
Effect of Rice (Oryza sativa L.) Ceramides Supplementation on Improving Skin Barrier Functions and Depigmentation: An Open-Label Prospective Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
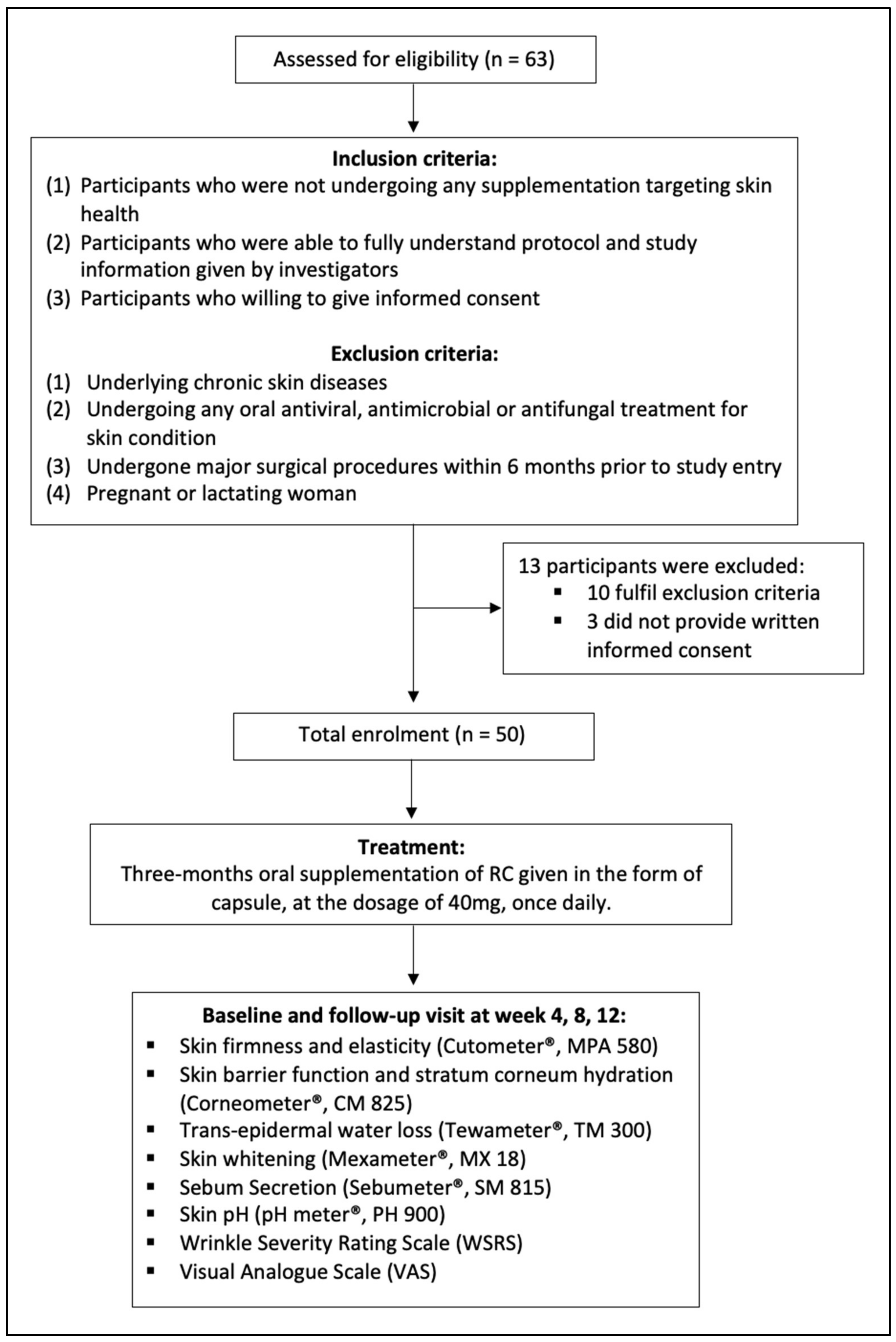
2.1. Study Design
2.2. Participants Selection
2.3. Supplementation
2.4. Skin Biophysical Measurements
2.5. Wrinkle Severity Rating Scale (WSRS)
2.6. Visual Analogue Scale (VAS)
2.7. Statistical Analysis
3. Results
3.1. Characteristics of Participant
3.2. Changes in Skin Barrier Function
3.3. Changes in Skin Firmness and Elasticity
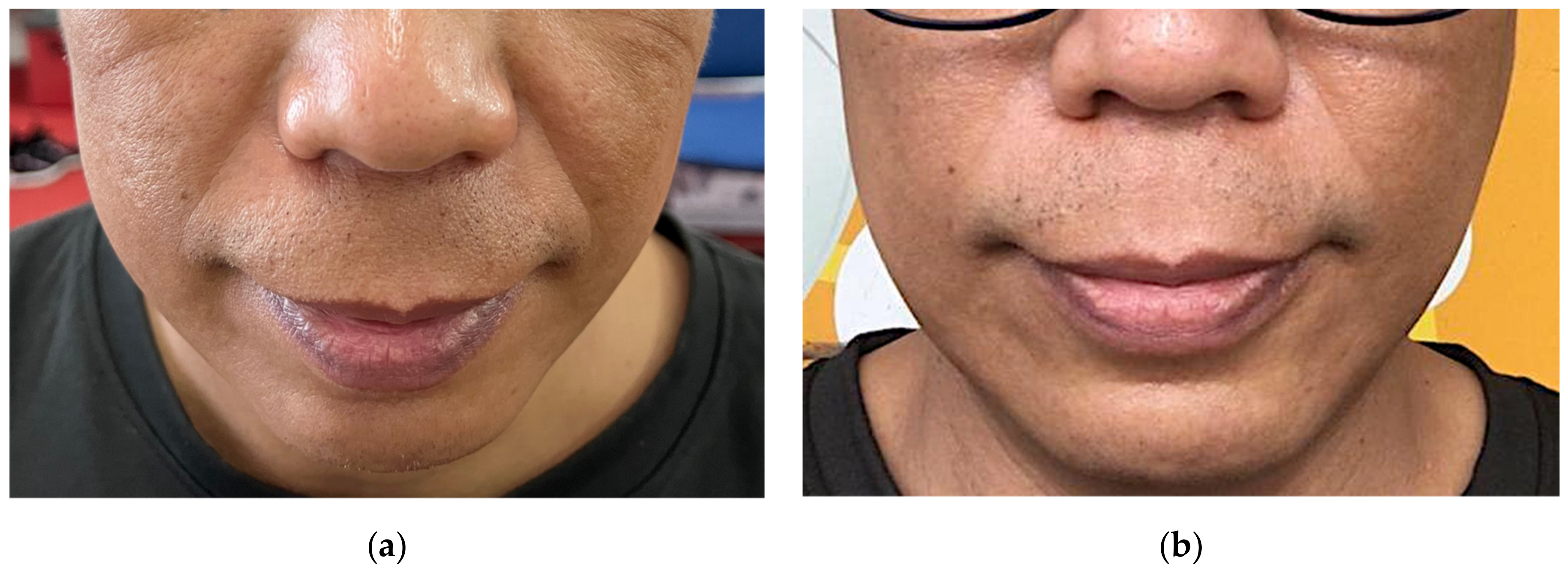
3.4. Changes in Skin Pigmentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weerheim, A.; Ponec, M. Determination of stratum corneum lipid profile by tape stripping in combination with high-performance thin-layer chromatography. Arch. Dermatol. Res. 2001, 293, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, E.; Kaykın, M.; Bektay, H.Ş.; Güngör, S. Recent Advances on Topical Application of Ceramides to Restore Barrier Function of Skin. Cosmetics 2019, 6, 52. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Fang, H.; Dang, E.; Wang, G. The role of ceramides in skin homeostasis and inflammatory skin diseases. J. Dermatol. Sci. 2019, 97, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Man, M.-Q.; Li, T.; Elias, P.M.; Mauro, T.M. Aging-associated alterations in epidermal function and their clinical signifi-cance. Aging 2020, 12, 5551–5565. [Google Scholar] [CrossRef]
- Agrawal, K.; Hassoun, L.A.; Foolad, N.; Borkowski, K.; Pedersen, T.L.; Sivamani, R.K.; Newman, J.W. Effects of atopic dermatitis and gender on sebum lipid mediator and fatty acid profiles. Prostaglandins Leukot. Essent. Fat. Acids 2018, 134, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Shamloul, N.; Hashim, P.W.; Nia, J.J.; Farberg, A.S.; Goldenberg, G. The role of vitamins and supplements on skin appearance. Cutis 2019, 104, 220–224. [Google Scholar]
- Maarouf, M.; Maarouf, C.; Yosipovitch, G.; Shi, V. The impact of stress on epidermal barrier function: An evidence-based review. Br. J. Dermatol. 2019, 181, 1129–1137. [Google Scholar] [CrossRef]
- Fujii, M. The Pathogenic and Therapeutic Implications of Ceramide Abnormalities in Atopic Dermatitis. Cells 2021, 10, 2386. [Google Scholar] [CrossRef]
- Ishida, K.; Takahashi, A.; Bito, K.; Draelos, Z.; Imokawa, G. Treatment with Synthetic Pseudoceramide Improves Atopic Skin, Switching the Ceramide Profile to a Healthy Skin Phenotype. J. Investig. Dermatol. 2020, 140, 1762–1770.e8. [Google Scholar] [CrossRef]
