
Efficacy and Safety of Armolipid Plus®: An Updated PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Synthesis
2.6. Publication Biases
3. Results
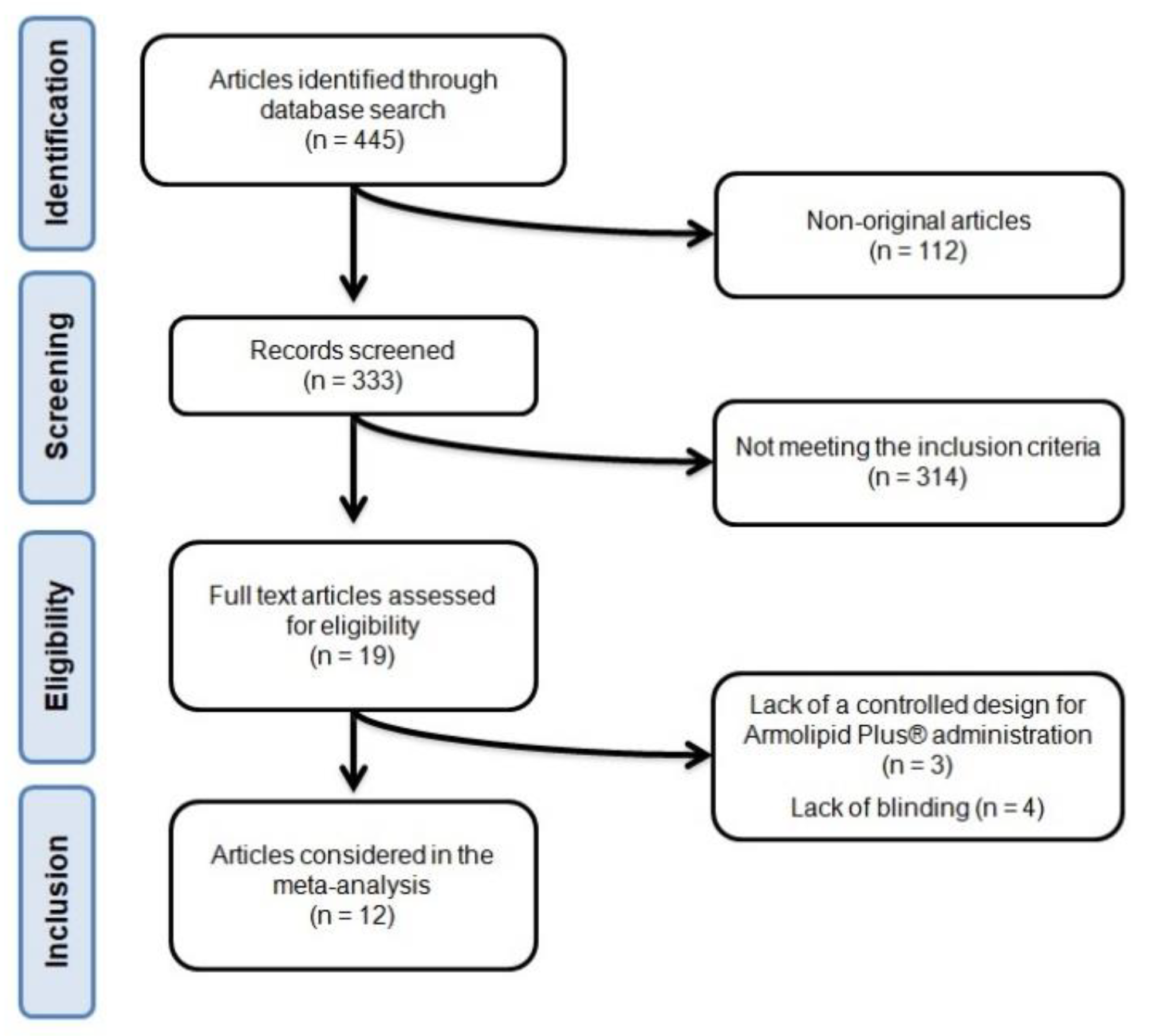
3.1. Flow and Characteristics of the Included Studies
