
The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Information Sources
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Risk of Bias and Quality Assessment in Individual Studies
2.6. Summary Measures
2.7. Data Synthesis
2.8. Meta-Bias/Risk of Bias across Studies
3. Results
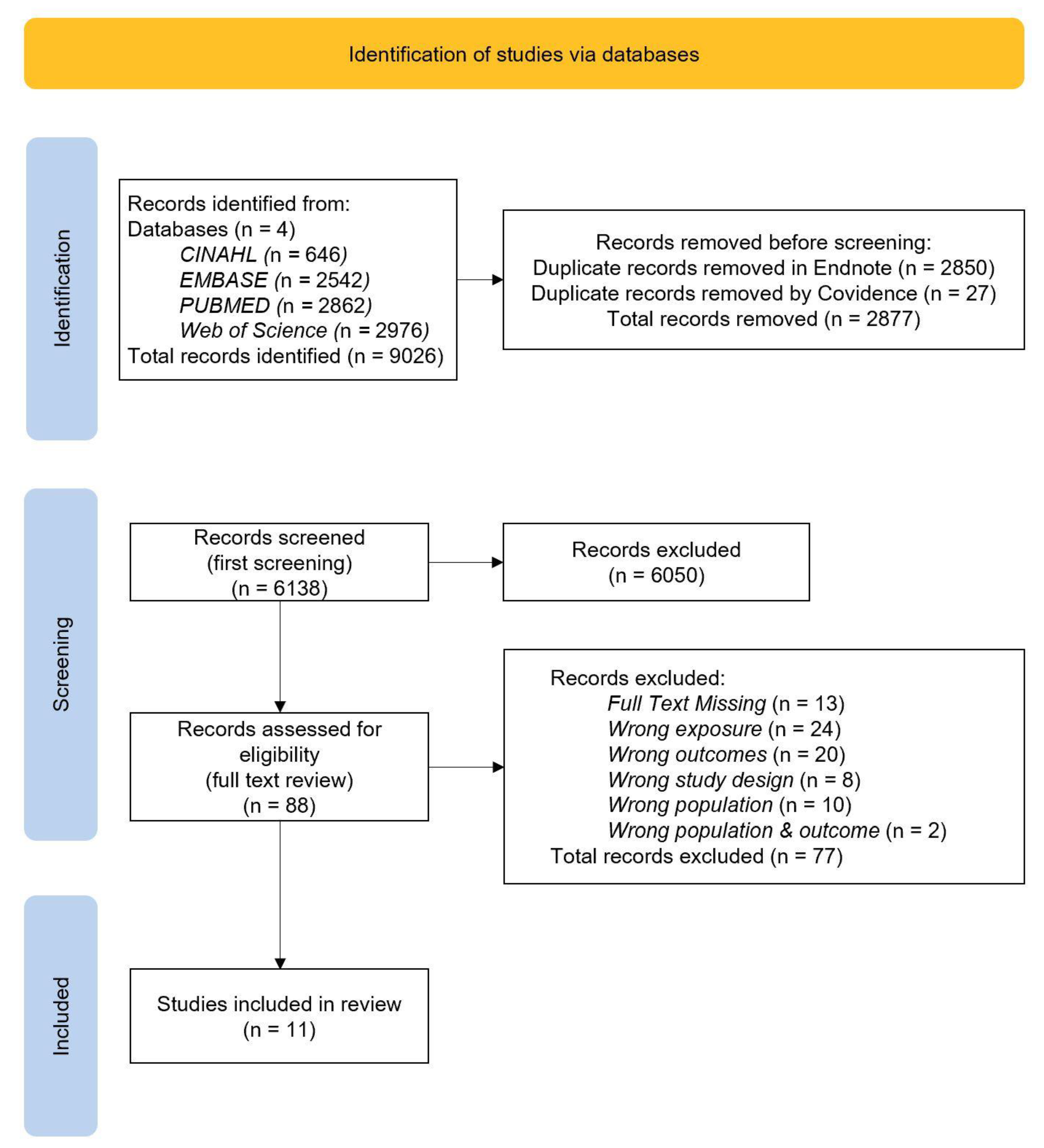
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Children’s Outcome Measures
3.2.2. Maternal Exposures
3.3. Results of Individual Studies
3.3.1. Studies on Child Body Composition (Continuous Variables)
3.3.2. Studies on Childhood Obesity Status (Categorical Variables)
3.4. Risk of Bias within Studies
4. Discussion
4.1. Strengths and Limitations
4.2. Implications and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Russell, C.G.; Russell, A. A biopsychosocial approach to processes and pathways in the development of overweight and obesity in childhood: Insights from developmental theory and research. Obes. Rev. 2019, 20, 725–749. [Google Scholar] [CrossRef] [PubMed]
- Wahlqvist, M.L.; Krawetz, S.A.; Rizzo, N.S.; Dominguez-Bello, M.G.; Szymanski, L.M.; Barkin, S.; Yatkine, A.; Waterland, R.A.; Mennella, J.A.; Desai, M.; et al. Early-life influences on obesity: From preconception to adolescence. Ann. N. Y. Acad. Sci. 2015, 1347, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Heslehurst, N.; Vieira, R.; Akhter, Z.; Bailey, H.; Slack, E.; Ngongalah, L.; Pemu, A.; Rankin, J. The association between maternal body mass index and child obesity: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002817. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.J.F.; Yeo, G.S.H. The genetics of obesity: From discovery to biology. Nat. Rev. Genet. 2022, 23, 120–133. [Google Scholar] [CrossRef]
- Drozdz, D.; Alvarez-Pitti, J.; Wójcik, M.; Borghi, C.; Gabbianelli, R.; Mazur, A.; Herceg-Čavrak, V.; Lopez-Valcarcel, B.G.; Brzeziński, M.; Lurbe, E.; et al. Obesity and Cardiometabolic Risk Factors: From Childhood to Adulthood. Nutrients 2021, 13, 4176. [Google Scholar] [CrossRef]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Tsolakis, C.; Cherouveim, E.D.; Skouras, A.Z.; Antonakis-Karamintzas, D.; Czvekus, C.; Halvatsiotis, P.; Savvidou, O.; Koulouvaris, P. The Impact of Obesity on the Fitness Performance of School-Aged Children Living in Rural Areas—The West Attica Project. Int. J. Environ. Res. Public Health 2022, 19, 11476. [Google Scholar] [CrossRef]
- Moussa, H.N.; Alrais, M.A.; Leon, M.G.; Abbas, E.L.; Sibai, B.M. Obesity epidemic: Impact from preconception to postpartum. Future Sci. OA 2016, 2, FSO137. [Google Scholar] [CrossRef]
