
Effect of Standardized Hydrangea serrata (Thunb.) Ser. Leaves Extract on Body Weight and Body Fat Reduction in Overweight or Obese Humans: A Randomized Double-Blind Placebo-Controlled Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Test Material
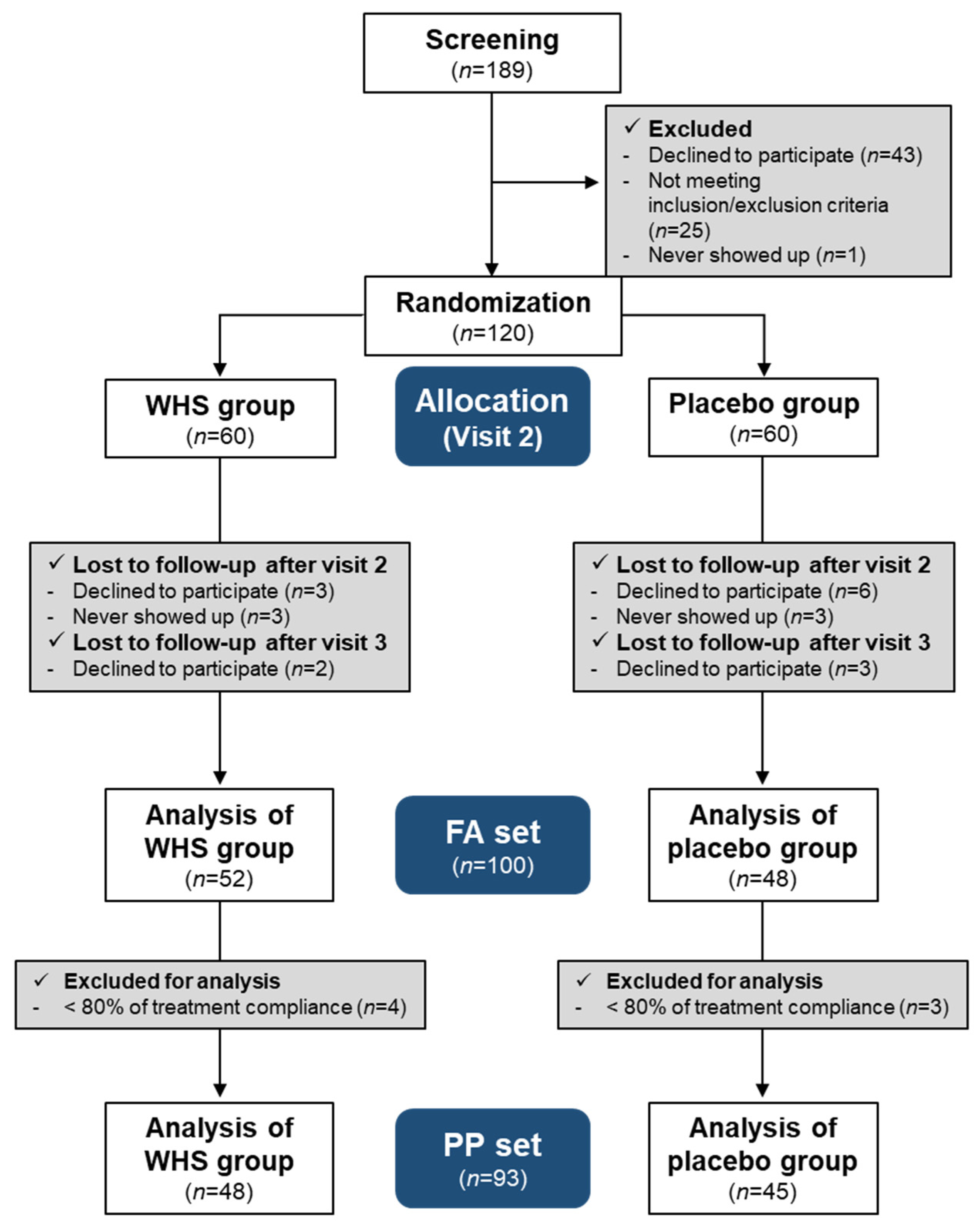
2.2. Subjects
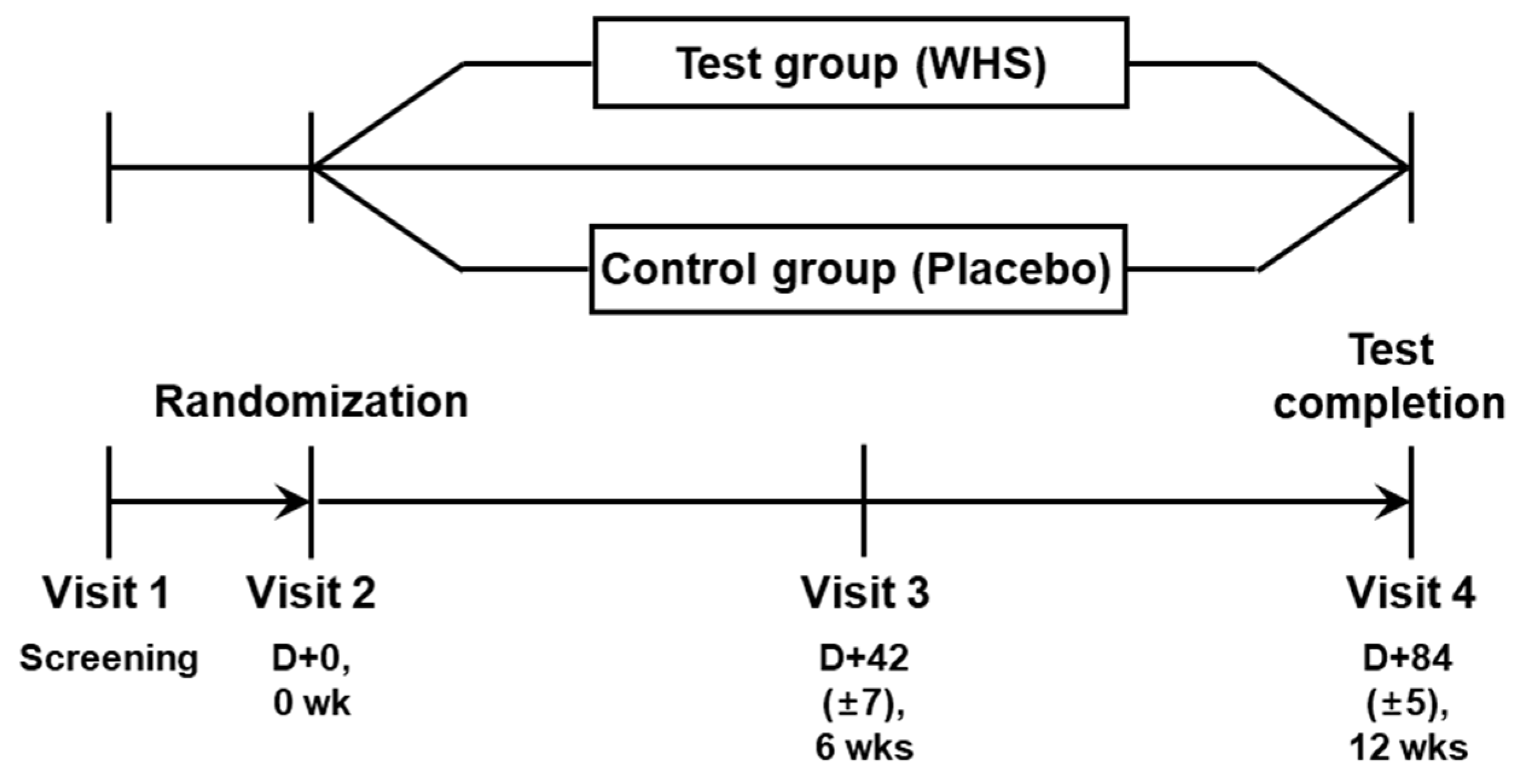
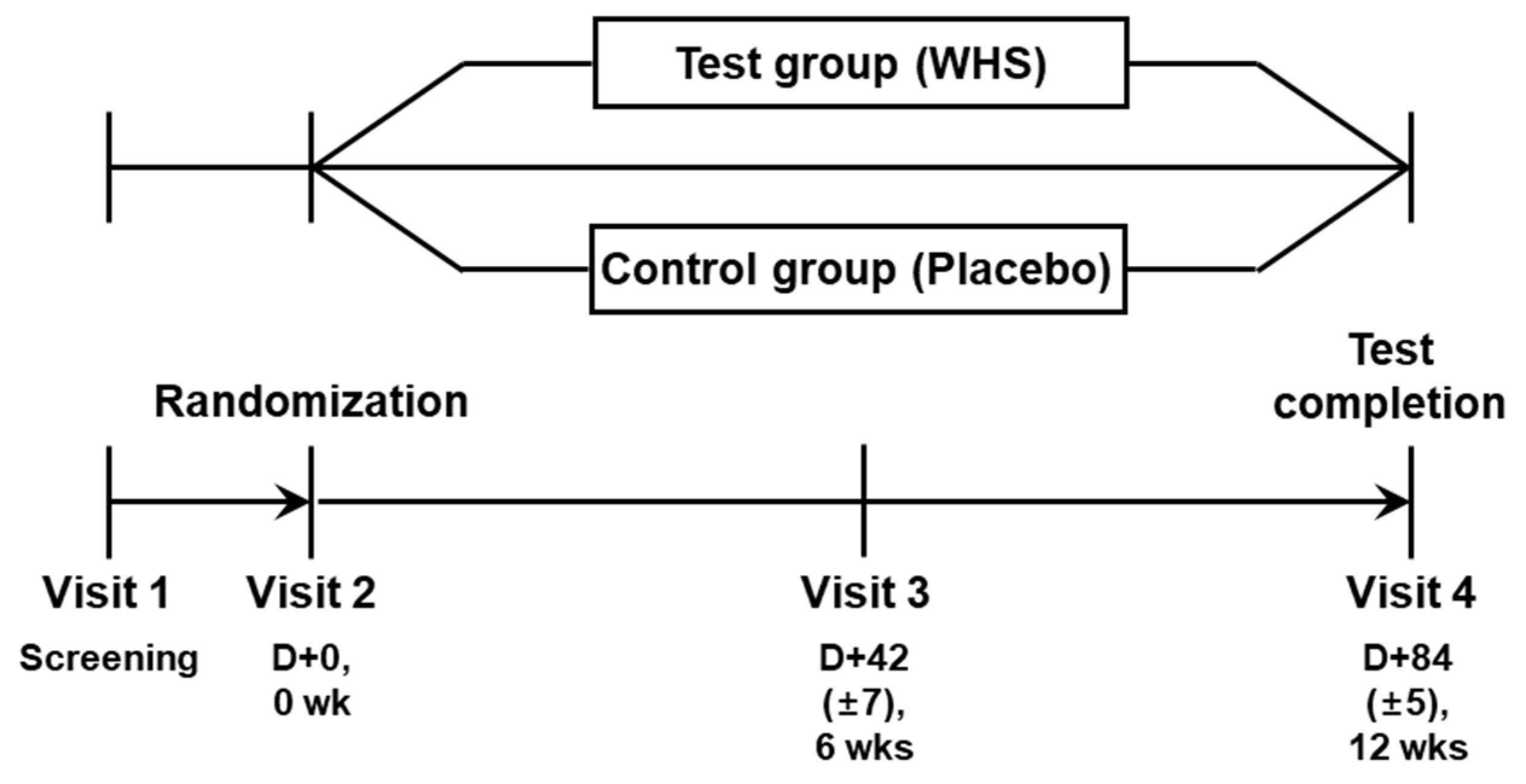
2.3. Study Design
2.4. Sample Size Determination and Power Calculation
2.5. Clinical Outcomes
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Subjects
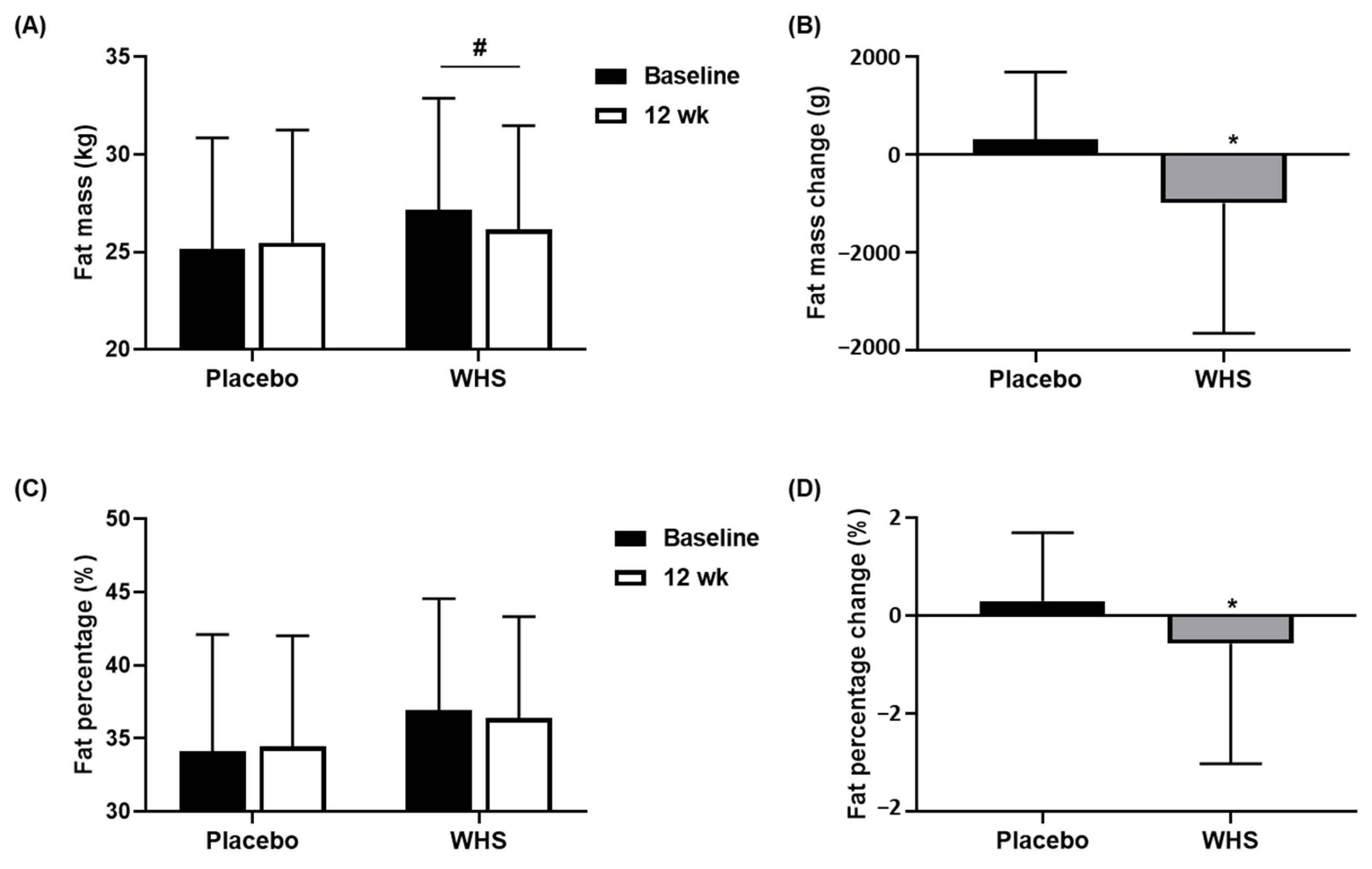
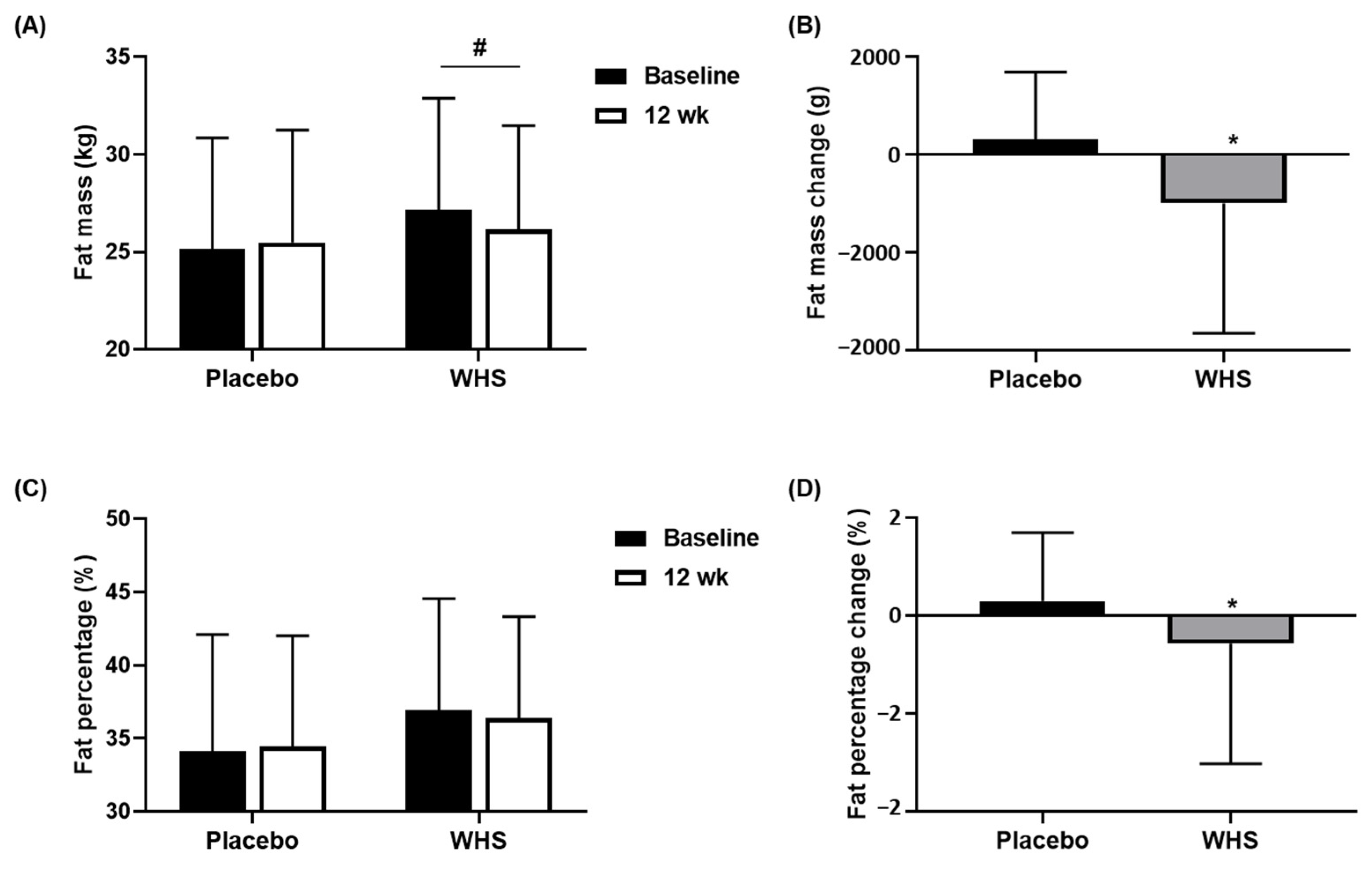
3.2. Effect of WHS on the Reduction of Fat Mass and Fat Percentage
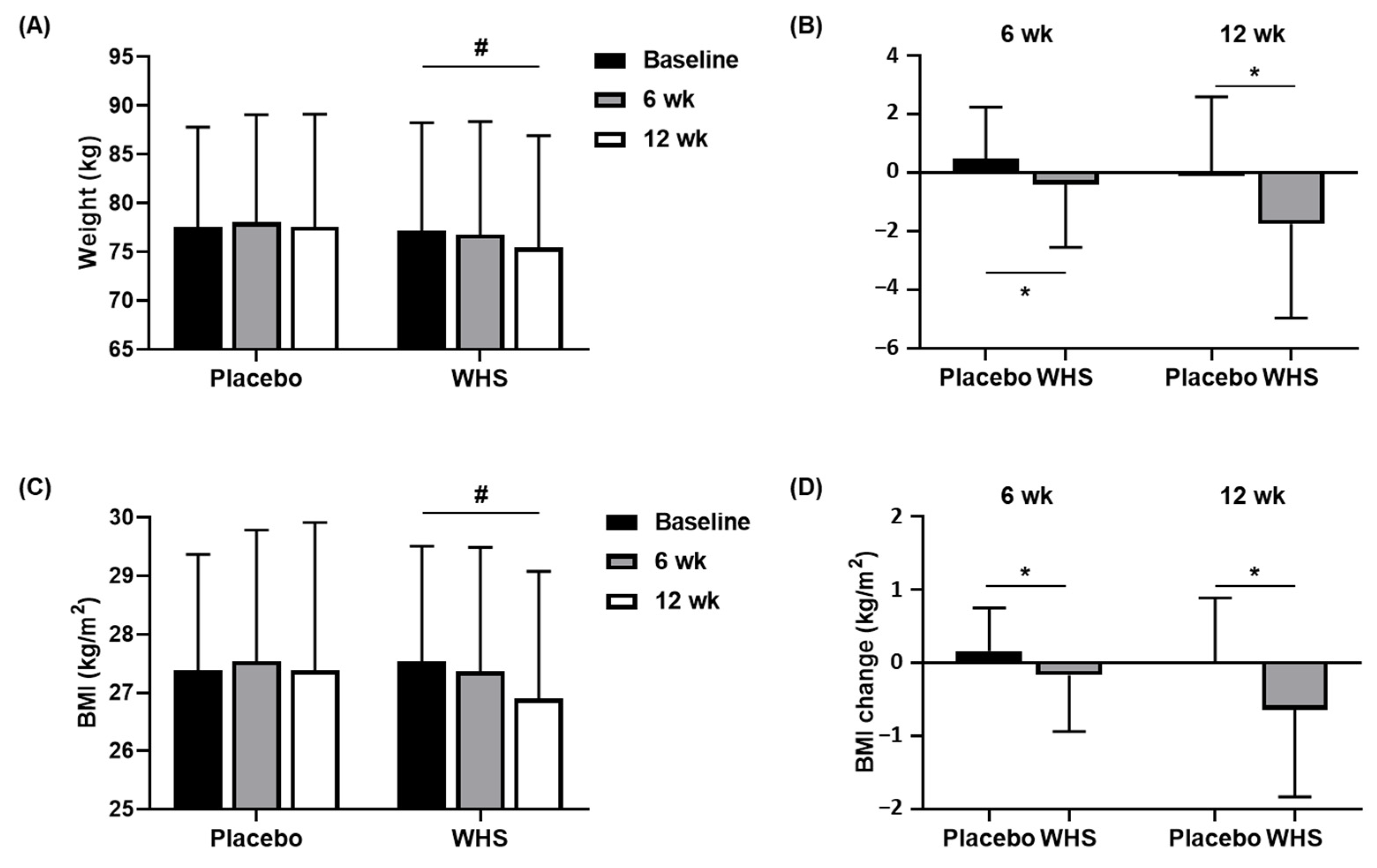
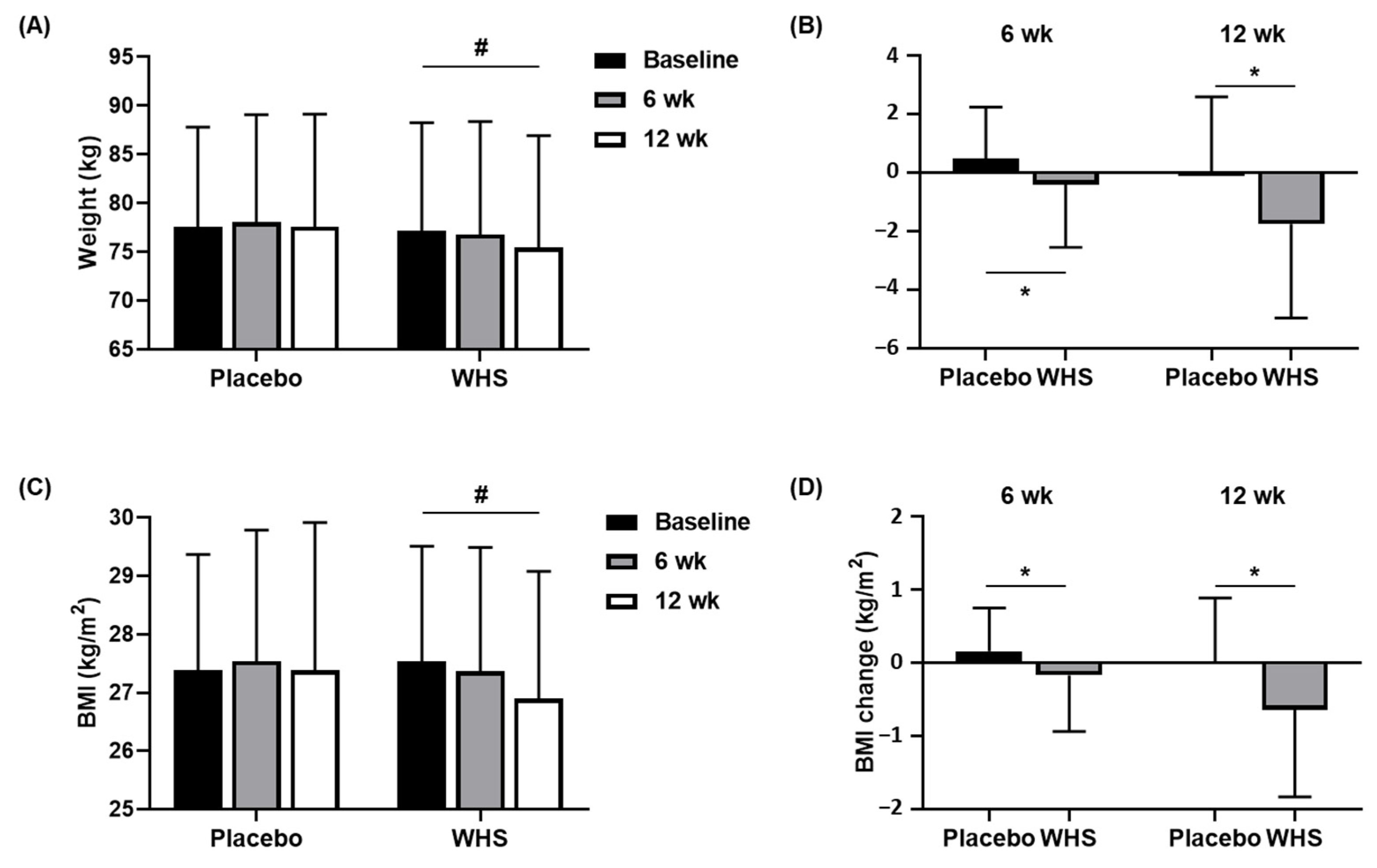
3.3. Effect of WHS on Body Weight and BMI
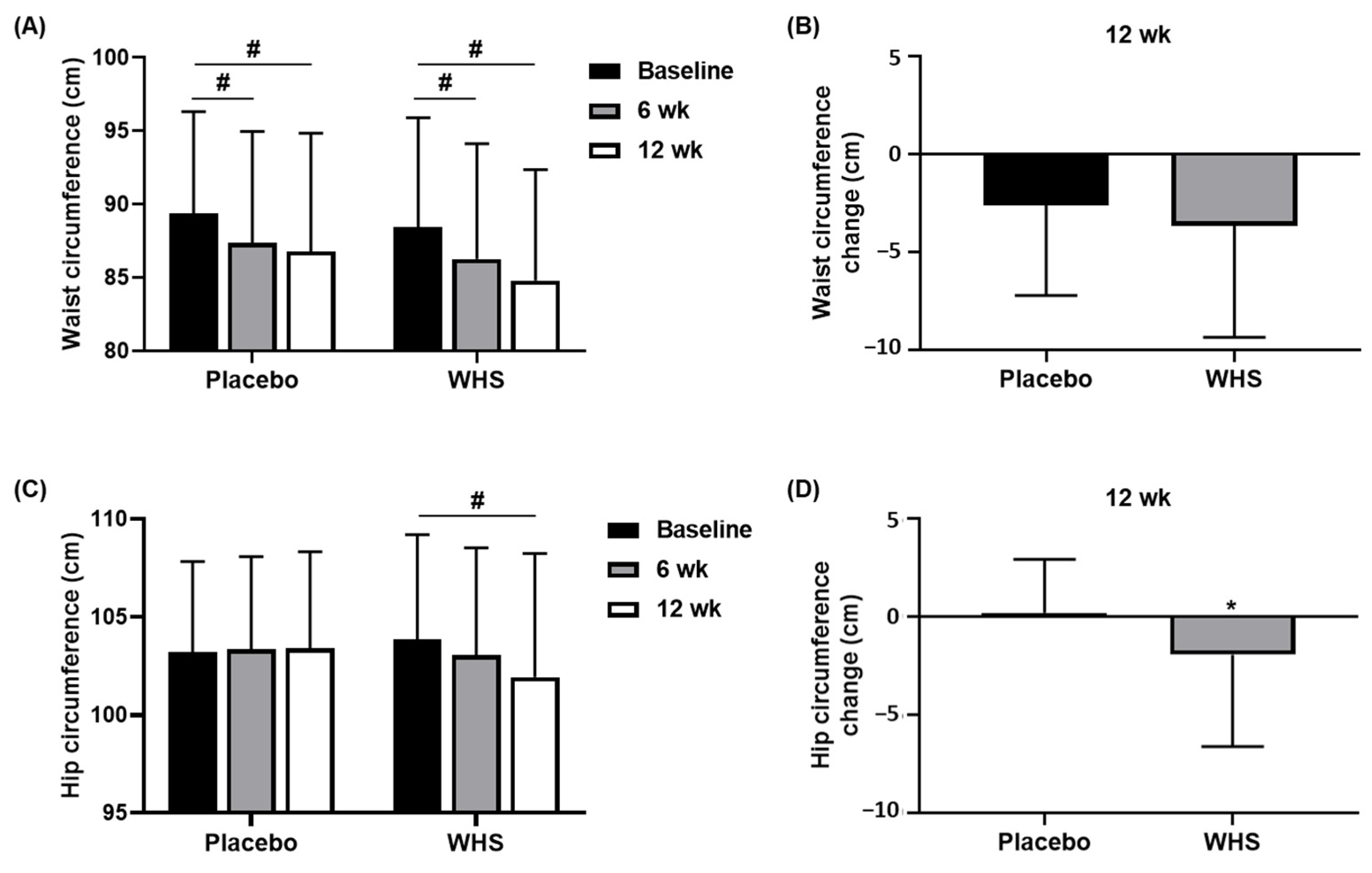
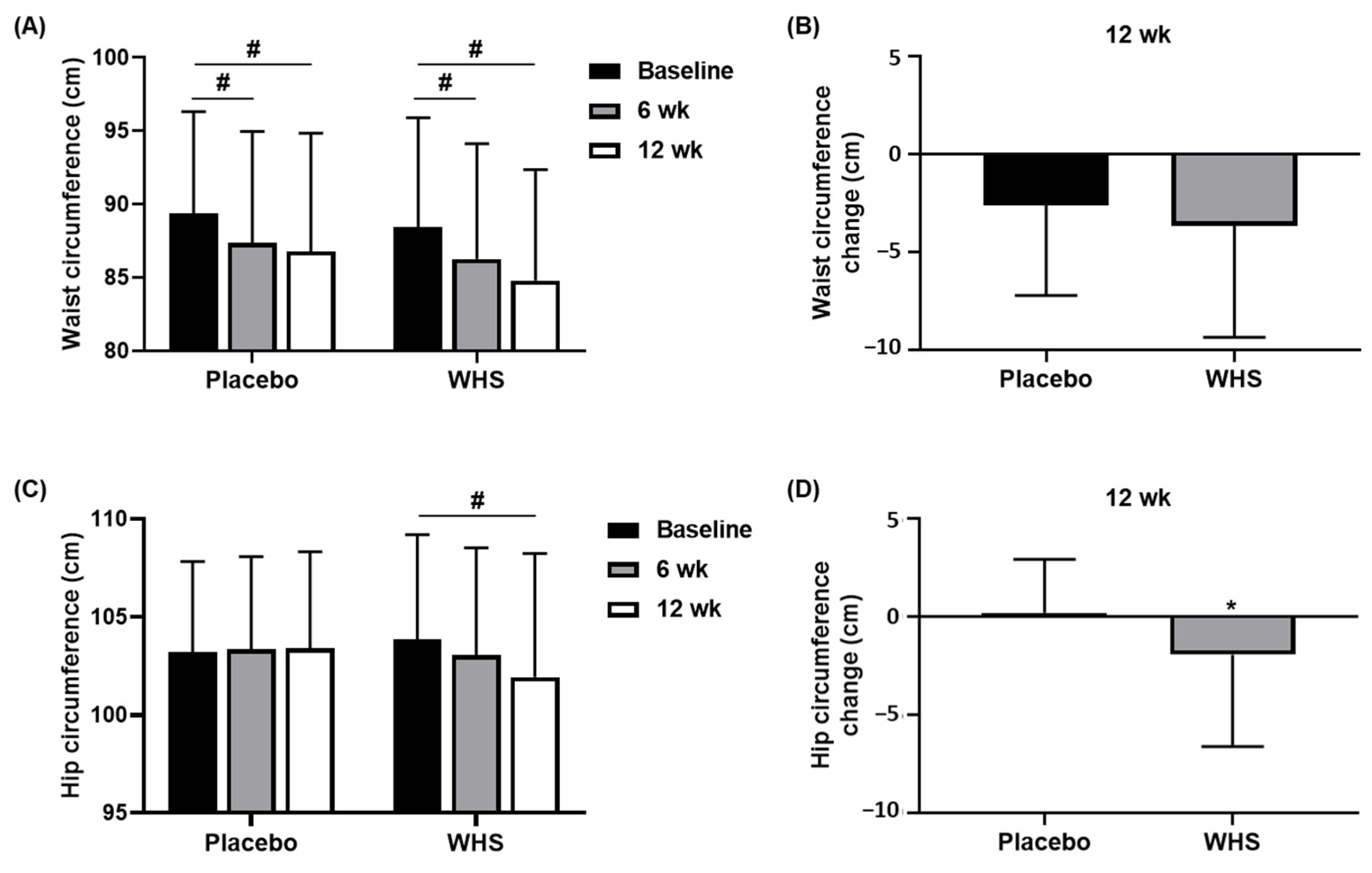
3.4. Effect of WHS on the Waist and Hip Circumferences
3.5. Effect of WHS on Body Fat Area
3.6. Effect of WHS on the Plasma Levels of Lipid Metabolism Markers and Adipokines
3.7. Safety Evaluation of WHS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wright, S.M.; Aronne, L.J. Causes of obesity. Abdom. Imaging 2012, 37, 730–732. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J.; Mantzoros, C.S. Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92, 82–97. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Pi-Sunyer, F.X. Obesity: Criteria and classification. Proc. Nutr. Soc. 2000, 59, 505–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weight Loss Agents. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Chang, E.; Kim, C.Y. Natural Products and Obesity: A Focus on the Regulation of Mitotic Clonal Expansion during Adipogenesis. Molecules 2019, 24, 1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J.; Le, B.; Lee, D.R.; Choi, B.K.; Yang, S.H. Cissus quadrangularis extract (CQR-300) inhibits lipid accumulation by downregulating adipogenesis and lipogenesis in 3T3-L1 cells. Toxicol. Rep. 2018, 5, 608–614. [Google Scholar] [CrossRef]
