Technology-Based Feedback and Its Efficacy in Improving Gait Parameters in Patients with Abnormal Gait: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Inclusion Criteria
- -
- Population: Mainly patients with a modified or abnormal gait (i.e., spatiotemporal gait parameters) due to a pathology such as cerebral palsy, hip orthoprosthesis, lower member amputation, knee ligamentoplasty, etc.
- -
- Interventions: application of technology-based feedback (haptic and/or visual and/or acoustic) to assist functional gait recovery as much as possible. The feedback had to be received by the patient directly (external feedback).
- -
- Comparisons: Any comparison between different kinds of feedback (visual, haptic, immediate/concurrent, retarded/terminal, etc.) applied using technology. Or any comparison between technological and non-technological feedback, usual care or an alternative exercise therapy/intervention not based on feedback.
- -
- Outcomes: Any validated measures of parameters or aspects associated to gait, such as: pain, functionality, balance, unload weight bearing, spatiotemporal parameters (speed, cadence, step length), kinematic data (range of movement-ROM) and score by specific gait assessment test or scale (i.e., Up and Go, chair-stand time).
- -
- Study design: Randomised controlled trials (RCTs).
- -
- Measure of methodological quality of RCT: A minimum of 4 points according to PEDro Scale. That is, “fair” and “high” quality studies [32] (see Quality Appraisal).
- -
- Language: Studies reported in English or Spanish.
- -
- Setting: Not limited to a particular setting.
2.3. Data Extraction
2.4. Quality Appraisal
3. Results
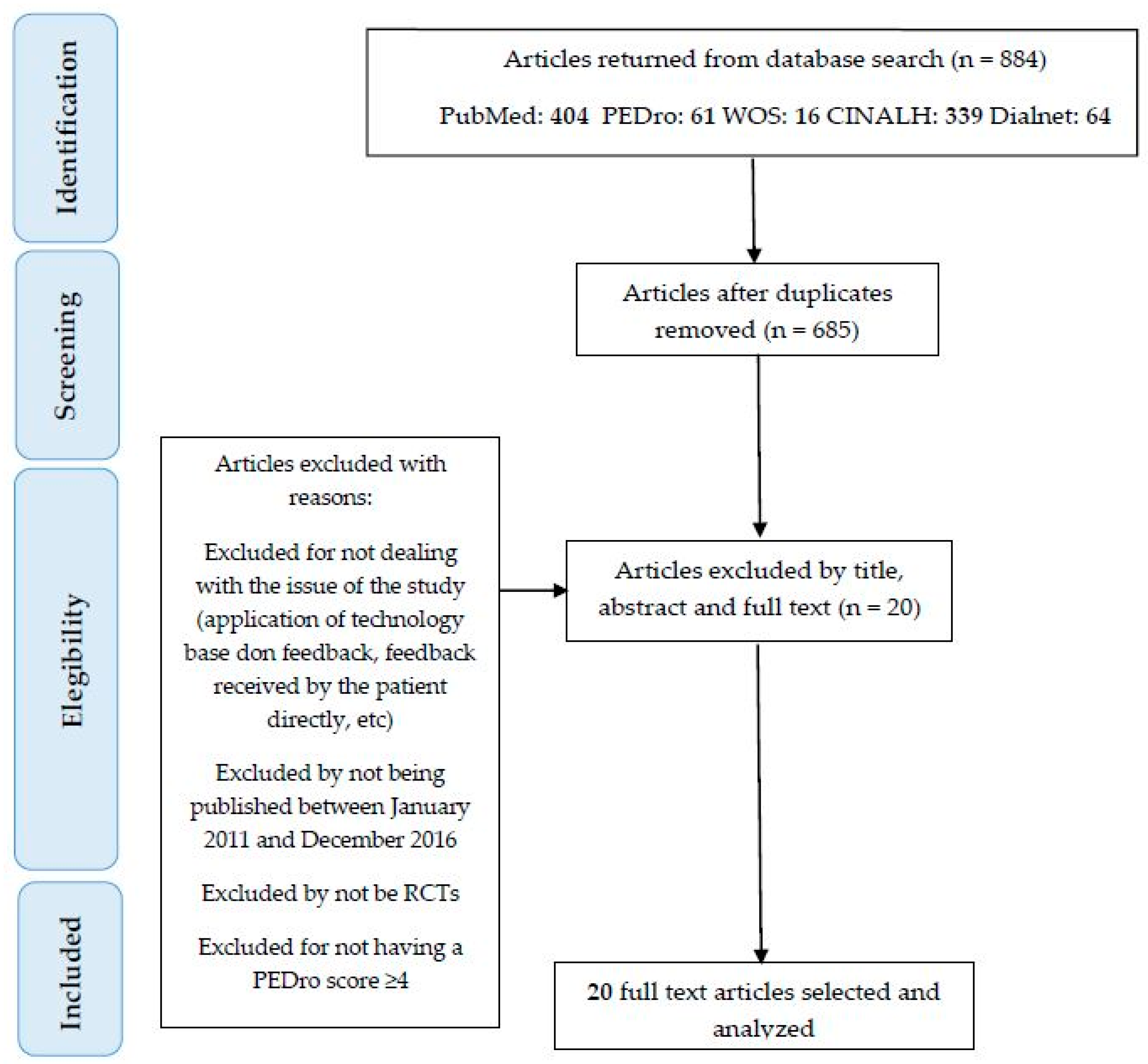
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Quality Assessment
3.4. Participant Characteristics
3.5. Feedback Technology
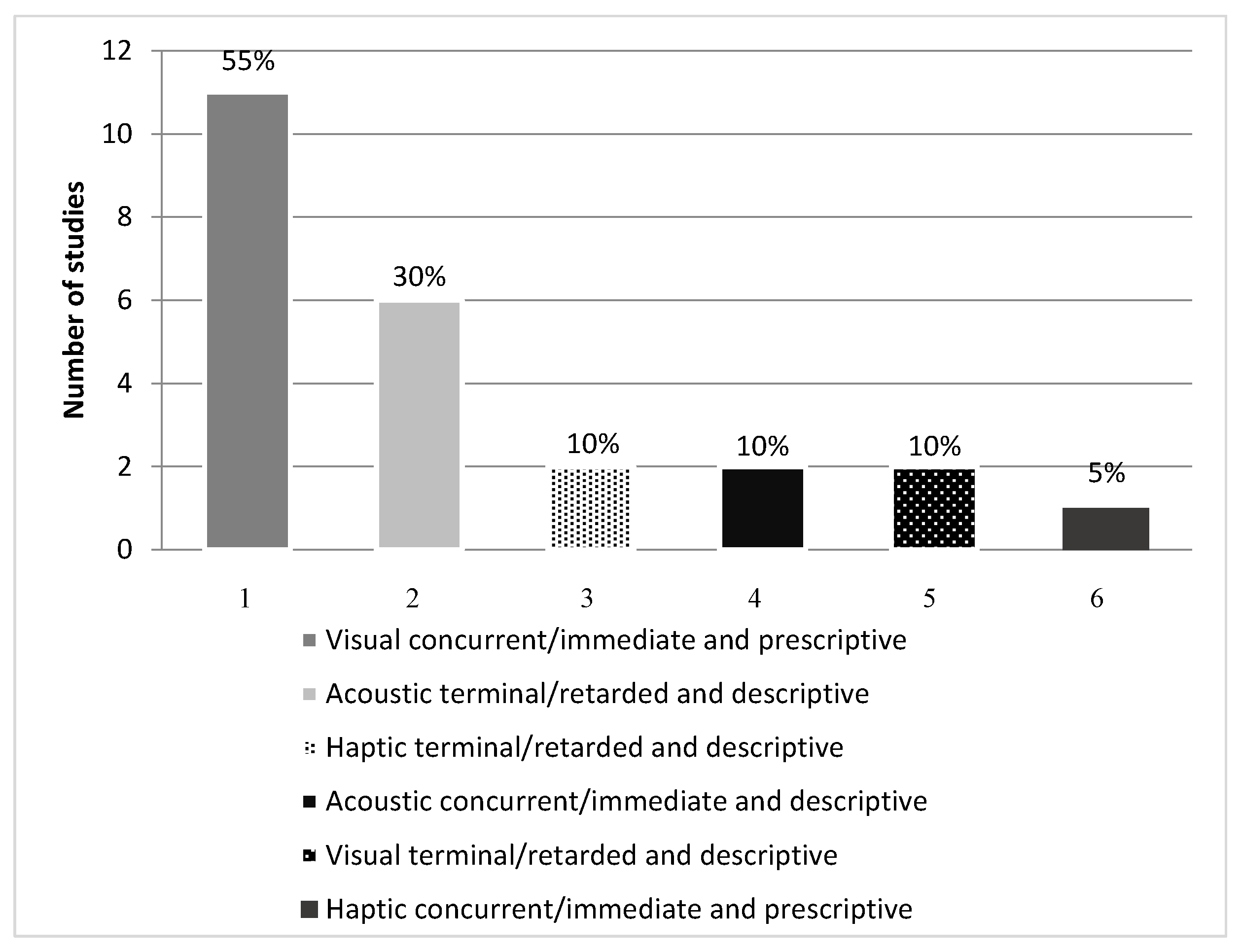
3.6. Feedback Modalities
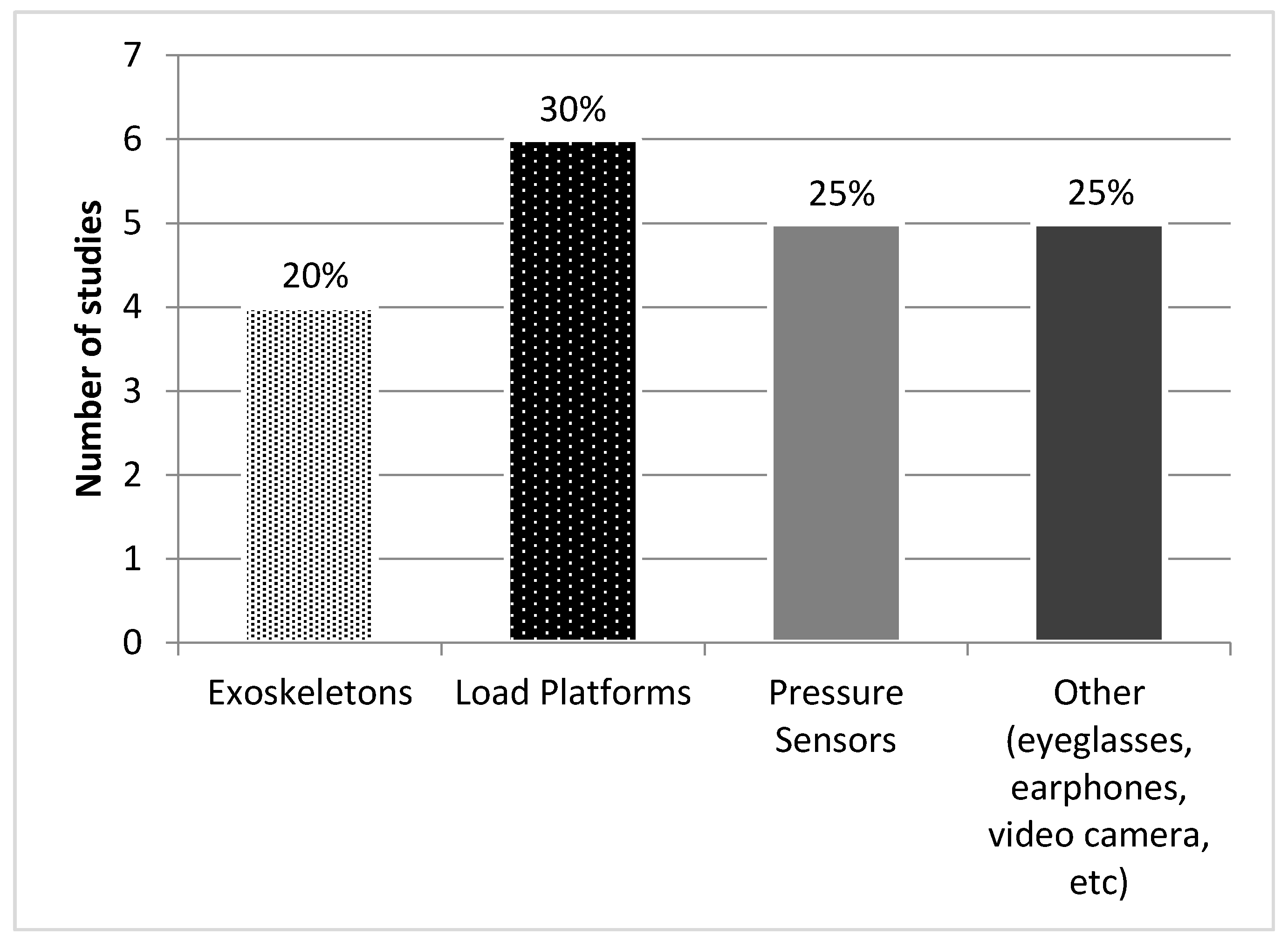
3.7. Assessment Technology
3.8. Interventions and Comparators
3.9. Outcome Measures and Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| 10MWT | 10-m Walk Test |
| ABC | Activities-Specific Balance Confidence |
| ADL | Activities of Daily Living |
| AFO | Ankle Foot Orthosis |
| CG | Control Group |
| CI | Confidence Interval |
| COPD | Chronic Obstructive Pulmonary Disease |
| CP | Cerebral Palsy |
| CT | Computed Tomography |
| ES | Effect Size |
| FAC | Functional Ambulation Classification |
| FC-RATE | Feedback Controlled Robotics Assisted Treadmill Exercise |
| FIM™ | Functional Independence Measure |
| FTS® | Functional Training System |
| FTSTS test | Five Times Sit To Stand |
| GAGT | GAR-Assisted Gait Training Group |
| GAR | Gait-Assistance Robot |
| GCB | “Bathroom Scale” Training Group |
| GCV | “Verbal Instruction” Training Group |
| GFB | “Haptic Biofeedback” Training Group |
| HRpeak | Peak Heart Rate |
| IG | Intervention Group |
| IQR | Barthel Index |
| IT | Information Technology |
| KOOS | Knee Injury and Osteoarthritis Outcome Score |
| KP | Knowledge of Performance |
| KR | Knowledge of Result |
| LCnp | Length of the Cycle of Non-Paretic Limb |
| LCp | Length of the Cycle of Paretic Limb |
| LDCW | Long Distance Corridor Walk |
| LLFDI | Late Life Function and Disability Index |
| LOS | Limit Of Stability |
| MAS | Modified Ashworth Scale |
| MRI | Magnetic Resonance Imaging |
| N | Total Sample |
| NEA | Normalized Error Area |
| OA | Osteoarthritis |
| OCGT | Overground Conventional Gait Training Group |
| Ppeak | Peak Work Rate |
| PBWS | Partial Body Weight Supported |
| PD | Parkinson´s Disease |
| RATE | Robotics Assisted Treadmill Exercise |
| RCTs | Randomised Controlled Trials |
| RERpeak | Peak Respiratory Exchange Ratio |
| Rfpeak | Peak Respiratory Rate |
| ROM | Range of Movement |
| SD | Standar Deviation |
| STFnp | Stance Phase of the Non-Paretic Limb |
| STFp | Stance Phase of the Paretic Limb |
| STP | Stance Time Period |
| SWFnp | Swing Phase of the Non-Paretic Limb |
| SWFp | Swing Phase of the Paretic Limb |
| Terr | Normalized Error in the Stride Period |
| TUG test | Timed Up and Go |
| UPDRS | United Parkinson´s Disease Rating Scale |
| VEpeak | Peak Ventilation Rate |
References
- Chamorro-Moriana, G.; Ridao-Fernández, C.; Ojeda, J.; Benítez-Lugo, M.; Sevillano, J.L. Reliability and validity study of the Chamorro Assisted Gait Scale for people with sprained ankles, walking with forearm crutches. PLoS ONE 2016, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chamorro-Moriana, G.; Rebollo-Roldán, J.; Jiménez-Rejano, J.J.; Chillón-Martínez, R.; Suárez-Serrano, C. Design and validation of GCH System 1.0 which measures the weight-bearing exerted on forearm crutches during aided gait. Gait Posture 2013, 37, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Whittle, M.W. Gait Analysis: An Introduction, 3rd ed.; Butterworth-Heinemann: Oxford, MS, USA, 2003; pp. 140–142. ISBN 9780702039225. [Google Scholar]
- Van Den Noort, J.C.; Steenbrink, F. Real time visual feedback for gait retraining: Toward application in knee osteoarthritis. Med. Biol. Eng. Comput. 2015, 53, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Druzbicki, M.; Guzik, A.; Przysada, G.; Kwolek, A.; Brzozowska-Magoń, A. Efficacy of gait training using a treadmill with and without visual biofeedback in patients after stroke: A randomized study. J. Rehabil. Med. 2015, 47, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Agresta, C.; Hall, J. Gait Retraining for Injured and Healthy Runners using Augmented Feedback: A Systematic Literature Review. J. Orthop. Sports Phys. Ther. 2015, 45, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Kim, Y.; Cha, Y.; In, T.; Hur, Y.; Chung, Y. Effects of gait training with a cane and an augmented pressure sensor for enhancement of weight bearing over the affected lower limb in patients with stroke : A randomized controlled pilot study. Clin. Rehabil. 2015, 29, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Isakov, E. Gait rehabilitation: A new biofeedback device for monitoring and enhancing weight-bearing over the affected lower limb. Eura Medic. 2007, 43, 21–26. [Google Scholar]
- Basta, D.; Rossi-Izquierdo, M.; Soto-Varela, A.; Greters, M.E.; Bittar, R.S.; Steinhagen-Thiessen, E.; Eckardt, R.; Harada, T.; Goto, F.; Ogawa, K.; et al. Efficacy of a vibrotactile neurofeedback training in stance and gait conditions for the treatment of balance deficits: A double-blind, placebo-controlled multicenter study. Otol. Neurotol. 2011, 32, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- Zanotto, D.; Rosati, G.; Spagnol, S.; Stegall, P.; Agrawal, S.K. Effects of Complementary Auditory Feedback in Robot-Assisted Lower Extremity Motor Adaptation. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 775–786. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.A.; Glass, N.A.; Teran-Yengle, P.; Singh, B.; Wallace, R.B.; Yack, H.J. Intensive Gait Training for Older Adults with Symptomatic Knee Osteoarthritis. Am. J. Phys. Med. Rehabil. 2015, 94, 848–858. [Google Scholar] [CrossRef] [PubMed]
