
Does Native Vitamin D Supplementation Have Pleiotropic Effects in Patients with End-Stage Kidney Disease? A Systematic Review of Randomized Trials

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Intervention Types
2.3. Types of Outcome Measures Reported
2.4. Search Strategy
2.5. Study Selection
2.6. Data Items
2.7. Data Synthesis and Analysis
2.8. Assessment of Risk of Bias
2.9. Measurement of Treatment Effect
2.10. Safety
3. Results
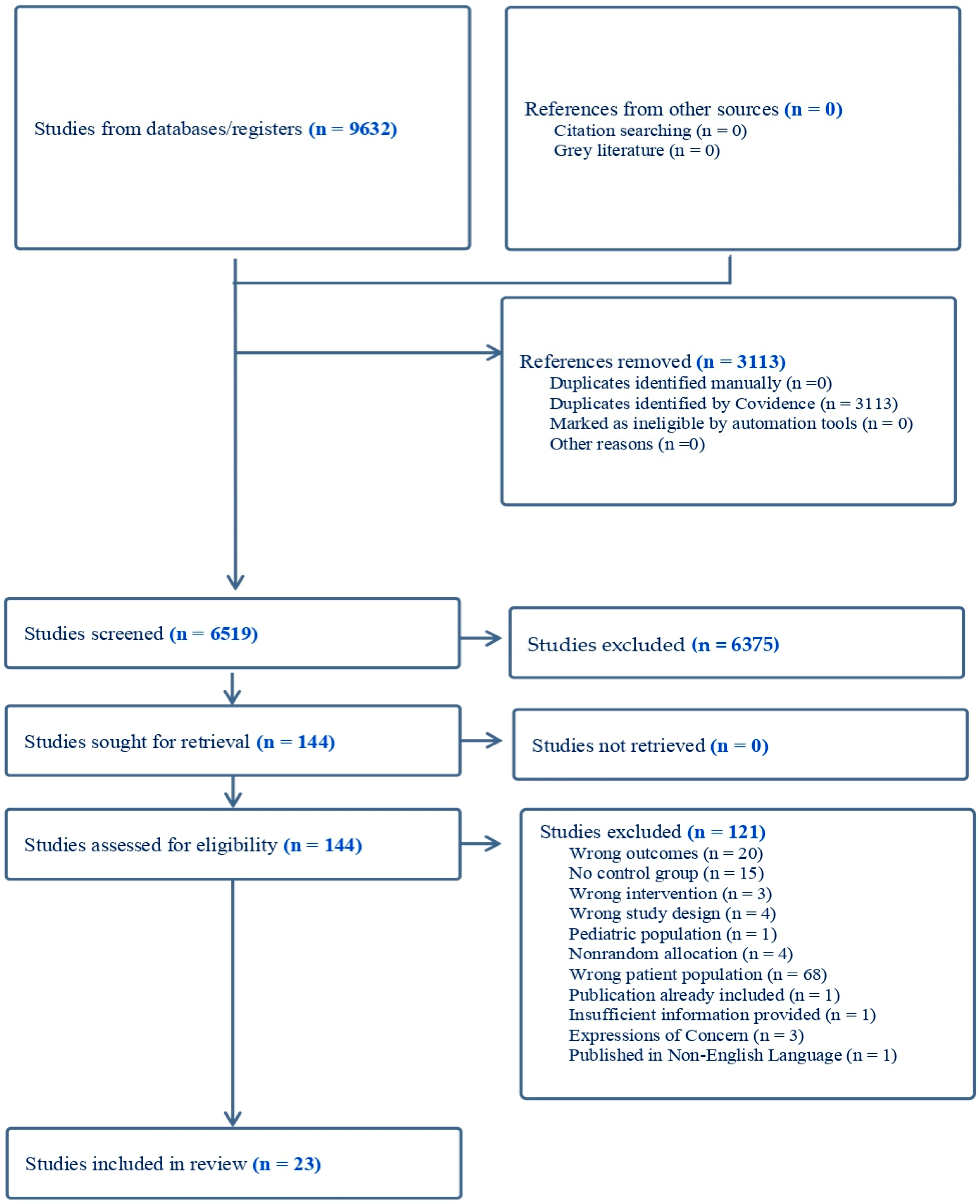
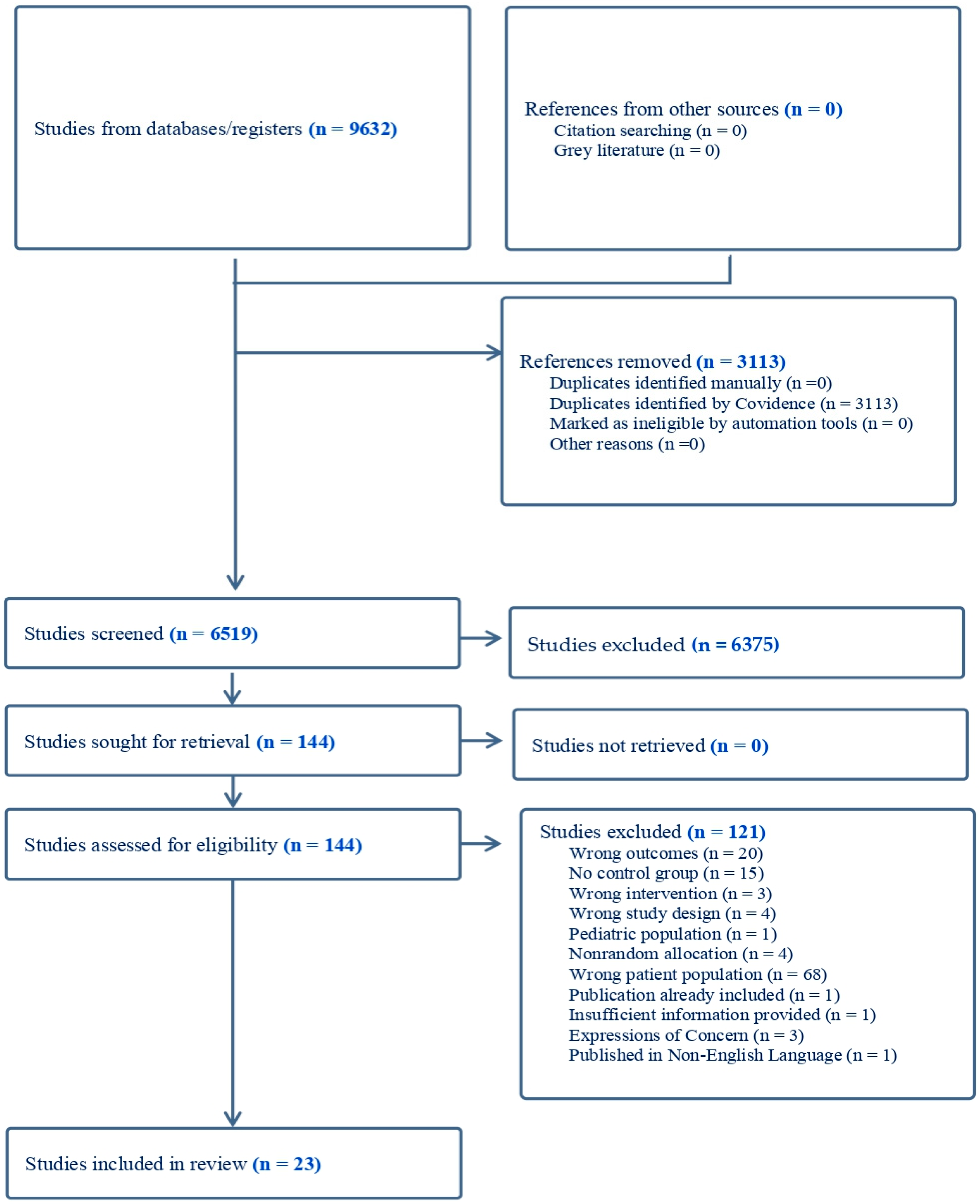
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. Vitamin D Supplementation and Mortality Outcomes
3.5. Vitamin D Supplementation and Cardiovascular Disease-Related Outcomes
3.6. Vitamin D Supplementation and Inflammation
3.7. Vitamin D Supplementation and Musculoskeletal Outcomes
3.8. Vitamin D Supplementation and Anemia, Pruritis, and Arteriovenous Fistula Maturation
3.9. Vitamin D and Metabolic/Nutritional Measures
3.10. Vitamin D Supplementation and Well-Being
3.11. Vitamin D and Changes in 25(OH)D, Hypercalcemia, and Vitamin D Toxicity
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Total Number of Records Identified for Each Database and Information Source Up to 31 January 2023
| Ovid MEDLINE | 2272 |
| Ovid Embase | 2984 |
| Ovid EBM Reviews for Cochrane CENTRAL | 1409 |
| Web of Science Core Collection | 2699 |
| medRxiv | 186 |
| ProQuest Dissertations and Theses Global | 82 |
| Total number of records | 9632 |
| Total number of records after removing duplicates in Covidence | 6519 |
Appendix B. Search Strategy Embase, MEDLINE, Cochrane CENTRAL, Web of Science, ProQuest Dissertations and Theses, medRxiv
References
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikle, D. Nonclassic Actions of Vitamin D. J. Clin. Endocrinol. Metab. 2009, 94, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González, E.A.; Sachdeva, A.; Oliver, D.A.; Martin, K.J. Vitamin D insufficiency and deficiency in chronic kidney disease. Am. J. Nephrol. 2004, 24, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Ravani, P.; Malberti, F.; Tripepi, G.; Pecchini, P.; Cutrupi, S.; Pizzini, P.; Mallamaci, F.; Zoccali, C. Vitamin D levels and patient outcome in chronic kidney disease. Kidney Int. 2009, 75, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Darssan, D.; Pascoe, E.M.; Johnson, D.W.; Pi, H.; Dong, J. Vitamin D status and mortality risk among patients on dialysis: A systematic review and meta-analysis of observational studies. Nephrol. Dial. Transpl. 2018, 33, 1742–1751. [Google Scholar] [CrossRef]
- Schiller, A.; Gadalean, F.; Schiller, O.; Timar, R.; Bob, F.; Munteanu, M.; Stoian, D.; Mihaescu, A.; Timar, B. Vitamin D deficiency—Prognostic marker or mortality risk factor in end stage renal disease patients with diabetes mellitus treated with hemodialysis—A prospective multicenter study. PLoS ONE 2015, 10, e0126586. [Google Scholar] [CrossRef] [Green Version]
- Turner, M.E.; Rowsell, T.S.; White, C.A.; Kaufmann, M.; Norman, P.A.; Neville, K.; Petkovich, M.; Jones, G.; Adams, M.A.; Holden, R.M. The metabolism of 1, 25 (OH) 2D3 in clinical and experimental kidney disease. Sci. Rep. 2022, 12, 10925. [Google Scholar] [CrossRef]
- Holden, R.M.; Mustafa, R.A.; Alexander, R.T.; Battistella, M.; Bevilacqua, M.U.; Knoll, G.; Mac-Way, F.; Reslerova, M.; Wald, R.; Acott, P.D.; et al. Canadian Society of Nephrology Commentary on the Kidney Disease Improving Global Outcomes 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder. Can. J. Kidney Health Dis. 2020, 7, 2054358120944271. [Google Scholar] [CrossRef]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.A.; Toussaint, N.D. Executive summary of the 2017 KDIGO Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD) Guideline Update: What’s changed and why it matters. Kidney Int. 2017, 92, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Bikle, D.D.; Patzek, S.; Wang, Y. Physiologic and pathophysiologic roles of extra renal CYP27b1: Case report and review. Bone Rep. 2018, 8, 255–267. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Glanville, J.; Foxlee, R.; Wisniewski, S.; Noel-Storr, A.; Edwards, M.; Dooley, G. Translating the Cochrane EMBASE RCT filter from the Ovid interface to Embase. com: A case study. Health Inf. Libr. J. 2019, 36, 264–277. [Google Scholar] [CrossRef]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Featherstone, R.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Paynter, R.; Rader, T.; et al. Technical Supplement to Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 6; Cochrane: London, UK, 2021. [Google Scholar]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Liu, Y.; Lian, Y.; Li, N.; Liu, H.; Li, G. Efficacy of High-Dose Supplementation With Oral Vitamin D3 on Depressive Symptoms in Dialysis Patients With Vitamin D3 Insufficiency: A Prospective, Randomized, Double-Blind Study. J. Clin. Psychopharmacol. 2016, 36, 229–235. [Google Scholar] [CrossRef]
- Jenabi, A.; Jabari, M.; Nabipour, M.; Khademi-Deljoo, B. The Efficacy of Oral Ergocalciferol on Changes in Parathyroid Hormone (iPTH) and One-Year Survival and Hemodialysis Factors of Patients with Chronic Renal Failure and Vitamin D Deficiency under Hemodialysis. J. Isfahan Med. Sch. 2019, 37, 190–197. [Google Scholar]
