
Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies

1
Research Center for Nutrition and Food Safety, Institute of Military Preventive Medicine, Third Military Medical University (Army Medical University), Chongqing 400038, China
2
Chongqing Medical Nutrition Research Center, Chongqing 400038, China
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Nutrients 2023, 15(10), 2402; https://doi.org/10.3390/nu15102402
Submission received: 9 April 2023
/
Revised: 12 May 2023
/
Accepted: 16 May 2023
/
Published: 21 May 2023
(This article belongs to the Section Phytochemicals and Human Health)
Abstract
:Rationale: Epidemiological studies that focus on the relationship between dietary isoflavone intake and the risk of breast cancer still lead to inconsistent conclusions. Herein, we conducted a meta-analysis of the latest studies to explore this issue. Method: We performed a systematic search using Web of Science, PubMed, and Embase from inception to August 2021. The robust error meta-regression (REMR) model and generalized least squares trend (GLST) model were used to establish dose–response relationships between isoflavones and breast cancer risk. Results: Seven cohort studies and 17 case-control studies were included in the meta-analysis, and the summary OR for breast cancer was 0.71 (95% CI 0.72–0.81) when comparing the highest to the lowest isoflavone intake. A subgroup analysis further showed that neither menopausal status nor ER status has a significant influence on the association between isoflavone intake and breast cancer risk, while the isoflavone intake doses and study design does. When the isoflavones exposure was less than 10 mg/day, no effects on breast cancer risk were detected. The inverse association was significant in the case-control studies but not in the cohort studies. In the dose–response meta-analysis of the cohort studies, we observed an inverse association between isoflavone intake and breast cancer: a 10 mg/day increase in isoflavone intake was related to reductions of 6.8% (OR = 0.932, 95% CI 0.90–0.96) and 3.2% (OR = 0.968, 95% CI 0.94–0.99) in breast cancer risk when using REMR and GLST, respectively. In the dose–response meta-analysis of the case-control studies, the inverse association for every 10 mg/day isoflavone intake was associated with breast cancer risk reductions by 11.7%. Conclusion: present evidence demonstrated that taking in dietary isoflavone is helpful in reducing the breast cancer risk.
1. Introduction
Breast cancer is the most commonly diagnosed cancer among women worldwide, with an estimated 2.3 million new cases in 2020, and the leading cause of cancer death, with 685,000 deaths in 2020 [1]. The number of new cases is expected to reach 4.4 million in 2070 [2], with patterns and trends varying in different countries. The incidence is generally higher in Western countries than in Asia, but it has quickly increased among Asian women, which has been attributed to the westernization of lifestyle [3], suggesting that in addition to genetic factors, lifestyle factors may contribute to the etiology of breast cancer. The role of estrogen in breast cancers has become increasingly evident. Soy, a traditional and popular food in Asian countries, contains isoflavone, which resembles 17β-estradiol and, thus, has the ability to bind to and activate estrogen receptors (ERs) in breast cancer [4]. It has been suggested that isoflavones play a role in reducing breast cancer risk by reducing the production of estrogen and reactive oxygen species and inhibiting cell proliferation, as per mechanistic studies [4]. However, conclusions on the relationship between isoflavone intake and breast cancer risk in epidemiological studies are still inconsistent [5,6,7,8].
Several meta-analyses have been performed in the past trying to draw a conclusion on the relationship between isoflavone intake and breast cancer risk [9,10,11]. However, their conclusions remain inconsistent due to the differences in their study inclusion criteria, among others. In addition, a considerable number of observational studies have been carried out since our team’s previous systematic review on this topic [12], which added new evidence on the relationship between isoflavone intake and breast cancer risk. Therefore, an updated meta-analysis is required to re-evaluate the relationship between isoflavone intake and breast cancer risk, including subgroup analyses and dose–response analyses.
In this systematic review, a comprehensive meta-analysis was performed to evaluate the probability association between dietary intake levels of isoflavones and breast cancer risk. Subgroup analyses were also carried out to assess the varieties of breast cancer risk among baseline characteristics such as menopausal status and ethnic groups. In addition, to provide a more clarified picture of the relationship between isoflavone intake levels and breast cancer, we conducted a dose–response meta-analysis to interpret our results.
2. Materials and Methods
2.1. Protocol and Guidance
This study is a systematic review and meta-analysis of isoflavone consumption and the risk of breast cancer in female humans. The recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) were followed. The protocol of this study was registered in the International Prospective Registry for Systematic Reviews (PROSPERO) in advance (CRD42021289115).
2.2. Inclusion Criteria
This review included observational studies (cohort or case control) undertaken in the adult female population that reported on the association between isoflavone consumption and the risk of breast cancer from January 2000 to August 2021, with a detailed description of the isoflavone intake dose, as well as the estimated effects in the form of a hazard ratio (HR) or odds ratio (OR) with a 95% confidence interval (95% CI). If data from the same cohort were used for different publications, we only included the latest published study to avoid replicated data. Due to the low absolute risk of breast cancer, all measures of relationships, including RR, IRR, and HR, are more likely equal to the estimates of the OR [13], which was used as the study’s outcome.
2.3. Exclusion Criteria
Studies conducted in vitro or with animals, reviews, notes, reports, short surveys, conference letters, and case reports were excluded. Studies that used urine or serum markers instead of pathological methods for the diagnosis of breast cancer were excluded. Studies without normalization or without analysis of 95% CIs were excluded as well.
2.4. Search Strategy
The PICO strategy (Population, Intervention/Exposure, Comparison, Outcomes) was used to determine an article’s eligibility (Table S1). A systematic search was carried out using the following public databases: Web of Science, PubMed, and Embase, from the database’s inception to 1 August 2021. Neither data nor language restrictions were applied. Two groups of keywords were utilized to search for articles through the Medical Subject Headings (MeSH). One group used to search for isoflavone were “isoflavones”, “genistein”, “daidzein”, “glycitein”, “biochanin”, “formononetin”, “soy”, “red clover”, “tofu”, and “soya”. The other group for breast cancer was “breast cancer”, “breast carcinoma”, “breast neoplasm”, and “breast tumor”. Details concerning the search strategies for each database are presented in Table S2.
2.5. Study Selection and Data Collection
After automatically removing the duplicates using Endnote X9, all titles and abstracts considered for potential inclusion were screened by two independent authors (J. N. Y. and H. S). Multiple publications by the same author, cohort, or institution were rigorously reviewed, and the studies with the most cases were included to avoid incorporating duplicates.
Two authors (J. N. Y. and H. S.) applied a standardized method to extract data independently. The following parameters were extracted: authors’ information, publication year, study design, country, study period, number of cases and subjects, age, diagnosis of breast cancer, isoflavone exposure range, exposure assessment, risk estimates with corresponding 95% CIs, and adjustment for potentially confounding factors.
Any disagreements during the study selection or data collection were resolved by discussion until a consensus was reached or by consulting another author (Y. Q.).
2.6. Quality Assessment of Evidence
Using the Newcastle–Ottawa Scale (NOS), two authors (J. N. Y. and H. S.) independently assessed the quality of each study [14]. Any disagreements were resolved by discussion until a consensus was reached or by consulting another author (Y. Q.).
2.7. Statistical Analysis
The statistical analyses were conducted using STATA version 16 (Stata Corp). p-Values were considered significant at the level of p < 0.05.
2.7.1. Meta-Analysis
The ORs and their 95% CIs were used to report the results. We performed a random-effects meta-analysis to estimate the pooled effect size for the highest in comparison with the lowest intakes of isoflavones. To assess the heterogeneity among studies, we calculated the Cochran Q and the I2 statistics [15]. For the Q statistic, p < 0.1 was considered significant. For the I2 statistic, a low level of heterogeneity was considered when I2 was less than 40%, a medium level for 40% < I2 < 60%, and a high level for I2 > 60%. A multivariate meta-regression analysis was conducted to identify the source of the heterogeneity.
2.7.2. Subgroup Analysis
For additional insight, subgroup analyses were conducted based on the study design (cohort study or case-control study), population (Asian or non-Asian), publication year (2001–2010 or 2010–2021), study quality (NOS score ≥ 7 or NOS score < 7), menopausal status (premenopausal or postmenopausal), isoflavone intake doses (≥10 mg or <10 mg), and estrogen receptor (ER) status (positive or negative).
2.7.3. Dose–Response Analysis
We selected the mean values of the isoflavone intake doses in each category to represent the average intake level. For studies that reported a range of isoflavone intakes, the midpoint of the upper and lower boundaries was regarded as the intake dose of each category. When the highest categories were open-ended, the dose was considered 1.2-fold that of the highest boundary [16].
The dose–response meta-analysis was performed in the cohort studies and case-control studies. In this analysis, we utilized a one-stage, robust error meta-regression (REMR) model [17] and a two-stage, generalized least squares trend (GLST) model [18] to estimate the potential curvilinear association between isoflavones and the risk of breast cancer. The GLST model’s method requires that the studies report ≥3 exposure categories, which was not specified in the REMR model. In both of the two methods, we modeled the dose using a restricted cubic spline model with 3 knots at 5%, 50%, and 95% of the distribution. In order to test the nonlinearity, the Wald test was used, with the null hypothesis that the coefficient of the second spline was zero. The GLST model and REMR model were used to investigate the linear dose–response association between a 10 mg/day increment in intake of isoflavones and the risk of breast cancer. Statistical analyses were performed using STATA version 16.0 (Stata Corp). p-Values were considered significant at the level of p < 0.05.
2.7.4. Risk of Publication Bias and Sensitivity Analysis
Sensitivity analyses were performed to identify whether the overall estimates were dependent on the effect size from a single study by excluding each study in turn [19]. Publication bias was evaluated using Begg’s funnel plot and Egger’s regression test [20]. The trim-and-fill method was performed for further analysis, if the Egger’s regression test was significant [21].