- Titta, L.; Trinei, M.; Stendardo, M.; Berniakovich, I.; Petroni, K.; Tonelli, C.; Riso, P.; Porrini, M.; Minucci, S.; Pelicci, P.G.; et al. Blood orange juice inhibits fat accumulation in mice. Int. J. Obes. 2010, 34, 578–588. [Google Scholar] [CrossRef] [Green Version]
- Cardile, V.; Graziano, A.C.; Venditti, A. Clinical evaluation of Moro (Citrus sinensis (L.) Osbeck) orange juice supplementation for the weight management. Nat. Prod. Res. 2015, 29, 2256–2260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boschmann, M.; Thielecke, F. The effects of epigallocatechin-3-gallate on thermogenesis and fat oxidation in obese men: A pilot study. J. Am. Coll. Nutr. 2007, 26, 389S–395S. [Google Scholar] [CrossRef]
- Lee, M.S.; Kim, C.T.; Kim, Y. Green tea (-)-epigallocatechin-3-gallate reduces body weight with regulation of multiple genes expression in adipose tissue of diet-induced obese mice. Ann. Nutr. Metab. 2009, 54, 151–157. [Google Scholar] [CrossRef]
- Nawaz, A.; Nishida, Y.; Takikawa, A.; Fujisaka, S.; Kado, T.; Aminuddin, A.; Nishimura, A.; Kuwano, T.; Watanabe, Y.; Igarashi, Y.; et al. Astaxanthin, a Marine Carotenoid, Maintains the Tolerance and Integrity of Adipose Tissue and Contributes to Its Healthy Functions. Nutrients 2021, 13, 4374. [Google Scholar] [CrossRef] [PubMed]
- Nishida, Y.; Nawaz, A.; Kado, T.; Takikawa, A.; Igarashi, Y.; Onogi, Y.; Wada, T.; Sasaoka, T.; Yamamoto, S.; Sasahara, M.; et al. Astaxanthin stimulates mitochondrial biogenesis in insulin resistant muscle via activation of AMPK pathway. J. Cachexia Sarcopenia Muscle 2020, 11, 