- Téllez-Rojo, M.M.; Trejo-Valdivia, B.; Roberts, E.; Muñoz-Rocha, T.V.; Bautista-Arredondo, L.F.; Peterson, K.E.; Cantoral, A. Influence of post-partum BMI change on childhood obesity and energy intake. PLoS ONE 2019, 14, e0224830. [Google Scholar] [CrossRef]
- Hales, C.N.; Barker, D.J. Type 2 (non-insulin-dependent) diabetes mellitus: The thrifty phenotype hypothesis. Diabetologia 1992, 35, 595–601. [Google Scholar] [CrossRef]
- Manios, Y.; Birbilis, M.; Moschonis, G.; Birbilis, G.; Mougios, V.; Lionis, C.; Chrousos, G.P. Childhood Obesity Risk Evaluation based on perinatal factors and family sociodemographic characteristics: CORE Index. Eur. J. Pediatr. 2013, 172, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Voerman, E.; Santos, S.; Patro Golab, B.; Gaillard, R.; Jaddoe, V.W.V.; Charles, M.-A.; Heude, B.; Chatzi, L.; Georgiu, V.; Chevrier, C.; et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: An individual participant data meta-analysis. PLoS Med. 2019, 16, e1002744. [Google Scholar] [CrossRef]
- Olson, C.M.; Demment, M.M.; Carling, S.J.; Strawderman, M.S. Associations Between Mothers’ and Their Children’s Weights at 4 Years of Age. Child. Obes. 2010, 6, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Retzloff, L.; Lumeng, J.C.; Kaciroti, N.; Rosenblum, K.; Miller, A.L. Longitudinal associations between maternal feeding and overweight in low-income toddlers. Appetite 2017, 113, 23–29. [Google Scholar] [CrossRef]
- Farpour-Lambert, N.J.; Ells, L.J.; Martinez de Tejada, B.; Scott, C. Obesity and Weight Gain in Pregnancy and Postpartum: An Evidence Review of Lifestyle Interventions to Inform Maternal and Child Health Policies. Front. Endocrinol. 2018, 9, 546. [Google Scholar] [CrossRef] [PubMed]
- Leonard, S.A.; Rasmussen, K.M.; King, J.C.; Abrams, B. Trajectories of maternal weight from before pregnancy through postpartum and associations with childhood obesity. Am. J. Clin. Nutr. 2017, 106, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Liberali, R.; Kupek, E.; Assis, M.A.A. Dietary Patterns and Childhood Obesity Risk: A Systematic Review. Child. Obes. 2020, 16, 70–85. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting Obesogenic Environments: The Development and Application of a Framework for Identifying and Prioritizing Environmental Interventions for Obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; O’Connor, T.M.; Fisher, J.O.; Micheli, N.E.; Papaioannou, M.A. Maternal feeding style and child weight status among Hispanic families with low-income levels: A longitudinal study of the direction of effects. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 30. [Google Scholar] [CrossRef] [PubMed]
