What is the Best Configuration of Wearable Sensors to Measure Spatiotemporal Gait Parameters in Children with Cerebral Palsy?

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol
2.3. Reference Spatiotemporal Parameters of Gait Using Laboratory Setting
2.3.1. Equipment
2.3.2. Spatiotemporal Parameters Computation
2.4. Spatiotemporal Parameters of Gait Using Wearable Setting
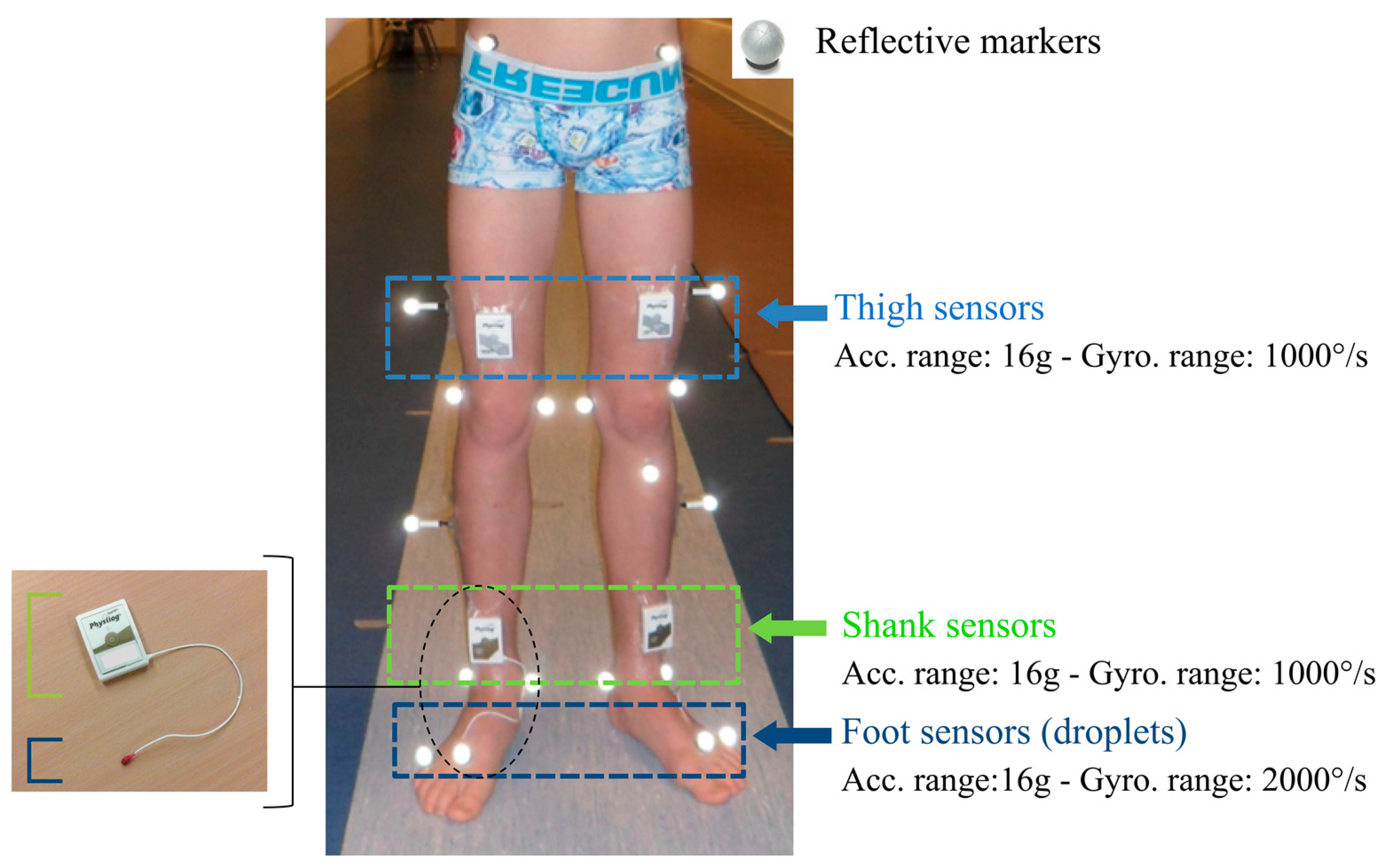
2.4.1. Equipment
2.4.2. Sensor Configuration and Associated Algorithm
2.5. Data Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Temporal Detection
4.2. Spatial Detection
4.3. Choice for Daily Life Assessment
4.4. Limitations and Perspectives
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sellier, E.; Platt, M.J.; Andersen, G.L.; Krägeloh-Mann, I.; De La Cruz, J.; Cans, C.; Cans, C.; Van Bakel, M.; Arnaud, C.; Delobel, M.; et al. Decreasing prevalence in cerebral palsy: A multi-site European population-based study, 1980 to 2003. Dev. Med. Child Neurol. 2016, 58, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Armand, S.; De Coulon, G.; Bonnefoy-mazure, A. Gait analysis in children with cerebral palsy. EFORT Open Rev. 2016, 1, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Carcreff, L.; Bonnefoy-mazure, A.; De Coulon, G.; Armand, S. Analyse quantifiée de la marche. Mov. Sport Sci. 2016, 3, 7–21. [Google Scholar] [CrossRef]
- Sutherland, D.H. The evolution of clinical gait analysis Part II Kinematics. Gait Posture 2002, 16, 159–179. [Google Scholar] [CrossRef]
- Desailly, E.; Daniel, Y.; Sardain, P.; Lacouture, P. Foot contact event detection using kinematic data in cerebral palsy children and normal adults gait. Gait Posture 2009, 29, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Ghoussayni, S.; Stevens, C.; Durham, S.; Ewins, D. Assessment and validation of a simple automated method for the detection of gait events and intervals. Gait Posture 2004, 20, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Bruening, D.A.; Ridge, S.T. Automated event detection algorithms in pathological gait. Gait Posture 2014, 39, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, R.; Rossi, S.; Castelli, E.; Patanè, F.; Mazzà, C.; Cappa, P. Effects of the calibration procedure on the metrological performances of stereophotogrammetric systems for human movement analysis. Meas. J. Int. Meas. Confed. 2017, 101, 265–271. [Google Scholar] [CrossRef]
