
The Joint Effect of Maternal Marital Status and Type of Household Cooking Fuel on Child Nutritional Status in Sub-Saharan Africa: Analysis of Cross-Sectional Surveys on Children from 31 Countries

 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
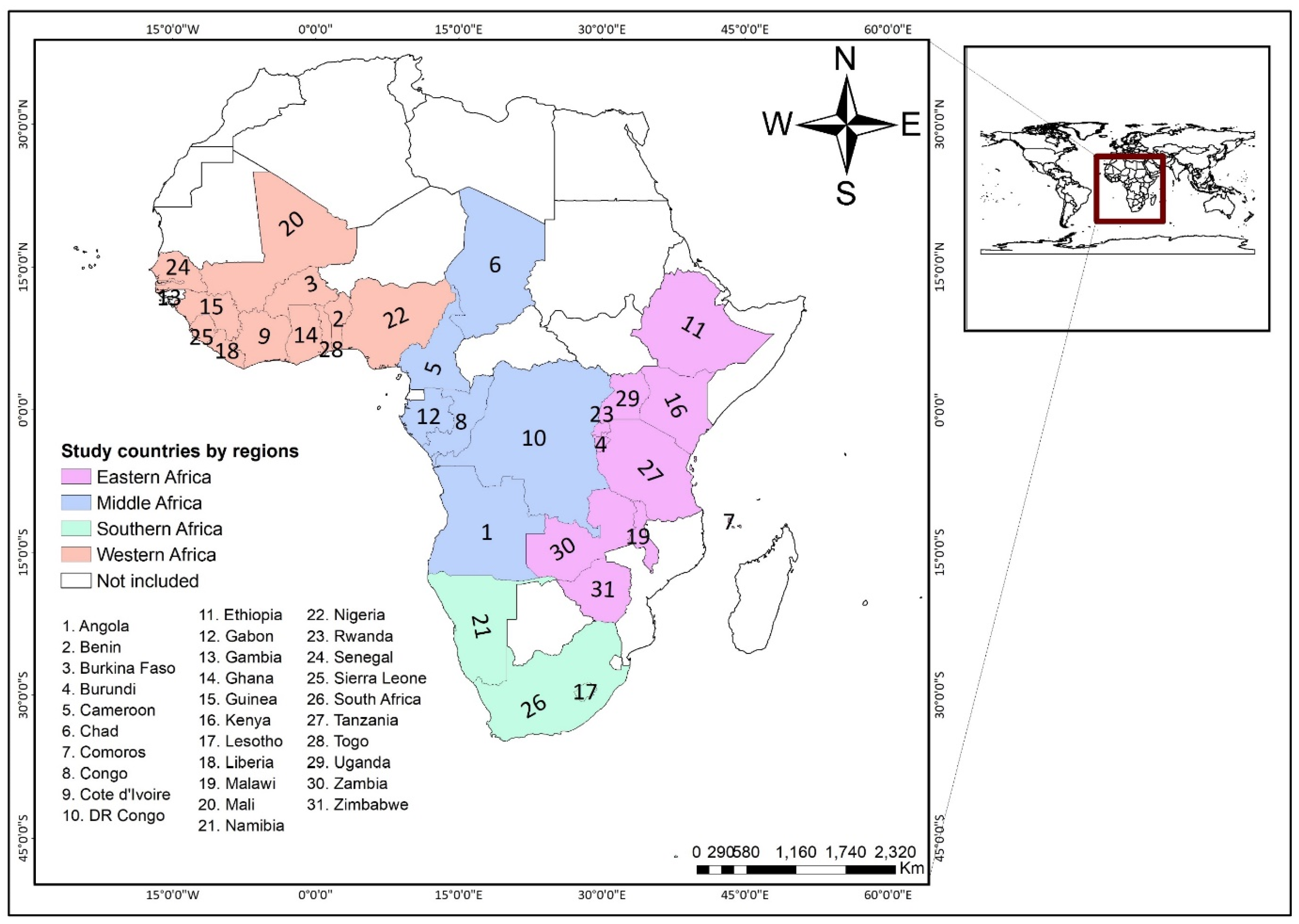
2.1. Data Source
2.2. Measures
2.2.1. Outcome Variables
- Stunting: children with height-for-age z-scores below minus 2 (−2.0) standard deviations less than the mean on the WHO Child Growth Standards (moderately or severely stunted) and children with height-for-age z-scores below minus 3 (−3.0) standard deviations less than the mean on the WHO Child Growth Standards (severely stunted) were combined to form the response group “Stunt” while those height-for-age z-scores equal to or higher than minus 2 (−2.0) standard deviations greater than the mean on the WHO Child Growth Standards were regarded as “not a stunt”.
- Wasting: children with weight-for-height z-scores below minus 2 (−2.0) standard deviations less than the mean on the WHO Child Growth Standards (moderately or severely wasting) and children with weight-for-height z-scores below minus 3 (−3.0) standard deviations less than the mean on the WHO Child Growth Standards (severely wasting) were combined to form the response group “Wasting” while those weight-for-height z-scores equal to or higher than minus 2 (−2.0) standard deviations greater than the mean on the WHO Child Growth Standards were regarded as “No wasting”.
- Underweight: children with weight-for-age z-scores below minus 2 (−2.0) standard deviations less than the mean on the WHO Child Growth Standards (moderately or severely underweight) and children with weight-for-age z-scores below minus 3 (−3.0) standard deviations less than the mean on the WHO Child Growth Standards (severely underweight) were combined to form the response group “Underweight” while those weight-for-age z-scores equal to or higher than minus 2 (−2.0) standard deviations greater than the mean on the WHO Child Growth Standards were regarded as “Not underweight”. For each of these variables, “age out of plausible limits”, “height out of plausible limits”, missing and “flagged” responses which constituted, 13, 744, 1833 and 3285 respectively were deemed invalid and dropped.