- Adane, A.A.; Dobson, A.; Tooth, L.; Mishra, G.D. Maternal preconception weight trajectories are associated with offsprings’ childhood obesity. Int. J. Obes. 2018, 42, 1265–1274. [Google Scholar] [CrossRef]
- Yoshida, S.; Kimura, T.; Noda, M.; Takeuchi, M.; Kawakami, K. Association of maternal prepregnancy weight and early childhood weight with obesity in adolescence: A population-based longitudinal cohort study in Japan. Pediatr. Obes. 2020, 15, e12597. [Google Scholar] [CrossRef]
- Yu, Z.; Han, S.; Zhu, J.; Sun, X.; Ji, C.; Guo, X. Pre-pregnancy body mass index in relation to infant birth weight and offspring overweight/obesity: A systematic review and meta-analysis. PLoS ONE 2013, 8, e61627. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.Y.; Junxiu, L.; Archer, E.; McDonald, S.M.; Jihong, L. Maternal Weight Gain in Pregnancy and Risk of Obesity among Offspring: A Systematic Review. J. Obes. 2014, 2014, 524939. [Google Scholar] [CrossRef] [PubMed]
- Gibson, L.; Allen, K.; Byrne, S.; Clark, K.; Blair, E.; Davis, E.; Zubrick, S. Childhood Overweight and Obesity: Maternal and Family Factors. J. Child Fam. Stud. 2016, 25, 3236–3246. [Google Scholar] [CrossRef]
- Ziauddeen, N.; Huang, J.Y.; Taylor, E.; Roderick, P.J.; Godfrey, K.M.; Alwan, N.A. Interpregnancy weight gain and childhood obesity: Analysis of a UK population-based cohort. Int. J. Obes. 2022, 46, 211–219. [Google Scholar] [CrossRef]
- Huang, D.Y.C.; Lanza, H.I.; Anglin, M.D. Trajectory of Adolescent Obesity: Exploring the Impact of Prenatal to Childhood Experiences. J. Child Fam. Stud. 2014, 23, 1090–1101. [Google Scholar] [CrossRef][Green Version]
- Kaar, J.L.; Crume, T.; Brinton, J.T.; Bischoff, K.J.; McDuffie, R.; Dabelea, D. Maternal obesity, gestational weight gain, and offspring adiposity: The exploring perinatal outcomes among children study. J. Pediatr. 2014, 165, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Ziauddeen, N.; Roderick, P.J.; Macklon, N.S.; Alwan, N.A. Predicting childhood overweight and obesity using maternal and early life risk factors: A systematic review. Obes. Rev. 2018, 19, 302–312. [Google Scholar] [CrossRef]
- BMJ. Study Design Search Filters. Available online: https://bestpractice.bmj.com/info/toolkit/learn-ebm/study-design-search-filters/ (accessed on 25 March 2022).
