Enabling the Internet of Mobile Crowdsourcing Health Things: A Mobile Fog Computing, Blockchain and IoT Based Continuous Glucose Monitoring System for Diabetes Mellitus Research and Care




Abstract
1. Introduction
- Type-1 DM (DM1): it is an autoimmune process that leads to remarkably diminished insulin levels.
- Type-2 DM (DM2): it arises from the compromised function of insulin-producing cells in the pancreas and insulin resistance in the peripheral tissues.
- Gestational Diabetes Mellitus (GDM): it occurs on pregnant women that suffer from above-normal blood glucose levels.
- A description of an IoT CGM-based system able to monitor glucose concentration values remotely and quickly inform patients and/or their care givers of a dangerous situation.
- The design of a system able to provide fast warnings by using fog computing gateways when the user is located in specific scenarios (e.g., inside the patient’s home, in a hospital or in a nursing home).
- A description of a mHealth blockchain-based decentralized architecture that does not depend on any central authority.
- The proposal of a data crowdsourcing mechanism that encourages collaboration by rewarding patients.
- The evaluation of the proposed architecture to assess the performance of the described decentralized storage and blockchain.
2. Related Work
2.1. CGM Applications
2.2. Fog Computing, Blockchain and Crowdsourcing for Healthcare Applications
- Novel IoT healthcare real-time applications can be provided thanks to decreasing latency.The fog allows for sharing computational and storage resources, which can be harnessed by distributed wireless sensor networks that can be deployed in hospitals or in other healthcare facilities.
- The fog can also connect multiple physical environments that are far from each other, easing device and user interaction and thus facilitating the development of new potential healthcare services.
- Since the fog can be scaled easily, it provides flexibility and ease of growth to large deployments.
3. Design of the System
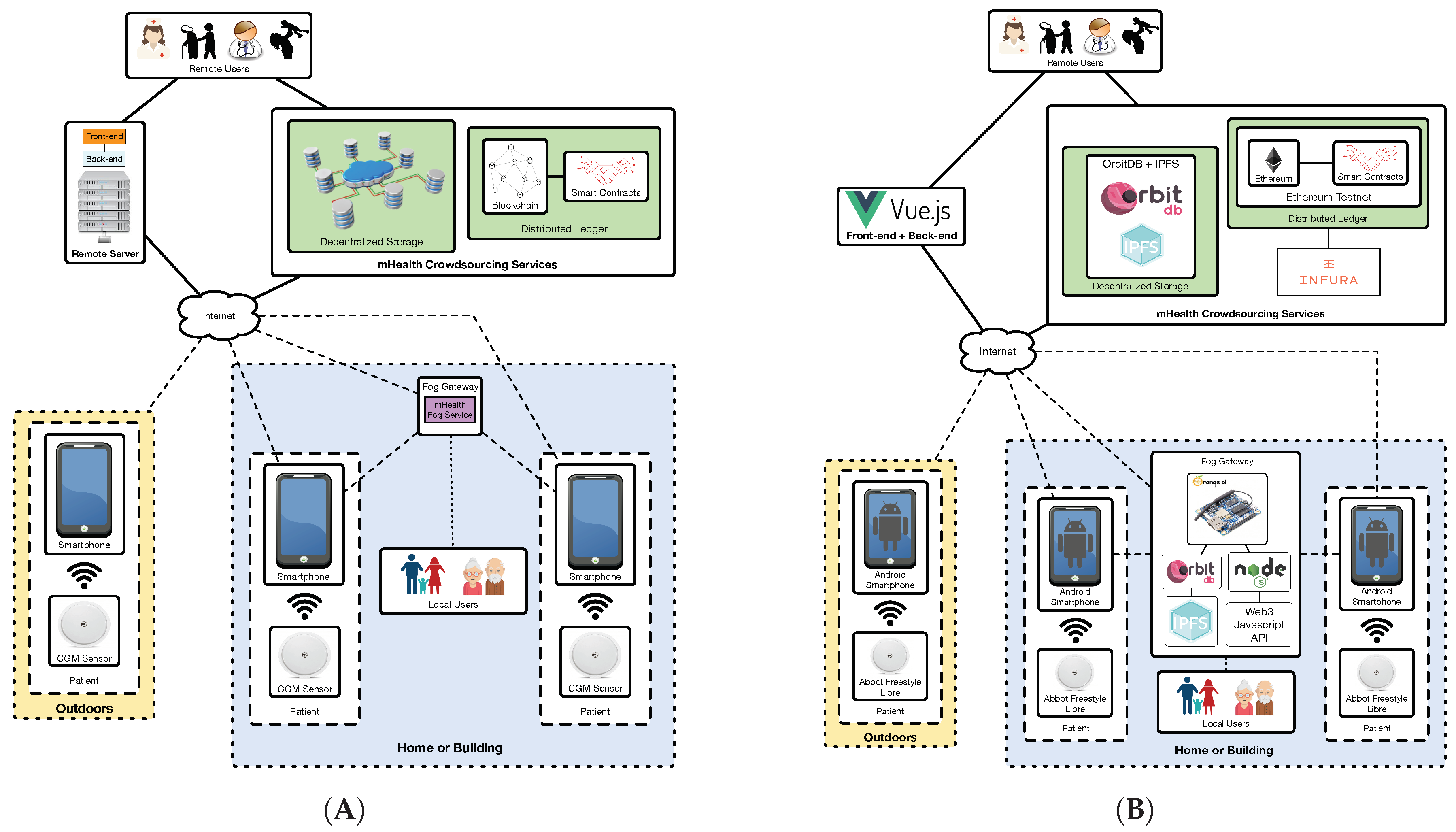
3.1. Communications Architecture
- In an area covered by a fog computing gateway. In this scenario the smartphone joins the network created by the fog gateway and sends to it the data collected from the CGM sensor. This may be the case of homes and certain buildings (e.g., hospitals, nursing homes), where fog gateway infrastructure can be easily deployed and managed.
- Out of range of the deployed fog computing gateways. Patients may move to certain areas where fog gateways are not in range (e.g., outdoors, in certain areas of a home/building). In such scenarios the smartphone should detect the lack of fog gateway connectivity and send the collected data directly to remote servers or services on the Internet.
- Remote server: it is essentially a front-end that provides a web interface to remote users in order to allow them to access the stored information in a user-friendly way. This server also runs a back-end service that is responsible for sending notifications to remote users through SMS or instant messaging services.
- Decentralized storage system: it is able to provide redundancy, cyber-attack protection and DApp support to the stored information. This storage system is able to replicate the collected information and distribute it automatically among multiple nodes. In this way, although one storage node is not available (e.g., due to maintenance, to a malfunction or to a cyber-attack), the information can be accessed through other nodes.
- Decentralized ledger: it is included to provide transparency and decentralization, and to enhance data authenticity and security. Specifically, a blockchain can be used to preserve user anonymity and transaction privacy, so that patient data can remain private to non-authorized parties [56]. Moreover, transparency is provided to the authorized third-parties that access the stored information, which allows them to monitor and analyze it in order to determine whether it has been tampered [57]. Furthermore, a blockchain provides decentralization by distributing the data among peers and thus avoiding the involvement of middlemen [58]. Regarding data authenticity, a blockchain can be used to provide accountability, which is essential to trust the information collected from the patients. With respect to smart contracts [37], they are able to automate event triggering by monitoring when certain requirements are fulfilled. For instance, a smart contract may be used together with an oracle (i.e., an external agent that retrieves and validates certain real-world information that is later sent to a blockchain) to detect that a user is going to run out of sensors and then automate the purchase of new ones. The designed decentralized ledger also includes a cryptocurrency-based incentive mechanism (whose functioning is detailed in the next subsection) to motivate patients to share their data in the crowdsourcing platform.
3.2. Data Crowdsourcing Incentive Mechanism
 ) was created on the Ethereum blockchain. GlucoCoin requires creating a digital wallet for every participant and implements all the software operations needed by a cryptocurrency, which essentially involve getting the balance from a user and sending an amount from one user to another.
) was created on the Ethereum blockchain. GlucoCoin requires creating a digital wallet for every participant and implements all the software operations needed by a cryptocurrency, which essentially involve getting the balance from a user and sending an amount from one user to another.4. Implementation
4.1. Implemented Architecture
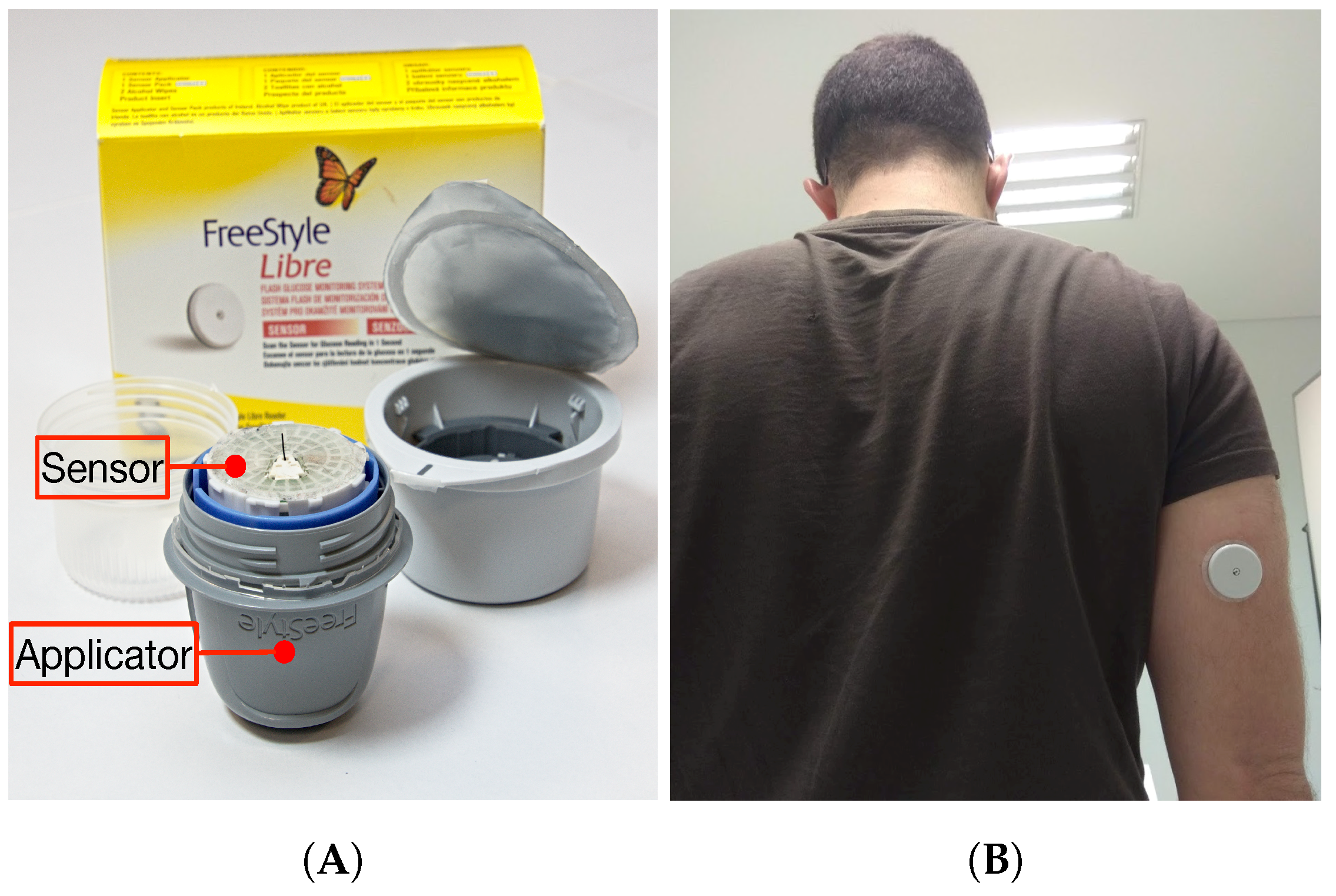
4.1.1. CGM Sensor
- Pointer fields: bytes 27 and 28 store, respectively, the position where the last trend and historic values were written.