3. Results
3.1. Characteristics of the Studies
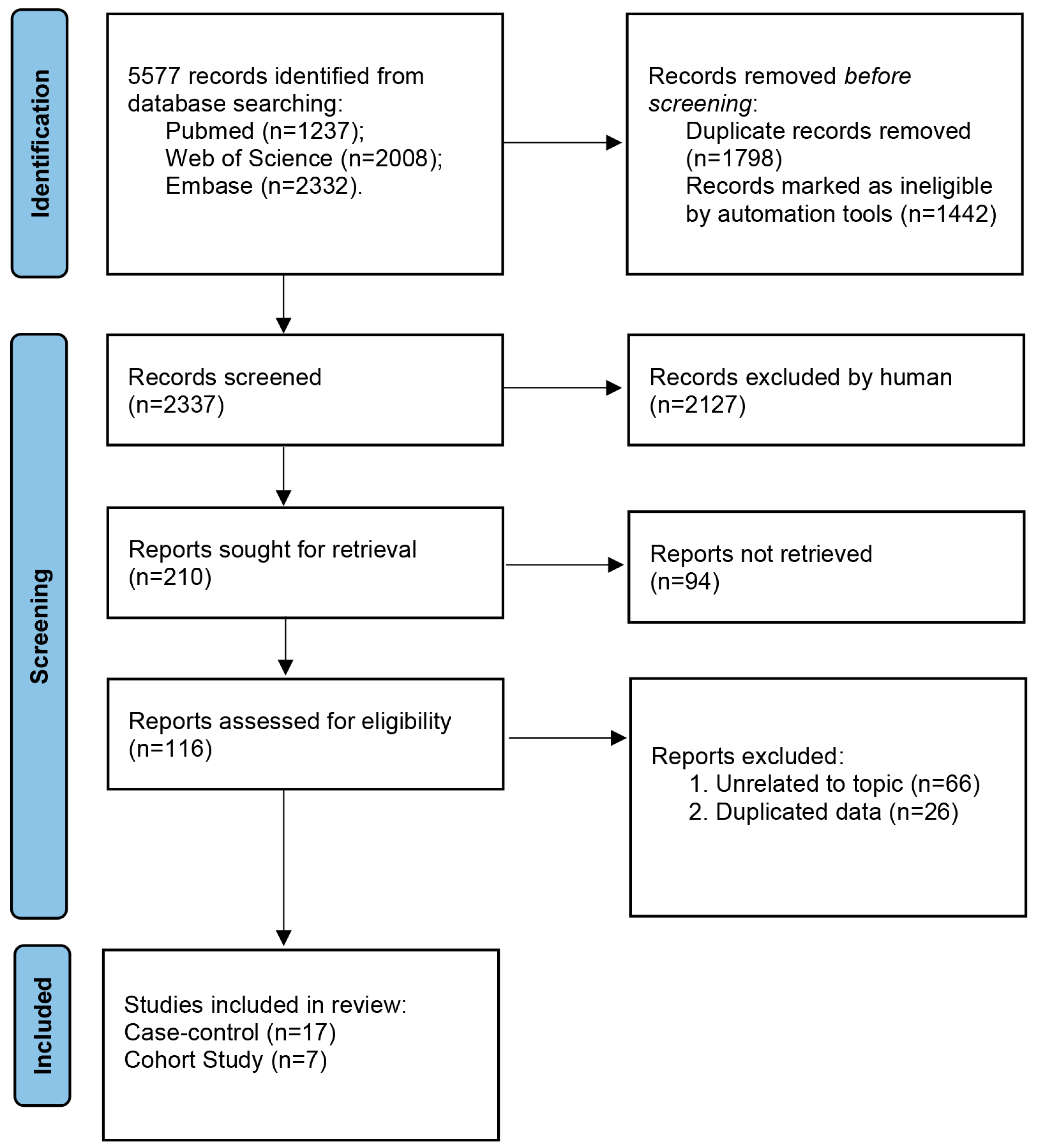
As shown in Figure 1, 5577 studies were identified based on our search strategy. After removing duplicate records and records marked as ineligible by automation tools, which screened out studies with “cell”, “mouse”, “rat”, etc., in the title or abstract, 2337 studies remained. After assessing the titles and abstracts of these studies, 2127 records were subsequently excluded based on our inclusion and exclusion criteria. After assessing the full text of the remaining 210 studies, 94 records were excluded because of the unavailability of the isoflavone intake dose data. After a thorough final review of the 116 remaining studies, 92 studies were excluded because they were unrelated to our topic (n = 66) and or because of data duplication (n = 26). There were 24 studies [5,6,7,8,9,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] that met our inclusion criteria and were included in this meta-analysis.
The overall quality of the included studies was relatively high. The average NOS score of the 24 included studies was 7.6, ranging from 6 to 9. Among these studies, eight achieved a score of 7, nine achieved a score of 8, and four achieved a score of 9. Detailed outcomes of the quality assessment for each study are presented in Figures S1 and S2.
A summary of the characteristics of the included studies is provided in Table 1 and described below. Of the 24 included studies, 17 were case-control studies [5,6,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36] and 7 were cohort studies [7,8,9,37,38,39,40]. The selected studies were published between 2001 and 2021 and were carried out in Asia [6,8,9,26,27,28,29,30,31,33,34,35,36,37,38,40], America [5,22,23,27,32,39], and Europe [7,24,25]. The study-specific, maximally adjusted ORs or HRs were extracted and pooled for the meta-analysis to evaluate the association of isoflavone and the risk of breast cancer in a total of 902,438 females. The verification of breast cancer in these studies was based on either a cancer registry record or a histological diagnosis. The exposure assessment of all included studies was based on a food frequency questionnaire (FFQ) via either face-to-face interviews or self-administrative questionnaires.
3.2. Meta-Analysis of Isoflavone Consumption and Risk of Breast Cancer
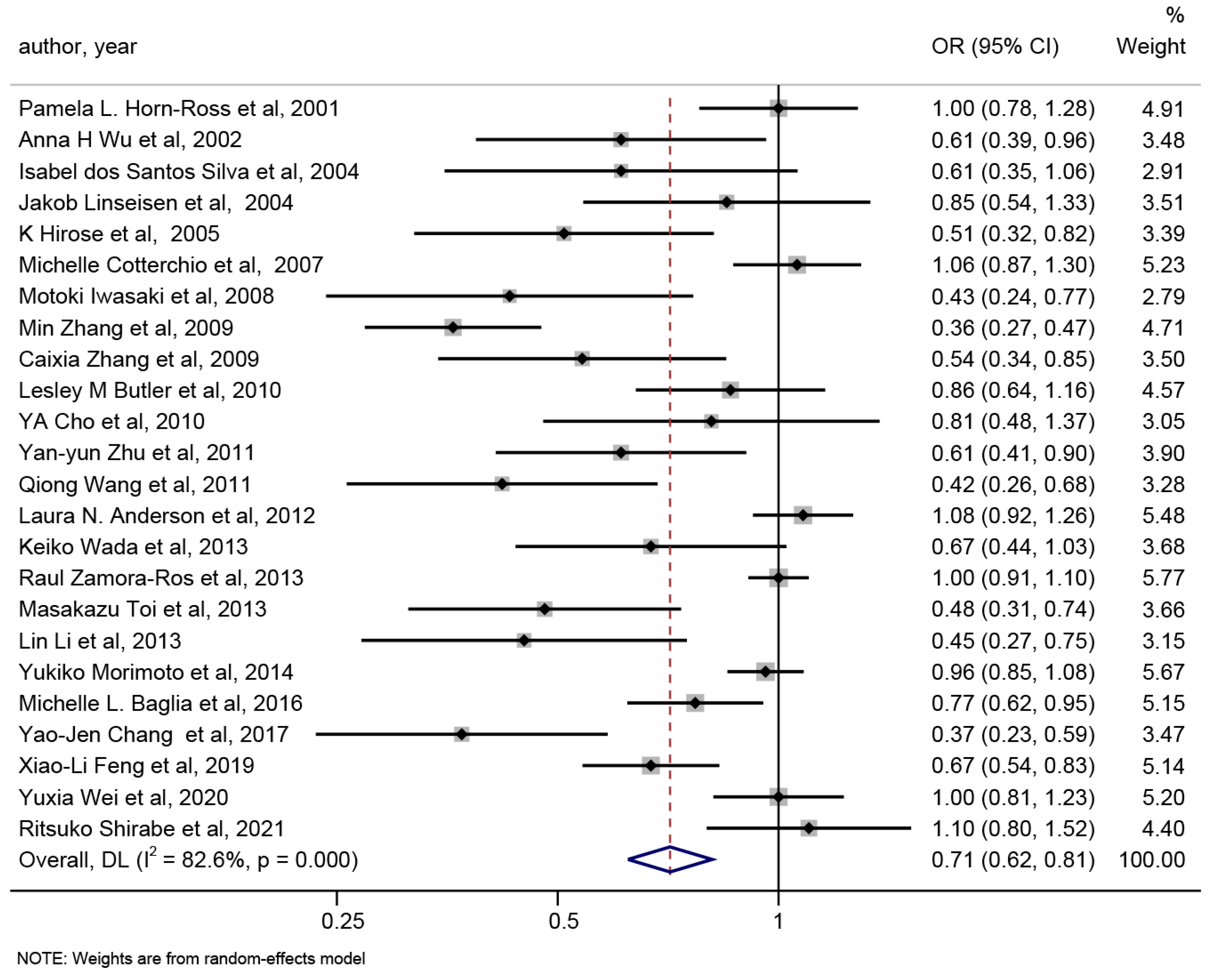
From each study and all studies combined, the estimated ORs for the highest versus lowest levels of isoflavone dietary intake are shown in Figure 2. A protective effect of isoflavone dietary intake on breast cancer risk (OR 0.71, 95% CI 0.62–0.81) were performed, but unneglectable heterogeneity existed (p < 0.001 for heterogeneity, I2 = 82.6%).
Therefore, a meta-regression was conducted to determine the possible sources of heterogeneity. In the meta-regression analysis, we explored the study design (cohort vs. case-control study), population (Asian vs. non-Asian), publication year, study quality, menopausal status (premenopausal vs. postmenopausal), and isoflavone intake dose and case number. As a result of the meta-regression, study design (p = 0.017), population (p = 0.009), and isoflavone intake dose (p = 0.038) were identified as potential sources of heterogeneity.
3.3. Subgroup Analysis of Isoflavone Consumption and the Risk of Breast Cancer
We performed a subgroup analysis according to the study design (cohort vs. case-control study), population (Asian vs. non-Asian), publication year (2001–2010 vs. 2010–2021), study quality (NOS score ≤ 7 vs. NOS score > 7), menopausal status (premenopausal vs. postmenopausal), isoflavone intake doses ≥ 10 mg vs. <10 mg), and ERs status (positive vs. negative). The pooled ORs are presented in Table 2, and detailed forest plots are provided in Figure S3. As the results show, the subgroup analysis based on isoflavone intake dose (p for interaction <0.001), population (p for interaction <0.001), and study design (p for interaction <0.001) could explain the between-study heterogeneity.