2.2.2. Key Predictor Variable
2.2.3. Covariates
2.3. Data Analyses
2.4. Ethical Approval
3. Results
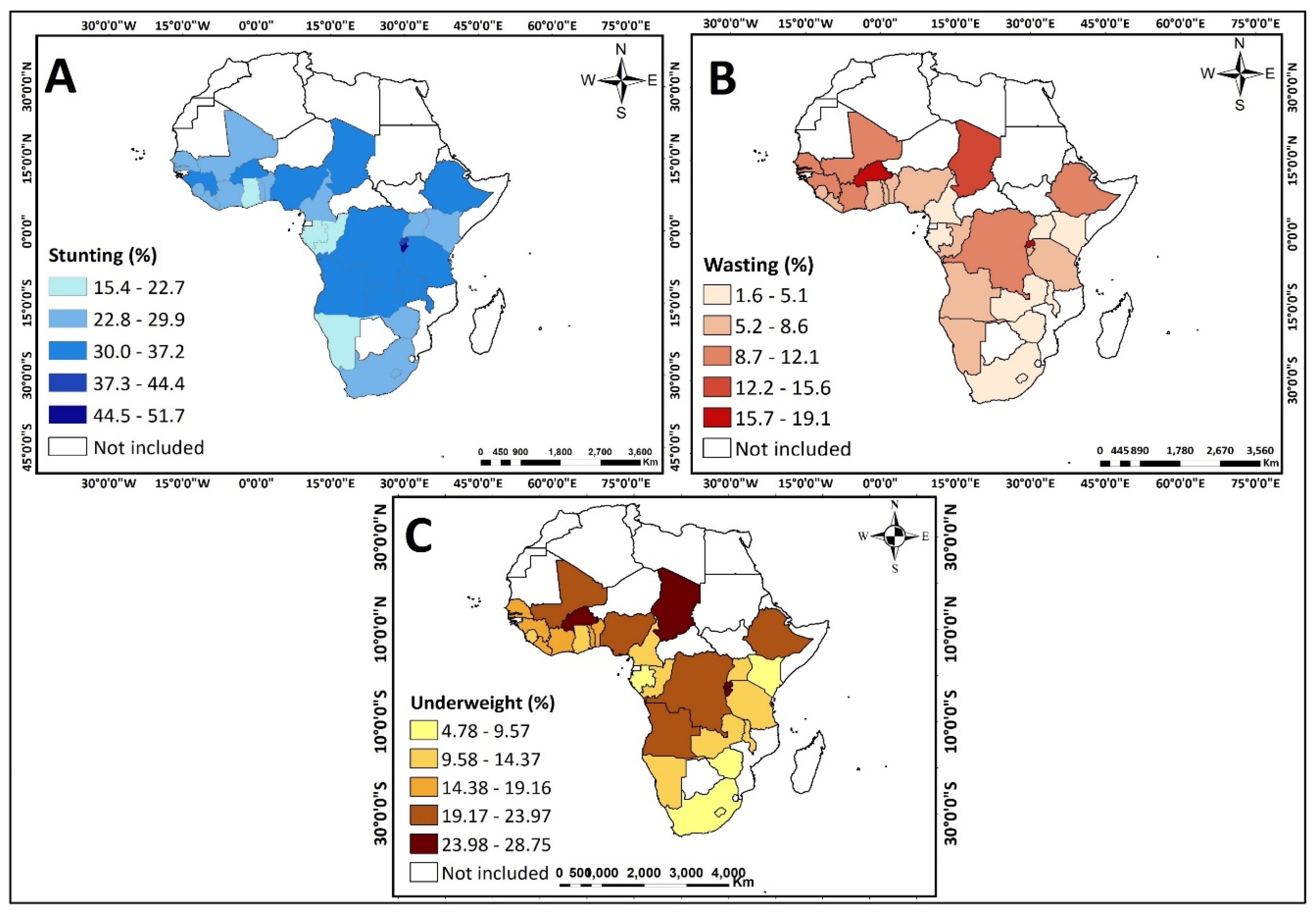
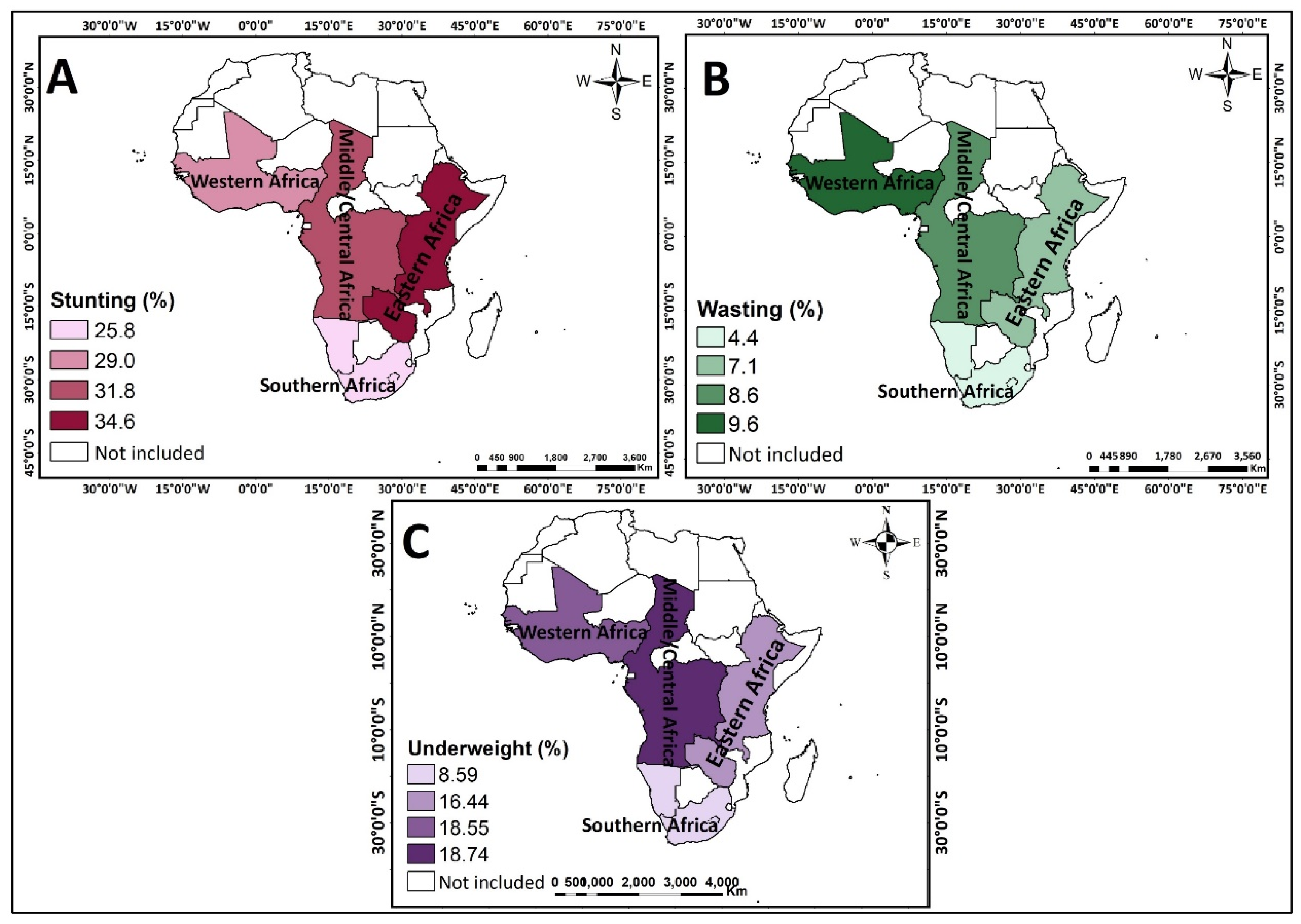
3.1. Descriptive Analysis on the Percentage of Children Who Were Stunted, Wasted and Underweight in the 31 Countries in SSA
3.2. Multivariate Analysis on the Joint Effect of Single-Motherhood and Unclean Household Cooking Fuel Use on Child Nutritional Status
4. Discussion
4.1. Strength and Limitations
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Remans, R.; Flynn, D.F.B.; Declerck, F.; Diru, W.; Fanzo, J.; Gaynor, K.; Lambrecht, I.; Mudiope, J.; Mutuo, P.K.; Nkhoma, P.; et al. Assessing nutritional diversity of cropping systems in African villages. PLoS ONE 2011, 6, e21235. [Google Scholar] [CrossRef] [Green Version]
- Ntoimo, L.F.C.; Odimegwu, C.O. Health effects of single motherhood on children in sub-Saharan Africa: A cross-sectional study. BMC Public Health 2014, 14, 1145. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. Briefing Note Series on SDG Global Indicators Related to Children. 2018. Available online: File:///C:/Users/iddri/AppData/Local/Temp/SDG-briefing-note-1_introduction.pdf (accessed on 6 March 2021).
- De Onis, M.; Blössner, M.; Borghi, E. Prevalence and trends of stunting among pre-school children, 1990–2020. Public Health Nutr. 2012, 15, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Devlin, K. Stunting limits learning and future earnings of children. World J. 2012, 40, 26. [Google Scholar]
- Darteh, E.K.M.; Acquah, E.; Kumi-Kyereme, A. Correlates of stunting among children in Ghana. BMC Public Health 2014, 14, 504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goudet, S.M.; Kimani-Murage, E.W.; Wekesah, F.; Wanjohi, M.; Griffiths, P.L.; Bogin, B.; Madise, N.J. How does poverty affect children’s nutritional status in Nairobi slums? A qualitative study of the root causes of undernutrition. Public Health Nutr. 2016, 20, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Saaka, M.; Wemakor, A.; Abizari, A.-R.; Aryee, P.A. How well do WHO complementary feeding indicators relate to nutritional status of children aged 6–23 months in rural Northern Ghana? BMC Public Health 2015, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Clark, S.; Hamplová, D. Single motherhood and child mortality in sub-Saharan Africa: A life course perspective. Demography 2013, 50, 1521–1549. [Google Scholar] [CrossRef] [PubMed]