- Trend value fields: they are 16 fields of 6 bytes between byte 29 and byte 124 that store the latest trend measurements. Such trend measurements are obtained every minute for the last 16 min. In the position that is indicated by the Trend Pointer it is placed the current measurement, while the average of the other 15 measures is actually the last historic value. Note that the collected data are raw values that need to be calibrated after adhering sensor and initializing it with the sensor reader, therefore a researcher that develops a non-official NFC-enabled app to read the sensor should calibrate it at least once with an accurate glucose reader (or compare the collected values with the ones actually shown by Abbot’s reader).
- Historic values: they are 32 values of 6 bytes that are located after the Trend values (from byte 125 to byte 316) and that represent the glucose concentration values obtained every 15 min for the last 8 h.
- Activity time: there are two bytes (317 and 318) that indicate the number of minutes since the sensor started to take measurements (i.e., since it was initialized with the official Abbot Freestyle reader), so they allow for obtaining the expiration date of the sensor.
4.1.2. Decentralized Storage
4.1.3. Smartphone App
4.1.4. Back-End and Front-End
4.1.5. Distributed Ledger
4.1.6. Fog Gateway
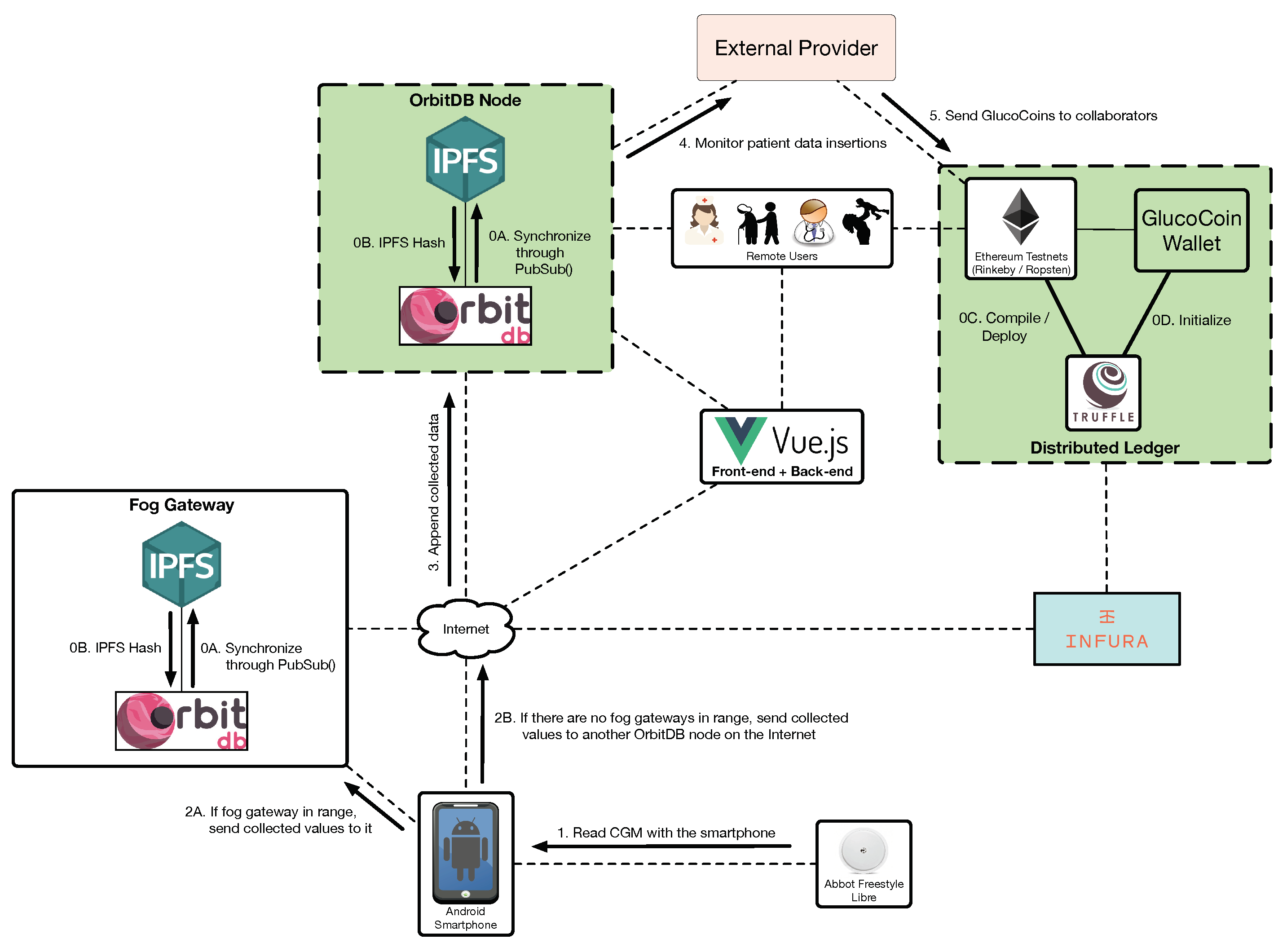
- OrbitDB and IPFS. Every fog gateway is actually an autonomous OrbitDB node that runs on IPFS and that synchronizes periodically with the other OrbitDB nodes deployed on the Internet.
- Node.js [83]. It is needed for executing JavaScript code outside of a browser, thus easing the interaction with Web3 and OrbitDB. In the case of Web3, in practice, the proposed implementation runs a Node.js instance that performs calls to the Web3 API in order to exchange requests with Infura, which interacts with Ethereum.
