The Association between the Lipids Levels in Blood and Risk of Age-Related Macular Degeneration


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction and Study Quality Assessment
2.4. Statistical Analysis
3. Results
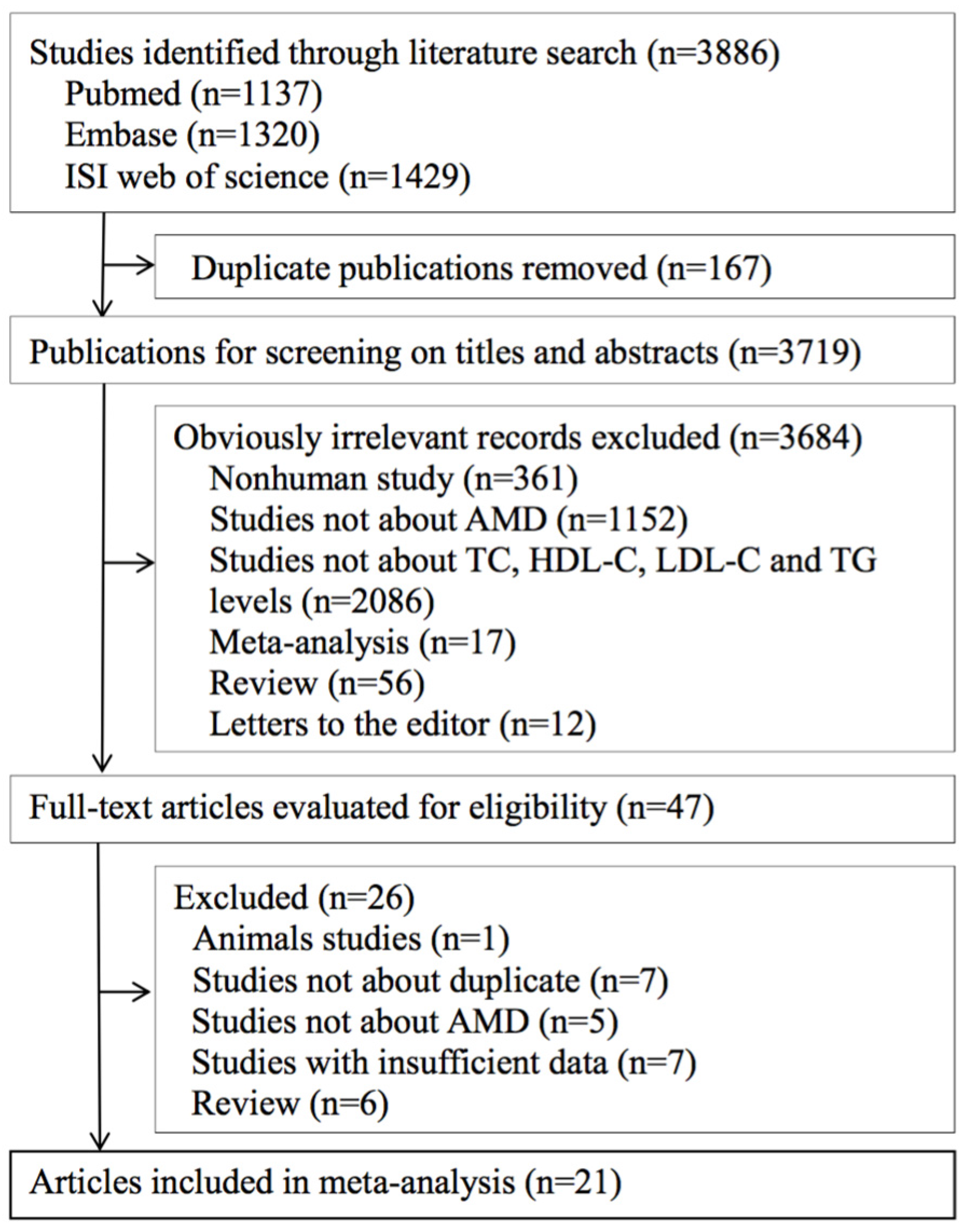
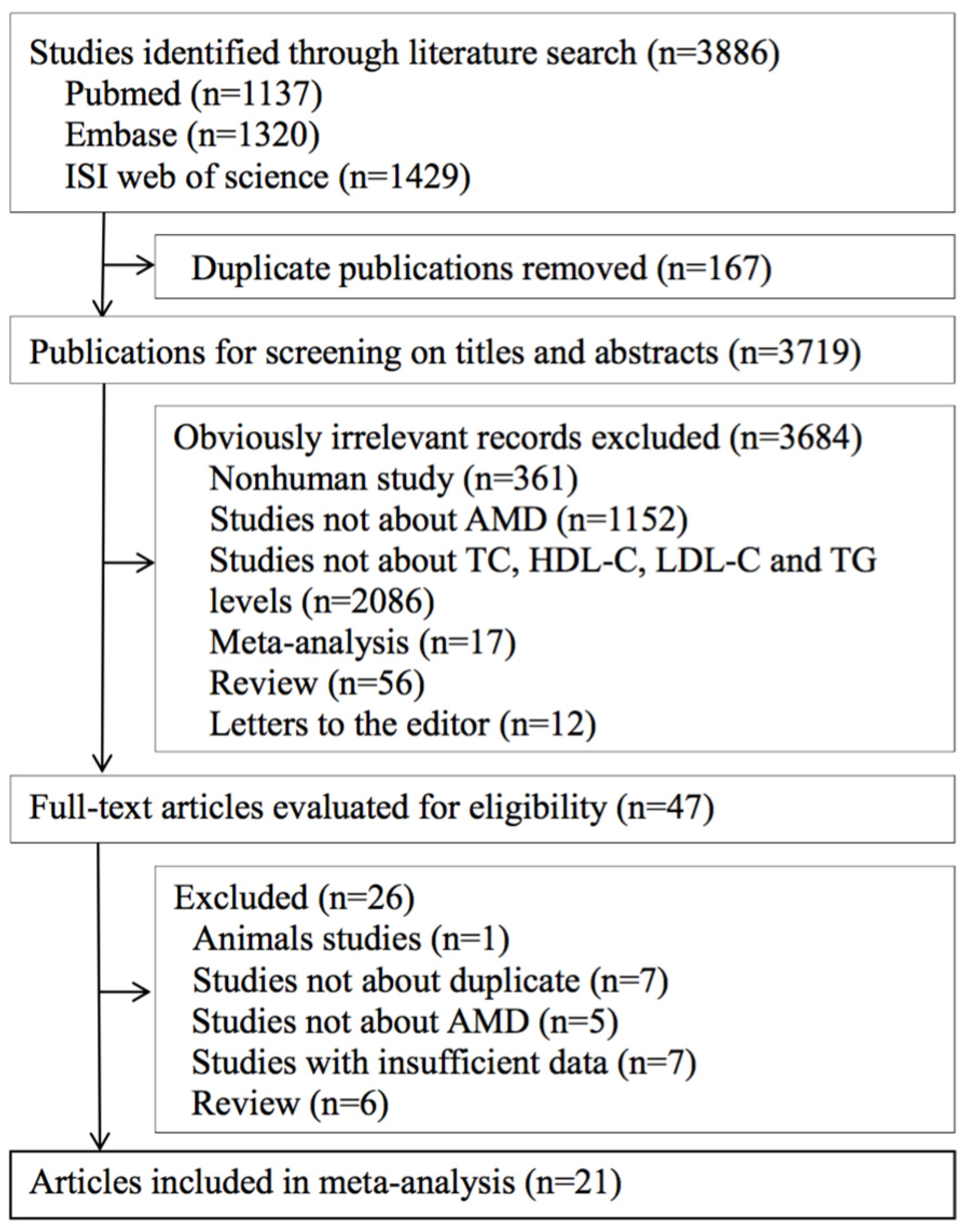
3.1. Literature Search
3.2. Study Characteristics
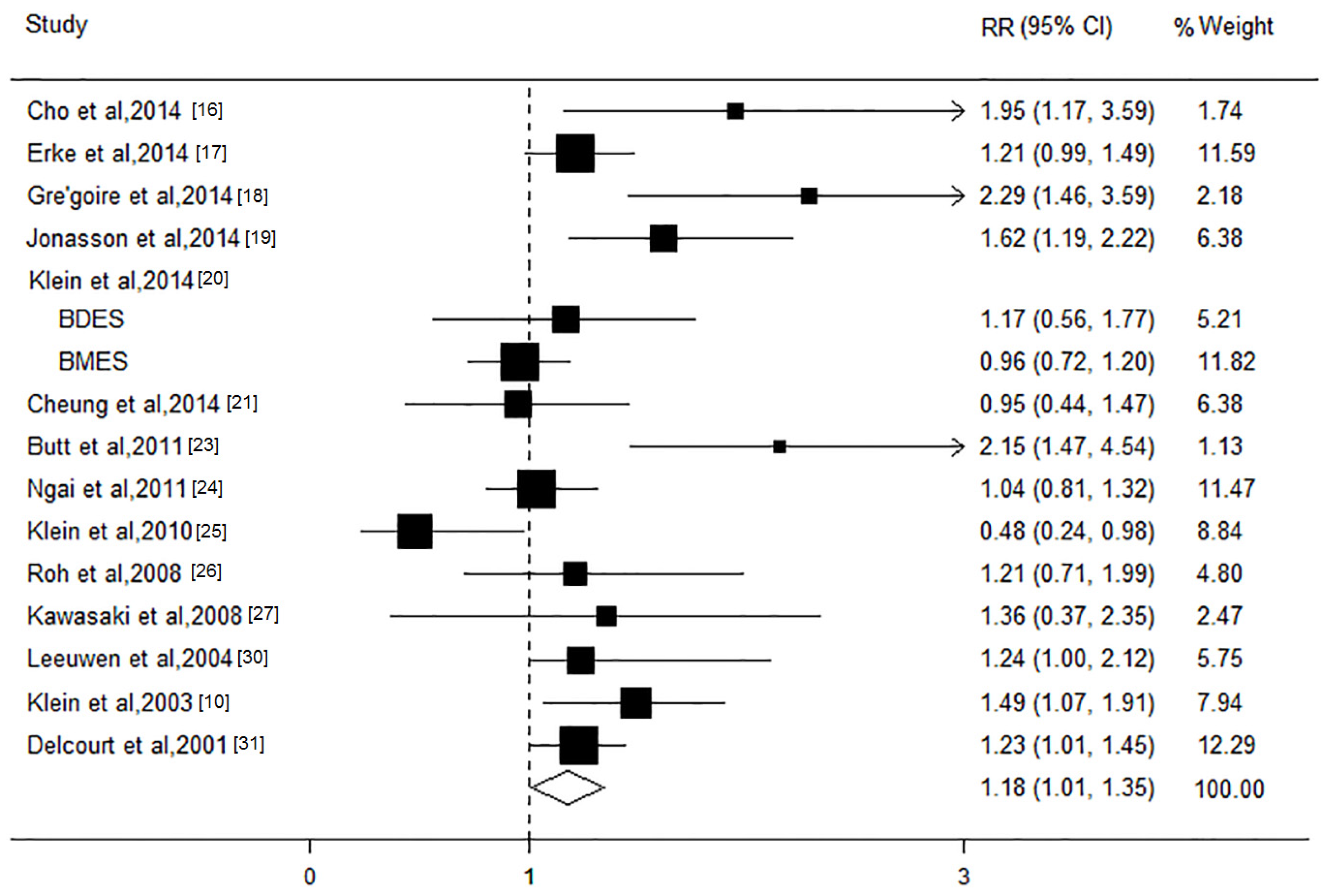
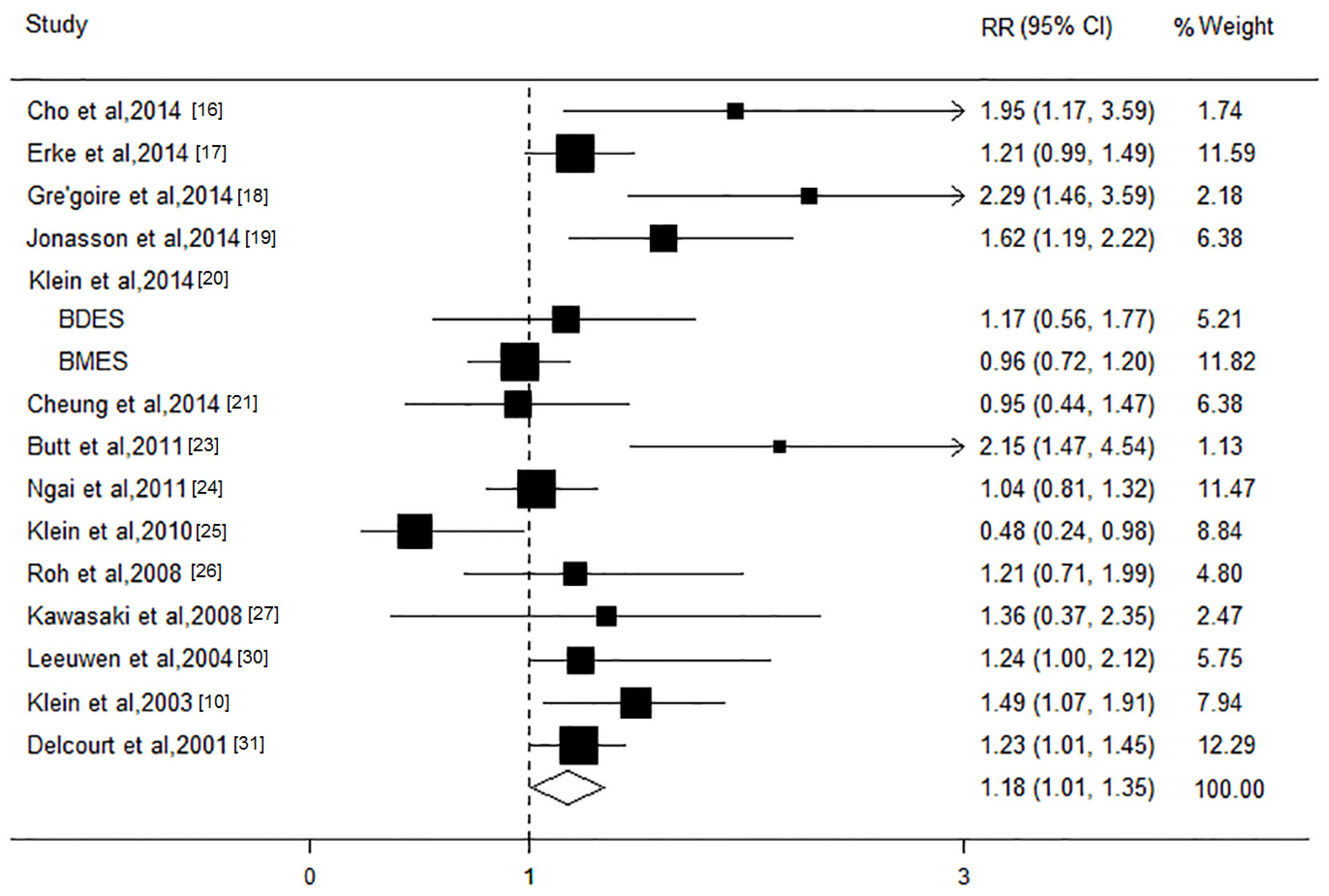
3.3. HDL-C Level and AMD Risk
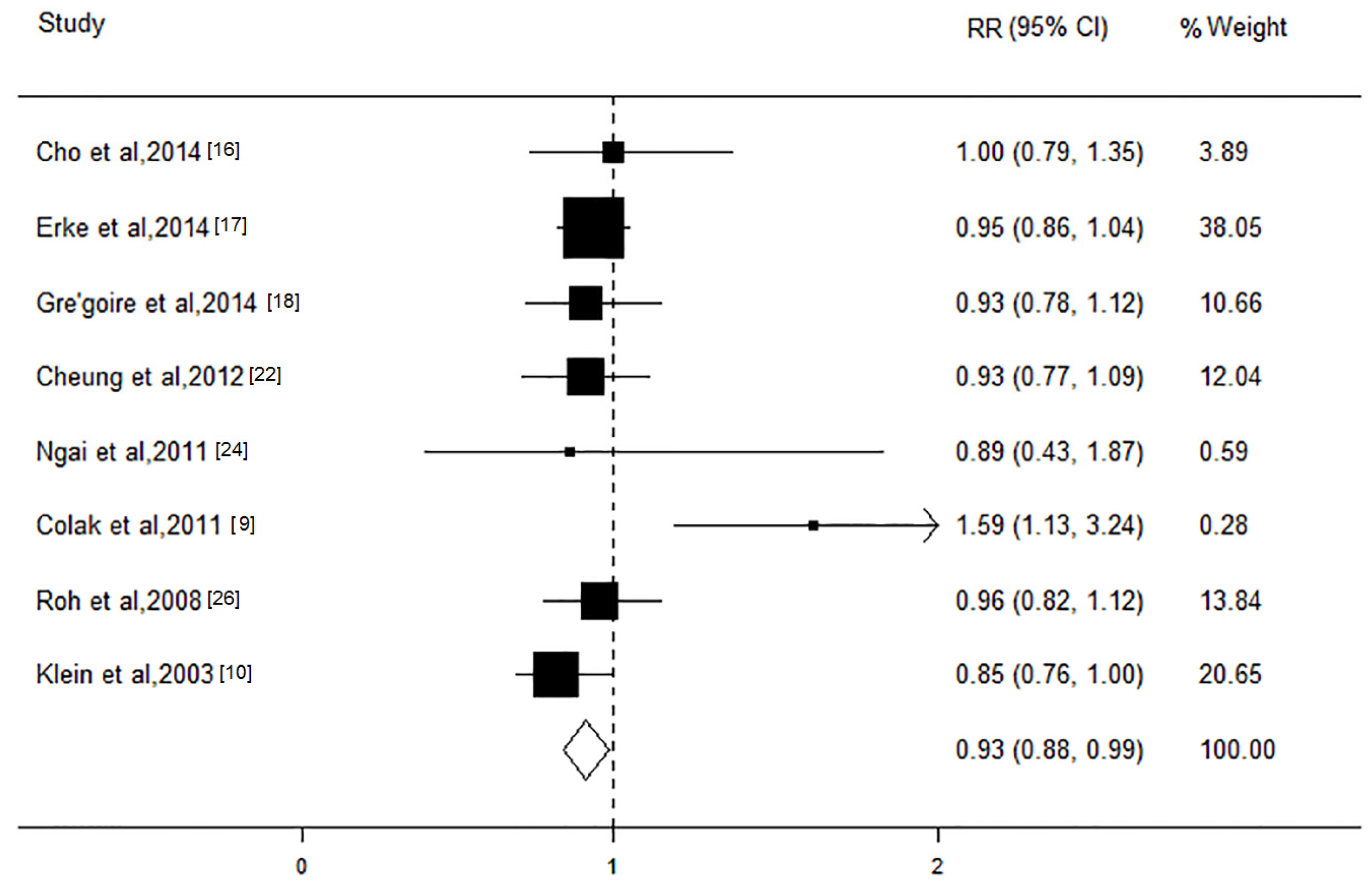
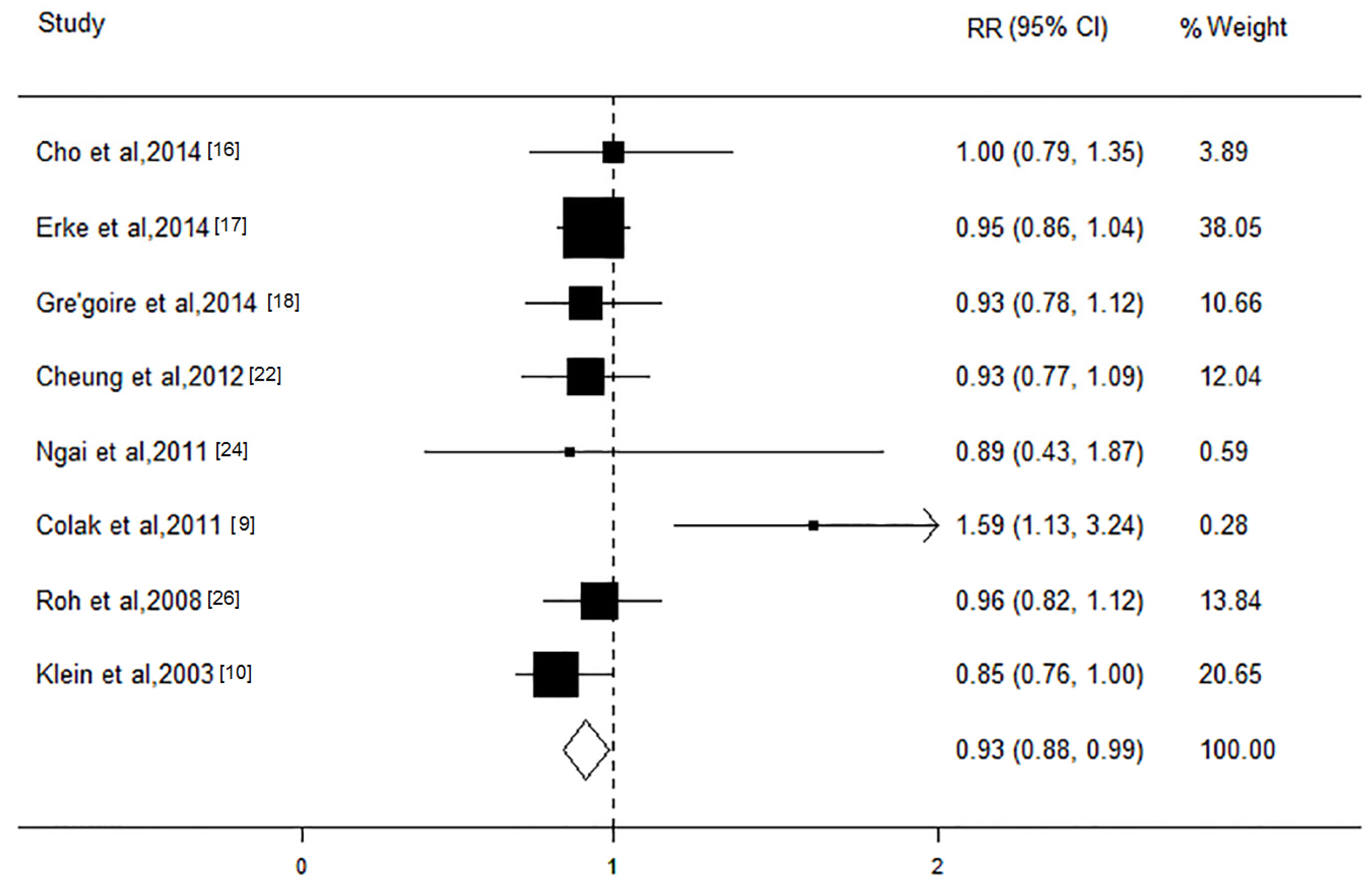
3.4. LDL-C Level and AMD Risk
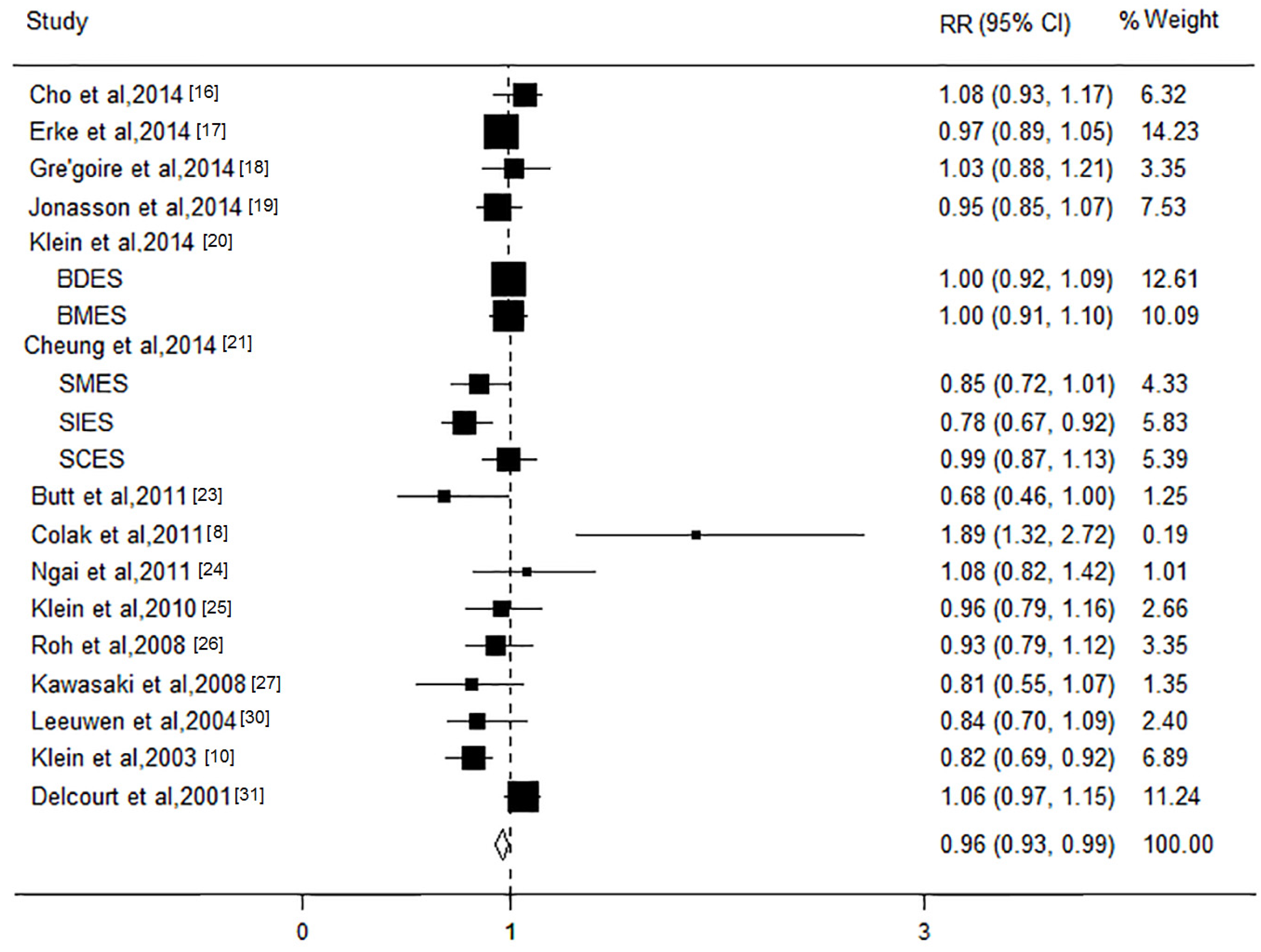
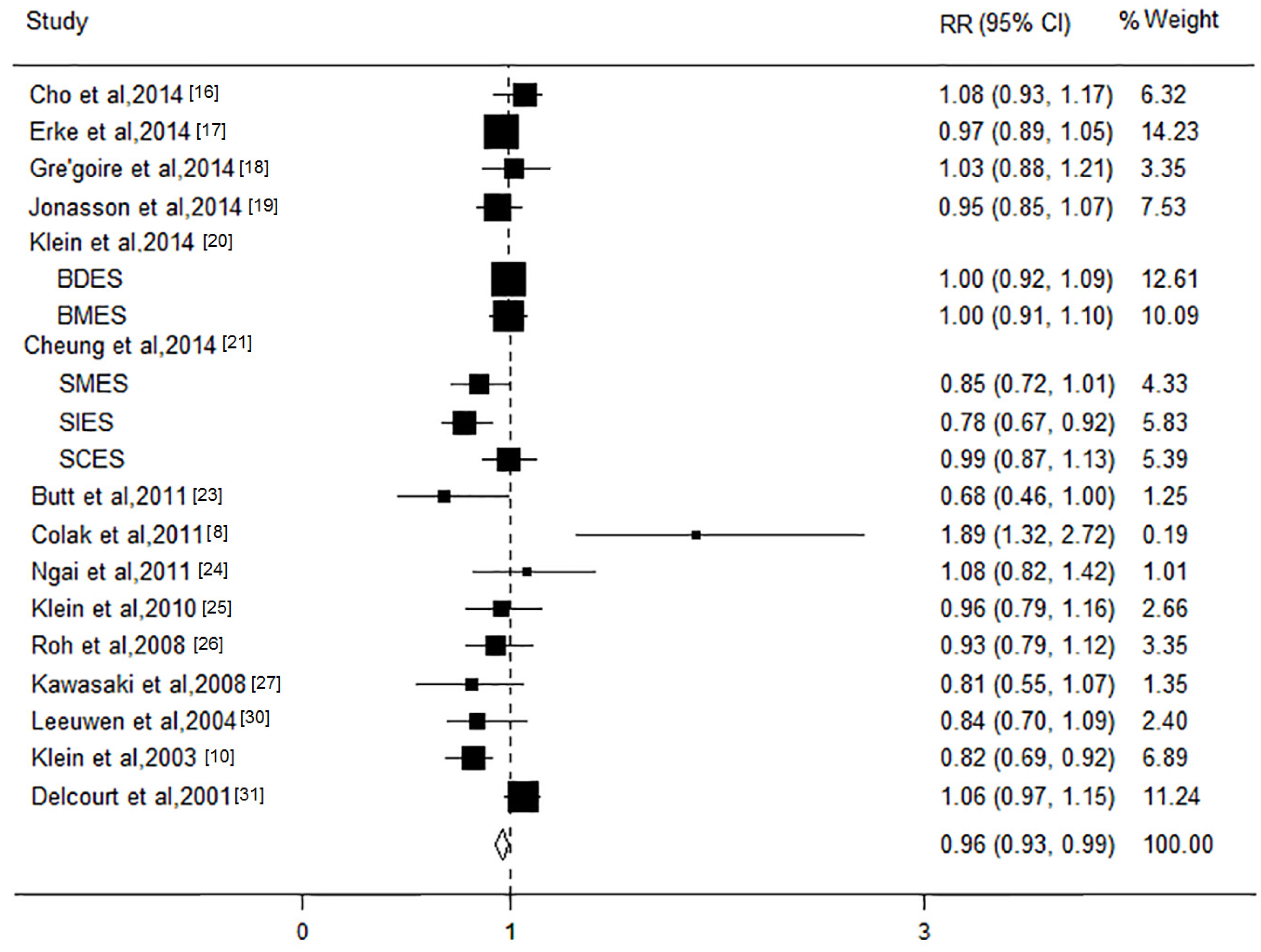
3.5. TC Level and AMD Risk
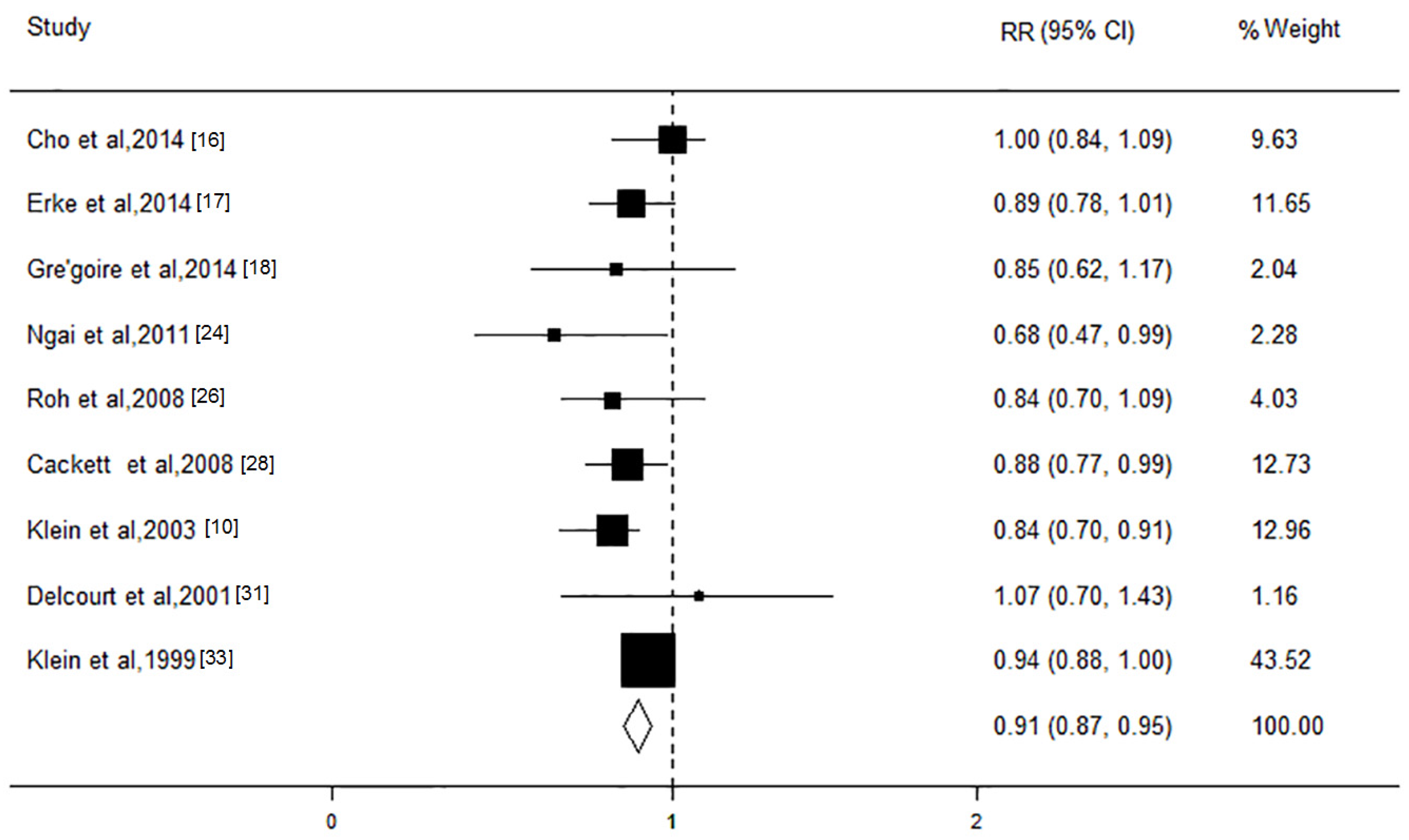
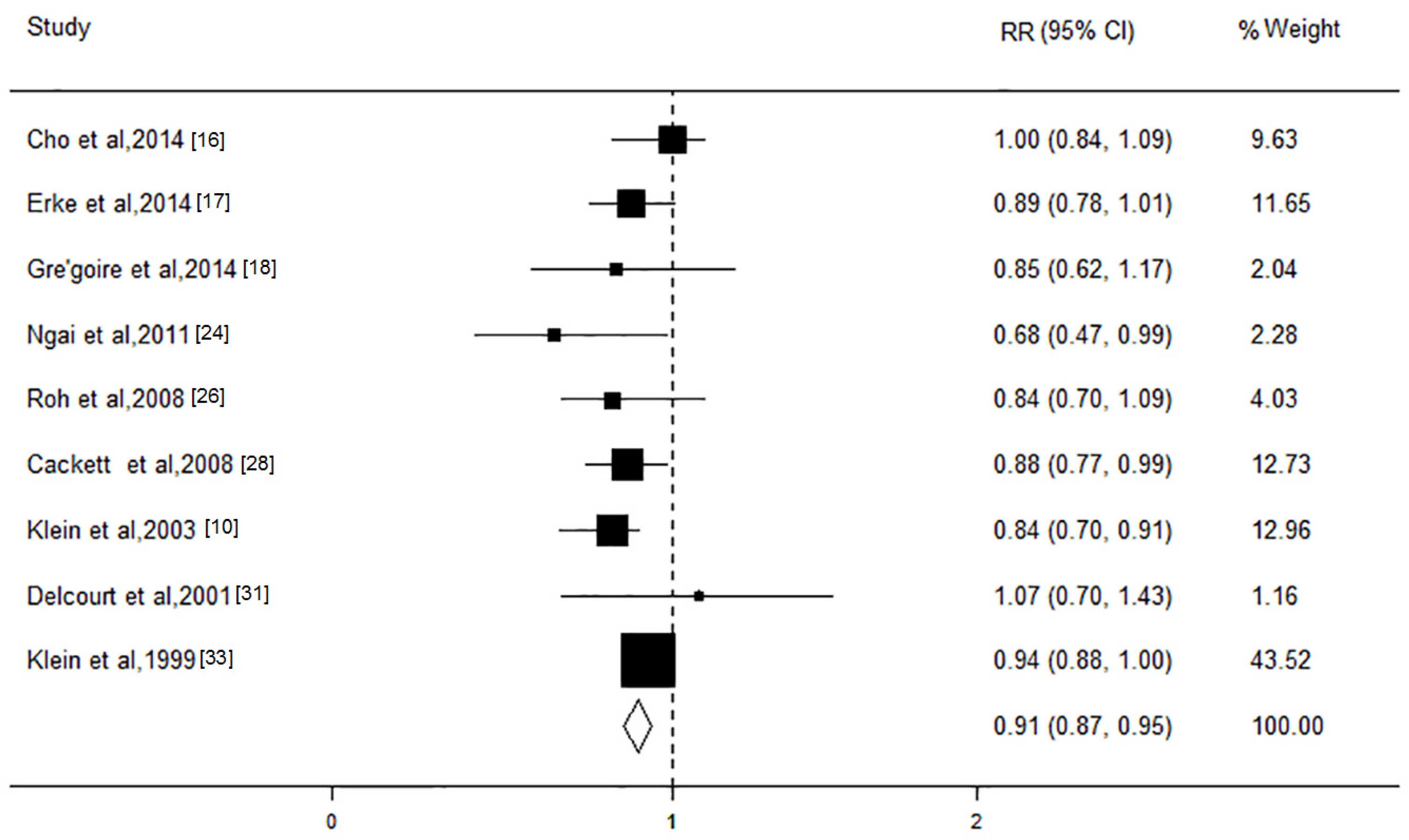
3.6. TG Level and AMD Risk
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lim, L.S.; Mitchell, P.; Seddon, J.M.; Holz, F.G.; Wong, T.Y. Age-related macular degeneration. Lancet 2012, 379, 1728–1738. [Google Scholar] [CrossRef]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health Blog 2014, 2, 106–116. [Google Scholar] [CrossRef]
- Jager, R.D.; Mieler, W.F.; Miller, J.W. Age-related macular degeneration. N. Engl. J. Med. 2008, 358, 2606–2617. [Google Scholar] [CrossRef]
- Seddon, J.M.; Reynolds, R.; Yu, Y.; Daly, M.J.; Rosner, B. Risk models for progression to advanced age-related macular degeneration using demographic, environmental, genetic, and ocular factors. Ophthalmology 2011, 118, 2203–2211. [Google Scholar] [CrossRef] [PubMed]
- Hogg, R.E.; Woodside, J.V.; Gilchrist, S.E.; Graydon, R.; Fletcher, A.E.; Chan, W.; Knox, A.; Cartmill, B.; Chakravarthy, U. Cardiovascular disease and hypertension are strong risk factors for choroidal neovascularization. Ophthalmology 2008, 115, 1046–1052. [Google Scholar] [CrossRef]
- Parhofer, K.G. Increasing HDL-cholesterol and prevention of atherosclerosis: A critical perspective. Atheroscler. Suppl. 2015, 18, 109–111. [Google Scholar] [CrossRef]
- Rizk, N.M.; El-Menyar, A.; Egue, H.; Souleman, W.I.; Mohamed, B.H.; Alali, K.; Farag, F.; Younes, N.; Al, S.J. The Association between Serum LDL Cholesterol and Genetic Variation in Chromosomal Locus 1p13.3 among Coronary Artery Disease Patients. BioMed Res. Int. 2015, 2015, 678924. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Lee, J.H.; Woo, S.J.; Ahn, J.; Shin, J.P.; Song, S.J.; Kang, S.W.; Park, K.H.; Epidemiologic Survey Committee of the Korean Ophthalmologic Society. Age-related macular degeneration: Prevalence and risk factors from Korean National Health and Nutrition Examination Survey, 2008 through 2011. Ophthalmology 2014, 121, 1756–1765. [Google Scholar] [CrossRef] [PubMed]
