
Associations between Serum Betaine, Methyl-Metabolizing Genetic Polymorphisms and Risk of Incident Type 2 Diabetes: A Prospective Cohort Study in Community-Dwelling Chinese Adults

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
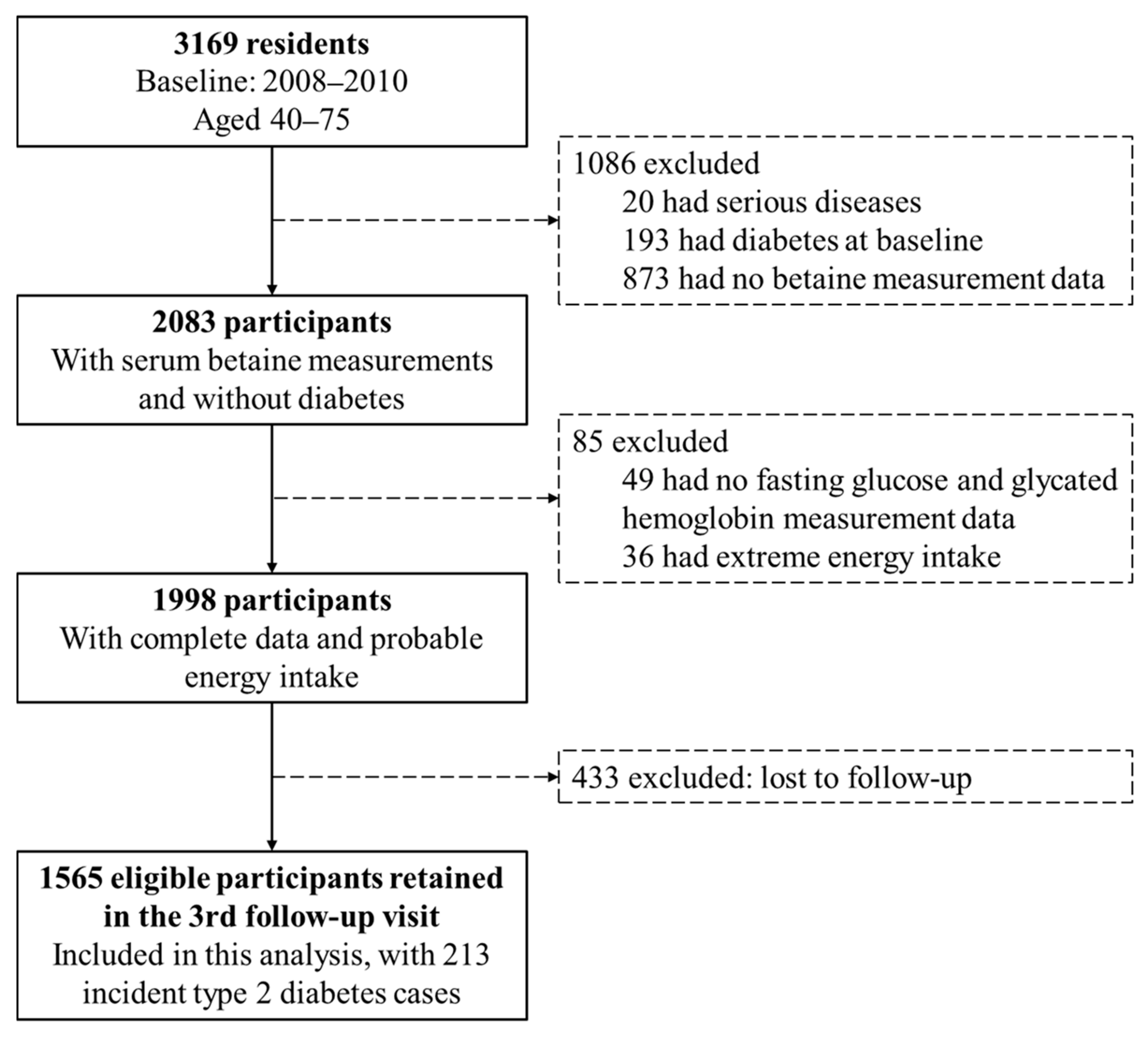