- Tamadon, M.R.; Soleimani, A.; Keneshlou, F.; Mojarrad, M.Z.; Bahmani, F.; Naseri, A.; Kashani, H.H.; Hosseini, E.S.; Asemi, Z. Note of Concern: Clinical Trial on the Effects of Vitamin D Supplementation on Metabolic Profiles in Diabetic Hemodialysis. Horm. Metab. Res. 2018, 50, e11. [Google Scholar] [CrossRef]
- Office, F.E. Expression of Concern: The Effects of Vitamin D Supplementation on Signaling Pathway of Inflammation and Oxidative Stress in Diabetic Hemodialysis: A Randomized, Double-Blind, Placebo-Controlled Trial. Front. Pharmacol. 2020, 11, 602201. [Google Scholar] [CrossRef]
- Sharif, D.A. The Effectiveness of Vitamin D Supplementation on Oxidative and Inflammatory Markers in Patients Suffering from End-stage Renal Disease, a Randomized Controlled Trial: Vitamin D and Oxidative and Inflammatory. Cell. Mol. Biol. 2022, 68, 7–15. [Google Scholar] [CrossRef]
- Mehrotra, A.; Heeger, P. Translational Science 2013 Abstracts. Clin. Transl. Sci. 2013, 6, 103–164. [Google Scholar] [CrossRef] [Green Version]
- Ambrus, A.M.C.; Almasi, C.; Berta, K.; Deak, G.; Horvath, C.; Lakatos, P.; Szabo, A.; Musci, I. Abstracts of the American Society of Nephrology 2003 Renal Week. November 12–17, 2003. San Diego, California, USA. J. Am. Soc. Nephrol. 2003, 14, 1a–1004a. [Google Scholar]
- Morrone, L.; Palmer, S.C.; Saglimbene, V.M.; Perna, A.; Cianciolo, G.; Russo, D.; Gesualdo, L.; Natale, P.; Santoro, A.; Mazzaferro, S.; et al. Calcifediol supplementation in adults on hemodialysis: A randomized controlled trial. J. Nephrol. 2022, 35, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Mieczkowski, M.; Żebrowski, P.; Wojtaszek, E.; Stompór, T.; Przedlacki, J.; Bartoszewicz, Z.; Sierdziński, J.; Wańkowicz, Z.; Niemczyk, S.; Matuszkiewicz-Rowińska, J. Long-term cholecalciferol administration in hemodialysis patients: A single-center randomized pilot study. Med. Sci. Monit. 2014, 20, 2228–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasse, H.; Huang, R.; Long, Q.; Zhao, Y.; Singapuri, S.; McKinnon, W.; Skardasis, G.; Tangpricha, V. Very high-dose cholecalciferol and arteriovenous fistula maturation in ESRD: A randomized, double-blind, placebo-controlled pilot study. J. Vasc. Access. 2014, 15, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, C.M.; Wu, C.C.; Hung, C.F.; Liao, M.T.; Shyu, J.F.; Hsu, Y.H.; Lu, C.L.; Wang, Y.H.; Zheng, J.Q.; Chang, T.J.; et al. Cholecalciferol Additively Reduces Serum Parathyroid Hormone Levels in Severe Secondary Hyperparathyroidism Treated with Calcitriol and Cinacalcet among Hemodialysis Patients. Nutrients 2018, 10, 196. [Google Scholar] [CrossRef] [Green Version]
- Khajehdehi, P. Effect of Vitamins on the Lipid Profile of Patients on Regular Hemodialysis. Scand. J. Urol. Nephrol. 2000, 34, 62–66. [Google Scholar] [CrossRef]
- Bhan, I.; Dobens, D.; Tamez, H.; Deferio, J.J.; Li, Y.C.; Warren, H.S.; Ankers, E.; Wenger, J.; Tucker, J.K.; Trottier, C.; et al. Nutritional Vitamin D Supplementation in Dialysis: A Randomized Trial. Clin. J. Am. Soc. Nephrol. 2015, 10, 611–619. [Google Scholar] [CrossRef] [Green Version]
- Miskulin, D.C.; Majchrzak, K.; Tighiouart, H.; Muther, R.S.; Kapoian, T.; Johnson, D.S.; Weiner, D.E. Ergocalciferol Supplementation in Hemodialysis Patients With Vitamin D Deficiency: A Randomized Clinical Trial. J. Am. Soc. Nephrol. 2016, 27, 1801–1810. [Google Scholar] [CrossRef] [Green Version]
- Brimble, K.S.; Ganame, J.; Margetts, P.; Jain, A.; Perl, J.; Walsh, M.; Bosch, J.; Yusuf, S.; Beshay, S.; Su, W.; et al. Impact of Bioelectrical Impedance-Guided Fluid Management and Vitamin D Supplementation on Left Ventricular Mass in Patients Receiving Peritoneal Dialysis: A Randomized Controlled Trial. Am. J. Kidney Dis. 2022, 79, 820–831. [Google Scholar] [CrossRef]
- Ayub, H.; Naseem, K.; Baig, F.A.; Ahmed, A.; Acharya, S.; Ahmed, W. Outcome of Cholecalciferol Supplementation on Bone Mineral metabolism in End Stage Renal Disease Patients in Comparison with Placebo-Randomized Control Trial. Pak. J. Med. Health Sci. 2022, 16, 700. [Google Scholar] [CrossRef]
- Delanaye, P.; Weekers, L.; Warling, X.; Moonen, M.; Smelten, N.; Médart, L.; Krzesinski, J.-M.; Cavalier, E. Cholecalciferol in haemodialysis patients: A randomized, double-blind, proof-of-concept and safety study. Nephrol. Dial. Transpl. 2013, 28, 1779–1786. [Google Scholar] [CrossRef] [Green Version]
- Gregório, P.C.; Bucharles, S.; Cunha, R.S.D.; Braga, T.; Almeida, A.C.; Henneberg, R.; Stinghen, A.E.M.; Barreto, F.C. In vitro anti-inflammatory effects of vitamin D supplementation may be blurred in hemodialysis patients. Clinics 2021, 76, e1821. [Google Scholar] [CrossRef]
- Hewitt, N.A.; O’Connor, A.A.; O’Shaughnessy, D.V.; Elder, G.J. Effects of cholecalciferol on functional, biochemical, vascular, and quality of life outcomes in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 1143–1149. [Google Scholar] [CrossRef] [Green Version]
