
Themes in Train-the-Trainer Nutrition Education Interventions Targeting Middle School Students: A Systematic Review

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
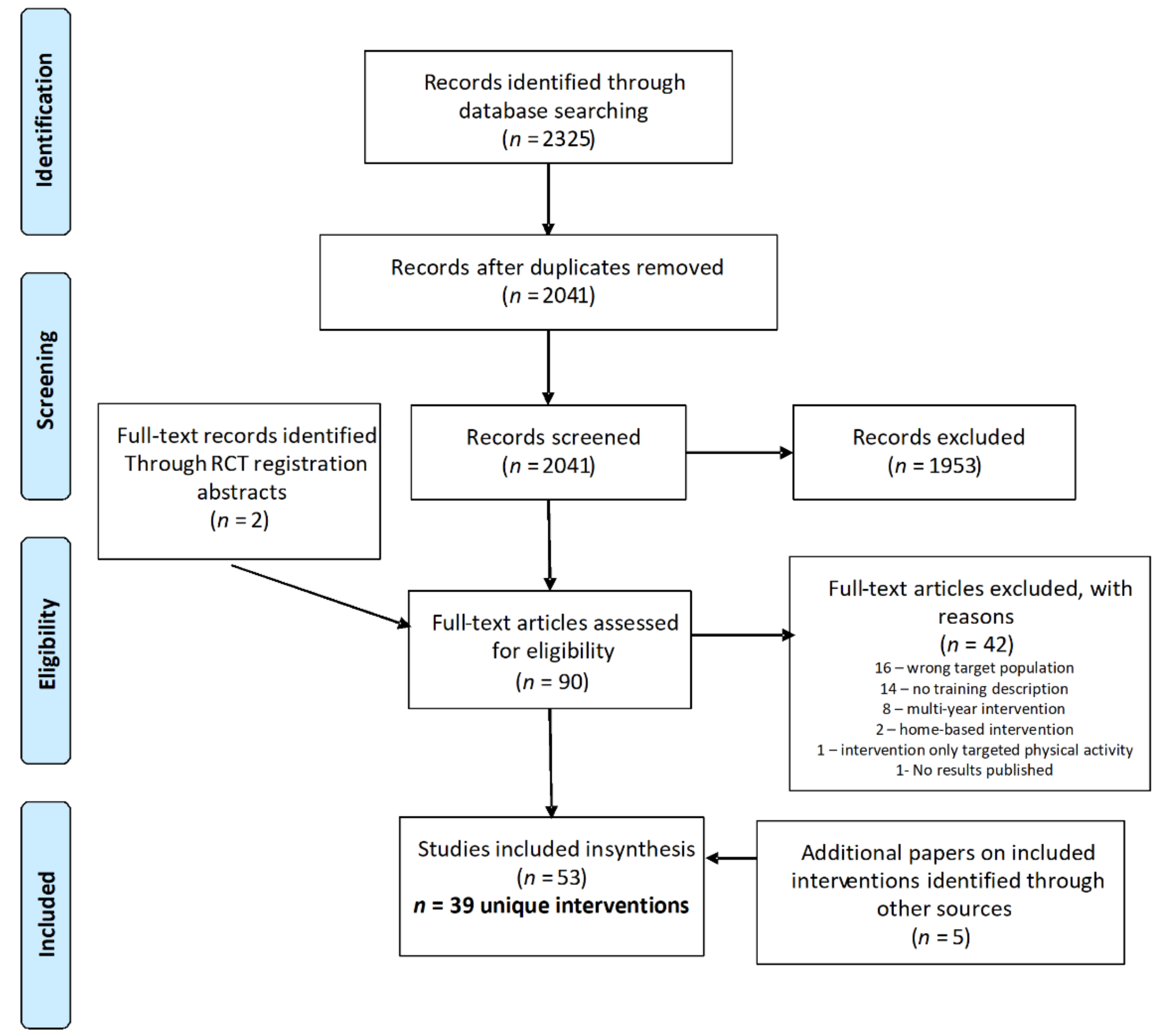
2.2. Secreening and Selection Process
2.3. Data Extraction and Synthesis Approach
2.4. Quality Assessment
3. Results
3.1. Group A: Classroom-Based Interventions That Trained Adults
3.2. Group B: Classroom-Based Interventions That Trained Cross-Age Peers
3.3. Group C: Classroom-Based Intereventions That Trained Same-Age Peers
3.4. Group D: Community, Afterschool, or Extracurricular Interventions That Trained Adults
3.5. Group E: Community, Afterschool or Extracurricular Interventions That Trained Cross-Age Peers
3.6. Group F: Community, Afterschool or Extracurricular Interventions That Trained Same-Age Peers
4. Discussion
4.1. Limitations
4.2. Application of Findings
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Herman, K.M.; Craig, C.L.; Gauvin, L.; Katzmarzyk, P.T. Tracking of obesity and physical activity from childhood to adulthood: The Physical Activity Longitudinal Study. Int. J. Pediatr. Obes. 2009, 4, 281–288. [Google Scholar] [CrossRef]
- Megari, K. Quality of life in chronic disease patients. Health Psychol. Res. 2013, 1, e27. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief, No. 288; National Center for Health Statistics: Hyattsville, MD, USA, 2017. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Fakhouri, T.H.; Hales, C.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity among Youths by Household Income and Education Level of Head of Household—United States 2011–2014. MMWR Morb. Mortal Wkly. Rep. 2018, 67, 186–189. [Google Scholar] [CrossRef]
- National Survey of Children’s Health Interactive Data Query: 2018–2019 National Survey of Children’s Health. Baltimore, MD: Data Resource Center for Child and Adolescent Health. Available online: https://www.childhealthdata.org/browse/survey/results?q=7620&r=1 (accessed on 10 March 2021).
- Kim, S.A.; Moore, L.V.; Galuska, D. Vital Signs: Fruit and vegetable intake among children—United States, 2003–2010. MMWR 2014, 63, 671–676. [Google Scholar] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among children age 4–13 years in the United States: Analyses of 2005–2010 NHANES data. Nutr. J. 2013, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rodrigo, C.; Wind, M.; Hildonen, C.; Bjelland, M.; Aranceta, J.; Klepp, K.-I.; Brug, J. The Pro Children Intervention: Applying the Intervention Mapping Protocol to Develop a School-Based Fruit and Vegetable Promotion Programme. Ann. Nutr. Metab. 2005, 49, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Jones, H.; Campbell, R. Obesity prevention and the Health promoting Schools framework: Essential components and barriers to success. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–17. [Google Scholar] [CrossRef]
- Kamath, C.C.; Vickers, K.S.; Ehrlich, A.; McGovern, L.; Johnson, J.; Singhal, V.; Paulo, R.; Hettinger, A.; Erwin, P.J.; Montori, V.M. Behavioral Interventions to Prevent Childhood Obesity: A Systematic Review and Metaanalyses of Randomized Trials. J. Clin. Endocrinol. Metab. 2008, 93, 4606–4615. [Google Scholar] [CrossRef] [PubMed]
- Meiklejohn, S.; Ryan, L.; Palermo, C. A Systematic Review of the Impact of Multi-Strategy Nutrition Education Programs on Health and Nutrition of Adolescents. J. Nutr. Educ. Behav. 2016, 48, 631–646.e1. [Google Scholar] [CrossRef]
- Murimi, M.W.; Moyeda-Carabaza, A.F.; Nguyen, B.; Saha, S.; Amin, R.; Njike, V. Factors that contribute to effective nutrition education interventions in children: A systematic review. Nutr. Rev. 2018, 76, 553–580. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Cherry, M.G.; Smith, H.; Perkins, E.; Boland, A. Reviewing Qualitative Evidence. In Doing a Systematic Review: A Student’s Guide, 2nd ed.; Boland, A., Cherry, M.G., Dicksson, R., Eds.; Sage Publications: London, UK, 2017; Chapter 11; pp. 193–222. [Google Scholar]
- Oliver, S.R.; Rees, R.; Clarke-Jones, L.; Milne, R.; Oakley, A.R.; Gabbay, J.; Stein, K.; Buchanan, P.; Gyte, G. A multidimensional conceptual framework for analysing public involvement in health services research. Health Expect. 2008, 11, 72–84. [Google Scholar] [CrossRef]
- Oliver, S.; Clarke-Jones, L.; Rees, R.; Milne, R.; Buchanan, P.; Gabbay, J.; Gyte, G.; Oakley, A.; Stein, K. Involving consumers in research and development agenda setting for the NHS: Developing an evidence-based approach. Health Technol. Assess. 2004, 8, 1–148. [Google Scholar] [CrossRef]
- Brunton, G.; Oliver, S.; Thomas, J. Innovations in framework synthesis as a systematic review method. Res. Synth. Methods 2020, 11, 316–330. [Google Scholar] [CrossRef] [PubMed]
- Noyes, J.; Booth, A.; Cargo, M. Qualitative evidence. In Cochrane Handbook for Systematic Reviews of Interventions, Version 6.2; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021; Chapter 21; updated on February 2021; Available online: www.training.cochrane.org/handbook (accessed on 23 July 2021).
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed on 23 July 2021).