- Carrié, L.; Virazels, M.; Dufau, C.; Montfort, A.; Levade, T.; Ségui, B.; Andrieu-Abadie, N. New Insights into the Role of Sphingolipid Metabolism in Melanoma. Cells 2020, 9, 1967. [Google Scholar] [CrossRef]
- Nguyen, J.K.; Masub, N.; Jagdeo, J. Bioactive ingredients in Korean cosmeceuticals: Trends and research evidence. J. Cosmet. Dermatol. 2020, 19, 1555–1569. [Google Scholar] [CrossRef] [PubMed]
- Tessema, E.N.; Gebre-Mariam, T.; Neubert, R.H.; Wohlrab, J. Potential Applications of Phyto-Derived Ceramides in Improving Epidermal Barrier Function. Ski. Pharmacol. Physiol. 2017, 30, 115–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heggar Venkataramana, S.; Puttaswamy, N.; Kodimule, S. Potential benefits of oral administration of AMORPHOPHALLUS KONJAC glycosylceramides on skin health—A randomized clinical study. BMC Complement. Med. Ther. 2020, 20, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokudome, Y.; Masutani, N.; Uchino, S.; Fukai, H. Recovery Effects of Oral Administration of Glucosylceramide and Beet Extract on Skin Barrier Destruction by UVB in Hairless Mice. Nutrients 2017, 9, 1178. [Google Scholar] [CrossRef] [Green Version]
- Son, D.J.; Jung, J.C.; Choi, Y.M.; Ryu, H.Y.; Lee, S.; Davis, B.A. Wheat Extract Oil (WEO) Attenuates UVB-Induced Photoaging via Collagen Synthesis in Human Keratinocytes and Hairless Mice. Nutrients 2020, 12, 300. [Google Scholar] [CrossRef] [Green Version]
- Kagotani, K.; Nakayama, H.; Zang, L.; Fujimoto, Y.; Hayashi, A.; Sono, R.; Nishimura, N.; Shimada, Y. Lecithin-Based Dermal Drug Delivery for Anti-Pigmentation Maize Ceramide. Molecules 2020, 25, 1595. [Google Scholar] [CrossRef] [Green Version]
- McGraw, M.J.; George, A.N.; Shearn, S.P.; Hall, R.L.; Haws, T.F. Principles of Good Clinical Practice; Pharmaceutical Press: London, UK, 2010. [Google Scholar]
- Lim, S.H.; Kim, S.M.; Lee, Y.W.; Ahn, K.J.; Choe, Y.B. Change of biophysical properties of the skin caused by ultraviolet radia-tion-induced photodamage in Koreans. Ski. Res. Technol. 2008, 14, 93–102. [Google Scholar]
- Day, D.J.; Littler, C.M.; Swift, R.W.; Gottlieb, S. The wrinkle severity rating scale. Am. J. Clin. Dermatol. 2004, 5, 49–52. [Google Scholar] [CrossRef]
- Klimek, L.; Bergmann, K.-C.; Biedermann, T.; Bousquet, J.; Hellings, P.; Jung, K.; Merk, H.; Olze, H.; Schlenter, W.; Stock, P.; et al. Visual analogue scales (VAS): Measuring in-struments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care. Allergo J. Int. 2017, 26, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Krutmann, J.; Liu, W.; Li, L.; Pan, X.; Crawford, M.; Sore, G.; Seite, S. Pollution and skin: From epidemiological and mechanistic studies to clinical implications. J. Dermatol. Sci. 2014, 76, 163–168. [Google Scholar] [CrossRef]