- Nanhoe-Mahabier, W.; Allum, J.H.; Pasman, E.P.; Overeem, S.; Bloem, B.R. The effects of vibrotactile biofeedback training on trunk sway in Parkinson’s disease patients. Parkinsonism Relat. Disord. 2012, 18, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Fernández, R.; Rodríguez, B.; Barcia, B.; Souto, S.; Chouza, M.; Martínez, S. Generalidades sobre Feedback (o retroalimentación). Fisioterapia 1998, 20, 3–11. [Google Scholar]
- Ochi, M.; Wada, F.; Saeki, S.; Hachisuka, K. Gait training in subacute non-ambulatory stroke patients using a full weight-bearing gait-assistance robot: A prospective, randomized, open, blinded-endpoint trial. J. Neurol. Sci. 2015, 353, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Quinzaños Fresnedo, J.; Sahagún Olmos, R.C.; León Hernández, S.R.; Pérez Zavala, R.; Quiñones Uriostegui, I.; Solano Salazar, C.J.; Cruz Lira, R.T.; Tinajero Santana, M.C. Efectos a corto plazo del entrenamiento de la marcha en una órtesis robótica (Lokomat®) con retroalimentación auditiva en pacientes con lesión medular incompleta crónica. Rehabilitacion 2015, 49, 30–37. [Google Scholar] [CrossRef]
- Stoller, O.; de Bruin, E.D.; Schindelholz, M.; Schuster-Amft, C.; de Bie, R.A.; Hunt, K.J. Efficacy of Feedback-Controlled Robotics-Assisted Treadmill Exercise to Improve Cardiovascular Fitness Early After Stroke. J. Neurol. Phys. Ther. 2015, 39, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Baram, Y.; Lenger, R. Gait Improvement in Patients with Cerebral Palsy by Visual and Auditory Feedback. Neuromodulation: Technol. Neural Interface 2012, 15, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Brasileiro, A.; Gama, G.; Trigueiro, L.; Ribeiro, T.; Silva, E.; Galvão, É.; Lindquist, A. Influence of visual and auditory biofeedback on partial body weight support treadmill training of individuals with chronic hemiparesis: A randomized controlled clinical trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 49–58. [Google Scholar] [PubMed]
- Byl, N.; Zhang, W.; Coo, S.; Tomizuka, M. Clinical impact of gait training enhanced with visual kinematic biofeedback: Patients with Parkinson’s disease and patients stable post stroke. Neuropsychologia 2015, 79, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.A.; Takacs, J.; Hart, K.; Massong, E.; Fechko, K.; Biegler, J. Comparison of mirror, raw video, and real-time visual biofeedback for training toe-out gait in individuals with knee osteoarthritis. Arch. Phys. Med. Rehabil. 2014, 95, 1912–1917. [Google Scholar] [CrossRef] [PubMed]
- Ki, K.I.; Kim, M.S.; Moon, Y.; Choi, J.D. Effects of auditory feedback during gait training on hemiplegic patients’ weight bearing and dynamic balance ability. J. Phys. Ther. Sci. 2015, 27, 1267–1269. [Google Scholar] [CrossRef] [PubMed]
- Lipsitz, L.A.; Lough, M.; Niemi, J.; Travison, T.; Howlett, H.; Manor, B. A shoe insole delivering subsensory vibratory noise improves balance and gait in healthy elderly people. Arch. Phys. Med. Rehabil. 2015, 96, 432–439. [Google Scholar] [CrossRef] [PubMed]
- El-Tamawy, M.; Darwish, M.; Khallaf, M. Effects of augmented proprioceptive cues on the parameters of gait of individuals with Parkinson′s disease. Ann. Indian Acad. Neurol. 2012, 15, 267. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.; Mountain, G.; Hammerton, J. A review of the evidence underpinning the use of visual and auditory feedback for computer technology in post-stroke upper-limb rehabilitation. Disabil. Rehabil. Assist. Technol. 2011, 6, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Thikey, H.; Grealy, M.; van Wijck, F.; Barber, M.; Rowe, P. Augmented visual feedback of movement performance to enhance walking recovery after stroke: Study protocol for a pilot randomised controlled trial. Trials 2012, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.C.; DeLuke, L.; Buerba, R.; Fan, R.E.; Zheng, Y.J.; Leslie, M.P.; Baumgaertner, M.R.; Grauer, J.N. Haptic biofeedback for improving compliance with lower-extremity partial weight bearing. Orthopedics 2014, 37, e993–e998. [Google Scholar] [CrossRef] [PubMed]
- Chamorro-Moriana, G.; Sevillano, J.L.; Ridao-Fernández, C. A compact forearm crutch based on force sensors for aided gait: Reliability and validity. Sensors 2016, 16, 925. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, D.H.; Bech, S.; Begault, D.R.; Adelstein, B.D. The relative importance of visual, auditory, and haptic information for the user’s experience of mechanical switches. Perception 2009, 38, 1560–1571. [Google Scholar] [CrossRef] [PubMed]
- Lefmann, S.; Russo, R.; Hillier, S. The effectiveness of robotic-assisted gait training for paediatric gait disorders: Systematic review. J. Neuroeng. Rehabil. 2017, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.A.; Chevidikunnan, M.F.; Khan, F.R.; Gaowgzeh, R.A. Effectiveness of knowledge of result and knowledge of performance in the learning of a skilled motor activity by healthy young adults. J. Phys. Ther. Sci. 2016, 28, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef]
- Yamato, T.P.; Maher, C.; Koes, B.; Moseley, A. The PEDro scale had acceptably high convergent validity, construct validity, and interrater reliability in evaluating methodological quality of pharmaceutical trials. J. Clin. Epidemiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Herbert, R.; Maher, C.; Moseley, A. PEDro. A database of randomized trials and systematic reviews in physiotherapy. Man Ther. 2000, 5, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [PubMed]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Academia and Clinic Annals of Internal Medicine Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Annu. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson’s disease: A pilot randomized controlled trial. Parkinsonism Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Khallaf, M.E.; Gabr, A.M.; Fayed, E.E. Effect of Task Specific Exercises, Gait Training, and Visual Biofeedback on Equinovarus Gait among Individuals with Stroke: Randomized Controlled Study. Neurol. Res. Int. 2014. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Mak, M.K.Y. Balance and Gait Training with Augmented Feedback Improves Balance Confidence in People with Parkinson’s Disease. Neurorehabil. Neural Repair 2014, 28, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Sungkarat, S.; Fisher, B.E.; Kovindha, A. Efficacy of an insole shoe wedge and augmented pressure sensor for gait training in individuals with stroke: A randomized controlled trial. Clin. Rehabil. 2011, 25, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Won, S.H.; Kim, J.C.; Oh, D.W. Effects of a novel walking training program with postural correction and visual feedback on walking function in patients with post-stroke hemiparesis. J. Phys. Ther. Sci. 2015, 27, 2581–2583. [Google Scholar] [CrossRef] [PubMed]
- Tzetzis, G.; Votsis, E.; Kourtessis, T. The effect of different corrective feedback methods on the outcome and self confidence of young athletes. J. Sports Sci. Med. 2008, 7, 371–378. [Google Scholar] [PubMed]
- Sardini, E.; Serpelloni, M.; Lancini, M. Wireless Instrumented Crutches for Force and Movement Measurements for Gait Monitoring. IEEE Trans. Instrum. Meas. 2015, 64, 3369–3379. [Google Scholar] [CrossRef]