- Chiari, L.; Della Croce, U.; Leardini, A.; Cappozzo, A. Human movement analysis using stereophotogrammetry. Part 2: Instrumental errors. Gait Posture 2005, 21, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, R.; Rossi, S.; Patanè, F.; Cappa, P. Technical quality assessment of an optoelectronic system for movement analysis. J. Phys. Conf. Ser. 2015, 588. [Google Scholar] [CrossRef]
- World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF The International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2002; Volume 1149. [Google Scholar]
- Holsbeeke, L.; Ketelaar, M.; Schoemaker, M.M.; Gorter, J.W. Capacity, Capability, and Performance: Different Constructs or Three of a Kind? Arch. Phys. Med. Rehabil. 2009, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Van Eck, M.; Dallmeijer, A.J.; Voorman, J.M.; Becher, J.G. Longitudinal study of motor performance and its relation to motor capacity in children with cerebral palsy. Dev. Med. Child Neurol. 2009, 51, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Smits, D.-W.; Gorter, J.W.; Van Schie, P.E.; Dallmeijer, A.J.; Ketelaar, M. How Do Changes in Motor Capacity, Motor Capability, and Motor Performance Relate in Children and Adolescents With Cerebral Palsy? Arch. Phys. Med. Rehabil. 2014, 95, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Keawutan, P.; Bell, K.; Davies, P.S.W.; Boyd, R.N. Systematic review of the relationship between habitual physical activity and motor capacity in children with cerebral palsy. Res. Dev. Disabil. 2014, 35, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Olivier, I.; Baker, C.; Cordier, J.; Thomann, G.; Nougier, V. Cognitive and motor aspects of a coincidence-timing task in Cerebral Palsy children. Neurosci. Lett. 2015, 602, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Li, Q. Inertial sensor-based methods in walking speed estimation: A systematic review. Sensors 2012, 12, 6102–6116. [Google Scholar] [CrossRef] [PubMed]
- Boutaayamou, M.; Denoël, V.; Brüls, O.; Demonceau, M.; Maquet, D.; Forthomme, B.; Croisier, J.-L.; Schwartz, C.; Verly, J.; Garraux, G. Algorithm for Temporal Gait Analysis Using Wireless Foot-Mounted Accelerometers; Springer: Cham, Switzerland, 2017; ISBN 978-3-319-54716-9. [Google Scholar]