- Carroll, C.; Booth, A.; Lloyd-Jones, M. Should We Exclude Inadequately Reported Studies from Qualitative Systematic Reviews? An Evaluation of Sensitivity Analyses in Two Case Study Reviews. Qual. Health Res. 2012, 22, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Arlinghaus, K.R.; Moreno, J.; Reesor, L.; Hernandez, D.C.; Johnston, C.A. Compañeros: High School Students Mentor Middle School Students to Address Obesity Among Hispanic Adolescents. Prev. Chronic Dis. 2017, 14, E92. [Google Scholar] [CrossRef][Green Version]
- Baskin, M.L.; Zunker, C.; Worley, C.B.; Dial, B.; Kimbrough, L. Design and implementation of a pilot obesity prevention program in a low-resource school. Health Educ. 2008, 109, 66–85. [Google Scholar] [CrossRef]
- Bell, S.L.; Audrey, S.; Cooper, A.; Noble, S.; Campbell, R. Lessons from a peer-led obesity prevention programme in English schools. Health Promot. Int. 2017, 32, 250–259. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Cowgill, B.O.; Klein, D.J.; Hawes-Dawson, J.; Uyeda, K.; Schuster, M.A. Two-Year BMI Outcomes From a School-Based Intervention for Nutrition and Exercise: A Randomized Trial. Pediatrics 2016, 137, e20152493. [Google Scholar] [CrossRef]
- Bogart, L.M.; Cowgill, B.O.; Elliott, M.N.; Klein, D.J.; Hawes-Dawson, J.; Uyeda, K.; Elijah, J.; Binkle, D.G.; Schuster, M.A. A Randomized Controlled Trial of Students for Nutrition and eXercise: A Community-Based Participatory Research Study. J. Adolesc. Health 2014, 55, 415–422. [Google Scholar] [CrossRef]
- Bogart, L.M.; Elliott, M.N.; Uyeda, K.; Hawes-Dawson, J.; Klein, D.J.; Schuster, M.A. Preliminary Healthy Eating Outcomes of SNaX, a Pilot Community-Based Intervention for Adolescents. J. Adolesc. Health 2011, 48, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.; Fredericks, L.; Wylie-Rosett, J. Strategies to Promote High School Students’ Healthful Food Choices. J. Nutr. Educ. Behav. 2011, 43, 414–418. [Google Scholar] [CrossRef][Green Version]
- Contento, I.R.; Koch, P.A.; Lee, H.; Calabrese-Barton, A. Adolescents Demonstrate Improvement in Obesity Risk Behaviors after Completion of Choice, Control & Change, a Curriculum Addressing Personal Agency and Autonomous Motivation. J. Am. Diet. Assoc. 2010, 110, 1830–1839. [Google Scholar] [CrossRef] [PubMed]
- Contento, I.R.; Koch, P.A.; Lee, H.; Sauberli, W.; Calabrese-Barton, A. Enhancing Personal Agency and Competence in Eating and Moving: Formative Evaluation of a Middle School Curriculum—Choice, Control, and Change. J. Nutr. Educ. Behav. 2007, 39, S179–S186. [Google Scholar] [CrossRef]
- Gray, H.L.; Contento, I.R.; Koch, P.A.; Di Noia, J. Mediating Mechanisms of Theory-Based Psychosocial Determinants on Behavioral Changes in a Middle School Obesity Risk Reduction Curriculum Intervention, Choice, Control, and Change. Child Obes. 2016, 12, 348–359. [Google Scholar] [CrossRef]
- Gray, H.L.; Contento, I.R.; Koch, P.A. Linking implementation process to intervention outcomes in a middle school obesity prevention curriculum, ‘Choice, Control and Change’. Health Educ. Res. 2015, 30, 248–261. [Google Scholar] [CrossRef]
- Lee, H.; Contento, I.R.; Koch, P. Using a Systematic Conceptual Model for a Process Evaluation of a Middle School Obesity Risk-Reduction Nutrition Curriculum Intervention: Choice, Control & Change. J. Nutr. Educ. Behav. 2013, 45, 126–136. [Google Scholar] [CrossRef]
- Dubuy, V.; De Cocker, K.; De Bourdeaudhuij, I.; Maes, L.; Seghers, J.; Lefevre, J.; De Martelaer, K.; Brooke, H.; Cardon, G. Evaluation of a real world intervention using professional football players to promote a healthy diet and physical activity in children and adolescents from a lower socio-economic background: A controlled pretest-posttest design. BMC Public Health 2014, 14, 457. [Google Scholar] [CrossRef][Green Version]
- Duncan, S.; Stewart, T.; McPhee, J.; Borotkanics, R.; Prendergast, K.; Zinn, C.; Meredith-Jones, K.; Taylor, R.; McLachlan, C.; Schofield, G. Efficacy of a compulsory homework programme for increasing physical activity and improving nutrition in children: A cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–12. [Google Scholar] [CrossRef]
- El Rayess, F.; Gandhi, M.; Mennillo, H. Mark, Set, Go! School-Based Nutrition and Physical Activity Program: A Five-Year Evaluation. Rhode Isl. Med. J. 2017, 100, 39–44. [Google Scholar]
- Fahlman, M.M.; Dake, J.A.; McCaughtry, N.; Martin, J. A Pilot Study to Examine the Effects of a Nutrition Intervention on Nutrition Knowledge, Behaviors, and Efficacy Expectations in Middle School Children. J. Sch. Health 2008, 78, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Hackett, A.F.; Davies, I.G.; Gobbi, R.; Mackintosh, K.A.; Warburton, G.L.; Stratton, G.; Van Sluijs, E.M.; Boddy, L.M. Promoting healthy weight in primary school children through physical activity and nutrition education: A pragmatic evaluation of the CHANGE! Randomised intervention study. BMC Public Health 2013, 13, 626. [Google Scholar] [CrossRef]
- Foley, B.C.; Shrewsbury, V.A.; Hardy, L.L.; Flood, V.M.; Byth, K.; Shah, S. Evaluation of a peer education program on student leaders’ energy balance-related behaviors. BMC Public Health 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- Franken, S.C.M.; Smit, C.R.; Buijzen, M. Promoting Water Consumption on a Caribbean Island: An Intervention Using Children’s Social Networks at Schools. Int. J. Environ. Res. Public Health 2018, 15, 713. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Dennisuk, L.A.; Christiansen, K.; Bhimani, R.; Johnson, A.; Alexander, E.; Lee, M.; Lee, S.H.; Rowan, M.; Coutinho, A.J. Development and implementation of Baltimore Healthy Eating Zones: A youth-targeted intervention to improve the urban food environment. Health Educ. Res. 2013, 28, 732–744. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Steeves, E.A.; Mui, Y.; Kharmats, A.Y.; Hopkins, L.C.; Dennis, D. B’More Healthy Communities for Kids: Design of a multi-level intervention for obesity prevention for low-income African American children. BMC Public Health 2014, 14, 942. [Google Scholar] [CrossRef] [PubMed]
- Sato, P.M.; Steeves, E.A.; Carnell, S.; Cheskin, L.J.; Trude, A.C.; Shipley, C.; Ruiz, M.J.M.; Gittelsohn, J. A youth mentor-led nutritional intervention in urban recreation centers: A promising strategy for childhood obesity prevention in low-income neighborhoods. Health Educ. Res. 2016, 31, 195–206. [Google Scholar] [CrossRef]
- Trude, A.C.B.; Steeves, E.A.; Shipley, C.; Surkan, P.J.; Sato, P.D.M.; Estep, T.; Clanton, S.; Lachenmayr, L.; Gittelsohn, J. A Youth-Leader Program in Baltimore City Recreation Centers: Lessons Learned and Applications. Health Promot. Pract. 2018, 19, 75–85. [Google Scholar] [CrossRef]
- Steeves, E.A.; Trude, A.C.B.; Ruggiero, C.F.; Ruiz, M.J.M.; Jones-Smith, J.; Porter, K.P.; Cheskin, L.; Hurley, K.; Hopkins, L.; Gittelsohn, J. Perceptions and Impact of a Youth-led Childhood Obesity Prevention Intervention among Youth-leaders. J. Hunger. Environ. Nutr. 2019, 16, 213–234. [Google Scholar] [CrossRef]
- Heo, M.; Jimenez, C.C.; Lim, J.; Isasi, C.R.; Blank, A.E.; Lounsbury, D.W.; Fredericks, L.; Bouchard, M.; Faith, M.S.; Wylie-Rosett, J.; et al. Effective nationwide school-based participatory extramural program on adolescent body mass index, health knowledge and behaviors. BMC Pediatr. 2018, 18, 7. [Google Scholar] [CrossRef]
- Irwin, C.; Irwin, R.; Richey, P.; Miller, M.; Boddie, J.; Dickerson, T. Get fit with the Grizzlies: A community-school-home initiative to fight childhood obesity led by a professional sports organization. Stud. Health Technol. Inform. 2012, 172, 163–167. [Google Scholar]
- Irwin, C.C.; Miller, M.E.; Somes, G.W.; Richey, P.A.; Irwin, R.L. Get Fit with the Grizzlies: A Community-School-Home Initiative to Fight Childhood Obesity. J. Sch. Health 2010, 80, 333–339. [Google Scholar] [CrossRef]