- Meireles, M.S.; Kamimura, M.A.; Dalboni, M.A.; Giffoni de Carvalho, J.T.; Aoike, D.T.; Cuppari, L. Effect of cholecalciferol on vitamin D-regulatory proteins in monocytes and on inflammatory markers in dialysis patients: A randomized controlled trial. Clin. Nutr. 2016, 35, 1251–1258. [Google Scholar] [CrossRef]
- Mose, F.H.; Vase, H.; Larsen, T.; Kancir, A.S.; Kosierkiewic, R.; Jonczy, B.; Hansen, A.B.; Oczachowska-Kulik, A.E.; Thomsen, I.M.; Bech, J.N.; et al. Cardiovascular effects of cholecalciferol treatment in dialysis patients—A randomized controlled trial. BMC Nephrol. 2014, 15, 50. [Google Scholar] [CrossRef]
- Naini, A.E.; Hedaiati, Z.P.; Gholami, D.; Pezeshki, A.H.; Moinzadeh, F. The effect of Vitamin D administration on treatment of anemia in end-stage renal disease patients with Vitamin D deficiency on hemodialysis: A placebo-controlled, double-blind clinical trial. J. Res. Med. Sci. 2015, 20, 745–750. [Google Scholar] [CrossRef]
- Seibert, E.; Heine, G.H.; Ulrich, C.; Seiler, S.; Köhler, H.; Girndt, M. Influence of Cholecalciferol Supplementation in Hemodialysis Patients on Monocyte Subsets: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Nephron Clin. Pract. 2013, 123, 209–219. [Google Scholar] [CrossRef]
- Seirafian, S.; Haghdarsaheli, Y.; Mortazavi, M.; Hosseini, M.; Moeinzadeh, F. The effect of oral vitamin D on serum level of N-terminal pro-B-type natriuretic peptide. Adv. Biomed. Res. 2014, 3, 261. [Google Scholar] [CrossRef]
- Shirazian, S.; Schanler, M.; Shastry, S.; Dwivedi, S.; Kumar, M.; Rice, K.; Miyawaki, N.; Ghosh, S.; Fishbane, S. The Effect of Ergocalciferol on Uremic Pruritus Severity: A Randomized Controlled Trial. J. Ren. Nutr. 2013, 23, 308–314. [Google Scholar] [CrossRef]
- Singer, R.; Chacko, B.; Talaulikar, G.; Karpe, K.; Walters, G. Placebo-controlled, randomized clinical trial of high-dose cholecalciferol in renal dialysis patients: Effect on muscle strength and quality of life. Clin. Kidney J. 2019, 12, 281–287. [Google Scholar] [CrossRef]
- Ulrich, C.; Trojanowicz, B.; Fiedler, R.; Kraus, F.B.; Stangl, G.I.; Girndt, M.; Seibert, E. Serum Testosterone Levels Are Not Modified by Vitamin D Supplementation in Dialysis Patients and Healthy Subjects. Nephron 2021, 145, 481–485. [Google Scholar] [CrossRef]
- Loosman, W.L.; Rottier, M.A.; Honig, A.; Siegert, C.E. Association of depressive and anxiety symptoms with adverse events in Dutch chronic kidney disease patients: A prospective cohort study. BMC Nephrol. 2015, 16, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentata, Y. Benefit–risk balance of native vitamin D supplementation in chronic hemodialysis: What can we learn from the major clinical trials and international guidelines? Ren. Fail. 2019, 41, 607–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, C.; Li, Y.C.; Zhao, S.M.; Li, Z.X. Evaluation of responses to vitamin D3 (cholecalciferol) in patients on dialysis: A systematic review and meta-analysis. J. Investig. Med. 2016, 64, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Fang, F.; Tang, J.; Jia, L.; Feng, Y.; Xu, P.; Faramand, A. Association between vitamin D supplementation and mortality: Systematic review and meta-analysis. BMJ 2019, 366, l4673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.; Shi, H.; Jia, J.; Li, D.; Lin, S. Vitamin D supplementation and mortality risk in chronic kidney disease: A meta-analysis of 20 observational studies. BMC Nephrol. 2013, 14, 199. [Google Scholar] [CrossRef] [Green Version]
- Bond, S.; Payne, R.; Wilson, E.; Chowdry, A.; Caskey, F.; Wheeler, D.; Hiemstra, T. Using the UK renal registry for a clinical trial in dialysis patients: The example of SIMPLIFIED. Trials 2015, 16, O15. [Google Scholar] [CrossRef] [Green Version]
- Jankowski, J.; Floege, J.; Fliser, D.; Böhm, M.; Marx, N. Cardiovascular Disease in Chronic Kidney Disease: Pathophysiological Insights and Therapeutic Options. Circulation 2021, 143, 1157–1172. [Google Scholar] [CrossRef]
- Cowie, M.R.; Mendez, G.F. BNP and congestive heart failure. Prog. Cardiovasc. Dis. 2002, 44, 293–321. [Google Scholar] [CrossRef]
- Bolland, M.J.; Grey, A.; Gamble, G.D.; Reid, I.R. The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: A trial sequential meta-analysis. Lancet Diabetes Endocrinol. 2014, 2, 307–320. [Google Scholar] [CrossRef]
- Pei, Y.-Y.; Zhang, Y.; Peng, X.-C.; Liu, Z.-R.; Xu, P.; Fang, F. Association of Vitamin D Supplementation with Cardiovascular Events: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 3158. [Google Scholar] [CrossRef]
- Bucharles, S.; Barberato, S.H.; Stinghen, A.E.M.; Gruber, B.; Piekala, L.; Dambiski, A.C.; Custodio, M.R.; Pecoits-Filho, R. Impact of cholecalciferol treatment on biomarkers of inflammation and myocardial structure in hemodialysis patients without hyperparathyroidism. J. Ren. Nutr. 2012, 22, 284–291. [Google Scholar] [CrossRef] [Green Version]
- Matias, P.J.; Jorge, C.; Ferreira, C.; Borges, M.; Aires, I.; Amaral, T.; Gil, C.; Cortez, J.; Ferreira, A. Cholecalciferol supplementation in hemodialysis patients: Effects on mineral metabolism, inflammation, and cardiac dimension parameters. Clin. J. Am. Soc. Nephrol. 2010, 5, 905–911. [Google Scholar] [CrossRef] [Green Version]