- Fatin, A.M.; Mathana Sundram, T.K.; Tan, S.S.E.; Seghayat, M.S.; Lee, C.K.; Rehman, N.; Tan, C.K. Classification and characteristics of pe-riorbital hyperpigmentation. Ski. Res. Technol. 2020, 26, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Suppiah, T.S.S.; Sundram, T.K.M.; Tan, E.S.S.; Lee, C.K.; Bustami, N.A.; Tan, C.K. Acne vulgaris and its association with dietary intake: A Malaysian perspective. Asia Pac. J. Clin. Nutr. 2018, 27, 1141–1145. [Google Scholar] [PubMed]
- Plikus, M.V.; Van Spyk, E.N.; Pham, K.; Geyfman, M.; Kumar, V.; Takahashi, J.S.; Andersen, B. The circadian clock in skin: Implications for adult stem cells, tissue regeneration, cancer, aging, and immunity. J. Biol. Rhythms 2015, 30, 163–182. [Google Scholar] [CrossRef] [Green Version]
- De Assis, L.V.M.; Tonolli, P.N.; Moraes, M.N.; Baptista, M.S.; de Lauro Castrucci, A.M. How does the skin sense sun light? An integrative view of light sensing molecules. J. Photochem. Photobiol. C Photochem. Rev. 2021, 47, 100403. [Google Scholar] [CrossRef]
- Narla, S.; Kohli, I.; Hamzavi, I.H.; Lim, H.W. Visible light in photodermatology. Photochem. Photobiol. Sci. 2020, 19, 99–104. [Google Scholar] [CrossRef]
- Chauhan, A.; Gretz, N. Role of Visible Light on Skin Melanocytes: A Systematic Review. Photochem. Photobiol. 2021, 97, 911–915. [Google Scholar] [CrossRef]
- Bonté, F.; Girard, D.; Archambault, J.-C.; Desmoulière, A. Skin changes during ageing. In Biochemistry and Cell Biology of Ageing: Part II Clinical Science; Springer Nature: Singapore; Gateway East: Singapore, 2019; pp. 249–280. [Google Scholar]
- Amini, F.; Thazin Oo, N.M.; Okechukwu, P.N.; Seghayat, M.S.; Ng, E.S.C. Polymorphisms in P53 and VEGFA genes in different sub-types of periorbital hyperpigmentation in a Malaysian Chinese population. Australas. J. Dermatol. 2019, 60, e99–e104. [Google Scholar] [CrossRef]
- Tan, E.S.S.; Leo, T.K.; Tan, C.K. Effect of tiger milk mushroom (Lignosus rhinocerus) supplementation on respiratory health, immunity and antioxidant status: An open-label prospective study. Sci. Rep. 2021, 11, 11781. [Google Scholar] [CrossRef]
- Amparo, T.R.; Seibert, J.B.; Vieira, P.M.D.A.; Teixeira, L.F.M.; Santos, O.D.H.D.; de Souza, G.H.B. Herbal medicines to the treatment of skin and soft tissue infections: Advantages of the multi-targets action. Phytother. Res. 2020, 34, 94–103. [Google Scholar] [CrossRef]