- Khandelwal, S.; Wickström, N. Novel methodology for estimating Initial Contact events from accelerometers positioned at different body locations. Gait Posture 2017. [Google Scholar] [CrossRef] [PubMed]
- Aminian, K.; Najafi, B.; Büla, C.; Leyvraz, P.F.; Robert, P. Spatio-temporal parameters of gait measured by an ambulatory system using miniature gyroscopes. J. Biomech. 2002, 35, 689–699. [Google Scholar] [CrossRef]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef]
- Esser, P.; Dawes, H.; Collett, J.; Feltham, M.G.; Howells, K. Assessment of spatio-temporal gait parameters using inertial measurement units in neurological populations. Gait Posture 2011, 34, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Trojaniello, D.; Cereatti, A.; Della Croce, U. Accuracy, sensitivity and robustness of five different methods for the estimation of gait temporal parameters using a single inertial sensor mounted on the lower trunk. Gait Posture 2014, 40, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Mansour, K.B.; Rezzoug, N.; Gorce, P. Analysis of several methods and inertial sensors locations to assess gait parameters in able-bodied subjects. Gait Posture 2015, 42, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Lanovaz, J.L.; Oates, A.R.; Treen, T.T.; Unger, J.; Musselman, K.E. Validation of a commercial inertial sensor system for spatiotemporal gait measurements in children. Gait Posture 2017, 51, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Van Den Noort, J.C.; Ferrari, A.; Cutti, A.G.; Becher, J.G.; Harlaar, J. Gait analysis in children with cerebral palsy via inertial and magnetic sensors. Med. Biol. Eng. Comput. 2013, 51, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Ferrari, A.; Garofalo, P.; Raggi, M.; Cappello, A.; Ferrari, A. “Outwalk”: A protocol for clinical gait analysis based on inertial and magnetic sensors. Med. Biol. Eng. Comput. 2010, 48, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Laudanski, A.; Yang, S.; Li, Q. A concurrent comparison of inertia sensor-based walking speed estimation methods. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBC, Boston, MA, USA, 30 August–3 September 2011; pp. 3484–3487. [Google Scholar] [CrossRef]