- Odimegwu, C.; Somefun, O.D.; De Wet, N. Contextual determinants of family dissolution in sub-Saharan Africa. Dev. S. Afr. 2017, 34, 721–737. [Google Scholar] [CrossRef]
- Owili, P.O.; Muga, M.A.; Pan, W.-C.; Kuo, H.-W. Cooking fuel and risk of under-five mortality in 23 Sub-Saharan African countries: A population-based study. Int. J. Environ. Health Res. 2017, 27, 191–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obasohan, P.E.; Walters, S.J.; Jacques, R.; Khatab, K. Risk factors associated with malnutrition among children under-five years in sub-Saharan African countries: A scoping review. Int. J. Environ. Res. Public Health 2020, 17, 8782. [Google Scholar] [CrossRef]
- Wali, N.; Agho, K.E.; Renzaho, A.M. factors associated with stunting among children under 5 years in five South Asian countries (2014–2018): Analysis of demographic health surveys. Nutrients 2020, 12, 3875. [Google Scholar] [CrossRef]
- Tanwi, T.S.; Chakrabarty, S.; Hasanuzzaman, S. Double burden of malnutrition among ever-married women in Bangladesh: A pooled analysis. BMC Womens Health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Ezeh, O.K.; Agho, K.E.; Dibley, M.J.; Hall, J.J.; Page, A.N. The effect of solid fuel use on childhood mortality in Nigeria: Evidence from the 2013 cross-sectional household survey. Environ. Health 2014, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Corsi, D.J.; Neuman, M.; E Finlay, J.; Subramanian, S.V. Demographic and health surveys: A profile. Int. J. Epidemiol. 2012, 41, 1602–1613. [Google Scholar] [CrossRef]
- Rutstein, S.O.; Rojas, G. Guide to DHS Statistics; ORC Macro: Calverton, MD, USA, 2006; Volume 38. [Google Scholar]
- DHS. Guide to DHS Statistics DHS-7: Nutritional Status. 2021. Available online: https://dhsprogram.com/data/Guide-to-DHS-Statistics/Nutritional_Status.htm (accessed on 11 March 2021).