- Jackson, C.J.; Mullis, R.M.; Hughes, M. Development of a theater-based nutrition and physical activity intervention for low-income, urban, African American adolescents. Prog. Community Health Partnersh. Res. Educ. Action 2010, 4, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Kipping, R.R.; Howe, L.; Jago, R.; Campbell, R.; Wells, S.; Chittleborough, C.; Mytton, J.; Noble, S.M.; Peters, T.; Lawlor, D.A. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ 2014, 348, g3256. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Jago, R.; Noble, S.M.; Chittleborough, C.R.; Campbell, R.; Mytton, J.; Howe, L.D.; Peters, T.J.; Kipping, R.R. The Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial: Study protocol for a randomized controlled trial. Trials 2011, 12, 181. [Google Scholar] [CrossRef]
- Koch, P.A.; Contento, I.R.; Gray, H.L.; Burgermaster, M.; Bandelli, L.; Abrams, E.; Di Noia, J. Food, Health, & Choices: Curriculum and Wellness Interventions to Decrease Childhood Obesity in Fifth-Graders. J. Nutr. Educ. Behav. 2019, 51, 440–455. [Google Scholar] [CrossRef]
- Kohlstadt, I.; Gittelsohn, J.; Fang, Y. NutriBee Intervention Improves Diet and Psychosocial Outcomes by Engaging Early Adolescents from Diverse and Disadvantaged Communities. J. Am. Coll. Nutr. 2016, 35, 1–9. [Google Scholar] [CrossRef]
- Kohlstadt, I.C.; Steeves, E.T.A.; Rice, K.; Gittelsohn, J.; Summerfield, L.M.; Gadhoke, P. Youth peers put the “invent” into NutriBee’s online intervention. Nutr. J. 2015, 14, 1–8. [Google Scholar] [CrossRef]
- Lepe, S.; Goodwin, J.; Mulligan, K.T.; Balestracci, K.; Sebelia, L.; Greene, G. Process Evaluation of a Policy, Systems, and Environmental Change Intervention in an Urban School District. J. Nutr. Educ. Behav. 2019, 51, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Leung, M.M.; Agaronov, A.; Entwistle, T.; Harry, L.; Sharkey-Buckley, J.; Freudenberg, N. Voices through Cameras. Health Promot. Pract. 2016, 18, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hu, X.; Zhang, Q.; Liu, A.; Fang, H.; Hao, L.; Duan, Y.; Xu, H.; Shang, X.; Ma, J.; et al. The nutrition-based comprehensive intervention study on childhood obesity in China (NISCOC): A randomised cluster controlled trial. BMC Public Health 2010, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Li, Y.; Zhang, Q.; Hu, X.L.; Liu, A.; Du, S.; Li, T.; Guo, H.; Li, Y.; Xu, G.; et al. Comprehensive school-based intervention to control overweight and obesity in China: A cluster randomized controlled trial. Asia Pac. J. Clin. Nutr. 2017, 26, 1139–1151. [Google Scholar]
- Linton, L.S.; Edwards, C.C.; Woodruff, S.I.; Millstein, R.A.; Moder, C. Youth Advocacy as a Tool for Environmental and Policy Changes That Support Physical Activity and Nutrition: An Evaluation Study in San Diego County. Prev. Chronic Dis. 2014, 11, E46. [Google Scholar] [CrossRef]
- Lo, E.; Coles, R.; Humbert, M.L.; Polowski, J.; Henry, C.J.; Whiting, S.J. Beverage intake improvement by high school students in Saskatchewan, Canada. Nutr. Res. 2008, 28, 144–150. [Google Scholar] [CrossRef]
- Luesse, H.B.; Luesse, J.E.; Lawson, J.; Koch, P.A.; Contento, I.R. In Defense of Food Curriculum: A Mixed Methods Outcome Evaluation in Afterschool. Health Educ. Behav. 2019, 46, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Mihas, C.; Mariolis, A.; Manios, Y.; Naska, A.; Arapaki, A.; Mariolis-Sapsakos, T.; Tountas, Y. Evaluation of a nutrition intervention in adolescents of an urban area in Greece: Short- and long-term effects of the VYRONAS study. Public Health Nutr. 2009, 13, 712–719. [Google Scholar] [CrossRef]
- Molaison, E.F.; Connell, C.L.; Stuff, J.E.; Yadrick, M.K.; Bogle, M. Influences on Fruit and Vegetable Consumption by Low-Income Black American Adolescents. J. Nutr. Educ. Behav. 2005, 37, 246–251. [Google Scholar] [CrossRef]
- Necheles, J.W.; Chung, E.Q.; Hawes-Dawson, J.; Ryan, G.W.; Williams, S.B.; Holmes, H.N.; Wells, K.B.; Vaiana, M.E.; Schuster, M.A.; Williams, L.B. The Teen Photovoice Project: A Pilot Study to Promote Health Through Advocacy. Prog. Community Health Partnersh. Res. Educ. Action 2007, 1, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Olivares, S.; Zacarías, I.; Andrade, M.; Kain, J.; Lera, L.; Vio, F.; Morón, C. Nutrition Education in Chilean Primary Schools. Food Nutr. Bull. 2005, 26, S179–S185. [Google Scholar] [CrossRef]
- Saez, L.; Legrand, K.; Alleyrat, C.; Ramisasoa, S.; Langlois, J.; Muller, L.; Omorou, A.Y.; De Lavenne, R.; Kivits, J.; LeComte, E.; et al. Using facilitator—Receiver peer dyads matched according to socioeconomic status to promote behaviour change in overweight adolescents: A feasibility study. BMJ Open 2018, 8, e019731. [Google Scholar] [CrossRef] [PubMed]
- Smit, C.R.; de Leeuw, R.N.; Bevelander, K.E.; Burk, W.J.; Buijzen, M. A social network-based intervention stimulating peer influence on children’s self-reported water consumption: A randomized control trial. Appetite 2016, 103, 294–301. [Google Scholar] [CrossRef]
- Stock, S.; Miranda, C.; Evans, S.; Plessis, S.; Ridley, J.; Yeh, S.; Chanoine, J.-P. Healthy Buddies: A Novel, Peer-Led Health Promotion Program for the Prevention of Obesity and Eating Disorders in Children in Elementary School. Pediatrics 2007, 120, e1059–e1068. [Google Scholar] [CrossRef]
- Tamiru, D.; Argaw, A.; Gerbaba, M.; Ayana, G.; Nigussie, A.; Belachew, T. Effect of integrated school-based nutrition education on optimal dietary practices and nutritional status of school adolescents in Southwest of Ethiopia: A quasi-experimental study. Int. J. Adolesc. Med. Health 2016, 29, 20160015. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-Y.; Boonpleng, W.; McElmurry, B.J.; Park, C.G.; McCreary, L. Lessons Learned in Using TAKE 10! With Hispanic Children. J. Sch. Nurs. 2009, 25, 163–172. [Google Scholar] [CrossRef]
- Tucker, S.; Lanningham-Foster, L.M. Nurse-Led School-Based Child Obesity Prevention. J. Sch. Nurs. 2015, 31, 450–466. [Google Scholar] [CrossRef]
- Wright, K.; Norris, K.; Giger, J.N.; Suro, Z. Improving Healthy Dietary Behaviors, Nutrition Knowledge, and Self-Efficacy among Underserved School Children with Parent and Community Involvement. Child. Obes. 2012, 8, 347–356. [Google Scholar] [CrossRef]
- Zhou, Z.; Li, S.; Yin, J.; Fu, Q.; Ren, H.; Jin, T.; Zhu, J.; Howard, J.; Lan, T.; Yin, Z.; et al. Impact on Physical Fitness of the Chinese CHAMPS: A Clustered Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4412. [Google Scholar] [CrossRef]
- Zhou, Z.; Dong, S.; Yin, J.; Fu, Q.; Ren, H.; Yin, Z. Improving Physical Fitness and Cognitive Functions in Middle School Students: Study Protocol for the Chinese Childhood Health, Activity and Motor Performance Study (Chinese CHAMPS). Int. J. Environ. Res. Public Health 2018, 15, 976. [Google Scholar] [CrossRef]
- Black, M.M.; Hager, E.R.; Le, K.; Anliker, J.; Arteaga, S.S.; DiClemente, C.; Gittelsohn, J.; Magder, L.; Papas, M.; Snitker, S.; et al. Challenge! Health Promotion/Obesity Prevention Mentorship Model Among Urban, Black Adolescents. Pediatrics 2010, 126, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Dzewaltowski, D.A.; Estabrooks, P.A.; Welk, G.; Hill, J.; Milliken, G.; Karteroliotis, K.; Johnston, J.A. Healthy Youth Places: A Randomized Controlled Trial to Determine the Effectiveness of Facilitating Adult and Youth Leaders to Promote Physical Activity and Fruit and Vegetable Consumption in Middle Schools. Health Educ. Behav. 2008, 36, 583–600. [Google Scholar] [CrossRef]
- Institute of Medicine. Fitness Measures and Health Outcomes in Youth; National Academies Press: Washington, DC, USA, 2012. [Google Scholar]
- Birch, L.; Perry, R.; Hunt, L.P.; Matson, R.; Chong, A.; Beynon, R.; Hamilton-Shield, J. What change in body mass index is associated with improvement in percentage body fat in childhood obesity? A meta-regression. BMJ Open 2019, 9, e028231. [Google Scholar] [CrossRef] [PubMed]
- Tugault-Lafleur, C.N.; Black, J.L.; IBarr, S. A Systematic Review of Methods to Assess Children’s Diets in the School Context. Adv. Nutr. 2017, 8, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Mangieri, H. Fueling Young Athletes; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Seebohar, B. Sports Nutrition for Youth Athletes. USA Triathlon. 25 July 2019. Available online: https://www.teamusa.org/USA-Triathlon/News/Blogs/Multisport-Lab/2019/July/25/Sports-Nutrition-for-Youth-Athletes (accessed on 22 September 2020).