A statistically significant protective effect of isoflavone intake on breast cancer was observed in the case-control studies (OR = 0.62, 95% CI 0.50–0.76), while no such effect was observed in the cohort studies (OR = 0.94, 95% CI 0.86–1.02). In addition, the pooled OR showed an inverse relationship between isoflavone intake and breast cancer in Asian women (OR = 0.62, 95% CI 0.52–0.74), while the relationship did not exist in n7uon-Asian women (OR = 0.97, 95% CI 0.88–1.06). When the highest isoflavone intake was lower than 10 mg/d, the negative relationship between isoflavone intake and breast cancer disappeared (OR = 1.01, 95% CI 0.94–1.08), whereas OR = 0.63, 95% CI 0.53–0.75, when the highest isoflavone intake was above 10 mg/d. However, a statistically significant difference in the protective effect of isoflavone intake on breast cancer was observed regardless of whether the women were pre- or postmenopausal and regardless of whether they were ER positive or negative.
3.4. Dose–Response Meta-Analysis of Isoflavone Consumption and the Risk of Breast Cancer
Next, we assessed the dose–response relationship between isoflavone intake and breast cancer risk using both REMR and GLST methods for the case-control studies and cohort studies, respectively.
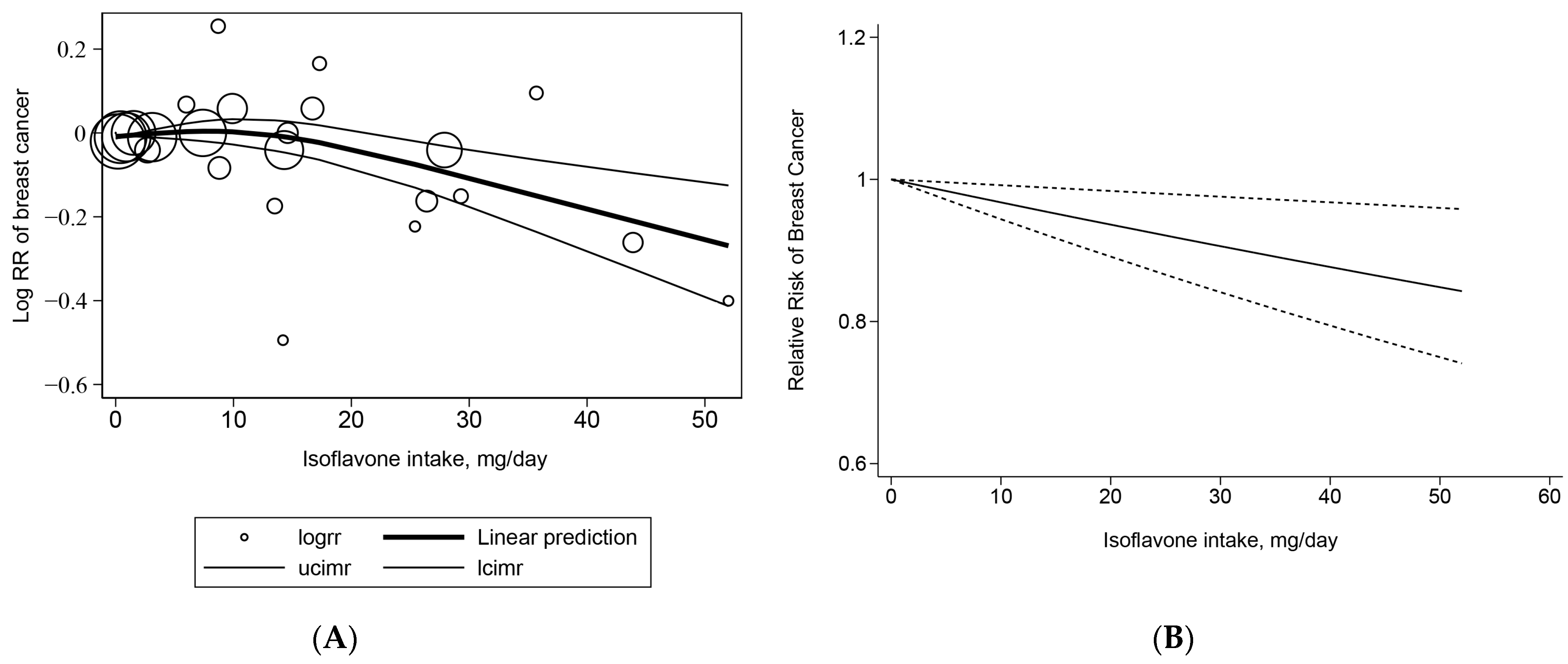
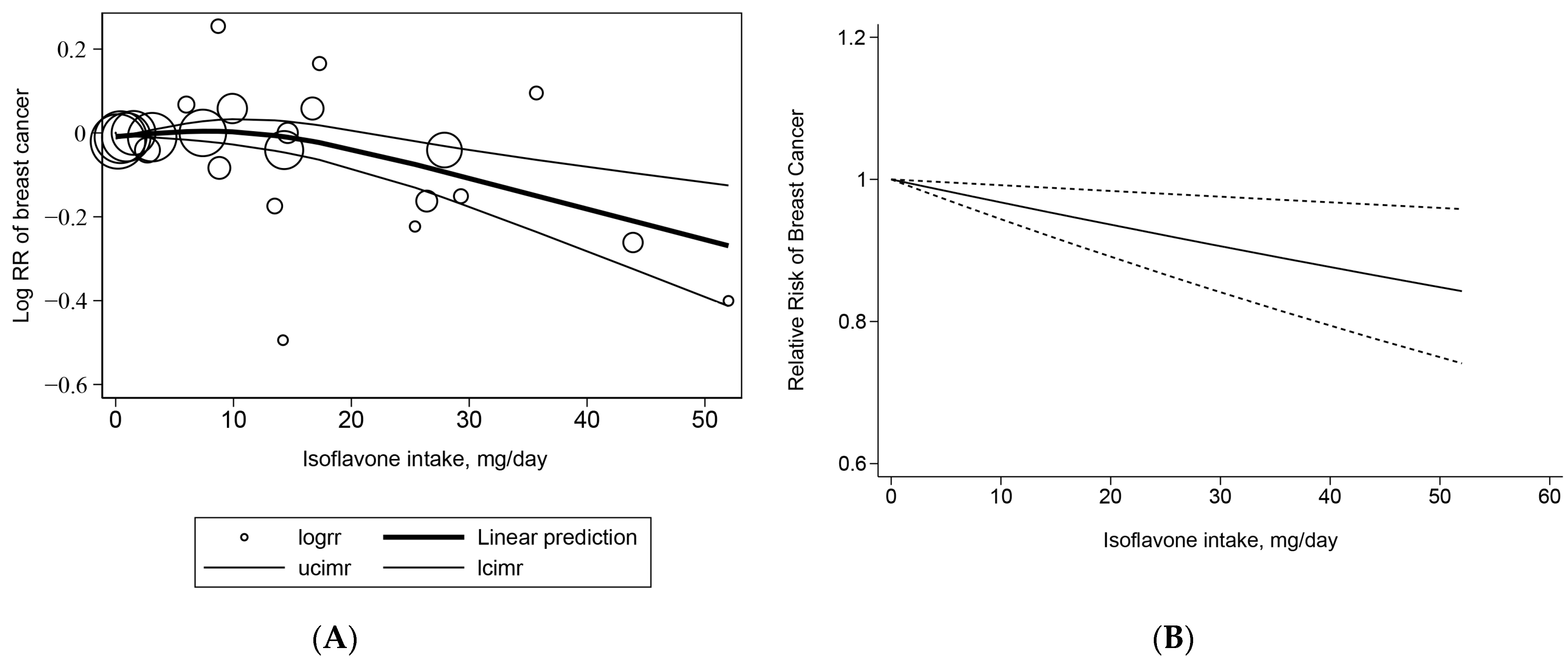
The cohort studies included seven studies both in the GLST model and the REMR model. When using the REMR method, the p-value for the nonlinear association was 0.0081. Therefore, the curvilinear dose–response REMR was used. We found that a 10 mg/day increase in isoflavone intake was associated with a 6.8% lower risk of breast cancer (OR = 0.932, 95% CI 0.90–0.96, p = 0.002) (Figure 3A). When using the GLST method, the p-value for the nonlinear association was 0.1141. Thus, the linear dose–response GLST was used. The pooled OR for breast cancer risk at a 10 mg/day increment in isoflavone dietary intake was 0.968 (95% CI 0.94–0.99, p = 0.009), which means there was a 3.2% decrease in the risk of breast cancer for an increase of 10 mg isoflavone intake per day (Figure 3B). It can be observed that the breast cancer risk is significantly reduced with an isoflavone intake of approximately 15 mg/day when using the REMR method.