- Colak, E.; Kosanović-Jaković, N.; Zorić, L.; Radosavljević, A.; Stanković, S.; Majkić-Singh, N. The association of lipoprotein parameters and C-reactive protein in patients with age-related macular degeneration. Ophthalmic Res. 2011, 46, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Marino, E.K.; Kuller, L.H.; Furberg, C.; Burke, G.L.; Hubbard, L.D. Early age-related maculopathy in the cardiovascular health study. Ophthalmology 2003, 110, 25–33. [Google Scholar] [CrossRef]
- Neale, B.M.; Fagerness, J.; Reynolds, R.; Sobrin, L.; Parker, M.; Raychaudhuri, S.; Tan, P.L.; Oh, E.C.; Merriam, J.E.; Souied, E.; et al. Genome-wide association study of advanced age-related macular degeneration identifies a role of the hepatic lipase gene (LIPC). Proc. Natl. Acad. Sci. USA 2010, 107, 7395–7400. [Google Scholar] [CrossRef] [PubMed]
- Yun, C.; Oh, J.; Ahn, S.E.; Hwang, S.Y.; Kim, S.W.; Huh, K. Peripapillary choroidal thickness in patients with early age-related macular degeneration and reticular pseudodrusen. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 427–435. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1001. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Cho, B.J.; Heo, J.W.; Kim, T.W.; Ahn, J.; Chung, H. Prevalence and risk factors of age-related macular degeneration in Korea: The Korea National Health and Nutrition Examination Survey 2010–2011. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Erke, M.G.; Bertelsen, G.; Peto, T.; Sjølie, A.K.; Lindekleiv, H.; Njølstad, I. Cardiovascular risk factors associated with age-related macular degeneration: The Tromsø Study. Acta Ophthalmol. 2014, 92, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Cougnard-Grégoire, A.; Delyfer, M.N.; Korobelnik, J.F.; Rougier, M.B.; Le Goff, M.; Dartigues, J.F.; Barberger-Gateau, P.; Delcourt, C. Elevated high-density lipoprotein cholesterol and age-related macular degeneration: The Alienor study. PLoS ONE 2014, 9, e90973. [Google Scholar]
- Jonasson, F.; Fisher, D.E.; Eiriksdottir, G.; Sigurdsson, S.; Klein, R.; Launer, L.J.; Harris, T.; Gudnason, V.; Cotch, M.F. Five-year incidence, progression, and risk factors for age-related macular degeneration: The age, gene/environment susceptibility study. Ophthalmology 2014, 121, 1766–1772. [Google Scholar] [CrossRef]