{kind=link}
| Population Trained | ||||
|---|---|---|---|---|
| Adults | Cross-Age Peers | Same-Age Peers | ||
| Intervention Setting | Classroom (part of school curriculum) | A | B | C |
| Afterschool, extracurricular, or school club activities occurring outside the classroom | D | E | F | |
| Author, Year | Intervention Name or Description | Population Characteristics: Grade Level/Age (Sample Size), Location | Group Receiving Training | Training Design | Intervention Frequency and Duration | Evaluation Indicators and Notable Results |
|---|---|---|---|---|---|---|
| Arlinghaus, 2017 1 [21] | Obesity prevention program with compañeros | 6th and 7th grade (n = 506), Houston, TX | PE teachers | Teachers were trained in leading all aspects of the intervention, which focused on basic physical activity and nutrition education. They were provided with strategies for using positive reinforcement and constructive feedback with students. Those who worked with cross-age peers (see Group B) met with them regularly to provide feedback and guidance. Teachers met weekly with research staff to discuss any issues. | Intervention was delivered during middle school students’ regularly scheduled PE class period for 6 months; 50 min a day, 5 days a week. One day each week focused specifically on healthy eating. | Outcome: change in anthropometrics; only students with BMI percentile at or above 85% at baseline (n = 189) were included in the analysis. Process: fidelity of implementation and a random assessment of 10% of classes to record frequency of positive reinforcement and constructive feedback. |
| Baskin, 2009 [22] | Described design, implementation and lessons learned from a pilot obesity prevention program implemented in a low-resource school | 7th and 8th grade (n = 113), Southern U.S. | PE teachers, health educator, and graduate students who served as teacher aids during lessons | Initial training provided when curriculum was finalized. Training emphasized active learning and hands-on activities. Researchers met quarterly with those implementing the intervention to address any issues that arose and discuss any program modifications. | Intervention was implemented over one school year. Students had a health education period once a week during their normally scheduled 50-min PE class. The curriculum included food demonstrations and tastings. | Outcome: changes in anthropometrics, health behaviors, dietary intake, and physical fitness. Process: meetings with school staff and research meetings were recorded and analyzed, and themes were identified. Focus groups were conducted with students and staff to determine acceptability. Results: In focus groups, students reported making changes to their diet and thought the program should continue and be expanded to 6th graders. They enjoyed interactive games but reported hesitancy to try new foods and dislike of “healthier” foods in the school cafeteria. |
| Bukhari, 2011 [27] | Diet for a Healthy Planet with Teen Battle Chefs curriculum | 9th grade (n = 98), Brooklyn, NY | Classroom teachers | 2-day training focusing on the skills necessary to teach program lesson plans. During program implementation, teachers completed an online lesson feedback survey to provide information about fidelity and feasibility. | 19-week program addressing state educational standards for high school and intermediate school. Offered as an elective at the school for a semester; class was daily for 1 h. | Outcome: changes in dietary behaviors, attitudes, and frequency of eating meals with friends and family. Results: Participants reported eating vegetables as snacks significantly more often post-intervention compared with a control group. Process: reach, focus groups with students, reflective exercises for students, dose delivered, and feasibility and fidelity as reported by teachers. Results: In focus groups, students reported eating more fruits and vegetables and an increased willingness to try new foods. |
| Contento, 2010 [28] +4 Papers [29,30,31,32] | Choice, Control and Change | 7th grade (n = 278 in pilot; n = 1136 in RCT), New York, NY | Science teachers | A 3-h intensive professional development session was held for teachers prior to the intervention start, and a follow-up 3-h training session was held in the middle of the intervention. A research staff member also attended one-third of all classroom sessions and met with each teacher weekly to provide support and feedback. | Curriculum consists of 24, 45-min, science and nutrition education lessons taught over 8–10 weeks. Some lessons were taught over multiple days for a total of 30–35 sessions. Curriculum aligns with national science standards. | Outcome: changes in food and activity choices; mediating variables measured included self-efficacy, outcome expectations, beliefs, attitudes, and perceived barriers. Results: Participants significantly decreased number of SSBs consumed and the portion size of SSBs compared to a control group. The pilot group additionally reported a significant increase in fruit and vegetable consumption, but the RCT intervention group did not. Process: teacher professional development, teacher implementation and student reception. Results: Student engagement level was evaluated by research staff during classroom sessions and the mean was 72%. Students were particularly engaged in hands-on activities. Mean student satisfaction with the program measured by survey was 2.9 on a 4-point scale. |
| Dubuy, 2014 2 [33] | Health Scores! | 10–14 years old (n = 605), Flanders, Belgium | Teachers | Prior to the intervention, teachers at participating schools received training on a range of activities related to healthy eating and physical activity. Further details about the teacher training and in-school curriculum were not provided in the paper. The key intervention strategy was using professional football players as credible role models for healthy lifestyle behaviors (see Group D). | 4 month in-school curriculum bookended at the start and end by clinics with a professional football team | Outcome: changes in dietary habits, frequency of breakfast consumption, eating attitudes and self-efficacy, and physical activity levels. Results: Those in the intervention group increased water and vegetable consumption, and this trended toward significance compared with the control group. Process: youth satisfaction with professional athlete clinics, response to videos and letters and overall satisfaction with the program. Results: Youth overall satisfaction with the intervention was 7.82 out of 10, and the two intervention topics most commonly recalled by youth when asked were breakfast and vegetables. |
| Duncan, 2019 [34] | Healthy Homework program | 7–10 years old (n = 675), Auckland and Dunedin, New Zealand | Classroom teachers at intervention schools and a lead teacher from each control school (who were permitted to implement the program after the final follow-up of the study) | Teachers received a half-day of training. 90 min was spent on the benefits of physical activity and healthy eating for students and previous strategies to integrate these topics into the curriculum. The second 90 min was spent on the program modules, examples of implementation and an opportunity for questions about the program. | 8-week in-class and applied compulsory homework teaching module (length of a school term in New Zealand) grounded in the national school curriculum. The in-class portion was delivered in 3 90-min sessions a week, and one session included a review of the previous week’s homework. An online portal allowed students to share homework-related information with other students, including those at other schools. | Outcome: changes in physical activity, dietary patterns, screen time, and anthropometrics. Results: Participants had a significant increase in fruit consumption post-intervention compared with a control group, but the change was not sustained at the 6-month follow up. Anecdotally, students seemed more engaged in the physical activity topics that nutrition ones during the intervention. |
| Fahlman, 2008 [36] | Michigan Model “What’s Food Got to Do With It?” curriculum | Middle school (n = 783), Large metropolitan area in Michigan | Classroom teachers | 8 h of in-service training was held on the curriculum and the textbook, “What’s Food Got to Do With It?” | 8-session nutrition module that is part of larger statewide health curriculum for middle school taught over the course of 1 month. | Outcome: changes in dietary intake, nutrition knowledge, and healthy eating efficacy expectations. Results: Participants significantly increased consumption of fruits and vegetables post-intervention compared with a control group. Of note, about one-third of the initial sample was lost to follow-up. |
| Fairclough, 2013 [37] | Children’s Health, Activity and Nutrition: Get Educated! (CHANGE!) | 10–11 years old (n = 318), Wigan, England | Year 6 Teachers | A 4-h training was provided to teachers in delivering the curriculum. | 20-week curriculum with weekly 60-minue classroom sessions that were aligned with the national primary school curriculum. Also included homework tasks. | Outcome: changes in anthropometrics, physical activity, sedentary time, and food intake. |
| Heo, 2018 3 [45] | HealthCorps | High school (n = 832), New York, NY | Program coordinator at each school teaches lessons, oversees program activities, and serves as a mentor for students Extra- curricular activities also develop youth from the target population as peer leaders (see Group F) | Coordinators receive three weeks of HealthCorps training over the summer as well as a week of professional development over the winter break. Coordinators also have weekly check-ins with program supervisors and at least one site visit from the program supervisor during the school year. | 10 classroom lessons are delivered as part of the curriculum. Were delivered over the course of a semester or school year, depending on the school. For students participating in program activities outside the classroom, total exposure could be up to 45 h over 36 weeks. | Outcome: changes in anthropometrics, knowledge, and health behavior. Results: Students participating in HealthCorps significantly increased fruit and vegetable intake; there was no change in the control group. Process: site visit by program supervisor to ensure fidelity. |
| Irwin, 2012 2 [46] +1 paper [47] | Get Fit with the Grizzlies | 4th and 5th grade (n = 888), Memphis, TN | PE teachers | Teachers attended a half-day training workshop on the 6-week curriculum and the support services that were available to them to implement the curriculum (included web support and special activities with the Memphis Grizzlies NBA team—see Group D). Teachers were also trained to administer the pre and post-tests for the intervention. Each teacher also received two one-on-one follow-up trainings at their school during the intervention. | 6-week mini-unit incorporated into PE curriculum; one lesson taught per week. Players, dancers and/or the mascot for the Memphis Grizzlies visited the schools for an assembly, and there was a district-wide Get Fit with the Grizzlies Achievement Day at Grizzlies home arena at the end of the program. | Outcome: changes in knowledge, eating behaviors, and physical activity habits. Results: Daily fruit servings increased significantly from pre to post- intervention. |
| Kipping, 2014 [49] +1 paper [50] | Active for Life Year 5 (AFLY5) (Adapted from Planet Health and Eat Well, Keep Moving interventions in the U.S.) | 9–10 years old (n = 2221), Bristol City and North Somerset, England | Year 5 classroom teachers and learning support assistants | The training was 8–9 h over the course of 1 day in a location away from school. During the training, the intervention rationale was explained, lessons and homework activities in the curriculum were discussed and taught by the trainers interactively. Teachers and assistants also had the opportunity to ask questions. At the training, teachers were given freedom to adapt materials to their style and the range of abilities for their students, but all of the knowledge and skills from the curriculum could be imparted. | The curriculum consisted of 16 in-class lessons with 10 parent-child interactive homework activities, delivered over a period of 6–7 months (two out of three school terms). | Outcome: changes in physical activity, screen time, food consumption, and anthropometrics. Results: Participants showed a significant decrease in energy drink consumption post-intervention compared with a control group. |