- Armah, F.A.; Ekumah, B.; Yawson, D.O.; Odoi, J.O.; Afitiri, A.-R.; Nyieku, F.E. Predictive probabilities of access to clean cooking: Evidence from the demographic and health surveys in 31 countries in sub-Saharan Africa. Environ. Justice 2019, 12, 118–131. [Google Scholar] [CrossRef] [Green Version]
- Amegah, A.K.; Boachie, J.; Näyhä, S.; Jaakkola, J.J.K. Association of biomass fuel use with reduced body weight of adult Ghanaian women. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Yaya, S.; Uthman, O.A.; Ekholuenetale, M.; Bishwajit, G.; Adjiwanou, V. Effects of birth spacing on adverse childhood health outcomes: Evidence from 34 countries in sub-Saharan Africa. J. Matern. Neonatal Med. 2019, 33, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amare, Z.Y.; Ahmed, M.E.; Mehari, A.B. Determinants of nutritional status among children under age 5 in Ethiopia: Further analysis of the 2016 Ethiopia demographic and health survey. Glob. Health 2019, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armah, F.A.; Ekumah, B.; Yawson, D.O.; Odoi, J.O.; Afitiri, A.-R.; Nyieku, F.E. Access to improved water and sanitation in sub-Saharan Africa in a quarter century. Heliyon 2018, 4, e00931. [Google Scholar] [CrossRef] [Green Version]
- Odjidja, E.N.; Christensen, C.; Gatasi, G.; Hakizimana, S.; Murorunkwere, H.; Masabo, J.-B.; Meguid, T. 2030 Countdown to combating malnutrition in Burundi: Comparison of proactive approaches for case detection and enrolment into treatment. Int. Health 2020. [Google Scholar] [CrossRef] [Green Version]
- Nkurunziza, S.; Meessen, B.; Van Geertruyden, J.-P.; Korachais, C. Determinants of stunting and severe stunting among Burundian children aged 6-23 months: Evidence from a national cross-sectional household survey, 2014. BMC Pediatr. 2017, 17, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akombi, B.J.; Agho, K.E.; Merom, D.; Renzaho, A.M.; Hall, J.J. Child malnutrition in sub-Saharan Africa: A meta-analysis of demographic and health surveys (2006–2016). PLoS ONE 2017, 12, e0177338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daboné, C.; Delisle, H.F.; Receveur, O. Poor nutritional status of schoolchildren in urban and peri-urban areas of Ouagadougou (Burkina Faso). Nutr. J. 2011, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Ekholuenetale, M.; Tudeme, G.; Onikan, A.; Ekholuenetale, C.E. Socioeconomic inequalities in hidden hunger, undernutrition, and overweight among under-five children in 35 sub-Saharan Africa countries. J. Egypt. Public Health Assoc. 2020, 95, 1–15. [Google Scholar] [CrossRef] [Green Version]
- United Nations. The Millennium Development Goals Report; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Islam, S.; Rana, J.; Mohanty, S.K. Cooking, smoking, and stunting: Effects of household air pollution sources on childhood growth in India. Indoor Air 2021, 31, 229–249. [Google Scholar] [CrossRef]
- Balietti, A.; Datta, S. The Impact of Indoor Solid Fuel Use on the Stunting of Indian Children. 2017. Available online: http://www.ancabalietti.net/wp-content/uploads/2017/04/Datta_Balietti_March2017.pdf (accessed on 3 March 2021).