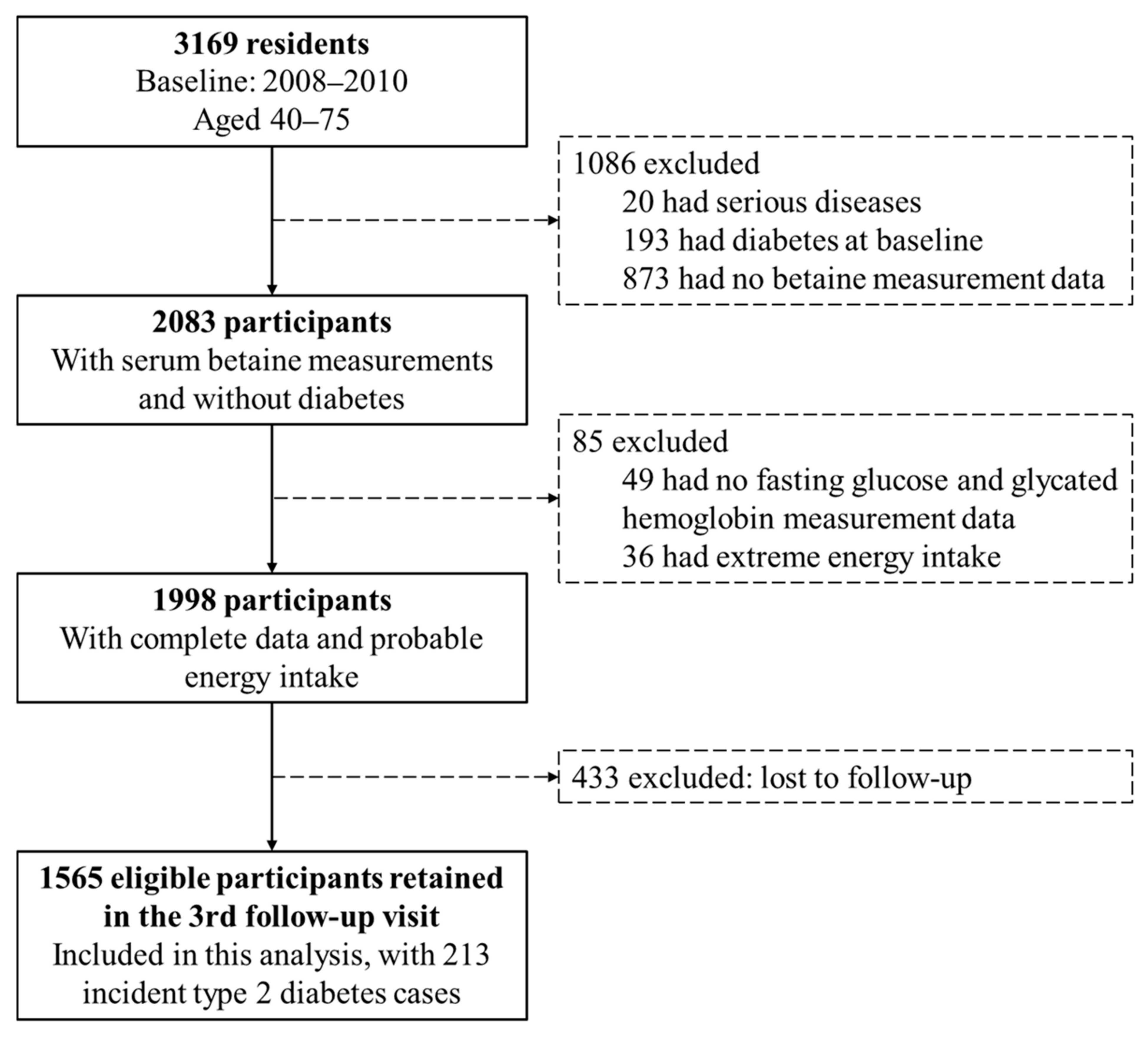
2.1. Design and Study Population
2.2. Measurement of Serum Betaine Concentrations
2.3. DNA Extraction, Genotyping and SNP Selection
2.4. Covariates Data Collection
2.5. Study Outcomes
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics of Study Participants
