
High Frequency Protein-Rich Meal Service to Promote Protein Distribution to Stimulate Muscle Function in Preoperative Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Nutritional Intervention
2.3. Secondary Outcome
2.4. Statistical Analysis
3. Results
3.1. Demographics
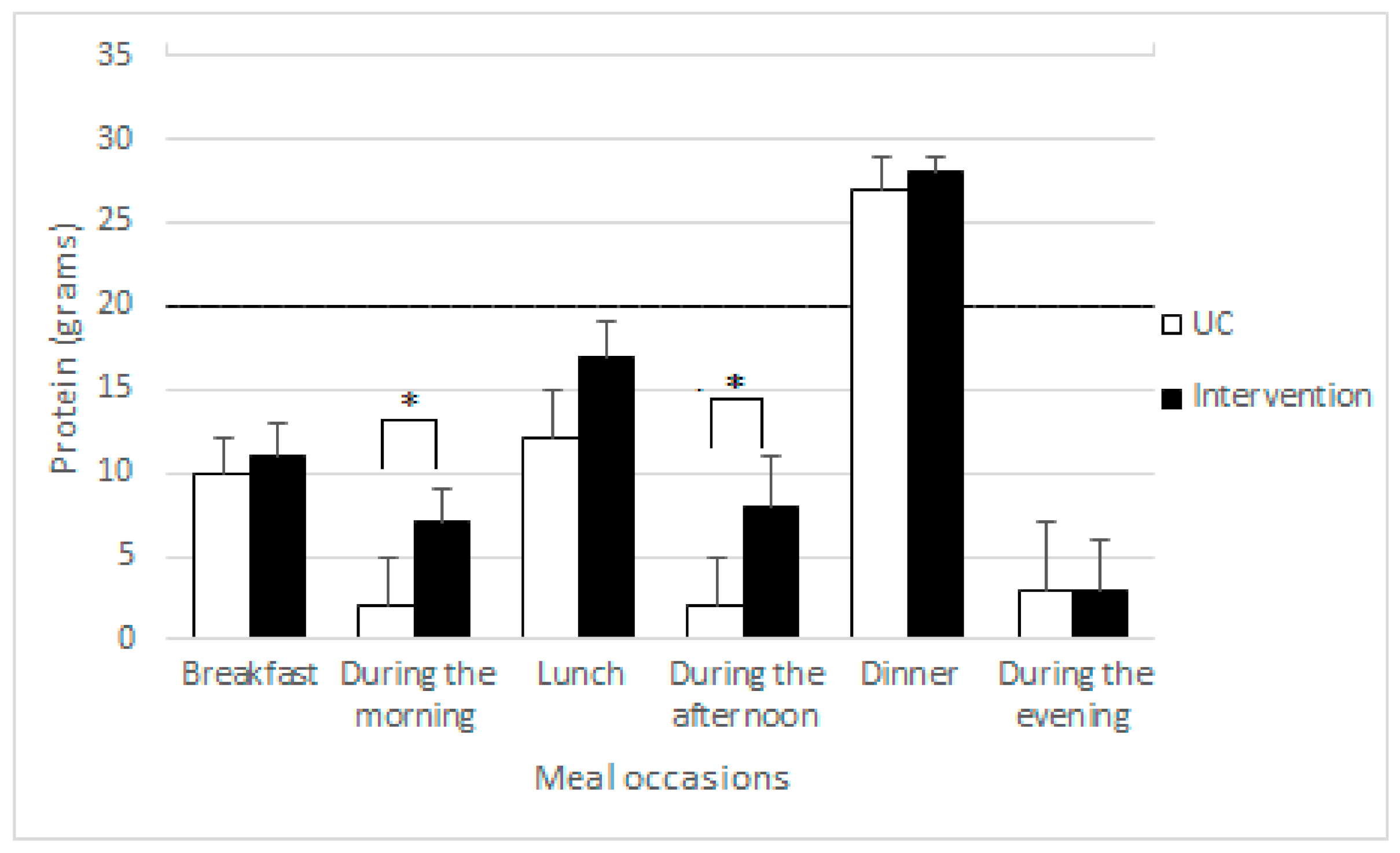
3.2. Dietary Intake
3.3. Handgrip Strength
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kouw, I.W.K.; Groen, B.B.L.; Smeets, J.S.J.; Kramer, I.F.; van Kranenburg, J.M.X.; Nilwik, R.; Geurts, J.A.P.; Ten Broeke, R.H.M.; Poeze, M.; van Loon, L.J.C.; et al. One Week of Hospitalization Following Elective Hip Surgery Induces Substantial Muscle Atrophy in Older Patients. J. Am. Med. Dir. Assoc. 2019, 20, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Sheffield-Moore, M.; Urban, R.J.; Sanford, A.P.; Aarsland, A.; Wolfe, R.R.; Ferrando, A.A. Essential amino acid and carbohydrate supplementation ameliorates muscle protein loss in humans during 28 days bedrest. J. Clin. Endocrinol. Metab. 2004, 89, 4351–4358. [Google Scholar] [CrossRef] [PubMed]
- Van Ancum, J.M.; Scheerman, K.; Jonkman, N.H.; Smeenk, H.E.; Kruizinga, R.C.; Meskers, C.G.M.; Maier, A.B. Change in muscle strength and muscle mass in older hospitalized patients: A systematic review and meta-analysis. Exp. Gerontol. 2017, 92, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Purcell, S.A.; Alish, C.; Pereira, S.L.; Deutz, N.E.; Heyland, D.K.; Goodpaster, B.H.; Tappenden, K.A.; Heymsfield, S.B. Implications of low muscle mass across the continuum of care: A narrative review. Ann. Med. 2018, 50, 675–693. [Google Scholar] [CrossRef] [Green Version]
- Galvan, E.; Arentson-Lantz, E.; Lamon, S.; Paddon-Jones, D. Protecting Skeletal Muscle with Protein and Amino Acid during Periods of Disuse. Nutrients 2016, 8, 404. [Google Scholar] [CrossRef] [Green Version]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Mamerow, M.M.; Mettler, J.A.; English, K.L.; Casperson, S.L.; Arentson-Lantz, E.; Sheffield-Moore, M.; Layman, D.K.; Paddon-Jones, D. Dietary protein distribution positively influences 24-h muscle protein synthesis in healthy adults. J. Nutr. 2014, 144, 876–880. [Google Scholar] [CrossRef] [Green Version]
- Murphy, C.H.; Oikawa, S.Y.; Phillips, S.M. Dietary Protein to Maintain Muscle Mass in Aging: A Case for Per-meal Protein Recommendations. J. Frailty Aging 2016, 5, 49–58. [Google Scholar] [CrossRef]
- Traylor, D.A.; Gorissen, S.H.M.; Phillips, S.M. Perspective: Protein Requirements and Optimal Intakes in Aging: Are We Ready to Recommend More Than the Recommended Daily Allowance? Adv. Nutr. 2018, 9, 171–182. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, R.R.; Miller, S.L.; Miller, K.B. Optimal protein intake in the elderly. Clin. Nutr. 2008, 27, 675–684. [Google Scholar] [CrossRef]