- Brégou Bourgeois, A.; Mariani, B.; Aminian, K.; Zambelli, P.Y.; Newman, C.J.; Bre, A. Spatio-temporal gait analysis in children with cerebral palsy using, foot-worn inertial sensors. Gait Posture 2014, 39, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Veilleux, L.-N.; Raison, M.; Rauch, F.; Robert, M.; Ballaz, L. Agreement of spatio-temporal gait parameters between a vertical ground reaction force decomposition algorithm and a motion capture system. Gait Posture 2015, 43, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Caldas, R.; Mundt, M.; Potthast, W.; Buarque, F.; Neto, D.L. A systematic review of gait analysis methods based on inertial sensors and adaptive algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, S.J.; Kepple, T.M.; McGuire, D.A.; Roman, N.L. Kinematic-based technique for event time determination during gait. Med. Biol. Eng. Comput. 1990, 28, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Barre, A.; Armand, S. Biomechanical ToolKit: Open-source framework to visualize and process biomechanical data. Comput. Methods Programs Biomed. 2014, 114, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; McDade, E.M.; Pertersen, R.C. Normative Spatiotemporal Gait Parameters in Older Adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Dadashi, F.; Mariani, B.; Rochat, S.; Büla, C.J.; Santos-Eggimann, B.; Aminian, K. Gait and foot clearance parameters obtained using shoe-worn inertial sensors in a large-population sample of older adults. Sensors 2014, 14, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Rochat, S.; Büla, C.J.; Martin, E.; Seematter-Bagnoud, L.; Karmaniola, A.; Aminian, K.; Piot-Ziegler, C.; Santos-Eggimann, B. What is the Relationship between Fear of Falling and Gait in Well-Functioning Older Persons Aged 65 to 70 Years? Arch. Phys. Med. Rehabil. 2010, 91, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Seematter-Bagnoud, L.; Santos-Eggimann, B.; Rochat, S.; Martin, E.; Karmaniola, A.; Aminian, K.; Piot-Ziegler, C.; Büla, C.J. Vulnerability in high-functioning persons aged 65 to 70 years: The importance of the fear factor. Aging Clin. Exp. Res. 2011, 22, 485–486. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.G.