- Tuttle, N.; Jacuinde, G. Design and Construction of a Novel Low-Cost Device to Provide Feedback on Manually Applied Forces. J. Orthop. Sport Phys. Ther. 2011. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Pohl, P.S.; Cardinale, C.; Green, A.; Scholtz, L.; Waters, C. Learning a partial-weight-bearing skill: Effectiveness of two forms of feedback. Phys. Ther. 1996, 76, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.G.; Lehmann, J. Training procedures and biofeedback methods to achieve controled partial weight bearing: An assessment. Arch. Phys. Med. Rehabil. 1975, 56, 449–455. [Google Scholar] [PubMed]
- Salmoni, A.W.; Schmidt, R.A. Knowledge of results and motor learning: A review and critical reappraisal. Psychol. Bull. 1984, 95, 355–386. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, R.; Rauter, G.; Riener, R.; Wolf, P. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: A review. Psychon. Bull. Rev. 2013, 20, 21–53. [Google Scholar] [CrossRef] [PubMed]
- Sülzenbrück, S.; Heuer, H. Type of visual feedback during practice influences the precision of the acquired internal model of a complex visuo-motor transformation. Ergonomics 2011, 54, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wu, T.; Xu, Z.; Gu, X. A pilot study of post-total knee replacement gait rehabilitation using lower limbs robot-assisted training system. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Kloos, A.D.; Kegelmeyer, D.A.; White, S. The impact of different types of assistive devices on gait measures and safety in Huntington’s disease. PLoS ONE 2012. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.S.; Russell, D.M.; Van Lunen, B.L.; Colberg, S.R.; Morrison, S. The impact of speed and time on gait dynamics. Hum. Mov. Sci. 2017, 54, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, P.R.P.; Silva, P.L.P.; Avelar, B.S.; Chagas, P.S.C.; Oliveira, L.C.P.; Mancini, M.C. Assessment of gait in toddlers with normal motor development and in hemiplegic children with mild motor impairment: A validity study. Brazilian J. Phys. Ther. 2013, 17, 359–366. [Google Scholar] [CrossRef]
- Yang, C.C.; Hsu, Y.L.; Shih, K.S.; Lu, J.M. Real-time gait cycle parameter recognition using a wearable accelerometry system. Sensors 2011, 11, 7314–7326. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: All primary data were extracted from the referenced sources. Full search strategy available from the authors on request. |




{kind=link}
{kind=link}
{kind=link}
| Terms and Strategies | Identifier |
|---|---|
| feedback or biofeedback or neurofeedback or proprioception | 1 |
| treatment or program * or exercise * or rehabilit * or training or educat * or “stimulation training” or teaching or learning | 2 |
| software or program * or technology or “biomedical technology” or system | 3 |
| gait or walking or ambulation or locomotion or “stair navigation” | 4 |
| Randomiza * or study or “clinical trial” | 5 |
| Trata * or program * or rehabilit * | 6 |
| feedback or biofeedback or neurofeedback or retroalimentación | 7 |
| marcha or ambul * or locomoción | 8 |
| Database | Search Strategy | Simplified Strategy |
|---|---|---|
| PubMed | (treatment or program * or exercise * or rehabilit * or training or educat * or “stimulation training” or teaching or learning) and (feedback or biofeedback or neurofeedback or proprioception) and (gait or walking or ambulation or locomotion or “stair navigation”) and (software or program * or technology or “biomedical technology” or system) | 2 and 1 and 4 and 3 |
| PEDro | feedback and gait | 1 and 4 |
| WOS | (feedback or biofeedback or neurofeedback or proprioception) and (gait or walking or ambulation or locomotion or “stair navigation”) and (software or program * or technology or “biomedical technology” or system) and (randomiza * or study or “clinical trial”) | 1 and 4 and 3 and 5 |
| CINAHL | (feedback or biofeedback or neurofeedback or proprioception) and (gait or walking or ambulation or locomotion or “stair navigation”) | 1 and 4 |
| Dialnet | (trata * or program * or rehabilit *)and (feedback or biofeedback or neurofeedback or retroalimentación) and (marcha or ambul * or locomoción) | 6 and 7 and 8 |
| Study Characteristics | Participant Characteristics | Feedback Technology/Feedback Modality | Intervention and Comparison | Outcomes Measurements |
|---|---|---|---|---|
| 1. Baram, Y.; 2012 [17] To study the effects of gait training with visual and auditory feedback cues on the walking abilities of patients with gait disorders due to cerebral palsy (CP) | N 1 = 35 Sex = 20 female (57.14%); 15 male (42.85%) Age = 12.2 ± 6.2 years Inclusion criteria: not specified Exclusion criteria: not specified | Eyeglasses with virtual reality/Visual prescriptive and concurrent (KP 2) Earphones with a clicking sound/Acoustic descriptive and terminal (KR 3) Assessment Technology: Accelerometer | CG 4 visual (n = 7)/CG auditory (n = 8): healthy individuals walk on a 10 m track without technological assistance. IG 5 visual feedback (n = 10): CP patients walk on a 10 m track with transversal lines (virtual reality) which change according to gait. IG auditory feedback (n = 10): CP patients walk on a 10m track while a “clip” is heard at each step. Frequency and duration: measurement before exercise without device, after 20´exercise and after 20´rest and again without the device. | Average Improvement (95% CI 6): IG visual feedback: Significant and effective (*): Walking Speed (m/s), Stride Length (m) Not significant: None IG auditory feedback: Significant and effective: Walking Speed (m/s) Not significant: Stride Length (m) |
| 2. Brasileiro, A. et al., 2015 [18] Immediate effects of visual/auditory biofeedback, combined with partial body weight supported (PBWS) treadmill training on the gait of people with chronic hemiparesis | N = 30 Sex = 12 female (40%); 18 male (60%) Age = 56.4 ± 6.9 years Inclusion criteria: chronic stroke status with hemiparesis, capable of walking with assistance or auxiliary aparatus, low or moderate velocity, free cognitive capacity Exclusion criteria: other visual and/or auditory neurological and orthopedic pathologies, hypertension during performance, not understanding instructions | Gait Trainer® System 2 y Biodex Unweighting System/Visual prescriptive and concurrent (KP) a Metronome Assessment Technology: 8-camera based motion capture system at 120 MHz with tracking markers located at the pelvis, thigh, leg and foot | CG (n = 10): gait training with parallel bars IG I (n = 10): idem + partial unweighting system and visual feedback for symmetry and stride length IG II (n = 10): idem + partial unweighting system and an acoustic stimulus (“beep” to a cadence of 115%) Frequency and duration: sessions of 20 min, two minute rest until heartbeat frequency reaches 75% | Pre-test vs. Post-test (95% CI): Spatiotemporal gait variables: Significant and effective: None Not significant: Speed (m/s), Stride length (m), Cadence (steps/min) Angular gait variables: Significant and effective: None Significant and not effective: Range Of Motion (ROM) Hip (°), ROM ankle (°) Not significant: ROM Knee (°) |