- Klein, R.; Myers, C.E.; Buitendijk, G.H.; Rochtchina, E.; Gao, X.; de Jong, P.T.; Sivakumaran, T.A.; Burlutsky, G.; McKean-Cowdin, R.; Hofman, A. Lipids, lipid genes, and incident age-related macular degeneration: The three continent age-related macular degeneration consortium. Am. J. Ophthalmol. 2014, 158, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.M.; Li, X.; Cheng, C.Y.; Zheng, Y.; Mitchell, P.; Wang, J.J.; Wong, T.Y. Prevalence, racial variations, and risk factors of age-related macular degeneration in Singaporean Chinese, Indians, and Malays. Ophthalmology 2014, 121, 1598–1603. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.M.; Tai, E.S.; Kawasaki, R.; Tay, W.T.; Lee, J.L.; Hamzah, H.; Wong, T.Y. Prevalence of and risk factors for age-related macular degeneration in a multiethnic Asian cohort. Arch. Ophthalmol. 2012, 130, 480–486. [Google Scholar] [PubMed]
- Butt, A.L.; Lee, E.T.; Klein, R.; Russell, D.; Ogola, G.; Warn, A.; Kingsley, R.M.; Yeh, J. Prevalence and risks factors of age-related macular degeneration in Oklahoma Indians: The Vision Keepers Study. Ophthalmology 2011, 118, 1380–1385. [Google Scholar] [CrossRef]
- Ngai, L.Y.; Stocks, N.; Sparrow, J.M.; Patel, R.; Rumley, A.; Lowe, G.; Smith, G.D.; Ben-Shlomo, Y. The prevalence and analysis of risk factors for age-related macular degeneration: 18-year follow-up data from the Speedwell eye study, United Kingdom. Eye (Lond.) 2011, 25, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Cruickshanks, K.J.; Nash, S.D.; Krantz, E.M.; Nieto, F.J.; Huang, G.H.; Pankow, J.S.; Klein, B.E. The prevalence of age-related macular degeneration and associated risk factors. Arch. Ophthalmol. 2010, 128, 750–758. [Google Scholar] [CrossRef] [PubMed]
- Roh, M.I.; Kim, J.H.; Byeon, S.H.; Koh, H.J.; Lee, S.C.; Kwon, O.W. Estimated prevalence and risk factor for age-related maculopathy. Yonsei Med. J. 2008, 49, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, R.; Wang, J.J.; Ji, G.J.; Taylor, B.; Oizumi, T.; Daimon, M.; Kato, T.; Kawata, S.; Kayama, T.; Tano, Y.; et al. Prevalence and risk factors for age-related macular degeneration in an adult Japanese population: The Funagata study. Ophthalmology 2008, 115, 1376–1381. [Google Scholar] [CrossRef] [PubMed]