- The EndNote Team. EndNote, 20, 64 Bit; Clarivate Analytics: Philadelphia, PA, USA, 2013. [Google Scholar]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Covidence Covidence for Systematic Reviews; Veritas Health Innovation: Melbourne, VIC, Australia, 2020.
- Academy of Nutrition and Dietetics. Evidence Analysis Manual: Steps in the Academy Evidence Analysis Process. 2016. Available online: https://www.andeal.org/vault/2440/web/files/2016_April_EA_Manual.pdf (accessed on 24 April 2022).
- National Health and Medical Research Council. NHMRC Levels of Evidence and Grades for Recommendations for Developers of Guidelines. 2009. Available online: https://www.nhmrc.gov.au/sites/default/files/images/NHMRC%20Levels%20and%20Grades%20(2009).pdf (accessed on 24 April 2022).
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- CDC. Child Development: Positive Parenting. Available online: https://www.cdc.gov/ncbddd/childdevelopment/positiveparenting/index.html (accessed on 2 June 2022).
- Ehrenthal, D.B.; Maiden, K.; Rao, A.; West, D.W.; Gidding, S.S.; Bartoshesky, L.; Carterette, B.; Ross, J.; Strobino, D. Independent relation of maternal prenatal factors to early childhood obesity in the offspring. Obstet. Gynecol. 2013, 121, 115–121. [Google Scholar] [CrossRef]
- Zafar Janjua, N.; Mahmood, B.; Aminul Islam, M.; Goldenberg, R.L. Maternal and Early Childhood Risk Factors for Overweight and Obesity among Low-Income Predominantly Black Children at Age Five Years: A Prospective Cohort Study. J. Obes. 2012, 2012, 457173. [Google Scholar] [CrossRef]
- Daraki, V.; Georgiou, V.; Papavasiliou, S.; Chalkiadaki, G.; Karahaliou, M.; Koinaki, S.; Sarri, K.; Vassilaki, M.; Kogevinas, M.; Chatzi, L. Metabolic profile in early pregnancy is associated with offspring adiposity at 4 years of age: The Rhea pregnancy cohort Crete, Greece. PLoS ONE 2015, 10, e0126327. [Google Scholar] [CrossRef]
- Kato, R.; Kubota, M.; Yasui, Y.; Hayashi, Y.; Higashiyama, Y.; Nagai, A. Retrospective tracking of young obese children back to birth in Japan: Special attention to the relationship with parental obesity. Asia Pac. J. Clin. Nutr. 2014, 23, 641–650. [Google Scholar] [CrossRef]
- Dias, M.d.S.; Matijasevich, A.; Barros, A.J.D.; Menezes, A.M.B.; Schneider, B.C.; Hartwig, F.P.; Barros, F.C.; Wehrmeister, F.C.; Goncalves, H.; Santos, I.S.; et al. Influence of maternal pre-pregnancy nutritional status on offspring anthropometric measurements and body composition in three Brazilian Birth Cohorts. Public Health Nutr. 2021, 24, 882–894. [Google Scholar] [CrossRef]
- Castillo, H.; Santos, I.S.; Matijasevich, A. Relationship between maternal pre-pregnancy body mass index, gestational weight gain and childhood fatness at 6–7 years by air displacement plethysmography. Matern. Child Nutr. 2015, 11, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Andres, A.; Hull, H.R.; Shankar, K.; Casey, P.H.; Cleves, M.A.; Badger, T.M. Longitudinal body composition of children born to mothers with normal weight, overweight, and obesity. Obesity 2015, 23, 1252–1258. [Google Scholar] [CrossRef]
- Kjaer, T.W.; Faurholt-Jepsen, D.; Medrano, R.; Elwan, D.; Mehta, K.; Christensen, V.B.; Wojcicki, J.M. Higher Birthweight and Maternal Pre-pregnancy BMI Persist with Obesity Association at Age 9 in High Risk Latino Children. J. Immigr. Minor. Health 2019, 21, 89–97. [Google Scholar] [CrossRef]