| 3. Byl et al., 2015 [19] evaluate if visual and kinematic feedback provided during supervised gait training would interfere or enhance mobility, endurance, balance, strength and flexibility in older individuals more than one year post stroke or Parkinson’s disease(PD) | N = 24 Sex = 13 female (54.2%); 11 male (45.8%) Age = 30–75 years Inclusion criteria: abnormal gait one year after stroke or Parkinson’s; speak English or use an interpreter; able to follow instructions; motivation and ability to walk a minimum of 100 steps Exclusion criteria: Not specified | iPad® with program LabVIEW/Visual prescriptive and concurrent (KP) Assessment Technology: Pressure sensors (shoe pad) Joint angle sensors (accelerometer, magnetometer and gyroscope) | CG (n = 12): conventional gait therapy (stairs, fitball, theraband, etc.) IG (n = 12): idem + visual cinematic feedback Frequency and duration: from 6 to 8 weeks with an average of 12 sessions of 90 min each. Encouraged to walk and take part in activities of daily living (ADL) | Post exercise–baseline difference scores: CG compared to IG (ES 7) Significant and effective: Gait Speed—10 m walk (m/s), Step length (m), Tinetti Score, Berg Balance, Strength (lbs) (affected), Strength (lbs) (unaffected), ROM (deg) (affected), ROM (deg) (unaffected) Not significant: 6 min walk (cm), Five Times Sit to Stand (FTSTS) Test (s), Timed Up and Go (TUG) (s) |
| 4. Druzbicki, M. et al., 2015 [5] Effects of gait training using a treadmill with and without visual biofeedback in patients in the late period after stroke, and to compare both training methods | N = 50 Sex = 18 female (36%); 32 male (64%) Mean Age = 62 years (range 38–79 years). Inclusion criteria: ischemic stroke, minimum 6 months walking, without rehabiliation for at least 6 months, autonomous gait, Brunnstrom Scale: 3–4, Ashworth ≤ 1 (lower limb musculature), Rankin Scale (disability): 3 Exclusion criteria: unstable hemodynamics, peripheral vascular disease, Mini Mental Test < 20 (cognition), significant gait disorders | Gait Trainer® System 2/Visual prescriptive and concurrent (KP) Signal confirming correct execution/Acoustic descriptive and terminal (KR) a Treadmill Assessment Technology: SMART de BTS Bioengineering (6-camera based system at 120 MHz with tracking markers located at the sacrum, pelvis, femur, fibula and foot) | CG (n = 25): conventional physiotherapy and treadmill program (balance, active and breathing exercises) IG (n = 25): idem + visual feedback (locates the position of the foot and where it should go) Frequency and duration: 15 to 20 min on the treadmill, 1 ½ hour sessions for 10 days plus two weeks of basic physiotherapy | Baseline—post-exercise Significant and effective: Stance phase of the non-paretic limb (STFnp) (% of cycle), Swing phase of the non-paretic limb (SWFnp) (% of cycle), Lenght of the cycle of non-paretic limb (LCnp) (%) Not significant: Cadence (steps/min), Velocity (m/s), Stance phase of the paretic limb (STFp) (% of cycle), Swing phase of the paretic limb (SWFp), Length of the cycle of paretic limb (LCp) (%), 10-m walk test (10MWT) (m/s), 2-min test (m), Test Up and Go (TUG) (s) |
| 5. El-Tamawy et al., 2012 [23] To determine the influence of paired proprioceptive cues on gait parameters of individuals with Parkinson´s Disease (PD) | N = 30 Sex = 9 female (30%); 21 male (70%) Age = 62.5 ± 6.1 years Inclusion criteria: walk independently for 6 min continuously on the treadmill, United Parkinson´s Disease Rating Scale (UPDRS) ADL/motor: light-moderate disability, diagnosed 3–5 years earlier, stable medication, ability to give informed consent Exclusion criteria: another gait-altering neuro-muscular-skeletal disorder; uncontrolled blood pressure, cardiovascular disease | Pressure sensor in the toe (OPTEC Co. Ltd., Japan)/Haptic prescriptive and concurrent (KR) a Treadmill Assessment Technology: Qualysis ProReflex movement capture (Qualysis Medical AB, Sweden) | CG (n = 15): conventional treatment (stretching, balance, transfers, etc.) IG (n = 15): Proprioceptive neuromuscular facilitation techniques + vibratory feedback (are activated when the foot is in the swing phase) + conventional treatment Frequency and duration: 3 sessions per week for 8 weeks. CG: sessions of 45´; IG: sessions of 51´–70´ | Baseline—Post-exercise Spatiotemporal Parameters of Gait: Significant and effective: Cadence (step/min), Stride Length (m), Walking Speed (km/h), Walking Distance (km) Not significant: None Lower Limb Angular Excursion: Significant and effective: Hip Flexion (°), Knee Flexion (°), Ankle Dorsiflexion (°) Not significant: None |
| 6. Fu, M.C. et al., 2014 [26] To assess a novel method of using real-time haptic (vibratory/vibrotactile) biofeedback to improve compliance with instructions for partial weight bearing | N = 30 Sex = 14 female (46.7%); 16 male (53.3%) Age = 22 to 32 years Inclusion criteria: good health, walk without assistance, coordination and strength of upper limbs for walking with sticks Exclusion criteria: restriction in lower limbs for bearing weight and impossibility of using sticks | Haptic feedback belt with 3 vibration motors (axle-less vibration motors Pololu 10 mm P/N 1636) + Processing unit (Arduino Nano, Italy) to know the moment at which to apply the feedback/Haptic descriptive and terminal (KR) Assessment Technology: Force plate with 4 pressure sensors in a boot (Sparkfun Electronics, SEN-10245) SmartStep System (for the dynamic validation of the system) | Participants instructed to unload lower limbs 25 lb (range accepted from 15 to 35 lb). Forearm crutches and systems of sensors are used. “Haptic Biofeedback” Training Group (GFB) (n = 10): receive vibrotactile signal if acceptable range is exceeded “Verbal Instruction” Training Group (GCV) (n = 10) “Bathroom Scale” Training Group (GCB) (n = 10) Frequency and duration: first take 50 practice steps | Comparison between GCV, GCB y GFB Significant and effective: Load on the boot (lb), Percentage of participants’ body weight (%) Not significant: None |
| 7. Ginis, P. et al., 2016 [38] Pilot RCT. To test the feasibility of training with a smartphone application (CuPiD system) in the home environment, and to discover the differential effects of CuPiD training versus conventional home-based gait intervention on gait, balance and health-related quality of life (HR-QoL) in Parkinson´s Disease (PD) | N = 38 Sex = Not specified Age = Not specified Inclusion criteria: walk for 10 min continuously; score of 24 or higher on Montreal Cognitive Assessment (MoCA); Hoehn & Yahr Stage II to III in ONstate and stable PD medication Exclusion criteria: severe medical conditions affecting gait other than PD, hearing or visual problems precluding benefiting from auditory feedback and likely to change medication regime during the course of the study. | CuPiD system: Smartphone (Galaxy S3-mini, Samsung, Korea) Docking station Two inertial measurement units (IMUs) (EXLs3, EXEL, srl., Italy) Applications used in this study: Instrumented cueing for freezing of gait training (FOG-cue app) Audiobiofeedback (ABF-gait app)/Acoustic descriptive and concurrent (KP) Assessment Technology: Earphones or smartphone´s speaker | CG (n = 18): to walk without feedback devices IG (n = 20): idem + feedback devices (ABF-gait app + FOG-cue app) Frequency and duration: 30 min walking, 3 sessions/week for 2 weeks | Pre-test vs. Post-test Not significant: Gait speed (m/s), Stride length (m), Four Square Step Test (FSST) (s), 2 Minute Walk Test (2MWT), MiniBESTest (0–32), Physical Activity Scale for the Elderly (PASE) (0–400), Unified Parkinson’s Disease Rating Scale (UPDRS) (0–132), New-FOG questionnaire (NFOG-Q) (0–28), Ziegler protocol (0–36), Falls Efficacy Scale-International (FES-1) (16–64), Short Form 36 (SF-36) (0–100) |
