

Effect of Targeted vs. Standard Fortification of Breast Milk on Growth and Development of Preterm Infants (≤32 Weeks): Results from an Interrupted Randomized Controlled Trial

Abstract
1. Introduction
1.1. Objectives
Research Hypothesis
1.2. Study Objectives
1.2.1. Primary Objective
1.2.2. Secondary Objectives
- feeding tolerance,
- velocity of weight gain,
- length and head growth
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.2.1. Study Setting
2.2.2. Eligibility Criteria
2.2.3. Inclusion Criteria
- Gestational age at birth ≤ 32 weeks
- Enteral feeding of at least 80 mL/kg/day
- 50% donor or maternal milk-based enteral feeding
- Parenteral/legal guardian consent
2.2.4. Exclusion Criteria
- Formula feeding
- Small for gestational age (birth weight < 3rd percentile)
- Presence of congenital abnormalities, which increase the risk of necrotizing enterocolitis such as hypoplastic left heart syndrome, transposition of the great arteries, omphalocele, gastroschisis
- Necrotizing enterocolitis (NEC)
- Withdrawal of feeding > 7 days
- Sepsis
- Death
2.2.5. Obtaining Informed Consent
2.2.6. Sample Size
2.3. Interventions
2.3.1. Explanation for the Choice of Comparators
2.3.2. Intervention Description
- Determination of macronutrient concentration in OMM/HDM.
- SF: Human milk fortifier, HMF Nutricia®.
- TF: Adding fat, protein, or carbohydrates to achieve the target levels of macronutrients.
2.3.3. Criteria for Discontinuing or Modifying Allocated Interventions
- Sepsis
- NEC
- Withdrawal of parental/guardian consent
- Poor feeding tolerance, defined as increasing abdominal distension >2 cm between inter-observer measurement or regurgitations after feeding >3 feeds per day
2.3.4. Strategies to Improve Adherence to Interventions
2.3.5. Relevant Concomitant Care Permitted or Prohibited during the Trial
2.4. Outcomes
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
- Growth (weight, length, and head circumference) was assessed at discharge and four months of corrected age.
- Feeding tolerance under the whole fortification period.
- Morbidity: Incidence of NEC, retinopathy of prematurity (ROP), bronchopulmonary dysplasia (BPD), intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL), sepsis, and pneumonia. The definitions are as follows:
- Feeding tolerance was defined as hemorrhagic residuals or vomiting of bile until pathological causes were ruled out (intestinal obstruction or ileus) [18]. Gastric residuals and abdominal girth were not routinely assessed. Isolated green or yellow residuals were considered unimportant.
- NEC: Stage II or III. Stage II requires clinical manifestations of a distended abdomen and radiological verification (intramural or portal gases). Stage III requires findings like in Stage II and more severe clinical symptoms (shock, need for a respirator). In surgically verified cases, radiological verification is not required [19].
- ROP: Stages I to V, diagnosed by an ophthalmologist according to international criteria [20].
- BPD: Need for oxygen, continuous positive airway pressure (CPAP,) or mechanical ventilation at 36+0 weeks of gestational age [21].
- IVH as defined by Volpe [18].
- PVL as defined by Volpe [18].
- Early- and late-onset sepsis was defined as positive blood or cerebral fluid culture at less and more than 72 h of age, respectively [22].