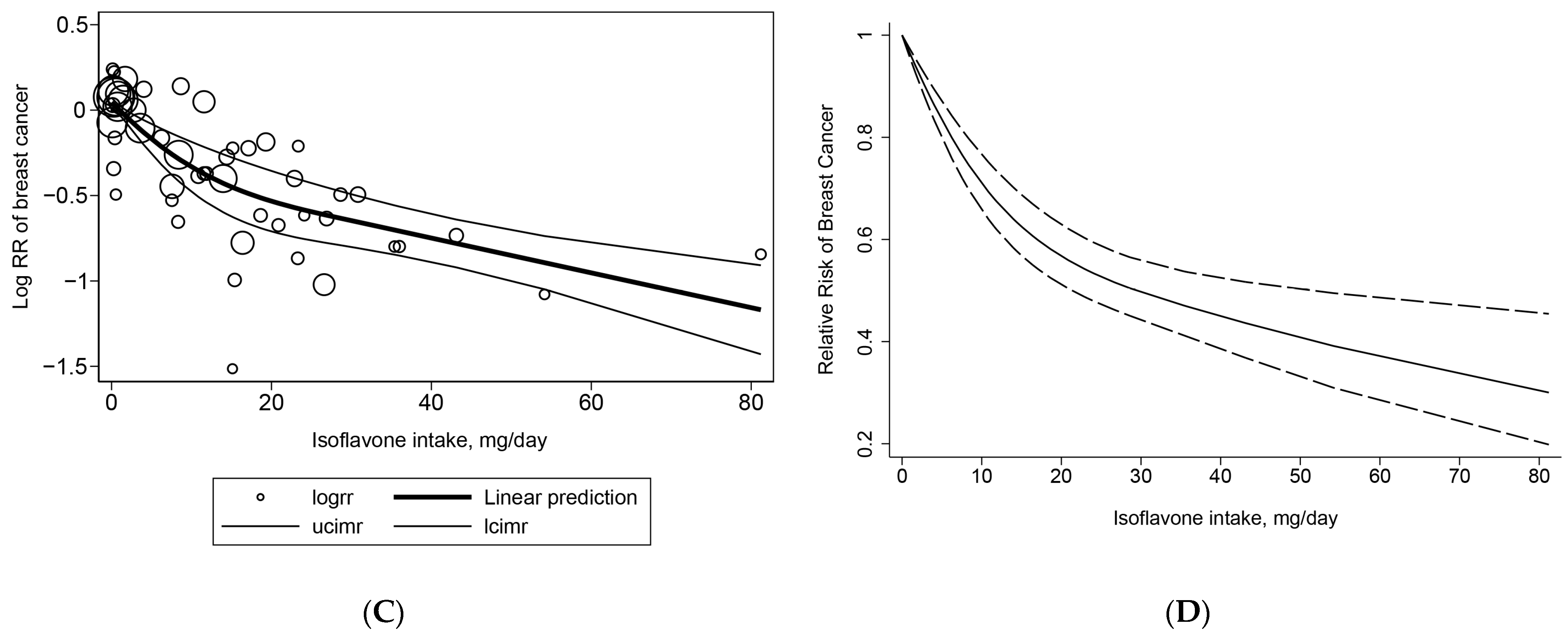
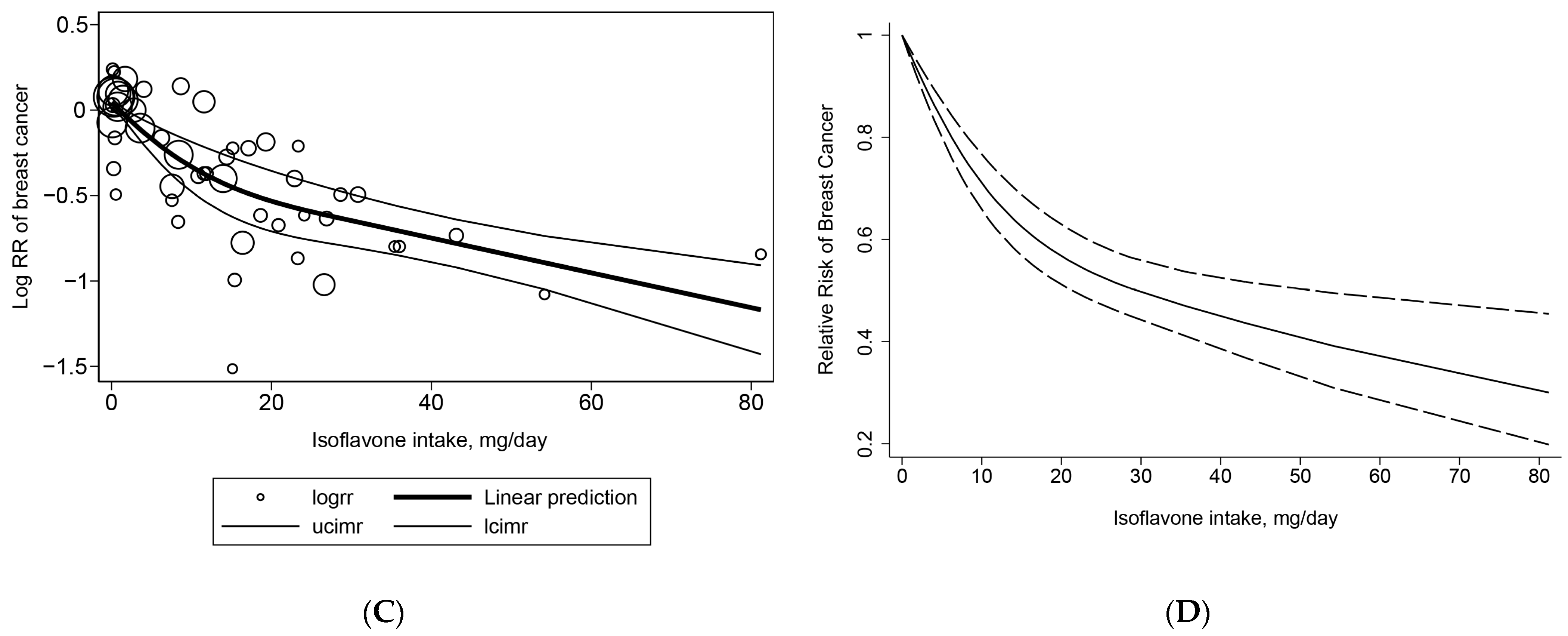
For the case-control studies, we finally involved 12 and 17 studies in the GLST model and REMR model, respectively. When using the REMR method (Figure 3C), we found a curvilinear association between isoflavone intake and breast cancer (p nonlinearity = 0.0129). With each 10 mg/day increment in isoflavone intake, the pooled risk of breast cancer was reduced by 11.7% (OR = 0.88, 95% CI 0.85–0.91, p < 0.001). When using the GLST method, we found a curvilinear association between isoflavone intake and breast cancer (p nonlinearity = 0.0002), an increase of 10 mg/day isoflavones intake was associated with a 19.3% lower risk of breast cancer (OR = 0.81, 95% CI 0.78–0.84, p < 0.001) (Figure 3D). The decrease in the breast cancer risk was slightly decelerated when the isoflavone intake was >20 mg/day, but no significant slowdown was observed using both methods.
3.5. Risk of Publication Bias
The publication biases were evaluated using Begg’s test and Egger’s test. The shape of the funnel plots showed asymmetry (Figure S4A, p = 0.001), and the Egger’s test found virtual publication bias (Figure S4B, p < 0.001). However, the trim-and-fill method failed to identify any potentially missing studies (Figure S4C), indicating the publication bias did not affect the results.
3.6. Sensitivity Analysis
By excluding individual studies at a clip, the contribution of individual studies on the overall results was assessed by testing the presence of noticeable changes in the overall result (Figure S5). In general, a few studies contributed intensive but insignificant weight to the overall results.
4. Discussion
In this observational-based meta-analysis, our results showed that dietary isoflavone intake has a negative correlation with breast cancer risk, suggesting a potential protective effect of isoflavone on breast cancer. However, we also noticed the non-negligible heterogeneity in the overall results. Using a meta-regression analysis, we found that the study design, isoflavone intake dose, and population might be the major sources of the heterogeneity. Regarding these concerned factors, we further conducted a subgroup analysis.
When we stratified by menopause status, estrogen receptor, publication year, and NOS score, the negative correlation was still significant, indicating that these factors might not be the key sources of the heterogeneity. Interestingly, the association was almost the same regarding menopause status (OR 0.76, 95% CI 0.63–0.92 in premenopausal vs. 0.75, 95% CI 0.62–0.90 in postmenopausal) and estrogen receptor (0.77, 95% CI 0.62–0.95 in ER+ vs. 0.77, 95% CI 0.52–1.15 in ER-), suggesting that menopause status and estrogen receptor had little effect on the correlation between isoflavone and breast cancer risk. Previous laboratory studies show that the sexual hormone was an important risk factor for breast cancer, and estrogen therapy is effective and validated [41]. Mechanistically, isoflavone is an estrogen-like compound that can bind and activate estrogen receptors (ERs) in breast cancer and, thus, was indicated to be effective in curing breast cancer [42]. However, our meta-analysis result showed that the up-to-date epidemiological evidence could not support the estrogen-like effect on breast cancer. One interesting hypothesis of the preventive effects of isoflavone on breast cancer is its inhibition of cancer initiation, which occurs at an early age when the cells are in good shape [43,44]. This means that the starting exposure time of isoflavone is important for the prevention of breast cancer. However, a limited number of epidemical studies have been published that support the hypothesis [23,32,45]. A case-control study in Asian American females indicated that the high consumption of isoflavone during adolescence was related to a reduced risk of breast cancer, even though the consumption was low during adult life [23]. Thanos et al. proposed that higher exposure to isoflavones during adolescence exhibited a decreased risk of breast cancer among non-Asian women [45], and a subsequent study by this team showed that the decreased risk may be relative to the ER and PR status [32]. Further, a recent large prospective cohort study that included more than 11,000 women aged above 50 reported that isoflavone supplements had a significant positive association with ER-negative breast cancer, although there was a significant inverse association with ER-positive breast cancer [46], which is inconsistent with our meta-analysis results that included all adult female data, further suggesting that the intake of isoflavone at an early age might greatly benefit breast cancer.
The subgroup analysis of the publication year and NOS score showed that the negative correlation was stronger in studies with an NOS score above seven than below seven, and it was stronger in studies published before 2010 than after 2010. The results suggest that some characteristics of the study may influence the risk estimate, although the combined ORs were still significant. One explanation could be the uncertainties in the isoflavone intake assessment. Soy, an isoflavone-rich food, is more often used as an ingredient in transformed food nowadays than in earlier times [47,48]. This ingredient significantly increases the exposure to isoflavones even in “non-soy eaters”, which could probably underestimate the isoflavone intake dose, thus increasing the heterogeneity in recent studies.