| 8. Hunt et al., 2014 [20] Crossover. To compare performance error and perceived difficulty during toe-out gait modification in people with knee osteoarthritis (OA) across three different types of visual feedback: mirror, raw video, and real-time biofeedback of toe-out angle | N = 20 Sex = 11 female (55%); 9 male (45%) Age = 65.4 ± 9.8 years Inclusion criteria: knee OA Exclusion criteria: replacement of lower limb joints, knee surgery or injections in the previous six months, rheumatoid arthritis, arthrosis in other lower limb joints, inability to walk on a treadmill unassisted for 15 min | Video camera placed directly in front of the participant/Visual prescriptive and concurrent (KP) Assessment Technology: A Motion Analysis Corporation’s motion capture system consisting of 10 capture cameras at 120 Hz and 22 passive reflective markers | Participants were trained to gait on treadmill to increase the divergence 10° during stance phase by comparison with convergence angle during the selected gait Stage A: Mirror positioned 3 m in front of the participant (with a green line depicting the target angle) Stage B: Video screen positioned 3.2 m in front of the participant, overlaying the raw video image of the foot with a green tape target Stage C: The same video screen, but streaming real-time toe-out angle (a thin black line) and a green tape target Frequency and duration: 2´–3´ to become familiar with the tool and 15´´ to record data | Results measured after the intervention (raw video vs. mirror vs. real-time feedback) Significant and effective: Toe-out error (°) Not significant: Perceived difficulty (0–10) |
| 9. Jung et al., 2015 [7] Effect of gait training when using a cane with an augmented pressure sensor for enhancement of weight-bearing over the affected lower limb on the peak pressure force of the cane, muscle activation & gait in patients with stroke | N = 21 Sex = 7 female (33.3%); 14 male (66.7%) Age = 56.4 ± 11.1 years Inclusion criteria: first unilateral stroke, Mini Mental Test ≥ 24, capable of walking with a cane, bearing more than 7% of body weight with cane in vertical position Exclusion criteria: cerebral aneurysm, hemianopia, dizziness, or other symptoms indicating vestibular impairment, impaired touch and pressure sensation on the non-affected hand, hemineglect, orthopedic disease influencing gait | Presssure sensor (CD 210-K200, Dacell Co. Ltd, Cheongju, Korea) and indicator (DN30W, Dacell Co. Ltd, Cheongju, Korea)/Acoustic descriptive and terminal (KR) Assessment Technology: Specific instrumented cane for this study GAITRite walkway system (CIR Systems Inc., Franklin, NJ, USA) + Surface electromyography (Telemyo 2400 G2, Telemetry EMG system, Noraxon, Scottsdale, AZ, USA) for gluteus medius and vastus medialis | CG (n = 10): gait training + conventional therapy IG (n = 11): idem + acoustic feedback (a beep is emitted when a weight above the threshold is borne) Frequency and duration: 30 minute sessions, five times a week for 4 weeks | Results measured pre-test vs. post-test (Mean difference, 95% CI) Significant and effective: Vertical Peak Force of the cane (% body weight), Muscle Activation (% non-paretic peak activity) gluteus medius and vastus medialis oblique, Single Support Phase of the affected side (% Gait Cycle), Walking Velocity (cm/s) Not significant: None |
| 10. Khallaf et al., 2014 [39] To investigate the effect of task specific exercises, gait training, and visual biofeedback on correcting equinovarus gait among individuals with stroke | N = 16 Sex = 4 female (25%); 12 male (75%) Age = 40.8 ± 2.89 years Inclusion criteria: first unilateral stroke, hemiparesis minimum 3 months, medically stable, capable of understanding the procedure and giving informed consent, Chedoke-McMaster Stroke ≥ stage 4 (motor recovery), Modified Ashworth Scale(MAS): spasticity < 2, capable of walking autonomously with or without assistance for 6´ Exclusion criteria: altered sensation; cognitive, mental and visual deficiency; contractures in ankle and knee; taking muscle relaxant | Pedography (Colored graphs simulating foot placement) + emed-q100 pressure platform with 6080 sensors over a sensor area of 475 × 320 mm² and resolution of four sensors/cm2 at 100 Hz./Visual descriptive and terminal (KR) Assessment Technology: A capacitance-based pressure platform (emed-q100, Novel GmbH, Munich, Germany) was used for detecting the Pattern of foot placement | CG (n = 8): programme of conventional physiotherapy (strengthening exercises for the foot evertors and ankle dorsiflexors in addition to prolonged stretching of the calf muscles, walk in parallel bars and solid ankle foot orthosis (AFO)) IG (n = 8): specific exercises(stretching, musclespecific progressive-resistive exercise, balance training, etc) + gait training + visual biofeedback Frequency and duration: 5 sessions per week for 8 weeks, 50 min for each session | Results measured Baseline vs. postintervention vs. one month after intervention Time of Contact (percentage average rollover period): Significant and effective: Hindfoot, First Metatarsal Head, Second Metatarsal Head, Third Metatarsal Head, Forth Metatarsal Head, Fifth Metatarsal Head Not significant: None Maximum Force (N/cm2): Significant and effective: Hindfoot, First Metatarsal Head, Second Metatarsal Head, Third Metatarsal Head, Forth Metatarsal Head, Fifth Metatarsal Head Not significant: None |
| 11. Ki et al., 2015 [21] To examine the effects of auditory feedback during gait on the weight bearing of patients with hemiplegia resulting from a stroke | N = 25 Sex = 6 female (24%); 19 male (76%) Age = 57.7 ± 10.75 years Inclusion criteria: Stroke minimum 6 months previously, mini-mental test ≥ 24, walk autonmously at least 10 m unassisted, no orthopedic aids Exclusion criteria: Not specified | Pressure meter Ped-AlertTM120 (ORBITEC, Madison, WI, USA)/Acoustic descriptive and terminal (KR) Assessment Technology: GAITRite (CIR Systems Inc, Franklin, NJ, USA) + software GAITRite GOLD, version 3.2b | CG (n = 13): walk on GAITrite without feedback + treatment of neurodevelopment IG (n = 12): idem + acoustic feedback (a beep every time 50% of the patient’s body weight was exceeded on the paretic leg) Frequency and duration: the training period was a total of 4 weeks | Pre-test vs. Post-test Significant and effective: Duration of the Stance Phase (%), Duration of the Single Limb Stance (%), TUG test (sec) Not significant: None |