- Xu, R.Y.; Zhou, Y.Q.; Zhang, X.M.; Wan, Y.P.; Gao, X. A two-year study of parental obesity status and childhood obesity in China. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 260–267. [Google Scholar] [CrossRef]
- Dhana, K.; Zong, G.; Yuan, C.; Schernhammer, E.; Zhang, C.; Wang, X.; Hu, F.B.; Chavarro, J.E.; Field, A.E.; Sun, Q. Lifestyle of women before pregnancy and the risk of offspring obesity during childhood through early adulthood. Int. J. Obes. 2018, 42, 1275–1284. [Google Scholar] [CrossRef]
- Vehapoglu, A.; Goknar, N.; Turel, O.; Torun, E.; Ozgurhan, G. Risk factors for childhood obesity: Do the birth weight, type of delivery, and mother’s overweight have an implication on current weight status? World J. Pediatr. 2017, 13, 457–464. [Google Scholar] [CrossRef]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Barker, D.J.P. In utero programming of chronic disease. Clin. Sci. 1998, 95, 115–128. [Google Scholar] [CrossRef]
- Marciniak, A.; Patro-Małysza, J.; Kimber-Trojnar, Ż.; Marciniak, B.; Oleszczuk, J.; Leszczyńska-Gorzelak, B. Fetal programming of the metabolic syndrome. Taiwan. J. Obstet. Gynecol. 2017, 56, 133–138. [Google Scholar] [CrossRef]
- Fernández-Barrés, S.; Romaguera, D.; Valvi, D.; Martínez, D.; Vioque, J.; Navarrete-Muñoz, E.M.; Amiano, P.; Gonzalez-Palacios, S.; Guxens, M.; Pereda, E.; et al. Mediterranean dietary pattern in pregnant women and offspring risk of overweight and abdominal obesity in early childhood: The INMA birth cohort study. Pediatr. Obes. 2016, 11, 491–499. [Google Scholar] [CrossRef]
- Campbell, M.K. Biological, environmental, and social influences on childhood obesity. Pediatr. Res. 2016, 79, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Güngör, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef]
- Weihrauch-Blüher, S.; Schwarz, P.; Klusmann, J.-H. Childhood obesity: Increased risk for cardiometabolic disease and cancer in adulthood. Metabolism 2019, 92, 147–152. [Google Scholar] [CrossRef]
- Baker, J.L.; Olsen, L.W.; Sørensen, T.I.A. Childhood Body-Mass Index and the Risk of Coronary Heart Disease in Adulthood. N. Engl. J. Med. 2007, 357, 2329–2337. [Google Scholar] [CrossRef]
- Juonala, M.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A.; Srinivasan, S.R.; Daniels, S.R.; Davis, P.H.; Chen, W.; et al. Childhood Adiposity, Adult Adiposity, and Cardiovascular Risk Factors. N. Engl. J. Med. 2011, 365, 1876–1885. [Google Scholar] [CrossRef]
- Tirosh, A.; Shai, I.; Afek, A.; Dubnov-Raz, G.; Ayalon, N.; Gordon, B.; Derazne, E.; Tzur, D.; Shamis, A.; Vinker, S.; et al. Adolescent BMI Trajectory and Risk of Diabetes versus Coronary Disease. N. Engl. J. Med. 2011, 364, 1315–1325. [Google Scholar] [CrossRef]
- Li, S.; Chen, W.; Srinivasan, S.R.; Xu, J.; Berenson, G.S. Relation of childhood obesity/cardiometabolic phenotypes to adult cardiometabolic profile: The Bogalusa Heart Study. Am. J. Epidemiol. 2012, 176 (Suppl. 7), S142–S149. [Google Scholar] [CrossRef]
- Song, J.W.; Chung, K.C. Observational studies: Cohort and case-control studies. Plast. Reconstr. Surg. 2010, 126, 2234–2242. [Google Scholar] [CrossRef]
- Lakshman, R.; Elks, C.E.; Ong, K.K. Childhood Obesity. Circulation 2012, 126, 1770–1779. [Google Scholar] [CrossRef]
- Zylke, J.W.; Bauchner, H. The Unrelenting Challenge of Obesity. JAMA 2016, 315, 2277–2278. [Google Scholar] [CrossRef]