2.5. Recruitment
2.6. Assignment of Interventions: Allocation
2.6.1. Sequence Generation
2.6.2. Concealment Mechanism
2.6.3. Implementation
2.7. Assignment of Interventions: Blinding
2.7.1. Who Was Blinded
2.7.2. Procedure for Unblinding if Needed
2.8. Plans for Assessment and Collection of Outcomes
Primary Outcome
2.9. Plans to Promote Participant Retention and Complete Follow-Up
2.10. Data Management
2.11. Confidentiality
2.12. Statistical Methods for Primary and Secondary Outcomes
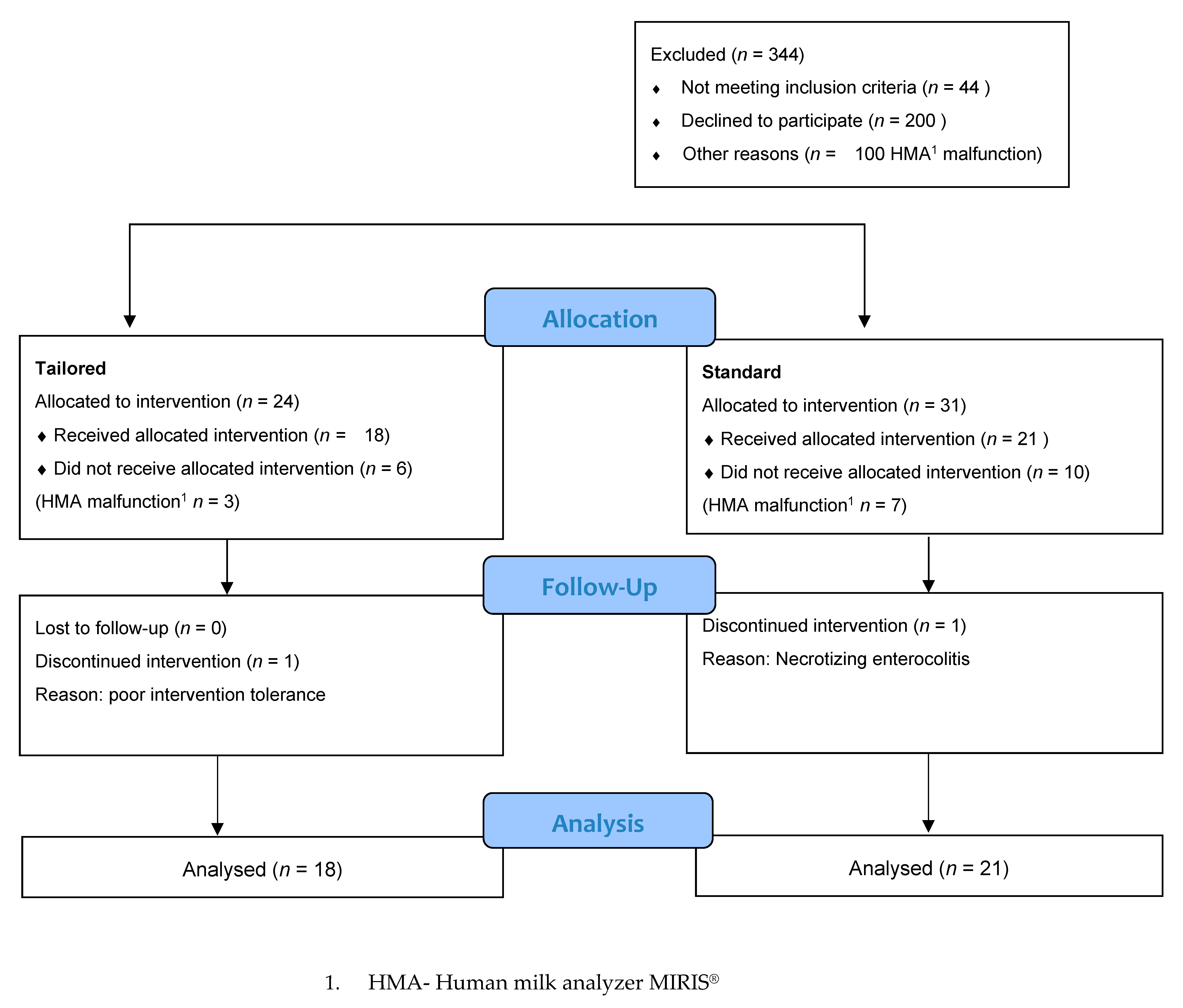
3. Results
3.1. Demographics
3.2. Milk Composition
3.3. Nutritional Intake and Growth
3.4. Secondary Outcomes
4. Discussion
4.1. Principal Findings
4.2. Comparison with Other Studies
4.3. Strengths and Limitations
4.4. Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, F.; Tang, Q.; Wang, Y.; Wu, J.; Ruan, H.; Lu, L.; Tao, Y.; Cai, W. Analysis of Nutrition Support in Very Low-Birth-Weight Infants with Extrauterine Growth Restriction. Nutr. Clin. Pract. 2018, 34, 436–443. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A.; Younes, N.; Lemons, J.A.; Fanaroff, A.A.; Donovan, E.F.; Wright, L.L.; Katsikiotis, V.; Tyson, J.E.; Oh, W.; Shankaran, S.; et al. Longitudinal Growth of Hospitalized Very Low Birth Weight Infants. Pediatrics 1999, 104, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.H.; Thomas, P.; Peabody, J. Extrauterine Growth Restriction Remains a Serious Problem in Prematurely Born Neonates. Pediatrics 2003, 111, 986–990. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral Nutrient Supply for Preterm Infants: Commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Boquien, C.-Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; et al. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef]
- Reali, A.; Greco, F.; Fanaro, S.; Atzei, A.; Puddu, M.; Moi, M.; Fanos, V. Fortification of maternal milk for very low birth weight (VLBW) pre-term neonates. Early Hum. Dev. 2010, 86 (Suppl. 1), 33–36. [Google Scholar] [CrossRef]
- Di Natale, C.; Coclite, E.; Di Ventura, L.; Di Fabio, S. Fortification of maternal milk for preterm infants. J. Matern.Fetal Neonatal Med. 2011, 24 (Suppl. 1), 41–43. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E.; the WAPM Working Group on Nutrition. Optimization of human milk fortification for preterm infants: New concepts and recommendations. J. Périnat. Med. 2010, 38, 233–238. [Google Scholar] [CrossRef]