| Koch, 2019 [51] | Food, Health, & Choices | 5th grade (n = 1159), New York, NY (North Manhattan and South Bronx) | Classroom teachers and graduate student “curriculum instructors” | Teachers received a stipend to attend a 6-h professional development workshop the week before school began. The workshop provided an overview of the intervention, and teachers had the opportunity to practice intervention activities. Curriculum instructors attended the professional development with the teachers, and had an additional 2-h training on the intervention, and weekly 2-h meetings with the research staff during the intervention. Classroom teachers and curriculum instructors co-taught the lessons. | 23 lessons replacing 2 mandated units in the science curriculum, delivered over 10 months. September—November was 2 lessons per week, December to April was 1 lesson per month (due to standardized testing preparation), and May was 2 lessons per week. | Outcome: changes in anthropometrics, dietary intake, outcome expectations, self-efficacy, behavioral intention, habit strength, goal-setting skills, competence, and motivation. Results: A wellness component was delivered in some schools that included a policy around foods that could be served during classroom activities. Students who received only the wellness intervention showed a significant decrease in SSB intake, but those who received the curriculum only or the curriculum and wellness together did not. |
| Lepe, 2019 [53] | Empowering Urban School Children to Increase Fruit and Vegetable Consumption Through EFNEP-Enhanced PSE Interventions (EMPOWER) | 5th grade (n = 312), Pawtucket, RI | School health teachers and EFNEP para- professional educators | Teachers were trained in the Fresh Fruit and Vegetable Program (FFVP) nutrition education curriculum by SNAP-Ed staff. EFENEP educators received 2 2-h training sessions on the Policy, Systems, and Environment (PSE) curriculum they would be delivering to students. Their training also included an in-depth orientation to process evaluation methods. | 10 30-min PSE lessons to be delivered every other week by trained EFNEP staff, designed to augment the 8-week FFVP curriculum taught by classroom teachers. | Outcome: changes in knowledge and fruit and vegetable consumption. Process: fidelity, dose delivered, dose received, reach, and program perception. Results: In focus groups, students reported asking for more fruits and vegetables at home, and school staff affirmed growth in student empowerment. Mis- communication between teachers and EFNEP educators was identified as a barrier to implementation. |
| Li, 2010 [56] +1 paper [57] | The nutrition-based comprehensive intervention study on childhood obesity in China (NISCOC) | 6–13 years old (n = 9867), Shanghai, Chongqing, Guangzhou, Jinan, Harbin, and Beijing, China | Teachers, classroom tutors, and health educators | A 2-day training was held for the school staff that would be implementing the intervention. The training covered integrating the program into the school curriculum and performing the intervention activities. Teachers practiced the lessons during the training to ensure understanding. | The intervention took place over 2 semesters and included 6 nutrition lectures that lasted a minimum of 40 min. A cartoon-style nutrition handbook was developed for the students that was to be used along with the lectures. | Outcome: changes in anthropometrics, glucose and lipid profiles, attitudes, knowledge, and nutrition practices. |
| Mihas, 2010 [61] | Vyronas Youth Regarding Obesity, Nutrition, and Attitudinal Styles (VYRONAS) | 12–13 years old (n = 191), Athens, Greece | Home economics teachers | Teachers attended two 3-h training seminars to learn about the objectives of the program, their role in delivering the intervention, and the importance of incorporating health and nutrition into the curriculum. | 12 1-h lessons were delivered in the classroom over a period of 12 weeks. Teachers were supervised by a health visitor or family doctor from the community when delivering the lessons. Two meetings were also held for parents providing information about healthy dietary habits for children. | Outcome: changes in anthropometrics and dietary intake. Results: Participants showed a significant increase in fruit consumption post-intervention compared with a control group, and this increase was sustained 12 months after the intervention. |
| Olivares, 2005 [64] | The program sought to design and validate appropriate nutrition education materials for Chilean primary school students and develop and validate a teacher training program that could be replicated throughout the country. | 3rd—7th grade, (n = 1701), Chile (intervention was implemented in schools throughout the country) | Classroom teachers | Participants received 3 days of training on the newly developed curriculum, which included a textbook, teacher’s guide, and practical guides for students that accompanied each of the modules. Some teachers who were particularly motivated by the training spontaneously trained colleagues when they returned to their respective schools. | The lessons were implemented over a period of 5 months. | Outcome: changes in knowledge and dietary intake. Results: Fruit and vegetable intake increased significantly among 10–11-year-old girls compared to a matching control group. SSB intake increased significantly among 8–9-year-olds in both the intervention and control groups. Process: teacher feedback on program perception. Results: Students were most engaged in activities where they prepared healthy foods. |
| Tsai, 2009 [69] | TAKE 10! | K-6th grade (n = 840), Chicago, IL | Teachers and a full-time volunteer | The training oriented the teachers and volunteer to the curriculum, provided strategies for integrating it into their other lessons, and connected health with academic learning. | The intervention was implemented over the course of a school year. Content was adapted to be appropriate for each grade level. The program includes daily 10-min physical activity breaks in the classroom and incorporates nutrition information into these breaks. | Outcome: changes in anthropometrics and nutrition and physical activity knowledge. Process: program perception evaluated through observations of the sessions and interviews with teachers and students at the end of the intervention. Results: Teachers were generally positive about the program and implemented 3–5 of the sessions per week. Students reported better concentration after moving during the sessions and recalled nutrition information they learned in the post-intervention interviews. |
| Tucker, 2015 2 [70] | Let’s Go 5–2-1–0 childhood obesity prevention intervention delivered by school nurses plus 1:1 or small group coaching by nursing students | 4th and 5th grade (n = 72), Location not specified; corresponding author affiliated with University of Iowa | School nurses Intervention also included nursing students as mentors (see Group D) | Training for school nurses on delivering the classroom portion of the intervention was not described in the paper. | School nurses delivered the Let’s Go 5–2-1–0 curriculum weekly during classroom instructional time in 10–15 increments. Dosage varied from 14–21 sessions. Nursing students had lunch with their assigned student/students weekly to discuss curriculum content and set health goals. | Outcome: changes in anthropometrics, physical activity levels, nutrition, family eating patterns and screen time. Results: Self-reported daily servings of fruits and vegetables increased significantly at both schools. |
| Zhou, 2019 2 [72] +1 paper [73] | Chinese Childhood Health, Activity and Motor Performance Study (Chinese CHAMPS) with both in-school and afterschool components | 7th grade (n = 680), Beijing, Wuhu, and Weifang, China | PE teachers Intervention also included afterschool program staff (see Group D) | 2-day training focusing on adolescent growth and development, designing age-appropriate physical activities, and instructional methods. Training facilitators demonstrated activities, and staff then had the opportunity to practice. | 8-month intervention; the in-school portion increased PE class to 3 days/week and implemented daily recess. As part of PE, students received fitness and nutrition education and bi-weekly text messages. | Outcome: Changes in physical fitness, anthropometrics, cognitive function, food habits and preferences, knowledge, physical activity Process: fidelity and dose received through periodic monitoring of sessions by research staff. |
| Author, Year | Intervention Name or Description | Population Characteristics: Grade Level/Age (Sample Size), Location | Group Receiving Training | Training Design | Intervention Frequency and Duration | Evaluation Indicators and Notable Results |
|---|---|---|---|---|---|---|
| Arlinghaus, 2017 1 [21] | School-based obesity prevention program with compañeros | 6th and 7th grade (n = 506), Houston, TX | High school students—“Compañeros” (based on the “promotoras” model of using peer health workers in the Hispanic community. | Cross-age peer leaders were trained daily for two weeks on intervention activities. In addition to the curriculum, they were trained to be able to identify strengths and weaknesses in their own eating habits and given ideas for how to engage in conversation with middle school students about healthy diet and activity habits. Training included opportunities to practice initiating conversations about the curriculum using different scenarios. They were also trained in providing praise and modeling healthy behavior. Throughout the intervention, they discussed the topic of focus with the PE teacher (see Group A) prior to each class and received regular feedback and support from the PE teacher. | Intervention was delivered during middle school students’ regularly scheduled PE class period for 6 months; 50 min a day, 5 days a week. One day each week focused specifically on healthy eating. | Outcome: change in anthropometrics; only students with BMI percentile at or above 85% at baseline (n = 189) were included in the analysis. Process: fidelity of implementation and a random assessment of 10% of classes to record frequency of positive reinforcement and constructive feedback. |
| El Rayess, 2017 [35] | Mark, Set, Go! | 5th and 6th grade (n = 954), Providence, RI | High school students in an experiential learning program that includes community internships | Cross-peers received an orientation and weekly training session. Training covered classroom management, small group teaching strategies, and a review of the material. | 9-week program (frequency of lessons not specified) | Outcome: changes in knowledge, dietary behaviors, anthropometrics, and physical activity Results: There was a significant decrease in the percentage of students reporting drinking soft drinks and juice at least once a day. In subgroup analysis, there was a significant decrease in both categories for girls and for students with overweight or obesity. |
| Foley, 2017 [38] | Students As LifeStyle Activists (SALSA) | Year 8 (same as U.S. 8th grade) *Focus of the study was the cross-age peers; subject number for year 8 students not available. Western Sydney, Australia | Year 10 students (n = 415) | Cross-age peers were trained by university students from health and education disciplines who worked themselves had received educator training from the project staff. The Year 10 students were trained to deliver the intervention in a one-day workshop and were given a scripted manual to use as a guide for delivering the intervention. As part of the training, students practiced delivering the lessons in front of one another. | Four 70-min lessons delivered to a Year 8 class by a small group of 4–6 cross-age peer educators. Length of time between first and fourth lesson varied (mean 25 days +/- 15.9) | Outcomes for cross-age peers: changes in dietary behaviors, physical activity, screen time and intention to change. Results: At follow-up, a significantly higher proportion was meeting recommendations for daily fruit and vegetable intake and drinking less than 1 cup of sugary beverages daily. Process: acceptability among cross-age peers Results: 91% would recommend the program to their peers; goal setting, leadership and teaching emerged as important themes, and 42% discussed program themes at home. |