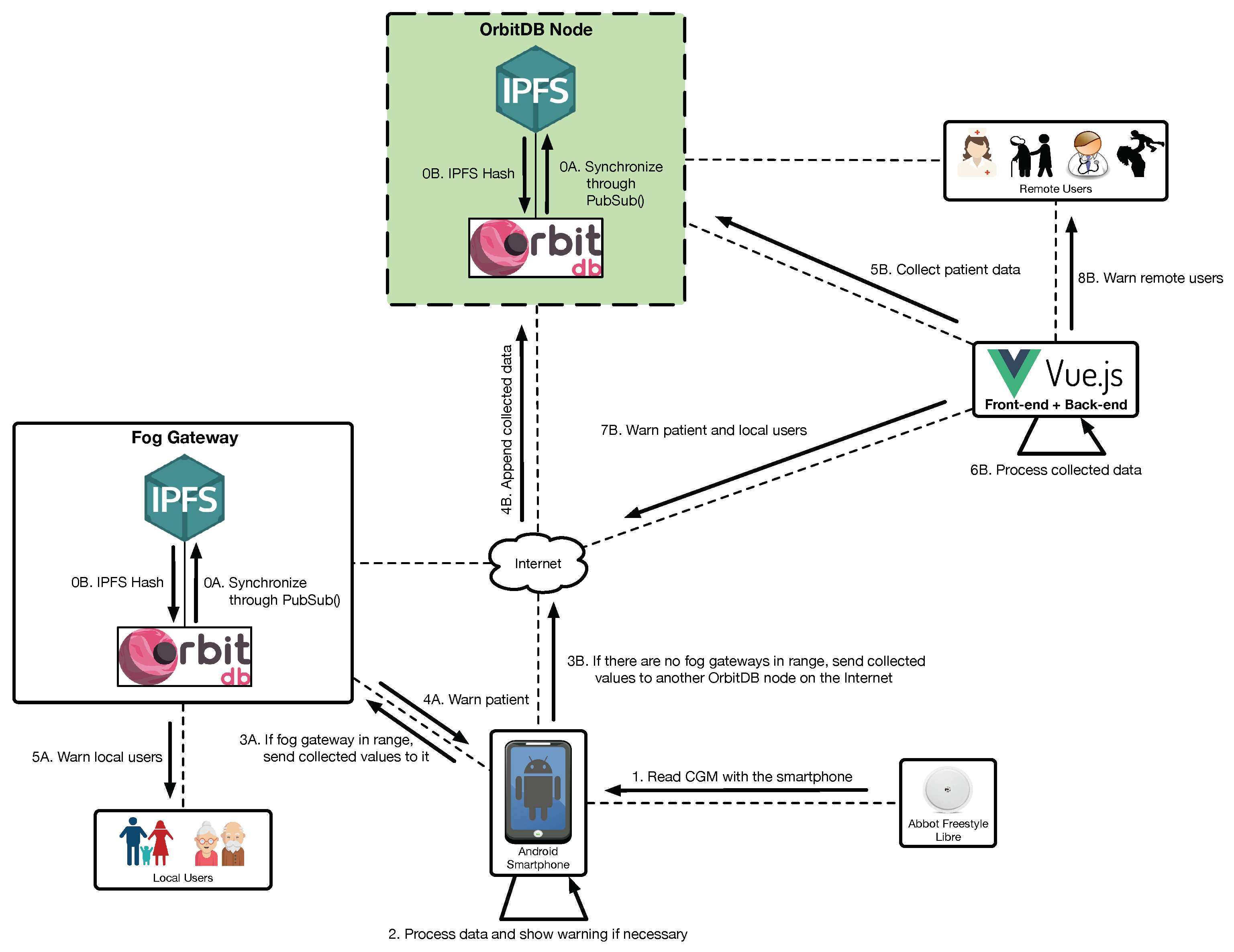
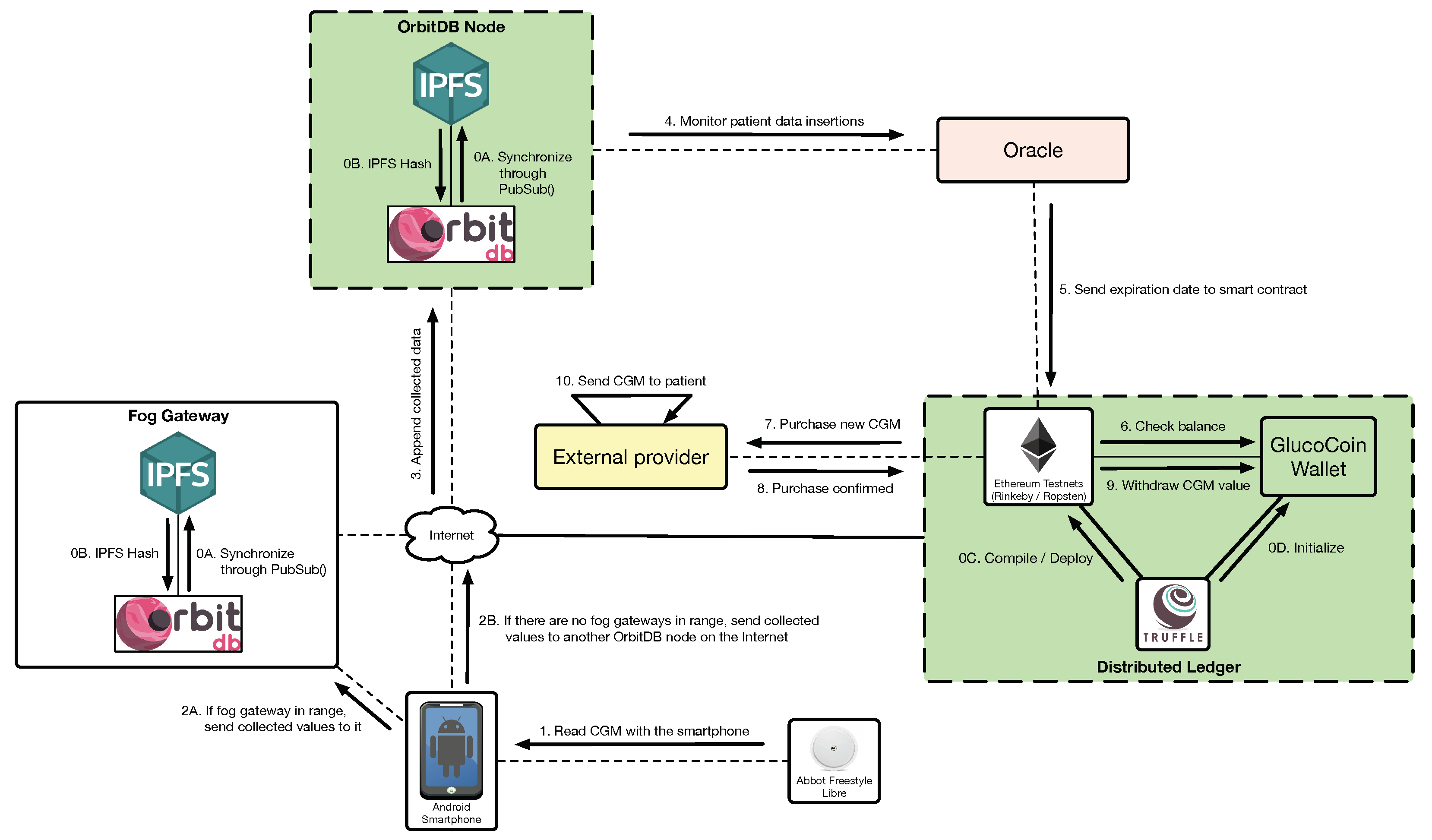
4.2. Regular Functioning of the System
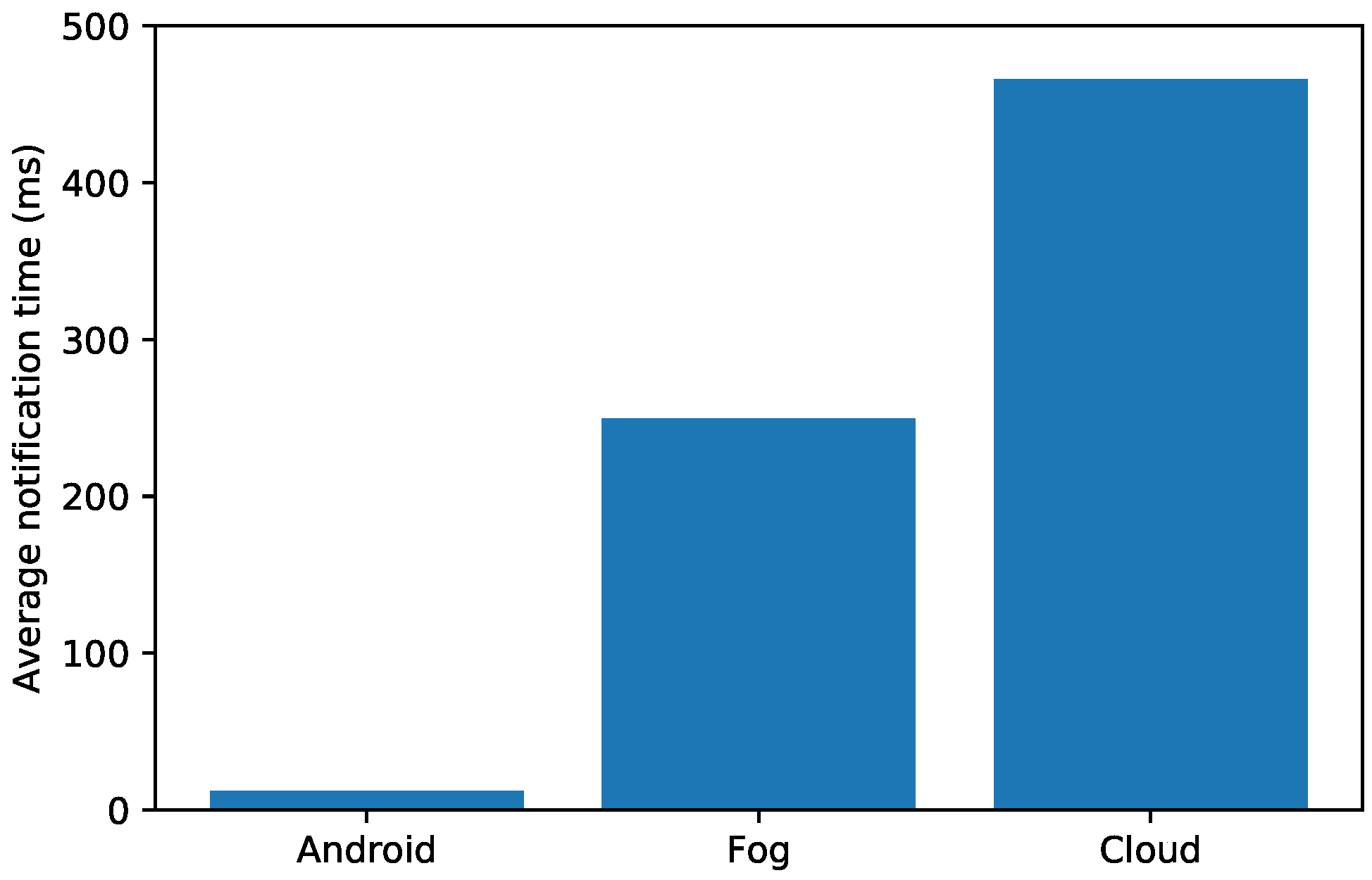
- Local warnings. For simple analyses, a smartphone is powerful enough to process the collected data and warn the user about a dangerous situation. Since the sensor data can be stored in the local database, the smartphone app can read such an information and then show notifications to the user (step 2).
- Fog warnings. If there is a fog gateway in range, the smartphone will send the collected values to it (step 3A) in order to store them in OrbitDB. The collected data can be accessed by the internal mHealth fog service, which can warn the patient (step 4A) and the local users (step 5A) in case of detecting a dangerous situation.
- Cloud warnings. If the smartphone detects no fog gateways, it sends the collected data to another OrbitDB node on the Internet (step 3B), which stores them (step 4B). Such data are retrieved periodically by the back-end (step 5B) in order to essentially show them to remote users through a web interface. In addition, the back-end processes the collected data (step 6B) and, if a dangerous situation is detected, it can warn local and remote users (steps 7B and 8B).