- Williams, C.B.; Mackenzie, K.C.; Gahagan, S. The Effect of Maternal Obesity on the Offspring. Clin. Obstet. Gynecol. 2014, 57, 508–515. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year, Study Type, Location | Sample | Maternal Exposure Timepoint | Child Outcomes | Methodology | Results | Quality | |||
|---|---|---|---|---|---|---|---|---|---|
| n | Age (Y) | Life-Cycle Time Point | Weight Measures | Weight Measures | Statistical Method | Confounding Factors | Size of Effect | Risk of Bias [36] and Limitations | |
| Continuous Outcome Measures | |||||||||
| Xu et al. (2019). Prospective; China [48] | 2066 | 6–14 | During Childhood | OW/OB | BMI-Z (>90th%) %BF BMI(kg/m2) WC (cm) | PROC MIXED | Paternal and maternal education, parent’s obesity status and BMI | Child BMI-Z (>90th%) and M-WS Mean difference (95% CI) DC-OW 0.19 (0.06, 0.32), p ≤ 0.001 DC-OB 0.33 (0.09, 0.57), p ≤ 0.001 Child %BF (%) and M-WS DC-OW 0.38 (95% CI 0.16, 0.61), p = 0.001 DC-OB 0.41 (95% CI 0.01, 0.84), p = 0.001 Child BMI (kg/m2) and M-WS DC-OW 0.21 (95% CI 0.12, 0.29), p ≤ 0.001 DC-OB 0.29 (95% CI 0.13, 0.45), p ≤ 0.001 Child WC (cm) and M-WS DC-OW 0.57 (95% CI 0.32, 0.83), p ≤ 0.001 DC-OB 0.76 cm (95% CI 0.28, 1.25), p ≤ 0.001 |  NEUTRAL NEUTRAL
|
| Ehrenthal et al. (2013). Prospective; United States [40] | 3302 | 4 | Pre-pregnancy | OW OB VOB | BMI-Z | Bonferroni Post hoc estimation | Child’s age Maternal height | Child BMI-Z and M-WS β (95% CI) PP-OW 0.261 (0.169, 0.355) PP-OB 0.497 (0.382, 0.611) PP-VOB 0.755 (0.636, 0.874) p ≤ 0.001 |  POSITIVE POSITIVE
|
| Dias et al. (2021). Prospective; Brazil [44] | 3467 | 10.9 (0.3 SD) | Pre-pregnancy | UW NW OW OB | BMI-Z WC (cm) %FMI | Linear regression | Family income at birth, maternal age, parity, maternal schooling, and maternal smoking during pregnancy. | Child BMI-Z and M-WS β (95% CI) PP-OW 0.33, (0.22, 0.45) PP-OB 0.83, (0.64, 1.01) Child WC (CM) and M-WS β (95%CI) PP-OW 3.21, (2.07, 4.34) PP-OB 6.95, (5.17, 8.72) Child %FMI and M-WS β (95% CI) PP-OW 3.83, (2.56, 5.11) PP-OB 6.84, (4.82, 8.87) | NEUTRAL
|
| Daraki et al. (2015). Prospective; Greece [42] | 879 | 5 | Pre-pregnancy | OW/OB (BMI > 25 kg/m2) | BMI WC (cm) WC (%) | Poisson and Linear regression | Child sex, height & TV watching at 4 Y; Maternal age, education, parity, smoking during pregnancy, gestational weight gain, birth weight, breast-feeding duration | Child BMI and M-WS β (95% CI) (model 3) PP-OW/OB 0.79 (0.36, 1.06) Child WC % and M-WS RR (95% CI) (model 3) PP-OW/OB 1.97 (1.11, 3.49) Child WC (cm) and M-WS β (95% CI) (model 3) PP-OW/OB 1.36 (0.55, 2.17) | POSITIVE
|
| Castillo et al. (2015). Prospective; Brazil [45] | 3156 | 6 | Pre-pregnancy | NW OW OB (BMI) | FM (kg) FMI %BF | Linear regression | Family income, Maternal Schooling, skin colour, age, parity, pre-gestational arterial hypertension, pre-gestational diabetes, Pp-BMI | Child FM (KG) and M-WS N, Mean (SD) PP-NW 1914, 5.9 (3.2) PP-OW 751, 6.9 (4.0) PP-OB 352, 8.0 (5.2) p ≤ 0.001 Child FMI and M-WS N, Mean (SD) PP-NW 1890, 4.0 (2.0) PP-OW 747, 4.5 (2.4) PP-OB 349, 5.3 (3.0) p ≤ 0.001 Child %BF and M-WS N, Mean (SD) PP-NW 1914, 23.0 (5.6) PP-OW 751, 24.7 (8.4) PP-OB 352, 26.8 (9.5) p ≤ 0.001 | POSITIVE
|