- Honda, H.; Qureshi, A.R.; Heimbürger, O.; Barany, P.; Wang, K.; Pecoits-Filho, R.; Stenvinkel, P.; Lindholm, B. Serum albumin, C-reactive protein, interleukin 6, and fetuin a as predictors of malnutrition, cardiovascular disease, and mortality in patients with ESRD. Am. J. Kidney Dis. 2006, 47, 139–148. [Google Scholar] [CrossRef]
- Bucharles, S.; Barberato, S.H.; Stinghen, A.E.; Gruber, B.; Meister, H.; Mehl, A.; Piekala, L.; Dambiski, A.C.; Souza, A.; Olandoski, M.; et al. Hypovitaminosis D is associated with systemic inflammation and concentric myocardial geometric pattern in hemodialysis patients with low iPTH levels. Nephron Clin. Pract. 2011, 118, c384–c391. [Google Scholar] [CrossRef]
- Zhang, Y.; Leung, D.Y.; Richers, B.N.; Liu, Y.; Remigio, L.K.; Riches, D.W.; Goleva, E. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase-1. J. Immunol. 2012, 188, 2127–2135. [Google Scholar] [CrossRef] [Green Version]
- Moslemi, E.; Musazadeh, V.; Kavyani, Z.; Naghsh, N.; Shoura, S.M.S.; Dehghan, P. Efficacy of vitamin D supplementation as an adjunct therapy for improving inflammatory and oxidative stress biomarkers: An umbrella meta-analysis. Pharmacol. Res. 2022, 186, 106484. [Google Scholar] [CrossRef]
- Mansournia, M.A.; Ostadmohammadi, V.; Doosti-Irani, A.; Ghayour-Mobarhan, M.; Ferns, G.; Akbari, H.; Ghaderi, A.; Talari, H.R.; Asemi, Z. The Effects of Vitamin D Supplementation on Biomarkers of Inflammation and Oxidative Stress in Diabetic Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Horm. Metab. Res. 2018, 50, 429–440. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Yang, S.; Zhou, Q.; Zhang, H.; Yi, B. Effects of Vitamin D Supplementation on Renal Function, Inflammation and Glycemic Control in Patients with Diabetic Nephropathy: A Systematic Review and Meta-Analysis. Kidney Blood Press. Res. 2019, 44, 72–87. [Google Scholar] [CrossRef]
- Carrero, J.J.; Qureshi, A.R.; Parini, P.; Arver, S.; Lindholm, B.; Bárány, P.; Heimbürger, O.; Stenvinkel, P. Low serum testosterone increases mortality risk among male dialysis patients. J. Am. Soc. Nephrol. 2009, 20, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Cigarrán, S.; Pousa, M.; Castro, M.J.; González, B.; Martínez, A.; Barril, G.; Aguilera, A.; Coronel, F.; Stenvinkel, P.; Carrero, J.J. Endogenous testosterone, muscle strength, and fat-free mass in men with chronic kidney disease. J. Ren. Nutr. 2013, 23, e89–e95. [Google Scholar] [CrossRef]
- Wang, N.; Han, B.; Li, Q.; Chen, Y.; Chen, Y.; Xia, F.; Lin, D.; Jensen, M.D.; Lu, Y. Vitamin D is associated with testosterone and hypogonadism in Chinese men: Results from a cross-sectional SPECT-China study. Reprod. Biol. Endocrinol. 2015, 13, 74. [Google Scholar] [CrossRef] [Green Version]
- Wehr, E.; Pilz, S.; Boehm, B.O.; März, W.; Obermayer-Pietsch, B. Association of vitamin D status with serum androgen levels in men. Clin. Endocrinol. 2010, 73, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Manoj, P.; Derwin, R.; George, S. What is the impact of daily oral supplementation of vitamin D3 (cholecalciferol) plus calcium on the incidence of hip fracture in older people? A systematic review and meta-analysis. Int. J. Older People Nurs. 2023, 18, e12492. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.M.; Eslick, G.D.; Nowson, C.; Smith, C.; Bensoussan, A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: A meta-analysis. Lancet 2007, 370, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Mapes, D.L.; Lopes, A.A.; Satayathum, S.; McCullough, K.P.; Goodkin, D.A.; Locatelli, F.; Fukuhara, S.; Young, E.W.; Kurokawa, K.; Saito, A.; et al. Health-related quality of life as a predictor of mortality and hospitalization: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. 2003, 64, 339–349. [Google Scholar] [CrossRef] [Green Version]
- Anand, S.; Kaysen, G.A.; Chertow, G.M.; Johansen, K.L.; Grimes, B.; Dalrymple, L.S.; Kurella Tamura, M. Vitamin D deficiency, self-reported physical activity and health-related quality of life: The Comprehensive Dialysis Study. Nephrol. Dial. Transpl. 2011, 26, 3683–3688. [Google Scholar] [CrossRef] [Green Version]
- Rayner, H.C.; Larkina, M.; Wang, M.; Graham-Brown, M.; van der Veer, S.N.; Ecder, T.; Hasegawa, T.; Kleophas, W.; Bieber, B.A.; Tentori, F. International comparisons of prevalence, awareness, and treatment of pruritus in people on hemodialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 2000–2007. [Google Scholar] [CrossRef] [Green Version]
- Sukul, N.; Speyer, E.; Tu, C.; Bieber, B.A.; Li, Y.; Lopes, A.A.; Asahi, K.; Mariani, L.; Laville, M.; Rayner, H.C. Pruritus and patient reported outcomes in non-dialysis CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 673–681. [Google Scholar] [CrossRef]
- Blachley, J.D.; Blankenship, D.M.; Menter, A.; Parker, T.F., 3rd; Knochel, J.P. Uremic pruritus: Skin divalent ion content and response to ultraviolet phototherapy. Am. J. Kidney Dis. 1985, 5, 237–241. [Google Scholar] [CrossRef]
- Gilchrest, B.A.; Rowe, J.W.; Brown, R.S.; Steinman, T.I.; Arndt, K.A. Relief of uremic pruritus with ultraviolet phototherapy. N. Eng. J. Med. 1977, 297, 136–138. [Google Scholar] [CrossRef]
