Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review

 ,
,  and
and 
Abstract
:1. Introduction
2. Methods
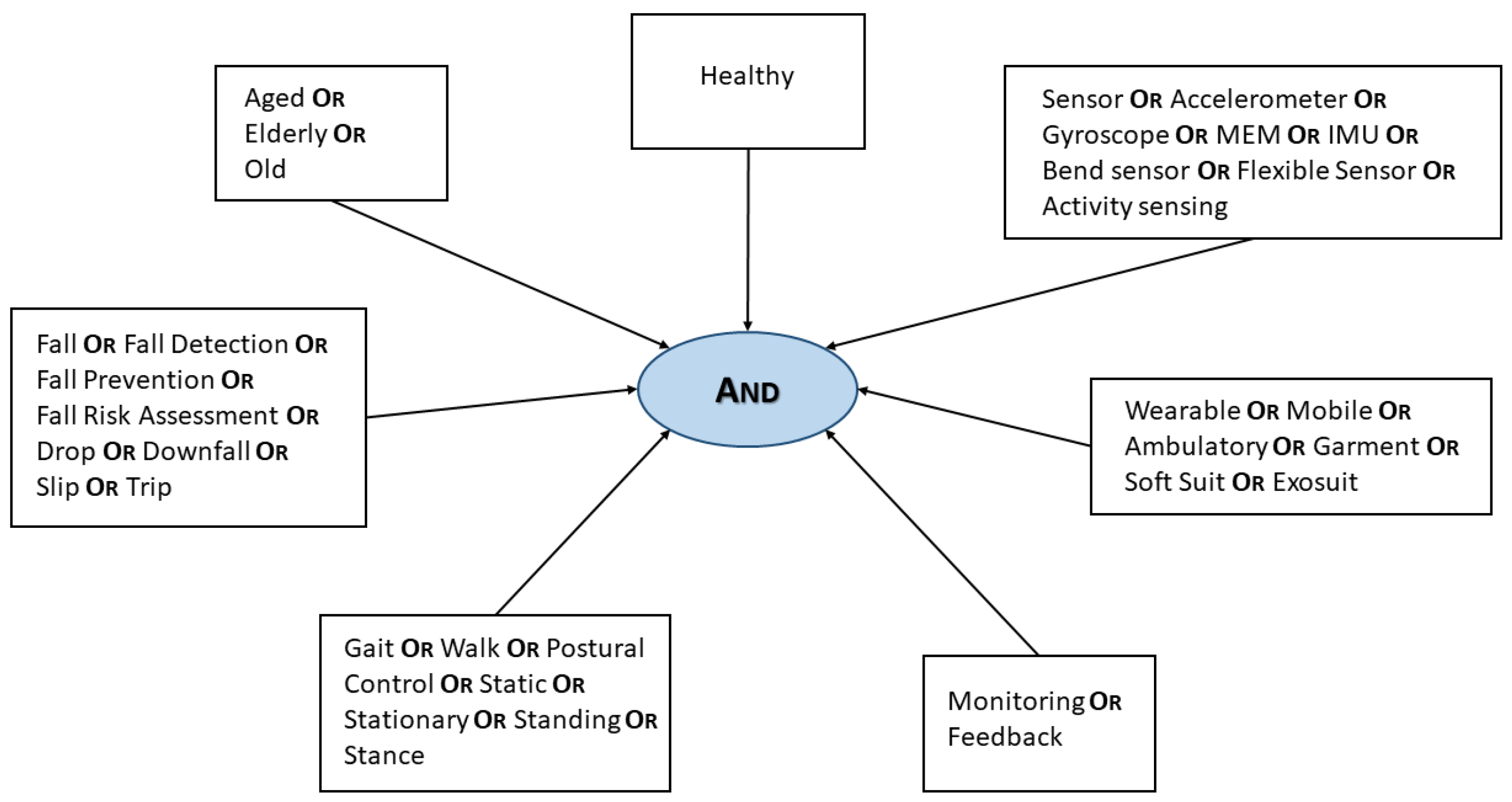
2.1. Keywords Definition
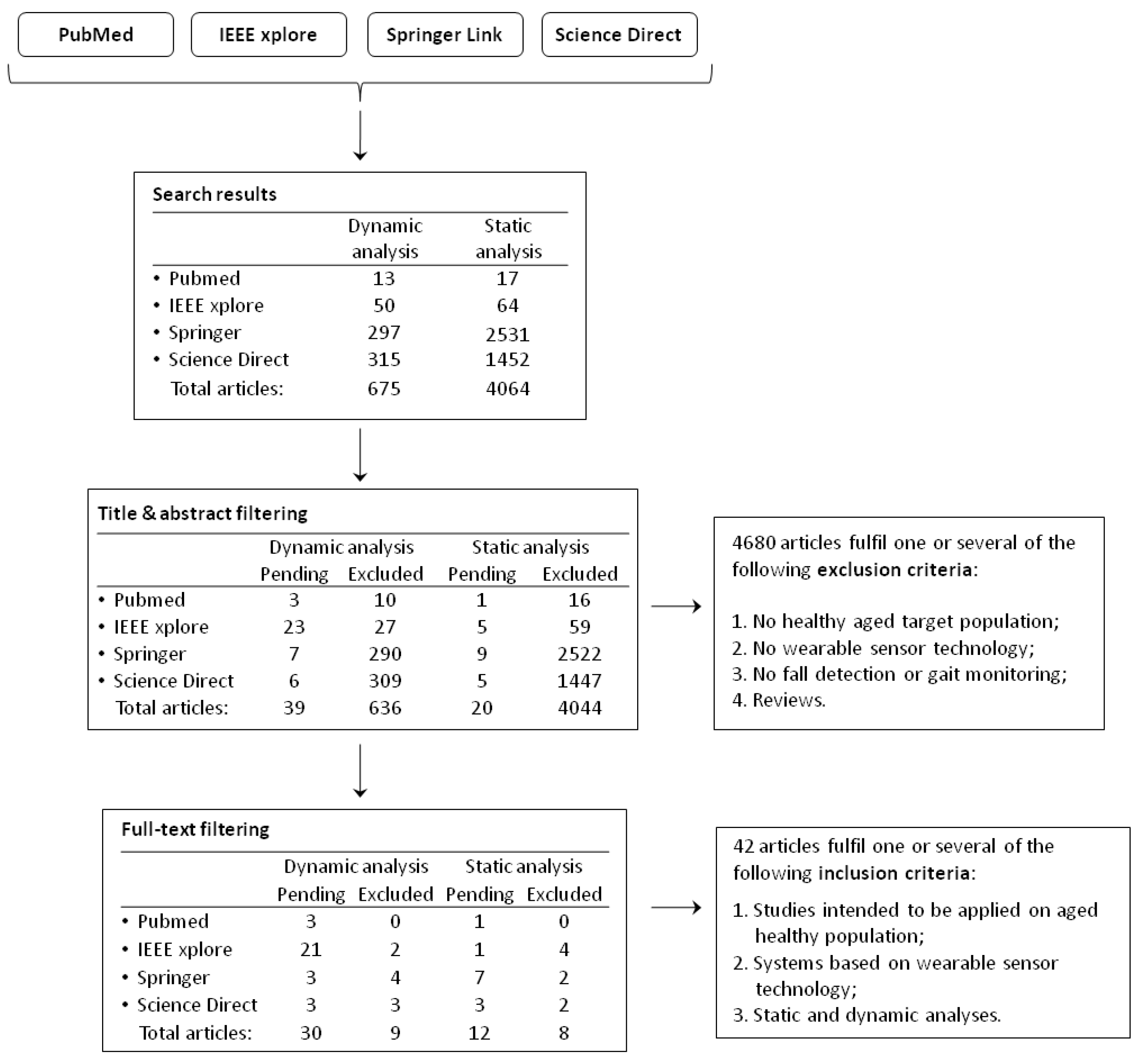
2.2. Literature Research Strategy
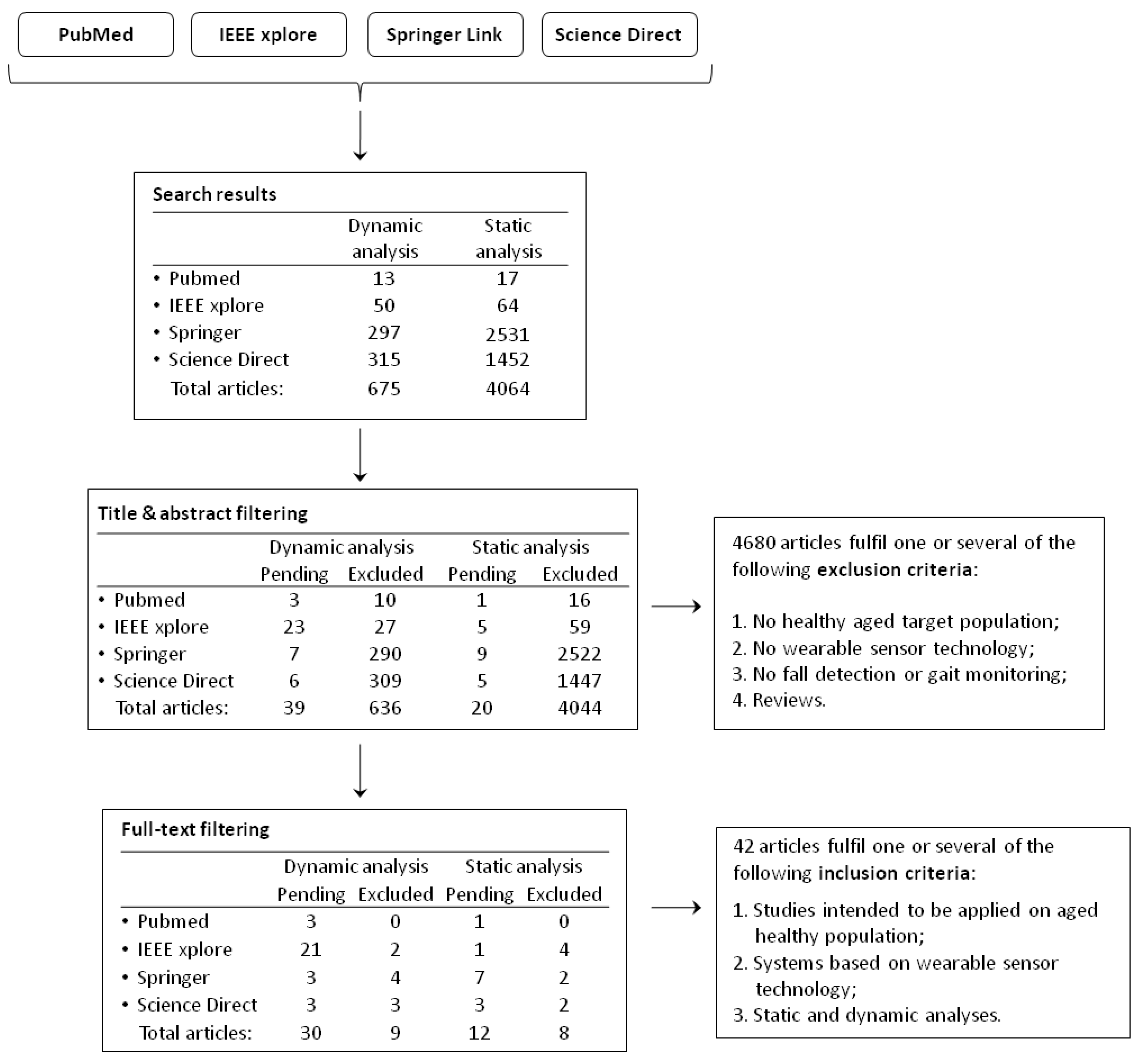
2.3. Study Selection and Screening Process
- all the studies that do not include healthy aged population as target;
- articles not including a wearable sensor technology;
- all the manuscripts not related to “fall risk assessment”, “fall prevention”, “fall detection” and “standing analysis”;
- all the review articles.
- all studies on healthy aged people or intended to be applied on an aged population;
- all systems based on a wearable sensor technology;
- gait and standing analysis have been included.
3. Results of the Bibliographic Research
- Author (year): the family name of the first author is reported, and the publication year between brackets;
- Participants (number/age): the number of volunteers considered in the study. For each population, the number of the subjects involved and their average age is reported;
- Number of sensors: how many sensors are used (simultaneously or not) within the study. In the case of compound sensors, each of the elementary sensing technology has been accounted for;
- Sensor type: the typology of sensors adopted in the study. Their acronyms are reported in Table 4. In case smartphones have been employed, we only reported the name of the actual sensors;
- Sensor placement: sensor attachment location;
- Task: the (one or more) task the participants have been asked to perform for the validation of the study. We chose to include activities implying oscillations of the center of mass, as they make falls more likely;
- Analysis: the type of performed analysis, i.e., static, dynamic or both.
4. Discussion
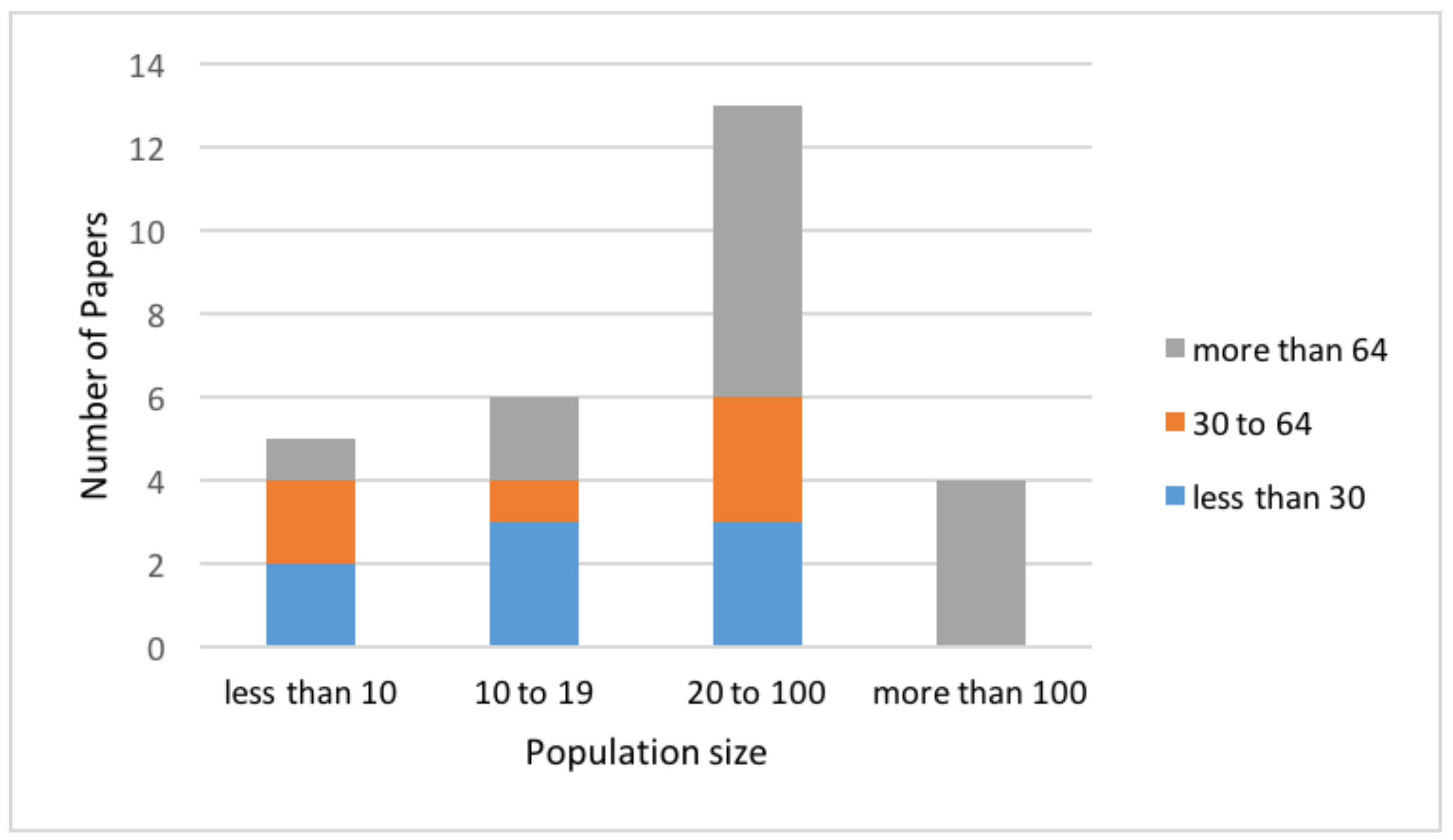
4.1. Participants
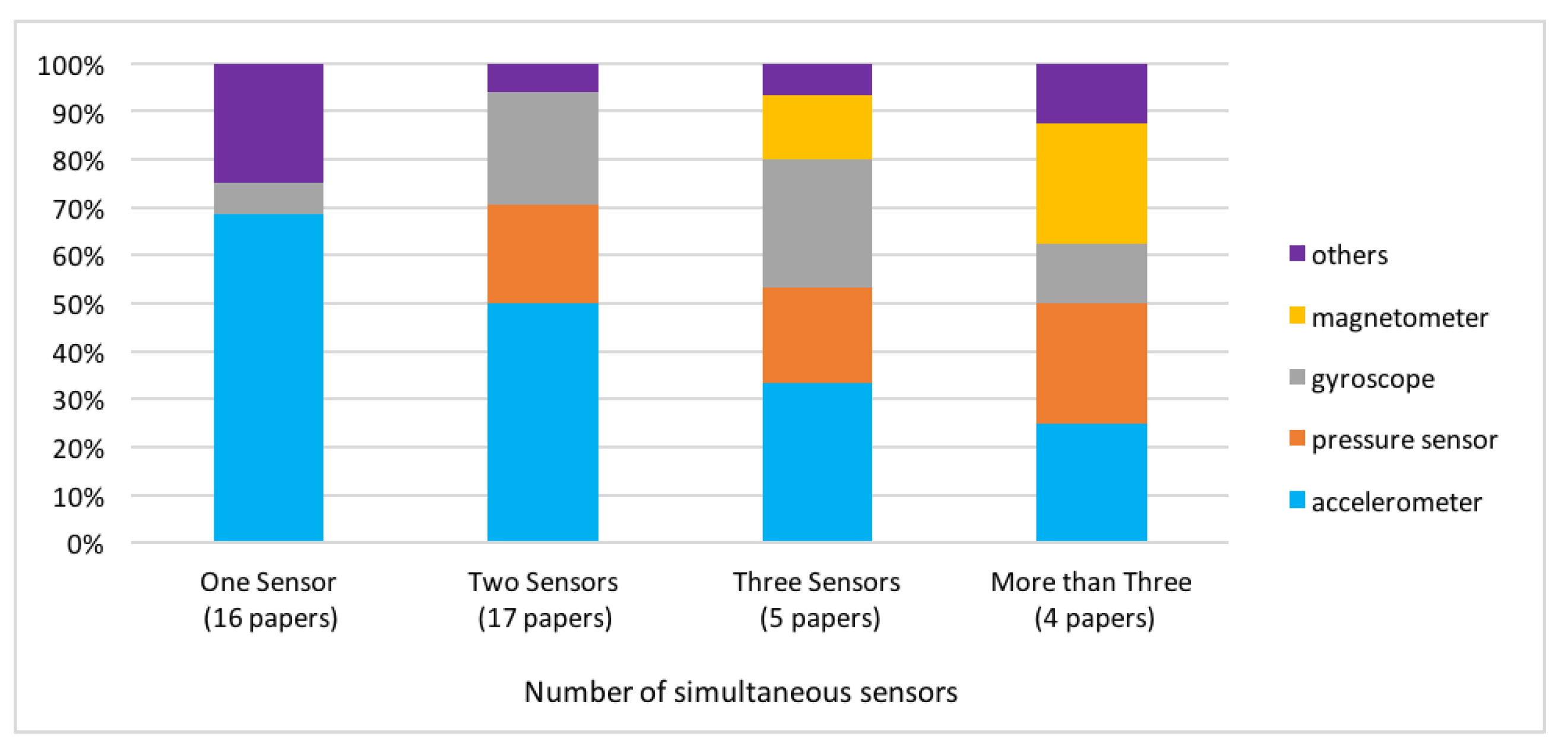
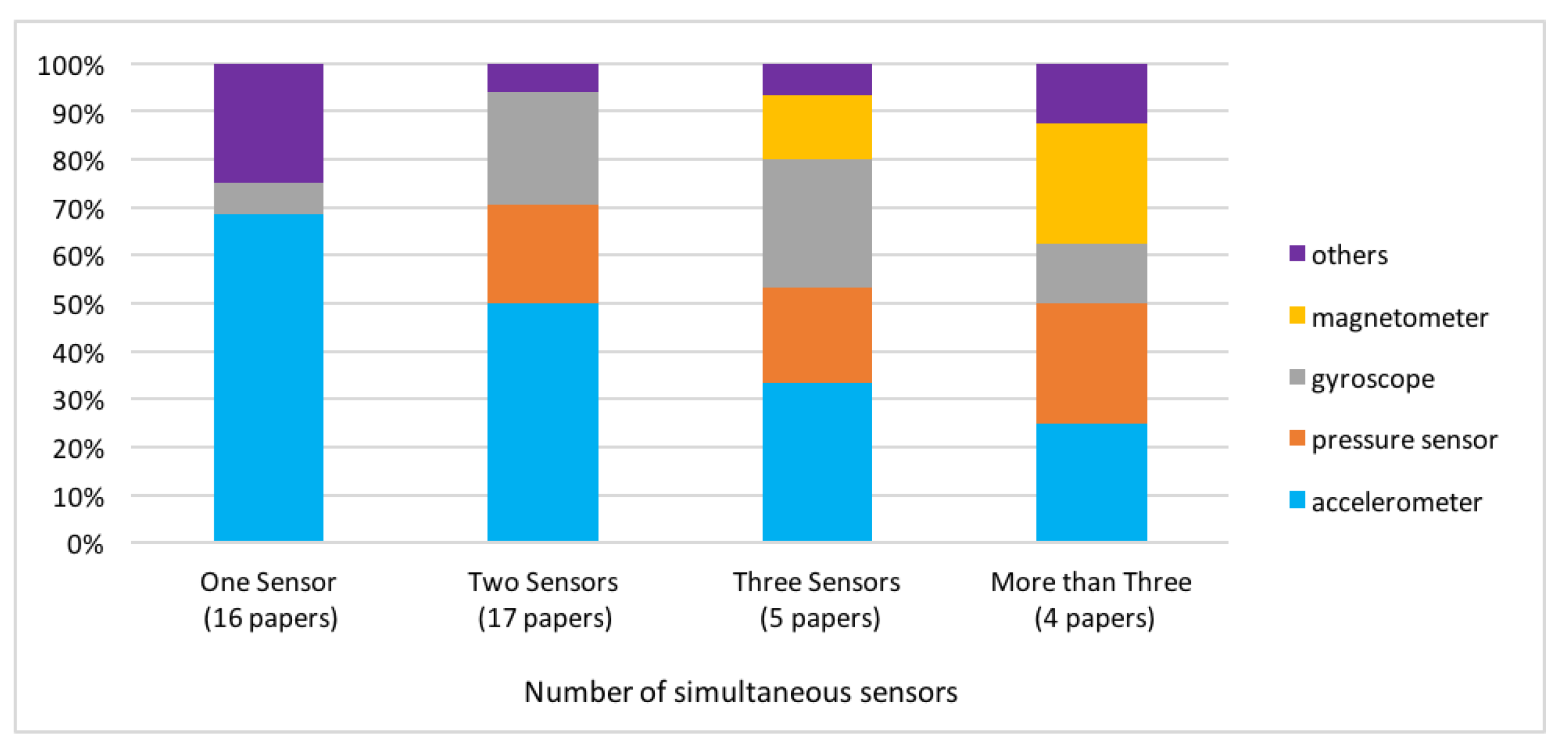
4.2. Typology of Sensors
4.2.1. Single Sensor
4.2.2. Two Sensors
4.2.3. Three or More Sensors
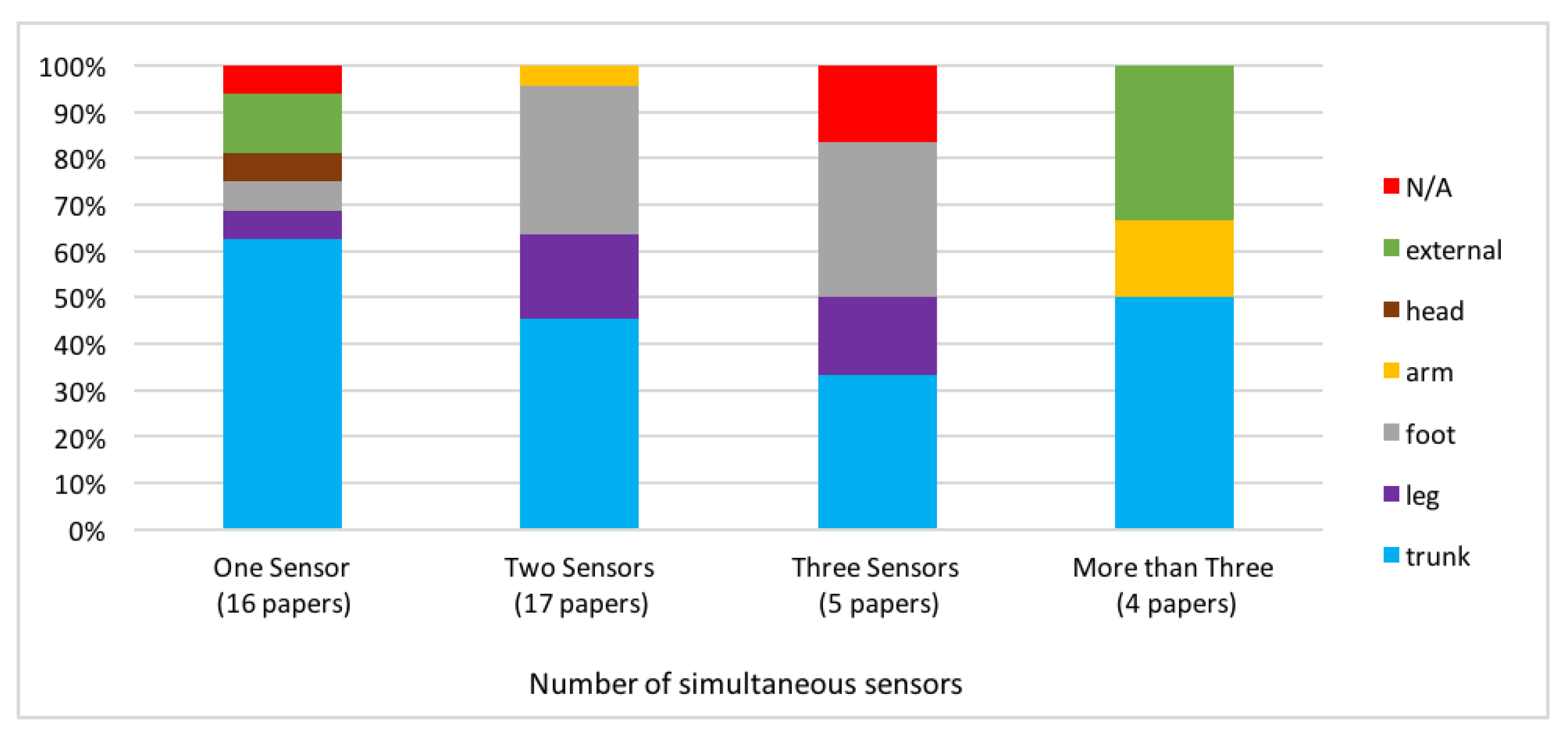
4.3. Position of Sensors
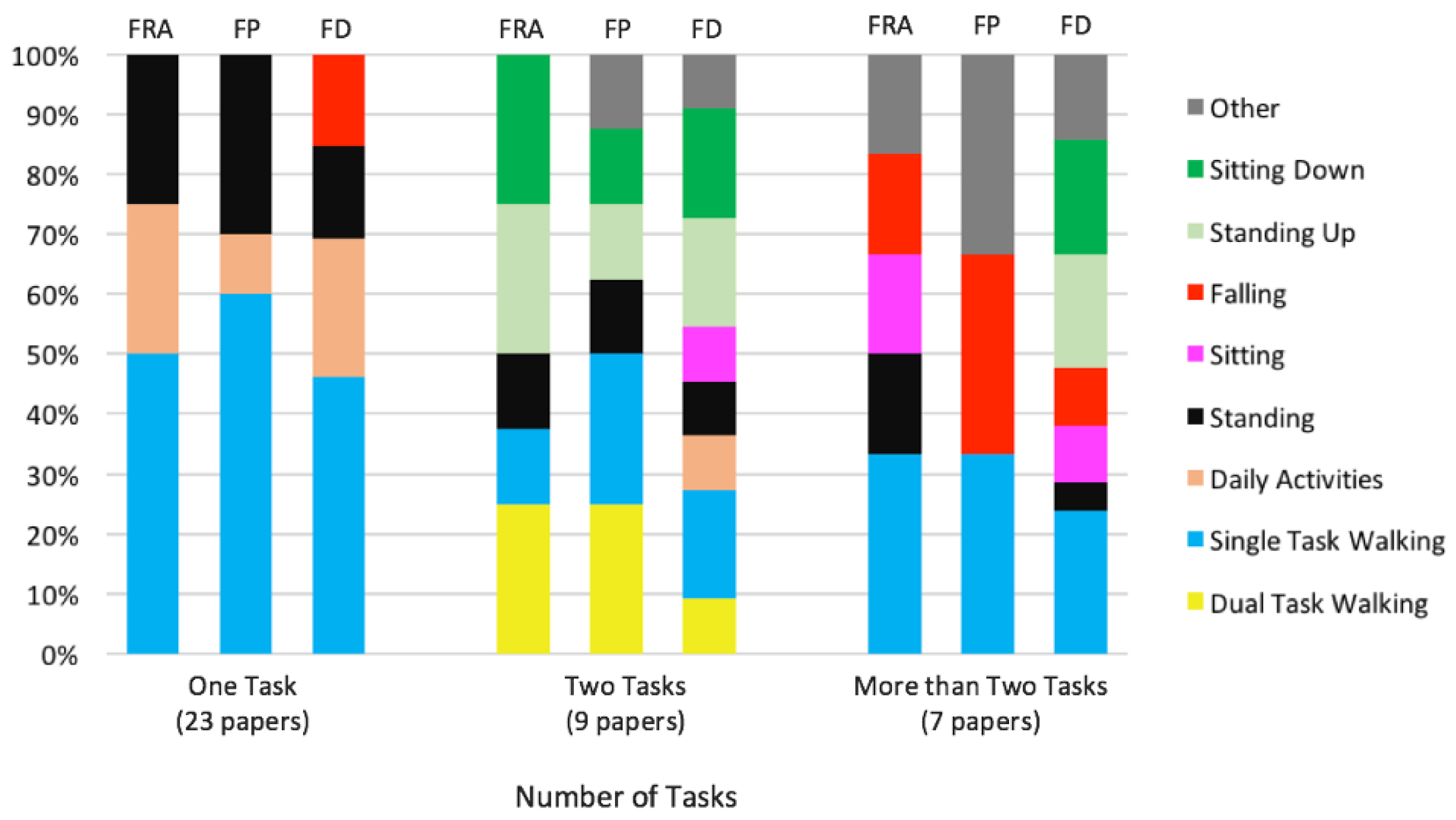
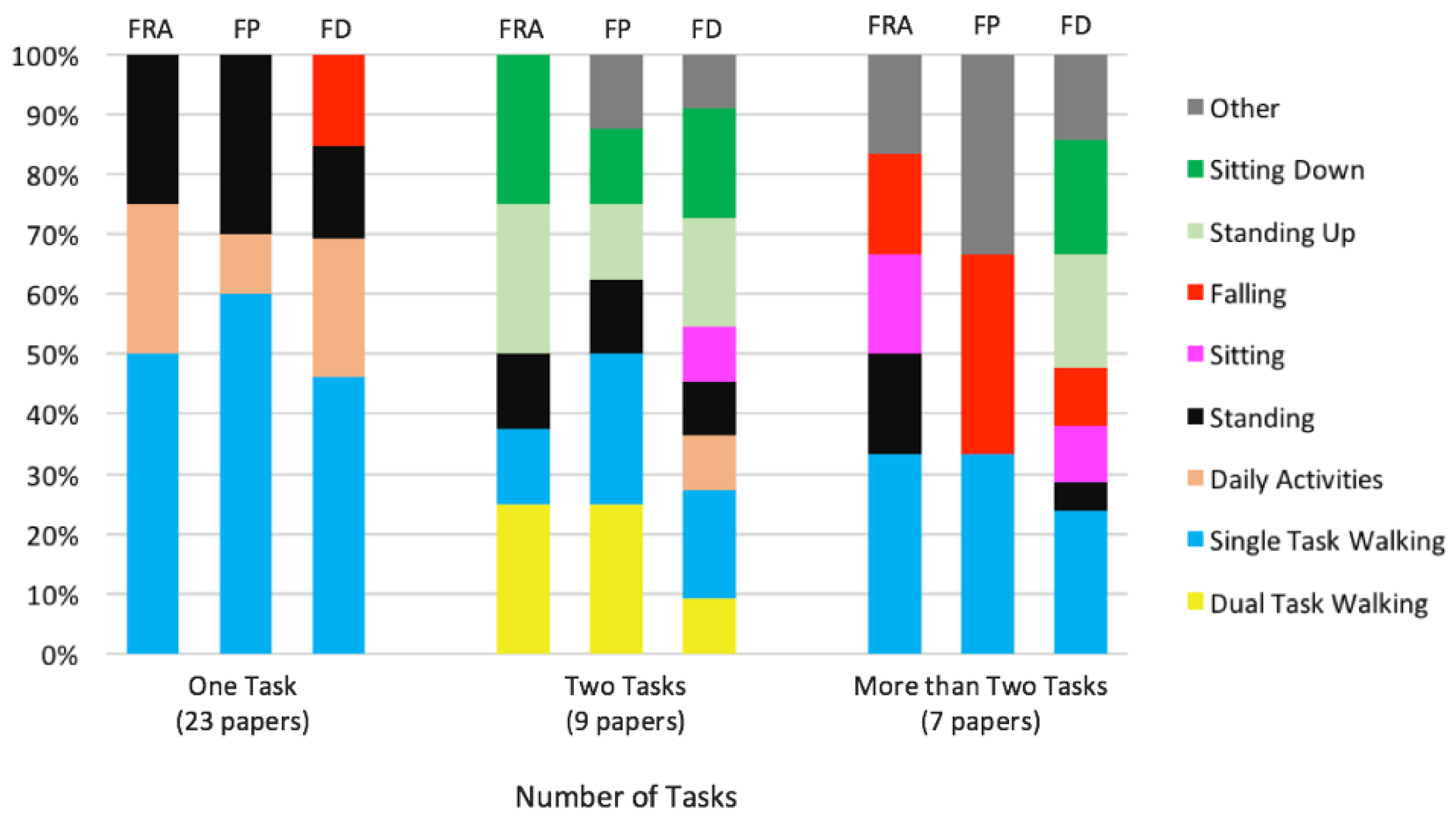
4.4. Tasks
4.4.1. One Task
4.4.2. Two Tasks
4.4.3. More than Two Tasks
5. Conclusions
Funding
Conflicts of Interest
Abbreviations
References
- Amboni, M.; Iuppariello, L.; Lista, I.; Rucco, R.; Varriale, P.; Picillo, M.; Iavarone, A.; Sorrentino, G.; Barone, P. Gait patterns associated with freezing of gait in patients with Parkinson’s disease. Mov. Disord. 2015, 30, S29–S30. [Google Scholar]
- Teasell, R.; McRae, M.; Foley, N.; Bhardwaj, A. The incidence and consequences of falls in stroke patients during inpatient rehabilitation: Factors associated with high risk. Arch. Phys. Med. Rehabil. 2002, 83, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, P.N.; Shumway-Cook, A.; Bamer, A.M.; Johnson, S.L.; Amtmann, D.; Kraft, G.H. Falls in multiple sclerosis. PM R 2011, 3, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Sherrington, C.; Menz, H.B. FALLS in Older People; NICE: London, UK, 2001. [Google Scholar]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- World Health Organizatio (WHO). Global Report on Falls: Prevention in Older Age; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Blake, A.; Morgan, K.; Bendall, M.; Dallosso, H.; Ebrahim, S.; Arie, T.; Fentem, P.; Bassey, E. Falls by elderly people at home: Prevalence and associated factors. Age Ageing 1988, 17, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Prudham, D.; Evans, J.G. Factors associated with falls in the elderly: A community study. Age Ageing 1981, 10, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Reinken, J.; Allan, B.; Martinez, G. Falls in old age: A study of frequency and related clinical factors. Age Ageing 1981, 10, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, B. Clinical and laboratory studies of falls in old people. Prospects for prevention. Clin. Geriatr. Med. 1985, 1, 513–524. [Google Scholar]