5. Experiments
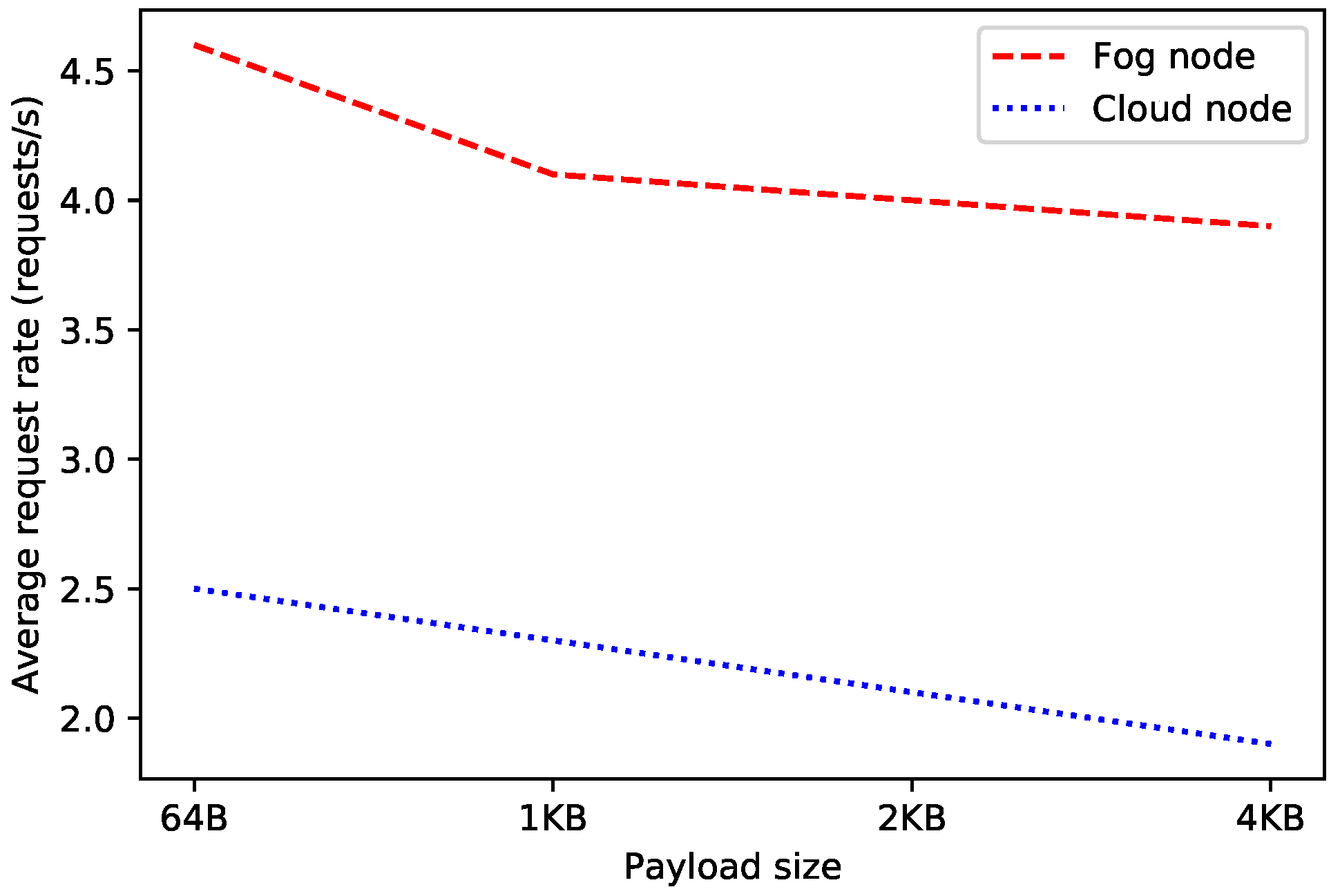
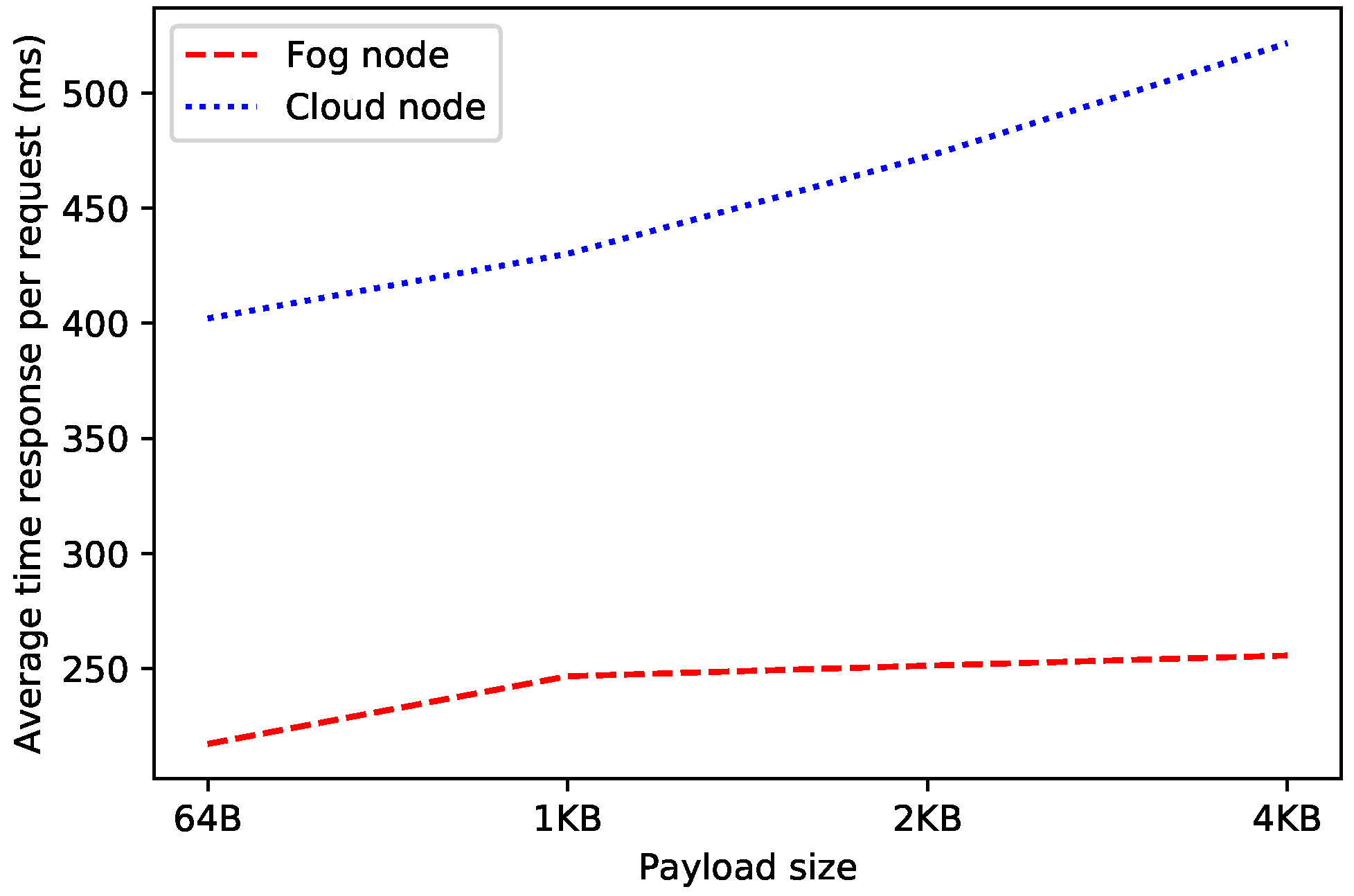
5.1. Baseline Performance of Fog and Cloud Nodes
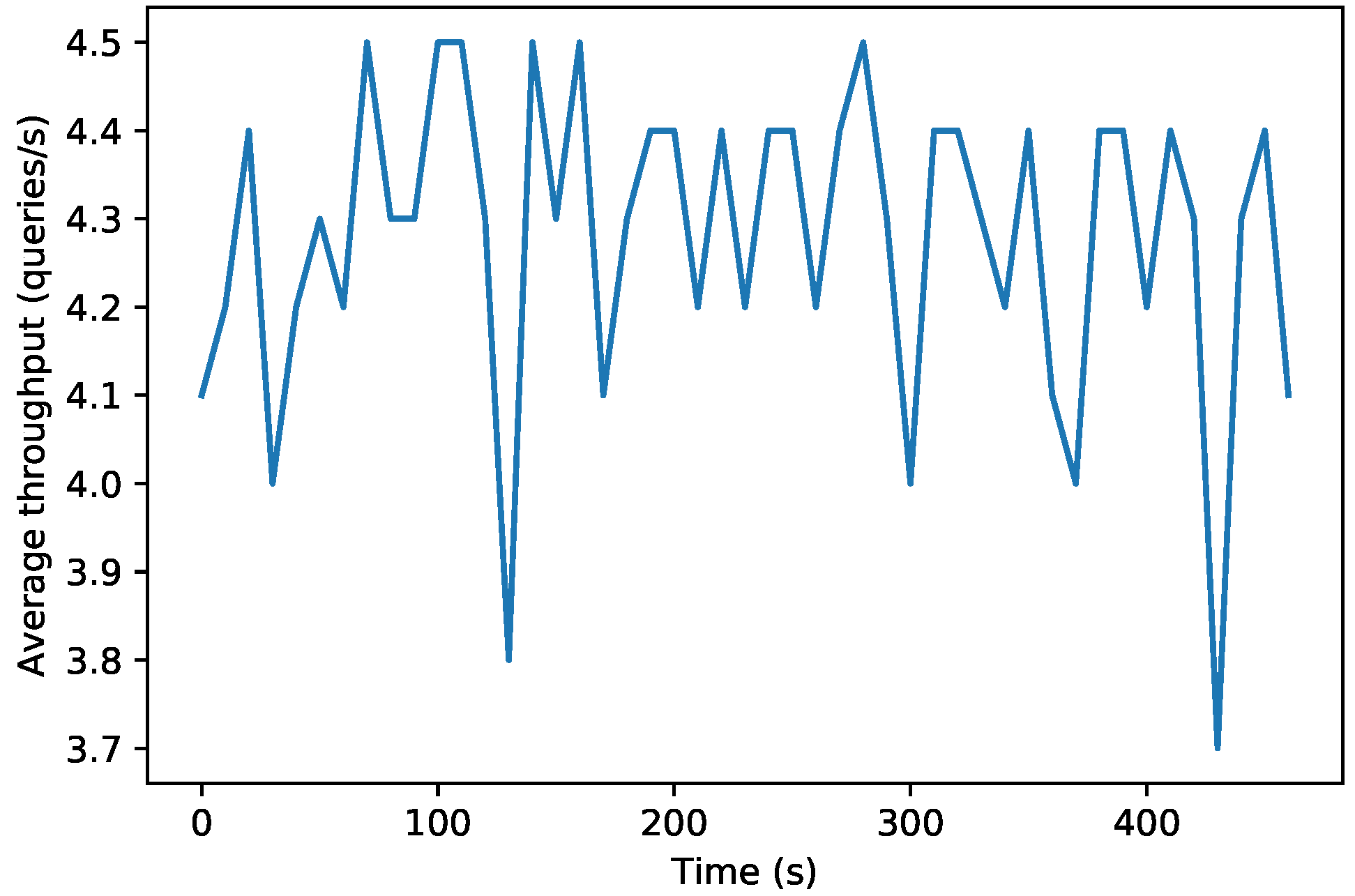
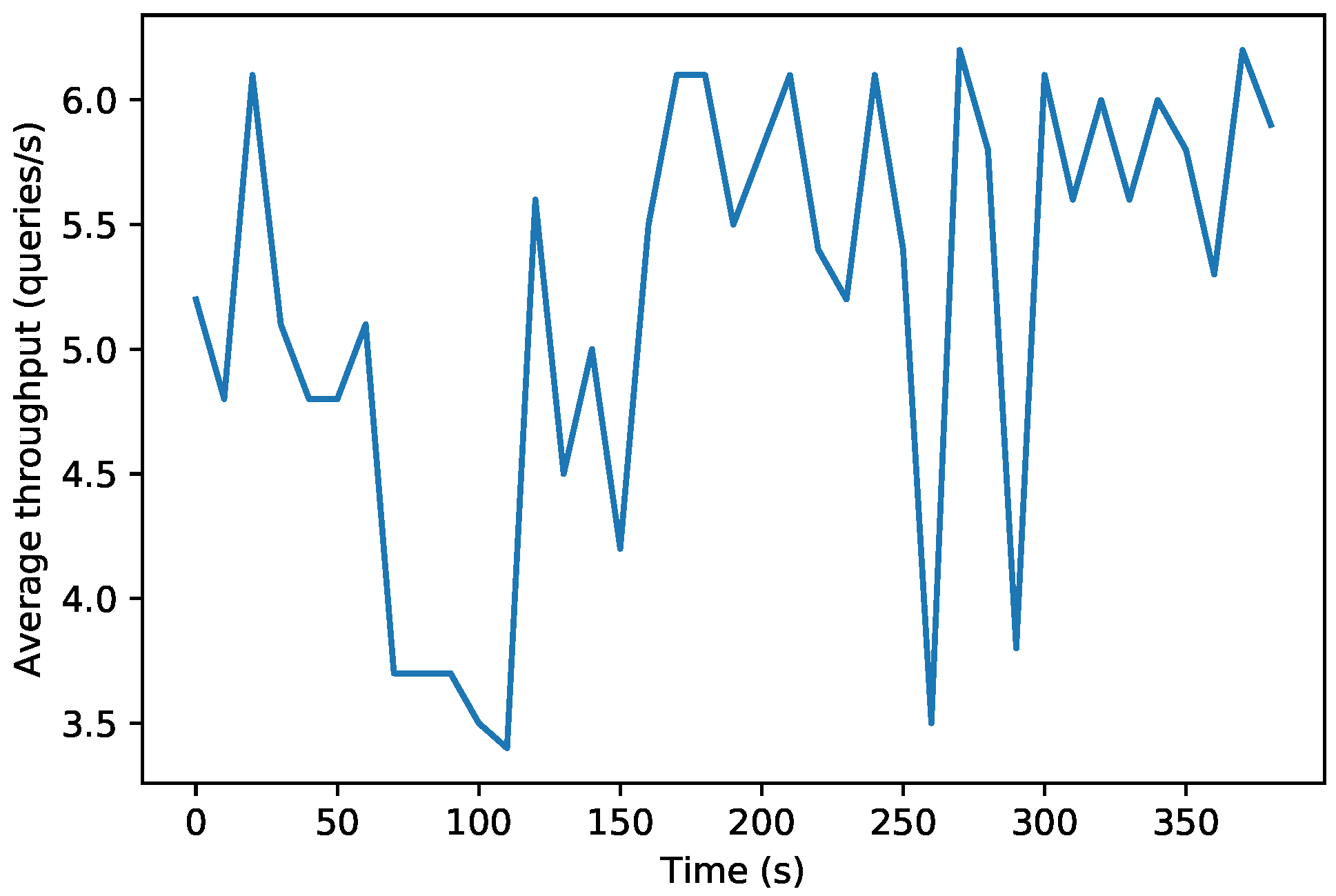
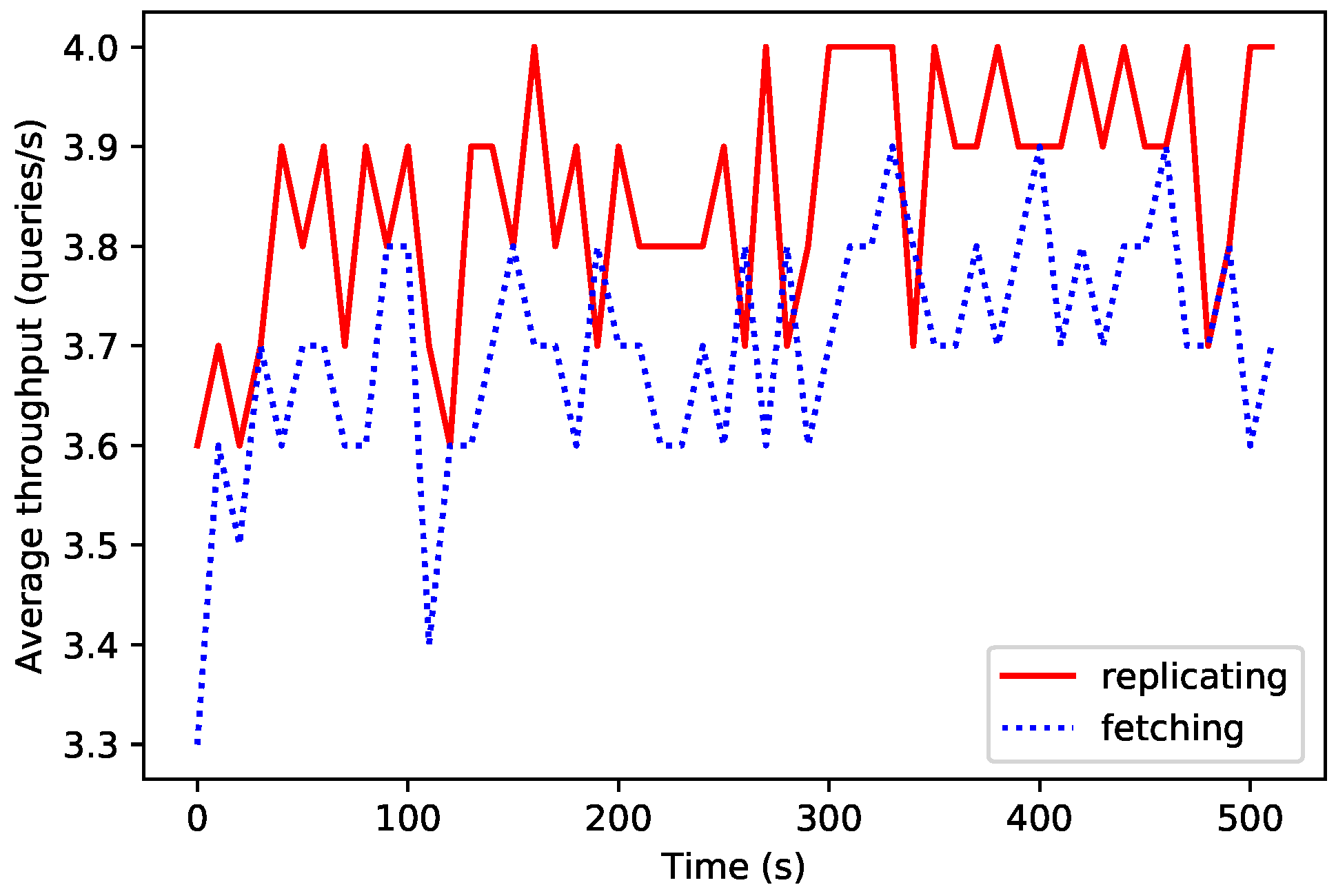
5.2. Performance of the Decentralized Database
5.3. Time Response of Event Warnings: Local, Fog and Cloud
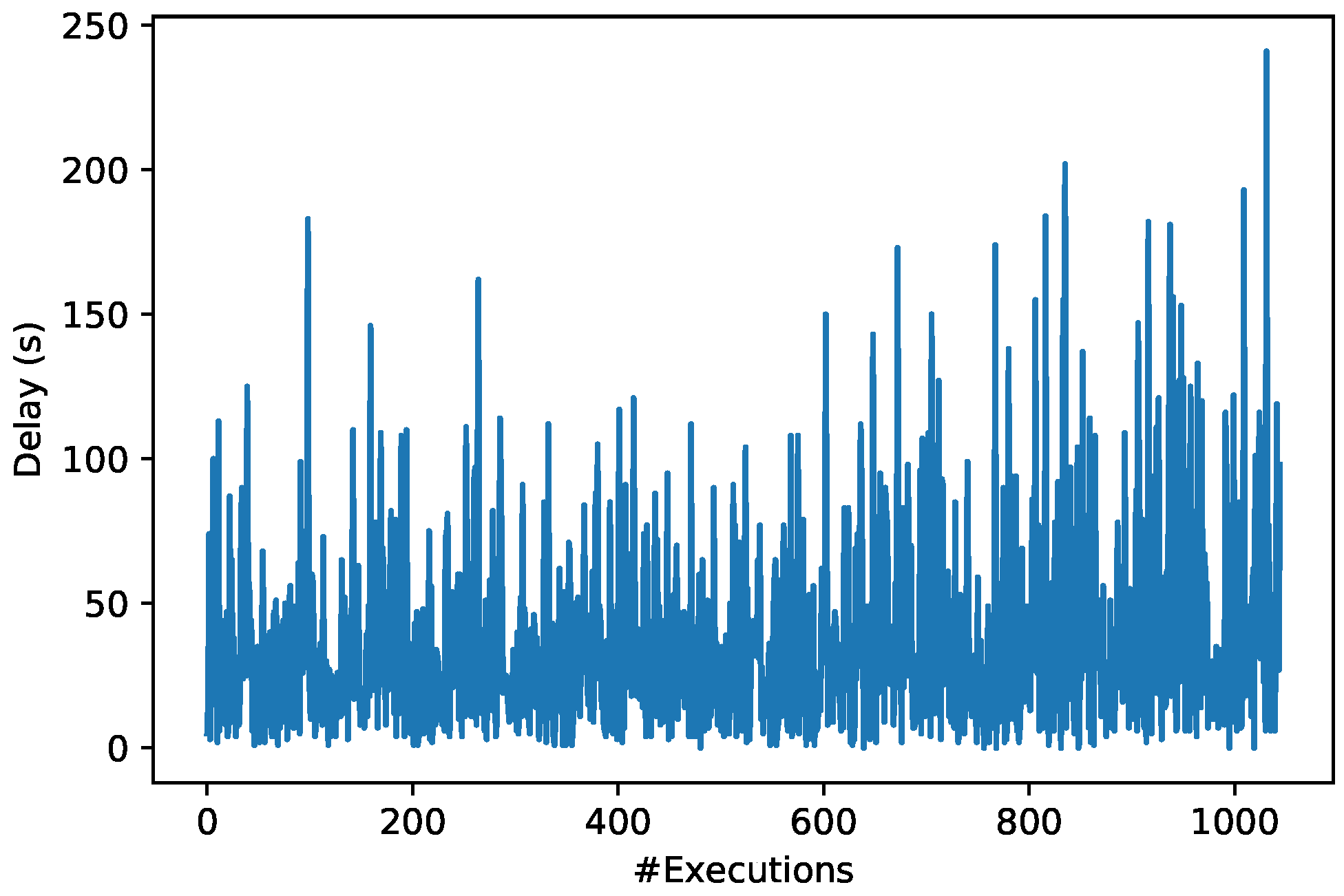
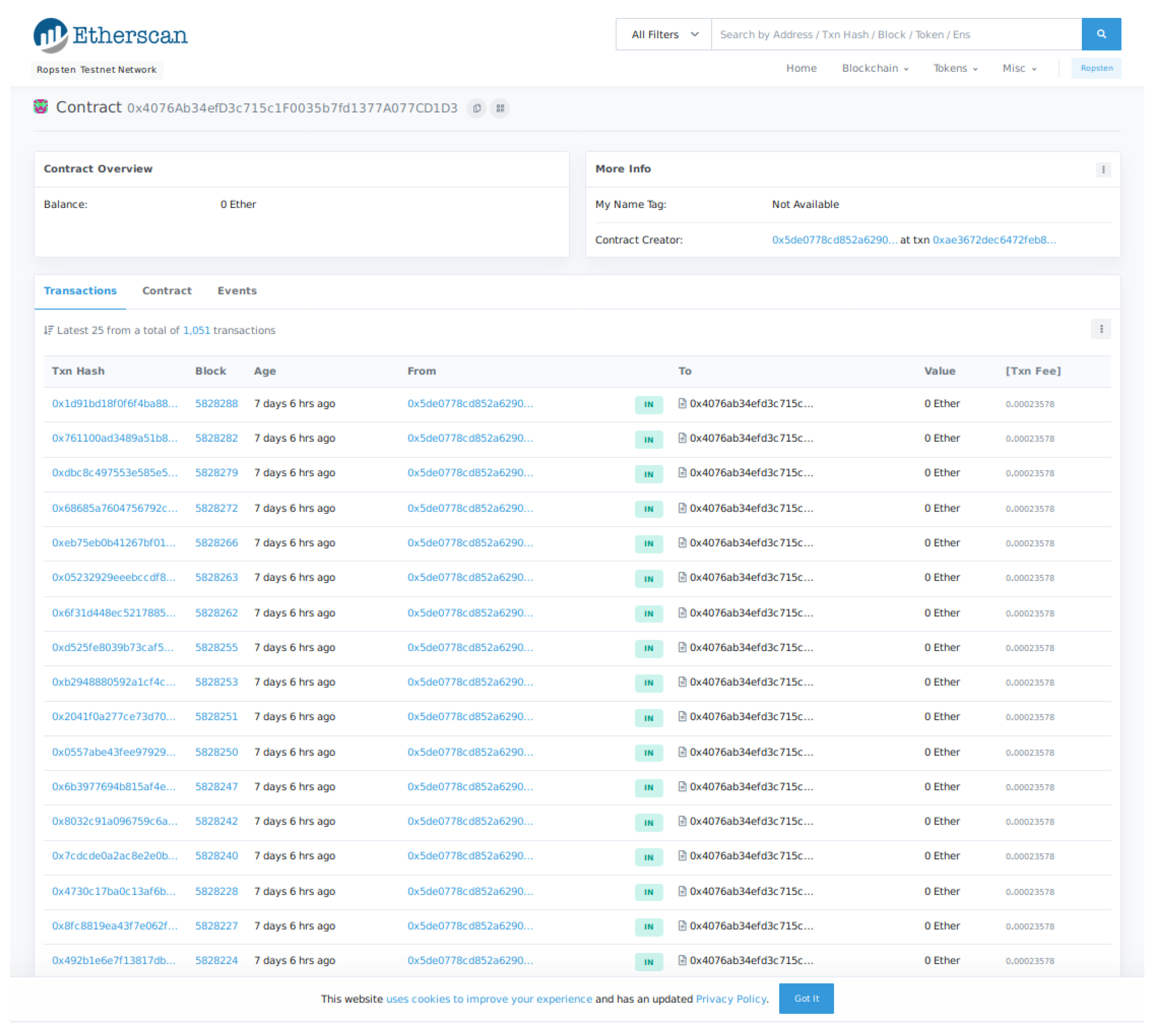
5.4. Blockchain Performance: Smart Contracts Execution Time
| Listing 1: Main code of the smart contract that controls GlucoCoin. |
pragma solidity >=0.4.25 <0.6.0;
contract GlucoCoin {
mapping (address => uint) balances;
event Transfer(address indexed _from address indexed _to, uint256 _value);
constructor() public {
balances[tx.origin] = 10000;
}
function sendCoin(address receiver, uint amount) public returns(bool sufficient) {
if (balances[msg.sender] < amount) return false;
balances[msg.sender] −= amount;
balances[receiver] += amount;
emit Transfer(msg.sender, receiver, amount);
return true;
}
function getBalanceInEth(address addr) public view returns(uint) {
return ConvertLib.convert(getBalance(addr),2);
}
function getBalance(address addr) public view returns(uint) {
return balances[addr];
}
}
|
6. Future Work
- Optimization of the hardware and software baseline performance. Although the obtained amounts of requests per second are high enough for the fog gateway (300 requests per second), the cloud should be improved in order to go above the achieved 200 requests per second.
- It should be further analyzed possible enhancements on the decentralized database performance, since in the experiments it was only possible to reach up to 6 write requests per second, which can be too restrictive in some practical scenarios.
- It would be ideal to perform trials on large sets of population and analyze the real performance of the system, the behavior of the patients regarding the incentive mechanisms and the usefulness of the collected data.
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Diabetes: Key Facts. Available online: http://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 31 May 2019).
- Benjamin, E.M. Self-Monitoring of Blood Glucose: The Basics. Clin. Diabetes 2002, 20, 45–47. [Google Scholar] [CrossRef]
- Torres, I.; Baena, M.G.; Cayon, M.; Ortego-Rojo, J.; Aguilar-Diosdado, M. Use of Sensors in the Treatment and Follow-up of Patients with Diabetes Mellitus. Sensors 2010, 10, 8. [Google Scholar] [CrossRef] [PubMed]
- Schmelzeisen-Redeker, G.; Schoemaker, M.; Kirchsteiger, H.; Freckmann, G.; Heinemann, L.; Del Re, L. Time Delay of CGM Sensors: Relevance, Causes, and Countermeasures. J. Diabetes Sci. Technol. 2015, 9, 1006–1015. [Google Scholar] [CrossRef] [PubMed]
- Fraga-Lamas, P.; Fernández-Caramés, T.M.; Noceda-Davila, D.; Díaz-Bouza, M.; Vilar-Montesinos, M.; Pena-Agras, J.D.; Castedo, L. Enabling automatic event detection for the pipe workshop of the shipyard 4.0. In Proceedings of the 2017 56th FITCE Congress, Madrid, Spain, 14–16 September 2017; pp. 20–27. [Google Scholar]
- Markakis, E.K.; Karras, K.; Zotos, N.; Sideris, A.; Moysiadis, T.; Corsaro, A.; Alexiou, G.; Skianis, C.; Mastorakis, G.; Mavromoustakis, C.X.; et al. EXEGESIS: Extreme Edge Resource Harvesting for a Virtualized Fog Environment. IEEE Commun. Mag. 2017, 55, 7. [Google Scholar] [CrossRef]
- Bonomi, F.; Milito, R.; Zhu, J.; Addepalli, S. Fog Computing and its Role in the Internet of Things. In Proceedings of the First Edition of the MCC Workshop on Mobile Cloud Computing, Helsinki, Finland, 17 August 2012; pp. 13–16. [Google Scholar]