- Spinowitz, B.; Pecoits-Filho, R.; Winkelmayer, W.C.; Pergola, P.E.; Rochette, S.; Thompson-Leduc, P.; Lefebvre, P.; Shafai, G.; Bozas, A.; Sanon, M.; et al. Economic and quality of life burden of anemia on patients with CKD on dialysis: A systematic review. J. Med. Econ. 2019, 22, 593–604. [Google Scholar] [CrossRef] [Green Version]
- Icardi, A.; Paoletti, E.; De Nicola, L.; Mazzaferro, S.; Russo, R.; Cozzolino, M. Renal anaemia and EPO hyporesponsiveness associated with vitamin D deficiency: The potential role of inflammation. Nephrol. Dial. Transpl. 2013, 28, 1672–1679. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Parameter | Inclusion Criteria |
|---|---|
| Population | End-stage kidney disease requiring dialysis treatment |
| Intervention | Native vitamin D |
| Comparison | Non-exposed control group |
| Outcomes | Any clinical or measured outcome |
| Settings | Randomized trials |
| Author Year Country # Centers | Population | Follow-Up (mo) | Intervention | Control | Randomized (n) | Included in Final Analysis (n) | Primary Outcome of the Trial | Clinical Outcome Measures Included In Review | Age (Mean (SD)) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VD | Control | VD | Control | VD | Control | |||||||
| Ambrus # 2003 * Hungary 1 [21] | HD | 12 | D3, 3000–9000 IU weekly | Standard care | 45 | 45 | NR | NR | Mineral metabolism and VD status | Femoral neck BMD (g/cm2) | 58 ± 15 | 56 ± 15 |
| Ayub 2022 Pakistan 1 [30] | HD 25D < 75 nmol/L | 2 | D3, 50,000 IU weekly in 25D < 37 nmol/L, 10,000 IU weekly in 25D 40–75 nmol/L | Placebo | 35 | 35 | Biomarkers of mineral metabolism | CRP, VAS for pain, albumin, Hb | 49.5 ± 10.1 | 46.9 ± 14 | ||
| Bhan 2015 United States 3 [27] | HD 25D < 80 nmol/L | 4 | D2, 50,000 IU weekly | Placebo | 36 | 36 | 36 | 36 | 25D levels | All-cause mortality, all-cause and cause-specific hospitalizations | 53 ± 17 | 59 ± 17 |
| D2, 50,000 IU monthly | 33 | 33 | 58 ± 16 | |||||||||
| Brimble 2022 Canada 6 [29] | PD | 12 | D3, 50,000 IU weekly for 8 weeks, followed by 10,000 IU weekly for 44 weeks and BIA guided care | Placebo and BIA guided care | 19 | 13 | 15 | 9 | Change in LV mass (cardiac MRI) | Composite of death, nonfatal CV event, transfer to HD, fractures | 61.5 ± 13.3 | 61.7 ± 11.9 |
| D3, 50,000 IU weekly for 8 weeks, followed by 10,000 IU weekly for 44 weeks and standard care | Placebo and standard care | 15 | 18 | 14 | 15 | |||||||
| Delanaye 2013 Belgium 3 [31] | HD 25D < 75 nmol/L | 12 | D3, 25,000 IU bi-weekly | Placebo | 22 | 21 | 16 | 14 | 25D levels | AAC score, PVW | 75 ± 9 | 73 ± 12 |
| Gregorio, 2021 * Brazil 1 [32] | HD 25D < 75 nmol/L | 6 | D3, 50,000 IU weekly. After 3 mo, patients with sufficient 25(OH)D received 50,000 IU monthly | Placebo | 18 | 14 | 12 | 11 | Inflammation (in vitro assays, CRP) | Hb, albumin | 59.0 ** [51.8–60.3] | 55.5 ** [50.5–65.23] |
| Hewitt 2013 Australia NR [33] | HD 25D < 60 nmol/L | 6 | D3, 50,000 IU weekly for 8 weeks, followed by monthly for 4 months | Placebo | 30 | 30 | 29 | 27 | Muscle strength | Functional capacity, HRQOL, PWV, fractures | 60 ** [53, 71] | 67 ** (54, 72) |
| Khajehdehi, 2000 Iran NR [26] | HD | 3 | D3, 50,000 IU daily | Placebo | 21 | 21 | 15 | 14 | Serum values of triglyceride, cholesterol, LDL-c, and HDL-c | Median 31.4 years | ||
| Mehrotra # 2013 * United States NR [20] | HD 25D < 62 nmol/L | 6 | D3, 50,000 IU weekly | Standard care | 51 | 28 | NR | NR | EPO dose | Hb | NR | NR |
| Meireles 2016 Brazil 1 [34] | HD, PD 25D < 50 nmol/L | 3 | D3, 50,000 IU twice weekly | Placebo | 28 | 27 | 20 | 18 | Expression of VDR in monocytes | CRP | 55.5 ± 14.2 | 56.5 ± 12.9 |
| Mieczkowski 2014 Poland 1 [23] | HD 25D < 50 nmol/L | 12 | D3, 2000 IU 3 times/week | Standard care | 8 | 11 | NR | NR | Vitamin D levels | BMD | 63 (52–79) | 46 (29–79) |
| Miskulin 2016 United States 12 [28] | HD 25D ≤ 75 nmol/L | 6 | D2, 50,000 IU weekly or weekly for 3 months then monthly (depending on baseline 25D status) | Placebo | 137 | 139 | 122 | 130 | EPO dose | CRP cardiovascular hospitalizations, falls, fractures | 61.0 ± 13.3 | 60.8 ± 13.9 |
| Morrone, 2021 * Italy 28 [22] | HD 25D < 75 nmol/L | 24 | Calcifediol, 40 mcg thrice weekly | Standard care | 143 | 141 | 143 | 141 | Nonfatal MI, nonfatal stroke, and death from any cause (except trauma) | Cardiovascular and non-cardiovascular mortality, fatal MI, fatal stroke | 67.1 ± 13.2 | 65.1 ± 12.6 |
| Mose 2014 Denmark 1 [35] | HD, PD | 6 | D3, 3000 IU daily | Placebo | 32 | 32 | 25 | 25 | p-BNP | 24-h BP, PWV, and CRP LVMI LVEF | 68 ± 9 | 67 ± 13 |
| Naini 2015 Iran 1 [36] | HD 25D < 75 nmol/L Hb < 110 gLl | 4 | VD not specified, 50,000 IU weekly for 12 weeks and then every three weeks until participants reached 650,000 IU | Placebo | 32 | 32 | 32 | 32 | Hb, EPO dose | 60 ± 19 | 62 ± 21 | |
| Seibert 2013 Germany 1 [37] | HD 25D < 80 nmol/l | 3 | D3, 20,000 IU twice weekly to once monthly depending on baseline VD status | Placebo | 19 | 19 | 15 | 18 | Number of CD14+ and CD16+ cells per mL of blood | CRP | 66.9 ± 10.8 | 67.4 ± 9.8 |
| Seirafian 2014 Iran 1 [38] | PD, 25D < 75 nmol/L | 3 | VD, 50,000 IU weekly for 12 weeks if 25D level was <25 nmol/L and for 8 weeks if 25–75 nmol/L | Placebo | 49 | 40 | 46 | 38 | BNP | Albumin | 55.1 ± 17.4 | 54.6 ± 13.5 |