- Upadhyay, A.K.; Singh, A.; Kumar, K.; Singh, A. Impact of indoor air pollution from the use of solid fuels on the incidence of life threatening respiratory illnesses in children in India. BMC Public Health 2015, 15, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlaudecker, E.P.; Steinhoff, M.C.; Moore, S.R. Interactions of diarrhea, pneumonia, and malnutrition in childhood: Recent evidence from developing countries. Curr. Opin. Infect. Dis. 2011, 24, 496. [Google Scholar] [CrossRef]
- Tielsch, J.M.; Katz, J.; Thulasiraj, R.D.; Coles, C.L.; Sheeladevi, S.; Yanik, E.L.; Rahmathullah, L. Exposure to indoor biomass fuel and tobacco smoke and risk of adverse reproductive outcomes, mortality, respiratory morbidity and growth among newborn infants in south India. Int. J. Epidemiol. 2009, 38, 1351–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dearden, K.; Crookston, B.; Madanat, H.; West, J.; Penny, M.; Cueto, S. What difference can fathers make? Early paternal absence compromises Peruvian children’s growth. Matern. Child Nutr. 2011, 9, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Bronte-Tinkew, J.; DeJong, G. Children’s nutrition in Jamaica: Do household structure and household economic resources matter? Soc. Sci. Med. 2004, 58, 499–514. [Google Scholar] [CrossRef]
- Gurmu, E.; Etana, D. Household structure and children’s nutritional status in Ethiopia. Genus 2013, 69, 113–130. [Google Scholar]
- Izugbara, C. Single motherhood and neonatal and infant mortality in Sierra Leone, Burkina Faso and Burundi. Public Health 2016, 135, 122–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertz, R.; Mattes, J.; Shook, A. When paid work invades the family: Single mothers in the COVID-19 pandemic. J. Fam. Issues 2020. [Google Scholar] [CrossRef]
- Gakidou, E.; Oza, S.; Fuertes, C.V.; Li, A.Y.; Lee, D.K.; Sousa, A.; Hogan, M.C.; Vander Hoorn, S.; Ezzati, M. Improving child survival through environmental and nutritional interventions: The importance of targeting interventions toward the poor. J. Am. Med. Assoc. 2007, 298, 1876–1887. [Google Scholar] [CrossRef] [Green Version]
- Odo, D.B.; Yang, I.A.; Knibbs, L.D. A systematic review and appraisal of epidemiological studies on household fuel use and its health effects using demographic and health surveys. Int. J. Environ. Res. Public Health 2021, 18, 1411. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Weighted N | Weighted % | Variable | Weighted N | Weighted % |
|---|---|---|---|---|---|
| Key outcome variables | Household characteristics | ||||
| Stunting | 40,453 | 31 | Wealth status | ||
| Wasting | 10,770 | 8 | Poor | 54,734 | 42 |
| Underweight | 22,503 | 17 | Middle | 26,262 | 20 |
| Rich | 48,650 | 38 | |||
| Key predictor variable | Age of household head | ||||
| Maternal marital status | Young-adults | 55,803 | 43 | ||
| Single | 14,071 | 11 | Middle-aged adults | 56,748 | 44 |
| Married | 2645 | 2 | Old-aged adults | 17,094 | 13 |
| Type of cooking fuel | 102,192 | 79 | Sex of household head | ||
| Clean Unclean | 10,725 | 8 | Male | 103,254 | 80 |
| Child characteristics | Female | 26,392 | 20 | ||
| Age | Access to electricity | ||||
| 0 | 39,906 | 31 | No | 89,364 | 69 |
| 1 | 36,828 | 28 | Yes | 40,272 | 31 |
| 2 | 26,214 | 20 | Type of toilet facility | ||
| 3 | 16,128 | 12 | Improved | 55,247 | 43 |
| 4 | 10,571 | 8 | Unimproved | 74,375 | 57 |
| Sex | Source of drinking water | ||||
| Male | 65,442 | 50 | Improved | 85,103 | 66 |
| Female | 64,204 | 50 | Unimproved | 44,531 | 34 |
| Birth order | Type of cooking fuel | ||||
| 1 | 25,421 | 20 | Unclean | 116,263 | 90 |
| 2 to 4 | 62,426 | 48 | Clean | 13,369 | 10 |
| 5 and above | 41,799 | 32 | Access to media (tv/radio/newspaper) | ||
| Perceived size at birth | No | 45,684 | 35 | ||
| Large | 43,855 | 34 | Yes | 83,962 | 65 |
| Average | 64,360 | 50 | Contextual factors | ||
| Small | 21,422 | 17 | Urbanicity | ||
| Weight at birth | Urban | 43,412 | 33 | ||
| Underweight | 7180 | 6 | Rural | 86,234 | 67 |
| Normal | 72,089 | 56 | Country | ||
| Not taken | 50,377 | 39 | Angola | 7384 | 6 |
| Stunting | Benin | 15,857 | 12 | ||