The subgroup analysis of the study design showed that the negative correlation between dietary isoflavone intake and breast cancer risk was only significant in case-control studies but not in cohort studies. Zhao et al. [10] also drew a similar conclusion in their recent meta-analysis. They performed a meta-analysis on cohort studies of dietary isoflavones intake and breast cancer risk, which showed no significant association between isoflavones intake and the risk of breast cancer regardless of high isoflavone intake (RR 0.99, 95% CI 0.91–1.09) or low intake (RR 0.99, 95% CI 0.92–1.05), although the included criteria were slightly different with our present study. In addition, other factors, including isoflavone intake dose and population, also contributed to the heterogeneity of our meta-analysis. Different populations have different eating habits. Specifically, Asians consume much more isoflavone-rich soy foods in their daily life, such as tofu in China and miso-soup in Japan. The studies on Asian populations and relatively high isoflavone intake doses are mostly consistent with each other. The subgroup analysis of the isoflavone intake dose showed that only the relatively high isoflavone intake (>10 mg/day) was negatively correlated with breast cancer, indicating that the protective effects of isoflavone on breast cancer might only occur when people take in enough isoflavone each day. Furthermore, the negative correlation between isoflavone intake and breast cancer risk was only observed in Asian adult women but not in non-Asian adult women. This phenomenon could partly be attributed to the different isoflavone intake doses due to the different eating habits, since Asian populations usually consume more isoflavone-rich food compared with non-Asian populations. As the previous studies report, the isoflavone intake of Asian populations ranges from 15 to 60 mg/day [49,50], which is merely <3 mg/day in non-Asian populations [51,52]. However, whether gene polymorphisms played a role remains to be explored. A similar trend in isoflavone intake has been demonstrated in the studies involved in the previous meta-analysis [12].
Considering the vital role of the isoflavone intake dose in breast cancer risk, we further performed a dose–response meta-analysis of isoflavone consumption and the risk of breast cancer. As the study design is another important factor that contributes to the heterogeneity, we performed a dose–response meta-analysis within the case-control studies and cohort studies, respectively. The GLST approach used in this article is a commonly used two-stage dose–response meta-analyses method. Using this method, we found a 3.2% decrease in the risk of breast cancer for an increase of 10 mg isoflavone intake per day in the cohort studies, which is consistent with Wei et al.’s results using the GLST method (HR 97% for every 10 mg isoflavone intake, 95% CI 0.95–0.99) [9]. Using the same method, a 19.3% decrease in the risk of breast cancer for an increase of 10 mg isoflavone intake per day was found in the case-control studies, which is much higher than the results in the cohort studies. However, the dose–response analysis of isoflavone intake and breast cancer within the case-control studies was not found in recent studies. Wang et al. reported a 10% (95% CI 7%–13%) decrease in the risk of breast cancer for an increase of 10 g tofu (an isoflavone-rich food) intake per day, within five case-control studies, using the same method. If converting tofu intake to isoflavone intake based on the median (237 µg isoflavone in 1 g tofu) in the previous study [53], the dose–response result of Wang et al. should be a 42.2% decrease in the risk of breast cancer for an increase of 10 mg isoflavone intake per day, which is also a substantially high number. The second method used in our study was RMER, a one-stage method for dose–response meta-analysis, which was recommended in a recent study [17]. Using this method, the decreased rate of breast cancer for every 10 mg of isoflavones was 6.8% and 11.7%, respectively, within the cohort studies and case-control studies. However, no comparable data were reported.
Although the association between isoflavone and breast cancer is dose-dependently inverse, the potentially detrimental effects of isoflavone at very high doses cannot be neglected. The leading concern is the potential detrimental effects on postmenopausal women, since high concentrations of estrogen could lead to endometrial carcinoma in aged women [54]. One RCT study reported that no significant adverse effects were observed in 224 postmenopausal women the United States who received supplementation with soy isoflavone at 120 mg/day for 3 years [55]. Another RCT study reported that six women developed endometrial hyperplasia but no endometrial cancer in 319 Italian postmenopausal women supplemented with 150 mg/day of soy isoflavones for 5 years [56]. More recently, no endometrial thickness hyperplasia or histopathological changes were observed in 399 postmenopausal women in Taiwan who were supplemented with 300 mg/day of soy isoflavones for 2 years [57] and 350 postmenopausal women in the United States supplemented with 154 mg/day of soy isoflavones for three years [58]. However, other potential hazards to the reproduction of a high dose of isoflavone should be taken into consideration. Some recent observational studies report potential detrimental effects on reproduction of isoflavone with high doses in Western women [59,60], which should also be taken into consideration. However, up-to-date evidence supports that a dose below 50 mg/day may not induce reproductive impairment.
There are several limitations in this study that should be noticed. First, in order to have a full view of the correlation between dietary isoflavone consumption and breast cancer risk, we included as much clinical evidence as possible according to our criteria, leading to the inevitable heterogeneity among study designs. In addition, quite a few of the studies included were case-control studies (17 of 24 studies). Therefore, recall and selection biases should be noticed. However, we tried to limit these biases by only keeping the cohort study data when a parallel case-control study was taken using the same cohort of this cohort study. Second, the isoflavone intake might be underestimated in Western countries, since soy is used as an ingredient in many transformed dishes, which might lead to a bias in the subgroup analysis stratified by intake dose. Third, in each study included in the present meta-analysis, different methods of assessing the intake dose of isoflavone were employed. For example, self-administered questionnaires, mail survey questionnaires, and multitype food-frequency questionnaires were used in these studies, which could potentially lead to bias. Fourth, the adjusted factors were different in each included study and, thus, might bias the association between dietary isoflavone intake and breast cancer risk. Fifth, genistein, daidzein, and glycitein are the major food-derived isoflavones, with different distributions in different food legumes and soy products [61]. In addition, there are certain differences in the metabolites and biological effects among them. For example, the bioavailability is higher in genistein [62], but the equol, the metabolite of daidzein, exerts significantly greater antioxidant activity and estrogenic activity on binding to the ER receptor compared with daidzein, thus leading to different biological effects [63]. However, most of the observational studies did not distinguish them in the FFQ survey, and only the total isoflavones intakes were calculated, which might lead to evitable heterogeneity among countries with different food preferences. As a result, the effect of various isoflavones on breast cancer risk requires further investigations.
In conclusion, evidence from observational studies suggest a dose–response inverse association between dietary isoflavone intake and breast cancer risk. However, heterogeneity and biases in the present studies require further well-designed prospective cohort and RCT studies to confirm our findings.
5. Conclusions