- Fernández-Caramés, T.M.; Fraga-Lamas, P.; Suárez-Albela, M.; Díaz-Bouza, M.A. A Fog Computing Based Cyber-Physical System for the Automation of Pipe-Related Tasks in the Industry 4.0 Shipyard. Sensors 2018, 18, 1961. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Albela, M.; Fernández-Caramés, T.M.; Fraga-Lamas, P.; Castedo, L. A Practical Evaluation of a High-Security Energy-Efficient Gateway for IoT Fog Computing Applications. Sensors 2017, 9, 1978. [Google Scholar] [CrossRef] [PubMed]
- Sen, K.C.; Ghosh, K. Designing Effective Crowdsourcing Systems for the Healthcare Industry. In Social Entrepreneurship: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2019; pp. 590–594. [Google Scholar]
- Brabham, D.C.; Ribisl, K.M.; Kirchner, T.R.; Bernhardt, J.M. Crowdsourcing Applications for Public Health. Am. J. Prev. Med. 2014, 46, 2–179. [Google Scholar]
- Sparacino, G.; Facchinetti, A.; Cobelli, C. ‘Smart’ Continuous Glucose Monitoring Sensors: On-Line Signal Processing Issues. Sensors 2010, 10, 6751–6772. [Google Scholar] [CrossRef] [PubMed]
- Facchinetti, A. Continuous Glucose Monitoring Sensors: Past, Present and Future Algorithmic Challenges. Sensors 2016, 16, 2093. [Google Scholar] [CrossRef] [PubMed]
- Sparacino, G.; Zanon, M.; Facchinetti, A.; Zecchin, C.; Maran, A.; Cobelli, C. Italian Contributions to the Development of Continuous Glucose Monitoring Sensors for Diabetes Management. Sensors 2012, 12, 13753–13780. [Google Scholar] [CrossRef]
- Cappon, G.; Acciaroli, G.; Vettoretti, M.; Facchinetti, A.; Sparacino, G. Wearable Continuous Glucose Monitoring Sensors: A Revolution in Diabetes Treatment. Electronics 2017, 6, 65. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, X.-L.; Li, Z.-H.; Zhu, Z.-G.; Qian, S.-H.; Flewitt, A.J. Current and Emerging Technology for Continuous Glucose Monitoring. Sensors 2017, 17, 182. [Google Scholar] [CrossRef] [PubMed]
- Rosetti, P.; Bondia, J.; Vehí, J.; Fanelli, C.G. Estimating Plasma Glucose from Interstitial Glucose: The Issue of Calibration Algorithms in Commercial Continuous Glucose Monitoring Devices. Sensors 2010, 10, 10936–10952. [Google Scholar] [CrossRef] [PubMed]
- Howsmon, D.P.; Cameron, F.; Baysal, N.; Ly, T.T.; Forlenza, G.P.; Maahs, D.M.; Buckingham, B.A.; Hahn, J.; Bequette, B.W. Continuous Glucose Monitoring Enables the Detection of Losses in Infusion Set Actuation (LISAs). Sensors 2017, 17, 161. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Schumacher, M. Sensor Monitoring of Physical Activity to Improve Glucose Management in Diabetic Patients: A Review. Sensors 2016, 16, 589. [Google Scholar] [CrossRef] [PubMed]
- Dasanayake, I.S.; Bevier, W.C.; Castorino, K.; Pinsker, J.E.; Seborg, D.E.; Doyle, F.J.; Dassau, E. Early Detection of Physical Activity for People With Type 1 Diabetes Mellitus. J. Diabetes Sci. Technol. 2015, 9, 6. [Google Scholar] [CrossRef] [PubMed]
- Peralta, G.; Iglesias-Urkia, M.; Barcelo, M.; Gomez, R.; Moran, A.; Bilbao, J. Fog computing based efficient IoT scheme for the Industry 4.0. In Proceedings of the IEEE International Workshop of Electronics, Control, Measurement, Signals and their Application to Mechatronics (ECMSM), Donostia, Spain, 24–26 May 2017. [Google Scholar]
- Ali, O.; Shrestha, A.; Soar, J.; Wamba, S.F. Cloud computing-enabled healthcare opportunities, issues, and applications: A systematic review. Int. J. Inf. Manag. 2018, 43, 146–158. [Google Scholar] [CrossRef]
- Froiz-Míguez, I.; Fernández-Caramés, T.M.; Fraga-Lamas, P.; Castedo, L. Design, Implementation and Practical Evaluation of an IoT Home Automation System for Fog Computing Applications Based on MQTT and ZigBee-WiFi Sensor Nodes. Sensors 2018, 18, 2660. [Google Scholar] [CrossRef]