| Severely/moderately stunting | 40,454 | 31 | Burkina Faso | 8908 | 7 |
| No stunting | 89,192 | 69 | Burundi | 4174 | 3 |
| Wasting | Cameroon | 2936 | 2 | ||
| Severely/moderately wasting | 10,770 | 8 | Chad | 6114 | 5 |
| No wasting | 118,876 | 92 | Comoros | 1523 | 1 |
| Underweight | Congo | 2620 | 2 | ||
| Not underweight | 107,136.99 | 83 | Cote d’Ivoire | 2190 | 2 |
| Underweight | 22,503.33 | 17 | DR Congo | 4842 | 4 |
| Mother’s characteristics | Ethiopia | 6585 | 5 | ||
| Maternal marital status | Gabon | 1998 | 2 | ||
| single | 16,718 | 13 | Gambia | 746 | 1 |
| Married | 112,928 | 87 | Ghana | 1908 | 1 |
| Maternal Age | Guinea | 2291 | 2 | ||
| 15–19 | 9230 | 7 | Kenya | 6082 | 5 |
| 20–49 | 120,416 | 93 | Lesotho | 1018 | 1 |
| Educational attainment | Liberia | 2035 | 2 | ||
| No education | 54,150 | 42 | Malawi | 4035 | 3 |
| Primary | 40,339 | 31 | Mali | 5785 | 4 |
| Secondary | 31,071 | 24 | Namibia | 1155 | 1 |
| Higher | 4086 | 3 | Nigeria | 7502 | 6 |
| Working status | Rwanda | 4424 | 3 | ||
| No | 46,034 | 36 | Senegal | 1989 | 2 |
| Yes | 83,505 | 64 | Siera Leone | 3052 | 2 |
| Antenatal visits during pregnancy | South Africa | 877 | 1 | ||
| No | 13,711 | 11 | Tanzania | 6088 | 5 |
| Yes | 113,765 | 88 | Togo | 2227 | 2 |
| Dont’ know | 2153 | 2 | Uganda | 2900 | 2 |
| Postnatal check within 2 months | Zambia | 6402 | 5 | ||
| No | 75,893 | 59 | Zimbabwe | 4000 | 3 |
| Yes | 53,753 | 41 | Geographic region | ||
| Place of delivery | Western Africa | 54,489 | 42 | ||
| Home | 40,300 | 31 | Eastern Africa | 42,213 | 33 |
| Health facility | 87,846 | 68 | Central Africa | 25,894 | 20 |
| Other | 1494 | 1 | South Africa | 7051 | 5 |
| Total | 129,646 | ||||
| Independent Variables | Stunting (Weighted %) | 95% CI | p-Value | Wasting (Weighted %) | 95% CI | p-Value | Underweight (Weighted %) | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Key predictor variables | |||||||||
| Maternal marital status | 0.382 | <0.001 | <0.001 | ||||||
| Single | 31.3 | 30.5–32.0 | 6.4 | 6.0–6.7 | 15.5 | 15.0–16.1 | |||
| Married | 31.2 | 30.9–31.5 | 8.6 | 8.4–8.8 | 17.6 | 17.4–17.9 | |||
| Type of cooking fuel | <0.001 | <0.001 | <0.001 | ||||||
| Unclean | 32.6 | 32.4–32.9 | 8.7 | 8.5–8.9 | 18.3 | 18.1–18.5 | |||
| Clean | 18.8 | 18.1–18.4 | 5.0 | 4.6–5.3 | 9 | 8.5–9.5 | |||
| Child characteristics | |||||||||
| Age of child | <0.001 | <0.001 | <0.001 | ||||||
| 0 | 16.8 | 16.4–17.2 | 11.1 | 10.8–11.4 | 13.56 | 13.2–13.0 | |||
| 1 | 36.3 | 35.8–36.8 | 9.7 | 9.4–10.0 | 19.97 | 19.6–20.4 | |||
| 2 | 43.5 | 42.9–44.1 | 6.2 | 5.9–6.5 | 20.59 | 20.1–21.1 | |||
| 3 | 37.2 | 36.438.0 | 4.3 | 4.0–4.6 | 16.84 | 16.3–17.4 | |||
| 4 | 28.2 | 27.3–29.0 | 4.4 | 4.0–4.8 | 15.35 | 14.7–16.1 | |||
| Sex of child | <0.001 | <0.001 | <0.001 | ||||||
| Male | 34.0 | 33.6–34.4 | 9.2 | 8.9–9.4 | 18.84 | 18.5–19.1 | |||
| Female | 28.3 | 28.0–28.7 | 7.5 | 7.2–7.7 | 15.85 | 15.6–16.1 | |||
| Birth order | <0.001 | <0.001 | <0.001 | ||||||
| 1 | 29.5 | 28.9–30.0 | 7.5 | 7.2–7.8 | 15.23 | 14.8–15.7 | |||
| 2 to 4 | 30.0 | 29.4–30.1 | 7.9 | 7.7–8.2 | 16.15 | 15.9–16.4 | |||
| 5 and above | 34.4 | 33.9–34.8 | 9.3 | 9.1–9.6 | 20.45 | 20.0–20.8 | |||
| Perceived size at birth | <0.001 | <0.001 | <0.001 | ||||||
| Large | 26.7 | 26.3–27.1 | 6.4 | 6.2–6.6 | 12.93 | 12.6–13.2 | |||
| Average | 31.4 | 31.0–31.8 | 8.3 | 8.1–8.5 | 17.02 | 16.7–17.3 | |||
| Small | 39.8 | 39.1–40.4 | 12.2 | 11.7–12.6 | 27.45 | 26.9–28.0 | |||
| Mother’s characteristics | |||||||||
| Maternal age | 0.604 | <0.001 | 0.189 | ||||||
| 15–19 | 31.0 | 30.0–31.9 | 9.6 | 9.0–10.2 | 17.68 | 16.9–18.5 | |||
| 20–49 | 31.2 | 31.0–31.5 | 8.2 | 8.1–8.4 | 17.33 | 17.1–17.5 | |||
| Educational attainment | <0.001 | <0.001 | <0.001 | ||||||
| No education | 36.6 | 36.2–37.0 | 11.5 | 11.3–11.8 | 24.02 | 23.7–24.3 | |||
| Primary | 32.6 | 32.1–33.0 | 6.4 | 6.2–6.7 | 15.1 | 14.8–15.5 | |||
| Secondary | 22.6 | 22.2–23.1 | 5.6 | 5.3–5.9 | 10.19 | 9.9–10.5 | |||
| Higher | 10.9 | 10.0–11.9 | 4.6 | 4.0–5.3 | 5.81 | 5.1–6.6 | |||
| Working status | 0.017 | <0.001 | <0.001 | ||||||