3.2. Serum Betaine and Risk of Incident Type 2 Diabetes
3.3. Methyl-Metabolizing Enzymes Genetic Polymorphisms and Incident of Type 2 Diabetes
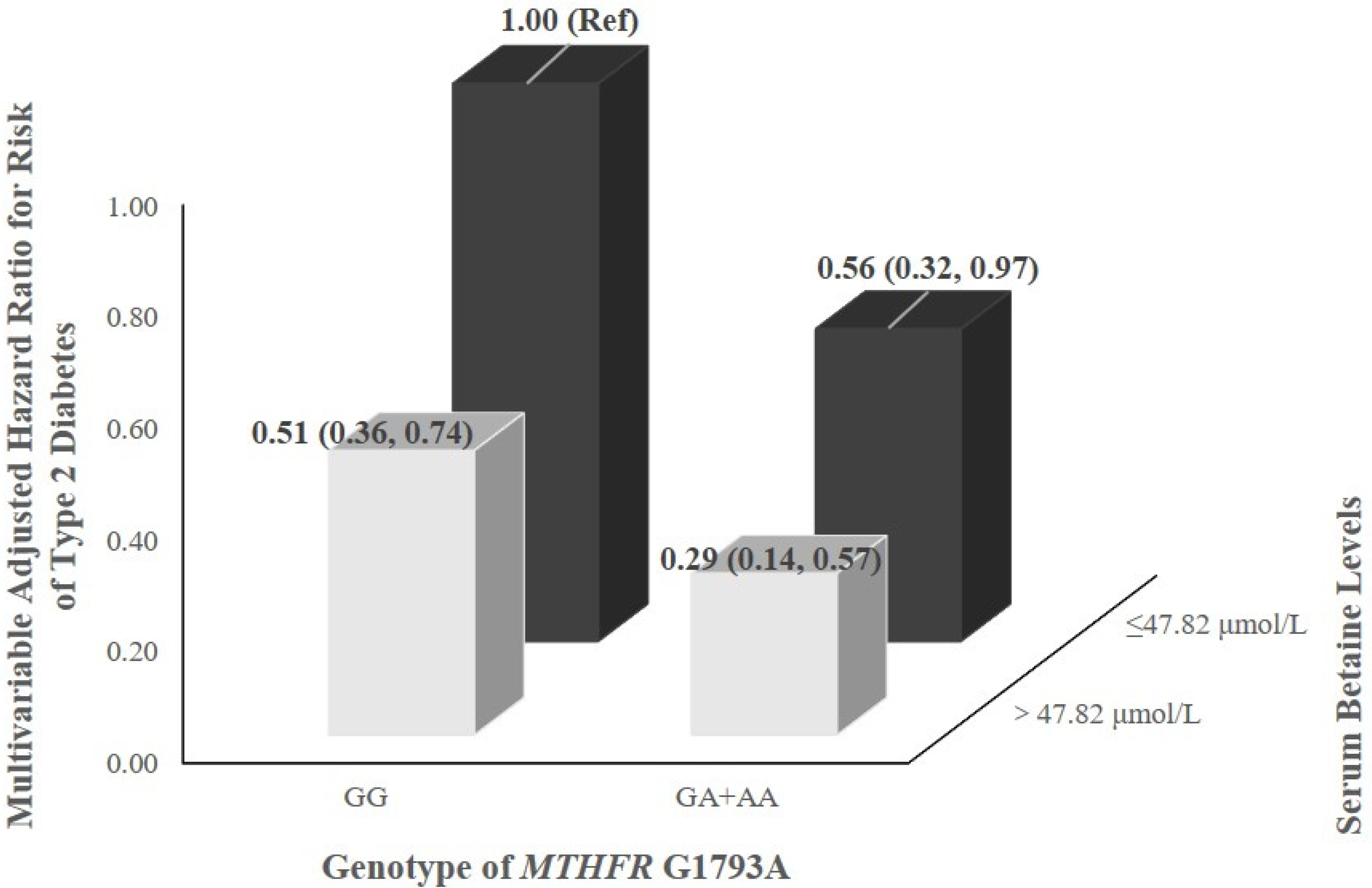
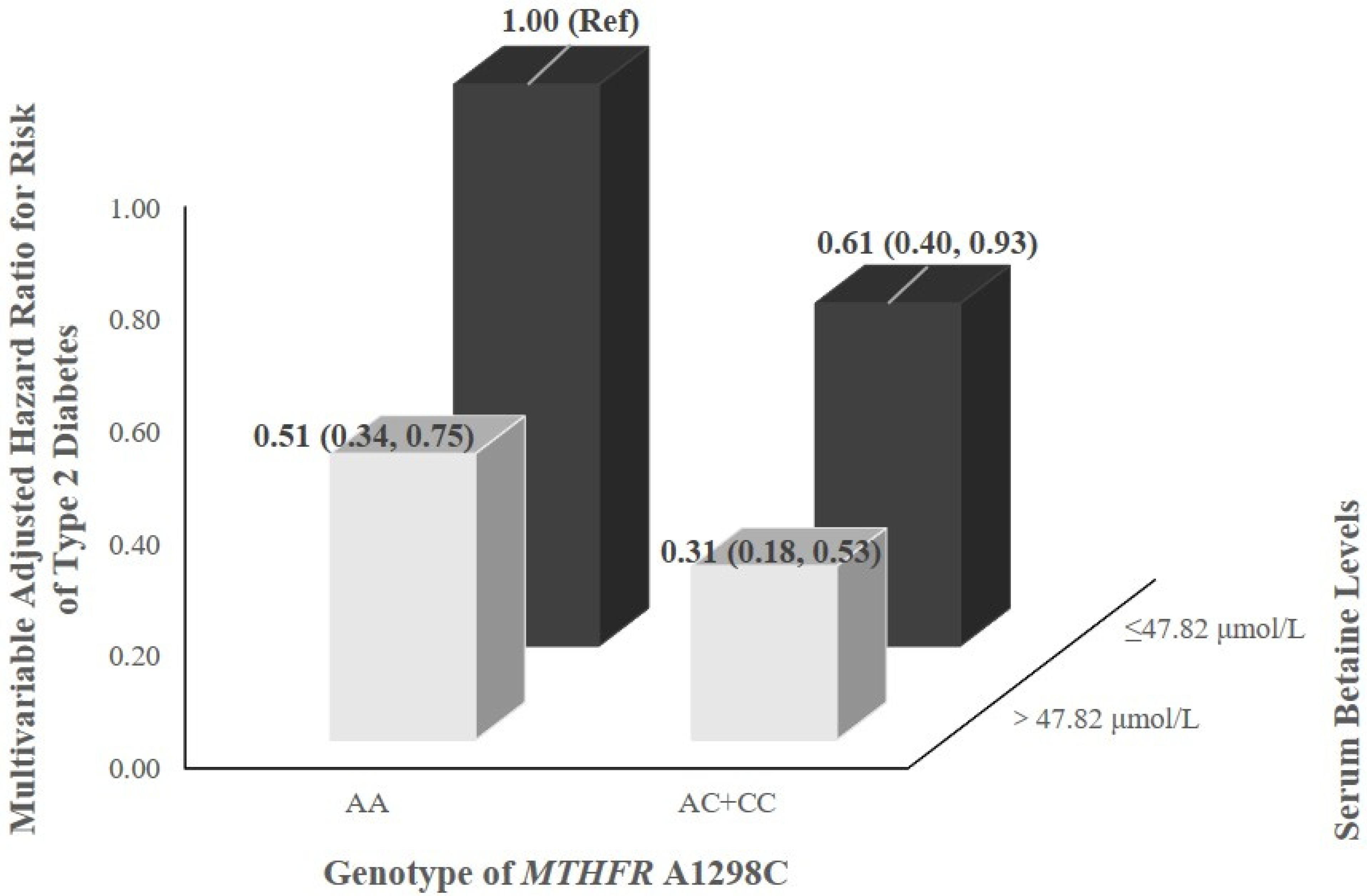