- Kannus, P.; Sievänen, H.; Palvanen, M.; Järvinen, T.; Parkkari, J. Prevention of falls and consequent injuries in elderly people. Lancet 2005, 366, 1885–1893. [Google Scholar] [CrossRef]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Moreland, J.D.; Richardson, J.A.; Goldsmith, C.H.; Clase, C.M. Muscle weakness and falls in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2004, 52, 1121–1129. [Google Scholar] [CrossRef] [PubMed]
- Holtzer, R.; Friedman, R.; Lipton, R.B.; Katz, M.; Xue, X.; Verghese, J. The relationship between specific cognitive functions and falls in aging. Neuropsychology 2007, 21, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Rucco, R.; Agosti, V.; Jacini, F.; Sorrentino, P.; Varriale, P.; De Stefano, M.; Milan, G.; Montella, P.; Sorrentino, G. Spatio-temporal and kinematic gait analysis in patients with Frontotemporal dementia and Alzheimer’s disease through 3D motion capture. Gait Posture 2017, 52, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.P.; Redfern, M.S.; Mazumdar, M. Predicting slips and falls considering required and available friction. Ergonomics 1999, 42, 1619–1633. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, M.C.; Cummings, S.R.; Hudes, E.S. Risk factors for injurious falls: A prospective study. J. Gerontol. 1991, 46, M164–M170. [Google Scholar] [CrossRef] [PubMed]
- Oliver, D.; Daly, F.; Martin, F.C.; McMurdo, M.E. Risk factors and risk assessment tools for falls in hospital in-patients: A systematic review. Age Ageing 2004, 33, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P.; Palvanen, M.; Niemi, S.; Parkkari, J. Alarming rise in the number and incidence of fall-induced cervical spine injuries among older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 180–183. [Google Scholar] [CrossRef]
- Davis, J.; Robertson, M.; Ashe, M.; Liu-Ambrose, T.; Khan, K.; Marra, C. International comparison of cost of falls in older adults living in the community: A systematic review. Osteoporosi. Int. 2010, 21, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Peel, N.M.; McClure, R.J.; Hendrikz, J.K. Health-protective behaviours and risk of fall-related hip fractures: a population-based case—Control study. Age Ageing 2006, 35, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for Preventing Falls in Older People Living in The Community; The Cochrane Library: London, UK, 2012. [Google Scholar]
- Cameron, I.D.; Murray, G.R.; Gillespie, L.D.; Robertson, M.C.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Database Syst. Rev. 2010, 1. [Google Scholar] [CrossRef]
- Society, A.G.; Society, G.; Prevention, O.F.; Panel, O.S. Guideline for the prevention of falls in older persons. J. Am. Geriatr. Soc. 2001, 49, 664–672. [Google Scholar] [CrossRef]
- Duarte, M.; Freitas, S.M. Revision of posturography based on force plate for balance evaluation. Braz. J. Phys. Ther. 2010, 14, 183–192. [Google Scholar] [CrossRef]
- Hamacher, D.; Singh, N.; Van Dieen, J.; Heller, M.; Taylor, W. Kinematic measures for assessing gait stability in elderly individuals: A systematic review. J. R. Soc. Interface 2011, 8, 1682–1698. [Google Scholar] [CrossRef] [PubMed]
- Ham, R.; Aldersea, P.; Porter, D. Wheelchair Users and Postural Seating: A Clinical Approach; WB Saunders Company: Philadelphia, PA, USA, 1998. [Google Scholar]