- Wojcik, K.Y.; Rechtman, D.J.; Lee, M.L.; Montoya, A.; Medo, E.T. Macronutrient Analysis of a Nationwide Sample of Donor Breast Milk. J. Am. Diet. Assoc. 2009, 109, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; et al. Target Fortification of Breast Milk with Fat, Protein, and Carbohydrates for Preterm Infants. J. Pediatr. 2013, 163, 1001–1007. [Google Scholar] [CrossRef]
- Fabrizio, V.; Trzaski, J.M.; Brownell, E.A.; Esposito, P.; Lainwala, S.; Lussier, M.M.; Hagadorn, J.I. Individualized versus standard diet fortification for growth and development in preterm infants receiving human milk. Cochrane Database Syst. Rev. 2020, 11, CD013465. [Google Scholar]
- McLeod, G.; Sherriff, J.; Hartmann, P.E.; Nathan, E.; Geddes, D.; Simmer, K. Comparing different methods of human breast milk fortification using measured v. assumed macronutrient composition to target reference growth: A randomised controlled trial. Br. J. Nutr. 2016, 115, 431–439. [Google Scholar] [CrossRef]
- Fusch, G.; Mitra, S.; Rochow, N.; Fusch, C. Target fortification of breast milk: Levels of fat, protein or lactose are not related. Acta Paediatr. 2014, 104, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Adjustable fortification of human milk fed to preterm infants: Does it make a difference? J. Perinatol. 2006, 26, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Rochow, N.; Raja, P.; Liu, K.; Fenton, T.; Landau-Crangle, E.; Göttler, S.; Jahn, A.; Lee, S.; Seigel, S.; Campbell, D.; et al. Physiological adjustment to postnatal growth trajectories in healthy preterm infants. Pediatr. Res. 2016, 79, 870–879. [Google Scholar] [CrossRef]
- Landau-Crangle, E.; Rochow, N.; Fenton, T.R.; Liu, K.; Ali, A.; So, H.Y.; Fusch, G.; Marrin, M.L.; Fusch, C. Individualized Postnatal Growth Trajectories for Preterm Infants. J. Parenter. Enter. Nutr. 2018, 42, 1084–1092. [Google Scholar] [CrossRef]
- Seliga-Siwecka, J.; Chmielewska, A.; Jasinska, K. Effect of targeted vs. standard fortification of breast milk on growth and development of preterm infants (≤32 weeks): Study protocol for a randomized controlled trial. Trials 2020, 21, 946. [Google Scholar] [CrossRef]
- Volpe, J.J. Neonatal Intraventricular Hemorrhage. N. Engl. J. Med. 1981, 304, 886–891. [Google Scholar] [CrossRef]
- Polberger, S.; Räihä, N.C.R.; Juvonen, P.; Moro, G.E.; Minoli, I.; Warm, A. Individualized Protein Fortification of Human Milk for Preterm Infants: Comparison of Ultrafiltrated Human Milk Protein and a Bovine Whey Fortifier. J. Pediatr. Gastroenterol. Nutr. 1999, 29, 332–338. [Google Scholar] [CrossRef]