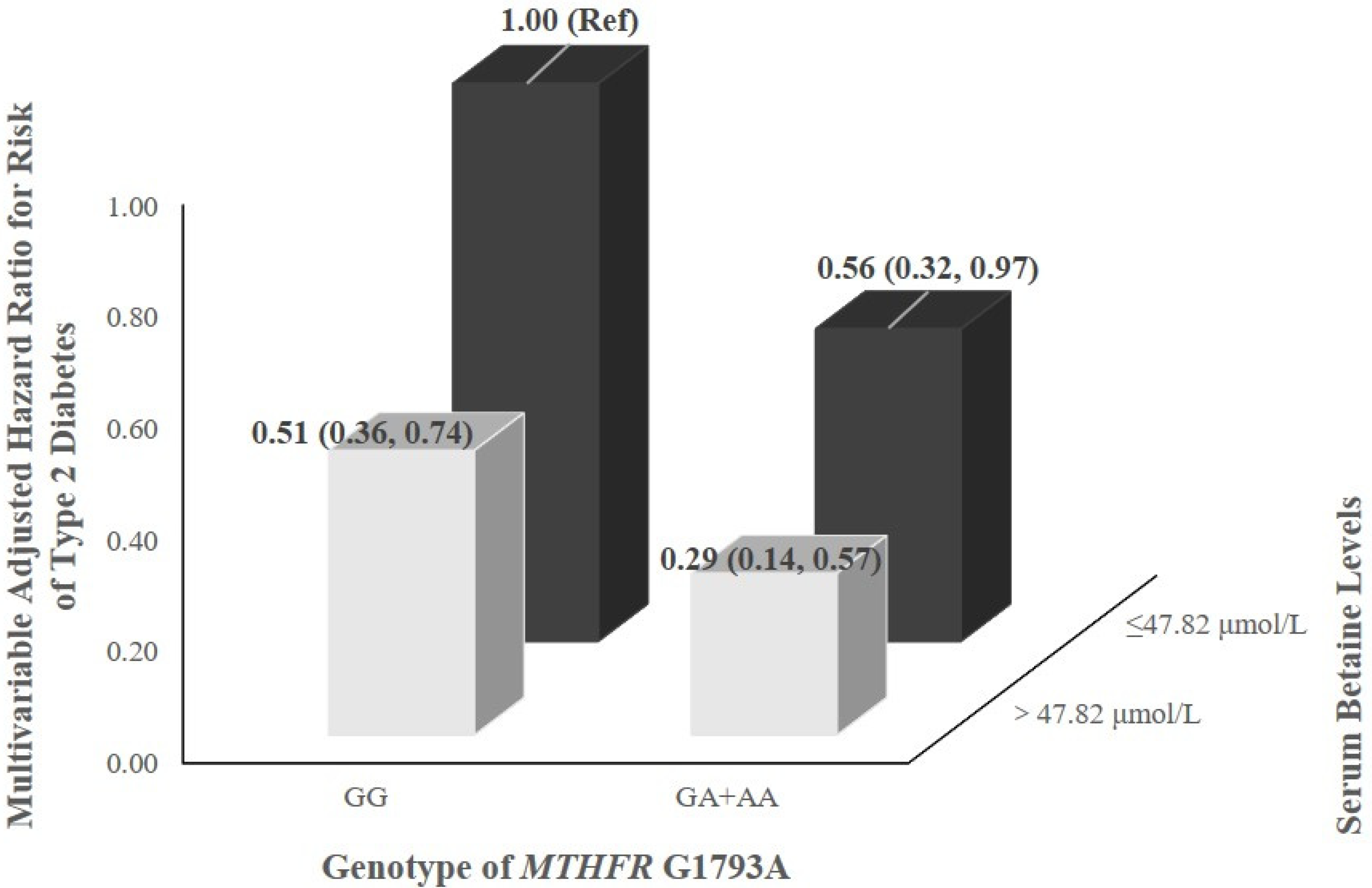
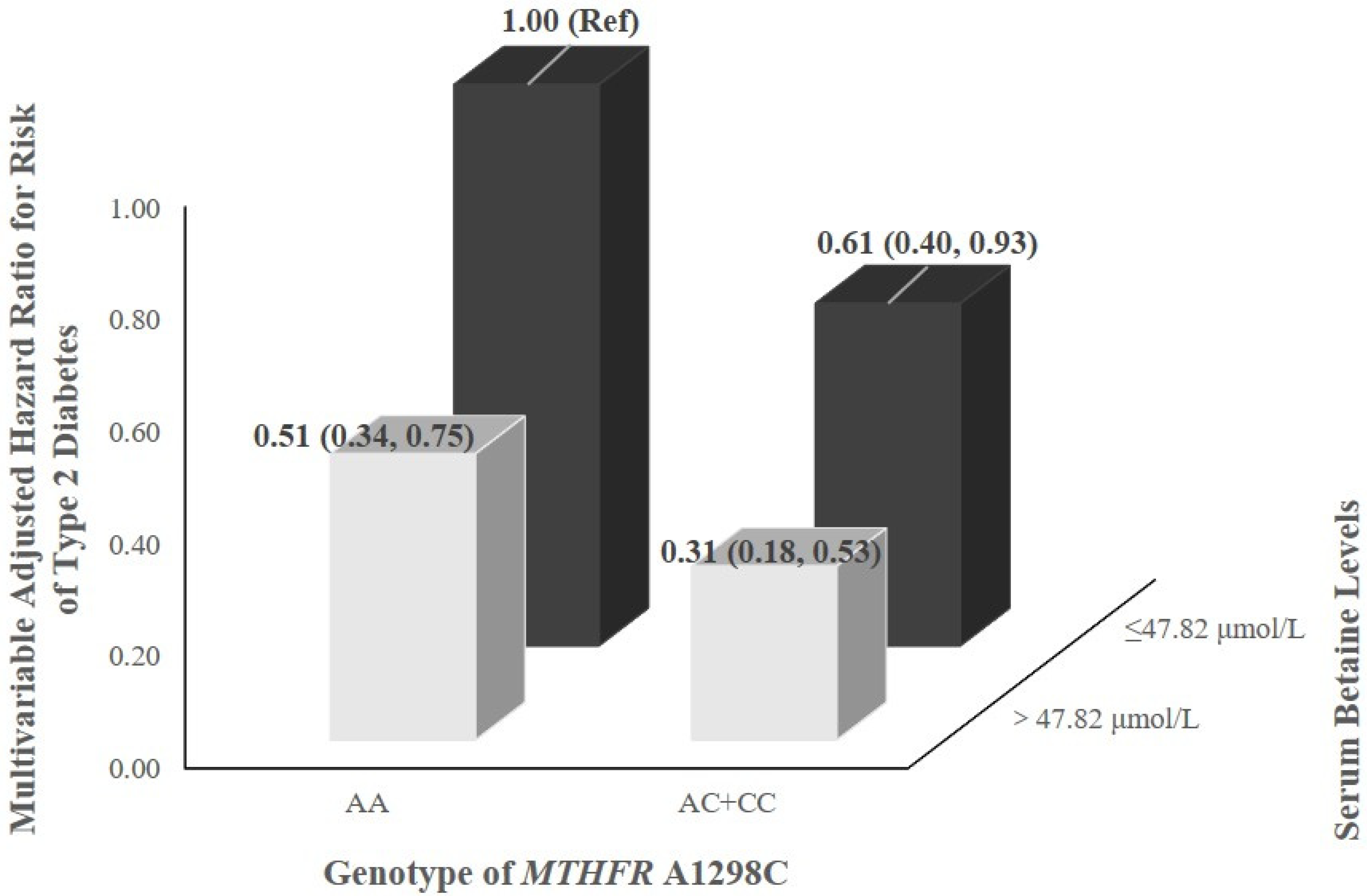
3.4. Interaction between Serum Betaine Levels and Genetic Polymorphisms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; Available online: https://www.diabetesatlas.org/en/ (accessed on 5 December 2021).