- Cackett, P.; Wong, T.Y.; Aung, T.; Saw, S.M.; Tay, W.T.; Rochtchina, E.; Mitchell, P.; Wang, J.J. Smoking, cardiovascular risk factors, and age-related macular degeneration in Asians: The Singapore Malay Eye Study. Am. J. Ophthalmol. 2008, 146, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.S.; Mitchell, P.; Smith, W.; Wang, J.J. Cardiovascular risk factors and the long-term incidence of age-related macular degeneration: The Blue Mountains Eye Study. Ophthalmology 2007, 114, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, R.; Klaver, C.C.; Vingerling, J.R.; Hofman, A.; van Duijn, C.M.; Stricker, B.H.; de Jong, P.T. Cholesterol and age-related macular degeneration: Is there a link? Am. J. Ophthalmol. 2004, 137, 750–752. [Google Scholar] [CrossRef] [PubMed]
- Delcourt, C.; Michel, F.; Colvez, A.; Hofman, A.; van Duijn, C.M.; Stricker, B.H.; de Jong, P.T. Associations of cardiovascular disease and its risk factors with age-related macular degeneration: The POLA study. Ophthalmic Epidemiol. 2001, 8, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.; Assink, J.; Klein, R.; Mitchell, P.; Klaver, C.C.; Klein, B.E.; Hofman, A.; Jensen, S.; Wang, J.J.; de Jong, P.T. Risk factors for age-related macular degeneration: Pooled findings from three continents. Ophthalmology 2001, 108, 697–704. [Google Scholar] [CrossRef]
- Andrade, I.G.; Costa-Carvalho, B.T.; da Silva, R.; Hix, S.; Kochi, C.; Suano-Souza, F.I.; Sarni, R.O. Risk of atherosclerosis in patients with ataxia telangiectasia. Ann. Nutr. Metab. 2015, 66, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Klein, B.E.; Jensen, S.C.; Mares-Perlman, J.A.; Cruickshanks, K.J.; Palta, M. Age-related maculopathy in a multiracial United States population: The National Health and Nutrition Examination Survey III. Ophthalmology 1999, 106, 1056–1065. [Google Scholar] [CrossRef]
- Mei, X.; Atkinson, D. Lipid-free apolipoprotein A-I Structure: Insights into HDL formation and atherosclerosis development. Arch. Med. Res. 2015, 46, 351–360. [Google Scholar] [CrossRef]
- Rader, D.J.; Tall, A.R. The not-so-simple HDL story: Is it time to revise the HDL cholesterol hypothesis? Nat. Med. 2012, 18, 1344–1346. [Google Scholar] [CrossRef]