| 12. Lipsitz L.A. et al.; 2015 [22] Crossover. To test whether sub-sensory vibratory noise applied to the sole of the foot using a novel piezoelectric vibratory insole can significantly improve sensation, enhance balance, and reduce gait variability in elderly people, as well as to determine the optimal level of vibratory noise and whether the therapeutic effect would endure and the user’s sensory threshold would remain constant during the course of a day | N = 12 Sex = 11 female (91.7%); 1 male (8.3%) Age = 73.8 ± 8.1 years Inclusion criteria: age 65–90 years, sense the vibrations in the insole, speak English, understand and provide informed consent, follow instructions Exclusion criteria: feet ulcers, Parkinson’s or other neurodegenerative diseases, chronic pain in lower limbs avoiding standing or walking, no equilibrium without support for 1´, not feeling the vibration when the insoles are set to maximum, uncomfortable with insoles, new drug in the previous 30 days, having participated in another study in the previous 30 days, any other condition deemed inappropriate by the researchers | Two piezoelectric actuators in insolates/insoles (2.5 cm diameter each)/Haptic descriptive and terminal (KR) Assessment Technology: Force platform Type 9286B force plate (Kistler Instrument Corp., Winterthur, Switzerland) GAITRite; CIR Systems, Inc. + software MATLAB | The correct vibration threshold was determined. Then, the stimulation of each insole was set at 0%, 70% and 85% of the threshold value in accordance with randomization. The values were modified in the middle and at the end of the session to check them with the reference value | Mean for Each Stimulation Level (95% CI) Significant and effective: TUG test (sec), Stride Time, left foot (sec) Not significant: Gait speed (cm/s), Stride Time, right foot (sec), Step Width (cm), Double Support (sec) |
| 13. Ochi et al., 2015 [14] To examine whether gait training with a gait-assistance robot (GAR) improves gait disturbances in subacute nonambulatory hemiplegic stroke patients more than over-ground conventional gait training | N = 26 Sex = 6 female (23.1%); 20 male (76.9%) Age = 63.65 ± 9.8 years Inclusion criteria: first stroke less than five weeks prior to the study, unilateral hemispheric brain damage confirmed by computed tomography (CT) or magnetic resonance imaging (MRI), age 40–85 years, serious palsy of lower limbs (level III), Functional Ambulation Classification (FAC) ≤ 2, autonomous gait before stroke, informed consent Exclusion criteria: height < 145 cm or > 180 cm, body weight ≥ 100 kg, marked limitation in ROM of lower limbs, cardiovascular, respiratory, kidney or muscular-skeletal illnesses, difficult communication | Load sensors inserted between the sole of the foot and the foot bed of the shoe (the visual feedback regarding the stance phase and load amount)/Visual prescriptive and concurrent (KR) a GAR (Gait-assisted robot) a Treadmill | Overground conventional gait training group (OCGT) (n = 13): physiotherapeutic treatment (ROM and muscle strengthening exercises), speech therapy and occupational therapy + OCGT therapy (gait with parallel bars with orthesis of knee–ankle) and gait without parallel bars using forearm crutches) GAR-assisted gait training group (GAGT) (n = 13): idem (except OCGT) + GAGT therapy (lights for the foot pressure biofeedback system). Frequency and duration: 5 days per week for 4 weeks. Session of 60´ for physiotherapy, 60´ for speech therapy and 60´for occupational therapy and 20´ for GAGT or OCGT therapies | Pre-test vs. Post-test Significant and effective: Functional Ambulation Classification (FAC), Functional Independence Measure (FIM™) mobility score Not significant: walking Speed (m/s) |
| 14. Quinzaños Fresnedo, J.; 2015 [15] Short-term effect of gait training of robotic orthoses with auditory feedback in patients with chronic incomplete spinal cord injury | N = 33 Sex = 24 female (77.4%); 7 male (22.6%) Age = 35.6 ± 16.4 years Inclusion criteria: Age: 18–65 years, hospitalized at National institute of Rehabilitation with incomplete spinal cord injury, American Spinal Injury Association (ASIA) scale: C-D, independent gait with technical help more than 6 months, informed consent Exclusion criteria: Not specified | Metronome Zoom GFX707II GuitarMulti-Effects Pedal (Zoom Corporation, Tokyo, Japón)/Acoustic descriptive and terminal (KR) a Forearm crutches a Walker Assessment Technology: Lokomat® (Hocoma, Volketswil, Suiza) GAITRite® System mat (CIR Industries, Clifton, NJ, USA) | CG (n = 16): functional recovery of the conventional gait IG (n = 17): Idem using Lokomat® (auditory feedback) Frequency and duration: 12 sessions of 20´, 4 sessions per week for 3 weeks | Post-test (CG vs. IG) Significant and effective: Walking Speed (cm/s), Cadence (step/min), Stride Left (cm), Stride Rigth (cm), Functional Ambulatory Profile (FAP) Not significant: None |
| 15. Segal, N.; 2015 [11] To determine whether individualized gait training is more effective than usual care for reducing mobility disability and pain in individuals with symptomatic knee osteoarthritis | N = 48 Sex = 32 female (66.67%); 16 male (33.33%) Age = 59.6 ± 6.4 years Inclusion criteria: activities of daily living (ADL) ≤ 9, > 18 years old, gait without help and to climb 2 steps, surgery more than 6 months prior to study, symptomatic knee osteoarthritis Exclusion criteria: amputation, severe back pain, serious heart or neurological illness, surgery in the previous 6 months, corticosteroid injections in the previous 3 months | Software (C-Motion, Inc., Germantown, MD, USA) + Optotrack, Model 3020 (force plate + 3D viewing system)/Visual prescriptive and concurrent (KR) a Treadmill Assessment Technology: Gaitway, h/p/cosmos sports & medical gmbh, Nussdorf-Traunstein, Germany Kistler Force plate Model 9286 with capture at 300 Hz | CG (n = 19): Conventional approach (use of pain medications for knee symptoms, knee surgery, and/or physical therapy) IG (n = 29): idem + gait training on treadmill by feedback to optimize movement of knees (skeleton model and target area) (the major goals in retraining gait were to move participants toward symmetrical and typical displacements of the trunk and pelvis about neutral frontal (x) and transverse (y) axes) Frequency and duration: 2 sessions per week for 3 months, session of 45´ for conventional treatment and 3 intervals of 8´ for training with feedback. 3–5´for resting and correction from physiotherapists | Post-test (CG vs. IG) (95% CI) After 3 months: Significant and effective: Late Life Function and Disability Index (LLFDI) basic lower limb function score, Knee Injury and Osteoarthritis Outcome Score (KOOS) symptoms, KOOS pain Not significant: Long Distance Corridor Walk (LDCW) time (sec), Chair-Stand Time (sec), Stair Climb Time (sec) After 6 months: Significant and effective: LLFDI basic lower limb function score, Chair-Stand Time (sec) Not significant: LDCW time (sec), Stair Climb Time (sec), KOOS symptoms, KOOS pain After 12 months: Significant and effective: Chair-Stand Time (sec), KOOS symptoms, KOOS pain Not significant: LLFDI basic lower limb function score, LDCW time (sec), Stair Climb Time (sec) |