241–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, C.H.; Kim, Y.; Kim, M.S.; Lee, S.; Yoo, S.H. The establishment of efficient bioconversion, extraction, and isolation processes for the production of phyllodulcin, a potential high intensity sweetener, from sweet hydrangea leaves (Hydrangea macrophylla Thunbergii). Phytochem. Anal. 2016, 27, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Han, H.S.; Lee, H.H.; Gil, H.S.; Chung, K.S.; Kim, J.K.; Kim, D.H.; Yoon, J.; Chung, E.K.; Lee, J.K.; Yang, W.M.; et al. Standardized hot water extract from the leaves of Hydrangea serrata (Thunb.) Ser. alleviates obesity via the AMPK pathway and modulation of the gut microbiota composition in high fat diet-induced obese mice. Food Funct. 2021, 12, 2672–2685. [Google Scholar] [CrossRef] [PubMed]
- Han, H.S.; Chung, K.S.; Shin, Y.K.; Lee, S.H.; Lee, K.T. Standardized Hydrangea serrata (Thunb.) Ser. Extract Ameliorates Obesity in db/db Mice. Nutrients 2021, 13, 3624. [Google Scholar] [CrossRef]
- Zhang, B.B.; Zhou, G.; Li, C. AMPK: An emerging drug target for diabetes and the metabolic syndrome. Cell Metab. 2009, 9, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Kola, B.; Grossman, A.B.; Korbonits, M. The role of AMP-activated protein kinase in obesity. Front. Horm Res. 2008, 36, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhang, L.; Li, B.; Jiang, H.; Duan, Y.; Xie, Z.; Shuai, L.; Li, J.; Li, J. AMP-Activated Protein Kinase (AMPK) Regulates Energy Metabolism through Modulating Thermogenesis in Adipose Tissue. Front. Physiol. 2018, 9, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myung, D.B.; Lee, J.H.; Han, H.S.; Lee, K.Y.; Ahn, H.S.; Shin, Y.K.; Song, E.; Kim, B.H.; Lee, K.H.; Lee, S.H.; et al. Oral Intake of Hydrangea serrata (Thunb.) Ser. Leaves Extract Improves Wrinkles, Hydration, Elasticity, Texture, and Roughness in Human Skin: A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2020, 12, 1588. [Google Scholar] [CrossRef]