| Andres et al. (2015). Prospective United States [46] | 325 | 3–6 | Pre-pregnancy | NW OW OB | BMI-Z %BF | Linear or restricted cubic splines | Race, gestational age, birth weight, mode of infant feeding | Child BMI-Z (5&6 Y) (Daughter) and M-WS PP-OW/OB Higher Scores, compared girls of NW Mothers, p ≤ 0.05 Child BMI-Z (3–6 Y) (Son) and M-WS PP-O Higher Scores compared to boys of OW or NW Mothers, p ≤ 0.05 Child %BF (2–6 Y) (Daughter) and M-WS PP-OB Higher %BF by 1.52% from, compared to girls from NW Mothers, p ≤ 0.05. Child %BF (2 Y) (Son) and M-WS PP-OB Higher %BF by 6 Y, by 4.8%, compared to boys from OW and NW Mothers (0.9%), p ≤ 0.05. | POSITIVE
|
| Categorical Outcome Measures | |||||||||
| Dhana et al. (2018). Prospective; United States [49] | 5701 | 9–14 | Pre-pregnancy | OW (25–29.9 kg/m2) OB (BMI > 30 kg/m2) | WS OB | Multivariable log-binominal regression models with generalised estimating equations | Mothers, age at birth, race/ethnicity, parity, pre-pregnancy alcohol intake, educational attainment of spouse/partner | Child OB and M-WS RR (95%CI) PP-OW 2.83 (2.35, 3.42) Child OB and M-WS RR (95%CI) PP-OB 4.15 (3.36, 5.13) | POSITIVE
|
| Zafar Janjua et al. (2012). Prospective; Greece [41] | 740 | 5 | Pre-pregnancy | LW&NW OW OB (BMI) | WS OB (>90th%) | Log binomial regression, Poisson regression with robust variance estimation | Mothers age, race, years of schooling, total number children in family, total number adults in home, employment status of mother, financial assistance, smoking status | Childhood OB and M-WS RR (95%CI) PP-OW 2.30 (1.29, 4.11), p = 0.005 Childhood OB and M-WS RR (95%CI) PP-OB 2.53 (1.49, 4.31), p ≤ 0.001; Normal ARR 1.00 | POSITIVE
|
| Kjaer et al. (2019). Prospective; United States [47] | 201 | 5–9 | Pre-pregnancy & During Childhood | OB BMI | OB | Multivariable logistic regression | Nil | Child OB (9 Y) and M-WS OR (95%CI) PP-OB 1.09 (1.00, 1.18), p = 0.04 Child OB compared to non-obese (9 Y) and M-WS (4 Y Postpartum) N/total [%]) DC-OB 25/48 [52%] vs. 24/82 [29%], p = 0.01 Child OB compared to non-obese (9 Y) and M-WS (4 Y Postpartum) N/total [%]) DC-OB 24/41 [59%] vs. 20/74 [27%], p = 0.03 Child OB compared to non-obese (9 Y) and M-WS (5 Y Postpartum) N/total [%]) DC-OB 21/44 [48%] vs. 19/69 [28%], p = 0.03 Child OB compared to non-obese (9 Y) and M-WS N/total [%]) PP-OB 17/53 [32%] vs. 10/90 [11%], p = 0.002 | NEUTRAL
|
| Vehapoglu et al. (2017). Retrospective; Turkey [50] | 4990 | 2–14 | During Childhood | NW OB (BMI > 30.0 kg/m2) | BMI OB | Multiple binary logistic regression | Model 2: Child age, gender, Mode of delivery, Breastfeeding duration, Timing of solid foods initiation Model 3: Maternal education level, smoking during pregnancy. | Child OB and M-WS OR (95%) (Model 2) DC-OB 3.91 (2.02–5.93) Child OB and M-WS OR (95%) (Model 3) DC-OB 3.84 (1.92–5.88) | POSITIVE
|
| Kato et al. (2014). Retrospective; Japan [43] | 2678 | 5 | During childhood | OB (BMI > 25 kg/m2) | WS OB (BMI > 90th%) | Chi-square test and Cochran-Armitage test | Nil | Child OB and M-WS (Total) OR (95%CI) DC-OB 2.14 (1.19, 3.86), p ≤ 0.01; AR = 5.8 Child (Daughter) OB and M-WS OR (95%CI) DC-OB 3.11 (1.54, 6.27), p ≤ 0.001; AR = 9.8 Child (Son) OB and M-WS OR (95%CI) DC-OB 1.01 (0.31, 3.35), p = 0.99; AR = 0.1 | NEUTRAL
|