- World Health Organization. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 5 December 2021).
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37, S81–S90. [Google Scholar] [CrossRef] [Green Version]
- Walford, G.A.; Ma, Y.; Clish, C.; Florez, J.C.; Wang, T.J.; Gerszten, R.E. Metabolite profiles of diabetes incidence and intervention response in the Diabetes Prevention Program. Diabetes 2016, 65, 1424–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, S.A. Betaine in human nutrition. Am. J. Clin. Nutr. 2004, 80, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obeid, R.; Awwad, H.M.; Rabagny, Y.; Graeber, S.; Herrmann, W.; Geisel, J. Plasma trimethylamine N-oxide concentration is associated with choline, phospholipids, and methyl metabolism. Am. J. Clin. Nutr. 2016, 103, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Lever, M.; McEntyre, C.J.; George, P.M.; Slow, S.; Elmslie, J.L.; Lunt, H.; Chambers, S.T.; Parry-Strong, A.; Krebs, J.D. Extreme urinary betaine losses in type 2 diabetes combined with bezafibrate treatment are associated with losses of dimethylglycine and choline but not with increased losses of other osmolytes. Cardiovasc. Drugs Ther. 2014, 28, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wang, Y.; Sun, G. High dietary choline and betaine intake is associated with low insulin resistance in the Newfoundland population. Nutrition 2017, 33, 28–34. [Google Scholar] [CrossRef]
- Gao, X.; Randell, E.; Tian, Y.; Zhou, H.; Sun, G. Low serum choline and high serum betaine levels are associated with favorable components of metabolic syndrome in Newfoundland population. J. Diabetes Complicat. 2019, 33, 107398. [Google Scholar] [CrossRef] [PubMed]
- Roe, A.J.; Zhang, S.; Bhadelia, R.A.; Johnson, E.J.; Lichtenstein, A.H.; Rogers, G.T.; Rosenberg, I.H.; Smith, C.E.; Zeisel, S.H.; Scott, T.M. Choline and its metabolites are differently associated with cardiometabolic risk factors, history of cardiovascular disease, and MRI-documented cerebrovascular disease in older adults. Am. J. Clin. Nutr. 2017, 105, 1283–1290. [Google Scholar] [CrossRef]
- Garcia, E.; Oste, M.C.J.; Bennett, D.W.; Jeyarajah, E.J.; Shalaurova, I.; Gruppen, E.G.; Hazen, S.L.; Otvos, J.D.; Bakker, S.J.L.; Dullaart, R.P.F.; et al. High Betaine, a Trimethylamine N-Oxide Related Metabolite, Is Prospectively Associated with Low Future Risk of Type 2 Diabetes Mellitus in the PREVEND Study. J. Clin. Med. 2019, 8, 1813. [Google Scholar] [CrossRef] [Green Version]
- Dibaba, D.T.; Johnson, K.C.; Kucharska-Newton, A.M.; Meyer, K.; Zeisel, S.H.; Bidulescu, A. The Association of Dietary Choline and Betaine With the Risk of Type 2 Diabetes: The Atherosclerosis Risk in Communities (ARIC) Study. Diabetes Care 2020, 43, 2840–2846. [Google Scholar] [CrossRef]
- Rhee, E.P.; Ho, J.E.; Chen, M.H.; Shen, D.; Cheng, S.; Larson, M.G.; Ghorbani, A.; Shi, X.; Helenius, I.T.; O’Donnell, C.J.; et al. A genome-wide association study of the human metabolome in a community-based cohort. Cell Metab. 2013, 18, 130–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilozumba, M.N.; Cheng, T.D.; Neuhouser, M.L.; Miller, J.W.; Beresford, S.A.A.; Duggan, D.J.; Toriola, A.T.; Song, X.; Zheng, Y.; Bailey, L.B.; et al. Associations between Plasma Choline Metabolites and Genetic Polymorphisms in One-Carbon Metabolism in Postmenopausal Women: The Women’s Health Initiative Observational Study. J. Nutr. 2020, 150, 2874–2881. [Google Scholar] [CrossRef]
- Shpichinetsky, V.; Raz, I.; Friedlander, Y.; Goldschmidt, N.; Wexler, I.D.; Ben-Yehuda, A.; Friedman, G. The association between two common mutations C677T and A1298C in human methylenetetrahydrofolate reductase gene and the risk for diabetic nephropathy in type II diabetic patients. J. Nutr. 2000, 130, 2493–2497. [Google Scholar] [CrossRef] [Green Version]
- de Aquino, S.N.; Hoshi, R.; Bagordakis, E.; Pucciarelli, M.G.; Messetti, A.C.; Moreira, H.; Bufalino, A.; Borges, A.; Rangel, A.L.; Brito, L.A.; et al. MTHFR rs2274976 polymorphism is a risk marker for nonsyndromic cleft lip with or without cleft palate in the Brazilian population. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Miao, Z.; Lin, J.S.; Mao, Y.; Chen, G.D.; Zeng, F.F.; Dong, H.L.; Jiang, Z.; Wang, J.; Xiao, C.; Shuai, M.; et al. Erythrocyte n-6 Polyunsaturated Fatty Acids, Gut Microbiota, and Incident Type 2 Diabetes: A Prospective Cohort Study. Diabetes Care 2020, 43, 2435–2443. [Google Scholar] [CrossRef] [PubMed]