- Layman, D.K.; Anthony, T.G.; Rasmussen, B.B.; Adams, S.H.; Lynch, C.J.; Brinkworth, G.D.; Davis, T.A. Defining meal requirements for protein to optimize metabolic roles of amino acids. Am. J. Clin. Nutr. 2015, 101, 1330s–1338s. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Hudson, J.L.; Iii, R.E.B.; Campbell, W.W. Protein Distribution and Muscle-Related Outcomes: Does the Evidence Support the Concept? Nutrients 2020, 12, 1441. [Google Scholar] [CrossRef]
- Bauer, J.M.; Verlaan, S.; Bautmans, I.; Brandt, K.; Donini, L.M.; Maggio, M.; McMurdo, M.E.; Mets, T.; Seal, C.; Wijers, S.L.; et al. Effects of a vitamin D and leucine-enriched whey protein nutritional supplement on measures of sarcopenia in older adults, the PROVIDE study: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2015, 16, 740–747. [Google Scholar] [CrossRef]
- Tieland, M.; van de Rest, O.; Dirks, M.L.; van der Zwaluw, N.; Mensink, M.; van Loon, L.J.; de Groot, L.C. Protein supplementation improves physical performance in frail elderly people: A randomized, double-blind, placebo-controlled trial. J. Am. Med. Dir. Assoc. 2012, 13, 720–726. [Google Scholar] [CrossRef]
- Deutz, N.E.P.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Tieland, M.; Beelen, J.; Laan, A.C.M.; Poon, S.; de Groot, L.; Seeman, E.; Wang, X.; Iuliano, S. An Even Distribution of Protein Intake Daily Promotes Protein Adequacy but Does Not Influence Nutritional Status in Institutionalized Elderly. J. Am. Med. Dir. Assoc. 2018, 19, 33–39. [Google Scholar] [CrossRef]
- Dijxhoorn, D.N.; van den Berg, M.G.A.; Kievit, W.; Korzilius, J.; Drenth, J.P.H.; Wanten, G.J.A. A novel in-hospital meal service improves protein and energy intake. Clin. Nutr. 2018, 37, 2238–2245. [Google Scholar] [CrossRef]
- Dijxhoorn, D.N.; IJmker-Hemink, V.E.; Wanten, G.J.A.; van den Berg, M.G.A. Strategies to increase protein intake at mealtimes through a novel high-frequency food service in hospitalized patients. Eur. J. Clin. Nutr. 2019, 73, 910–916. [Google Scholar] [CrossRef]
- IJmker-Hemink, V.E.; Wanten, G.J.A.; de Nes, L.C.F.; van den Berg, M.G.A. Effect of a Preoperative Home-Delivered, Protein-Rich Meal Service to Improve Protein Intake in Surgical Patients: A Randomized Controlled Trial. JPEN J. Parenter. Enter. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Byers, T. Dietary assessment resource manual. J. Nutr. 1994, 124, 2245s–2317s. [Google Scholar] [CrossRef] [PubMed]
