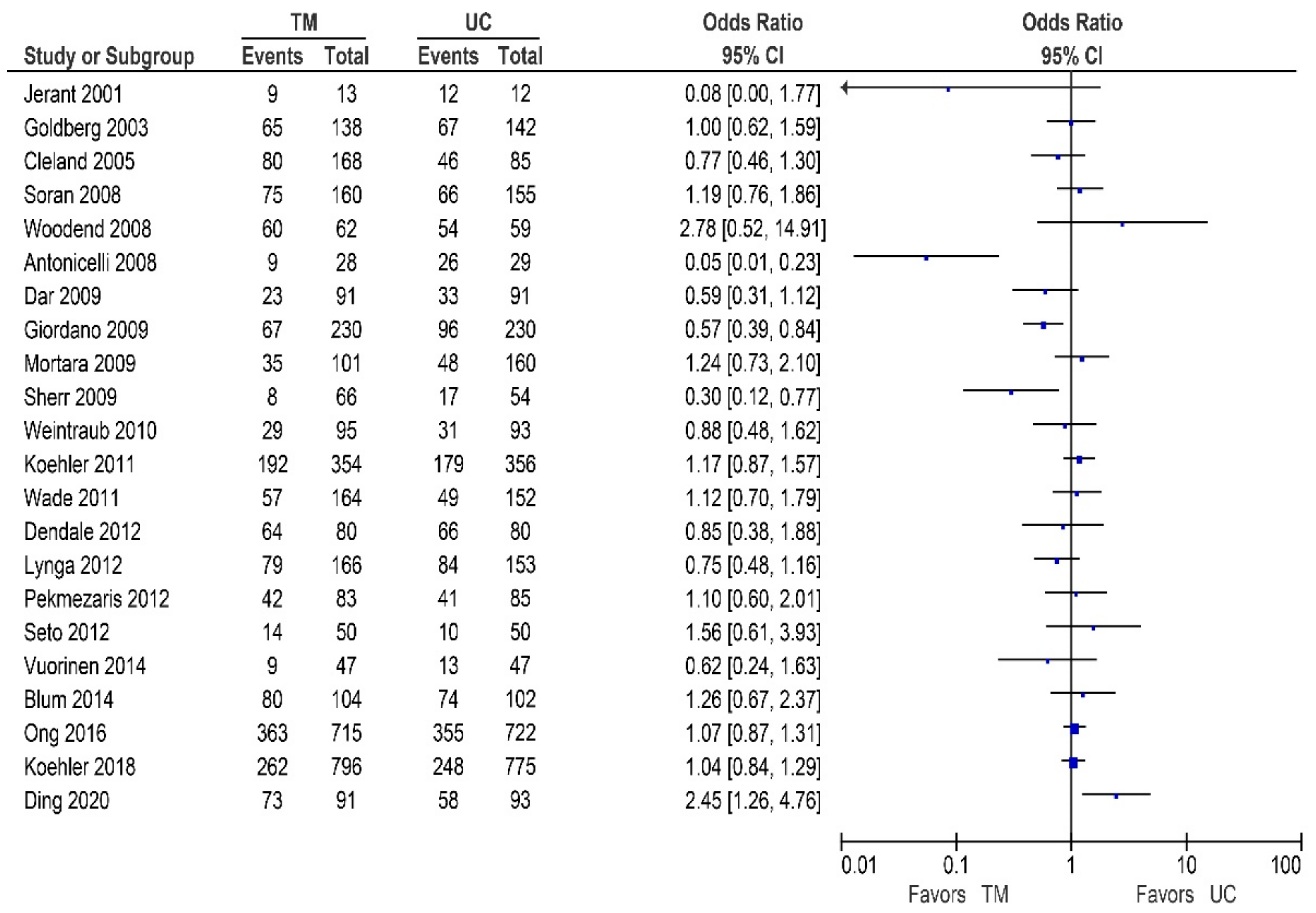
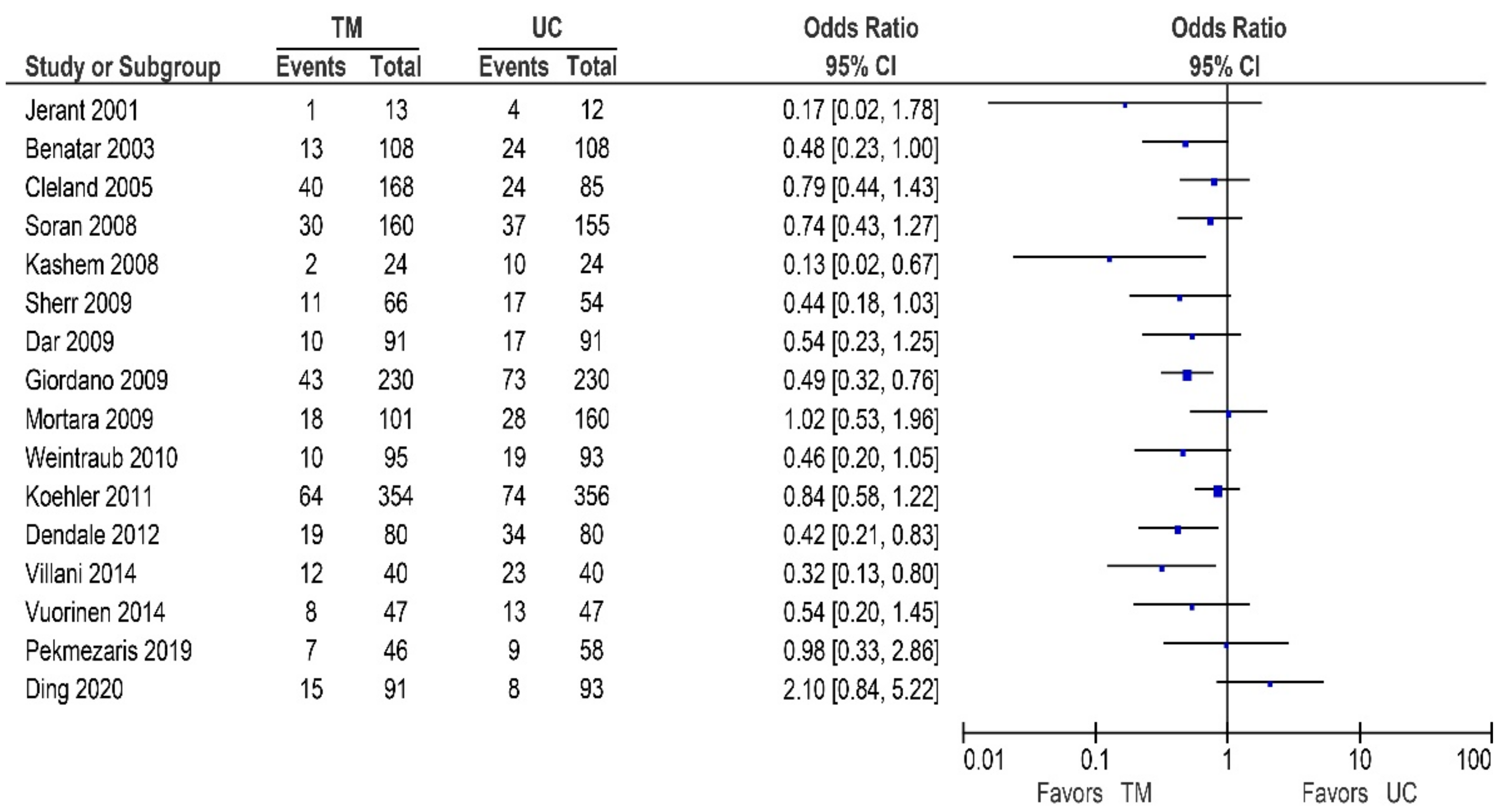
| Ding et al. (2020) [48] | 91 | 93 | 2 | 1 | 2.07 (0.18–23.21) | 73 | 58 | 2.45 (1.26–4.76) | 15 | 8 | 2.10 (0.84–5.22) | EQ-5D TM +4.05; UC +1.10 p = 0.13 |
| Pekmezaris et al. (2019) [49] | 46 | 58 | NA | NA | NA | NA | NA | NA | 7 | 9 | 0.98 (0.33–2.86) | MLWHFQ TM −26.4; UC −32.1 p = 0.50 PHQ-9 TM −2.2; UC −3.0 p = 0.43 |
| Park et al. (2019) [50] | 60 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Koehler et al. (2018) [51] | 796 | 775 | 61 | 89 | 0.64 (0.45–0.90) | 262 | 248 | 1.04 (0.84–1.29) | NA | NA | NA | MLWHFQ TM −3.08; UC −1.98 p = 0.26 |
| Ong et al. (2016) [52] | 715 | 722 | 92 | 106 | 0.86 (0.64–1.16) | 363 | 355 | 1.07 (0.87–1.31) | NA | NA | NA | MLWHFQ TM −32.6; UC −28.5 p = 0.02 |
| Vuorinen et al. (2014) [53] | 47 | 47 | 0 | 0 | Not estimable | 9 | 13 | 0.62 (0.24–1.63) | 8 | 13 | 0.54 (0.20–1.45) | NA |
| Villani et al. (2014) [54] | 40 | 40 | 5 | 9 | 0.49 (0.15–1.63) | NA | NA | NA | 12 | 23 | 0.32 (0.13–0.80) | PHQ-9 TM −2.8; UC +3.8 p < 0.01 |
| Blum and Gotlieb (2014) [55] | 104 | 102 | 49 | 45 | 1.13 (0.65–1.95) | 80 | 74 | 1.26 (0.67–2.37) | NA | NA | NA | SF-36—physical health TM +1; UC +3 p = NS SF-36—mental health TM +3; UC +6 p = NS MLWFHQ TM −18; UC −19 p = NS |