- Nosaka, N.; Maki, H.; Suzuki, Y.; Haruna, H.; Ohara, A.; Kasai, M.; Tsuji, H.; Aoyama, T.; Okazaki, M.; Igarashi, O.; et al. Effects of margarine containing medium-chain triacylglycerols on body fat reduction in humans. J. Atheroscler. Thromb. 2003, 10, 290–298. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.; Kim, D.; Kim, J.S. Body Fat Distribution and the Risk of Incident Metabolic Syndrome: A Longitudinal Cohort Study. Sci. Rep. 2017, 7, 10955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjorndal, B.; Burri, L.; Staalesen, V.; Skorve, J.; Berge, R.K. Different adipose depots: Their role in the development of metabolic syndrome and mitochondrial response to hypolipidemic agents. J. Obes. 2011, 2011, 490650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaess, B.M.; Pedley, A.; Massaro, J.M.; Murabito, J.; Hoffmann, U.; Fox, C.S. The ratio of visceral to subcutaneous fat, a metric of body fat distribution, is a unique correlate of cardiometabolic risk. Diabetologia 2012, 55, 2622–2630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iikuni, N.; Lam, Q.L.; Lu, L.; Matarese, G.; La Cava, A. Leptin and Inflammation. Curr. Immunol. Rev. 2008, 4, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Sengupta, P. Men and mice: Relating their ages. Life Sci. 2016, 152, 244–248. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Allison, D.B.; Vasselli, J.R.; Pietrobelli, A.; Greenfield, D.; Nunez, C. Garcinia cambogia (hydroxycitric acid) as a potential antiobesity agent: A randomized controlled trial. JAMA 1998, 280, 1596–1600. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.E.; Jeon, S.M.; Park, K.H.; Lee, W.S.; Jeong, T.S.; McGregor, R.A.; Choi, M.S. Does Glycine max leaves or Garcinia Cambogia promote weight-loss or lower plasma cholesterol in overweight individuals: A randomized control trial. Nutr. J. 2011, 10, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.H.; Tsai, T.H.; Kao, Y.H.; Hwang, K.C.; Tseng, T.Y.; Chou, P. Effect of green tea extract on obese women: A randomized, double-blind, placebo-controlled clinical trial. Clin. Nutr. 2008, 27, 363–370. [Google Scholar] [CrossRef]
- Keithley, J.K.; Swanson, B.; Mikolaitis, S.L.; DeMeo, M.; Zeller, J.M.; Fogg, L.; Adamji, J. Safety and efficacy of glucomannan for weight loss in overweight and moderately obese adults. J. Obes. 2013, 2013, 610908. [Google Scholar] [CrossRef] [PubMed]
- Chong, P.W.; Beah, Z.M.; Grube, B.; Riede, L. IQP-GC-101 reduces body weight and body fat mass: A randomized, double-blind, placebo-controlled study. Phytother. Res. 2014, 28, 1520–1526. [Google Scholar] [CrossRef] [Green Version]
- Taghizadeh, M.; Farzin, N.; Taheri, S.; Mahlouji, M.; Akbari, H.; Karamali, F.; Asemi, Z. The Effect of Dietary Supplements Containing Green Tea, Capsaicin and Ginger Extracts on Weight Loss and Metabolic Profiles in Overweight Women: A Randomized Double-Blind Placebo-Controlled Clinical Trial. Ann. Nutr. Metab. 2017, 70, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.S.; Beaman, J.L.; He, Y.; Guo, Z.; Sun, H. Reduction of body fat and improved lipid profile associated with daily consumption of a Puer tea extract in a hyperlipidemic population: A randomized placebo-controlled trial. Clin. Interv. Aging 2016, 11, 367–376. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Oh, M.R.; Kim, M.G.; Chae, H.J.; Chae, S.W. Anti-obesity effects of Yerba Mate (Ilex Paraguariensis): A randomized, double-blind, placebo-controlled clinical trial. BMC Complement. Altern. Med. 2015, 15, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.S.; Song, M.Y.; Kim, H. The anti-obesity effect of Ephedra sinica through modulation of gut microbiota in obese Korean women. J. Ethnopharmacol. 