- Weijs, P.J.; Sauerwein, H.P.; Kondrup, J. Protein recommendations in the ICU: G protein/kg body weight—which body weight for underweight and obese patients? Clin. Nutr. 2012, 31, 774–775. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Stobaus, N.; Gonzalez, M.C.; Schulzke, J.D.; Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 2011, 30, 135–142. [Google Scholar] [CrossRef]
- Langius, J.V.W.; Kruizenga, H.; Reijven, N. Measuring Handgrip Strength; Nutiritonal Assessment Platform: Maastricht, The Netherlands, 2017. [Google Scholar]
- Bertenshaw, E.J.; Lluch, A.; Yeomans, M.R. Satiating effects of protein but not carbohydrate consumed in a between-meal beverage context. Physiol. Behav. 2008, 93, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Nieuwenhuizen, W.F.; Weenen, H.; Rigby, P.; Hetherington, M.M. Older adults and patients in need of nutritional support: Review of current treatment options and factors influencing nutritional intake. Clin. Nutr. 2010, 29, 160–169. [Google Scholar] [CrossRef]
- Westerterp-Plantenga, M.S. The significance of protein in food intake and body weight regulation. Curr. Opin. Clin. Nutr. Metab. Care 2003, 6, 635–638. [Google Scholar] [CrossRef] [Green Version]
- Abbott, R.A.; Whear, R.; Thompson-Coon, J.; Ukoumunne, O.C.; Rogers, M.; Bethel, A.; Hemsley, A.; Stein, K. Effectiveness of mealtime interventions on nutritional outcomes for the elderly living in residential care: A systematic review and meta-analysis. Ageing Res. Rev. 2013, 12, 967–981. [Google Scholar] [CrossRef]
- Beelen, J.; Vasse, E.; Janssen, N.; Janse, A.; de Roos, N.M.; de Groot, L. Protein-enriched familiar foods and drinks improve protein intake of hospitalized older patients: A randomized controlled trial. Clin. Nutr. 2018, 37, 1186–1192. [Google Scholar] [CrossRef]
- Frongillo, E.A.; Isaacman, T.D.; Horan, C.M.; Wethington, E.; Pillemer, K. Adequacy of and satisfaction with delivery and use of home-delivered meals. J. Nutr. Elder. 2010, 29, 211–226. [Google Scholar] [CrossRef]
- Keller, H.H. Meal programs improve nutritional risk: A longitudinal analysis of community-living seniors. J. Am. Diet Assoc. 2006, 106, 1042–1048. [Google Scholar] [CrossRef]
- Lee, K.; Raiz, L. The Home-Delivered Meals Program: A Promising Intervention for Suburban Older Adults Living Alone. Care Manag. J. 2015, 16, 195–202. [Google Scholar] [CrossRef]
- Roy, M.A.; Payette, H. Meals-on-wheels improves energy and nutrient intake in a frail free-living elderly population. J. Nutr. Health Aging 2006, 10, 554–560. [Google Scholar]