| Shirazian 2013 United States 1 [39] | HD, with excessive pruritis | 3 | D3, 50,000 IU weekly | Placebo | 25 | 25 | 25 | 25 | Pruritus severity | 66.1 ± 14.7 | 66.2 ± 13.7 | |
| Singer 2019 Australia 1 [40] | PD, HD 25D < 50 nmol/L | 12 | D3, 50,000 IU weekly | Placebo | 36 | 32 | 29 | 26 | KDQOL-SF, grip strength | Blood pressure, cardiac ischemia | 59.5 ± 15.6 | 63.8 ± 14.2 |
| Ulrich 2021 Germany 1 [41] | HD | 3 | D3, 800 IU daily | Placebo | 19 | 19 | 15 | 18 | Testosterone | 66.9 ± 10.8 | 67.4 ± 9.8 | |
| Wang 2016 China 3 [15] | HD, PD 25D 37–80 nmol/L | 12 | D3, 50,000 IU weekly | Placebo | 373 | 373 | 362 | 364 | BDI-II | MDDs, vascular depression CRP | NR | NR |
| Wasse, 2014 United States 1 [24] | HD preparing to receive AVF within 4 weeks | 0.75 | D3, 200,000 IU weekly | Placebo | 25 | 27 | 20 | 24 | 25D levels | Arteriovenous access maturation at 6 months | 49.9 ± 10.9 | 52.1 ± 14.9 |
| Zheng *, 2018 Taiwan [25] | HD, with severe SHPT | 6 | D3, 500 IU daily; Cinacalcet, 30 mcg daily; calcitriol (unique dose) | Placebo, Cinacalcet 30 mcg daily, Calcitriol (unique dose) | 30 | 30 | 27 | 28 | Serum iPTH < 300 pg/mL | 10% improvement in femoral neck BMD | 66.2 ± 12.8 | 65.6 ± 13.4 |
| Author | Randomization Process | Effect of Assignment to Intervention | Effect of Adhering to Intervention | Missing Outcome Data | Measurement of Outcomes | Selection of the Reported Results |
|---|---|---|---|---|---|---|
| Ambrus #, 2003 [21] | Some concerns | High | High | High | Some concerns | Some concerns |
| Ayub, 2022 [30] | Some concerns | High | High | High | Low | Some concerns |
| Bhan, 2015 [27] | Low | Low | Low | Low | Low | Low |
| Brimble, 2022 [29] | Low | Low | Low | Low | Low | Low |
| Delanaye, 2013 [31] | Low | Low | Low | Some concerns | Low | Low |
| Gregorio, 2021 [32] | Some concerns | Low | Low | High | Low | Some concerns |
| Hewitt, 2013 [33] | Low | Low | Low | Low | Low | Low |
| Khajehdehi, 2000 [26] | High risk | High | High | High | Low | Some concerns |
| Mehrotra #, 2013 [20] | Some concerns | High | High | High | High | Some concerns |
| Meireles, 2016 [34] | Low | Low | Some concerns | High | Low | Low |
| Mieczkowski, 2014 [23] | Low | High | High | High | Some concerns | Some |
| Miskulin, 2016 [28] | Low | Low | Low | Low | Low | Low |
| Morrone, 2021 [22] | Low | Low | Some concerns | Low | Some concerns | Low |
| Mose, 2014 [35] | Low | Low | Low | Low | Low | Some concerns |
| Naini, 2015 [36] | Some concerns | Some concerns | High | High | Low | Low |
| Seibert, 2013 [37] | Low | Low | Low | Low | Low | Low |
| Seirafian, 2014 [38] | Some concerns | Low | Low | Low | Low | Low |
| Shirazian, 2013 [39] | Low | Low | Low | Low | Low | Some concerns |
| Singer, 2019 [40] | Low | Low | Low | low | Low | Low |
| Ulrich, 2021 [41] | Low | Some concerns | Some concerns | High | Low | Low |
| Wang, 2016 [15] | Low | Low | Some | Low | Low | Some concerns |
| Wasse, 2014 [24] | Some concerns | Low | Low | low | Low | Low |
| Zheng, 2018 [25] | High | Low | Low | Low | High | High |
| Author, Year | Length of Follow-Up (mo) | Study Arms | Randomized (n) | Lost to Follow-Up (n) | Included in Final Analysis (n) | Outcome Details | Outcome Measurements | p Value * |
|---|---|---|---|---|---|---|---|---|
| End of Follow-Up | ||||||||
| All-cause mortality | ||||||||
| Bhan, 2015 [27] | 4 1 | D2 weekly | 36 | 0 | 36 | All-cause mortality (n,%) | 3 (8.3%) | 0.08 |
| D2 monthly | 33 | 0 | 33 | 0 (0%) | ||||
| Placebo | 36 | 0 | 36 | 5 (13.9%) | ||||
| Brimble, 2022 [29] | 12 2 | D3, BIA, or standard care | 34 | 0 | 34 | All-cause mortality (n,%) | 4 (12%) | 0.004 |
| Placebo, BIA, or standard care | 31 | 0 | 31 | 12 (39%) | ||||
| Morrone, 2021 [22] | 24 | Calcifediol | 143 | 26 | 143 | Death (any cause, excluding trauma or accidental) (n,%) | 33 (23.1%) | HR (95% CI): 1.11 (0.67–1.83) ns |
| Standard care | 141 | 28 | 141 | 28 (19.9%) | ||||
| Singer, 2019 [40] | 12 | D3 | 36 | 7 | 29 | Death (n,%) | 1 (3%) | 0.54 |
| Placebo | 32 | 6 | 26 | 0 (0%) | ||||
| Hospitalizations and adverse events (excluding cardiovascular events) | ||||||||
| Bahn, 2015 [27] | 4 1 | D2 weekly | 36 | 0 | 36 | Hospitalization (n,%) | 14 (38.9%) | 0.89 |
| D2 monthly | 33 | 0 | 33 | 11 (33.3%) | ||||
| Placebo | 36 | 0 | 36 | 13 (36.1%) | ||||
| D2 weekly | 36 | 0 | 36 | Infections (n,%) | 11 (30.6%) | 0.56 | ||
| D2 monthly | 33 | 0 | 33 | 11 (33.3%) | ||||
| Placebo | 36 | 0 | 36 | 8 (22.2%) | ||||
| D2 weekly | 36 | 0 | 36 | Respiratory events (n,%) | 3 (8.3%) | 0.92 | ||
| D2 monthly | 33 | 0 | 33 | 2 (6.1%) | ||||
| Placebo | 36 | 0 | 36 | 3 (8.3%) | ||||
| D2 weekly | 36 | 0 | 36 | Adverse events (n,%) | 33 (91.7%) | 0.22 | ||
| D2 monthly | 33 | 0 | 33 | 26 (78.8%) | ||||
| Placebo | 36 | 0 | 36 | 28 (77.8%) | ||||
| Brimble, 2022 [29] | 12 2 | D3 | 34 | 0 | 34 | Limb amputation (n,%) | 1 (3%) | 0.2 |
| Placebo | 31 | 0 | 31 | 2 (7%) | ||||
| D3 | 34 | 0 | 34 | Hospitalizations per patient (n,%) | 2 (1–3) | 0.7 | ||
| Placebo | 31 | 0 | 31 | 2 (1–3) | ||||
| Miskulin, 2016 [28] | 6 | D2 | 137 | 15 | 122 | All-cause hospitalization IRR | 0.82 (0.60 to 1.12) | 0.20 |