- Pope, P. Posture management and special seating. In Neurological Physiotherapy; Churchill Livingstone: London, UK, 2002. [Google Scholar]
- Terrier, P.; Reynard, F. Effect of age on the variability and stability of gait: A cross-sectional treadmill study in healthy individuals between 20 and 69 years of age. Gait Posture 2015, 41, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, ii7–ii11. [Google Scholar] [CrossRef] [PubMed]
- Lugade, V.; Lin, V.; Chou, L.S. Center of mass and base of support interaction during gait. Gait Posture 2011, 33, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Baltich, J.; von Tscharner, V.; Nigg, B.M. Degradation of postural control with aging. Proc. Instit. Mech. Eng. Part H J. Eng. Med. 2015, 229, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Porter, S.; Nantel, J. Older adults prioritize postural stability in the anterior—Posterior direction to regain balance following volitional lateral step. Gait Posture 2015, 41, 666–669. [Google Scholar] [CrossRef] [PubMed]
- Batista, W.O.; Junior, A.; de Drummond, E.; Porto, F.; Pereira, F.D.; Santana, R.F.; Gurgel, J.L. Influence of the length of institutionalization on older adults’ postural balance and risk of falls: A transversal study. Rev. Lat.-Am. Enferm. 2014, 22, 645–653. [Google Scholar] [CrossRef]
- Liu, K.; Wang, H.; Xiao, J. The multivariate largest Lyapunov exponent as an age-related metric of quiet standing balance. Comput. Math. Methods Med. 2015, 2015, 309756. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Pai, Y.C. Can stability really predict an impending slip-related fall among older adults? J. Biomech. 2014, 47, 3876–3881. [Google Scholar] [CrossRef] [PubMed]
- Lizama, L.E.C.; Pijnappels, M.; Rispens, S.M.; Reeves, N.P.; Verschueren, S.M.; van Dieën, J.H. Mediolateral balance and gait stability in older adults. Gait Posture 2015, 42, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Turcato, A.; Ramat, S. Studying postural sway using wearable sensors: Fall prediction. In Proceedings of the XII Mediterranean Conference on Medical and Biological Engineering and Computing, Chalkidiki, Greece, 27–30 May 2010; pp. 620–623. [Google Scholar]
- Deshmukh, P.M.; Russell, C.M.; Lucarino, L.E.; Robinovitch, S.N. Enhancing clinical measures of postural stability with wearable sensors. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2012, 2012, 4521–4524. [Google Scholar] [PubMed]
- Similä, H.; Immonen, M.; Ermes, M. Accelerometry-based assessment and detection of early signs of balance deficits. Comput. Biol. Med. 2017, 85, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Aminian, K.; Mariani, B.; Paraschiv-Ionescu, A.; Hoskovec, C.; Büla, C.; Penders, J.; Tacconi, C.; Marcellini, F. Foot worn inertial sensors for gait assessment and rehabilitation based on motorized shoes. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2011, 2011, 5820–5823. [Google Scholar] [PubMed]
- Bounyong, S.; Adachi, S.; Ozawa, J.; Yamada, Y.; Kimura, M.; Watanabe, Y.; Yokoyama, K. Fall risk estimation based on co-contraction of lower limb during walking. In Proceedings of the IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 7–11 January 2016; pp. 331–332. [Google Scholar]
- Canning, C.G.; Paul, S.S.; Nieuwboer, A. Prevention of falls in Parkinson’s disease: A review of fall risk factors and the role of physical interventions. Neurodegener. Dis. Manag. 2014, 4, 203–221. [Google Scholar] [CrossRef] [PubMed]
- Okuma, Y. Freezing of gait and falls in Parkinson’s disease. J. Parkinson Dis. 2014, 4, 255–260. [Google Scholar]
- Gunn, H.J.; Newell, P.; Haas, B.; Marsden, J.F.; Freeman, J.A. Identification of risk factors for falls in multiple sclerosis: A systematic review and meta-analysis. Phys. Ther. 2013, 93, 504. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, L.; Gustafson, Y. Patient falls in stroke rehabilitation: A challenge to rehabilitation strategies. Stroke 1995, 26, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Horikawa, E.; Matsui, T.; Arai, H.; Seki, T.; Iwasaki, K.; Sasaki, H. Risk of falls in Alzheimer’s disease: A prospective study. Intern. Med. 2005, 44, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, P.L.; Solomont, J.; Kowall, N.; Hausdorff, J.M. Influence of executive function on locomotor function: Divided attention increases gait variability in Alzheimer’s disease. J. Am. Geriatr. Soc. 2003, 51, 1633–1637. [Google Scholar] [CrossRef] [PubMed]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Review of fall risk assessment in geriatric populations using inertial sensors. J. Neuroeng. Rehabil. 2013, 10, 91. [Google Scholar] [CrossRef] [PubMed]
- Scanaill, C.N.; Carew, S.; Barralon, P.; Noury, N.; Lyons, D.; Lyons, G.M. A review of approaches to mobility telemonitoring of the elderly in their living environment. Ann. Biomed. Eng. 2006, 34, 547–563. [Google Scholar] [CrossRef] [PubMed]
- Shany, T.; Redmond, S.; Marschollek, M.; Lovell, N. Assessing fall risk using wearable sensors: A practical discussion. Z. Gerontol. Geriatr. 2012, 45, 694–706. [Google Scholar] [CrossRef] [PubMed]
- Igual, R.; Medrano, C.; Plaza, I. Challenges, issues and trends in fall detection systems. Biomed. Eng. Online 2013, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xue, M.; Mei, Z.; Bambang Oetomo, S.; Chen, W. A Review of Wearable Sensor Systems for Monitoring Body Movements of Neonates. Sensors 2016, 16, 2134. [Google Scholar] [CrossRef] [PubMed]
- Baloh, R.W.; Fife, T.D.; Zwerling, L.; Socotch, T.; Jacobson, K.; Bell, T.; Beykirch, K. Comparison of static and dynamic posturography in young and older normal people. J. Am. Geriatr. Soc. 1994, 42, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Buatois, S.; Gueguen, R.; Gauchard, G.C.; Benetos, A.; Perrin, P.P. Posturography and risk of recurrent falls in healthy non-institutionalized persons aged over 65. Gerontology 2006, 52, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Whitney, S.L.; Marchetti, G.F.; Schade, A.I. The relationship between falls history and computerized dynamic posturography in persons with balance and vestibular disorders. Arch. Phys. Med. Rehabil. 2006, 87, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Ricci, N.A.; de Faria Figueiredo Gonçalves, D.; Coimbra, A.M.V.; Coimbra, I.B. Sensory interaction on static balance: A comparison concerning the history of falls of community-dwelling elderly. Geriatr. Gerontol. Int. 2009, 9, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Maki, B.E. Gait changes in older adults:maki1997gait predictors of falls or indicators of fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [PubMed]
- Kahle, J.T.; Highsmith, M.J.; Hubbard, S.L. Comparison of nonmicroprocessor knee mechanism versus C-Leg on Prosthesis Evaluation Questionnaire, stumbles, falls, walking tests, stair descent, and knee preference. J. Rehabil. Res. Dev. 2008, 45, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.G.; Dingwell, J.B. Dynamic stability of superior vs. inferior segments during walking in young and older adults. Gait Posture 2009, 30, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Aloqlah, M.; Lahiji, R.; Loparo, K.; Mehregany, M. A headband for classifying human postures. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 31 August–4 September 2010; pp. 382–385. [Google Scholar]