- Holm, P.I.; Ueland, P.M.; Kvalheim, G.; Lien, E.A. Determination of choline, betaine, and dimethylglycine in plasma by a high-throughput method based on normal-phase chromatography-tandem mass spectrometry. Clin. Chem. 2003, 49, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.X.; Ho, S.C. Validity and reproducibility of a food frequency questionnaire among Chinese women in Guangdong province. Asia Pac. J. Clin. Nutr. 2009, 18, 240–250. [Google Scholar]
- Yang, Y.X. China Food Composition; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Desquilbet, L.; Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Svingen, G.F.; Schartum-Hansen, H.; Pedersen, E.R.; Ueland, P.M.; Tell, G.S.; Mellgren, G.; Njolstad, P.R.; Seifert, R.; Strand, E.; Karlsson, T.; et al. Prospective Associations of Systemic and Urinary Choline Metabolites with Incident Type 2 Diabetes. Clin. Chem. 2016, 62, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Papandreou, C.; Bullo, M.; Zheng, Y.; Ruiz-Canela, M.; Yu, E.; Guasch-Ferre, M.; Toledo, E.; Clish, C.; Corella, D.; Estruch, R.; et al. Plasma trimethylamine-N-oxide and related metabolites are associated with type 2 diabetes risk in the Prevencion con Dieta Mediterranea (PREDIMED) trial. Am. J. Clin. Nutr. 2018, 108, 163–173. [Google Scholar] [CrossRef]
- Du, J.; Shen, L.; Tan, Z.; Zhang, P.; Zhao, X.; Xu, Y.; Gan, M.; Yang, Q.; Ma, J.; Jiang, A.; et al. Betaine Supplementation Enhances Lipid Metabolism and Improves Insulin Resistance in Mice Fed a High-Fat Diet. Nutrients 2018, 10, 131. [Google Scholar] [CrossRef] [Green Version]
- Ejaz, A.; Martinez-Guino, L.; Goldfine, A.B.; Ribas-Aulinas, F.; De Nigris, V.; Ribo, S.; Gonzalez-Franquesa, A.; Garcia-Roves, P.M.; Li, E.; Dreyfuss, J.M.; et al. Dietary Betaine Supplementation Increases Fgf21 Levels to Improve Glucose Homeostasis and Reduce Hepatic Lipid Accumulation in Mice. Diabetes 2016, 65, 902–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Kim, S.M.; Lee, B.; Lee, E.K.; Chung, K.W.; Moon, K.M.; An, H.J.; Kim, K.M.; Yu, B.P.; Chung, H.Y. Effect of betaine on hepatic insulin resistance through FOXO1-induced NLRP3 inflammasome. J. Nutr. Biochem. 2017, 45, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.M.; Abdalla, M.; Payne, A.; Fernandez-Tajes, J.; Thurner, M.; Nylander, V.; Gloyn, A.L.; Mahajan, A.; McCarthy, M.I. A Multi-omic Integrative Scheme Characterizes Tissues of Action at Loci Associated with Type 2 Diabetes. Am. J. Hum. Genet. 2020, 107, 1011–1028. [Google Scholar] [CrossRef]
- Rady, P.L.; Szucs, S.; Grady, J.; Hudnall, S.D.; Kellner, L.H.; Nitowsky, H.; Tyring, S.K.; Matalon, R.K. Genetic polymorphisms of methylenetetrahydrofolate reductase (MTHFR) and methionine synthase reductase (MTRR) in ethnic populations in Texas; a report of a novel MTHFR polymorphic site, G1793A. Am. J. Med. Genet. 2002, 107, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, I.; Tran, P.; Christensen, B.; Sibani, S.; Rozen, R. A second genetic polymorphism in methylenetetrahydrofolate reductase (MTHFR) associated with decreased enzyme activity. Mol. Genet. Metab. 1998, 64, 169–172. [Google Scholar] [CrossRef]
- Chen, X.L.; Wang, Y.M.; Zhao, F.; Chen, Z.; Yang, X.; Sun, C.; Gao, Y.; Yang, T.G.; Tian, G.; Chen, Y.M.; et al. Methylenetetrahydrofolate reductase polymorphisms and colorectal cancer prognosis: A meta-analysis. J. Gene Med. 2019, 21, e3114. [Google Scholar] [CrossRef] [PubMed]
- Mtiraoui, N.; Ezzidi, I.; Chaieb, M.; Marmouche, H.; Aouni, Z.; Chaieb, A.; Mahjoub, T.; Vaxillaire, M.; Almawi, W.Y. MTHFR C677T and A1298C gene polymorphisms and hyperhomocysteinemia as risk factors of diabetic nephropathy in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2007, 75, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Benrahma, H.; Abidi, O.; Melouk, L.; Ajjemami, M.; Rouba, H.; Chadli, A.; Oudghiri, M.; Farouqui, A.; Barakat, A. Association of the C677T polymorphism in the human methylenetetrahydrofolate reductase (MTHFR) gene with the genetic predisposition for type 2 diabetes mellitus in a Moroccan population. Genet Test Mol. Biomark. 2012, 16, 383–387. [Google Scholar] [CrossRef]