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Salarian, A.; Burkhard, P.R.; Vingerhoets, F.J.G.; Jolles, B.M.; Aminian, K. A novel approach to reducing number of sensing units for wearable gait analysis systems. IEEE Trans. Biomed. Eng. 2013, 60, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Hoskovec, C.; Rochat, S.; Büla, C.; Penders, J.; Aminian, K. 3D gait assessment in young and elderly subjects using foot-worn inertial sensors. J. Biomech. 2010, 43, 2999–3006. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Helbostad, J.L.; Moe-Nilssen, R.; Zijlstra, W.; Aminian, K. Does walking strategy in older people change as a function of walking distance? Gait Posture 2009, 29, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Jiménez, M.C.; Vingerhoets, F.J.G.; Aminian, K. On-shoe wearable sensors for gait and turning assessment of patients with parkinson’s disease. IEEE Trans. Biomed. Eng. 2013, 60, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Berker, A.N.; Yalçin, M.S. Cerebral Palsy: Orthopedic Aspects and Rehabilitation. Pediatr. Clin. N. Am. 2008, 55, 1209–1225. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis. Expert Rev. Med. Devices 2016, 13, 641–659. [Google Scholar] [CrossRef] [PubMed]
- Washabaugh, E.P.; Kalyanaraman, T.; Adamczyk, P.G.; Claflin, E.S.; Krishnan, C. Validity and repeatability of inertial measurement units for measuring gait parameters. Gait Posture 2017, 55, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Steinwender, G.; Saraph, V.; Scheiber, S.; Zwick, E.B.; Uitz, C.; Hackl, K. Intrasubject repeatability of gait analysis data in normal and spastic children. Clin. Biomech. 2000, 15, 134–139. [Google Scholar] [CrossRef]
- Hegde, N.; Bries, M.; Sazonov, E. A Comparative Review of Footwear-Based Wearable Systems. Electronics 2016, 5, 48. [Google Scholar] [CrossRef]
- Paraschiv-Ionescu, A.; Perruchoud, C.; Buchser, E.; Aminian, K. Barcoding human physical activity to assess chronic pain conditions. PLoS ONE 2012. [Google Scholar] [CrossRef] [PubMed]
- Attal, F.; Mohammed, S.; Dedabrishvili, M.; Chamroukhi, F.; Oukhellou, L.; Amirat, Y. Physical Human Activity Recognition Using Wearable Sensors. Sensors 2015, 15, 31314–31338. [Google Scholar] [CrossRef] [PubMed]