- Bertolotti, G.; Cristiani, A.; Colagiorgio, P.; Romano, F.; Bassani, E.; Caramia, N.; Ramat, S. A Wearable and Modular Inertial Unit for Measuring Limb Movements and Balance Control Abilities. IEEE Sens. J. 2016, 16, 3496–3499. [Google Scholar] [CrossRef]
- Caldara, M.; Locatelli, P.; Comotti, D.; Dellerma, N.; Corenzi, A.; Pessione, M. Application of a wireless BSN for gait and balance assessment in the elderly. In Proceedings of the IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015. [Google Scholar]
- Chen, Y.C.; Lin, Y.W. Indoor RFID gait monitoring system for fall detection. In Proceedings of the 2nd International Symposium on Aware Computing (ISAC), Tainan, Taiwan, 1–4 November 2010; pp. 207–212. [Google Scholar]
- Cheng, J.; Chen, X.; Shen, M. A Framework for Daily Activity Monitoring and Fall Detection Based on Surface Electromyography and Accelerometer Signals. IEEE J. Biomed. Health Inform. 2013, 17, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Cola, G.; Avvenuti, M.; Vecchio, A.; Yang, G.; Lo, B. An On-Node Processing Approach for Anomaly Detection in Gait. IEEE Sens. J. 2015, 15, 6640–6649. [Google Scholar] [CrossRef]
- Crispim, C.; Bathrinarayanan, V.; Fosty, B.; Konig, A.; Romdhane, R.; Thonnat, M.; Bremond, F. Evaluation of a monitoring system for event recognition of older people. In Proceedings of the 10th IEEE International Conference on Advanced Video and Signal Based Surveillance, Krakow, Poland, 27–30 August 2013. [Google Scholar]
- Curone, D.; Bertolotti, G.M.; Cristiani, A.; Secco, E.L.; Magenes, G. A real-time and self-calibrating algorithm based on triaxial accelerometer signals for the detection of human posture and activity. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1098–1105. [Google Scholar] [CrossRef] [PubMed]
- De la Guia Solaz, M.; Bourke, A.; Conway, R.; Nelson, J.; ÓLaighin, G. Real-time low-energy fall detection algorithm with a Programmable Truncated MAC. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2010, 2010, 2423–2426. [Google Scholar] [PubMed]
- Di Rosa, M.; Hausdorff, J.M.; Stara, V.; Rossi, L.; Glynn, L.; Casey, M.; Burkard, S.; Cherubini, A. Concurrent validation of an index to estimate fall risk in community dwelling seniors through a wireless sensor insole system: A pilot study. Gait Posture 2017, 55, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Diraco, G.; Leone, A.; Siciliano, P. In-home hierarchical posture classification with a time-of-flight 3D sensor. Gait Posture 2014, 39, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Luque, F.J.; Zapata, J.; Ruiz, R. A system for ubiquitous fall monitoring at home via a wireless sensor network. In Proceedings of the annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Buenos Aires, Argentina, 1–4 September 2010; pp. 2246–2249. [Google Scholar]
- Ganea, R.; Paraschiv-lonescu, A.; Aminian, K. Detection and classification of postural transitions in real-world conditions. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Gopalai, A.A.; Senanayake, S.A.A. A wearable real-time intelligent posture corrective system using vibrotactile feedback. IEEE/ASME Trans. Mechatron. 2011, 16, 827–834. [Google Scholar] [CrossRef]
- Greene, B.; McGrath, D.; Foran, T.; Doheny, E.; Caulfield, B. Body-worn sensor based surrogates of minimum ground clearance in elderly fallers and controls. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC, Honolulu, HI, USA, 30 August–3 September 2011; pp. 6499–6502. [Google Scholar]
- Hegde, N.; Sazonov, E.S. SmartStep 2.0-A completely wireless, versatile insole monitoring system. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Washington, DC, USA, 9–12 November 2015; pp. 746–749. [Google Scholar]