- ten Haaf, D.; van Dongen, E.; Nuijten, M.; Eijsvogels, T.; de Groot, L.; Hopman, M. Protein intake and distribution in relation to physical functioning and quality of life in community-dwelling elderly people: Acknowledging the role of physical activity. Nutrients 2018, 10, 506. [Google Scholar] [CrossRef] [Green Version]
- Farsijani, S.; Morais, J.A.; Payette, H.; Gaudreau, P.; Shatenstein, B.; Gray-Donald, K.; Chevalier, S. Relation between mealtime distribution of protein intake and lean mass loss in free-living older adults of the NuAge study. Am. J. Clin. Nutr. 2016, 104, 694–703. [Google Scholar] [CrossRef]
- Bollwein, J.; Diekmann, R.; Kaiser, M.J.; Bauer, J.M.; Uter, W.; Sieber, C.C.; Volkert, D. Distribution but not amount of protein intake is associated with frailty: A cross-sectional investigation in the region of Nurnberg. Nutr. J. 2013, 12, 109. [Google Scholar] [CrossRef] [Green Version]
- Tieland, M.; Borgonjen-Van den Berg, K.J.; van Loon, L.J.; de Groot, L.C. Dietary protein intake in community-dwelling, frail, and institutionalized elderly people: Scope for improvement. Eur. J. Nutr. 2012, 51, 173–179. [Google Scholar] [CrossRef]
- Iuliano, S.; Woods, J.; Robbins, J. Consuming two additional serves of dairy food a day significantly improves energy and nutrient intakes in ambulatory aged care residents: A feasibility study. J. Nutr. Health Aging 2013, 17, 509–513. [Google Scholar] [CrossRef]
- Groen, B.B.; Res, P.T.; Pennings, B.; Hertle, E.; Senden, J.M.; Saris, W.H.; van Loon, L.J. Intragastric protein administration stimulates overnight muscle protein synthesis in elderly men. Am. J. Physiol. Endocrinol. Metab. 2012, 302, E52–E60. [Google Scholar] [CrossRef]
- Kouw, I.W.; Holwerda, A.M.; Trommelen, J.; Kramer, I.F.; Bastiaanse, J.; Halson, S.L.; Wodzig, W.K.; Verdijk, L.B.; van Loon, L.J. Protein ingestion before sleep increases overnight muscle protein synthesis rates in healthy older men: A randomized controlled trial. J. Nutr. 2017, 147, 2252–2261. [Google Scholar] [CrossRef] [Green Version]
- Snijders, T.; Trommelen, J.; Kouw, I.W.K.; Holwerda, A.M.; Verdijk, L.B.; van Loon, L.J.C. The Impact of Pre-sleep Protein Ingestion on the Skeletal Muscle Adaptive Response to Exercise in Humans: An Update. Front. Nutr. 2019, 6, 17. [Google Scholar] [CrossRef] [Green Version]
- Trommelen, J.; Van Loon, L.J. Pre-sleep protein ingestion to improve the skeletal muscle adaptive response to exercise training. Nutrients 2016, 8, 763. [Google Scholar] [CrossRef] [Green Version]
- Farsijani, S.; Payette, H.; Morais, J.A.; Shatenstein, B.; Gaudreau, P.; Chevalier, S. Even mealtime distribution of protein intake is associated with greater muscle strength, but not with 3-y physical function decline, in free-living older adults: The Quebec longitudinal study on Nutrition as a Determinant of Successful Aging (NuAge study). Am. J. Clin. Nutr. 2017, 106, 113–124. [Google Scholar] [CrossRef]