- Izumi-Nagai, K.; Nagai, N.; Ohgami, K.; Satofuka, S.; Ozawa, Y.; Tsubota, K.; Umezawa, K.; Ohno, S.; Oike, Y.; Ishida, S. Macular pigment lutein is antiinflammatory in preventing choroidal neovascularization. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Margrain, T.H.; Boulton, M.; Marshall, J.; Sliney, D.H. Do blue light filters confer protection against age-related macular degeneration? Prog. Retin. Eye Res. 2004, 23, 523–531. [Google Scholar] [CrossRef]
- Hima Bindu, G.; Rao, V.S.; Kakkar, V.V. Friend turns foe: Transformation of anti-inflammatory HDL to proinflammatory HDL during acute-phase response. Cholesterol 2011, 2011, 274629. [Google Scholar]
- Eren, E.; Yilmaz, N.; Aydin, O. High density lipoprotein and it’s dysfunction. Open Biochem. J. 2012, 6, 78–93. [Google Scholar] [CrossRef] [PubMed]
- Pikuleva, I.A.; Curcio, C.A. Cholesterol in the retina: The best is yet to come. Prog. Retin. Eye Res. 2014, 41, 64–89. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Stambolian, D.; Edwards, A.O.; Branham, K.E.; Othman, M.; Jakobsdottir, J.; Tosakulwong, N.; Pericak-Vance, M.A.; Campochiaro, P.A.; Klein, M.L.; et al. Genetic variants near TIMP3 and high-density lipoprotein–associated loci influence susceptibility to age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2010, 107, 7401–7406. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, M.; Han, Y.; Zhang, R.; Ma, L. ABCA1 rs1883025 polymorphism and risk of age-related macular degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F.; Han, Y.; Zhang, R.; Qin, L.; Wang, M.X.; Ma, L. CETP/LPL/LIPC gene polymorphisms and susceptibility to age-related macular degeneration. Sci. Rep. 2015, 5, 15711. [Google Scholar] [CrossRef]
- Tserentsoodol, N.; Sztein, J.; Campos, M.; Gordiyenko, N.V.; Fariss, R.N.; Lee, J.W.; Fliesler, S.J.; Rodriguez, I.R. Uptake of cholesterol by the retina occurs primarily via a low density lipoprotein receptor-mediated process. Mol. Vis. 2006, 12, 1306–1318. [Google Scholar] [PubMed]
- Yin, L.; Shi, Y.; Liu, X.; Zhang, H.; Gong, Y.; Gu, Q.; Wu, X.; Xu, X. A rat model for studying the biological effects of circulating LDL in the choriocapillaris-BrM-RPE complex. Am. J. Pathol. 2012, 180, 541–549. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Ethnicity | Study Design | Sample | Sex (% male) | Mean Age | Blood Lipid Indicators Associated with AMD | Classification Criteria | Diagnosis Method | AMD Subtype | Study Quality * | Adjustment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cho et al., 2014 [16] | Asian | Cross-sectional | 7899 | 43.3 | 59.0 | TC, HDL, LDL, TG | ICGS | Fundus photography | Early and late AMD | High | Age |