2014, 152, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.S.; Han, H.S.; Lee, S.B.; Myung, D.B.; Lee, K.; Lee, S.H.; Kim, H.J.; Lee, K.T. Chemical Constituents from Leaves of Hydrangea serrata and Their Anti-photoaging Effects on UVB-Irradiated Human Fibroblasts. Biol. Pharm. Bull. 2019, 42, 424–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, H.S.; Shin, J.S.; Myung, D.B.; Ahn, H.S.; Lee, S.H.; Kim, H.J.; Lee, K.T. Hydrangea serrata (Thunb.) Ser. Extract Attenuate UVB-Induced Photoaging through MAPK/AP-1 Inactivation in Human Skin Fibroblasts and Hairless Mice. Nutrients 2019, 11, 533. [Google Scholar] [CrossRef] [Green Version]
- Myung, D.B.; Han, H.S.; Shin, J.S.; Park, J.Y.; Hwang, H.J.; Kim, H.J.; Ahn, H.S.; Lee, S.H.; Lee, K.T. Hydrangenol Isolated from the Leaves of Hydrangea serrata Attenuates Wrinkle Formation and Repairs Skin Moisture in UVB-Irradiated Hairless Mice. Nutrients 2019, 11, 2354. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Placebo (n = 45) | WHS (n = 48) | p-Value |
|---|---|---|---|
| Sex (M/F) | 26/19 | 20/28 | 0.1204 1 |
| Age | 30.47 ± 9.62 | 32.71 ± 10.98 | 0.3189 2 |
| Drinker (Y/N) | 25/20 | 26/22 | 0.9363 3 |
| Smoker (Y/N) | 35/10 | 33/15 | 0.6810 3 |
| Variable | Period | Placebo (n = 45) | WHS (n = 48) | p-Value |
|---|---|---|---|---|
| Total cholesterol (mg/dL) | Week 0 | 196.80 ± 34.35 | 196.44 ± 34.70 | |
| Week 12 | 192.31 ± 26.88 | 198.00 ± 28.72 | ||
| Δ (0–12) | −4.49 ± 21.12 | 1.56 ± 23.12 | 0.1917 1 | |
| HDL-cholesterol (mg/dL) | Week 0 | 55.69 ± 12.61 | 58.52 ± 12.22 | |
| Week 12 | 53.84 ± 10.41 | 56.73 ± 11.78 | ||
| Δ (0–12) | −1.84 ± 7.56 | −1.79 ± 10.20 | 0.8716 2 | |
| LDL-cholesterol (mg/dL) | Week 0 | 128.67 ± 29.42 | 129.04 ± 31.48 | |