- Howcroft, J.; Kofman, J.; Lemaire, E.D. Feature selection for elderly faller classification based on wearable sensors. J. Neuroeng. Rehabil. 2017, 14, 47. [Google Scholar] [CrossRef] [PubMed]
- Howcroft, J.; Kofman, J.; Lemaire, E. Prospective fall-risk prediction models for older adults based on wearable sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 1812–1820. [Google Scholar] [CrossRef] [PubMed]
- Howcroft, J.; Kofman, J.; Lemaire, E.D.; McIlroy, W.E. Analysis of dual-task elderly gait in fallers and non-fallers using wearable sensors. J. Biomech. 2016, 49, 992–1001. [Google Scholar] [CrossRef] [PubMed]
- Jian, H.; Chen, H. A portable fall detection and alerting system based on k-NN algorithm and remote medicine. China Commun. 2015, 12, 23–31. [Google Scholar] [CrossRef]
- Jiang, S.; Zhang, B.; Wei, D. The elderly fall risk assessment and prediction based on gait analysis. In Proceedings of the IEEE 11th International Conference on Computer and Information Technology (CIT), Pafos, Cyprus, 31 August–2 September 2011; pp. 176–180. [Google Scholar]
- Karel, J.M.; Senden, R.; Janssen, J.E.; Savelberg, H.; Grimm, B.; Heyligers, I.; Peeters, R.; Meijer, K. Towards unobtrusive in vivo monitoring of patients prone to falling. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 5018–5021. [Google Scholar]
- Micó-Amigo, M.E.; Kingma, I.; Ainsworth, E.; Walgaard, S.; Niessen, M.; van Lummel, R.C.; van Dieën, J.H. A novel accelerometry-based algorithm for the detection of step durations over short episodes of gait in healthy elderly. J. Neuroeng. Rehabil. 2016, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Aminian, K.; Loew, F.; Blanc, Y.; Robert, P.A. Measurement of stand-sit and sit-stand transitions using a miniature gyroscope and its application in fall risk evaluation in the elderly. IEEE Trans. Biomed. Eng. 2002, 49, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, K.; Velipasalar, S. Wearable camera-and accelerometer-based fall detection on portable devices. IEEE Embed. Syst. Lett. 2016, 8, 6–9. [Google Scholar] [CrossRef]
- Paoli, R.; Fernández-Luque, F.J.; Doménech, G.; Martínez, F.; Zapata, J.; Ruiz, R. A system for ubiquitous fall monitoring at home via a wireless sensor network and a wearable mote. Expert Syst. Appl. 2012, 39, 5566–5575. [Google Scholar] [CrossRef]
- Qu, W.; Lin, F.; Wang, A.; Xu, W. Evaluation of a low-complexity fall detection algorithm on wearable sensor towards falls and fall-alike activities. In Proceedings of the IEEE Signal Processing in Medicine and Biology Symposium (SPMB), Philadelphia, PA, USA, 13 December 2014; pp. 1–6. [Google Scholar]
- Sazonov, E.S.; Hegde, N.; Tang, W. Development of SmartStep: An insole-based physical activity monitor. In Proceedings of the 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 7209–7212. [Google Scholar]
- Stone, E.E.; Skubic, M. Unobtrusive, continuous, in-home gait measurement using the Microsoft Kinect. IEEE Trans. Biomed. Eng. 2013, 60, 2925–2932. [Google Scholar] [CrossRef] [PubMed]
- Szurley, J.; Druzgalski, C. A novel approach in remote monitoring and assessment of patient balance. In Proceedings of the Pan American Health Care Exchanges (PAHCE), Mexico City, Mexico, 16–20 March 2009; p. 143. [Google Scholar]
- Tamura, T. Wearable accelerometer in clinical use. In Proceedings of the IEEE-EMBS 27th Annual International Conference of the Engineering in Medicine and Biology Society, Shanghai, China, 17–18 January 2006; pp. 7165–7166. [Google Scholar]
- Tang, Y.; Ran, L.; Li, C. A feasibility study on human gait monitoring using a wearable K-band radar. In Proceedings of the 46th European Microwave Conference (EuMC), London, UK, 4–6 Octomber 2016; pp. 918–921. [Google Scholar]