| Seto et al. (2012) [56] | 50 | 50 | 3 | 0 | 7.44 (0.37–147.92) | 14 | 10 | 1.56 (0.61–3.93) | NA | NA | NA | MLWHFQ TM −8.9; UC −0.5 p = 0.05 |
| Pekmezaris et al. (2012) [57] | 83 | 85 | NA | NA | NA | 42 | 41 | 1.10 (0.60–2.01) | NA | NA | NA | NA |
| Lyngå et al. (2012) [58] | 166 | 153 | 5 | 8 | 0.56 (0.18–1.76) | 79 | 84 | 0.75 (0.48–1.16) | NA | NA | NA | NA |
| Dendale et al. (2012) [59] | 80 | 80 | 4 | 14 | 0.25 (0.08–0.79) | 64 | 66 | 0.85 (0.38–1.88) | 19 | 34 | 0.42 (0.21–0.83) | NA |
| Wade et al. (2011) [60] | 164 | 152 | 6 | 6 | 0.92 (0.29–2.93) | 57 | 49 | 1.12 (0.70–1.79) | NA | NA | NA | SF-36—physical health TM −0.17; UC +1.67 p = 0.13 SF-36—mental health TM −0.75; UC +0.04 p = 0.34 |
| Koehler et al. (2011) [61] | 354 | 356 | 54 | 55 | 0.99 (0.65–1.48) | 192 | 179 | 1.17 (0.87–1.57) | 64 | 74 | 0.84 (0.58–1.22) | SF-36—physical health TM 54.3; UC 49.9 p < 0.05 PHQ-9 Similar improvement between groups p > 0.05 |
| Weintraub et al. (2010) [62] | 95 | 93 | 1 | 4 | 0.24 (0.03–2.16) | 29 | 31 | 0.88 (0.48–1.62) | 10 | 19 | 0.46 (0.20–1.05) | NA |
| Scherr et al. (2009) [63] | 66 | 54 | 0 | 1 | 0.27 (0.01–6.72) | 8 | 17 | 0.30 (0.12–0.77) | 11 | 17 | 0.44 (0.18–1.03) | NA |
| Mortara et al. (2009) [24] | 101 | 160 | 8 | 9 | 1.44 (0.54–3.87) | 35 | 48 | 1.24 (0.73–2.10) | 18 | 28 | 1.02 (0.53–1.96) | NA |
| Giordano et al. (2009) [62] | 138 | 142 | 11 | 26 | 0.39 (0.18–0.82) | 67 | 96 | 0.57 (0.39–0.84) | 43 | 73 | 0.49 (0.32–0.76) | NA |