- Fasel, B.; Duc, C.; Dadashi, F.; Bardyn, F.; Savary, M.; Farine, P.A.; Aminian, K. A wrist sensor and algorithm to determine instantaneous walking cadence and speed in daily life walking. Med. Biol. Eng. Comput. 2017, 55, 1773–1785. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Configuration Name | Shanks and Thighs | Shanks | Feet | ||
|---|---|---|---|---|---|
| Abbreviation | ShTh | Sh | Feet | ||
| Sensor placement | On the anterior side of each shank and thigh | On the anterior side of each shank | On top of each foot | ||
| Associated algorithm | Authors | Salarian et al. 2004 [39] | Salarian et al. 2013 [40] | Mariani et al. 2010, 2013 [41,42] | |
| Calibration on sensor axis | No calibration needed as the pitch axis is assumed systematically aligned with the mediolateral axis of the body | Sensor axes vertically aligned using the gravity component during motionless periods and the orientation was obtained by maximizing the pitch angular velocity of the foot throughout the gait trial. | |||
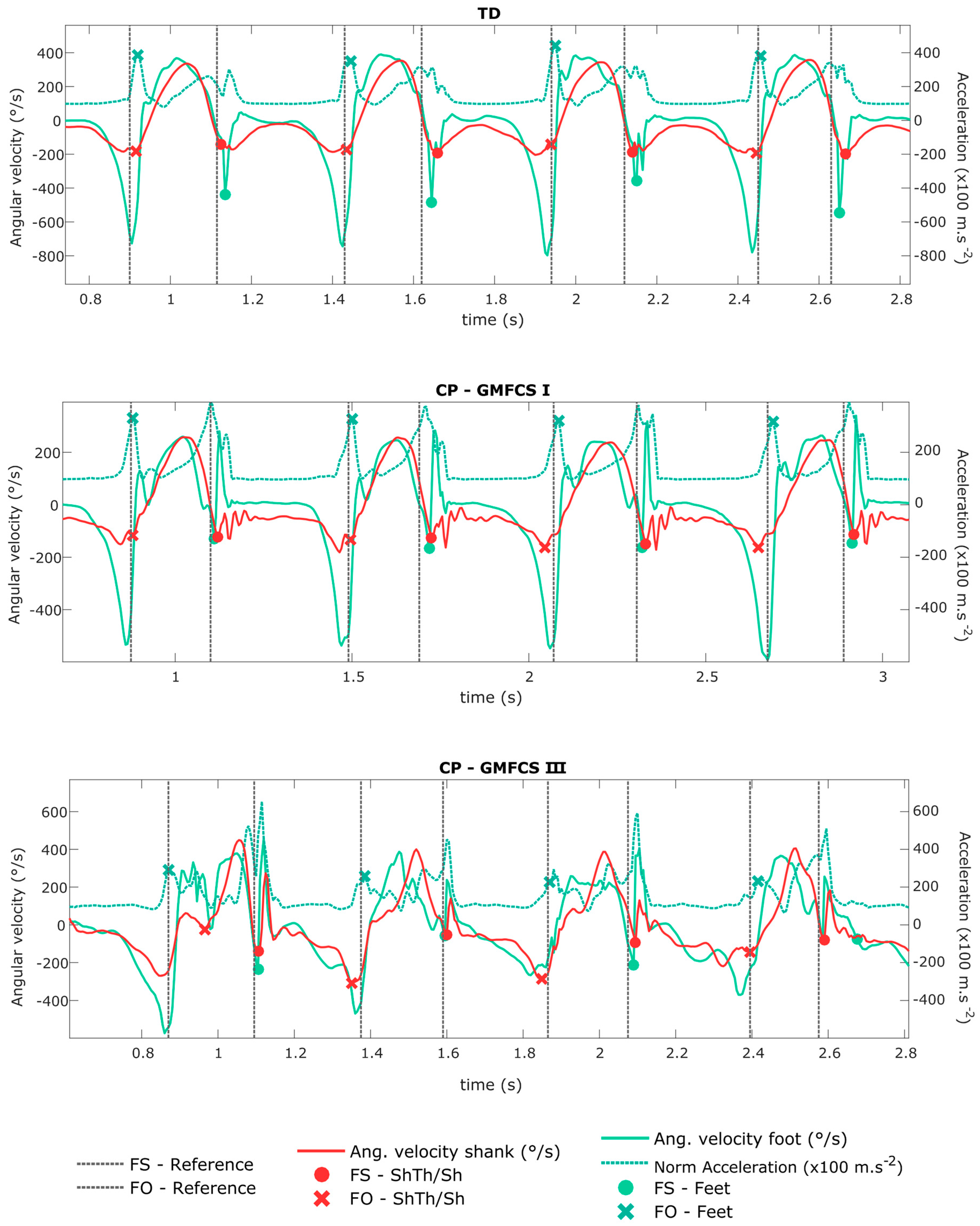
| Events (temporal) detection method | Peak detection on pitch angular velocity of shanks | Peak detection on pitch angular velocity and norm of acceleration of feet | |||
| Spatial detection method | Application of a double pendulum model [20] from shank and thigh angles (calculated by integration of shanks and thigh angular velocities) and segments lengths. | Application of a double pendulum model [20] from shank and thigh angles estimated only from shanks angular velocities and segments lengths. Thigh angles estimated from shank angles using Fourier series and least square optimization. | De-drifted double integration of gravity-free acceleration between two successive and identical events (foot flat) | ||
| Spatio-temporal computation | Temporal parameter divided by spatial parameter | De-drifted single integration of gravity-free acceleration between two successive and identical events (foot flat) | |||
| Outputs gait parameters | n = 24; includes:
| n = 55; includes:
| |||
| Population used for validation | Healthy adults, elderly, patients with a total hip replacement, patients with coxarthrosis [20,43], and Parkinson’s disease (PD) adults [39] | Healthy adults, patients with a total hip replacement, patients with coxarthrosis, and PD patients [40]. | Young, elderly adults and PD patients [41,44] | Children with cerebral palsy (CP) [29] | |