- Yeom, M.; Kim, S.H.; Lee, B.; Han, J.J.; Chung, G.H.; Choi, H.D.; Lee, H.; Hahm, D.-H. Oral administration of glucosylceramide ameliorates inflamma-tory dry-skin condition in chronic oxazolone-induced irritant contact dermatitis in the mouse ear. J. Dermatol. Sci. 2012, 67, 101–110. [Google Scholar] [CrossRef]
- Oyewole, A.; Birch-Machin, M.A. Sebum, inflammasomes and the skin: Current concepts and future perspective. Exp. Dermatol. 2015, 24, 651–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drakou, K.; Tsianni, A.; Vrani, F.; Kefala, V.; Rallis, E. Revealing the Correlation between Altered Skin Lipids Composition and Skin Disorders. Cosmetics 2021, 8, 88. [Google Scholar] [CrossRef]
- Sowell, J.; Pena, S.M.; Elewski, B.E. Seborrheic Dermatitis in Older Adults: Pathogenesis and Treatment Options. Drugs Aging 2022, 39, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.; Schiavi, M.; Seidenari, S. Capacitance, transepidermal water loss and causal level of sebum in healthy subjects in relation to site, sex and age. Int. J. Cosmet. Sci. 1995, 17, 77–85. [Google Scholar] [CrossRef]
- Khazaka, C. Sebumeter: Information and Operating Instructions for the Multi Probe Adapter MPA and Its Probes; Courage+Khazaka Electronic GmbH: Cologne, Germany, 2004. [Google Scholar]
- Luebberding, S.; Krueger, N.; Kerscher, M. Age-related changes in skin barrier function—Quantitative evaluation of 150 female subjects. Int. J. Cosmet. Sci. 2012, 35, 183–190. [Google Scholar] [CrossRef]
- Ludovici, M.; Kozul, N.; Materazzi, S.; Risoluti, R.; Picardo, M.; Camera, E. Influence of the sebaceous gland density on the stratum corneum lipidome. Sci. Rep. 2018, 8, 11500. [Google Scholar] [CrossRef]
- Uchida, Y.; Park, K. Ceramides in Skin Health and Disease: An Update. Am. J. Clin. Dermatol. 2021, 22, 853–866. [Google Scholar] [CrossRef]
- Verdier-Sévrain, S.; Bonté, F. Skin hydration: A review on its molecular mechanisms. J. Cosmet. Dermatol. 2007, 6, 75–82. [Google Scholar] [CrossRef]
- Jansen van Rensburg, S.; Franken, A.; Du Plessis, J.L. Measurement of transepidermal water loss, stratum corneum hydration and skin surface pH in occupational settings: A review. Ski. Res. Technol. 2019, 25, 595–605. [Google Scholar] [CrossRef] [Green Version]
- Rahrovan, S.; Fanian, F.; Mehryan, P.; Humbert, P.; Firooz, A. Male versus female skin: What dermatologists and cosmeticians should know. Int. J. Women’s Dermatol. 2018, 4, 122–130. [Google Scholar] [CrossRef]