| Dar et al. (2009) [65] | 91 | 91 | 6 | 5 | 1.21 (0.36–4.13) | 23 | 33 | 0.59 (0.31–1.12) | 10 | 17 | 0.54 (0.23–1.25) | MLWHFQ No difference between groups p = 0.60 EQ-5D No difference between groups p = 0.50 |
| Woodend et al. (2008) [66] | 62 | 59 | 5 | 4 | 1.21 (0.31–4.73) | 60 | 54 | 2.78 (0.52–14.91) | NA | NA | NA | MLWHFQ No difference between groups p = 0.18 |
| Soran et al. (2008) [67] | 160 | 155 | 11 | 17 | 0.60 (0.27–1.32) | 75 | 66 | 1.19 (0.76–1.86) | 30 | 37 | 0.74 (0.43–1.27) | SF-12—physical health TM 32.3; UC 33.0 p = 0.51 SF-12—mental health TM 50.2; UC 51.1 p = 0.51 KCCQ—overall summary score TM 60.2; UC 59.9 p = 0.92 |
| Kashem et al. (2008) [68] | 24 | 24 | 1 | 1 | 1.00 (0.06–16.97) | NA | NA | NA | 2 | 10 | 0.13 (0.02–0.67) | |
| Balk et al. (2008) [69] | 101 | 113 | 9 | 8 | 1.28 (0.48–3.46) | NA | NA | NA | NA | NA | NA | Dutch Heart Failure Knowledge Score No difference between groups p = 0.61 |
| Antonicelli et al. (2008) [70] | 28 | 29 | 3 | 5 | 0.58 (0.12–2.68) | 9 | 26 | 0.05 (0.01–0.23) | NA | NA | NA | SF-36—health perception TM + 31; UC + 8 p = 0.61 |
| Cleland et al. (2005) [32] | 168 | 85 | 28 | 20 | 0.65 (0.34–1.24) | 80 | 46 | 0.77 (0.46–1.30) | 40 | 24 | 0.79 (0.44–1.43) | |