- Kraemer, F.A.; Braten, A.E.; Tamkittikhun, N.; Palma, D. Fog Computing in Healthcare—A Review and Discussion. IEEE Access 2017, 5, 9206–9222. [Google Scholar] [CrossRef]
- Wac, K.; Bargh, M.S.; Van Beijnum, B.j.F.; Bults, R.G.A.; Pawar, P.; Peddemors, A. Power- and delay-awareness of health telemonitoring services: The mobihealth system case study. IEEE J. Sel. Areas Commun. 2009, 27, 4. [Google Scholar] [CrossRef]
- Monteiro, A.; Dubey, H.; Mahler, L.; Yang, Q.; Mankodiya, K. Fit: A Fog Computing Device for Speech Tele-Treatments. In Proceedings of the IEEE International Conference on Smart Computing, St. Louis, MO, USA, 18–20 May 2016. [Google Scholar]
- Fernández-Caramés, T.M.; Fraga-Lamas, P. Towards The Internet of Smart Clothing: A Review on IoT Wearables and Garments for Creating Intelligent Connected E-Textiles. Electronics 2018, 7, 405. [Google Scholar] [CrossRef]
- López, G.; Custodiod, V.; Moren, J.I. LOBIN: E-Textile and Wireless-Sensor-Network-Based Platform for Healthcare Monitoring in Future Hospital Environments. IEEE Trans. Inf. Technol. Biomed. 2016, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Sood, S.K. Fog Assisted-IoT Enabled Patient Health Monitoring in Smart Homes. IEEE Int. Things J. 2018, 5, 3. [Google Scholar] [CrossRef]
- Sood, S.K.; Mahajan, I. A Fog-Based Healthcare Framework for Chikungunya. IEEE Int. Things J. 2018, 5, 2. [Google Scholar] [CrossRef]
- Khezr, S.; Moniruzzaman, M.; Yassine, A.; Benlamri, R. Blockchain Technology in Healthcare: A Comprehensive Review and Directions for Future Research. Appl. Sci. 2019, 9, 1736. [Google Scholar] [CrossRef]
- Zhang, P.; Schmidt, D.C.; White, J.; Lenz, G. Blockchain technology use cases in healthcare. In Advances in Computers; Elsevier: Amsterdam, The Netherlands, 2018; Volume 111, pp. 1–41. [Google Scholar]
- Ethereum Official Webpage. Available online: https://www.ethereum.org/ (accessed on 31 May 2019).
- Hyperledger Official Webpage. Available online: https://www.hyperledger.org/ (accessed on 31 May 2019).
- IOTA Official Webpage. Available online: https://www.iota.org/ (accessed on 31 May 2019).
- Fu, Y.; Zhu, J. Big Production Enterprise Supply Chain Endogenous Risk Management Based on Blockchain. IEEE Access 2019, 7, 15310–15319. [Google Scholar] [CrossRef]
- Christidis, K.; Devetsikiotis, M. Blockchains and smart contracts for the Internet of Things. IEEE Access 2016, 4, 2292–2303. [Google Scholar] [CrossRef]
- Mettler, M. Blockchain technology in healthcare: The revolution starts here. In Proceedings of the IEEE 18th International Conference on e-Health Networking, Applications and Services (Healthcom), Munich, Germany, 14–17 September 2016. [Google Scholar]
- Kuo, T.T.; Kim, H.E.; Ohno-Machado, L. Blockchain distributed ledger technologies for biomedical and health care applications. J. Am. Med. Inf. Assoc. 2017, 24, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Roman-Belmonte, J.M.; De la Corte-Rodriguez, H.; Rodriguez-Merchan, E.C.C.; la Corte-Rodriguez, H.; Carlos Rodriguez-Merchan, E. How Blockchain Technology Can Change Medicine. Postgrad. Med. 2018, 130, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Agbo, C.C.; Mahmoud, Q.H.; Eklund, J.M. Blockchain Technology in Healthcare: A Systematic Review. Healthcare 2019, 7, 56. [Google Scholar] [CrossRef]
- Hölbl, M.; Kompara, M.; Kamišalić, A.; Nemec Zlatolas, L. A Systematic Review of the Use of Blockchain in Healthcare. Symmetry 2018, 10, 470. [Google Scholar] [CrossRef]