- Nam, G.; Baek, J.H.; Koh, J.S.; Hwang, J.-K. The seasonal variation in skin hydration, sebum, scaliness, brightness and elasticity in Korean females. Ski. Res. Technol. 2014, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sahle, F.F.; Gebre-Mariam, T.; Dobner, B.; Wohlrab, J.; Neubert, R.H. Skin Diseases Associated with the Depletion of Stratum Corneum Lipids and Stratum Corneum Lipid Substitution Therapy. Ski. Pharmacol. Physiol. 2014, 28, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Hiranuma, T.; Watanabe, K.; Yamashita, T.; Okazaki, T.; Tokudome, Y. Role of collagen degradation pathway in sphingomyelin synthase 2-deficient mouse skin. Biomed. Dermatol. 2021, 5, 1. [Google Scholar] [CrossRef]
- Summers, S.A.; Chaurasia, B.; Holland, W.L. Metabolic Messengers: Ceramides. Nat. Metab. 2019, 1, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.-S.; Kim, S.-Y.; Chung, J.-H.; Kim, K.-H.; Eun, H.-C.; Park, K.-C. Delayed ERK activation by ceramide reduces melanin synthesis in human melanocytes. Cell. Signal. 2002, 14, 779–785. [Google Scholar] [CrossRef]
- Kim, D.-S.; Kim, S.-Y.; Moon, S.-J.; Chung, J.-H.; Kim, K.-H.; Cho, K.-H.; Park, K.-C. Ceramide Inhibits Cell Proliferation through Akt/PKB Inactivation and Decreases Melanin Synthesis in Mel-Ab Cells. Pigment Cell Res. 2001, 14, 110–115. [Google Scholar] [CrossRef]
- Ando, H.; Kondoh, H.; Ichihashi, M.; Hearing, V.J. Approaches to identify inhibitors of melanin biosynthesis via the quality control of tyrosinase. J. Investig. Dermatol. 2007, 127, 751–761. [Google Scholar] [CrossRef] [Green Version]
- Jang, Y.-S.; Kang, Y.-J.; Kim, T.-J.; Bae, K. Temporal expression profiles of ceramide and ceramide-related genes in wild-type and mPer1/mPer2 double knockout mice. Mol. Biol. Rep. 2012, 39, 4215–4221. [Google Scholar] [CrossRef]
- De Assis, L.V.M.; Moraes, M.N.; Castrucci, A.M.D.L. The molecular clock in the skin, its functionality, and how it is disrupted in cutaneous melanoma: A new pharmacological target? Cell. Mol. Life Sci. 2019, 76, 3801–3826. [Google Scholar] [CrossRef]
- Reuben, U.; Ismail, A.F.; Ahmad, A.L.; Maina, H.M.; Daud, A. Occupational and environmental risk factors influencing the in-ducement of erythema among nigerian laboratory university workers with multiple chemical exposures. Int. J. Environ. Res. Public Health 2019, 16, 1334. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Kim, S.; Yun, H.S.; Kwon, S. Anti-inflammatory effect of the ceramide mixture extracted from genetically modified Saccharomyces cerevisiae. Biotechnol. Bioprocess Eng. 2017, 22, 653–658. [Google Scholar] [CrossRef]