| Goldberg et al. (2003) [71] | 138 | 142 | 11 | 26 | 0.39 (0.18–0.82) | 65 | 67 | 1.00 (0.62–1.59) | NA | NA | NA | SF-36—physical health TM + 6.7; UC + 4.3 p = 0.15 SF-36—mental health TM + 5.9; UC + 5.2 p = 0.73 |
| Benatar et al. (2003) [72] | 108 | 108 | NA | NA | NA | NA | NA | NA | 13 | 24 | 0.48 (0.23–1.00) | MLWHFQ TM − 21.5; UC − 26.3 p = 0.98 |
| Jerant et al. (2001) [42] | 13 | 12 | 0 | 0 | Not estimable | 9 | 12 | 0.08 (0.00–1.77) | 1 | 4 | 0.17 (0.02–1.78) | |
| de Lusignan et al. (2001) [73] | 10 | 10 | 2 | 3 | 0.58 (0.07–4.56) | NA | NA | NA | NA | NA | NA | GHQ RM − 4; UC − 7 p = NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veenis, J.F.; Radhoe, S.P.; Hooijmans, P.; Brugts, J.J. Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go? Sensors 2021, 21, 887. https://doi.org/10.3390/s21030887
Veenis JF, Radhoe SP, Hooijmans P, Brugts JJ. Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go? Sensors. 2021; 21(3):887. https://doi.org/10.3390/s21030887
Chicago/Turabian StyleVeenis, Jesse F., Sumant P. Radhoe, Petra Hooijmans, and Jasper J. Brugts. 2021. "Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go?" Sensors 21, no. 3: 887. https://doi.org/10.3390/s21030887
APA StyleVeenis, J. F., Radhoe, S. P., Hooijmans, P., & Brugts, J. J. (2021). Remote Monitoring in Chronic Heart Failure Patients: Is Non-Invasive Remote Monitoring the Way to Go? Sensors, 21(3), 887. https://doi.org/10.3390/s21030887