- Cichosz, S.L.; Stausholm, M.N.; Kronborg, T.; Vestergaard, P.; Hejlesen, O. How to use blockchain for diabetes health care data and access management: An operational concept. J. Diabetes Sci. Technol. 2019, 13, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Azbeg, K.; Ouchetto, O.; Andaloussi, S.J.; Fetjah, L.; Sekkaki, A. Blockchain and IoT for Security and Privacy: A Platform for Diabetes Self-management. In Proceedings of the 2018 4th International Conference on Cloud Computing Technologies and Applications (Cloudtech), Brussels, Belgium, 26–28 November 2018; pp. 1–5. [Google Scholar]
- Hernández-Rojas, D.L.; Fernández-Caramés, T.M.; Fraga-Lamas, P.; Escudero, C.J. Design and Practical Evaluation of a Family of Lightweight Protocols for Heterogeneous Sensing through BLE Beacons in IoT Telemetry Applications. Sensors 2018, 18, 57. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Caramés, T.M.; Fraga-Lamas, P. A Review on Human-Centered IoT-Connected Smart Labels for the Industry 4.0. IEEE Access 2018, 6, 25939–25957. [Google Scholar] [CrossRef]
- An, J.; Gui, X.; Wang, Z.; Yang, J.; He, X. A Crowdsourcing Assignment Model Based on Mobile Crowd Sensing in the Internet of Things. IEEE Int. Things J. 2015, 2, 358–369. [Google Scholar] [CrossRef]
- Phuttharak, J.; Loke, S.W. A Review of Mobile Crowdsourcing Architectures and Challenges: Toward Crowd-Empowered Internet-of-Things. IEEE Access 2019, 7, 304–324. [Google Scholar] [CrossRef]
- Ren, Y.; Liu, W.; Wang, T.; Li, X.; Xiong, N.N.; Liu, A. A Collaboration Platform for Effective Task and Data Reporter Selection in Crowdsourcing Network. IEEE Access 2019, 7, 19238–19257. [Google Scholar] [CrossRef]
- Guo, W.; Zhou, S.; Chen, Y.; Wang, S.; Chu, X.; Niu, Z. Simultaneous Information and Energy Flow for IoT Relay Systems with Crowd Harvesting. IEEE Commun. Mag. 2016, 54, 143–149. [Google Scholar] [CrossRef]
- Abualsaud, K.; Elfouly, T.M.; Khattab, T.; Yaacoub, E.; Sabry Ismail, L.; Ahmed, M.H.; Guizani, M. A Survey on Mobile Crowd-Sensing and Its Applications in the IoT Era. IEEE Access 2019, 7, 3855–3881. [Google Scholar] [CrossRef]
- Ranard, B.L.; Ha, Y.P.; Meisel, Z.F.; Asch, D.A.; Hill, S.S.; Becker, L.B.; Seymour, A.K.; Merchant, R.M. Crowdsourcing—Harnessing the masses to advance health and medicine, a systematic review. J. Gen. Int. Med. 2014, 29, 187–203. [Google Scholar] [CrossRef]
- Tucker, J.D.; Day, S.; Tang, W.; Bayus, B. Crowdsourcing in medical research: Concepts and applications. PeerJ 2019, 7, e6762. [Google Scholar] [CrossRef] [PubMed]
- Freifeld, C.C.; Chunara, R.; Mekaru, S.R.; Chan, E.H.; Kass-Hout, T.; Iacucci, A.A.; Brownstein, J.S. Participatory epidemiology: Use of mobile phones for community-based health reporting. PLoS Med. 2010, 7, e100036. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.; Chuah, M.C. Incentivising high quality crowdsourcing clinical data for disease prediction. In Proceedings of the Second IEEE/ACM International Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Philadelphia, PA, USA, 17–19 July 2017; pp. 185–194. [Google Scholar]
- Fernández-Caramés, T.M.; Fraga-Lamas, P. A Review on the Use of Blockchain for the Internet of Things. IEEE Access 2018, 6, 32979–33001. [Google Scholar] [CrossRef]
- Fraga-Lamas, P.; Fernández-Caramés, T.M. A Review on Blockchain Technologies for an Advanced and Cyber-Resilient Automotive Industry. IEEE Access 2019, 7, 17578–17598. [Google Scholar] [CrossRef]
- Fernández-Caramés, T.M.; Fraga-Lamas, P. A Review on the Application of Blockchain for the Next Generation of Cybersecure Industry 4.0 Smart Factories. IEEE Access 2019, 7, 45201–45218. [Google Scholar] [CrossRef]
- Dexcom Official Webpage. Available online: https://www.dexcom.com (accessed on 31 May 2019).