, Overall Positive Risk of Bias Score, If most of the answers to the above validity questions are “Yes” (including criteria 2, 3, 6, 7 and at least one additional “Yes”; , Neutral Risk of Bias Score, If the answers to validity criteria questions 2, 3, 6, and 7 do not indicate that the study is exceptionally strong [36].| Zafar Janjua et al. (2012) [41] | Xu et al. (2019) [48] | Vehapoglu et al. (2017) [50] | Kjaer et al. (2019) [47] | Kato et al. (2014) [43] | Ehrenthal et al. (2013) [40] | Dias et al. (2021) [44] | Dhana et al. (2018) [49] | Daraki et al. (2015) [42] | Castillo et al. (2015) [45] | Andres et al. (2015) [46] | ||
| OVERALL RATING | | | | | | | | | | | | |
| RELEVANCE QUESTIONS | ||||||||||||
| 1 | Would implementing the studied intervention or procedure (if found successful) result in improved outcomes for the patients/clients/population group? (NA for some epidemiological studies) |  | | | | | | | | | | |
| 2 | Did the authors study an outcome (dependent variable) or topic that the patients/clients/population group would care about? |  | | | | | | | | | | |
| 3 | Is the focus of the intervention or procedure (independent variable) or topic of study a common issue of concern to dietetics practice? | | | | | | | | | | | |
| 4 | Is the intervention or procedure feasible? (NA for some epidemiological studies) | | | | | | | | | | | |
| VALIDITY QUESTIONS | ||||||||||||
| 1 | Was the research question clearly stated? | | | | | | | |  | | | |
| 2 | Was the selection of study subjects/patients free from bias? | |  | | | | | | | | | |
| 3 | Were study groups comparable? | | | | | | | | | | | |
| 4 | Was method of handling withdrawals described? | | | | | | | | | | | |
| 5 | Was blinding used to prevent introduction of bias? | | | | | | | | | | | |
| 6 | Were intervention/therapeutic regimens/exposure factor or procedure and any comparison(s) described in detail? Were intervening factors described? | | | | | | | | | | | |
| 7 | Were outcomes clearly defined and the measurements valid and reliable? | | | | | | | | | | | |
| 8 | Was the statistical analysis appropriate for the study design and type of outcome indicators? | | | | | | | | | | | |
| 9 | Are conclusions supported by results with biases and limitations taken into consideration? | | | | | | | | | | | |
| 10 | Is bias due to study’s funding or sponsorship unlikely? | | | | | | | | | | | |
Overall Positive Risk of Bias Score, If most of the answers to the above validity questions are “Yes” (including criteria 2, 3, 6, 7 and at least one additional “Yes”; Neutral Risk of Bias Score, If the answers to validity criteria questions 2, 3, 6, and 7 do not indicate that the study is exceptionally strong; not applicable; Yes; No; Unclear [36].Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannino, A.; Sarapis, K.; Moschonis, G. The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review. Nutrients 2022, 14, 5125. https://doi.org/10.3390/nu14235125
Mannino A, Sarapis K, Moschonis G. The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review. Nutrients. 2022; 14(23):5125. https://doi.org/10.3390/nu14235125
Chicago/Turabian StyleMannino, Adriana, Katerina Sarapis, and George Moschonis. 2022. "The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review" Nutrients 14, no. 23: 5125. https://doi.org/10.3390/nu14235125
APA StyleMannino, A., Sarapis, K., & Moschonis, G. (2022). The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review. Nutrients, 14(23), 5125. https://doi.org/10.3390/nu14235125