- Poodineh, M.; Saravani, R.; Mirhosseini, M.; Sargazi, S. Association of Two Methylenetetrahydrofolate Reductase Polymorphisms (rs1801133, rs1801131) with the Risk of Type 2 Diabetes in South-East of Iran. Rep. Biochem. Mol. Biol. 2019, 8, 178–183. [Google Scholar] [PubMed]
- Ericson, U.C.; Ivarsson, M.I.; Sonestedt, E.; Gullberg, B.; Carlson, J.; Olsson, H.; Wirfalt, E. Increased breast cancer risk at high plasma folate concentrations among women with the MTHFR 677T allele. Am. J. Clin. Nutr. 2009, 90, 1380–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimian, M.; Hosseinzadeh Colagar, A. Human MTHFR-G1793A transition may be a protective mutation against male infertility: A genetic association study and in silico analysis. Hum. Fertil. 2018, 21, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Hazra, A.; Wu, K.; Kraft, P.; Fuchs, C.S.; Giovannucci, E.L.; Hunter, D.J. Twenty-four non-synonymous polymorphisms in the one-carbon metabolic pathway and risk of colorectal adenoma in the Nurses’ Health Study. Carcinogenesis 2007, 28, 1510–1519. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.F.; Luo, W.P.; Lin, F.Y.; Lian, Z.Q.; Mo, X.F.; Yan, B.; Xu, M.; Huang, W.Q.; Huang, J.; Zhang, C.X. Dietary choline and betaine intake, choline-metabolising genetic polymorphisms and breast cancer risk: A case-control study in China. Br. J. Nutr. 2016, 116, 961–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzini, E.; Ruggeri, S.; Polito, A. Homocysteine: Its possible emerging role in at-risk population groups. Int. J. Mol. Sci. 2020, 21, 1421. [Google Scholar] [CrossRef] [Green Version]
- Ogier de Baulny, H.; Gerard, M.; Saudubray, J.M.; Zittoun, J. Remethylation defects: Guidelines for clinical diagnosis and treatment. Eur. J. Pediatr. 1998, 157, S77–S83. [Google Scholar] [CrossRef]
- Lee, J.E.; Jacques, P.F.; Dougherty, L.; Selhub, J.; Giovannucci, E.; Zeisel, S.H.; Cho, E. Are dietary choline and betaine intakes determinants of total homocysteine concentration? Am. J. Clin. Nutr. 2010, 91, 1303–1310. [Google Scholar] [CrossRef]
- Wang, H.; Hu, C.; Xiao, S.H.; Wan, B. Association of tagging SNPs in the MTHFR gene with risk of type 2 diabetes mellitus and serum homocysteine levels in a Chinese population. Dis. Markers 2014, 2014, 725731. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Sex-Specific Quartiles of Serum Betaine Levels | p | p-Trend | ||||
|---|---|---|---|---|---|---|
| Q1 (n = 391) | Q2 (n = 393) | Q3 (n = 391) | Q4 (n = 390) | |||
| Serum betaine, μmol/L | ||||||
| Females | 25.60 ± 7.74 | 41.58 ± 2.97 | 50.72 ± 2.91 | 68.90 ± 13.71 | <0.001 | <0.001 |
| Males | 31.47 ± 8.50 | 48.35 ± 3.14 | 58.73 ± 2.98 | 77.02 ± 12.32 | ||
| Age, years | 57.59 ± 4.97 | 57.47 ± 4.92 | 57.69 ± 5.09 | 57.26 ± 4.91 | 0.659 | 0.504 |
| WHR | 0.88 ± 0.07 | 0.89 ± 0.06 | 0.88 ± 0.06 | 0.87 ± 0.07 | 0.002 | 0.014 |
| Energy intake, kcal/day | 1829.86 ± 534.72 | 1814.73 ± 480.77 | 1827.31 ± 507.30 | 1819.52 ± 489.09 | 0.973 | 0.872 |
| Physical activity, MET × hours/day | 25.83 ± 6.86 | 25.50 ± 7.25 | 25.84 ± 7.85 | 25.68 ± 6.65 | 0.901 | 0.939 |
| Females | 271 (69.3) | 272 (69.2) | 270 (69.1) | 271 (69.5) | 0.999 | 0.971 |
| Education levels | 0.043 | 0.341 | ||||
| Less than high school | 122 (31.2) | 112 (28.5) | 124 (31.7) | 105 (26.9) | ||
| High school | 161 (41.2) | 181 (46.1) | 183 (46.8) | 205 (52.6) | ||
| College or above | 108 (27.6) | 100 (25.4) | 84 (21.5) | 80 (20.5) | ||
| Household income, yuan/month/person | 0.786 | 0.624 | ||||
| <1500 | 147 (37.6) | 127 (32.3) | 136 (34.8) | 139 (35.6) | ||
| 1500–3000 | 176 (45.0) | 183 (46.6) | 179 (45.8) | 175 (44.9) | ||
| ≥3000 | 68 (17.4) | 83 (21.1) | 76 (19.4) | 76 (19.5) | ||
| Smoking status | 0.985 | 0.702 | ||||
| Non-smoker | 329 (84.1) | 332 (84.5) | 331 (84.7) | 332 (85.1) | ||
| Smoker | 62 (15.9) | 61 (15.5) | 60 (15.3) | 58 (14.9) | ||
| Alcohol drinking | 0.247 | 0.196 | ||||
| Non-alcohol drinker | 364 (93.1) | 362 (92.1) | 373 (95.4) | 368 (94.4) | ||
| Alcohol drinker | 27 (6.9) | 31 (7.9) | 18 (4.6) | 22 (5.6) | ||