- Medtronic Official Webpage. Available online: https://www.medtronic.com (accessed on 31 May 2019).
- Abbott Official Webpage. Available online: https://www.abbott.com/ (accessed on 31 May 2019).
- Agency for Quality and Accreditation in Health Care and Social Welfare (AAZ); Main Association of Austrian Social Security Institutions (HVB); The Norwegian Institute of Public Health (NIPHNO). Continuous Glucose Monitoring (CGM Real-Time) and Flash Glucose Monitoring (FGM) as Personal, Standalone Systems in Patients with Diabetes Mellitus Treated with Insulin; Joint Assessment; Zagreb: EUnetHTA; 27 July 2018; Report No.: OTJA08. Available online: https://www.eunethta.eu/wp-content/uploads/2018/07/OTJA08_CGM-real-time-and-FGM-aspersonal2c-standalone-systems-in-patients-with-diabetes-mellitus-treatedwith-insulin.pdf (accessed on 31 May 2019).
- Libre Monitor Official GitHub Page. Available online: https://github.com/UPetersen/LibreMonitor (accessed on 31 May 2019).
- Limitter Official GitHub Page. Available online: https://github.com/JoernL/LimiTTer (accessed on 31 May 2019).
- OrbitDB: Peer-to-Peer Database for the Decentralized Web. Github Repository. Available online: https://github.com/orbitdb/orbit-db (accessed on 31 March 2019).
- IPFS Official Webpage. Available online: https://ipfs.io/ (accessed on 31 March 2019).
- OrbitDB HTTP API Official GitHub. Available online: https://github.com/orbitdb/orbit-db-http-api (accessed on 31 May 2019).
- Vue.js Framework Official Website. Available online: https://vuejs.org/ (accessed on 31 May 2019).
- Telegram Official Website. Available online: https://telegram.org/ (accessed on 31 May 2019).
- Twilio Official Website. Available online: https://www.twilio.com/ (accessed on 31 May 2019).
- Rinkeby’s Official Website. Available online: https://www.rinkeby.io/ (accessed on 31 May 2019).
- Ropsten’s Official GitHub Page. Available online: https://github.com/ethereum/ropsten (accessed on 31 May 2019).
- Rinkeby’s Ether Faucet. Available online: https://faucet.rinkeby.io/ (accessed on 31 May 2019).
- Metamask Ether Faucet. Available online: https://faucet.metamask.io/ (accessed on 31 May 2019).
- Truffle Official Website. Available online: https://truffleframework.com (accessed on 31 May 2019).
- Raspberry Pi 3 Official Webpage. Available online: https://www.raspberrypi.org/products/ (accessed on 31 May 2019).
- Banana Pi Official Webpage. Available online: http://www.banana-pi.org/ (accessed on 31 May 2019).
- Odroid-XU4 Official Webpage. Available online: https://www.odroid.co.uk/hardkernel-odroid-xu4 (accessed on 31 May 2019).
- Orange Pi Zero Plus Official Webpage. Available online: http://www.orangepi.org/OrangePiZeroPlus/ (accessed on 31 May 2019).
- Armbian—Linux for ARM Development Boards Official Webpage. Available online: https://www.armbian.com/ (accessed on 31 May 2019).
- Web3 Official GitHub Page. Available online: https://github.com/ethereum/web3.js/ (accessed on 31 May 2019).
- Infura Official Website. Available online: https://infura.io/dashboard (accessed on 31 May 2019).
- Node.js Official Website. Available online: https://nodejs.org/en/ (accessed on 31 May 2019).
- Miaomiao Official GitHub Page. Available online: http://miaomiao.cool (accessed on 31 May 2019).
- Official OrbitDB Benchmarking Scripts. Available online: https://github.com/orbitdb/orbit-db/tree/master/benchmarks (accessed on 31 May 2019).
- Bitcoin Official Web Page. Available online: https://bitcoin.org/en/ (accessed on 15 July 2019).
- Statista Statics on Bitcoin’s Average Transaction Time. Available online: https://www.statista.com/statistics/793539/bitcoin-transaction-confirmation-time/ (accessed on 15 July 2019).
- Wallet Related to the Blockchain Performance Tests of the Article. Available online: https://ropsten.etherscan.io/address/0x4076ab34efd3c715c1f0035b7fd1377a077cd1d3 (accessed on 27 June 2019).
- Sharding Official Web Page. Available online: https://github.com/ethereum/wiki/wiki/Sharding-roadmap (accessed on 25 February 2019).
- Raiden Official Web Page. Available online: https://raiden.network/101.html (accessed on 25 February 2019).
- Poon, J.; Buterin, V. Plasma: Scalable autonomous smart contracts. White Paper 2017, 1–47. [Google Scholar]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Models | Dexcom G4 Platinum | Dexcom G5 Mobile | Dexcom G6 | Medtronic Guardian Connect | Medtronic iPro 2 Prof | Medtronic MiniMed 670G | Abbot Freestyle Libre | Abbot Freestyle Libre 2 | Roche Eversense XL | |
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | ||||||||||
| Duration | 7 days | 7 days | 10 days | 6 days | 6 days | 7 days | 14 days | 14 days | 180 days | |
| Daily calibration | Yes | Yes | No (manual calibration is available if the start-up calibration code is lost) | Yes | Yes | Yes | No | No | Yes | |
| Alarms | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | |
| Price | € 1100 (Kit with a receiver, a transmitter and 4 sensors) | € 1270 (Kit with a receiver, a transmitter and 4 sensors) | € 1000 (Kit with a receiver, a transmitter and 3 sensors lasting 10 days each) | It varies depending on its use (ad-hoc, partial or intensive) | Not publicly available | Transmitter: $ 699, sensors ranging from $ 50–$ 75, depending on the number of purchased units | € 169.90 (Kit with one reader and two sensors) | € 169.90 (Kit with one reader and two sensors) | € 399 for the transmitter and 1399 for one sensor | |
| Data transmission | Automatic, every 5 min | Automatic, every 5 min | Automatic, every 5 min | Automatic, every 5 min | Automatic, every 5 min | Automatic, every 5 min | Manual | Manual | Automatic, every 5 min | |
| Reading range | Max. 6 m | Max. 6 m | Max. 6 m | Max. 6 m | - | - | Max. 10 cm | - | ||
| Remote monitoring | No | Yes (iOS/Android app) | Yes (iOS/Android app) | Yes (iOS app) | Yes (iOS/Android app) | - | Yes (Android app) | - | Yes (iOS app) | |
| Communications | Bluetooth | Bluetooth | Bluetooth | Bluetooth | - | - | NFC | NFC, BLE | Bluetooth | |
| MARD | 13% | 9% | 9% | 13.60% | 11 % | 8.7% | 11.40% | 9.5% | 11.60% | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Caramés, T.M.; Froiz-Míguez, I.; Blanco-Novoa, O.; Fraga-Lamas, P. Enabling the Internet of Mobile Crowdsourcing Health Things: A Mobile Fog Computing, Blockchain and IoT Based Continuous Glucose Monitoring System for Diabetes Mellitus Research and Care. Sensors 2019, 19, 3319. https://doi.org/10.3390/s19153319
Fernández-Caramés TM, Froiz-Míguez I, Blanco-Novoa O, Fraga-Lamas P. Enabling the Internet of Mobile Crowdsourcing Health Things: A Mobile Fog Computing, Blockchain and IoT Based Continuous Glucose Monitoring System for Diabetes Mellitus Research and Care. Sensors. 2019; 19(15):3319. https://doi.org/10.3390/s19153319
Chicago/Turabian StyleFernández-Caramés, Tiago M., Iván Froiz-Míguez, Oscar Blanco-Novoa, and Paula Fraga-Lamas. 2019. "Enabling the Internet of Mobile Crowdsourcing Health Things: A Mobile Fog Computing, Blockchain and IoT Based Continuous Glucose Monitoring System for Diabetes Mellitus Research and Care" Sensors 19, no. 15: 3319. https://doi.org/10.3390/s19153319
APA StyleFernández-Caramés, T. M., Froiz-Míguez, I., Blanco-Novoa, O., & Fraga-Lamas, P. (2019). Enabling the Internet of Mobile Crowdsourcing Health Things: A Mobile Fog Computing, Blockchain and IoT Based Continuous Glucose Monitoring System for Diabetes Mellitus Research and Care. Sensors, 19(15), 3319. https://doi.org/10.3390/s19153319