- Şimşek, G.K.; Dizdar, E.A.; Arayıcı, S.; Canpolat, F.E.; Sarı, F.N.; Uraş, N.; Oguz, S.S. Comparison of the Effect of Three Different Fortification Methods on Growth of Very Low Birth Weight Infants. Breastfeed. Med. 2019, 14, 63–68. [Google Scholar] [CrossRef]
- Maas, C.; Mathes, M.; Bleeker, C.; Vek, J.; Bernhard, W.; Wiechers, C.; Peter, A.; Poets, C.F.; Franz, A.R. Effect of Increased Enteral Protein Intake on Growth in Human Milk-Fed Preterm Infants: A Randomized Clinical Trial. JAMA Pediatr. 2017, 171, 16–22. [Google Scholar] [CrossRef] [PubMed]
- De Halleux, V.; Rigo, J. Variability in human milk composition: Benefit of individualized fortification in very-low-birth-weight infants. Am. J. Clin. Nutr. 2013, 98, 529S–535S. [Google Scholar] [CrossRef] [PubMed]
- Morlacchi, L.; Mallardi, D.; Giannì, M.L.; Roggero, P.; Amato, O.; Piemontese, P.; Consonni, D.; Mosca, F. Is targeted fortification of human breast milk an optimal nutrition strategy for preterm infants? An interventional study. J. Transl. Med. 2016, 14, 195. [Google Scholar] [CrossRef] [PubMed]
- Bulut, O.; Coban, A.; Uzunhan, O.; Ince, Z. Effects of Targeted Versus Adjustable Protein Fortification of Breast Milk on Early Growth in Very Low-Birth-Weight Preterm Infants: A Randomized Clinical Trial. Nutr. Clin. Pract. 2019, 35, 335–343. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Ali, A.; Bhatia, A.; So, H.Y.; Iskander, R.; Chessell, L.; el Helou, S.; Fusch, C. Individualized target fortification of breast milk with protein, carbohydrates, and fat for preterm infants: A double-blind randomized controlled trial. Clin. Nutr. 2021, 40, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Fusch, S.; Fusch, G.; Yousuf, E.I.; Rochow, M.; So, H.Y.; Fusch, C.; Rochow, N. Individualized Target Fortification of Breast Milk: Optimizing Macronutrient Content Using Different Fortifiers and Approaches. Front. Nutr. 2021, 8, 652641. [Google Scholar] [CrossRef]
- Quan, M.; Wang, D.; Gou, L.; Sun, Z.; Ma, J.; Zhang, L.; Wang, C.; Schibler, K.; Li, Z. Individualized Human Milk Fortification to Improve the Growth of Hospitalized Preterm Infants. Nutr. Clin. Pract. 2019, 35, 680–688. [Google Scholar] [CrossRef]
- Agakidou, E.; Karagiozoglou-Lampoudi, T.; Parlapani, E.; Fletouris, D.J.; Sarafidis, K.; Tzimouli, V.; Diamanti, E.; Agakidis, C. Modifications of Own Mothers’ Milk Fortification Protocol Affect Early Plasma IGF-I and Ghrelin Levels in Preterm Infants. A Randomized Clinical Trial. Nutrients 2019, 11, 3056. [Google Scholar] [CrossRef]
- Trading Economics. Available online: https://tradingeconomics.com/poland/gdp (accessed on 21 December 2022).