| Mean errors (±sd) against reference | Against force plate and optoelectronic system (ELITE, BTS, Milan, Italy)
Against Instrumented walkway (GaitRite, Franklin, USA):
| Against force plate and optoelectronic system (ELITE, BTS, Milan, Italy)
| Against force plate and optoelectronic system (Vicon, Oxford Metrics, Oxford, UK)
For PD adults:
| Against force plate and optoelectronic system (Vicon, Oxford Metrics, Oxford, UK)
| |
| TD | CP | ||
|---|---|---|---|
| N | 11 | 15 | |
| GMFCS I | GMFCS II-III | ||
| 7 | 8 | ||
| Unilateral | Bilateral | ||
| 5 | 10 | ||
| Sex Number of girls in the group (%) | 5 (45) | 8 (55) | |
| Age in years mean ± std | 13.5 ± 2.9 | 12.8 ± 3.1 | |
| TD | CP | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| GMFCS I | GMFCS II-III | ||||||||
| Healthy sides | Non-paretic side | Paretic side | Paretic sides | ||||||
| Cycle detection | n (%) | n (%) | n (%) | n (%) | |||||
| Number of non-detected cycle | ShTh/Sh | 3 (0.1) | 0 (0.0) | 0 (0) | 58 (2.4) | ||||
| Feet | 18 (0.8) | 24 (1.0) | 3 (0.1) | 170 (7.4) | |||||
| Gait event | Error mean (SD) | Error mean (SD) | Error mean (SD) | Error mean (SD) | |||||
| Foot strike | ShTh/Sh | 0.040 (0.021) | 0.042 (0.030) | 0.037 (0.051) | 0.053 (0.048) | ||||
| (s) | Feet | 0.047 (0.020) | 0.048 (0.020) | 0.051 (0.053) | 0.077 (0.299) | ||||
| Foot off | ShTh/Sh | −0.011 (0.021) | −0.004 (0.029) | −0.008 (0.045) | −0.011 (0.063) | ||||
| (s) | Feet | 0.012 (0.021) | 0.014 (0.018) | 0.020 (0.018) | 0.029 (0.058) | ||||
| STP | Mean (SD) | Error | Mean (SD) | Error | Mean (SD) | Error | Mean (SD) | Error | |
| mean (SD) | mean (SD) | mean (SD) | mean (SD) | ||||||
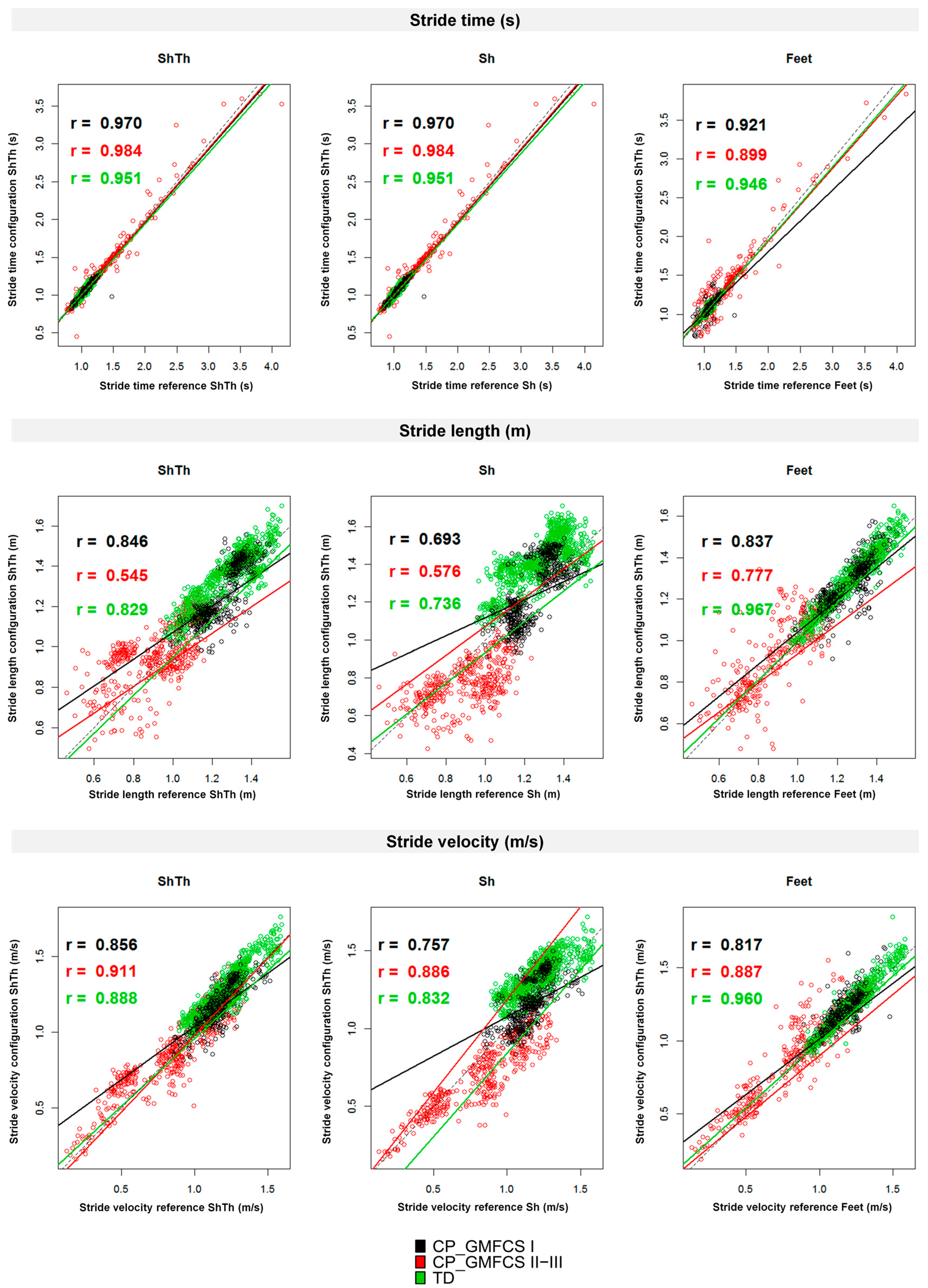
| Stride time | Reference | 1.061 (0.080) | 1.095 (0.073) | 1.055 (0.092) | 1.197 (0.388) | ||||
| (s) | ShTh/Sh | 1.064 (0.082) | 0.000 (0.023) | 1.091 (0.090) | 0.001 (0.017) | 1.055 (0.091) | 0.000 (0.031) | 1.200 (0.393) | 0.003 (0.072) |
| Feet | 1.061 (0.083) | 0.000 (0.022) | 1.096 (0.073) | 0.001 (0.019) | 1.052 (0.101) | 0.000 (0.057) | 1.312 (0.431) | 0.012 (0.129) | |
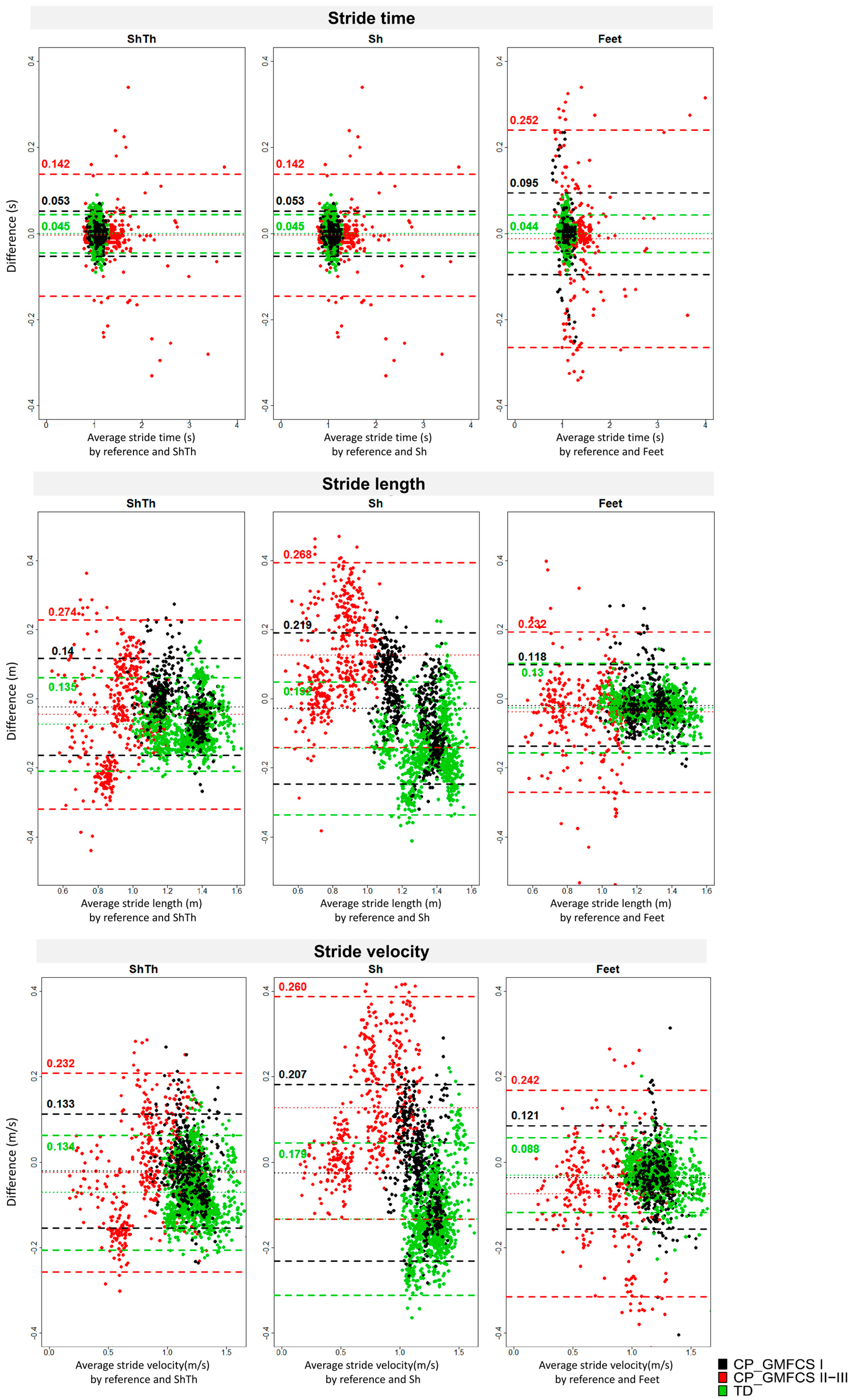