| No | 30.8 | 30.3–31.2 | 9.6 | 9.4–9.9 | 18.16 | 17.8–18.5 | |||
| Yes | 31.4 | 31.1–31.8 | 7.6 | 7.4–7.7 | 16.91 | 16.7–17.3 | |||
| Antenatal visits during pregnancy | <0.001 | <0.001 | <0.001 | ||||||
| No | 41.7 | 41.0–42.6 | 12.5 | 12.0–13.1 | 28.42 | 27.7–29.2 | |||
| Yes | 30.0 | 29.8–30.3 | 7.8 | 7.7–8.0 | 16.1 | 15.9–16.3 | |||
| Dont’know | 26.3 | 24.4–28.2 | 7.6 | 6.5–8.8 | 13.07 | 11.7–14.6 | |||
| Postnatal check within 2 months | <0.001 | 0.748 | <0.001 | ||||||
| No | 33.0 | 32.6–33.3 | 8.3 | 8.1–8.5 | 18.54 | 18.3–18.8 | |||
| Yes | 28.7 | 28.3–29.1 | 8.4 | 8.1–8.6 | 15.69 | 15.4–16.0 | |||
| Place of delivery | <0.001 | <0.001 | <0.001 | ||||||
| Home | 38.5 | 38.1–39.0 | 11.2 | 11.0–11.5 | 24.9 | 24.5–25.3 | |||
| Health facility | 27.8 | 27.5–28.1 | 7.0 | 6.8–7.1 | 13.87 | 13.6–14.1 | |||
| Other | 34.8 | 32.4–37.3 | 7.5 | 6.2–9.0 | 19.26 | 17.3–21.4 | |||
| Household characteristics | |||||||||
| Wealth status | <0.001 | <0.001 | <0.001 | ||||||
| Poor | 37.2 | 36.8–37.6 | 9.4 | 9.1–9.6 | 21.28 | 20.9–21.6 | |||
| Middle | 32.6 | 32.0–33.2 | 8.2 | 7.9–8.6 | 17.8 | 17.3–18.3 | |||
| Rich | 23.7 | 23.4–24.1 | 7.2 | 6.9–7.4 | 12.71 | 12.4–13.0 | |||
| Age of household head | 0.680 | 0.791 | <0.001 | ||||||
| Young-adults | 31.5 | 31.1–32.0 | 8.2 | 7.9–8.4 | 16.8 | 16.5–17.1 | |||
| Middle-aged adults | 30.9 | 30.5–31.3 | 8.5 | 8.2–8.7 | 17.83 | 17.5–18.1 | |||
| Old-aged adults | 31.1 | 30.4–31.8 | 8.3 | 7.9–8.7 | 17.61 | 17.0–18.2 | |||
| Sex of household head | <0.05 | <0.001 | <0.001 | ||||||
| Male | 31.4 | 31.1–31.7 | 8.7 | 8.5–8.9 | 17.78 | 17.5–18.0 | |||
| Female | 30.5 | 30.0–31.0 | 6.9 | 6.6–7.3 | 15.72 | 15.3–16.2 | |||
| Access to electricity | <0.001 | <0.001 | <0.001 | ||||||
| No | 35.3 | 35.0–35.6 | 9.2 | 9.0–9.4 | 20.01 | 19.7–20.3 | |||
| Yes | 22.1 | 21.7–22.5 | 6.3 | 6.0–6.5 | 11.47 | 11.1–11.8 | |||
| Type of toilet facility | <0.001 | <0.001 | <0.001 | ||||||
| Improved | 26.8 | 26.4–27.2 | 6.4 | 6.2–6.6 | 13.07 | 12.8–13.3 | |||
| Unimproved | 34.5 | 34.1–34.8 | 9.7 | 9.5–9.9 | 20.54 | 20.3–20.8 | |||
| Source of drinking water | <0.001 | <0.05 | <0.001 | ||||||
| Improved | 30.1 | 29.8–30.4 | 8.2 | 8.0–8.4 | 16.64 | 16.4–16.9 | |||
| Unimproved | 33.4 | 32.9–33.8 | 8.5 | 8.3–8.8 | 18.72 | 18.4–19.1 | |||
| Access to media (tv/radio/newspaper) | <0.001 | <0.001 | <0.001 | ||||||
| No | 37.9 | 37.4–38.3 | 10.0 | 9.7–10.2 | 22.43 | 22.0–22.8 | |||
| Yes | 27.6 | 27.3–27.9 | 7.4 | 7.2–7.6 | 14.6 | 14.4–14.8 | |||
| Contextual factors | |||||||||
| Urbanicity | <0.001 | <0.001 | <0.001 | ||||||
| Urban | 23.6 | 23.2–24.0 | 6.6 | 6.3–6.8 | 12.12 | 11.8–12.4 | |||
| Rural | 35.0 | 34.7–35.4 | 9.2 | 9.0–9.4 | 20 | 19.7–20.3 | |||
| Geographic region | <0.001 | <0.001 | <0.001 | ||||||
| Western Africa | 29.0 | 28.6–29.4 | 9.6 | 9.4–9.8 | 18.55 | 18.2–18.9 | |||
| Eastern Africa | 34.6 | 34.1–35.0 | 7.1 | 6.9–7.4 | 16.44 | 16.1–16.8 | |||
| Central Africa | 31.8 | 31.3–32.4 | 8.6 | 8.3–8.9 | 18.74 | 18.3–19.2 | |||
| South Africa | 25.8 | 24.7–26.8 | 4.4 | 3.9–4.9 | 8.59 | 8.0–9.3 |
| Key Predictor Variable | Model 0 | Model I | Model II | Model III | Model IV | Model V |
|---|---|---|---|---|---|---|
| OR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | ||
| Fixed effects | ||||||
| Maternal marital status-Cooking fuel | ||||||
| Married-clean | 1 | 1 | 1 | 1 | 1 | |
| Single unclean | 2.22 *** (2.08–2.36) | 1.65 *** (1.54–1.77) | 1.49 *** (1.39–1.60) | 1.83 *** (1.71–1.95) | 1.27 *** (1.17–1.47) | |
| Single clean | 1.25 *** (1.12–1.39) | 1.21 *** (1.08–1.36) | 1.22 *** (1.09–1.36) | 1.23 *** (1.10–1.37) | 1.18 * (1.05–1.32) | |
| Married-unclean | 2.25 *** (2.03–2.26) | 1.49 *** (1.41–1.59) | 0.04 *** (1.32–1.48) | 1.76 *** (1.66–1.87) | 1.25 *** (1.17–1.33) | |
| Random effects | ||||||
| PSU Variance (95% CI) | 0.02 (0.18–0.03) | 0.02 (0.02–0.3) | 0.02 (0.02–0.03) | 0.02 (0.01–0.03) | 0.02 (0.01–0.03) | 0.02 (0.01–0.03) |
| ICC | 0.007 | 0.007 | 0.006 | 0.006 | 0.006 | 0.006 |
| LR Test | 161.74 *** | 141.62 *** | 111.82 *** | 118.11 *** | 121.89 *** | 105.02 *** |
| Wild χ2 | Reference | 864.24 *** | 10,324.15 *** | 2958.64 *** | 2061.47 *** | 11,264.12 *** |