| Lo, 2008 2 [59] | Fluids Used Effectively for Living (FUEL) | Grade 9 (n = 113), Saskatchewan, Canada | University students (worked with same-age peers from the target population, see Group C) | Two-week training intensive that oriented the cross-age peers to the content and also aimed to build teamwork among them. Cross-age peers also provided leadership for the same-age peers. | Six-week program, one 45-min session each week | Outcome: changes in beverage intake, knowledge, and attitudes. Results: Significant decrease in SSB intake post-intervention, sustained through 3-month follow up among group with cross-age and same-age peers (three other comparison groups without peer educators did not show significant change). Process: participant satisfaction with content and delivery of the program. Results: 71% enjoyed the intervention and 77% would suggest it to others. |
| Author, Year | Intervention Name or Description | Population Characteristics: Grade Level/Age (Sample Size), Location | Group Receiving Training | Training Design | Intervention Frequency and Duration | Evaluation Indicators and Notable Results |
|---|---|---|---|---|---|---|
| Lo, 2008 1 [59] | Fluids Used Effectively for Living (FUEL) | Grade 9 (n = 113), Saskatchewan, Canada | Same-age, Grade 9 peers (worked with cross-age peers, see Group B) | Had their own two-week training intensive to orient them to the content and build teamwork. They were connected to cross-age peers for guidance. | Six-week program, one 45-min session each week | Outcome: changes in beverage intake, knowledge, and attitudes Process: participant satisfaction with content and delivery of the program. See Table 2 for results |
| Stock, 2007 [67] | Healthy Buddies | 4th–7th grade (n = 199) British Columbia, Canada | Cross-age peers. In this case, the students in the target age range for the study were the older peers | Cross-age peers received a lesson from the intervention teacher once a week and then taught that lesson to their younger “buddies” that same week. Older students still developing leadership skills were paired with another older student with strong leadership ability. | 21 weeks—the cross-age peers receive (45 min) and then deliver (30 min) a lesson once per week. Paired classes also had two 30-min structured physical activity sessions together weekly. | Outcome: changes in height, weight, blood pressure, and heart rate; 9-min run, knowledge of nutrition and physical activity, and eating and physical activity behaviors. |
| Author, Year | Intervention Name or Description | Population Characteristics: Grade Level/Age (Sample Size), Location | Group Receiving Training | Training Design | Intervention Frequency and Duration | Evaluation Indicators and Notable Results |
|---|---|---|---|---|---|---|
| Dubuy, 2014 1 [33] | Health Scores! | 10–14 years old (n = 605), Flanders, Belgium | Professional football players hosted a start clinic and end clinic prior to and at the conclusion of the classroom-based portion of the intervention (see Group A) | While the professional athletes did not receive formal training from the research staff, the football clubs were responsible for organizing the start and end clinics, and athlete promotion of healthy behaviors was a key part of the intervention. At the clinics, the professional athletes participated in activities with the youth that encouraged a healthy diet and physical activity and handed out lifestyle contracts that youth signed. Athletes also filmed two video messages that were shown to the youth at school and sent two letters reminding students of the importance of eating healthy and being active. | 4 month in-school curriculum bookended by the start and end clinics with a professional football team | Outcome: changes in dietary habits, frequency of breakfast consumption, eating attitudes and self-efficacy, and physical activity levels. Process: youth satisfaction with professional athlete clinics, response to videos and letters and overall satisfaction with the program See Table 1 for results |
| Gittelsohn, 2013 2 [40] | Baltimore Healthy Eating Zones | 10–14 years old (n = 242), Baltimore, MD | Public health graduate students | 2-day initial training with periodic booster sessions. Once trained, they visited rec centers and corner stores participating in the intervention at least weekly and offered cooking classes at rec centers. Also worked with cross-peer educators at each rec center site (see Group E). | Four phases, each 10 weeks long. Interventionists and cross-age peers were to hold one session per week at rec centers. | Process: reach and dose measured against implementation standards developed by the research team. |
| Irwin, 2012 1 [46] +1 paper [47] | Get Fit with the Grizzlies | 4th and 5th grade (n = 888), Memphis, TN | Memphis Grizzlies players and staff | While athletes did not receive formal training, they participated as role models in the intervention by making visits to assemblies in participating schools and hosting an achievement day for youth who completed the program. | 6-week mini-unit incorporated into PE curriculum; one lesson taught per week. Players, dancers and/or the mascot for the Memphis Grizzlies visited the schools for an assembly, and there was a district-wide Get Fit with the Grizzlies Achievement Day at Grizzlies home arena at the end of the program. | Outcome: changes in knowledge, eating behaviors, and physical activity habits. See Table 1 for results |
| Kohlstatdt, 2016 2 [52] +1 paper [53] | NutriBee | 4th–7th grade (n = 179), New Mexico, Michigan, Maryland and Guam | School teachers and health professionals. Intervention was conducted in afterschool or weekend clubs, or in camp settings | Received 1–3 h of experiential in-person instruction designed to parallel the format of the intervention itself, including a culminating game show. Also received an instructor training manual and informational video. After completion of the intervention, instructors received a stipend and certificate | 10 2-h modules delivered across varying time frames ranging from 4 days (in camp settings) to 1 month (club that met once/week) | Outcome: changes in dietary knowledge, intentions, outcome expectations, self-efficacy, and dietary intake. Results: Selection of dried and fresh fruit and bottled water increased, and consumption of sugary sports drinks decreased. Process: measured dose, fidelity, and acceptability. Results: Acceptability was based on appropriateness of difficulty and appropriateness of length. Scores ranged from 1.5 to 1.8 out of a maximum of 2. |
| Linton, 2014 [58] | Youth Engagement and Action for Health (YEAH!) | Age range was 9–22 years across all groups: 6 middle school, 6 high school, 8 community center groups and 1 church youth group (n = 136), San Diego, CA | Adult mentors/ leaders of youth groups in a variety of settings (after-school programs, community organizations, religious organizations) who are interested in nutrition or physical activity- related community advocacy projects. | Training is a half-day session that covers gathering necessary resources for the project, conducting a community assessment of factors related to healthy eating and/or active living, identifying community decision makers, and advocacy. Adult leaders receive the YEAH! manual as part of the training and have access to ongoing technical support from the Sand Diego County Childhood Obesity Initiative throughout their projects. | Groups are run independently, and length varies by project; average was 9 sessions over a 10-week period. With guidance from an adult mentor, youth groups assess their food and built environment, prioritize problems identified in the assessment, and develop and implement an action plan to advocate with decision makers for change in their community. | Outcome: changes in attitude, perception of control, self-efficacy, readiness to act as social change advocates and health behavior. Process: retention of youth throughout project, number of meetings with decision makers. Results: 73% of youth participants across all groups remained engaged throughout their group’s project. 19 of 20 groups in the evaluation had in-person meetings or presentations with decision makers. 11 groups reported changes in the community as a result of their work, and 4 reported pending changes. |
| Luesse, 2019 [60] | In Defense of Food afterschool curriculum | 6th–8th grade (n = 32), New York, NY | Afterschool program teachers | Before the start of the intervention, afterschool teachers received a 2-h professional development training on the curriculum. Two weeks into the intervention, teachers received an additional 1-h follow-up training. They also had access to support as needed throughout the intervention period. | 10 weeks, one 2-h afterschool session each week. The curriculum is divided into 3 units of 3 lessons each and a final culminating lesson. | Outcome: changes in dietary intake, outcome expectations, self-efficacy, self-regulation skills and autonomous motivation. Results: There was a significant increase in fruit and vegetable intake post- intervention. Qualitative: assessment of student understanding and ability to apply “food rules” from each lesson and semi-structured interviews with youth to better understand target outcomes. Results: Youth best understood “rules” related to drinking water and moderation. In interviews, youth noted that the social and physical environment made it difficult to decrease consumption of processed foods even when they desired to do so. |
| Molaison, 2005 [62] | Qualitative study that examined factors that mediate fruit and vegetable consumption among southern, low-income black adolescents to aid in planning an intervention | 10–13 years old (n = 42), 2 counties in the lower Delta region of Mississippi | Graduate students and research staff who were of the same ethnic or racial background as the youth. | 3-day workshop provided training in standardized focus group methods. | Focus groups were conducted with youth enrolled in the 5-week National Youth Sports Program. Groups were segmented by gender and age: 10–11, 12, and 13, for 6 groups total. Each focus group met once during the 5-week summer program session. | Qualitative: focus group transcripts were coded, and themes were identified. Results: Taste and method of preparation were major factors limiting fruit and vegetable consumption, especially for vegetables. Additional limiting factors were lack of availability of fruits and vegetables at home or in neighborhood stores and limited control over their food options. Most had family support for fruit and vegetable consumption, but not peer support. |
| Tucker, 2015 1 [70] | Let’s Go 5-2–1-0 childhood obesity prevention intervention delivered by school nurses plus 1:1 or small group coaching by nursing students | 4th and 5th grade (n = 72), Location not specified; corresponding author affiliated with University of Iowa | Nursing students Intervention also included classroom component with school nurses (see Group A) | Training was provided in the 5-2–1-0 curriculum, basic motivational interviewing (MI) principles for behavior change, and role modeling healthy behavior. Training included a didactic portion, role playing, and use of videos. At one nursing school, training consisted of an initial 4-h session followed by weekly sessions of practice and role plays. At the other nursing school, a 2-h training session was provided. | The intervention ran from September to April in one school and January to April in the other school. School nurses delivered the Let’s Go 5-2–1-0 curriculum weekly during classroom instructional time in 10–15 increments. Dosage varied from 14–21 sessions. Nursing students had lunch with their assigned student/students once a week to discuss curriculum content and set goals for intervention topics. | Outcome: changes in anthropometric measurements, physical activity levels, nutrition, family eating patterns, and screen time. See Table 1 for results |
| Wright, 2012 [71] | Kids Nutrition and Fitness | 8–12 years old (n = 251), Los Angeles, CA | An advanced practice nurse, registered nurses, a physical education specialist, and community health workers (some of whom were parent volunteers) | Training took place in a full-day, in-person session that covered all intervention protocols, including culturally relevant information and examples for the nutrition education component. Retraining was provided on an as-needed basis if instructors were not following the intervention protocol during session observations. | 6-week afterschool program with weekly 90-min sessions. Students were recruited and went through the program in waves of 14–28 at a time. Beyond the curriculum, the intervention also included school and community-level activities, including physical and mental health services through local clinics. | Outcome: changes in anthropometrics, dietary behaviors, food preferences, knowledge, and self-efficacy Results: Self-reported intake of fruit, vegetables and 100% fruit juice increased significantly at post-intervention and was sustained at 12-month follow-up. Process: intervention fidelity assessed by session observations, focus groups with parents. |