| 16. Shen, X.; 2014 [40] To explore whether balance and gait training with augmented feedback can enhance balance confidence in Parkinson´s Disease (PD) patients immediately after treatment and at 3–12 month follow-ups | N = 51 Sex = 20 female (39.2%); 31 male (60.8%) Age = 64.3 ± 8.25 years Inclusion criteria: Idiopathic Parkinson’s, stable medication, independent gait for 10 m, capable of following instructions (Mini-Mental Test > 23.19) Exclusion criteria: other neurological conditions, non-compensated cardiovascular disease, visual impairment, recent muscular-skeletal disorders in the back or lower limbs which alter gait and balance | KSD Technology Co Ltd., Shenzhen, China/Visual descriptive and terminal (KP) Smart-EquiTest Balance Master (NeuroCom International Inc., Clackamas, OR, USA)/Visual prescriptive concurrent (KP) a Treadmill Assessment Technology: GAITRite walkway (CIR Systems Inc., Havertown, PA, USA) Smart-EquiTest Balance Master (NeuroCom International Inc., Clackamas, OR, USA) | CG (active control group, CON) (n = 25): strength training of lower limbs (2 × 15 repetitions with 60% RM) IG (balance and gait training group, BAL) (n = 26): gait and balance training by visual and verbal feedback Frequency and duration: 12 weeks (eight in lab and four at home). Sessions of 60´, three sessions per week in lab; and sessions of 20´, five sessions per week at home | Pre-test vs. Post-test vs. Post-test (3 months) vs. post-test (12 months) Immediately after treatment: Significant and effective: Activities-Specific Balance Confidence (ABC) Scale (0–100), Movement velocity (°/s), Stride Length (cm) Not significant: End Point Excursion (Limit of Stability, LOS) (%), Gait Velocity (cm/s), After three months: Significant and effective: Activities-Specific Balance Confidence (ABC) Scale (0–100), Stride Length (cm), End Point Excursion (Limit of Stability, LOS) (%), Gait Velocity (cm/s), Stride Length (cm) Not significant: None After six months: Significant and effective: Activities-Specific Balance Confidence (ABC) Scale (0–100), Gait Velocity (cm/s), Stride Length (cm) Not significant: Movement velocity (°/s), End Point Excursion (Limit of Stability, LOS) (%) |
| 17. Stoller, O. et al., 2015 [16] Pilot RCT. Efficacy and feasibility of feedback-controlled robotics-assisted treadmill exercise (FC-RATE) for cardiovascular rehabilitation in persons with severe impairments shortly after stroke | N = 20 Sex = five female (36%); nine male (64%) Age = 61 ± 11 years Inclusion criteria: First stroke less than 20 weeks prior to study, >18 years old, functional gait, understand the study and give informed consent Exclusion criteria: counter indications for the cardiopulmonar stress test or for the use of the device (bone instability, serious contractures, and lower limb vascular disorders), neurological illness (spinal cord injury, multiple schlerosis, and Parkinson’s), lung diseases (COPD), dementia | Lokolift, Hocoma AG + Software LabVIEW (Versión 2009, National Instruments, Austin, TX, USA) (lokomat connected to this software (Hocoma AG, Volketswil, Switzerland))/Visual prescriptive and concurrent (KR) a Treadmill (h/p/cosmos sports & medical GmbH) Assessment Technology: Ergospirometry (MetaMax 3B, cortex Biophysik GmbH, Leipzig, Germany) Pulsometre (T31, Polar Electro, Kempele, Oulu, Finlandia) + receiver plate (HRMI, Sparkfun, Boulder, CO, USA) | CG (n = 7): RATE + conventional therapy (physiotherapy, speech therapy and conventional therapy) IG (n = 7): idem (except RATE) + FC-RATE Frequency and duration: Sessions of 30´. Three sessions per week for four weeks | Pre-test vs. post-test Significant and effective: None Not significant: Peak Oxygen Uptake (VO2 PEAK) absolute (mL Kg/min), VO2 PEAK relative (mL Kg/min), Peak Work Rate (PPEAK) (W), Peak Ventilation Rate (VEPEAK) (L/min), Peak Respiratory Rate (RfPEAK) (L/min), Peak Heart Rate (HRPEAK) (beats/min), Peak Respiratory Exchange Ratio (RERPEAK) (VCO2/VO2) |
| 18. Sungkarat, S.; 2011 [41] To determine whether external feedback to promote symmetrical weight distribution during standing and walking would improve gait performance and balance in people with stroke | N = 35 Sex = 11 female (31.4%); 24 male (68.6%) Age = 53 ± 9.3 years Inclusion criteria: first unilateral stroke with hemiparesis, Orpington Evaluation: 3.2–5.2, gait minimum 10 m with or without help, stable health condition to understand rules and participation Exclusion criteria: comorbidity or complication which impedes gait training, cognitive and/or communicative deterioration, severe leg spasticity, negligence, miss more than 3 sessions | Tecnology I-ShoWS (Insole Shoe Wedge and Sensors) consists of: footswitch for non-paretic foot with acoustic feedback during swing phase Lateral wedge insole of 7° in non-paretic foot to force change of weight in the paretic foot Pressure switch on paretic foot with acoustic feedback about weight bearing during stance fase of this foot (if weight is exceeded) (Pedal actuator/Acoustic descriptive and terminal (KR) (Pressure sensor/Acoustic descriptive and terminal (KR) Assessment Technology: GAITRite Electronic walkway system (CIR systems Inc., Clifton, NJ, USA) | CG (n = 18): programme of conventional retraining IG (n = 17): readaptation of gait using a wedge as an insole and set-up sensors (I-ShoWS). Frequency and duration: 15 sessions of 60 min for five days a week. Each session divided into 30 min gait retraining and the other 30 min for other conventional rehabilitation treatments | Pre-test vs. post-test Significant and effective: Gait Speed (cm/s), Step Length Asymmetry Ratio (m), Single Support Time Asymmetry Ratio (sec), Berg Balance Scale (points), Timed Up and Go (sec), Loading on Paretic Leg during Stance (%body weight) Not significant: None |
| 19. Won et al., 2015 [42] Effects of a novel walking training program with postural correction and visual feedback on walking function in patients with post-stroke hemiparesis | N = 16 Sex = 8 female (50%); 8 male (50%) Age = 60.35 ± 15.35 years Inclusion criteria: Stroke more than 6 months ago, Mini-mental test > 25, without orthopedic or cardiopulmonary problems, and with no psychological or emotional disorders Exclusion criteria: Not specified | Rear camera presenting body alignment in the coronal plane and load cells incorporated in a base plate under the treadmill (FTS)®/Visual prescriptive and concurrent (KP) Assessment Technology: Functional Training System, Marpe Co., Ltd., Jeonju, Korea | CG (n = 8): functional recovery of gait IG (n = 8): idem + postural correction using elastic bands + visual feedback during gait Frequency and duration: 30 min walking, twice a day for two weeks (speed adjusted to 2–4 m/s) | Pre-test vs. post-test Significant and effective: Step Length Ratio, Step Time Ratio, Stride Length (cm), Stance Phase Ratio, Swing Phase Ratio, 10-m Walk Test (10MWT) (sec) Not significant: None |
| 20. Zanotto, D. et al., 2013 [10] To investigate whether the most commonly used combination of feedback (i.e., haptic and visual) could be either enhanced by adding acoustic feedback or successfully substituted with a combination of kinetic guidance and acoustic feedback | N = 32 Sex = 12 female (37.5%); 20 male (62.5%) Age = 24.7 ± 3.8 years Inclusion criteria: right handed, without musculoskeletal or neurological problems Exclusion criteria: Not specified | ALEX II®: Exoesqueleto + Software + pressure sensor (interlink electronic FSR 4065) in the shoe + Speakers + Real time controller (PPC DS1103 controller Board2, dSPACE GmbH, Paderborn, Germany): Acoustic prescriptive and terminal (KR) Acoustic descriptive and concurrent (KP) Visual prescriptive and concurrent (KP) Assessment Technology: Load cells built into a baseplate under the walking belt of the treadmill | Kinetic guidance (robot) CG (n = 8): visual feedback (board) that shows a way next to the ankles IG I (n = 8): complex and continuous acoustic feedback (information of gait performance) IG II (n = 8): simple acoustic feedback by pressure sensor that produces a “beep” to mark the step. IG III (n = 8): visual feedback (CG) in combination with simple acoustic feedback (IG II) Frequency and duration: not specified | Pre-test vs. Post-test Normalized Error Area (NEA): Significant and effective: IG II and IG III Not significant: IG I NEA stance: Significant and effective: IG I Not significant: IG II and IG III NEA early swing: Significant and effective: IG I, IG II and IG II Not significant: None NEA late swing: Significant and effective: IG I, IG II and IG III Not significant: None ROM x: Significant and effective: IG II and IG III Not significant: IG I ROM y: Significant and effective: IG II and IG III Not significant: IG I Normalized Error in Stride Period (Terr): Significant and effective: IG I, IG II, IG III Not significant: None Stance Time Period (STP) ratio: Significant and effective: None Not significant: IG I, IG II and IG III |