This updated meta-analysis showed that dietary isoflavone intake has a protective effect on breast cancer risk, with a significant dose–response correlation, regardless of premenopausal or postmenopausal conditions. Future prospective cohort studies or RCTs are also needed to determine the causality of this relationship.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu15102402/s1, Figure S1: Risk of bias graph: (A) risk bias in cohort studies; (B) risk bias in case-control studies. Green circles, low risk of bias; yellow circles, unclear risk of bias; red circles, high risk of bias. Figure S2: Risk of bias summary: (A) risk bias in cohort studies; (B) risk bias in case-control studies. Figure S3: Subgroup analyses of isoflavone intake and the risk of breast cancer: (A) subgroup analyses by study design; (B) subgroup analyses by population; (C) subgroup analyses by publication year; (D) subgroup analyses by study quality; (E) subgroup analyses by menopausal status; (F) subgroup analyses by isoflavone intake doses; (G) subgroup analyses by estrogen receptor status. Figure S4: Publication bias plot: (A) funnel plot of the odds ratio of 24 studies on isoflavone intake and the risk of breast cancer, Begg’s test, p = 0.001; (B) Egger’s publication bias plot, Egger’s test, p = 0.000; (C) trim-and-fill analysis plot, no imputed studies are predicted. Figure S5. Plots of sensitivity analyses by sequential removal of each study. Table S1: Description of population, intervention/exposure, comparison, and outcome (PICO). Table S2: Search strategies including the key terms and the queries for each database.
Author Contributions
Conceptualization, M.M., Y.Q. and J.Y.; methodology, H.S. and J.Y.; software, H.S.; validation, Y.Q.; formal analysis, J.Y. and H.S.; investigation, Y.Q., J.Y. and H.S.; data curation, J.Y. and H.S.; writing—original draft preparation, J.Y. and H.S.; writing—review and editing, M.M. and Y.Q.; visualization, J.Y. and H.S.; supervision, M.M. and Y.Q.; project administration, Y.Q.; funding acquisition, M.M. and Y.Q. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the CNS (China Nutrition Society) Research Fund for DRIs.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Soerjomataram, I.; Bray, F. Planning for tomorrow: Global cancer incidence and the role of prevention 2020–2070. Nat. Rev. Clin. Oncol. 2021, 18, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Winters, S.; Martin, C.; Murphy, D.; Shokar, N.K. Chapter One—Breast Cancer Epidemiology, Prevention, and Screening. In Progress in Molecular Biology and Translational Science; Lakshmanaswamy, R., Ed.; Academic Press: Cambridge, MA, USA, 2017; Volume 151, pp. 1–32. [Google Scholar]
- Kim, I.S. Current Perspectives on the Beneficial Effects of Soybean Isoflavones and Their Metabolites for Humans. Antioxidants 2021, 10, 1064. [Google Scholar] [CrossRef] [PubMed]
- Cotterchio, M.; Boucher, B.A.; Kreiger, N.; Mills, C.A.; Thompson, L.U. Dietary phytoestrogen intake--lignans and isoflavones--and breast cancer risk (Canada). Cancer Causes Control 2008, 19, 259–272. [Google Scholar] [CrossRef]
- Zhu, Y.-Y.; Zhou, L.; Jiao, S.-C.; Xu, L.-Z. Relationship Between Soy Food Intake and Breast Cancer in China. Asian Pac. J. Cancer Prev. 2011, 12, 2837–2840. [Google Scholar]
- Zamora-Ros, R.; Ferrari, P.; Gonzalez, C.A.; Tjonneland, A.; Olsen, A.; Bredsdorff, L.; Overvad, K.; Touillaud, M.; Perquier, F.; Fagherazzi, G.; et al. Dietary flavonoid and lignan intake and breast cancer risk according to menopause and hormone receptor status in the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. Breast Cancer Res. Treat. 2013, 139, 163–176. [Google Scholar] [CrossRef]
- Baglia, M.L.; Zheng, W.; Li, H.; Yang, G.; Gao, J.; Gao, Y.T.; Shu, X.O. The association of soy food consumption with the risk of subtype of breast cancers defined by hormone receptor and HER2 status. Int. J. Cancer 2016, 139, 742–748. [Google Scholar] [CrossRef]
- Wei, Y.; Lv, J.; Guo, Y.; Bian, Z.; Gao, M.; Du, H.; Yang, L.; Chen, Y.; Zhang, X.; Wang, T.; et al. Soy intake and breast cancer risk: A prospective study of 300,000 Chinese women and a dose-response meta-analysis. Eur. J. Epidemiol. 2020, 35, 567–578. [Google Scholar] [CrossRef]
- Zhao, T.T.; Jin, F.; Li, J.G.; Xu, Y.Y.; Dong, H.T.; Liu, Q.; Xing, P.; Zhu, G.L.; Xu, H.; Miao, Z.F. Dietary isoflavones or isoflavone-rich food intake and breast cancer risk: A meta-analysis of prospective cohort studies. Clin. Nutr. 2019, 38, 136–145. [Google Scholar] [CrossRef]
- Okekunle, A.P.; Gao, J.; Wu, X.; Feng, R.; Sun, C. Higher dietary soy intake appears inversely related to breast cancer risk independent of estrogen receptor breast cancer phenotypes. Heliyon 2020, 6, e04228. [Google Scholar] [CrossRef]
- Xie, Q.; Chen, M.L.; Qin, Y.; Zhang, Q.Y.; Xu, H.X.; Zhou, Y.; Mi, M.T.; Zhu, J.D. Isoflavone consumption and risk of breast cancer: A dose-response meta-analysis of observational studies. Asia Pac. J. Clin. Nutr. 2013, 22, 118–127. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Phillips, A.N. Meta-analysis: Principles and procedures. Bmj 1997, 315, 1533–1537. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Symp. Syst. Rev. Beyond Basics 2014. [Google Scholar]
- Ioannidis, J.P.; Patsopoulos, N.A.; Evangelou, E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ 2007, 335, 914–916. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Cook, N.R.; Bergstr?M, A.; Hsieh, C.C. A two-stage hierarchical regression model for meta-analysis of epidemiologic nonlinear dose-response data. Comput. Stat. Data Anal. 2009, 53, 4157–4167. [Google Scholar] [CrossRef]
- Xu, C.; Doi, S.A.R. The robust error meta-regression method for dose-response meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 138–144. [Google Scholar] [CrossRef]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose–response data. Stata J. 2006, 6, 40–57. [Google Scholar] [CrossRef]
- Cro, S.; Morris, T.P.; Kenward, M.G.; Carpenter, J.R. Reference-based sensitivity analysis via multiple imputation for longitudinal trials with protocol deviation. Stata J. 2016, 16, 443–463. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Horn-Ross, P.L.; John, E.M.; Lee, M.; Stewart, S.L.; Koo, J.; Sakoda, L.C.; Shiau, A.C.; Goldstein, J.; Davis, P.; Perez-Stable, E.J. Phytoestrogen consumption and breast cancer risk in a multiethnic population: The Bay Area Breast Cancer Study. Am. J. Epidemiol. 2001, 154, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.H.; Wan, P.; Hankin, J.; Tseng, C.C.; Yu, M.C.; Pike, M.C. Adolescent and adult soy intake and risk of breast cancer in Asian-Americans. Carcinogenesis 2002, 23, 1491–1496. [Google Scholar] [CrossRef]
- dos Santos Silva, I.; Mangtani, P.; McCormack, V.; Bhakta, D.; McMichael, A.J.; Sevak, L. Phyto-oestrogen intake and breast cancer risk in South Asian women in England: Findings from a population-based case-control study. Cancer Causes Control 2004, 15, 805–818. [Google Scholar] [CrossRef]
- Linseisen, J.; Piller, R.; Hermann, S.; Chang-Claude, J.; German Case-Control, S. Dietary phytoestrogen intake and premenopausal breast cancer risk in a German case-control study. Int. J. Cancer 2004, 110, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Hirose, K.; Imaeda, N.; Tokudome, Y.; Goto, C.; Wakai, K.; Matsuo, K.; Ito, H.; Toyama, T.; Iwata, H.; Tokudome, S.; et al. Soybean products and reduction of breast cancer risk: A case-control study in Japan. Br. J. Cancer 2005, 93, 15–22. [Google Scholar] [CrossRef]
- Iwasaki, M.; Hamada, G.S.; Nishimoto, I.N.; Netto, M.M.; Motola, J., Jr.; Laginha, F.M.; Kasuga, Y.; Yokoyama, S.; Onuma, H.; Nishimura, H.; et al. Dietary isoflavone intake and breast cancer risk in case-control studies in Japanese, Japanese Brazilians, and non-Japanese Brazilians. Breast Cancer Res. Treat. 2009, 116, 401–411. [Google Scholar] [CrossRef]
- Zhang, M.; Yang, H.; Holman, C.D. Dietary intake of isoflavones and breast cancer risk by estrogen and progesterone receptor status. Breast Cancer Res. Treat. 2009, 118, 553–563. [Google Scholar] [CrossRef]
- Cho, Y.A.; Kim, J.; Park, K.S.; Lim, S.Y.; Shin, A.; Sung, M.K.; Ro, J. Effect of dietary soy intake on breast cancer risk according to menopause and hormone receptor status. Eur. J. Clin. Nutr. 2010, 64, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Ho, S.C.; Lin, F.; Cheng, S.; Fu, J.; Chen, Y. Soy product and isoflavone intake and breast cancer risk defined by hormone receptor status. Cancer Sci. 2010, 101, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Li, H.; Tao, P.; Wang, Y.P.; Yuan, P.; Yang, C.X.; Li, J.Y.; Yang, F.; Lee, H.; Huang, Y. Soy isoflavones, CYP1A1, CYP1B1, and COMT polymorphisms, and breast cancer: A case-control study in southwestern China. DNA Cell Biol. 2011, 30, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.N.; Cotterchio, M.; Boucher, B.A.; Kreiger, N. Phytoestrogen intake from foods, during adolescence and adulthood, and risk of breast cancer by estrogen and progesterone receptor tumor subgroup among Ontario women. Int. J. Cancer 2013, 132, 1683–1692. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhang, M.; Holman, C.D. Population versus hospital controls in the assessment of dietary intake of isoflavone for case-control studies on cancers in China. Nutr. Cancer 2013, 65, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Toi, M.; Hirota, S.; Tomotaki, A.; Sato, N.; Hozumi, Y.; Anan, K.; Nagashima, T.; Tokuda, Y.; Masuda, N.; Ohsumi, S.; et al. Probiotic Beverage with Soy Isoflavone Consumption for Breast Cancer Prevention: A Case-control Study. Curr. Nutr. Food Sci. 2013, 9, 194–200. [Google Scholar] [CrossRef]