| Zhou, 2019 1 [72] +1 paper [73] | Chinese Childhood Health, Activity and Motor Performance Study (Chinese CHAMPS) with both in-school and afterschool components | 7th grade (n = 680), Beijing, Wuhu, and Weifang, China | Afterschool program staff Intervention also included classroom component with PE teachers (see Group A) | 1-day training focusing on adolescent growth and development, designing age-appropriate physical activities, and instructional methods. Training facilitators demonstrated activities, and staff then had the opportunity to practice. | 8-month intervention. The afterschool portion of the intervention added 45 min of moderate to vigorous physical activity (MVPA) 2 days a week, provided fitness and nutrition education, and bi-weekly text messages to students. | Outcome: Changes in physical fitness, anthropometrics, cognitive function, food habits and preferences, knowledge, and physical activity. Process: fidelity and dose received through periodic monitoring of sessions by research staff. |
| Author, Year | Intervention Name or Description | Population Characteristics: Grade Level/Age (Sample Size), Location | Group Receiving Training | Training Design | Intervention Frequency and Duration | Evaluation Indicators and Notable Results |
|---|---|---|---|---|---|---|
| Gittelsohn, 2013 1 [40] | Baltimore Healthy Eating Zones | 10–14 years old (n = 242) Baltimore, MD | Cross-age peers, 13–18 years old. 2–3 applicants were selected by the director at each rec center site | Trained to assist interventionists (see Group D) in program delivery at rec centers prior to the start of the intervention and provided with a procedures manual. Cross-age peers were to accompany interventionists, assist in activities and communication with customers at corner stores and eventually be able to lead activities independently. Cross-age peers were provided with a $100 monthly honorarium. | Four phases, each 10 weeks long. Interventionists and cross-age peers were to hold one session per week at rec centers. | Process: reach and dose measured against implementation standards developed by the research team. Results: 58% of rec center visits by interventionists had a cross-age peer also present for the activity. Cross-age peers averaged 0.2 rec center visits per week or 2.1 per phase (Standard was 1 visit per week or 10 per phase). |
| Gittelsohn, 2014 [41] +3 papers [42,43,44] | B’More Healthy Communities for Kids | 10–14 years old (n = 508), Baltimore, MD | Wave 1: College students (18–22 years) Wave 2: High school students (15–18 years) | Interested cross-age peers had to complete an application and interview. For those selected, 12 training sessions were held prior to the start of the intervention (27 h of training), and bi-weekly booster training sessions were held throughout the intervention. Trained cross-age peers were grouped into 3–5 to deliver the program at rec centers. College students were paid for completion of the training program and time teaching sessions at rec centers. High school students received service learning hours and small financial incentives. Curriculum provided to cross-age peers included ice breakers, a script of questions to use during discussions. Leaders were combined into groups of 3–5 to deliver the intervention in rec centers. | 14 60-min sessions taught bi-weekly over 6 months | Outcomes for cross-age peers (n = 25): changes in anthropometrics, dietary intake, food behaviors, psychosocial factors, and leadership skills. Process: dose, reach, and fidelity; qualitative interviews with cross-age peers after Wave 1. Results: In open-ended comments, youth participants reported enjoying games and cooking lessons. Discussions were the most challenging element in terms of youth engagement. Level of interest in topics varied; using poster board for youth to write on topics increased engagement. In interviews, cross-age peers indicated more scenarios/role-playing during training would have been helpful, nutrition content for youth should not be overly complicated, and important that cross-age peers are representative of the community in which they are working. |
| Kohlstatdt, 2016 1 [52] +1 paper [53] | NutriBee | 4th–7th grade (n = 170), New Mexico, Michigan, Maryland and Guam | High school students | Cross-age peers worked with a subject matter expert coach to connect their interests with nutrition in the form of a project that would be part of the NutriBee intervention material. The projects and questions were incorporated into the curriculum as 1 of the 10 2-h modules of the program. Upon completion, cross-age peers received a stipend, certificate, and service learning credit. | 10 2-h modules delivered across varying time frames ranging from 4 days (in camp settings) to 1 month (club that met once/week). | Outcome: changes in dietary knowledge, intentions, outcome expectations, self-efficacy, and dietary intake. See Table 4 for results. |
| Saez, 2018 2 [65] | Peer intervention was carried out within the larger PRALIMAP-INÈS (Promotion de l’ALIMentation et l’Activité Physique-INEgalité de Santé) | Grade 9 (last year of middle school) and Grade 10 (first year of high school) (n = 32), Vosges, France | Cross-age peers (peer ambassadors) had participated in the program the previous year and were one year ahead of the target population in school (Intervention also used same-age peers; see Group F) To be eligible, peers had to have a demonstrated ability to control their weight and be of a similar socioeconomic background as the target population. | Peers received a 2-h training session at the start of the school year, in groups of 2–4 at a time or individually if grouping was not possible. During the training, cross-age peers considered the strengths they would bring as intervention facilitators. They then brainstormed activities they could lead and practiced role-playing various scenarios they might encounter. Following role-playing, they received feedback and debriefing tips. Cross-age peers discussed their planned activities with the program coordinator; financial support was available if needed for the activities. They had regular contact with the program coordinator throughout the school year via phone and text messages for follow-up and support and had a mid-year face-to-face meeting. | Target was for cross-age peers to plan and carry out four activities with their assigned small group of younger peers throughout the school year. The peer intervention was part of a larger health intervention in the school setting and was meant to be more informal in its approach, where activities could also be conducted outside of school. | Outcome: changes in physical activity, mental health, and perceived health and quality of life Process: satisfaction, perceived appropriateness, dose received, and practicality Results: A total of 5 cross-age peers were trained and remained active out of 20 potential facilitators who initially accepted the invitation, and 1 successfully organized and implemented an activity. Youth were significantly more likely to accept the peer intervention when offered by the peer rather than an adult professional. Interestingly, though some youth reported mistrust of peers and concerns about social exclusion. Facilitators had a high need for support from the program coordinator and despite addressing this topic in the training, struggled to come of up with ideas for activities. Training feedback indicated that more than 2 h was needed, and more practical ideas for activities and interpersonal skills training would be helpful. |
| Author, Year | Intervention Name or Description | Population Characteristics: Grade Level/Age (Sample Size), Location | Group Receiving Training | Training Design | Intervention Frequency and Duration | Evaluation Indicators and Notable Results |
|---|---|---|---|---|---|---|
| Bell, 2017 [23] | Activity and Healthy Eating in ADolescence (AHEAD) | Year 8 (equivalent to U.S. 7th grade) (n = 99 in pilot, n = 928 in exploratory trial), Bristol, UK | Peers leaders from within the target population. In the pilot, 19% were trained as peer supporters and in the exploratory trial, 17% were trained. All Year 8 students filled out a nomination questionnaire and those with the most nominations were invited to a peer leader recruitment meeting. | Initial training for peer leaders was a two-day out-of-school event. Sessions used drama, food preparation, technology and games to deliver key nutrition and physical activity messages to peer leaders. Content supported school curriculum and national school health programs. Each peer leader received a diary to write about interactions with their peers; diaries included healthy challenges to encourage behavior change. Peer leaders walked to the training to promote active transport, and food and drinks served at the training were prepared on site, with the help of peer leaders when possible. Trainers included master’s degree students and professional health and well-being trainers. Four school-based follow-up sessions were held with peer leaders throughout the school year. | Peer leaders were tasked with informally diffusing the health messages they learned in the training and modeling healthy behavior over the course of the school year. Post-intervention behavioral questionnaires were used to assess the extent of the diffusion, and focus groups were conducted with non-peer leader intervention participants. | Outcome: changes in diet and physical activity behaviors. Results: Post-intervention, students ate significantly more servings of fruit a day and ate breakfast significantly more often than students from a comparable control group. Process: recruitment and retention rates for peer leaders, structured observation and evaluation of training sessions, post- intervention focus groups with both peer leaders and non-peer leader intervention participants. Results: Peer leaders responded especially well to hands-on activities, games and role-playing in the trainings. School-based trainings were less enjoyable to students than the initial trainings held offsite. About 1/3 of intervention participants were aware of having talked with a peer leader about healthy messages and reported that this encouraged them to increase healthy behaviors. |
| Bogart, 2016 [24] +2 papers [25,26] | Students for Nutrition and eXercise (SNaX) | 7th grade (n = 399 in pilot, n = 2997 in RCT), Los Angeles, CA | Peer leaders from within the target population. 21% of 7th graders were trailed during the pilot and 23% were trained during the RCT. A different group of leaders was recruited each week and each leader was asked to also recruit a partner for lunchtime activities. | Peer leaders attended a training session where they were taught to discuss SNaX messages with peers and family using motivational interviewing (MI) techniques. During the training, they engaged in role-playing using MI. They then recruited a friend to co-facilitate two lunchtime educational sessions with them. Peer leader training sessions were conducted by bachelor’s level facilitators who were themselves trained by a Ph.D. level clinical psychologist (4 h on motivational interviewing) and a Ph.D. level public health researcher (20 h on intervention content). | 5 weeks with two lunchtime sessions per week facilitated by peer leaders that could include taste tests and giving out of promotional items. Intervention also included school food environment changes and school-wide marketing of SNaX messages. | Outcome: changes in school lunch participation and cafeteria purchases, BMI classification change over time, attitudes about the cafeteria and water consumption, intentions to drink water, and water consumption. Results: Fruit servings significantly increased in intervention schools, and students also drank tap water significantly more often post-intervention compared with control schools. Process: researchers monitored peer leader training sessions for coverage of all session elements. |