| Model fitness | ||||||
| Log-likelihood | −81,022.8 | −80,532.1 | −74,861.3 | −79,409.4 | −79,911.5 | −74,213.7 |
| AIC | 162,049.6 | 161,074.3 | 149,770.6 | 158,846.9 | 159,841 | 148,501.4 |
| Number of clusters | 1608 | 1608 | 1608 | 1608 | 1608 | 1608 |
| Key Predictor Variable | Model 0 | Model I | Model II | Model III | Model IV | Model V |
|---|---|---|---|---|---|---|
| OR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | ||
| Fixed effects | ||||||
| Maternal marital status-Cooking fuel | ||||||
| Married-clean | 1 | 1 | 1 | 1 | 1 | |
| Single unclean | 1.46 *** (1.30–1.63) | 1.23 ** (1.09–1.39) | 1.12 (0.99–1.27) | 1.32 *** (1.17–1.49) | 1.17 * (1.03–1.33) | |
| Single clean | 0.92 (0.74–1.14) | 0.91 (0.73–1.13) | 0.94 (0.75–1.17) | 0.97 (0.78–1.20) | 0.97 (0.78–1.21) | |
| Married-unclean | 1.98 *** (1.80–2.19) | 1.35 *** (1.22–1.50) | 1.45 *** (1.30–1.61) | 1.69 *** (1.54–1.88) | 1.24 *** (1.11–1.39) | |
| Random effects | ||||||
| PSU Variance (95% CI) | 0.04 (0.03–0.06) | 0.4 (0.03–0.06) | 0.04 (0.03–0.05) | 0.04 (0.03–0.05) | 0.04 (0.03–0.5) | 0.04 (0.03–0.5) |
| ICC | 0.012 | 0.013 | 0.012 | 0.012 | 0.013 | 0.012 |
| LR Test | 84.12 *** | 86.79 *** | 78.58 *** | 82.1 *** | 86.54 *** | 77.54 *** |
| Wild χ2 | Reference | 302.86 *** | 3430.13 *** | 813.45 *** | 633.06 *** | 3623.65 *** |
| Model fitness | ||||||
| Log-likelihood | −37,598.7 | −37,423.4 | −35,695.6 | −37,145.5 | −37,243.6 | −35,562.1 |
| AIC | 75,201.42 | 74,856.82 | 71,439.27 | 74,319.03 | 74,505.22 | 71,198.25 |
| Number of clusters | 1608 | 1608 | 1608 | 1608 | 1608 | 1608 |
| Key Predictor Variable | Model 0 | Model I | Model II | Model III | Model IV | Model V |
|---|---|---|---|---|---|---|
| OR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | ||
| Fixed effects | ||||||
| Marital status-Cooking fuel | ||||||
| Married-clean | 1 | 1 | 1 | 1 | 1 | |
| Single unclean | 2.26 *** (2.08–2.47) | 1.62 *** (1.48–1.77) | 1.46 *** (1.32–1.60) | 1.87 *** (1.71–2.04) | 1.41 *** (1.28–1.55) | |
| Single clean | 1.21 *** (1.13–1.52) | 1.28 * (1.10–1.50) | 1.29 * (1.11–1.50) | 1.38 *** (1.19–1.61) | 1.33 *** (1.14–1.55) | |
| Married-unclean | 2.60 *** (2.41–2.80) | 1.56 *** (1.44–1.69) | 1.61 *** (1.48–1.74) | 2.01 *** (1.86–2.18) | 1.33 *** (1.22–1.45) | |
| Random effects | ||||||
| PSU Variance (95% CI) | 0.03 (0.02–0.04) | 0.03 (0.02–0.04) | 0.02 (0.02–0.03) | 0.03 (0.02–0.03) | 0.03 (0.02–0.04) | 0.02 (0.02–0.03) |
| ICC | 0.009 | 0.009 | 0.007 | 0.008 | 0.008 | 0.007 |
| LR Test | 124.1 *** | 118.46 *** | 76.82 *** | 101.51 *** | 115.42 *** | 80.61 *** |
| Wild χ2 | Reference | 707.76 *** | 6725.19 *** | 2423.9 *** | 1821.05 *** | 7154.32 *** |
| Model fitness | ||||||
| Log-likelihood | −60,841.6 | −60,404.4 | −57,078.2 | −59,474.5 | −59,780.2 | −56,749.8 |
| AIC | 121,687.2 | 120,818.7 | 114,204.4 | 118,977 | 119,578.4 | 113,573.6 |
| Number of clusters | 1608 | 1608 | 1608 | 1608 | 1608 | 1608 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amadu, I.; Seidu, A.-A.; Duku, E.; Okyere, J.; Hagan, J.E., Jr.; Hormenu, T.; Ahinkorah, B.O. The Joint Effect of Maternal Marital Status and Type of Household Cooking Fuel on Child Nutritional Status in Sub-Saharan Africa: Analysis of Cross-Sectional Surveys on Children from 31 Countries. Nutrients 2021, 13, 1541. https://doi.org/10.3390/nu13051541
Amadu I, Seidu A-A, Duku E, Okyere J, Hagan JE Jr., Hormenu T, Ahinkorah BO. The Joint Effect of Maternal Marital Status and Type of Household Cooking Fuel on Child Nutritional Status in Sub-Saharan Africa: Analysis of Cross-Sectional Surveys on Children from 31 Countries. Nutrients. 2021; 13(5):1541. https://doi.org/10.3390/nu13051541
Chicago/Turabian StyleAmadu, Iddrisu, Abdul-Aziz Seidu, Eric Duku, Joshua Okyere, John Elvis Hagan, Jr., Thomas Hormenu, and Bright Opoku Ahinkorah. 2021. "The Joint Effect of Maternal Marital Status and Type of Household Cooking Fuel on Child Nutritional Status in Sub-Saharan Africa: Analysis of Cross-Sectional Surveys on Children from 31 Countries" Nutrients 13, no. 5: 1541. https://doi.org/10.3390/nu13051541