- Van de Ven, P.; O’Brien, H.; Nelson, J.; Clifford, A. Unobtrusive monitoring and identification of fall accidents. Med. Eng. Phys. 2015, 37, 499–504. [Google Scholar] [CrossRef] [PubMed]
- van Schooten, K.S.; Pijnappels, M.; Rispens, S.M.; Elders, P.J.; Lips, P.; Daffertshofer, A.; Beek, P.J.; van Dieen, J.H. Daily-life gait quality as predictor of falls in older people: A 1-year prospective cohort study. PLoS ONE 2016, 11, e0158623. [Google Scholar] [CrossRef] [PubMed]
- Vincenzo, J.L.; Glenn, J.M.; Gray, S.M.; Gray, M. Balance measured by the sway balance smart-device application does not discriminate between older persons with and without a fall history. Aging Clin. Exp. Res. 2016, 28, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Zhang, Q.; Li, M.; Li, H.; Ning, Y.; Xie, G.; Zhao, G.; Ma, Y.; Gao, X.; Jin, Z. A wearable pre-impact fall early warning and protection system based on MEMS inertial sensor and GPRS communication. In Proceedings of the IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015; pp. 1–6. [Google Scholar]
- Yuan, X.; Yu, S.; Dan, Q.; Wang, G.; Liu, S. Fall detection analysis with wearable MEMS-based sensors. In Proceedings of the 16th International Conference on Electronic Packaging Technology (ICEPT), Changsha, China, 11–14 August 2015; pp. 1184–1187. [Google Scholar]
- Perry, J.; Davids, J.R. Gait analysis: Normal and pathological function. J. Pediatr. Orthop. 1992, 12, 815. [Google Scholar] [CrossRef]
- Doherty, T.J. Invited review: Aging and sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef]
- Schwenk, M.; Mohler, J.; Wendel, C.; D”Huyvetter, K.; Fain, M.; Taylor-Piliae, R.; Najafi, B. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: Baseline results of the Arizona frailty cohort study. Gerontology 2015, 61, 258–267. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Participants (Number/Age) | Number of Sensors | Sensor Type | Sensor Position | Task Type | Goals | Validation | Analysis |
|---|---|---|---|---|---|---|---|---|
| Aloqlah (2010) [63] | (3/n.a.) | 1 | A | HD | STN | FP, FRA | ACC | Both |
| Aminian (2011) [42] | (10/26.1 ± 2.8)&(10/71 ± 4.6) | 3 | A, P, G | FT | SW | FP | Sens , Spec | Dyn |
| Bertolotti (2016) [64] | (18/n.a.) | 4 | A, P, G, M | TR, AR | SU, SD, B | FD | n.a. | Dyn |
| Bounyong (2016) [43] | (52/72 ± 6.1) | 2 | A | LG | SW | FRA | ACC | Dyn |
| Caldara (2015) [65] | (5/31 ± 6)&(4/70.8 ± 7) | 4 | A, P, G, M | TR | SW | FD, FP, FRA | n.a. | Dyn |
| Chen (2010) [66] | (1/n.a.) | 1 | A | FT | SW | FP | Pc | Dyn |
| Cheng (2013) [67] | (10/24 ± 2) | 2 | A, EMG | LG | SW, SU, SD | FD | Sens = , Spec = | Dyn |
| Cola (2015) [68] | (30/32.9 ± 12.2) | 1 | A | TR | SW | FD, FRA | ACC = | Dyn |
| Crispim-Junior (2013) [69] | (29/65) | 1 | C | EXT | SW, DA | FD | Sens = | Dyn |
| Curone (2010) [70] | (6/29.5) | 1 | A | TR | SU, SD, SW | FD | Pc | Both |
| De la Guia Solaz (2010) [71] | (10/23.7 ± 2.2)&(10/77.2 ± 4.3) | 2 | A, P | TR | SU, SD, SW, F | FD | ACC , Pc, | Dyn |
| Deshmukh (2012) [40] | (4/n.a.) | 3 | A, G, M | LG | STN | FRA | n.a. | Static |
| Di Rosa (2017) [72] | (29/71.1 ± 6.9) | 2 | A, P | FT | DA | FRA | ACC | Dyn |
| Diraco (2014) [73] | (18/38 ± 6) | 1 | T | EXT | STN | FD | Pc | Static |
| Fernandez-Luque (2010) [74] | (n.a./n.a.) | 4 | A, P, M, IR | EXT | DA | FD, FRA | n.a. | Dyn |
| Ganea (2012) [75] | (35/54.2 ± 5.7) | 2 | A, G | TR, LG | SU, SD | FD, FP, FRA | ACC = | Dyn |
| Gopalai (2011) [76] | (12/23.45 ± 1.45) | 2 | A, G | TR | STN | FP, FRA | n.a. | n.a. |
| Greene (2011) [77] | (114/71 ± 6.6) | 2 | A, G | LG | SW | FD | n.a. | Dyn |
| Hegde (2015) [78] | (n.a./n.a.) | 3 | A, P, G | FT | n.a. | FD, FRA | n.a. | Dyn |
| Howcroft (2017) [79] | (100/75.5 ± 6.7) | 2 | A, P | TR, HD, LG, FT | SW | FP, FRA | ACC , Sens , Spec | Dyn |