| Study | Criteria | Total Score | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
| 1. Baram, Y. et al., 2012 [17] | X | ✓ | X | ✓ | X | X | X | ✓ | ✓ | X | X | 4 |
| 2. Brasileiro, A. et al., 2015 [18] | X | ✓ | X | ✓ | X | X | X | ✓ | ✓ | ✓ | ✓ | 6 |
| 3. Byl, N. et al., 2015 [19] | ✓ | ✓ | X | X | X | X | X | ✓ | X | ✓ | ✓ | 4 |
| 4. Drużbicki, M. et al., 2015 [5] | ✓ | ✓ | ✓ | ✓ | X | X | ✓ | ✓ | ✓ | ✓ | ✓ | 8 |
| 5. El-Tamawy, M. et al., 2012 [23] | ✓ | ✓ | X | ✓ | X | X | ✓ | ✓ | X | ✓ | ✓ | 6 |
| 6. Fu, M.C. et al., 2014 [26] | ✓ | ✓ | X | X | X | X | X | ✓ | ✓ | ✓ | X | 4 |
| 7. Ginis, P. et al., 2016 [38] | ✓ | ✓ | X | ✓ | X | X | X | ✓ | ✓ | ✓ | ✓ | 6 |
| 8. Hunt, M.A. et al., 2014 [20] | ✓ | ✓ | X | ✓ | X | X | X | ✓ | ✓ | ✓ | ✓ | 6 |
| 9. Jung, K. et al., 2015 [7] | ✓ | ✓ | ✓ | ✓ | X | X | ✓ | ✓ | X | ✓ | ✓ | 7 |
| 10. Khallaf, M.E. et al., 2014 [39] | ✓ | ✓ | ✓ | ✓ | X | X | X | X | X | ✓ | ✓ | 5 |
| 11. Ki, K. et al., 2015 [21] | ✓ | ✓ | X | ✓ | X | X | X | ✓ | X | ✓ | ✓ | 5 |
| 12. Lipsitz, L.A. et al., 2015 [22] | ✓ | ✓ | ✓ | X | X | X | ✓ | X | X | ✓ | X | 4 |
| 13. Ochi, M. et al., 2015 [14] | ✓ | ✓ | ✓ | ✓ | X | X | ✓ | X | X | ✓ | ✓ | 6 |
| 14. Quinzaños Fresnedo, J. et al., 2015 [15] | ✓ | ✓ | X | ✓ | X | X | X | ✓ | ✓ | ✓ | ✓ | 6 |
| 15. Segal, N.A. et al., 2015 [11] | ✓ | ✓ | ✓ | ✓ | X | X | X | X | X | ✓ | ✓ | 5 |
| 16. Shen, X. et al., 2014 [40] | ✓ | ✓ | X | ✓ | X | X | ✓ | ✓ | ✓ | ✓ | ✓ | 7 |
| 17. Stoller, O. et al., 2015 [16] | ✓ | ✓ | ✓ | ✓ | X | X | ✓ | X | ✓ | ✓ | ✓ | 7 |
| 18. Sungkarat, S. et al., 2011 [41] | ✓ | ✓ | ✓ | ✓ | X | X | ✓ | ✓ | X | ✓ | ✓ | 7 |
| 19. Won, S.H. et al., 2015 [42] | ✓ | ✓ | ✓ | ✓ | X | X | X | ✓ | ✓ | ✓ | ✓ | 7 |
| 20. Zanotto, D. et al., 2013 [10] | ✓ | ✓ | X | ✓ | X | X | X | ✓ | ✓ | ✓ | ✓ | 6 |
| Feedback | Knowledge Performance | Knowledge Result | Concurrent/Immediate | Terminal/Retarded | Descriptive | Prescriptive | |
|---|---|---|---|---|---|---|---|
| 1. Baram, Y.; 2012 [17] | Visual | X | X | X | |||
| Acoustic | X | X | X | ||||
| 2. Brasileiro, A. et al., 2015 [18] | Visual | X | X | X | |||
| 3. Byl et al., 2015 [19] | Visual | X | X | X | |||
| 4. Druzbicki, M. et al., 2015 [5] | Visual | X | X | X | |||
| Acoustic | X | X | X | ||||
| 5. El-Tamawy et al., 2012 [23] | Haptic | X | X | X | |||
| 6. Fu, M.C. et al., 2014 [26] | Haptic | X | X | X | |||
| 7. Ginis, P. et al., 2016 [38] | Acoustic | X | X | X | |||
| 8. Hunt et al., 2014 [20] | Visual | X | X | X | |||
| 9. Jung et al., 2015 [7] | Acoustic | X | X | X | |||
| 10. Khallaf et al., 2014 [39] | Visual | X | X | X | |||
| 11. Ki et al., 2015 [21] | Acoustic | X | X | X | |||
| 12. Lipsitz, L.A. et al., 2015 [22] | Haptic | X | X | X | |||
| 13. Ochi et al., 2015 [14] | Visual | X | X | X | |||
| 14. Quinzaños Fresnedo, J.; 2015 [15] | Acoustic | X | X | X | |||
| 15. Segal, N.; 2015 [11] | Visual | X | X | X | |||
| 16. Shen, X.; 2014 [40] | Visual | X | X | X | |||
| Visual | X | X | X | ||||
| 17. Stoller, O. et al., 2015 [16] | Visual | X | X | X | |||
| 18. Sungkarat, S.; 2011 [41] | Acoustic | X | X | X | |||
| Acoustic | X | X | X | ||||
| 19. Won et al., 2015 [42] | Visual | X | X | X | |||
| 20. Zanotto, D. et al., 2013 [10] | Acoustic | X | X | X | |||
| Acoustic | X | X | X | ||||
| Visual | X | X | X |
| Feedback | Walking Speed (m/s) | Stride Length (m) | Cadence (steps/min) | TUG (s) | Berg Balance | 10MWT (m/s) | 2MWT (m) | ROM Hip (°) | ROM Knee (°) | ROM Ankle (°) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Baram, Y.; 2012 [17] | Visual | X | X | ||||||||
| Acoustic | X | X | |||||||||
| 2. Brasileiro, A. et al., 2015 [18] | Visual | X | X | X | X | X | X | ||||
| 3. Byl et al., 2015 [19] | Visual | X | X | X | X | ||||||
| 4. Druzbicki, M. et al., 2015 [5] | Visual | X | X | X | X | ||||||
| Acoustic | X | X | X | X | |||||||
| 5. El-Tamawy et al., 2012 [23] | Haptic | X | X | X | X | X | X | ||||
| 6. Fu, M.C. et al., 2014 [26] | Haptic | ||||||||||
| 7. Ginis, P. et al., 2016 [38] | Acoustic | X | X | X | |||||||
| 8. Hunt et al., 2014 [20] | Visual | ||||||||||
| 9. Jung et al., 2015 [7] | Acoustic | X | |||||||||
| 10. Khallaf et al., 2014 [39] | Visual | ||||||||||
| 11. Ki et al., 2015 [21] | Acoustic | X | |||||||||
| 12. Lipsitz, L.A. et al., 2015 [22] | Haptic | X | X | ||||||||
| 13. Ochi et al., 2015 [14] | Visual | X | |||||||||
| 14. Quinzaños-Fresnedo, J.; 2015 [15] | Acoustic | X | X | ||||||||
| 15. Segal, N.; 2015 [11] | Visual | ||||||||||
| 16. Shen, X.; 2014 [40] | Visual (AT *) | X | X | ||||||||
| Visual (3m *1) | X | X | |||||||||
| Visual (6m) | X | X | |||||||||
| 17. Stoller, O. et al., 2015 [16] | Visual | ||||||||||
| 18. Sungkarat, S.; 2011 [41] | Acoustic | X | X | X | |||||||
| 19. Won et al., 2015 [42] | Visual | X | X | ||||||||
| 20. Zanotto, D. et al., 2013 [10] | Acoustic | ||||||||||
| Visual |
 ; Significant and not effective =
; Significant and not effective =  ; Not significant =
; Not significant =  ; * After Treatment; * 1 months; TUG = Test Up and Go; 10MWT = 10 meters Walk Time; 2MWT = 2-min test; ROM = Range Of Motion.
; * After Treatment; * 1 months; TUG = Test Up and Go; 10MWT = 10 meters Walk Time; 2MWT = 2-min test; ROM = Range Of Motion.© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chamorro-Moriana, G.; Moreno, A.J.; Sevillano, J.L. Technology-Based Feedback and Its Efficacy in Improving Gait Parameters in Patients with Abnormal Gait: A Systematic Review. Sensors 2018, 18, 142. https://doi.org/10.3390/s18010142
Chamorro-Moriana G, Moreno AJ, Sevillano JL. Technology-Based Feedback and Its Efficacy in Improving Gait Parameters in Patients with Abnormal Gait: A Systematic Review. Sensors. 2018; 18(1):142. https://doi.org/10.3390/s18010142
Chicago/Turabian StyleChamorro-Moriana, Gema, Antonio José Moreno, and José Luis Sevillano. 2018. "Technology-Based Feedback and Its Efficacy in Improving Gait Parameters in Patients with Abnormal Gait: A Systematic Review" Sensors 18, no. 1: 142. https://doi.org/10.3390/s18010142
APA StyleChamorro-Moriana, G., Moreno, A. J., & Sevillano, J. L. (2018). Technology-Based Feedback and Its Efficacy in Improving Gait Parameters in Patients with Abnormal Gait: A Systematic Review. Sensors, 18(1), 142. https://doi.org/10.3390/s18010142