| Park et al., 2014 [8] | Asian | Cross-sectional | 14352 | 48.3 | 58.2 | TC, HDL, LDL, TG | ICGS | Fundus photography | Early and late AMD | High | Age, gender, and smoking status |
| Erke et al., 2014 [17] | European | Cross-sectional | 2631 | 42.5 | 72.8 | TC, HDL, LDL, TG | ICGS | Fundus photography | Early AMD | High | Age, gender, smoking, and systolic blood pressure |
| Gre’goire et al., 2014 [18] | European | Cross-sectional | 963 | 38.1 | 80.2 | TC, HDL, LDL, TG | ICGS | Fundus photography | Early and late AMD | High | Age, gender, educational level, smoking, BMI, hypertension, hypolipidemic drug, cardiovascular disease, diabetes, ApoE2, ApoE4, CFH Y402H, ARMS2 A69S, LIPC(rs10468017), LIPC(rs493258) LPL, ABCA1 and CETP polymorphisms |
| Jonasson et al., 2014 [19] | European | Cohort | 2868 | 42.4 | 74.7 | TC, HDL | WARMGS | Fundus photography | Early and late AMD | High | Age and gender |
| Klein et al., 2014 [20] | American/European/Australian | Cohort | 6953 | 43.5 | 63.4 | TC, HDL | WARMGS | Fundus photography | Early and late AMD | High | Age, sex, body mass index, history of smoking status, diabetes status, hypertension status, and statin use |
| Cheung et al., 2014 [21] | Asian | Cross-sectional | 9799 | NR | 54.0 | TC, HDL, LDL | WARMGS | Fundus photography | Early and late AMD | High | Age, gender, body mass index, hypertension, diabetes, current smoker, alcohol consumption, chronic kidney disease, and race |
| Cheung et al., 2012 [22] | Asian | Cross-sectional | 3172 | 49.2 | 53.7 | TC, HDL, LDL | WARMGS | Fundus photography | Total AMD | High | Age and race |
| Butt et al., 2011 [23] | American | Cross-sectional | 1019 | 39.9 | 62.4 | TC, HDL | WARMGS | Fundus photography | Total AMD | High | Age, gender, and smoking |
| Colak et al., 2011 [9] | European | Cross-sectional | 163 | NR | 66.6 | TC, LDL | AREDS | Fundus photography | Total AMD | Low | NR |
| Ngai et al., 2011 [24] | European | Cohort | 949 | 100.0 | 71.1 | TC, HDL, LDL, TG | WARMGS | Fundus photography | Total AMD | High | Age, systolic BP, CRP, BMI, and blood glucose |
| Klein et al., 2010 [25] | American | Cross-sectional | 2810 | 45.7 | 49.0 | TC, HDL | WARMGS | Fundus photography | Early AMD | High | Age, gender, and familial correlations |