| Sex-Specific Quartiles of Serum Betaine Levels | |||||
|---|---|---|---|---|---|
| Q1 (n = 391) | Q2 (n = 393) | Q3 (n = 391) | Q4 (n = 390) | p-Trend | |
| Number of cases | 76 | 58 | 43 | 36 | - |
| Person years at risk | 2915.77 | 3063.16 | 3091.28 | 3097.66 | - |
| Model 1 1 | 1.00 (ref) | 0.73 (0.52, 1.03) | 0.53 (0.37, 0.78) | 0.45 (0.30, 0.66) | <0.001 |
| Model 2 2 | 1.00 (ref) | 0.74 (0.52, 1.04) | 0.54 (0.37, 0.78) | 0.45 (0.30, 0.67) | <0.001 |
| Model 3 3 | 1.00 (ref) | 0.68 (0.48, 0.96) | 0.55 (0.38, 0.80) | 0.46 (0.31, 0.69) | <0.001 |
| Genotype (n = 1134) | ||
|---|---|---|
| Non-Mutated Group | Heterozygous or Homozygous Mutated Group | |
| MTHFR G1793A (rs2274976) | GG | GA + AA |
| Cases/n. | 134/878 | 24/256 |
| Model 1 1 | 1.00 (ref) | 0.59 (0.38, 0.92) |
| Model 2 2 | 1.00 (ref) | 0.60 (0.39, 0.92) |
| Model 3 3 | 1.00 (ref) | 0.54 (0.35, 0.84) |
| MTHFR A1298C (rs1801131) | AA | AC + CC |
| Cases/n. | 110/686 | 48/448 |
| Model 1 1 | 1.00 (ref) | 0.65 (0.46, 0.91) |
| Model 2 2 | 1.00 (ref) | 0.64 (0.46, 0.90) |
| Model 3 3 | 1.00 (ref) | 0.61 (0.43, 0.86) |
| MTHFR C677T (rs1801133) | CC | CT + TT |
| Cases/n. | 81/645 | 77/489 |
| Model 1 1 | 1.00 (ref) | 1.31 (0.96, 1.79) |
| Model 2 2 | 1.00 (ref) | 1.30 (0.95, 1.78) |
| Model 3 3 | 1.00 (ref) | 1.33 (0.97, 1.81) |
| CHDH A318C (rs9001) | AA | AC + CC |
| Cases/n. | 70/503 | 88/631 |
| Model 1 1 | 1.00 (ref) | 1.01 (0.73, 1.38) |
| Model 2 2 | 1.00 (ref) | 1.01 (0.74, 1.38) |
| Model 3 3 | 1.00 (ref) | 0.99 (0.72, 1.36) |
| BHMT G742A (rs3733890) | GG | GA + AA |
| Cases/n. | 64/468 | 94/666 |
| Model 1 1 | 1.00 (ref) | 1.01 (0.74, 1.39) |
| Model 2 2 | 1.00 (ref) | 1.02 (0.74, 1.40) |
| Model 3 3 | 1.00 (ref) | 0.91 (0.66, 1.26) |
| n | Quartile of Serum Betaine Levels | p-Trend | p-Interaction | |||||
|---|---|---|---|---|---|---|---|---|
| Q1 (n = 289) | Q2 (n = 280) | Q3 (n = 286) | Q4 (n = 279) | |||||
| MTHFR G1793A (rs2274976) | 0.017 | |||||||
| GG | 878 | 1.00 (ref) | 0.71 (0.47, 1.08) | 0.47 (0.29, 0.76) | 0.40 (0.23, 0.68) | <0.001 | ||
| GA + AA | 256 | 1.00 (ref) | 0.34 (0.10, 1.10) | 0.35 (0.11, 1.11) | 0.33 (0.11, 0.97) | 0.039 | ||
| MTHFR A1298C (rs1801131) | 0.007 | |||||||
| AA | 686 | 1.00 (ref) | 0.77 (0.48, 1.23) | 0.51 (0.30, 0.86) | 0.38 (0.21, 0.70) | <0.001 | ||
| AC + CC | 448 | 1.00 (ref) | 0.44 (0.21, 0.95) | 0.36 (0.16, 0.81) | 0.33 (0.15, 0.76) | 0.003 | ||
| MTHFR C677T (rs1801133) | 0.086 | |||||||
| CC | 645 | 1.00 (ref) | 0.49 (0.28, 0.86) | 0.39 (0.21, 0.72) | 0.37 (0.20, 0.71) | 0.001 | ||
| CT + TT | 489 | 1.00 (ref) | 1.01 (0.58, 1.77) | 0.57 (0.31, 1.07) | 0.38 (0.18, 0.79) | 0.003 | ||
| CHDH A318C (rs9001) | 0.787 | |||||||
| AA | 503 | 1.00 (ref) | 0.68 (0.38, 1.22) | 0.44 (0.22, 0.86) | 0.29 (0.14, 0.61) | <0.001 | ||
| AC + CC | 631 | 1.00 (ref) | 0.67 (0.39, 1.14) | 0.51 (0.28, 0.91) | 0.49 (0.26, 0.91) | 0.009 | ||
| BHMT G742A (rs3733890) | 0.355 | |||||||
| GG | 468 | 1.00 (ref) | 0.74 (0.39, 1.38) | 0.56 (0.28, 1.11) | 0.37 (0.17, 0.80) | 0.007 | ||
| GA + AA | 666 | 1.00 (ref) | 0.62 (0.37, 1.02) | 0.40 (0.22, 0.71) | 0.37 (0.20, 0.69) | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, X.; Huang, R.; Li, S.; Fang, A.; Chen, Y.; Chen, S.; Wang, F.; Lin, X.; Liu, Z.; Zhu, H. Associations between Serum Betaine, Methyl-Metabolizing Genetic Polymorphisms and Risk of Incident Type 2 Diabetes: A Prospective Cohort Study in Community-Dwelling Chinese Adults. Nutrients 2022, 14, 362. https://doi.org/10.3390/nu14020362
Lu X, Huang R, Li S, Fang A, Chen Y, Chen S, Wang F, Lin X, Liu Z, Zhu H. Associations between Serum Betaine, Methyl-Metabolizing Genetic Polymorphisms and Risk of Incident Type 2 Diabetes: A Prospective Cohort Study in Community-Dwelling Chinese Adults. Nutrients. 2022; 14(2):362. https://doi.org/10.3390/nu14020362
Chicago/Turabian StyleLu, Xiaoting, Rongzhu Huang, Shuyi Li, Aiping Fang, Yuming Chen, Si Chen, Fan Wang, Xinlei Lin, Zhaoyan Liu, and Huilian Zhu. 2022. "Associations between Serum Betaine, Methyl-Metabolizing Genetic Polymorphisms and Risk of Incident Type 2 Diabetes: A Prospective Cohort Study in Community-Dwelling Chinese Adults" Nutrients 14, no. 2: 362. https://doi.org/10.3390/nu14020362