| Week 12 | 118.80 ± 23.19 # | 123.54 ± 25.39 | ||
| Δ (0–12) | −9.87 ± 21.14 | −5.50 ± 25.75 | 0.3755 1 | |
| Triglyceride (mg/dL) | Week 0 | 138.73 ± 112.89 | 115.19 ± 71.28 | |
| Week 12 | 124.24 ± 112.77 | 90.10 ± 52.55 # | ||
| Δ (0–12) | −14.49 ± 95.13 | −25.08 ± 63.71 | 0.3934 2 |
| Variable | Period | Placebo (n = 45) | WHS (n = 48) | p-Value 1 |
|---|---|---|---|---|
| Adiponectin (μg/mL) | Week 0 | 5.43 ± 1.94 | 6.18 ± 2.85 | |
| Week 12 | 4.88 ± 1.72 # | 6.00 ± 2.46 | ||
| Δ (0–12) | −0.55 ± 0.98 | −0.18 ± 1.92 | 0.1232 | |
| Leptin (ng/mL) | Week 0 | 10.20 ± 8.84 | 11.30 ± 7.63 | |
| Week 12 | 10.19 ± 8.77 | 10.09 ± 8.07 | ||
| Δ (0–12) | −0.01 ± 4.96 | −1.21 ± 5.73 | 0.4675 |
| Variable | Period | Placebo (n = 45) | WHS (n = 48) | p-Value |
|---|---|---|---|---|
| AST (U/L) | Week 0 | 23.85 ± 9.74 | 24.25 ± 8.52 | |
| Week 12 | 24.44 ± 9.49 | 29.62 ± 24.50 | ||
| Δ (0–12) | 0.17 ± 7.32 | 5.04 ± 25.05 | 0.8791 2 | |
| ALT (U/L) | Week 0 | 25.43 ± 16.79 | 26.60 ± 15.72 | |
| Week 12 | 24.33 ± 18.41 | 34.54 ± 64.83 | ||
| Δ (0–12) | −0.52 ± 9.34 | 8.10 ± 63.32 | 0.7455 2 | |
| γ-GTP (U/L) | Week 0 | 28.78 ± 18.66 | 27.13 ± 18.27 | |
| Week 12 | 29.42 ± 26.28 | 24.63 ± 19.21 | ||
| Δ (0–12) | 0.77 ± 13.26 | −2.17 ± 7.95 | 0.1433 2 | |
| Creatinine (mg/dL) | Week 0 | 0.73 ± 0.16 | 0.70 ± 0.15 | |
| Week 12 | 0.77 ± 0.19 | 0.73 ± 0.16 | ||
| Δ (0–12) | 0.03 ± 0.09 | 0.03 ± 0.06 | 0.9558 1 | |
| BUN (mg/dL) | Week 0 | 12.57 ± 3.51 | 12.38 ± 2.79 | |
| Week 12 | 12.57 ± 3.89 | 12.52 ± 3.57 | ||
| Δ (0–12) | 0.03 ± 3.07 | 0.18 ± 3.54 | 0.8495 2 | |
| hs-CRP (mg/L) | Week 0 | 2.48 ± 6.21 | 1.09 ± 1.09 | |
| Week 12 | 1.59 ± 2.88 | 1.22 ± 1.49 | ||
| Δ (0–12) | −0.90 ± 4.56 | 0.14 ± 0.86 | 0.7986 2 | |
| Systolic blood pressure (mmHg) | Week 0 | 130.22 ± 12.53 | 128.00 ± 11.42 | |
| Week 12 | 124.83 ± 13.14 | 123.46 ± 12.45 | ||