| Roh et al., 2008 [26] | Asian | Cross-sectional | 9530 | 56.9 | 52.9 | TC, HDL, LDL, TG | WARMGS | Fundus photography | Total AMD | High | Age and hepatitis B infection |
| Kawasaki et al., 2008 [27] | Asian | Cross-sectional | 1625 | 44.1 | 60.4 | TC, HDL | WARMGS | Fundus photography | Early and late AMD | High | Age and gender |
| Cackett et al., 2008 [28] | Asian | Cross-sectional | 3280 | 48.0 | 58.7 | TC, HDL, LDL, TG | WARMGS | Fundus photography | Early and late AMD | High | Age |
| Tan et al., 2007 [29] | Australian | Cohort | 2454 | 42.4 | 70.6 | TC, HDL, LDL, TG | WARMGS | Fundus photography | Early and late AMD | High | Age, gender, smoking, white cell count, family history of AMD, and very fair skin color |
| Leeuwen et al., 2004 [30] | European | Cohort | 5836 | NR | 69.6 | TC, HDL | WARMGS | Fundus photography | Total AMD | Low | Age, gender, time of follow-up, BMI, smoking, atherosclerosis, alcohol intake, and apolipoprotein E genotype |
| Klein et al., 2003 [10] | American | Cross-sectional | 2361 | 39.5 | 78.5 | TC, HDL, LDL, TG | WARMGS | Fundus photography | Early AMD | High | Age, gender, and race |
| Delcourt et al., 2001 [31] | European | Cross-sectional | 2584 | 43.7 | 70.1 | TC, HDL, TG | ICGS | Fundus photography | Early and late AMD | High | Age, gender, smoking, educational level, and plasma α-tocopherol. |
| Smith et al., 2001 [32] | American/European/Australian | Cross-sectional | 14752 | 42.6 | 66.0 | TC, HDL | WARMGS | Fundus photography | Late AMD | High | Age |
| Klein et al., 1999 [33] | American | Cross-sectional | 8270 | 48.1 | 56.3 | TC, HDL, TG | WARMGS | Fundus photography | Early AMD | High | Age |
| Variables | HDL | TC | LDL | TG | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | RR (95% CI) | PH | PM | n | RR (95% CI) | PH | PM | n | RR (95% CI) | PH | PM | n | RR (95% CI) | PH | PM | |
| Any AMD | 15 | 1.18 (1.01, 1.35) | 0.007 | 18 | 0.96 (0.93, 0.99) | 0.001 | 8 | 0.93 (0.88, 0.99) | 0.83 | 9 | 0.91 (0.87, 0.94) | 0.42 | ||||
| Early AMD | 11 | 1.10 (1.01, 1.19) | <0.001 | 11 | 0.95 (0.92, 0.99) | 0.08 | 4 | 0.95 (0.88, 0.99) | 0.99 | 8 | 0.91 (0.87, 0.95) | 0.62 | ||||
| Late AMD | 8 | 1.14 (0.81, 1.46) | 0.25 | 8 | 0.97 (0.88, 1.06) | 0.56 | 4 | 1.00 (0.86, 1.13) | 0.30 | 5 | 0.96 (0.82, 1.11) | 0.34 | ||||
| GA | 3 | 0.99 (0.23, 1.75) | 0.44 | 3 | 0.81 (0.62, 1.00) | 0.39 | - | - | ||||||||
| CNV | 3 | 1.06 (0.51, 1.62) | 0.57 | 3 | 1.04 (0.86, 1.22) | 0.26 | - | - | ||||||||