| Franken, 2018 [39] | Share H2O (based on intervention conducted by Smit, 2016) | 5th and 6th grade (n = 377), Aruba | Peer leaders from within the target population. The 15% of boys and 15% of girls with the most nominations from their classmates were invited to attend the training to become peer leaders. | Training was 90 min and held during school hours. Peer leaders learned about the benefits of water consumption, worked on formulating their own arguments for increasing water consumption, practiced strategies for promoting water consumption with their peers and were encouraged to set an example with their own water consumption. Peer leaders received follow-up training sessions in weeks two and five of the intervention. | Peer leaders were tasked with promoting water consumption to their peers through their social networks over a period of 8 weeks. | Outcome: changes in consumption of water and SSBs and behavioral intention around beverage consumption. Students were also asked how often their friends consumed water and how often their friends approved or disapproved of them consuming water. Results: Students in the intervention group consumed significantly less SSBs post-intervention compared with control group. Those with a high perception of their friends’ approval for drinking water consumed significantly more water. |
| Heo, 2018 1 [45] | HealthCorps | High school (n = 832), New York, NY | Students from among the target population could elect to join the Youth Lead Action Research program or participate in facilitating lunchroom activities. | Paper does not include description of formalized training for same-age peers; leadership in healthy eating comes through participation in the program activities beyond the classroom. In Youth Lead Action Research, students learn research methods to identify health needs in their school or community and develop projects that address those needs. In the lunchroom, youth work alongside the program coordinator (see Group A) to share samples of healthy foods and engage with their peers on a monthly basis. | 10 classroom lessons are delivered as part of the curriculum. Were delivered over the course of a semester or school year, depending on the school. For students participating in program activities outside the classroom, total exposure could be up to 45 h over a maximum 36 weeks. | Outcome: changes in anthropometrics, knowledge, and health behavior. Results: Students participating in HealthCorps significantly increased fruit and vegetable intake post-intervention; there was no change in fruit and vegetable consumption from pre to post-intervention in the comparison group. Process: site visit by program supervisor to ensure fidelity in curriculum delivery. |
| Jackson, 2010 [48] | Healthy 4 Life | 6th–8th grade (n = 15) Urban area, southeastern GA | Intervention participants themselves developed a theater production that communicated nutrition and physical activity to friends and family. | Each session began with nutrition and physical activity topics, team-building activities introduced theater dynamics, students made a healthy recipe or snack after the theater activity and ended with a physical activity session. | 6 weeks, 75-min afterschool sessions twice per week. Throughout the six weeks, students used what they learned about nutrition, physical activity, and theater to develop a play, Getting on Track, which they gave as a dinner theater performance for family and friends. | Changes in knowledge, food and physical activity choices, and behavioral norms. Results: Small sample size gave insufficient power to generate statistical significance, but more students reported choosing fruit over sweets post- intervention. |
| Leung, 2017 [55] | Intervention incorporated photovoice into a food justice curriculum for middle school youth. | 6th–8th grade (n = 12) East Harlem, NY | Intervention participants themselves used photovoice to conduct a community food assessment and conduct a food justice project, then presented their photos and projects to the community. | Sessions covered photography and photovoice; the food system and environmental influences on food choices; a community food assessment photographing barriers and facilitators of eating healthy in the neighborhood; discussions of potential solutions to community food issues and roles youth could play in promoting change; and interviews of community members to understand their experience of the food environment. Throughout the intervention, facilitators reinforced the role of youth as researchers and active participants in changing their community. | 24 weeks total. The first 10 weeks focused on photovoice and included 6 90-min sessions at an afterschool program and 3 photo assignments. In the second 14 weeks, youth developed and implemented a food justice project. A celebration and photo exhibit were held at the end of the 24 weeks where youth shared and discussed their photos and project with community members. | Qualitative interviews and subsequent analysis to identify themes. Results: Through photos and focus groups, participants: (1) expressed distrust of the food industry, (2) identified the abundance of low-cost, unhealthy foods and product placement as barriers to healthy choices, (3) noted the importance family influence on their food choices and also their potential to be change agents in their family, (4) expressed concern about the health of family members and their own health, and (5) identified strategies for improving the food environment. |
| Necheles, 2007 [63] | The Teen Photovoice Project | 13–17 years old (n = 13), Los Angeles, CA | Intervention participants, all of whom were members of the Youth Advisory Board from the UCLA/RAND Center for Adolescent Health Promotion (the center), used photovoice and resulting themes to create health education messages that were then presented to the community. | Sessions covered photography and photovoice, qualitative research methods, sorting and selecting photos, creating narrative on photos, generating themes, generating ideas for health education products, planning for opening exhibit. | Over a period of five months, youth participated in 9 2-h afterschool sessions. In small groups, they selected a concept for a health education poster, photos to use on the poster and the text for communicating the health message. An opening exhibit for the posters was held at the California Science Center. | Outcomes of the project were the creation of the posters and the opening exhibit. Results: Following the project, youth encouraged the center to do more research on childhood obesity using youth participatory research methods. One student took the initiative to share photos of unhealthy food sold in the school cafeteria with the school foodservice director and advocated for healthier options. |
| Saez, 2018 2 [65] | Peer intervention was carried out within the larger PRALIMAP-INÈS (Promotion de l’ALIMentation et l’Activité Physique-INEgalité de Santé) | Grade 9 (last year of middle school) and Grade 10 (first year of high school) (n = 32), Vosges, France | Same-age peers (peer entrepreneurs) were in the same year in school as the target population. (Intervention also used cross-age peers; see Group E) To be eligible, peers had to have a demonstrated ability to control their weight and be of a similar socioeconomic background as the target population. | Peers received a 2-h training session at the start of the school year, in groups of 2–4 at a time or individually if grouping was not possible. During the training, same-age peers considered the strengths they would bring as intervention facilitators. They then brainstormed activities they could lead and practiced role-playing various scenarios they might encounter. Following role-playing, they received feedback and debriefing tips. Same-age peers discussed their planned activities with the program coordinator; financial support was available if needed for the activities. They had regular contact with the program coordinator throughout the school year via phone and text messages for follow-up and support and had a mid-year face-to-face meeting. | Target was for cross-age peers to plan and carry out four activities with their assigned small group of younger peers throughout the school year. The peer intervention was part of a larger health intervention in the school setting and was meant to be more informal in its approach, where activities could also be conducted outside of school. | Outcome: physical activity, mental health, and perceived health and quality of life Results: A total of 7 cross-age peers were trained and remained active out of 36 potential facilitators who initially accepted the invitation, and 5 successfully organized and implemented at least one activity. For additional evaluation results see Table 5. |
| Smit, 2016 [66] | Share H2O | 9–13 years old (n = 210), The Netherlands | Peer leaders from within the target population. The 15% of boys and 15% of girls with the most nominations from their classmates were invited to attend the training to become peer leaders. | Training was 90 min and held during school hours. Peer leaders learned about the benefits of water consumption, worked on formulating their own arguments for increasing water consumption, practiced strategies for promoting water consumption with their peers, and were encouraged to set an example with their own water consumption. Water consumption from reusable bottles was also connected to environmental health. During the training, peer leaders identified drinking water themselves and sharing the health and environmental benefits of water consumption as key messages. Follow-up training sessions were provided during weeks 2 and 4 of the intervention. | Peer leaders were tasked with promoting water consumption to their peers through their social networks over a period of 8 weeks. | Outcome: water and SSB consumption, intention to drink more water. Results: Students in the intervention group reported a significant increase in water consumption and a significant decrease in SSB consumption post-intervention compared to a control group. |
| Tamiru, 2016 [68] | A peer-led nutrition education intervention that included health promotion through school media and clubs, as well as school and community events | 11–19 years old (n = 992), Jimma, Ethiopia | Peer leaders selected from among the target population | Peer leaders had a training session with the research team to learn about their role and responsibilities. Leaders were provided with health promotion materials to use in group education. Teachers held peer dialogue sessions throughout the intervention to support peer educators. | Over 8 months, peer leaders taught a group of fellow students via demonstration and role-playing in weekly sessions. | Outcome: changes in knowledge, attitude, dietary quality and variety, and anthropometric measurements. The study also assessed food insecurity and its relationship to dietary intake. Results: Youth from food secure households had significantly higher dietary diversity compared with those from food insecure households. More than 2/3 of students reported their food was selected by their parent/guardian as opposed to self- selected. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
St. Pierre, C.; Guan, W.; Barry, L.; Dease, G.; Gottlieb, S.; Morris, A.; Merrill, J.; Sacheck, J.M. Themes in Train-the-Trainer Nutrition Education Interventions Targeting Middle School Students: A Systematic Review. Nutrients 2021, 13, 2749. https://doi.org/10.3390/nu13082749
St. Pierre C, Guan W, Barry L, Dease G, Gottlieb S, Morris A, Merrill J, Sacheck JM. Themes in Train-the-Trainer Nutrition Education Interventions Targeting Middle School Students: A Systematic Review. Nutrients. 2021; 13(8):2749. https://doi.org/10.3390/nu13082749
Chicago/Turabian StyleSt. Pierre, Christine, Win Guan, Leah Barry, Grace Dease, Sydney Gottlieb, Arielle Morris, Jamison Merrill, and Jennifer M. Sacheck. 2021. "Themes in Train-the-Trainer Nutrition Education Interventions Targeting Middle School Students: A Systematic Review" Nutrients 13, no. 8: 2749. https://doi.org/10.3390/nu13082749
APA StyleSt. Pierre, C., Guan, W., Barry, L., Dease, G., Gottlieb, S., Morris, A., Merrill, J., & Sacheck, J. M. (2021). Themes in Train-the-Trainer Nutrition Education Interventions Targeting Middle School Students: A Systematic Review. Nutrients, 13(8), 2749. https://doi.org/10.3390/nu13082749