- Takeda, S.; Miyasaka, K.; Shrestha, S.; Manse, Y.; Morikawa, T.; Shimoda, H. Lycoperoside H, a Tomato Seed Saponin, Improves Epidermal Dehydration by Increasing Ceramide in the Stratum Corneum and Steroidal Anti-Inflammatory Effect. Molecules 2021, 26, 5860. [Google Scholar] [CrossRef] [PubMed]
- Richters, R.; Falcone, D.; Uzunbajakava, N.; Verkruysse, W.; van Erp, P.; van de Kerkhof, P. What Is Sensitive Skin? A Systematic Literature Review of Objective Measurements. Ski. Pharmacol. Physiol. 2014, 28, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Kida, N.; Sokabe, T.; Kashio, M.; Haruna, K.; Mizuno, Y.; Suga, Y.; Nishikawa, K.; Kanamaru, A.; Hongo, M.; Oba, A.; et al. Importance of transient receptor potential vanilloid 4 (TRPV4) in epidermal barrier function in human skin keratinocytes. Pflügers Arch. Eur. J. Physiol. 2012, 463, 715–725. [Google Scholar] [CrossRef]
- Proksch, E.; Brandner, J.M.; Jensen, J.-M. The skin: An indispensable barrier. Exp. Dermatol. 2008, 17, 1063–1072. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Frequency (%) |
|---|---|
| Sex (n/%) Male Female | 17 (34.0) 33 (66.0) |
| Age (years) (n/%) 21–30 31–40 >40 | 17 (34.0) 17 (34.0) 16 (32.0) |
| Parameters | Baseline | First Follow-Up | Second Follow-Up | Third Follow-Up | ap-Value | bp-Value | cp-Value |
|---|---|---|---|---|---|---|---|
| TEWL (g/h/m2) | |||||||
| Cheek | 21.23 ± 5.01 | 14.20 ± 6.15 | 14.10 ± 6.59 | 13.39 ± 5.06 | <0.001 * | 0.652 | 0.185 |
| Neck | 18.38 ± 5.13 | 11.44 ± 2.47 | 10.50 ± 1.19 | 9.72 ± 2.23 | <0.001 * | 0.524 | 0.396 |
| Arm | 14.45 ± 5.51 | 9.59 ± 3.84 | 8.32 ± 3.18 | 8.79 ± 3.22 | <0.001 * | 0.677 | <0.05 * |
| Skin Hydration (AU) | |||||||
| Cheek | 61.10 ± 14.95 | 60.65 ± 14.50 | 66.53 ± 13.94 | 75.05 ± 14.80 | <0.001 * | 0.544 | 0.605 |
| Neck | 58.07 ± 16.40 | 57.78 ± 13.06 | 60.81 ± 14.42 | 67.56 ± 15.77 | <0.001 * | 0.475 | 0.096 |
| Arm | 38.96 ± 12.98 | 38.17 ± 10.35 | 45.25 ± 12.62 | 51.40 ± 13.97 | <0.001 * | 0.625 | 0.078 |
| Sebum Production (AU) | |||||||
| Cheek | 35.18 ± 10.33 | 51.6 ± 20.40 | 68.34 ± 19.21 | 75.74 ± 28.48 | <0.001 * | 0.425 | <0.01 * |
| Neck | 23.40 ± 5.69 | 37.54 ± 12.11 | 53.34 ± 22.83 | 66.36 ± 22.36 | <0.001 * | 0.935 | <0.05 * |
| Arm | 1.78 ± 0.45 | 3.00 ± 0.10 | 4.60 ± 0.21 | 5.68 ± 1.04 | <0.001 * | 0.23 | 0.316 |
| Skin pH | |||||||
| Cheek | 6.02 ± 0.34 | 6.09 ± 0.37 | 6.10 ± 0.44 | 6.01 ± 0.33 | 0.475 | 0.066 | 0.936 |
| Neck | 5.83 ± 0.29 | 5.86 ± 0.30 | 5.95 ± 0.38 | 5.89 ± 0.32 | 0.226 | 0.497 | 0.952 |