| Design | ||||||||||||||||
| Cross-sectional | 10 | 1.23 (0.97, 1.49) | 0.01 | 0.93 | 14 | 0.94 (0.87, 1.01) | <0.001 | 0.86 | 7 | 0.93 (0.88, 0.99) | 0.73 | 0.75 | 8 | 0.92 (0.89, 0.96) | 0.29 | 0.92 |
| Cohort | 5 | 1.08 (0.93, 1.24) | 0.24 | 5 | 0.98 (0.93, 1.03) | 0.55 | 1 | 0.89 (0.17, 1.61) | 1 | 0.68 (0.42, 0.94) | ||||||
| Ethnicity | ||||||||||||||||
| Asian | 4 | 1.17 (0.81, 1.53) | 0.49 | 0.76 | 6 | 0.92 (0.81, 1.02) | <0.001 | 0.78 | 3 | 0.95 (0.85, 1.06) | 0.91 | 0.67 | 3 | 0.93 (0.83, 1.03) | 0.12 | 0.74 |
| European | 6 | 1.24 (1.10, 1.39) | 0.09 | 7 | 1.00 (0.92, 1.08) | 0.06 | 4 | 0.95 (0.87, 1.03) | 0.68 | 4 | 0.87 (0.77, 0.96) | 0.34 | ||||
| American | 4 | 1.06 (0.55, 1.57) | 0.004 | 4 | 0.89 (0.76, 1.02) | 0.02 | 1 | 0.85 (0.73, 0.98) | 2 | 0.90 (0.80, 0.99) | 0.12 | |||||
| Australian | 1 | 0.96 (0.72, 1.20) | 1 | 1.00 (0.91, 1.07) | - | - | ||||||||||
| Classification criteria | ||||||||||||||||
| WARMGS | 11 | 1.09 (0.91, 1.28) | 0.03 | 0.52 | 13 | 0.91 (0.86, 0.97) | 0.04 | 0.54 | 4 | 0.95 (0.87, 1.03) | 0.91 | 0.23 | 5 | 0.90 (0.85, 0.94) | 0.21 | 0.33 |
| ICGS | 4 | 1.34 (1.13, 1.55) | 0.14 | 4 | 1.02 (0.97, 1.08) | 0.36 | 3 | 0.91 (0.82, 0.99) | 0.72 | 4 | 0.96 (0.90, 1.02) | 0.35 | ||||
| AREDS | - | 1 | 1.89 (1.19, 2.59) | 1 | 1.59 (1.04, 2.14) | |||||||||||
| Age (years) | ||||||||||||||||
| <65 | 9 | 1.06 (0.82, 1.30) | 0.03 | 0.84 | 10 | 0.93 (0.87, 1.00) | 0.01 | 0.83 | 3 | 0.95 (0.85, 1.06) | 0.91 | 0.55 | 4 | 0.94 (0.90, 0.98) | 0.23 | 0.12 |
| ≥65 | 6 | 1.24 (1.10, 1.39) | 0.09 | 8 | 0.97 (0.89, 1.06) | <0.001 | 5 | 0.92 (0.85, 0.99) | 0.54 | 5 | 0.86 (0.78, 0.93) | 0.47 | ||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Wang, M.; Zhang, X.; Zhang, Q.; Nie, J.; Zhang, M.; Liu, X.; Ma, L. The Association between the Lipids Levels in Blood and Risk of Age-Related Macular Degeneration. Nutrients 2016, 8, 663. https://doi.org/10.3390/nu8100663
Wang Y, Wang M, Zhang X, Zhang Q, Nie J, Zhang M, Liu X, Ma L. The Association between the Lipids Levels in Blood and Risk of Age-Related Macular Degeneration. Nutrients. 2016; 8(10):663. https://doi.org/10.3390/nu8100663
Chicago/Turabian StyleWang, Yafeng, Mingxu Wang, Xiaoqing Zhang, Qianyu Zhang, Jing Nie, Ming Zhang, Xiaohong Liu, and Le Ma. 2016. "The Association between the Lipids Levels in Blood and Risk of Age-Related Macular Degeneration" Nutrients 8, no. 10: 663. https://doi.org/10.3390/nu8100663