3.2. Risk of Bias Assessment
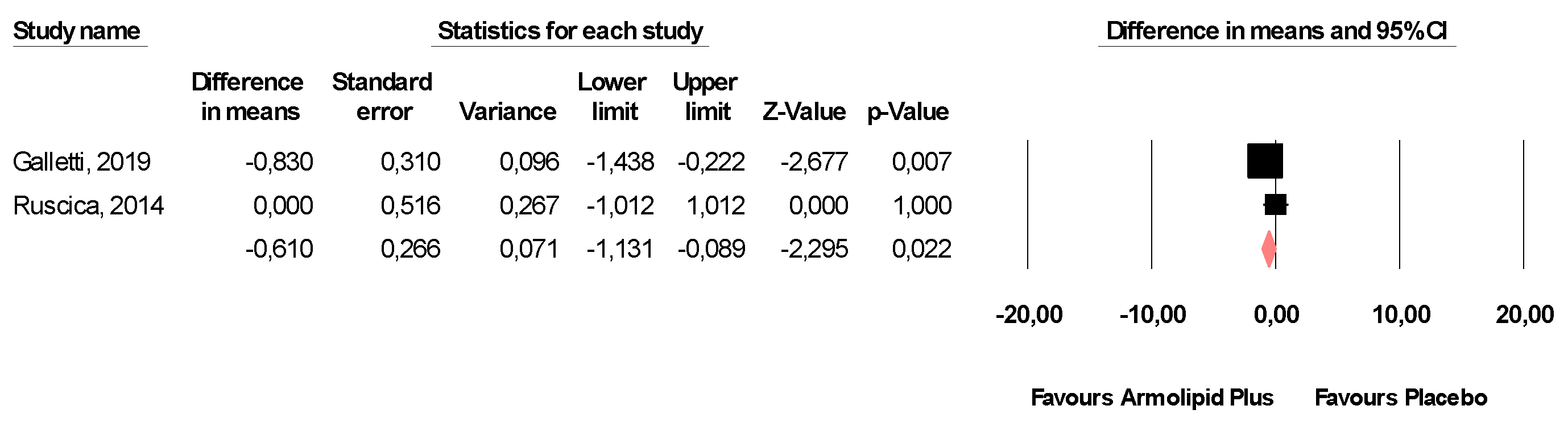
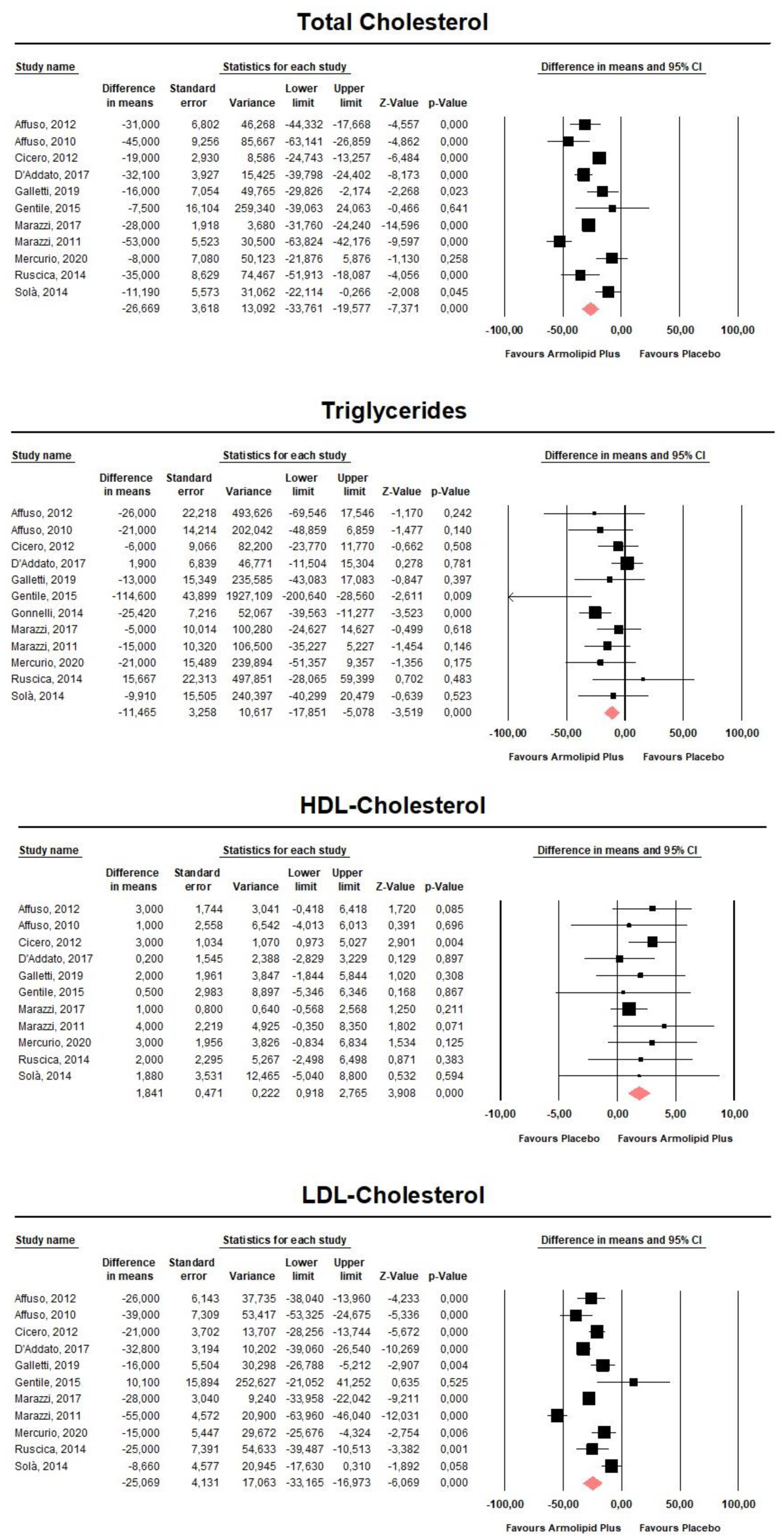
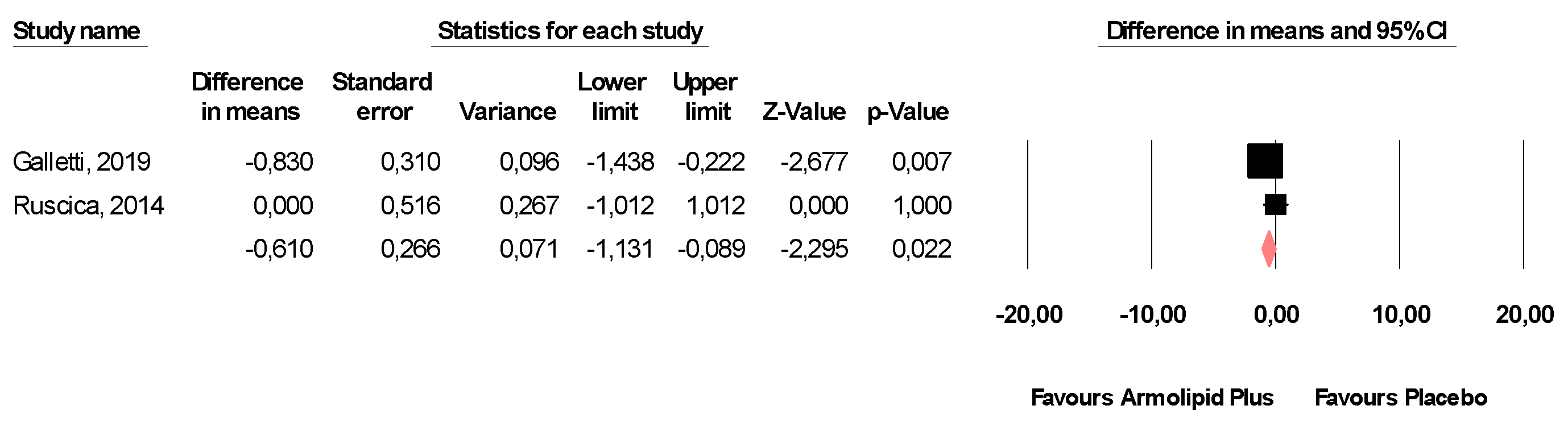
3.3. Effect of Armolipid Plus® on Anthropometric Measures, Blood Pressure, Serum Lipids, and Other Metabolic Parameters
3.4. Safety Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Cardiovascular Diseases. Available online: http://www.who.int/mediacentre/factsheets/fs317/en/ (accessed on 26 December 2020).