| Howcroft (2017) [80] | (76/75.2 ± 6.6) | 2 | A, P | TR, HD, LG, FT | SW, DW | FP, FRA | ACC , Sens , Spec | Dyn |
| Howcroft (2016) [81] | (100/75.5 ± 6.7) | 2 | A, P | TR, HD, LG, FT | SW, DW | FD, FP, FRA | n.a. | Dyn |
| Jian (2015) [82] | (8/33) | 2 | A, G | TR | F | FD | n.a. | Dyn |
| Jiang (2011) [83] | (48/40) | 3 | A, P, C | n.a. | SW, STN | FP, FRA | n.a. | Dyn |
| Karel (2010) [84] | (41/24 ± 4)&(50/67 ± 5) | 1 | A | TR | SW | FD | Sens , Spec | Dyn |
| Micó-Amigo (2016) [85] | (20/73.7 ± 7.9) | 2 | A, G | TR, LG | SW | FD, FP, FRA | n.a. | Dyn |
| Najafi (2002) [86] | (11/79 ± 6) | 1 | G | TR | SU, SD | FRA | Sens , Spec | Dyn |
| Ozcan (2016) [87] | (n.a./n.a.) | 2 | A, G | TR | n.a. | FD | Sens , Spec | Static |
| Paoli (2011) [88] | (1/n.a.) | >4 | A, P, M, IR | TR | DA | FD | n.a. | Both |
| Qu (2016) [89] | (10/25) | 1 | A | TR | F | FD | ROC curve | Dyn |
| Sazonov (2013) [90] | (1/n.a.) | 2 | A, P | FT | STN, STT, SW | FD, FRA | n.a. | Both |
| Simila (2017) [41] | (42/74.17 ± 5.57) | 1 | A | TR | SW | FP, FRA | Sens , Spec | Dyn |
| Stone (2013) [91] | (15/67) | 1 | K | n.a. | SW | FD | n.a. | Dyn |
| Szurley (2009) [92] | (n.a./n.a.) | 1 | A | TR | n.a. | FP | n.a. | Dyn |
| Tamura (2005) [93] | (6/66.3 ± 5) | 1 | A | TR | SU, SD | FD | Pc | Dyn |
| Tang (2016) [94] | (1/n.a.) | 1 | R | LG | SW, STR | FD, FP | n.a. | Dyn |
| Turcato (2010) [39] | (5/26 ± 6) | 2 | A, W | TR | STN | FP | ACC | Static |
| Van de Ven (2015) [95] | (1 /n.a.) | 2 | A, P | FT | STN, STT | FD | n.a. | Dyn |
| van Schooten (2016) [96] | (319/75.5 ± 6.9) | 1 | A | TR | DA | FD, FP, FRA | n.a. | Dyn |
| Vincenzo (2016) [97] | (57/74.35 ± 6.53) | 1 | A | TR | STN | FD | n.a. | Static |
| Yao (2015) [98] | (9/25) | 3 | A, G, M | TR | SW, F, R | FD, FP, FRA | n.a. | Dyn |
| Yuan (2015) [99] | (n.a./n.a.) | 2 | A, G | TR | F, STT, L | FD | n.a. | Both |
| Task Type | Acronym |
|---|---|
| Standing | STN |
| Single Task Walking | SW |
| Dual Task Walking | DW |
| Standing Up | SU |
| Sitting Down | SD |
| Bending | B |
| Daily Activities | DA |
| Falling | F |
| Running | R |
| Sitting | STT |
| Lying | L |
| Stairs | STR |
| Sensor Position | Anatomical Location | Acronym |
|---|---|---|
| Head | HD | |
| Foot | Shoes, heel | FT |
| Trunk | L3, L5, sternum, waist, pelvis, neck, chest | TR |
| Arm | Wrist, forearm | AR |
| Leg | Thigh, cruris, ankle, shank, knee | LG |
| External | EXT |
| Sensor Type | Acronym |
|---|---|
| Accelerometer | A |
| Gyroscope | G |
| Pressure sensors | P |
| Magnetometer | M |
| Radar | R |
| Time-of-flight (TOF) Camera | T |
| Kinect console | K |
| Wii console | W |
| Electromyography | EMG |
| Infrared sensors | IR |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rucco, R.; Sorriso, A.; Liparoti, M.; Ferraioli, G.; Sorrentino, P.; Ambrosanio, M.; Baselice, F. Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review. Sensors 2018, 18, 1613. https://doi.org/10.3390/s18051613
Rucco R, Sorriso A, Liparoti M, Ferraioli G, Sorrentino P, Ambrosanio M, Baselice F. Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review. Sensors. 2018; 18(5):1613. https://doi.org/10.3390/s18051613
Chicago/Turabian StyleRucco, Rosaria, Antonietta Sorriso, Marianna Liparoti, Giampaolo Ferraioli, Pierpaolo Sorrentino, Michele Ambrosanio, and Fabio Baselice. 2018. "Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review" Sensors 18, no. 5: 1613. https://doi.org/10.3390/s18051613
APA StyleRucco, R., Sorriso, A., Liparoti, M., Ferraioli, G., Sorrentino, P., Ambrosanio, M., & Baselice, F. (2018). Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review. Sensors, 18(5), 1613. https://doi.org/10.3390/s18051613