- Chang, Y.J.; Hou, Y.C.; Chen, L.J.; Wu, J.H.; Wu, C.C.; Chang, Y.J.; Chung, K.P. Is vegetarian diet associated with a lower risk of breast cancer in Taiwanese women? BMC Public Health 2017, 17, 800. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.L.; Ho, S.C.; Mo, X.F.; Lin, F.Y.; Zhang, N.Q.; Luo, H.; Zhang, X.; Zhang, C.X. Association between flavonoids, flavonoid subclasses intake and breast cancer risk: A case-control study in China. Eur. J. Cancer Prev. 2020, 29, 493–500. [Google Scholar] [CrossRef]
- Butler, L.M.; Wu, A.H.; Wang, R.; Koh, W.P.; Yuan, J.M.; Yu, M.C. A vegetable-fruit-soy dietary pattern protects against breast cancer among postmenopausal Singapore Chinese women. Am. J. Clin. Nutr. 2010, 91, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Nakamura, K.; Tamai, Y.; Tsuji, M.; Kawachi, T.; Hori, A.; Takeyama, N.; Tanabashi, S.; Matsushita, S.; Tokimitsu, N.; et al. Soy isoflavone intake and breast cancer risk in Japan: From the Takayama study. Int. J. Cancer 2013, 133, 952–960. [Google Scholar] [CrossRef]
- Morimoto, Y.; Maskarinec, G.; Park, S.Y.; Ettienne, R.; Matsuno, R.K.; Long, C.; Steffen, A.D.; Henderson, B.E.; Kolonel, L.N.; Le Marchand, L.; et al. Dietary isoflavone intake is not statistically significantly associated with breast cancer risk in the Multiethnic Cohort. Br. J. Nutr. 2014, 112, 976–983. [Google Scholar] [CrossRef]
- Shirabe, R.; Saito, E.; Sawada, N.; Ishihara, J.; Takachi, R.; Abe, S.K.; Shimazu, T.; Yamaji, T.; Goto, A.; Iwasaki, M.; et al. Fermented and nonfermented soy foods and the risk of breast cancer in a Japanese population-based cohort study. Cancer Med. 2021, 10, 757–771. [Google Scholar] [CrossRef]
- You, C.P.; Tsoi, H.; Man, E.P.S.; Leung, M.H.; Khoo, U.S. Modulating the Activity of Androgen Receptor for Treating Breast Cancer. Int. J. Mol. Sci. 2022, 23, 15342. [Google Scholar] [CrossRef]
- Islam, M.S.; Afrin, S.; Jones, S.I.; Segars, J. Selective Progesterone Receptor Modulators-Mechanisms and Therapeutic Utility. Endocr. Rev. 2020, 41, bnaa012. [Google Scholar] [CrossRef]
- Khan, S.A.; Chatterton, R.T.; Michel, N.; Bryk, M.; Lee, O.; Ivancic, D.; Heinz, R.; Zalles, C.M.; Helenowski, I.B.; Jovanovic, B.D.; et al. Soy isoflavone supplementation for breast cancer risk reduction: A randomized phase II trial. Cancer Prev. Res. 2012, 5, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Lamartiniere, C.A.; Moore, J.B.; Brown, N.M.; Thompson, R.; Hardin, M.J.; Barnes, S. Genistein suppresses mammary cancer in rats. Carcinogenesis 1995, 16, 2833–2840. [Google Scholar] [CrossRef] [PubMed]
- Thanos, J.; Cotterchio, M.; Boucher, B.A.; Kreiger, N.; Thompson, L.U. Adolescent dietary phytoestrogen intake and breast cancer risk (Canada). Cancer Causes Control 2006, 17, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Touillaud, M.; Gelot, A.; Mesrine, S.; Bennetau-Pelissero, C.; Clavel-Chapelon, F.; Arveux, P.; Bonnet, F.; Gunter, M.; Boutron-Ruault, M.C.; Fournier, A. Use of dietary supplements containing soy isoflavones and breast cancer risk among women aged >50 y: A prospective study. Am. J. Clin. Nutr. 2019, 109, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Beaubernard, L.; Lamothe, V.; Bennetau-Pelissero, C. New Evaluation of Isoflavone Exposure in the French Population. Nutrients 2019, 11, 2308. [Google Scholar] [CrossRef]
- Villares, A.; Rostagno, M.A.; García-Lafuente, A.; Guillamón, E.; Martínez, J.A. Content and Profile of Isoflavones in Soy-Based Foods as a Function of the Production Process. Food Bioprocess Technol. 2011, 4, 27–38. [Google Scholar] [CrossRef]
- Messina, M.; Nagata, C.; Wu, A.H. Estimated Asian adult soy protein and isoflavone intakes. Nutr. Cancer 2006, 55, 1–12. [Google Scholar] [CrossRef]
- Jun, S.; Shin, S.; Joung, H. Estimation of dietary flavonoid intake and major food sources of Korean adults. Br. J. Nutr. 2016, 115, 480–489. [Google Scholar] [CrossRef]
- Vieux, F.; Maillot, M.; Rehm, C.D.; Drewnowski, A. Flavonoid Intakes in the US Diet Are Linked to Higher Socioeconomic Status and to Tea Consumption: Analyses of NHANES 2011-16 Data. J. Nutr. 2020, 150, 2147–2155. [Google Scholar] [CrossRef]
- Sebastian, R.S.; Wilkinson Enns, C.; Goldman, J.D.; Martin, C.L.; Steinfeldt, L.C.; Murayi, T.; Moshfegh, A.J. A New Database Facilitates Characterization of Flavonoid Intake, Sources, and Positive Associations with Diet Quality among US Adults. J. Nutr. 2015, 145, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Jackowiak, H.; Packa, D.; Wiwart, M.; Perkowski, J. Scanning electron microscopy of Fusarium damaged kernels of spring wheat. Int. J. Food Microbiol. 2005, 98, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Constantine, G.D.; Kessler, G.; Graham, S.; Goldstein, S.R. Increased Incidence of Endometrial Cancer Following the Women’s Health Initiative: An Assessment of Risk Factors. J. Womens Health 2019, 28, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Alekel, D.L.; Van Loan, M.D.; Koehler, K.J.; Hanson, L.N.; Stewart, J.W.; Hanson, K.B.; Kurzer, M.S.; Peterson, C.T. The soy isoflavones for reducing bone loss (SIRBL) study: A 3-y randomized controlled trial in postmenopausal women. Am. J. Clin. Nutr. 2010, 91, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Unfer, V.; Casini, M.L.; Costabile, L.; Mignosa, M.; Gerli, S.; Di Renzo, G.C. Endometrial effects of long-term treatment with phytoestrogens: A randomized, double-blind, placebo-controlled study. Fertil. Steril. 2004, 82, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Tai, T.Y.; Tsai, K.S.; Tu, S.T.; Wu, J.S.; Chang, C.I.; Chen, C.L.; Shaw, N.S.; Peng, H.Y.; Wang, S.Y.; Wu, C.H. The effect of soy isoflavone on bone mineral density in postmenopausal Taiwanese women with bone loss: A 2-year randomized double-blind placebo-controlled study. Osteoporos. Int. 2012, 23, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Quaas, A.M.; Kono, N.; Mack, W.J.; Hodis, H.N.; Felix, J.C.; Paulson, R.J.; Shoupe, D. Effect of isoflavone soy protein supplementation on endometrial thickness, hyperplasia, and endometrial cancer risk in postmenopausal women: A randomized controlled trial. Menopause 2013, 20, 840–844. [Google Scholar] [CrossRef]
- Jacobsen, B.K.; Jaceldo-Siegl, K.; Knutsen, S.F.; Fan, J.; Oda, K.; Fraser, G.E. Soy isoflavone intake and the likelihood of ever becoming a mother: The Adventist Health Study-2. Int. J. Womens Health 2014, 6, 377–384. [Google Scholar] [CrossRef]
- Andrews, M.A.; Schliep, K.C.; Wactawski-Wende, J.; Stanford, J.B.; Zarek, S.M.; Radin, R.G.; Sjaarda, L.A.; Perkins, N.J.; Kalwerisky, R.A.; Hammoud, A.O.; et al. Dietary factors and luteal phase deficiency in healthy eumenorrheic women. Hum. Reprod. 2015, 30, 1942–1951. [Google Scholar] [CrossRef]
- Wiseman, H.; Casey, K.; Clarke, D.B.; Barnes, K.A.; Bowey, E. Isoflavone aglycon and glucoconjugate content of high- and low-soy U.K. foods used in nutritional studies. J. Agric. Food Chem. 2002, 50, 1404–1410. [Google Scholar] [CrossRef]
- Setchell, K.D.; Brown, N.M.; Desai, P.; Zimmer-Nechemias, L.; Wolfe, B.E.; Brashear, W.T.; Kirschner, A.S.; Cassidy, A.; Heubi, J.E. Bioavailability of pure isoflavones in healthy humans and analysis of commercial soy isoflavone supplements. J. Nutr. 2001, 131, 1362S–1375S. [Google Scholar] [CrossRef] [PubMed]
- Ju, Y.H.; Fultz, J.; Allred, K.F.; Doerge, D.R.; Helferich, W.G. Effects of dietary daidzein and its metabolite, equol, at physiological concentrations on the growth of estrogen-dependent human breast cancer (MCF-7) tumors implanted in ovariectomized athymic mice. Carcinogenesis 2006, 27, 856–863. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the study’s screening process.
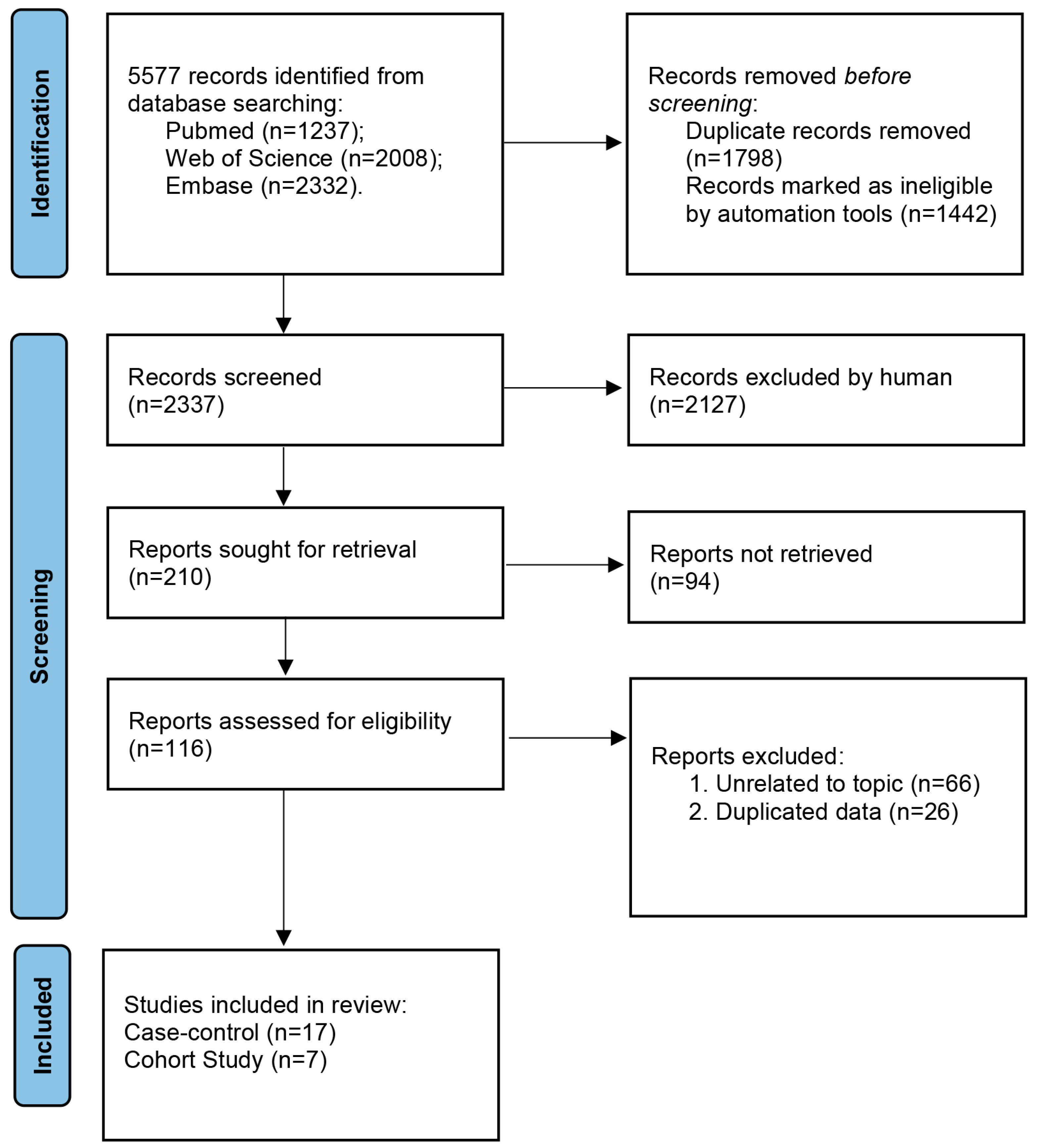
Figure 2.
Forest plot of the association between isoflavone intake and risk of breast cancer (highest versus lowest category meta-analysis). The size of the box representing the point estimate for each study in the forest plot is in proportion to the contribution of that study’s weight estimate to the summary estimate. The horizontal lines indicate the 95% CIs. The diamond denotes the pooled odds ratio. The dotted line represents the average of pooled odds ratio [5,6,7,8,9,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40].
Figure 2.
Forest plot of the association between isoflavone intake and risk of breast cancer (highest versus lowest category meta-analysis). The size of the box representing the point estimate for each study in the forest plot is in proportion to the contribution of that study’s weight estimate to the summary estimate. The horizontal lines indicate the 95% CIs. The diamond denotes the pooled odds ratio. The dotted line represents the average of pooled odds ratio [5,6,7,8,9,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40].

Figure 3.
Dose–response meta-analysis of the association between isoflavone dietary intake and breast cancer risk: (A) cohort studies, estimated using the REMR model; (B) cohort studies, estimated using the GLST model; (C) case-control studies, estimated using the REMR model; (D) case-control studies, estimated using the GLST model.
Figure 3.