| Placebo | 139 | 9 | 130 | 1.00 (ref) | ||||
| D2 | 137 | 15 | 122 | Infection-related hospitalization IRR | 1.03 (0.50 to 2.10) | 0.95 | ||
| Placebo | 139 | 9 | 130 | 1.00 (ref) | ||||
| Morrone, 2021 [22] | 24 | Calcifediol | 143 | 26 | 143 | Hospitalization (n,%) | 21 (14.7%) | 0.51 |
| Standard care | 141 | 28 | 141 | 16 (11.3%) | ||||
| Calcifediol | 143 | 26 | 143 | Serious adverse events (n,%) | 45 (31.5%) | 0.48 | ||
| Standard care | 141 | 28 | 141 | 39 (27.0%) | ||||
| Calcifediol | 143 | 26 | 143 | Non-CV death (n,%) | 24 (16.8) | HR (95% CI): 1.13 (0.63–2.04) | ||
| Standard care | 141 | 28 | 141 | 20 (14.2) | ||||
| Singer, 2019 [40] | 12 | D3 | 36 | 7 | 29 | Hospital admission (n,%) | 22 (61%) | 0.63 |
| placebo | 32 | 6 | 26 | 17 (53%) | ||||
| Author, Year | Length of Follow-Up (Mo) | Study Arms | Randomized (n) | Lost to Follow-Up (n) | Included in Final Analysis (n) | Outcome Details | Outcome Measurements | p Value * | |
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | ||||||||
| Surrogate cardiovascular endpoints | |||||||||
| Brimble, 2022 [29] | 12 | D3 | 34 | 5 | 29 | LVM (g) 1 | 144.2 ± 50.2 | 134.3 ± 47.1 | 0.6 |
| Placebo | 31 | 7 | 24 | 142.8 ± 52.3 | 136.3 ± 52.7 | ||||
| D3 | 34 | 5 | 29 | LVMI (g/m2) | 76.0 ± 25.4 | 69.1 ± 21.6 | 0.4 | ||
| Placebo | 31 | 7 | 24 | 73.2 ±23.0 | 70.6 ± 24.5 | ||||
| D3 | 34 | 5 | 29 | LVEF (%) | 58.5 ± 8.6 | 56.5 ± 10.0 | 0.7 | ||
| Placebo | 31 | 7 | 24 | 56.5 ± 10.3 | 56.5 ± 8.7 | ||||
| Delayne, 2013 [31] | 12 | D3 | 22 | 6 | 16 | AAC score | 8 ± 5 | 10 ± 6 | 0.89 |
| Placebo | 21 | 7 | 14 | 8 ± 8 | 1 ± 7 | ||||
| Hewitt, 2013 [33] | 6 | D3 | 30 | 9 | 21 | PWV (m/s) | NR | 9.3 ± 3.3 | 0.76 |
| Placebo | 30 | 6 | 24 | NR | 10.5 ± 2.8 | ||||
| Mose, 2014 [35] | 6 | D3 | 32 | 7 | 25 | 24 h SBP (mmHg) | 135 ± 18 | 130 ± 14 | 0.511 |
| Placebo | 32 | 7 | 25 | 136 ± 22 | 127 ± 23 | ||||
| D3 | 32 | 7 | 25 | 24 h DBP (mmHg) | 73 ± 9 | 71 ± 8 | 0.451 | ||
| Placebo | 32 | 7 | 25 | 73 ± 10 | 69 ± 10 | ||||
| D3 | 32 | 10 | 22 | PWV (m/s) | 9.7 ± 2.5 | 10.5 ± 4.0 | 0.269 | ||
| Placebo | 32 | 13 | 19 | 10.0 ± 2.0 | 10.1 ±2.5 | ||||
| D3 | 32 | 10 | 22 | LVEF % 2 | 53 ± 14 | 56 ± 12 | 0.515 | ||
| Placebo | 32 | 8 | 24 | 52 ± 14 | 52 ± 17 | ||||
| D3 | 32 | 10 | 22 | LVMI (g/m2) | 123 ± 34 | 127 ± 50 | 0.397 | ||
| Placebo | 32 | 8 | 24 | 116 ± 36 | 111 ± 39 | ||||
| Cardiovascular events (death, MI, stroke) | |||||||||
| Bahn, 2015 [27] | 4 3 | D2 weekly | 36 | 0 | 36 | CV events (n, %) | 6 (16.7%) | 0.31 | |
| D2 monthly | 33 | 0 | 33 | 2 (6.1%) | |||||
| Placebo | 36 | 0 | 36 | 3 (8.3%) | |||||
| Brimble, 2022 [29] | 12 | D3 | 34 | 0 | 34 | CV events (n, %) | 5 (15%) | 0.4 | |
| Placebo | 31 | 0 | 31 | 7 (23%) | |||||
| D3 | 34 | 0 | 34 | Deaths from CV cause (n,%) | 1 (3%) | 0.03 | |||
| Placebo | 31 | 0 | 31 | 6 (19%) | |||||
| Placebo | 31 | 0 | 31 | 2 (7%) | |||||
| Miskulin, 2016 [28] | 6 | D2 | 137 | 15 | 122 | CV disease hospitalization IRR | 0.60 (0.33–1.09) | 0.1 | |
| Placebo | 139 | 9 | 130 | 1.00 (ref) | |||||
| Morrone, 2021 [22] | 24 | Calcifediol | 143 | 26 | 143 | Cardiovascular Death (n,%) | 9 (6.3%) | HR (95 CI): 1.06 (0.41–2.74) | |
| Standard care | 141 | 28 | 141 | 8 (5.7%) | |||||
| Standard care | 141 | 28 | 141 | 0 (0%) | |||||
| Biomarker outcomes (BNP) | |||||||||
| Mose, 2014 [35] | 6 | D3 | 32 | 7 | 25 | BNP (pmol/L) | 61 (26, 378) | 95 (35, 363) | 0.82 |
| Placebo | 32 | 7 | 25 | 81 (24, 186) | 50 (30, 265) | ||||
| Placebo | 32 | 7 | 25 | 10 (4, 19) | 8 (6, 23) | ||||
| Seirafian, 2014 [38] | 3 | VD | 49 | 3 | 46 | Pro-BNP (pg/mL) | 8951 ± 1631 | 895.9 ± 779.6 | 0.50 ** |
| Placebo | 40 | 2 | 38 | 7933 ± 1492 | 736.7 ± 797.9 | 0.52 ** | |||
| Author, Year | Length of Follow-Up (mo) | Study Arms | Randomized (n) | Lost to Follow-Up (n) | Included in Final Analysis (n) | Outcome Details | Outcome Measurements | p Value * | |
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End of Follow-Up | ||||||||
| Ayub, 2022 [30] | 2 | D3 | 35 | CRP (mg/dL) | 6.8 ± 4.2 | 5.0 ± 3.7 | 0.005 | ||
| Placebo | 35 | 7.9 ± 4.5 | 7.5 ± 3.8 | ||||||
| Gregiorio, 2021 [32] | 6 | D3 | 18 | 6 | 12 | hs-CRP (mg/dL) | 0.44 [0.25, 1.2] | 0.57 [0.17, 2.0] | ns |
| Placebo | 14 | 3 | 11 | 0.25 [0.1, 1.1] | 0.44 [0.2, 1.9] | ||||
| Hewitt, 2013 [33] | 6 | D3 | 30 | 9 | 21 | CRP (mg/L) | 9 [5, 17] | NR | ns |
| Placebo | 30 | 6 | 24 | 10 [5, 20] | NR | ||||
| Miereles, 2016 [34] | 3 | D3 | 28 | 8 | 20 | CRP (mg/dL) | 0.50 [0.1, 1.3] | 0.28 [0.1, 0.6] | <0.05 ** |
| Placebo | 27 | 9 | 18 | 0.57 [0.2, 1.7] | 0.48 [0.2, 1.7] | ||||
| Miskulin, 2016 [28] | 6 | D2 | 137 | 15 | 122 | hs-CRP (mg/L) | 5.1 [1.8, 10.3] | 5.9 * [2.0, 14.5] | 0.22 |
| Placebo | 139 | 9 | 130 | 3.8 [1.5, 12.0] | 4.4 [1.7, 10.9] | ||||
| Mose, 2014 [35] | 6 | D3 | 32 | 7 | 25 | CRP (mg/L) | 3.4 [1.1, 13.3] | 3.9 [1.1, 11.3] | 0.24 |
| Placebo | 32 | 7 | 25 | 4.5 [1.7, 11.7] | 2.5 [1.6, 13.9] | ||||
| Seibert, 2013 [37] | 3 | D3 | 19 | 4 | 15 | CRP (mg/L) | 4.8 [0.6–33.2] | 7.5 [0.6–36.9] | ns |
| Placebo | 19 | 1 | 18 | 5.6 [0.8–19.4] | 4.2 [0.6–14.5] | ns | |||