- Belfort, M.B.; Woodward, L.J.; Cherkerzian, S.; Pepin, H.; Ellard, D.; Steele, T.; Fusch, C.; Grant, P.E.; Inder, T.E. Targeting human milk fortification to improve very preterm infant growth and brain development: Study protocol for Nourish, a single-center randomized, controlled clinical trial. BMC Pediatr. 2021, 21, 167. [Google Scholar] [CrossRef]
- Fusch, G.; Rochow, N.; Choi, A.; Fusch, S.; Poeschl, S.; Ubah, A.O.; Lee, S.-Y.; Raja, P.; Fusch, C. Rapid measurement of macronutrients in breast milk: How reliable are infrared milk analyzers? Clin. Nutr. 2015, 34, 465–476. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Tailored (n = 18) | Standard (n = 21) | ||||
|---|---|---|---|---|---|---|
| n (%) | Mean ± SD | Median (Q1; Q3) | n (%) | Mean ± SD | Median (Q1; Q3) | |
| Gender, male | 9 (50.0) | - | - | 10 (47.6) | - | - |
| Gestational week | - | 29.22 ± 2.02 | 29.50 (28.00; 31.00) | - | 28.24 ± 2.62 | 29.00 (26.00; 31.00) |
| Birth weight, g | - | 1361.11 ± 454.30 | 1315.00 (1047.50; 1685.00) | - | 1250.95 ± 429.68 | 1200.00 (1000.00; 1620.00) |
| Birth length, cm | - | 41.33 ± 5.69 | 43.00 (37.50; 45.00) | - | 38.88 ± 6.14 | 39.00 (35.00; 45.00) |
| Head circumference, cm | - | 25.89 ± 7.21 | 28.25 (25.00; 30.00) | - | 25.40 ± 6.58 | 27.00 (24.00; 29.00) |
| Birth weight z-score | - | 0.39 ± 1.17 | 0.58 (-0.74; 1.13) | - | 0.62 ± 1.19 | 0.54 (−0.06; 1.21) |
| Birth length z-score | - | 1.42 ± 1.63 | 1.79 (0.22; 2.67) | - | 1.03 ± 1.72 | 1.21 (−0.03; 2.14) |
| Head circumference z-score | - | 0.55 ± 1.39 | 0.68 (-0.34; 1.64) | - | 0.68 ± 1.09 | 0.98 (−0.05; 1.70) |
| 80 mL/kg/day of maternal or human donor milk, day | - | 6.44 ± 4.67 | 6.00 (4.00; 6.75) | - | 7.90 ± 5.91 | 6.00 (5.00; 9.00) |
| 50% donor or maternal milk-based enteral feeding | 18 (100.0) | - | - | 21 (100.0) | - | - |
| Milk type/source–mother | 17 (94.4) | - | - | 21 (100.0) | - | - |
| Milk type/source–formula | 1 (5.6) | - | - | 1 (4.8) | - | - |
| Milk type/source–donor | 13 (72.2) | - | - | 13 (61.9) | - | - |
| Variable | Tailored | Standard | MD (95% CI) | p |
|---|---|---|---|---|
| Milk volume, mL | ||||
| Day 0 | - | - | - | - |
| Week 1 (1/2) | 241.60 ± 78.80 | 220.39 ± 65.79 | 21.21 (−30.10; 72.52) | 0.406 |
| Week 4 (2/2) | 305.60 ± 106.79 | 264.00 ± 114.45 | 41.60 (−62.39; 145.59) | 0.412 |
| Last measurement | 323.29 ± 114.93 | 313.60 ± 127.25 | 9.69 (−71.86; 91.25) | 0.811 |
| No. of HMF pieces | ||||
| Day 0 | - | - | - | - |
| Week 1 (1/2) | 8.94 ± 9.33 | 8.55 ± 7.94 | 0.38 (−5.55; 6.32) | 0.896 |
| Week 4 (2/2) | 20.00 ± 7.48 | 17.20 ± 8.70 | 2.80 (−4.83; 10.43) | 0.450 |
| Last measurement | 21.21 ± 7.43 | 16.50 ± 8.45 | 4.71 (−0.65; 10.06) | 0.083 |
| Protein, g/100 mL | ||||
| Day 0 | 2.02 ± 0.34 | - | - | - |
| Week 1 (1/2) | 2.00 ± 0.34 | 1.91 ± 0.22 | 0.09 (−0.10; 0.29) | 0.328 |
| Week 4 (2/2) | 1.37 ± 0.24 | 1.32 ± 0.15 | 0.05 (−0.14; 0.24) | 0.582 |
| Last measurement | 1.34 ± 0.26 | 1.38 ± 0.25 | −0.04 (−0.21; 0.13) | 0.640 |
| Glucose, g/100 mL | ||||
| Day 0 | 7.50 (7.10; 7.80) | - | - | - |
| Week 1 (1/2) | 7.60 (7.07; 7.80) | 7.40 (7.05; 7.60) | 0.20 (−0.10; 0.50) | 0.219 |
| Week 4 (2/2) | 7.60 (7.53; 7.77) | 7.90 (7.67; 8.00) | −0.30 (−0.50; 0.00) | 0.039 |
| Week 4 (2/2) (w/o one patient) | 7.60 (7.60; 7.80) | 7.90 (7.67; 8.00) | −0.30 (−0.40; 0.00) | 0.069 |
| Week 4 (2/2) (w/o one patient) | 7.67 ± 0.18 | 7.86 ± 0.22 | −0.19 (−0.39; 0.00) | 0.051 |
| Last measurement | 7.70 (7.60; 7.80) | 7.80 (7.60; 7.90) | −0.10 (-0.20; 0.10) | 0.348 |
| Fat, g/100 mL | ||||
| Day 0 | 3.36 ± 1.44 | - | - | - |
| Week 1 (1/2) | 3.48 ± 1.40 | 3.65 ± 1.20 | 8.00 (−17.00; 8.00) | 0.417 |
| Week 4 (2/2) | 4.06 ± 1.56 | 3.82 ± 0.56 | −0.10 (−0.80; 0.80) | 0.940 |
| Last measurement | 4.19 ± 1.48 | 3.52 ± 1.05 | 0.68 (−0.17; 1.53) | 0.113 |
| Energy, kcal/100 mL | ||||
| Day 0 | - | - | - | - |
| Week 1 (1/2) | 71.06 ± 12.38 | 71.21 ± 12.04 | −0.15 (-8.57; 8.27) | 0.972 |
| Week 4 (2/2) | 73.50 ± 12.20 | 73.10 ± 4.93 | 0.40 (−8.35; 9.15) | 0.925 |
| Last measurement | 75.35 ± 12.18 | 69.20 ± 10.06 | 6.15 (−1.27; 13.57) | 0.101 |
| Variable | Week 1/at Birth | Week 4/Study End | MD (95% CI) | p |
|---|---|---|---|---|
| Week 1 to week 4, tailored group (n = 8) | ||||
| Weight, g | 1379.56 ± 441.49 | 2011.67 ± 647.56 | 632.11 (359.94; 904.28) | 0.001 |
| Weight z-score | 0.00 ± 1.14 | 0.02 ± 0.89 | 0.02 (−0.72; 0.76) | 0.947 |
| Week 1 to week 4, standard group (n = 8) | ||||
| Weight, g | 1264.56 ± 365.98 | 1866.33 ± 570.42 | 601.78 (414.70; 788.86) | <0.001 |
| Weight z-score | 0.24 ± 1.15 | 0.29 ± 1.06 | 0.05 (−0.26; 0.36) | 0.723 |
| At birth to study end, tailored group (n = 18) | ||||
| Weight, g | 1361.11 ± 454.30 | 2253.22 ± 838.63 | 892.11 (548.76; 1235.46) | <0.001 |
| Length, cm | 41.33 ± 5.69 | 48.50 ± 6.02 | 7.17 (4.81; 9.53) | <0.001 |
| Head circumference, cm | 25.89 ± 7.21 | 32.53 ± 3.06 | 6.64 (3.34; 9.93) | 0.001 |
| Weight z-score | 0.39 ± 1.17 | −0.38 ± 1.35 | −0.78 (−1.05; −0.50) | <0.001 |
| Length z-score | 1.42 ± 1.63 | 1.30 ± 1.91 | −0.12 (−0.88; 0.64) | 0.749 |
| Head circumference z-score | 0.55 ± 1.39 | 0.74 ± 1.51 | 0.19 (−0.55; 0.93) | 0.592 |