Dose–response meta-analysis of the association between isoflavone dietary intake and breast cancer risk: (A) cohort studies, estimated using the REMR model; (B) cohort studies, estimated using the GLST model; (C) case-control studies, estimated using the REMR model; (D) case-control studies, estimated using the GLST model.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of studies included in the meta-analysis.
| Author | Publication Year | Study Design | Population | Study Period | Case/Subjects | Verification of Breast Cancer | Exposure Range (mg/day) | Variables of Adjustment | Exposure Assessment |
|---|---|---|---|---|---|---|---|---|---|
| Keiko Wada | 2013 | Cohort | Asian | 1992–2008 | 172/15,607 | Cancer registry record | <19.9 vs. >67.4 | 2, 3, 5, 6, 7, 8, 11, 15, 22, 28 | FFQ |
| Lesley M Butler | 2010 | Cohort | Asian | 1993–2005 | 629/34,028 | Histologically confirmed | <4.6 vs. >33.9 | 2, 6, 7, 10, 12, 22, 42, 43 | FFQ |
| Michelle L. Baglia | 2016 | Cohort | Asian | 1996–2011 | 1034/70,578 | Cancer registry record | <11.1 vs. >55 | 2, 5, 7, 8, 10, 12, 22, 28, 44 | FFQ |
| Raul Zamora-Ros | 2013 | Cohort | Non-Asian | 1992–2010 | 11,576/334,850 | Histologically confirmed | <0.22 vs. >1.36 | 2, 3, 5, 7, 8, 9, 11, 12, 13, 15, 20, 22, 28, 33 | FFQ |
| Ritsuko Shirabe | 2021 | Cohort | Asian | 1990–2013 | 825/46,714 | Histologically confirmed | <9.1 vs. >44.8 | 2, 3, 6, 10, 11, 12, 13, 14, 15, 18, 19, 20, 22, 23, 28, 45 | FFQ |
| Yukiko Morimoto | 2014 | Cohort | Non-Asian | 1993–2007 | 4769/84,550 | Cancer registry record | <3.2 vs. >20.3 | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16 | FFQ |
| Yuxia Wei | 2020 | Cohort | Asian | 2004–2016 | 2289/300,852 | Cancer registry record | <4.5 vs. >19.1 | 2, 3, 6, 7, 8, 9, 12, 13, 15, 17, 18, 19, 20, 28, 30 | FFQ |
| Yan-yun Zhu | 2011 | Case control | Asian | 2008~2011 | 62/108 | Histologically confirmed | <7.56 vs. >28.83 | 10, 13, 15, 21, 22, 30, 31 | FFQ |
| Min Zhang | 2009 | Case control | Asian | 2004–2005 | 158/410 | Histologically confirmed | <7.78 vs. >25.40 | 2, 3, 7, 8, 9, 10, 12, 13, 15, 22, 23, 24, 28, 31 | FFQ |
| Caixia Zhang | 2009 | Case control | Asian | 2007–2008 | 140/249 | Histologically confirmed | <3.26 vs. >16.89 | 2, 3, 10, 12, 13, 21, 28, 30 | FFQ |
| Anna H Wu | 2002 | Case control | Non-Asian | 1995–1998 | 130/278 | Cancer registry record | <1.79 mg/1000 kcal vs. >12.68 mg/1000 kcal | 2, 3, 7, 8, 10, 11, 13, 15, 22, 25, 26, 27, 28 | FFQ |
| Motoki Iwasaki | 2008 | Case control | Asian | 2001–2006 | 850/1700 | Histologically confirmed | <8.7 vs. >71.3 | 6, 8, 10, 13, 28, 32 | FFQ |
| Pamela L. Horn-Ross | 2001 | Case control | Non-Asian | 1995–1998 | 292/694 | Cancer registry record | <1.048 vs. >2.774 | 1, 2, 3, 6, 7, 8, 10, 11, 12, 19, 21, 22 | FFQ |
| K Hirose | 2005 | Case control | Asian and Non-Asian | 2001–2002 | 36/174 | Histologically confirmed | <7.61 vs. >11.87 | 2, 3, 5, 6, 12, 13, 15, 20, 22, 29, 28 | FFQ |
| Isabel dos Santos Silva | 2004 | Case control | Non-Asian | 1995–1999 | 239/714 | Cancer registry record | <0.125 mg/1862 kcal vs. >0.470 mg/1862 kcal | 3, 5, 7, 10, 19, 20, 26 | FFQ |
| Michelle Cotterchio | 2007 | Case control | Non-Asian | 2002–2003 | 3000/6370 | Histologically confirmed | <0.082 vs. >1.237 | 5, 10, 11, 21, 22, 33 | FFQ |
| Y. A. Cho | 2010 | Case control | Asian | 2007–2008 | 138/257 | Histologically confirmed | <8.5 vs. >23.7 | 2, 3, 6, 7, 8, 10, 11, 12, 13, 15, 22, 28, 34, 35 | FFQ |
| Masakazu Toi | 2013 | Case control | Asian | 2007–2009 | 101/266 | Cancer registry record | <18.76 vs. >43.75 | 3, 6, 7, 10, 11, 12, 19, 20, 21, 22, 28, 36, 46 | FFQ |
| Jakob Linseisen | 2004 | Case control | Non-Asian | 1992–1995 | 278/944 | Histologically confirmed | <0.1737 vs. >0.4147 | 2, 6, 7, 10, 12,13, 19 | FFQ |
| Lin Li | 2013 | Case control | Asian | 2009–2010 | 113/189 | Cancer registry record | <12.49 vs. >35.12 | 6, 7, 8, 9,10, 12, 13, 15, 17, 24, 28, 31, 37, 38 | FFQ |
| Xiao-Li Feng | 2019 | Case control | Asian | 2007–2008 | 456/843 | Histologically confirmed | <3.41 vs. >13.05 | 2, 7, 9, 15, 17, 22, 28, 31 | FFQ |
| Yao-Jen Chang | 2017 | Case control | Asian | 2010–2013 | 233/449 | Cancer registry record | <22 vs. >22 | 22, 28 | FFQ |
| Qiong Wang | 2011 | Case control | Asian | 2007–2009 | 181/299 | Histologically confirmed | <9.95 vs. >23.55 | 2, 5, 9, 12, 13, 19, 39, 40, 41 | FFQ |
| Laura N. Anderson | 2012 | Case control | Non-Asian | 2002–2003 | 476/1587 | Histologically confirmed | <0.122 vs. >0.497 | 5, 10, 11, 21, 22, 33 | FFQ |
FFQ, food frequency questionnaire. Variables of adjustment: (1) ethnicity; (2) BMI; (3) age at menarche; (4) age at cohort entry; (5) age at first live birth; (6) parity; (7) education; (8) menopausal status; (9) oral contraceptive use; (10) family history of breast cancer; (11) menopausal hormone use; (12) total energy intake; (13) smoking; (14) diabetes; (15) alcohol; (16) hypertension; (17) household income; (18) standing height; (19) lactation; (20) age at menopause; (21) history of breast disease; (22) age; (23) residential area; (24) tea drinking; (25) birthplace; (26) pregnancy; (27) dark leafy greens during adolescence; (28) physical activity; (29) motives for consultation; (30) vegetables and fruit intake; (31) passive smoking; (32) vitamin supplement use; (33) dietary fiber intake; (34) current use of dietary supplements; (35) occupation; (36) birth weight; (37) household size; (38) BMI 5 year ago; (39) total protein intake; (40) total fat intake; (41) number of abortions; (42) interview year; (43) dialect group; (44) season of recruitment; (45) received mammography; (46) BMI at the approximate age of 20.
Table 2.
Subgroup analyses of isoflavone intake and the risk of breast cancer (highest versus lowest category meta-analysis).
Table 2.
Subgroup analyses of isoflavone intake and the risk of breast cancer (highest versus lowest category meta-analysis).
| Outcome of Interest | No. of Studies | OR (95% CI) | pheterogenity | I2 (%) | p for Interaction |
|---|---|---|---|---|---|
| Study design | |||||
| Case control | 17 | 0.62 (0.50, 0.76) | 0.000 | 83.8% | 0.000 |
| Cohort | 7 | 0.94 (0.86, 1.02) | 0.178 | 32.7% | |
| Population | |||||
| Non-Asian | 8 | 0.97 (0.88, 1.06) | 0.092 | 43.0% | 0.000 |
| Asian | 18 | 0.62 (0.52, 0.74) | 0.000 | 75.6% | |
| Publication year | |||||
| Before 2010 | 11 | 0.67 (0.52, 0.87) | 0.000 | 81.5% | 0.462 |
| After 2010 | 13 | 0.75 (0.64, 0.87) | 0.000 | 82.3% | |
| Study quality | |||||
| NOS score ≤ 7 | 10 | 0.77 (0.63, 0.93) | 0.000 | 77.4% | 0.362 |
| NOS score > 7 | 14 | 0.68 (0.56, 0.82) | 0.000 | 84.2% | |
| Menopausal status | |||||
| Premenopausal | 16 | 0.76 (0.63, 0.92) | 0.000 | 66.6% | 0.897 |
| Postmenopausal | 16 | 0.75 (0.62, 0.90) | 0.000 | 78.3% | |
| Isoflavone highest intake | |||||
| <10 mg/d | 6 | 1.01 (0.94, 1.08) | 0.452 | 0.0% | 0.000 |
| ≥10 mg/d | 18 | 0.63 (0.53, 0.75) | 0.000 | 81.4% | |
| ER status | |||||
| ER+ | 7 | 0.77 (0.62, 0.95) | 0.000 | 75.7% | 0.981 |
| ER− | 7 | 0.77 (0.52, 1.15) | 0.000 | 84.1% |
OR, odds ratio; CI, confidence interval; p heterogenity, p for heterogeneity within subgroups; NOS, Newcastle–Ottawa Scale; ER, estrogen receptor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yang, J.; Shen, H.; Mi, M.; Qin, Y. Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies. Nutrients 2023, 15, 2402. https://doi.org/10.3390/nu15102402
AMA Style
Yang J, Shen H, Mi M, Qin Y. Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies. Nutrients. 2023; 15(10):2402. https://doi.org/10.3390/nu15102402
Chicago/Turabian StyleYang, Jining, Hui Shen, Mantian Mi, and Yu Qin. 2023. "Isoflavone Consumption and Risk of Breast Cancer: An Updated Systematic Review with Meta-Analysis of Observational Studies" Nutrients 15, no. 10: 2402. https://doi.org/10.3390/nu15102402
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.