| Stride length | Reference | 1.276 (0.144) | 1.267(0.108) | 1.242 (0.104) | 0.896 (0.161) | ||||
| (m) | ShTh | 1.351 (0.135) | 0.075 (0.069) | 1.297 (0.145) | 0.030 (0.078) | 1.262 (0.134) | 0.019 (0.066) | 0.942 (0.143) | 0.046 (0.140) |
| Sh | 1.420 (0.133) | 0.144 (0.098) | 1.298 (0.179) | 0.031 (0.124) | 1.269 (0.157) | 0.027 (0.104) | 0.770 (0.118) | −0.126(0.137) | |
| Feet | 1.295 (0.151) | 0.025 (0.037) | 1.296 (0.095) | 0.023 (0.036) | 1.257 (0.118) | 0.018 (0.069) | 0.916 (0.182) | 0.039 (0.118) | |
| Stride velocity | Reference | 1.201 (0.155) | 1.167 (0.110) | 1.184 (0.104) | 0.810 (0.283) | ||||
| (m/s) | ShTh | 1.277 (0.154) | 0.073 (0.067) | 1.193 (0.129) | 0.026 (0.072) | 1.201 (0.129) | 0.018 (0.065) | 0.834 (0.252) | 0.024 (0.118) |
| Sh | 1.338 (0.115) | 0.133 (0.091) | 1.193 (0.160) | 0.025 (0.116) | 1.208 (0.143) | 0.024 (0.098) | 0.683 (0.212) | −0.127 (0.133) | |
| Feet | 1.233 (0.165) | 0.030 (0.045) | 1.200 (0.093) | 0.036 (0.039) | 1.216 (0.117) | 0.035 (0.070) | 0.831(0.286) | 0.073 (0.123) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carcreff, L.; Gerber, C.N.; Paraschiv-Ionescu, A.; De Coulon, G.; Newman, C.J.; Armand, S.; Aminian, K. What is the Best Configuration of Wearable Sensors to Measure Spatiotemporal Gait Parameters in Children with Cerebral Palsy? Sensors 2018, 18, 394. https://doi.org/10.3390/s18020394
Carcreff L, Gerber CN, Paraschiv-Ionescu A, De Coulon G, Newman CJ, Armand S, Aminian K. What is the Best Configuration of Wearable Sensors to Measure Spatiotemporal Gait Parameters in Children with Cerebral Palsy? Sensors. 2018; 18(2):394. https://doi.org/10.3390/s18020394
Chicago/Turabian StyleCarcreff, Lena, Corinna N. Gerber, Anisoara Paraschiv-Ionescu, Geraldo De Coulon, Christopher J. Newman, Stéphane Armand, and Kamiar Aminian. 2018. "What is the Best Configuration of Wearable Sensors to Measure Spatiotemporal Gait Parameters in Children with Cerebral Palsy?" Sensors 18, no. 2: 394. https://doi.org/10.3390/s18020394
APA StyleCarcreff, L., Gerber, C. N., Paraschiv-Ionescu, A., De Coulon, G., Newman, C. J., Armand, S., & Aminian, K. (2018). What is the Best Configuration of Wearable Sensors to Measure Spatiotemporal Gait Parameters in Children with Cerebral Palsy? Sensors, 18(2), 394. https://doi.org/10.3390/s18020394