| At birth to study end, standard group (n = 21) | ||||
| Weight, g | 1250.95 ± 429.68 | 2041.48 ± 843.51 | 790.52 (465.30; 1115.75) | <0.001 |
| Length, cm | 39.42 ± 5.76 | 44.90 ± 7.10 | 5.48 (3.37; 7.58) | <0.001 |
| Head circumference, cm | 25.42 ± 6.75 | 30.70 ± 4.05 | 5.28 (1.71; 8.84) | 0.006 |
| Weight z-score | 0.62 ± 1.19 | −0.35 ± 1.21 | −0.97 (−1.32; −0.61) | <0.001 |
| Length z-score | 1.21 ± 1.55 | 0.56 ± 1.80 | −0.65 (−1.13; −0.18) | 0.009 |
| Head circumference z-score | 0.66 ± 1.12 | −0.05 ± 1.43 | −0.72 (−1.15; −0.28) | 0.003 |
| Variable | Tailored (n = 18) | Standard (n = 21) | p |
|---|---|---|---|
| Poor feeding tolerance | 6 (33) | 3 (14.3) | |
| Sepsis | 0 (0.0) | 0 (0.0) | - |
| Necrotizing enterocolitis | 0 (0.0) | 1 (4.8) | >0.999 |
| Intraventricular haemorrhage 1 | 0 (0.0) | 1 (4.8) | >0.999 |
| Intraventricular haemorrhage 2 | 2 (11.1) | 6 (28.6) | 0.247 |
| Intraventricular haemorrhage 3 | 0 (0.0) | 2 (9.5) | 0.490 |
| Periventricular leukomalacia | 0 (0.0) | 0 (0.0) | - |
| Bronchopulmonary dysplasia | 3 (17.7) | 8 (38.1) | 0.260 |
| Retinopathy of premature | 7 (38.9) | 7 (33.3) | 0.980 |
| Death | 0 (0.0) | 0 (0.0) | - |
| Late onset sepsis | 0 (0.0) | 1 (4.8) | >0.999 |
| Enteral feeding suspended for at least 7 days | 1 (5.6) | 1 (4.8) | >0.999 |
| >50% formula feeding | 2 (11.1) | 1 (4.8) | 0.586 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seliga-Siwecka, J.; Fiałkowska, J.; Chmielewska, A. Effect of Targeted vs. Standard Fortification of Breast Milk on Growth and Development of Preterm Infants (≤32 Weeks): Results from an Interrupted Randomized Controlled Trial. Nutrients 2023, 15, 619. https://doi.org/10.3390/nu15030619
Seliga-Siwecka J, Fiałkowska J, Chmielewska A. Effect of Targeted vs. Standard Fortification of Breast Milk on Growth and Development of Preterm Infants (≤32 Weeks): Results from an Interrupted Randomized Controlled Trial. Nutrients. 2023; 15(3):619. https://doi.org/10.3390/nu15030619
Chicago/Turabian StyleSeliga-Siwecka, Joanna, Justyna Fiałkowska, and Anna Chmielewska. 2023. "Effect of Targeted vs. Standard Fortification of Breast Milk on Growth and Development of Preterm Infants (≤32 Weeks): Results from an Interrupted Randomized Controlled Trial" Nutrients 15, no. 3: 619. https://doi.org/10.3390/nu15030619
APA StyleSeliga-Siwecka, J., Fiałkowska, J., & Chmielewska, A. (2023). Effect of Targeted vs. Standard Fortification of Breast Milk on Growth and Development of Preterm Infants (≤32 Weeks): Results from an Interrupted Randomized Controlled Trial. Nutrients, 15(3), 619. https://doi.org/10.3390/nu15030619