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Colantonio, L.D.; Bittner, V.; Reynolds, K.; Levitan, E.B.; Rosenson, R.S.; Banach, M.; Kent, S.T.; Derose, S.F.; Zhou, H.; Safford, M.M.; et al. Association of Serum Lipids and Coronary Heart Disease in Contemporary Observational Studies. Circulation 2016, 133, 256–264. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics—2016 Update: A Report from the American Heart Association. American Heart Association Statistics Committee, Stroke Statistics Subcommittee. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC); Taddei, C.; Jackson, R.; Zhou, B.; Bixby, H.; Danaei, G.; Di Cesare, M.; Kuulasmaa, K.; Hajifathalian, K.; Bentham, J.; et al. National trends in total cholesterol obscure heterogeneous changes in HDL and non-HDL cholesterol and total-to-HDL cholesterol ratio: A pooled analysis of 458 population-based studies in Asian and Western countries. Int. J. Epidemiol. 2019, 49, 173–192. [Google Scholar] [CrossRef]
- Wilson, P.W.F.; Polonsky, T.S.; Miedema, M.D.; Khera, A.; Kosinski, A.S.; Kuvin, J.T. Systematic Review for the 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1144–e1161. [Google Scholar] [CrossRef]
- Zeitouni, M.; Sabouret, P.; Kerneis, M.; Silvain, J.; Collet, J.-P.; Bruckert, E.; Montalescot, G. 2019 ESC/EAS Guidelines for management of dyslipidaemia: Strengths and limitations. Eur. Hear. J. Cardiovasc. Pharmacother. 2020, 77. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Atherosclerosis 2016, 252, 207–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Poli, A.; Barbagallo, C.M.; Cicero, A.F.; Corsini, A.; Manzato, E.; Trimarco, B.; Bernini, F.; Visioli, F.; Bianchi, A.; Canzone, G.; et al. Nutraceuticals and functional foods for the control of plasma cholesterol levels. An intersociety position paper. Pharmacol. Res. 2018, 134, 51–60. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Colletti, A.; Bajraktari, G.; Descamps, O.; Djuric, D.M.; Ezhov, M.; Fras, Z.; Katsiki, N.; Langlois, M.; Latkovskis, G.; et al. Lipid-lowering nutraceuticals in clinical practice: Position paper from an International Lipid Expert Panel. Nutr. Rev. 2017, 75, 731–767. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.M.; Toth, P.P.; Giglio, R.V.; Banach, M.; Noto, M.; Nikolic, D.; Montalto, G.; Rizzo, M. Nutraceuticals as an Important Part of Combination Therapy in Dyslipidaemia. Curr. Pharm. Des. 2017, 23, 2496–2503. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Colletti, A. Food and plant bioactives for reducing cardiometabolic disease risk: An evidence based approach. Food Funct. 2017, 8, 2076–2088. [Google Scholar] [CrossRef] [PubMed]
- Barrios, V.; Escobar, C.; Cicero, A.F.G.; Burke, D.; Fasching, P.; Banach, M.; Bruckert, E. A nutraceutical approach (Armolipid Plus) to reduce total and LDL cholesterol in individuals with mild to moderate dyslipidemia: Review of the clinical evidence. Atheroscler. Suppl. 2017, 24, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. For the PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Report Version 5.0.2.2009; John Wiley and Sons Ltd.: Chichester, UK, 2010. [Google Scholar]
- Fogacci, F.; Ferri, N.; Toth, P.P.; Ruscica, M.; Corsini, A.; Cicero, A.F.G. Efficacy and Safety of Mipomersen: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Drugs 2019, 79, 751–766. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Version 3; Biostat: Englewood, NJ, USA, 2005; Volume 104. [Google Scholar]
- Follmann, D.; Elliott, P.; Suh, I.; Cutler, J. Variance imputation for overviews of clinical trials with continuous response. J. Clin. Epidemiol. 1992, 45, 769–773. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res. Methodol. 2014, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Melsen, W.G.; Bootsma, M.C.J.; Rovers, M.M.; Bonten, M.J.M. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Haenszel, W.; Hon, N.B. Statistical approaches to the study of cancer with particular reference to case registers. J. Chronic Dis. 1956, 4, 589–599. [Google Scholar] [CrossRef]
- Fogacci, F.; Banach, M.; Cicero, A.F.G. Resveratrol effect on patients with non-alcoholic fatty liver disease: A matter of dose and treatment length. Diabetes Obes. Metab. 2018, 20, 1798–1799. [Google Scholar] [CrossRef]
- Fogacci, F.; Rizzo, M.; Krogager, C.; Kennedy, C.; Georges, C.M.; Knežević, T.; Liberopoulos, E.; Vallée, A.; Pérez-Martínez, P.; Wenstedt, E.F.; et al. Safety Evaluation of α-Lipoic Acid Supplementation: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Clinical Studies. Antioxidants 2020, 9, 1011. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Affuso, F. A nutraceutical combination improves insulin sensitivity in patients with metabolic syndrome. World J. Cardiol. 2012, 4, 77–83. [Google Scholar] [CrossRef]
- Affuso, F.; Ruvolo, A.; Micillo, F.; Saccà, L.; Fazio, S. