
High Dose of Caffeine Mouth Rinse Increases Resistance Training Performance in Men

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
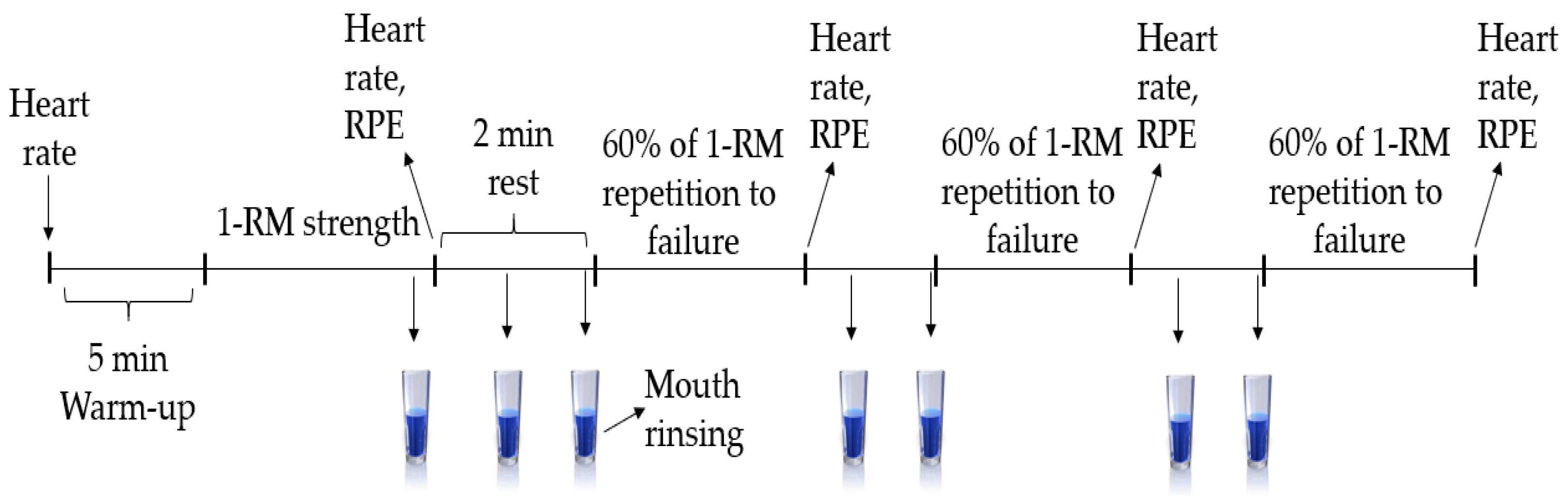
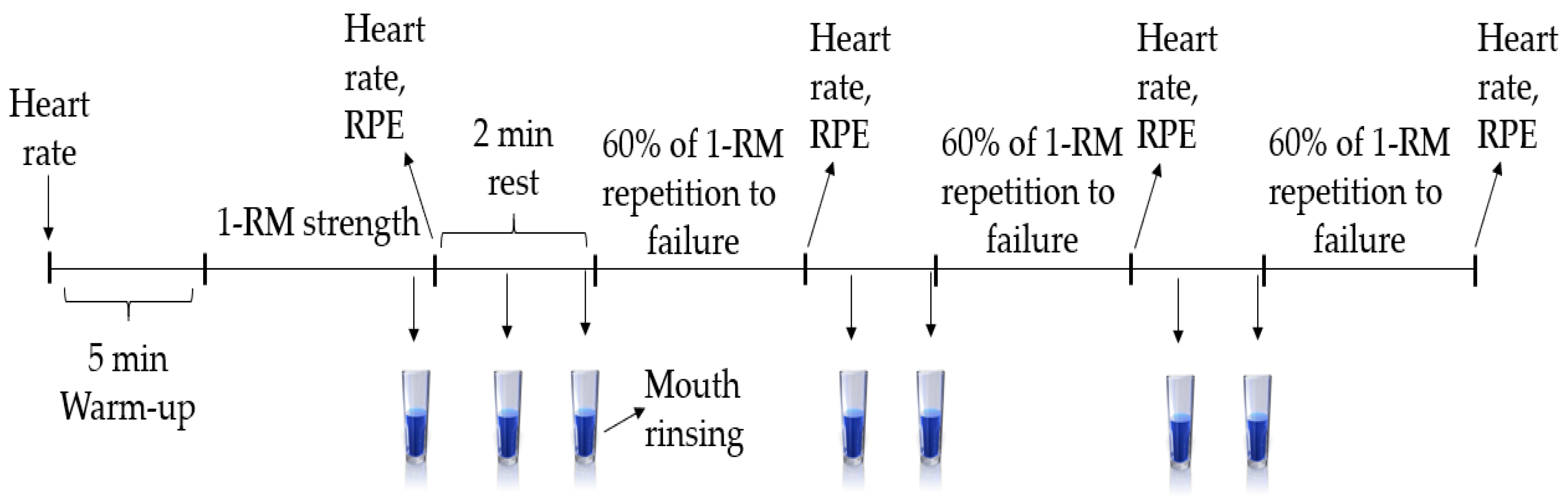
2.2. Study Design
2.3. Maximal Strength (1-RM) and 60% of 1-RM Muscular Endurance Test Protocol
2.4. Mouth Rinsing Protocol
2.5. Statistical Analysis
3. Results
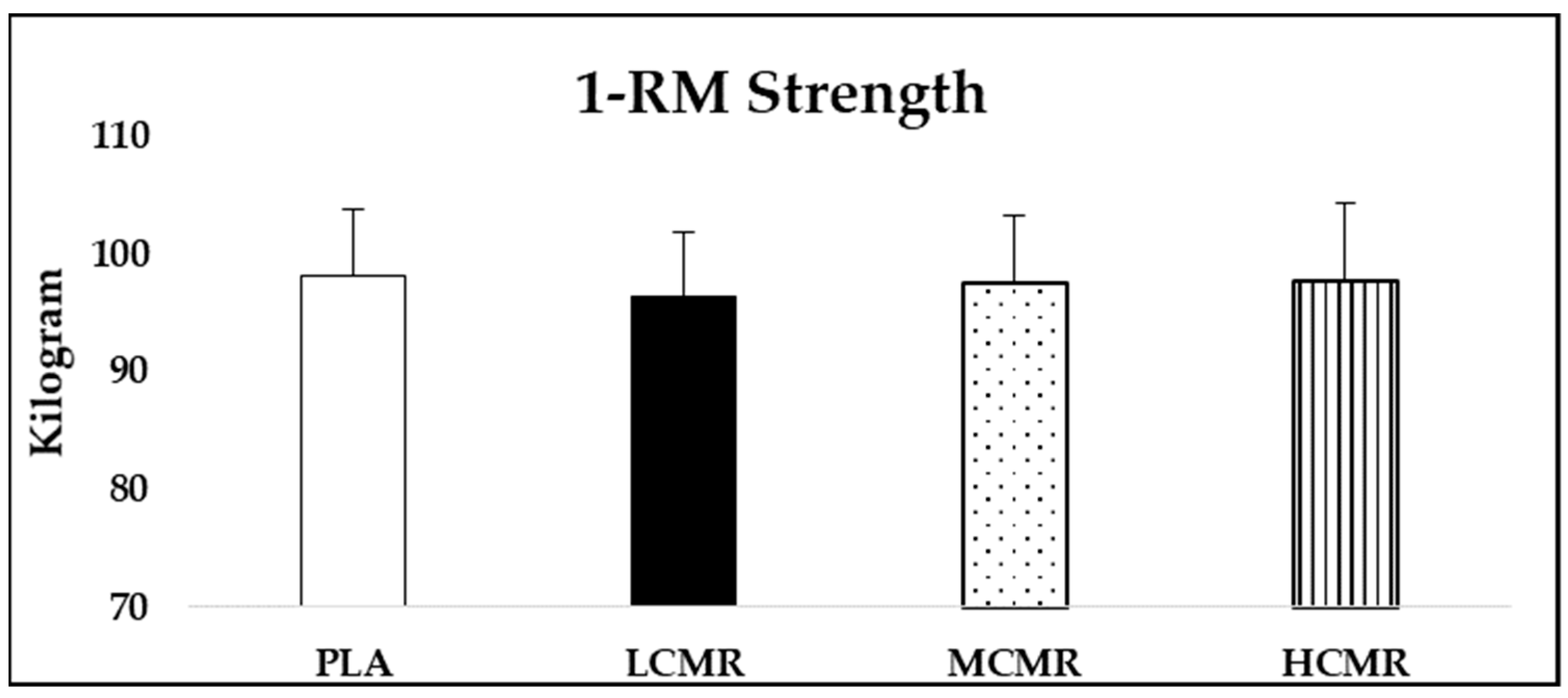
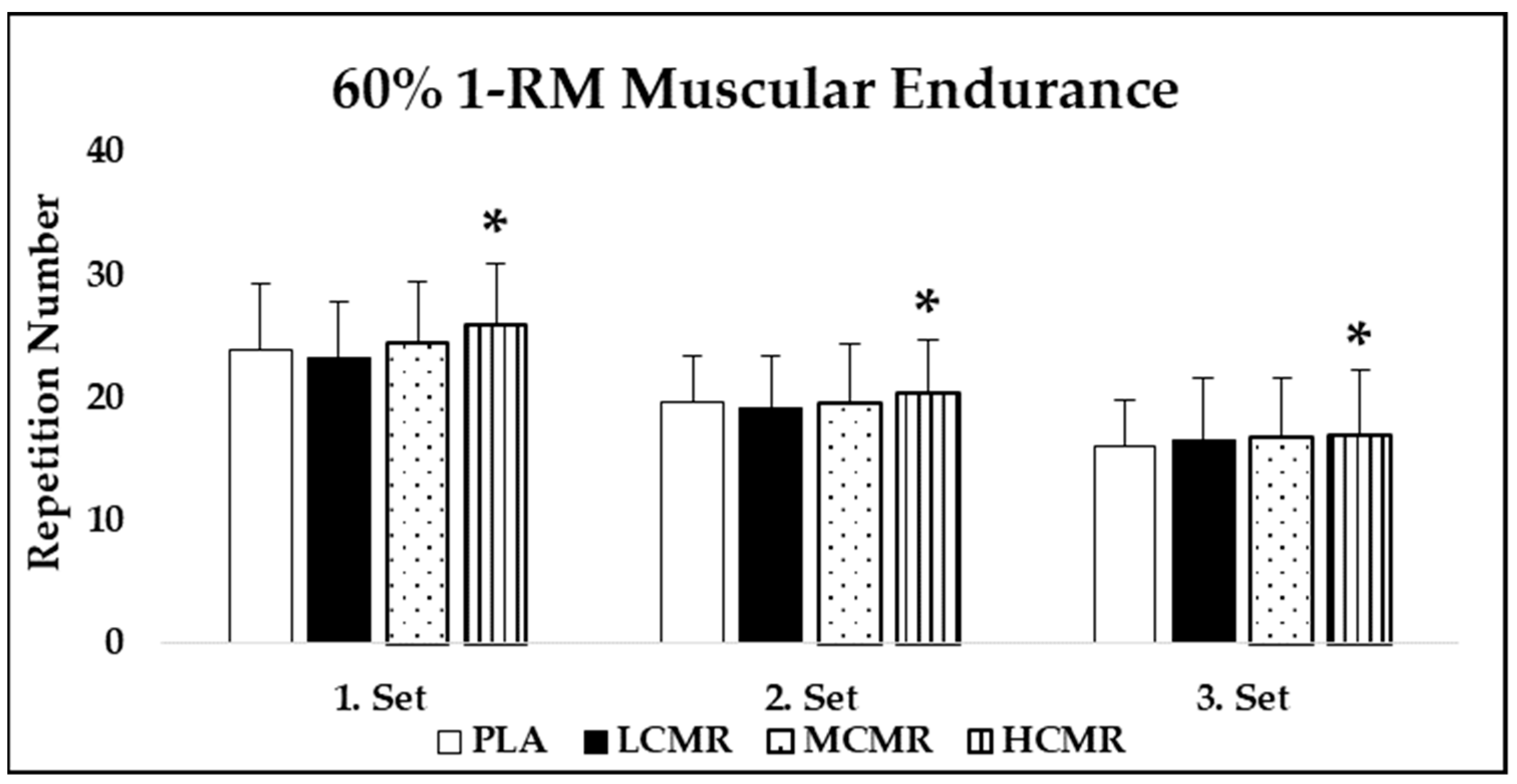
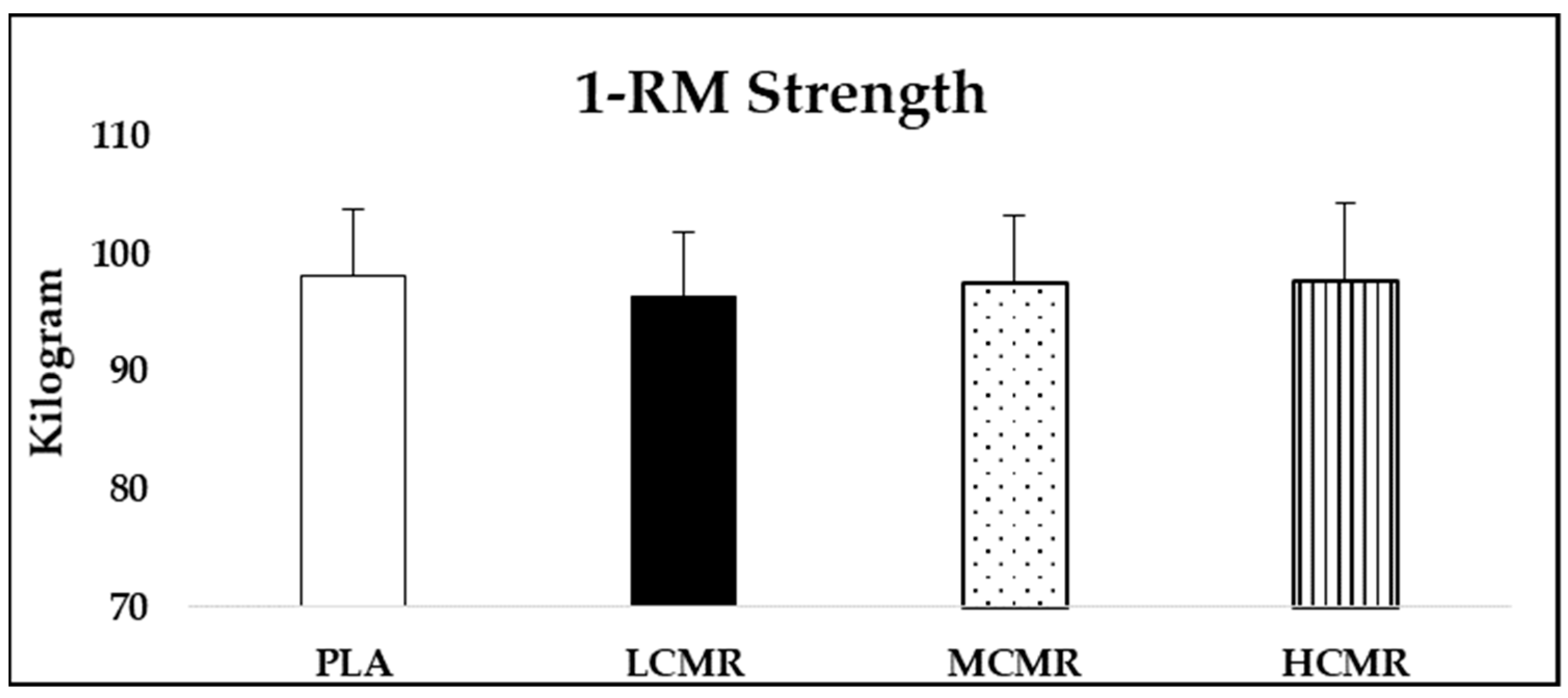
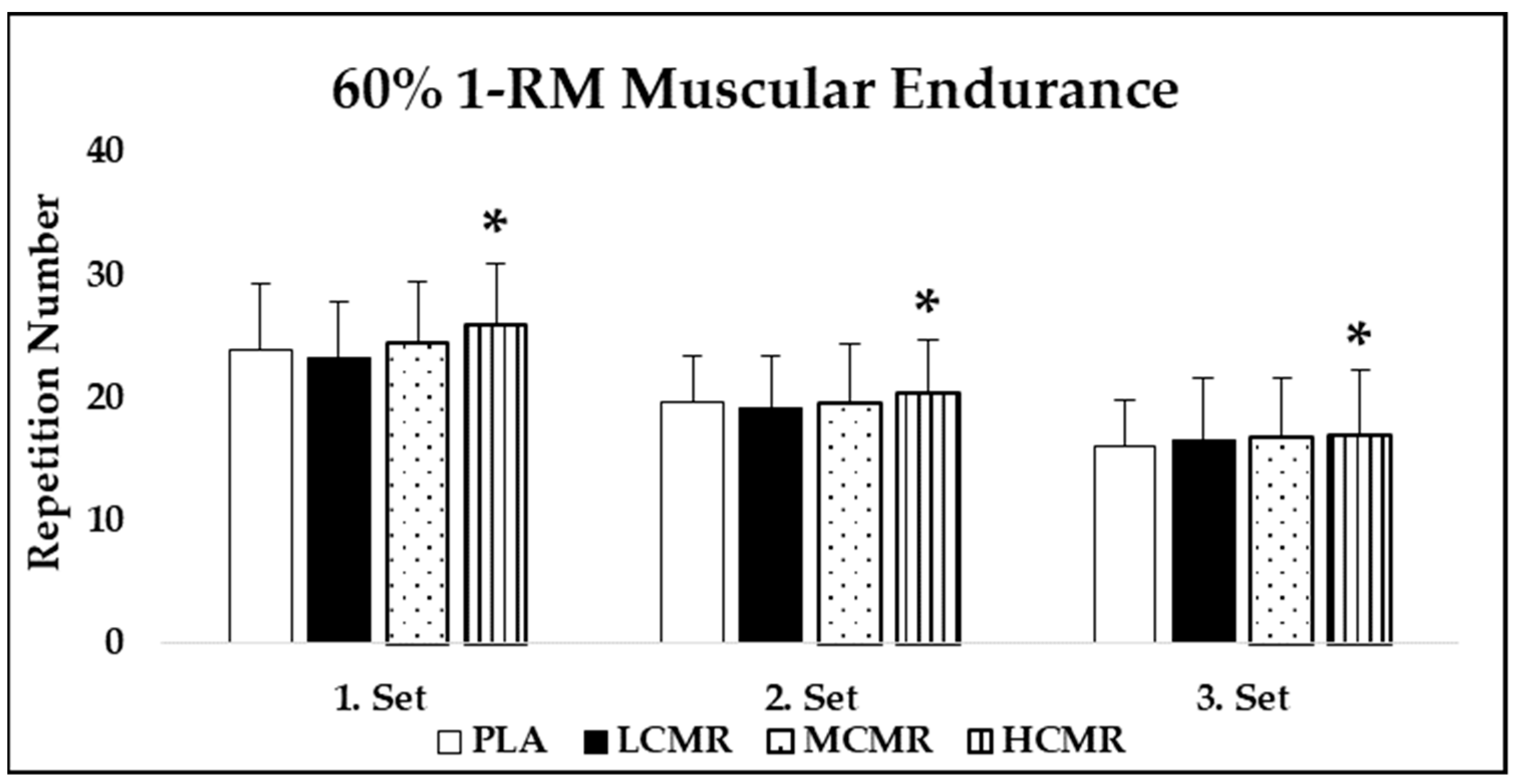
3.1. Strength (1-RM) and 60% of 1-RM Muscular Endurance Performance
3.2. Heart Rate and Ratings of Perceived Exertion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knapik, J.J.; Steelman, R.A.; Hoedebecke, S.S.; Austin, K.G.; Farina, E.K.; Lieberman, H.R. Prevalence of dietary supplement use by athletes: Systematic review and meta-analysis. Sports Med. 2016, 46, 103–123. [Google Scholar] [CrossRef] [Green Version]
- Southward, K.; Rutherfurd-Markwick, K.J.; Ali, A. The effect of acute caffeine ingestion on endurance performance: A systematic review and meta-analysis. Sports Med. 2018, 48, 1913–1928. [Google Scholar] [CrossRef]
- Raya-González, J.; Rendo-Urteaga, T.; Domínguez, R.; Castillo, D.; Rodríguez-Fernández, A.; Grgic, J. Acute effects of caffeine supplementation on movement velocity in resistance exercise: A systematic review and meta-analysis. Sports Med. 2020, 50, 717–729. [Google Scholar] [CrossRef]
- Grgic, J.; Trexler, E.T.; Lazinica, B.; Pedisic, Z. Effects of caffeine intake on muscle strength and power: A systematic review and meta-analysis. J. Int. Soc. Sports Nutr. 2018, 15, 11. [Google Scholar]
- Palito, M.D.; Souza, D.B.; Casonatto, J.; Farinatti, P. Acute effect of caffeine consumption on isotonic muscular strength and endurance: A systematic review and meta-analysis. Sci. Sports 2016, 31, 119–128. [Google Scholar]
- Karayigit, R.; Naderi, A.; Akca, F.; Cruz, C.J.G.D.; Sarshin, A.; Yasli, B.C.; Ersoz, G.; Kaviani, M. Effects of different doses of caffeinated coffee on muscular endurance, cognitive performance, and cardiac autonomic modulation in caffeine naïve female athletes. Nutrients 2021, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J. Effects of caffeine on resistance exercise: A review of recent research. Sports Med. 2021, 51, 2281–2298. [Google Scholar] [CrossRef]
- Karayigit, R.; Sahin, M.A.; Sari, C.; Sisman, A.; Yildiz, H.; Buyukcelebi, H.; Ersoz, G. The effects of low-dose caffeinated coffee ingestion on strength and muscular endurance performance in male athletes. Prog. Nutr. 2021, 23, e2021001. [Google Scholar]
- Waller, G.; Dolby, M.; Steele, J.; Fisher, J.P. A low caffeine dose improves maximal strength, but not relative muscular endurance in either heavier-or lighter-loads, or perceptions of effort or discomfort at task failure in females. PeerJ 2020, 8, e9144. [Google Scholar]
- Wilk, M.; Krzysztofik, M.; Filip, A.; Zajac, A.; Del Coso, J. The effects of high doses of caffeine on maximal strength and muscular endurance in athletes habituated to caffeine. Nutrients 2019, 11, 1912. [Google Scholar] [CrossRef] [Green Version]
- Grgic, J.; Sabol, F.; Venier, S.; Mikulic, I.; Bratkovic, N.; Schoenfeld, B.J.; Pickering, C.; Bishop, D.J.; Pedisic, Z.; Mikulic, P. What dose of caffeine to use: Acute effects of 3 doses of caffeine on muscle endurance and strength. Int. J. Sports Physiol. Perform. 2020, 15, 470–477. [Google Scholar] [CrossRef]
- Pallares, J.G.; Fernandez-Elias, V.E.; Ortega, J.F.; Munoz, G.; Munoz-Guerra, J.; Mora-Rodriguez, R. Neuromuscular responses to incremental caffeine doses: Performance and side effects. Med. Sci. Sports Exerc. 2013, 45, 2184–2192. [Google Scholar] [CrossRef]
- Wickham, K.A.; Spriet, L.L. Administration of caffeine in alternate forms. Sports Med. 2018, 48, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Ferraz da Silva, W.; Lopes-Silva, J.P.; Felippe, L.J.C.; Ferreira, G.A.; Lima-Silva, A.E.; Silva-Cavalcante, M.D. Is caffeine mouth rinsing an effective strategy to improve physical and cognitive performance? A systematic review. Crit. Rev. Food Sci. Nutr. 2021. [Google Scholar] [CrossRef]
- Kamimori, G.H.; Karyekar, C.S.; Otterstetter, R.; Cox, D.S.; Balkin, T.J.; Belenky, G.L.; Eddington, N.D. The rate of absorption and relative bioavailability of caffeine administered in chewing gum versus capsules to normal healthy volunteers. Int. J. Pharm. 2002, 234, 159–167. [Google Scholar] [CrossRef]
- Gam, S.; Guelfi, K.J.; Fournier, P.A. Mouth rinsing and ingesting a bitter solution improves sprint cycling performance. Med. Sci. Sports Exerc. 2014, 46, 1648–1657. [Google Scholar] [CrossRef]
- Pickering, C. Are caffeine’s performance-enhancing effects partially driven by its bitter taste? Med. Hypotheses 2019, 131, 109301. [Google Scholar] [PubMed]
- Beaven, C.M.; Maulder, P.; Pooley, A.; Kilduff, L.; Cook, C. Effects of caffeine and carbohydrate mouth rinses on repeated sprint performance. Appl. Physiol. Nutr. Metab. 2013, 38, 633–637. [Google Scholar] [CrossRef]
- Bottoms, L.; Hurst, H.; Scriven, A.; Lynch, F.; Bolton, J.; Vercoe, L.; Shore, Z.; Barry, G.; Sinclair, J. The effect of caffeine mouth rinse on self-paced cycling performance. Comp. Exerc. Physiol. 2014, 10, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Dolan, P.; Witherbee, K.E.; Peterson, K.M.; Kerksick, C.M. Effect of carbohydrate, caffeine, and carbohydrate+caffeine mouth rinsing on intermittent running performance in collegiate male lacrosse athletes. J. Strength Cond. Res. 2017, 31, 2473–2479. [Google Scholar] [CrossRef]
- Melo, A.A.; Bastos-Silva, V.J.; Moura, F.A.; Bini, R.R.; Lima-Silva, A.E.; Araujo, G.G. Caffeine mouth rinse enhances performance, fatigue tolerance and reduces muscle activity during moderate-intensity cycling. Biol. Sport 2021, 38, 517–523. [Google Scholar] [CrossRef]
- Doering, T.M.; Fell, J.W.; Leveritt, M.D.; Desbrow, B.; Shing, C.M. The effect of a caffeinated mouth-rinse on endurance cycling time-trial performance. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 90–97. [Google Scholar] [CrossRef]
- Ehlert, A.M.; Twiddy, H.M.; Wilson, P.B. The effects of caffeine mouth rinsing on exercise performance: A systematic review. Int. J. Sport Nutr. Exerc. Metab. 2020, 30, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; Davis, L.; Avela, J.; Hakkinen, K. Neuromuscular fatigue during dynamic maximal strength and hypertrophic resistance loadings. J. Electromyogr. Kinesiol. 2012, 22, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Smilios, I.; Hakkinen, K.; Tokmakidis, S.P. Power output and electromyographic activity during and after a moderate load muscular endurance session. J. Strength Cond. Res. 2010, 24, 2122–2131. [Google Scholar] [CrossRef]
- Clarke, N.D.; Kornilios, E.; Richardson, D.L. Carbohydrate and caffeine mouth rinses do not affect maximum strength and muscular endurance performance. J. Strength Cond. Res. 2015, 29, 2926–2931. [Google Scholar] [CrossRef] [Green Version]
- Clark, A.J. The reaction between acetyl choline and muscle cells. J. Physiol. 1926, 61, 530–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bühler, R.; Lachenmeier, D.W.; Schlegel, K.; Winkler, G. Development of a tool to assess the caffeine intake among teenagers and young adults. Ernahrungs Umschau. 2014, 61, 58–63. [Google Scholar]
- Filip, A.; Wilk, M.; Krzysztofik, M.; Del Coso, J. Inconsistency in the ergogenic effect of caffeine in athletes who regularly consume caffeine: Is it due to the disparity in the criteria that defines habitual caffeine intake? Nutrients 2020, 12, 1087. [Google Scholar] [CrossRef] [Green Version]
- Pataky, M.W.; Womack, C.J.; Saunders, M.J.; Goffe, J.L.; D’Lugos, A.C.; El-sohemy, A.; Luden, N.D. Caffeine and 3-km cycling performance: Effects of mouth rinsing, genotype, and time of day. Scand. J. Med. Sci. Sports 2016, 26, 613–619. [Google Scholar] [CrossRef]
- Kizzi, J.; Sum, A.; Houston, F.E.; Lawrence, D.H. Influence of a caffeine mouth rinse on sprint cycling following glycogen depletion. Eur. J. Sport Sci. 2016, 16, 1087–1094. [Google Scholar] [CrossRef] [Green Version]
- Borg, G. Perceived exertion: A note on history and methods. Med. Sci. Sports Exerc. 1973, 5, 90–93. [Google Scholar] [CrossRef]
- Karayigit, R.; Forbes, S.C.; Naderi, A.; Candow, D.G.; Yildirim, U.C.; Akca, F.; Aras, D.; Yasli, B.C.; Sisman, A.; Mor, A.; et al. Different doses of carbohydrate mouth rinse have no effect on exercise performance in resistance trained women. Int. J. Environ. Res. Public Health 2021, 18, 3463. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.T.; Farias da Silva, J.V.; Bueno, N.B. Effects of caffeine supplementation on muscle endurance, maximum strength, and perceived exertion in adults submitted to strength training: A systematic review and meta-analyses. Crit. Rev. Food. Sci. Nutr. 2021, 61, 2587–2600. [Google Scholar] [CrossRef]
- Grgic, J.; Del Coso, J. Ergogenic effects of acute caffeine intake on muscular endurance and muscular strength in women: A meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 5773. [Google Scholar] [CrossRef]
- Norum, M.; Risvang, L.C.; Bjornsen, T.; Dimitriou, L.; Ronning, P.O.; Bjorgen, M.; Raastad, T. Caffeine increases strength and power performance in resistance-trained females during early follicular phase. Scand. J. Med. Sci. Sports 2020, 30, 2116–2129. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.L.; Park, N.D.; Maresca, R.D.; McKibans, K.I.; Millard-Stafford, M.L. Effect of caffeine ingestion on muscular strength and endurance: A meta-analysis. Med. Sci. Sports Exerc. 2010, 42, 1375–1387. [Google Scholar] [CrossRef]
- Shield, A.; Zhou, S. Assessing voluntary muscle activation with the twitch interpolation technique. Sports Med. 2004, 34, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Bazzucchi, I.; Felici, F.; Macaluso, A.; De Vito, G. Differences between young and older women in maximal force, force fluctuations, and surface EMG during isometric knee extension and elbow flexion. Muscle Nerve 2004, 30, 626–635. [Google Scholar] [PubMed]
- De Pauw, K.; Roelands, B.; Knaepen, K.; Polfliet, M.; Stiens, J.; Meeusen, R. Effects of caffeine and maltodextrin mouth rinsing on p300, brain imaging, and cognitive performance. J. Appl. Physiol. 2015, 118, 776–782. [Google Scholar] [CrossRef]
- Marinho, A.H.; Mendes, E.V.; Vilela, R.A.; Bastos-Silva, V.J.; Araujo, G.G.; Balikian, P. Caffeine mouth rinse has no effects on anaerobic energy yield during a Wingate test. J. Sports Med. Phys. Fitness 2020, 60, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Karuk, H.N.; Nalcakan, G.R.; Pekünlü, E. Effects of carbohydrate and caffeine combination mouth rinse on anaerobic performance of highly trained male athletes. Eur. J. Sport Sci. 2021. [Google Scholar] [CrossRef]
- Haase, L.; Cerf-Ducastel, B.; Murphy, C. Cortical activation in response to pure taste stimuli during the physiological states of hunger and satiety. Neuroimage 2009, 44, 1008–1021. [Google Scholar] [PubMed] [Green Version]
- Figueiredo, N.; Queiroz, M.; Felicio, F.P.; Ferreira, J.; Gerosa-Neto, J.; Mota, J.F.; da Silva, R.; Ghedini, P.C.; Saunders, B.; Pimentel, G.D. Acute caffeine mouth rinsing does not improve 10-km running performance in CYP1A2 C-allele carriers. Clin. Nutr. Espen. 2021, 42, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Fernando, P.B.; Davis, R.R.; Per, A.; Luis, S.M.; Juan, R.S.; Ricardo, M.S.; Carlos, Q.E.; Juan Manuel, Y.G.; Juan Jose, G.B. Time course of recovery from resistance exercise with different set configurations. J. Strength Cond. Res. 2020, 34, 2867–2876. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| PLA | LCMR | MCMR | HCMR | |||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |
| Heart Rate (Beat/min) | ||||||||
| Pre-Test | 63.57 | 5.13 | 67.78 | 5.78 | 63.85 | 4.63 | 63.57 | 4.76 |
| Post 1-RM | 134.85 | 17.62 | 133.00 | 14.30 | 132.92 | 14.45 | 130.50 | 14.58 |
| 1. set | 144.64 | 16.91 | 150.00 | 15.52 | 146.78 | 14.69 | 153.85 | 11.09 |
| 2. set | 155.92 | 12.65 | 156.78 | 9.72 | 154.64 | 11.90 | 154.50 | 13.23 |
| 3. set | 157.57 | 10.01 | 159.28 | 15.61 | 157.85 | 12.00 | 154.35 | 12.99 |
| Ratings of Perceived Exertion (RPE) (6–20) | ||||||||
| Post 1-RM | 14.78 | 1.52 | 14.78 | 1.71 | 15.42 | 1.22 | 15.00 | 1.24 |
| 1. set | 18.42 | 1.39 | 18.57 | 1.78 | 18.21 | 1.36 | 17.50 * | 1.22 |
| 2. set | 18.92 | 1.49 | 18.78 | 1.12 | 18.57 | 0.85 | 17.71 * | 1.20 |
| 3. set | 18.92 | 1.54 | 19.07 | 1.59 | 19.35 | 0.92 | 18.00 * | 1.56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karayigit, R.; Koz, M.; Sánchez-Gómez, A.; Naderi, A.; Yildirim, U.C.; Domínguez, R.; Gur, F. High Dose of Caffeine Mouth Rinse Increases Resistance Training Performance in Men. Nutrients 2021, 13, 3800. https://doi.org/10.3390/nu13113800
Karayigit R, Koz M, Sánchez-Gómez A, Naderi A, Yildirim UC, Domínguez R, Gur F. High Dose of Caffeine Mouth Rinse Increases Resistance Training Performance in Men. Nutrients. 2021; 13(11):3800. https://doi.org/10.3390/nu13113800
Chicago/Turabian StyleKarayigit, Raci, Mitat Koz, Angela Sánchez-Gómez, Alireza Naderi, Ulas Can Yildirim, Raúl Domínguez, and Fatih Gur. 2021. "High Dose of Caffeine Mouth Rinse Increases Resistance Training Performance in Men" Nutrients 13, no. 11: 3800. https://doi.org/10.3390/nu13113800
APA StyleKarayigit, R., Koz, M., Sánchez-Gómez, A., Naderi, A., Yildirim, U. C., Domínguez, R., & Gur, F. (2021). High Dose of Caffeine Mouth Rinse Increases Resistance Training Performance in Men. Nutrients, 13(11), 3800. https://doi.org/10.3390/nu13113800