| Arm | 5.73 ± 0.33 | 5.77 ± 0.27 | 5.87 ± 0.35 | 5.79 ± 0.27 | 0.112 | 0.986 | 0.52 |
| VAS | 5.33 ± 1.27 | 5.81 ± 1.29 | 6.57 ± 1.40 | 7.08 ± 1.31 | <0.001 * | 0.41 | 0.776 |
| Parameters | Baseline | First Follow-Up | Second Follow-Up | Third Follow-Up | ap-Value | bp-Value | cp-Value |
|---|---|---|---|---|---|---|---|
| Skin Firmness and Elasticity (VEU) | |||||||
| Cheek | 0.562 ± 0.134 | 0.606 ± 0.116 | 0.610 ± 0.111 | 0.662 ± 0.131 | <0.001 * | 0.347 | 0.851 |
| Neck | 0.775 ± 0.065 | 0.782 ± 0.074 | 0.759 ± 0.092 | 0.829 ± 0.073 | <0.001 * | 0.741 | 0.938 |
| Arm | 0.785 ± 0.042 | 0.789 ± 0.060 | 0.795 ± 0.063 | 0.817 ± 0.056 | <0.01 * | 0.578 | 0.994 |
| WSRS | 1.92 ± 0.89 | 1.78 ± 0.88 | 1.70 ± 0.86 | 1.60 ± 0.78 | <0.01 * | 0.499 | 0.74 |
| Parameters | Baseline | First Follow-Up | Second Follow-Up | Third Follow-Up | ap-Value | bp-Value | cp-Value |
|---|---|---|---|---|---|---|---|
| Melanin Index (MI) (AU) | |||||||
| Cheek | 175.72 ± 60.86 | 171.77 ± 58.26 | 162.79 ± 60.24 | 152.58 ± 55.31 | <0.001 * | 0.325 | 0.093 |
| Neck | 137.50 ± 39.98 | 128.05 ± 48.19 | 126.53 ± 51.41 | 113.20 ± 43.96 | <0.001 * | 0.727 | 0.116 |
| Arm | 135.27 ± 46.34 | 131.07 ± 40.99 | 127.53 ± 39.27 | 114.74 ± 37.35 | <0.001 * | 0.163 | 0.09 |
| Erythema Index (EI) (AU) | |||||||
| Cheek | 329.80 ± 79.83 | 312.00 ± 87.18 | 301.46 ± 80.80 | 278.00 ± 82.49 | <0.001 * | 0.078 | 0.25 |
| Neck | 255.53 ± 70.95 | 246.35 ± 66.49 | 237.78 ± 64.30 | 216.76 ± 60.47 | <0.001 * | 0.184 | 0.096 |
| Arm | 196.22 ± 57.68 | 192.43 ± 52.72 | 182.94 ± 43.94 | 171.67 ± 51.69 | <0.001 * | 0.104 | 0.836 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leo, T.K.; Tan, E.S.S.; Amini, F.; Rehman, N.; Ng, E.S.C.; Tan, C.K. Effect of Rice (Oryza sativa L.) Ceramides Supplementation on Improving Skin Barrier Functions and Depigmentation: An Open-Label Prospective Study. Nutrients 2022, 14, 2737. https://doi.org/10.3390/nu14132737
Leo TK, Tan ESS, Amini F, Rehman N, Ng ESC, Tan CK. Effect of Rice (Oryza sativa L.) Ceramides Supplementation on Improving Skin Barrier Functions and Depigmentation: An Open-Label Prospective Study. Nutrients. 2022; 14(13):2737. https://doi.org/10.3390/nu14132737
Chicago/Turabian StyleLeo, Teik Kee, Eugenie Sin Sing Tan, Farahnaz Amini, Navedur Rehman, Edmond Siah Chye Ng, and Chung Keat Tan. 2022. "Effect of Rice (Oryza sativa L.) Ceramides Supplementation on Improving Skin Barrier Functions and Depigmentation: An Open-Label Prospective Study" Nutrients 14, no. 13: 2737. https://doi.org/10.3390/nu14132737