| Δ (0–12) | −6.60 ± 14.01 | −4.98 ± 12.55 | 0.4538 2 | |
| Diastolic blood pressure (mmHg) | Week 0 | 78.88 ± 10.48 | 78.12 ± 9.98 | |
| Week 12 | 75.50 ± 11.12 | 75.25 ± 9.52 | ||
| Δ (0–12) | −4.71 ± 11.35 | −2.73 ± 8.61 | 0.3266 1 | |
| Pulse (beats/min) | Week 0 | 83.03 ± 11.85 | 84.15 ± 11.62 | |
| Week 12 | 80.81 ± 13.36 | 81.02 ± 11.78 | ||
| Δ (0–12) | −3.48 ± 12.71 | −3.04 ± 12.14 | 0.8596 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, H.-S.; Chung, K.-S.; Shin, Y.-K.; Yu, J.-S.; Kang, S.-H.; Lee, S.-H.; Lee, K.-T. Effect of Standardized Hydrangea serrata (Thunb.) Ser. Leaves Extract on Body Weight and Body Fat Reduction in Overweight or Obese Humans: A Randomized Double-Blind Placebo-Controlled Study. Nutrients 2022, 14, 208. https://doi.org/10.3390/nu14010208
Han H-S, Chung K-S, Shin Y-K, Yu J-S, Kang S-H, Lee S-H, Lee K-T. Effect of Standardized Hydrangea serrata (Thunb.) Ser. Leaves Extract on Body Weight and Body Fat Reduction in Overweight or Obese Humans: A Randomized Double-Blind Placebo-Controlled Study. Nutrients. 2022; 14(1):208. https://doi.org/10.3390/nu14010208
Chicago/Turabian StyleHan, Hee-Soo, Kyung-Sook Chung, Yu-Kyong Shin, Jae-Sik Yu, Seung-Hyun Kang, Sun-Hee Lee, and Kyung-Tae Lee. 2022. "Effect of Standardized Hydrangea serrata (Thunb.) Ser. Leaves Extract on Body Weight and Body Fat Reduction in Overweight or Obese Humans: A Randomized Double-Blind Placebo-Controlled Study" Nutrients 14, no. 1: 208. https://doi.org/10.3390/nu14010208
APA StyleHan, H.-S., Chung, K.-S., Shin, Y.-K., Yu, J.-S., Kang, S.-H., Lee, S.-H., & Lee, K.-T. (2022). Effect of Standardized Hydrangea serrata (Thunb.) Ser. Leaves Extract on Body Weight and Body Fat Reduction in Overweight or Obese Humans: A Randomized Double-Blind Placebo-Controlled Study. Nutrients, 14(1), 208. https://doi.org/10.3390/nu14010208