- Jespersen, S.E.; Agergaard, J. Evenness of dietary protein distribution is associated with higher muscle mass but not muscle strength or protein turnover in healthy adults: A systematic review. Eur. J. Nutr. 2021. [Google Scholar] [CrossRef]
- Biolo, G.; Ciocchi, B.; Stulle, M.; Bosutti, A.; Barazzoni, R.; Zanetti, M.; Antonione, R.; Lebenstedt, M.; Platen, P.; Heer, M.; et al. Calorie restriction accelerates the catabolism of lean body mass during 2 wk of bed rest. Am. J. Clin. Nutr. 2007, 86, 366–372. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | UC Group 1 (n = 50) | Intervention Group (n = 52) | |
|---|---|---|---|
| Gender, n (%) | Male | 29 (58) | 22 (42) |
| Age, years, mean ± SD 1 | 62 ± 13 | 63 ± 12 | |
| BMIa, kg/m2, mean ± SD 1 | 27 ± 4 | 28 ± 6 | |
| MUST 1, n (%) | 0 | 41 (82) | 44 (85) |
| 1 | 7 (14) | 5 (10) | |
| ≥2 | 2 (4) | 3 (6) | |
| Protein intake relative to requirements (%), mean ± SD 1 | 80 ± 25 | 77 ± 21 | |
| Energy intake relative to requirements (%), mean ± SD 1 | 85 ± 24 | 83 ± 23 | |
| Oncological disease, n (%) | 12 (24) | 12 (23) | |
| Department, n (%) | General Surgery | 15 (30) | 16 (31) |
| Orthopedics | 11 (22) | 11 (21) | |
| Urology & Gynecology | 24 (48) | 25 (48) | |
| Handgrip strength, mean ± SD 1 | 35 ± 16 | 32 ± 12 | |
| <2 Meal Occasions Threshold of 20 g 1 | ≥2 Meal Occasions Threshold of 20 g 1 | p-Value | |
|---|---|---|---|
| Handgrip strength (kg) | 31 ± 12 | 44 ± 15 | 0.026 |
| Protein intake relative to requirements (%) | 80 ± 20 | 96 ± 35 | 0.001 |
| Energy intake relative to requirements (%) | 93 ± 24 | 104 ± 26 | 0.044 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
IJmker-Hemink, V.; Moolhuijzen, N.; Wanten, G.; van den Berg, M. High Frequency Protein-Rich Meal Service to Promote Protein Distribution to Stimulate Muscle Function in Preoperative Patients. Nutrients 2021, 13, 1232. https://doi.org/10.3390/nu13041232
IJmker-Hemink V, Moolhuijzen N, Wanten G, van den Berg M. High Frequency Protein-Rich Meal Service to Promote Protein Distribution to Stimulate Muscle Function in Preoperative Patients. Nutrients. 2021; 13(4):1232. https://doi.org/10.3390/nu13041232
Chicago/Turabian StyleIJmker-Hemink, Vera, Nicky Moolhuijzen, Geert Wanten, and Manon van den Berg. 2021. "High Frequency Protein-Rich Meal Service to Promote Protein Distribution to Stimulate Muscle Function in Preoperative Patients" Nutrients 13, no. 4: 1232. https://doi.org/10.3390/nu13041232