| Wang, 2016 [15] | 12 | D3 | 362 | 0 | 362 | hs-CRP (mg/L) | 9.1 ± 3.3 | 8.4 ± 3.1 | 0.48 |
| Placebo | 364 | 0 | 364 | 10.5 ± 2.6 | 10.3 ± 3.6 | ||||
| Author, Year | Length of Follow-Up (mo) | Study Arms | Randomized (n) | Lost to Follow-Up (n) | Included in Final Analysis (n) | Outcome Details | Outcome Measurements | p Value * | |
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Study Exit | ||||||||
| Miskulin, 2016 [28] | 6 | D2 | 137 | 15 | 122 | Falls IRR | 1.03 (0.56–1.88) | 0.94 | |
| Placebo | 139 | 9 | 130 | 1.00 (ref) | |||||
| D2 | 137 | 15 | 122 | Fractures IRR | 5.13 (0.60–43.88) | 0.14 | |||
| Placebo | 139 | 9 | 130 | 1.00 (ref) | |||||
| Brimble, 2022 [29] | 12 | D3 | 34 | 0 | 34 | Fractures (n, %) | 1 (3%) | 0.5 | |
| Placebo | 31 | 0 | 31 | 2 (7%) | |||||
| Hewitt, 2013 [33] | 6 | D3 | 30 | 9 | 21 | Fractures (n) | 1 | ns | |
| Placebo | 30 | 6 | 24 | 0 | |||||
| D3 | 30 | 9 | 21 | Grip strength (kg, 95 CI) | 23 [19, 28] | 24 [21, 28] | 0.28 | ||
| Placebo | 30 | 6 | 24 | 21 [17, 25] | 21 [17, 24] | ||||
| Singer, 2019 [40] | 12 | D3 | 36 | 7 | 29 | Grip strength (kg, IQR) | 27.5 (22, 37.5] | 26 [22, 38] | 0.81 |
| Placebo | 32 | 6 | 26 | 24 [20, 35.8] | 27 [19, 39] | ||||
| Ambrus, 2003 [21] | 12 | VD | 45 | NR | NR | FN-BMD | 0.75 ± 0.16 | 0.75 ± 0.16 | <0.01 |
| Placebo | 45 | NR | NR | 0.74 ± 0.17 | 0.70 ± 0.16 | ||||
| Zheng, 2018 [25] | 4 | D3 | 30 | 3 | 27 | FN-BMD (g/cm2) | 0.57 ± 0.04 | 0.67 ± 0.07 | <0.05 ** |
| Placebo | 30 | 2 | 28 | 0.58 ± 0.05 | 0.62 ± 0.06 | <0.05 ** | |||
| D3 | 30 | 3 | 27 | LS-BMD (g/cm2) | 0.91 ± 0.09 | 0.96 ± 0.10 | <0.05 ** | ||
| Placebo | 30 | 2 | 28 | 0.89 ± 0.07 | 0.94 ± 0.08 | <0.05 ** | |||
| Mieczkowski, 2014 [23] | 12 | D3 | 8 | NR | NR | Z score, radius | NSR 1 | NSR 1 | ns ** |
| Standard care | 11 | NR | NR | NSR 1 | NSR 1 | ns ** | |||
| D3 | 8 | NR | NR | Z score L1–L4 | NSR 1 | NSR 1 | ns ** | ||
| Standard care | 11 | NR | NR | NSR 1 | NSR 1 | ns ** | |||
| D3 | 8 | NR | NR | Z score, femur | NSR 1 | NSR 1 | ns ** | ||
| Standard care | 11 | NR | NR | NSR 1 | NSR 1 | ns ** | |||
| Ulrich, 2021 [41] | 3 | D3 | 19 | 4 | 15 | Testosterone (nmol/L) | 8.0 ± 3.7 (M) 1.3 ± 1.0 (F) | 7.8 ± 3.8 (M) 1.2 ± 1.0 (F) | ns ** |
| Placebo | 19 | 1 | 18 | 11.9 ± 5.0 (M) 0.8 ± 0.5 (F) | 11.6 ± 4.0 (M) 0.7 ± 0.4 (F) | ns ** | |||
| Author, Year | Length of Follow-Up (mo) | Study Arms | Randomized (n) | Lost to Follow-Up (n) | Included in Final Analysis (n) | Outcome Details | Outcome Measurements | p Value | |
|---|---|---|---|---|---|---|---|---|---|
| Baseline | End of Follow-Up | ||||||||
| Ayub, 2022 [30] | 2 | D3 | 35 | NR | NR | Hb (g/dL) | 10.1 ± 1.4 | 10.4 ± 1.4 | 0.503 * |
| Placebo | 35 | NR | NR | 10.2 ± 1.6 | 10.2 ± 1.6 | ||||
| Gregorio, 2021 [32] | 6 | D3 | 18 | 6 | 12 | Hb (g/dL) | 11.8 ± 1.1 | 11.6 ± 0.7 | Ns * |
| Placebo | 14 | 3 | 11 | 12.0 ± 1.3 | 12.1 ± 1.4 | ||||
| Mehortotra 1, 2013 [20] | 6 | D3 | 51 | NR | EPO dose (mcg/week) | 40 | 25 | 0.028 ** | |
| Standard care | 28 | 19 | 50 | NR | ns ** | ||||
| D3 | 51 | NR | Hb (g/dL) | 11.8 | 11.2 | 0.17 ** | |||
| Standard care | 28 | 19 | 11.5 | NR | ns ** | ||||
| Miskulin, 2016 [28] | 6 | D2 | 137 | 15 | 122 | EPO dose (units/week) | 5800 [2600, 12,200] | 7000 [2500, 16,000] | 0.78 * |
| Placebo | 139 | 9 | 130 | 5400 [2400, 11,500] | 6050 [2000, 11,800] | ||||
| Naini, 2015 [36] | 4 | VD | 32 | 0 | 22 | EPO dose (units/week) | NR 3 | NR | <0.001 ** |
| Placebo | 32 | 0 | 22 | NR | NR | ns ** | |||
| VD-male | 16 | 0 | 16 | Hb (mg/dL) | 9.8 ±1.6 | 10.6 ±1.1 | Ns * | ||
| VD-female | 16 | 0 | 16 | 10.1 ± 1.7 | 11.2 ± 1.2 | ||||
| Placebo-male | 16 | 0 | 16 | 9.2 ±1.4 | 10.1 ±0.8 | ||||
| Placebo-female | 16 | 0 | 16 | 9.2 ± 1.5 | 10.2 ± 0.9 | ||||
| Shirazian, 2013 [39] | 3 | D3 | 25 | 0 | 25 | Change in pruritus survey score | - | −38.9% | 0.34 * |
| Placebo | 25 | 0 | 25 | - | −47.5% | ||||
| Wasse, 2014 [24] | 0.75 2 | D3 | 25 | 5 | 20 | % Successful AVF/AVG use at 6 mo | - | 45% | 0.8 * |
| Placebo | 27 | 3 | 24 | - | 54% | ||||
| D3 | 25 | 5 | 20 | % AVF maturation | - | 41% | 0.7 * | ||
| Placebo | 27 | 3 | 24 | - | 50% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilkey, N.G.; Novosel, O.; Roy, A.; Wilson, T.E.; Sharma, J.; Khan, S.; Kapuria, S.; Adams, M.A.; Holden, R.M. Does Native Vitamin D Supplementation Have Pleiotropic Effects in Patients with End-Stage Kidney Disease? A Systematic Review of Randomized Trials. Nutrients 2023, 15, 3072. https://doi.org/10.3390/nu15133072
Pilkey NG, Novosel O, Roy A, Wilson TE, Sharma J, Khan S, Kapuria S, Adams MA, Holden RM. Does Native Vitamin D Supplementation Have Pleiotropic Effects in Patients with End-Stage Kidney Disease? A Systematic Review of Randomized Trials. Nutrients. 2023; 15(13):3072. https://doi.org/10.3390/nu15133072
Chicago/Turabian StylePilkey, Nathan G., Olivia Novosel, Angélique Roy, Tristin E. Wilson, Jaya Sharma, Sono Khan, Sanjana Kapuria, Michael A. Adams, and Rachel M. Holden. 2023. "Does Native Vitamin D Supplementation Have Pleiotropic Effects in Patients with End-Stage Kidney Disease? A Systematic Review of Randomized Trials" Nutrients 15, no. 13: 3072. https://doi.org/10.3390/nu15133072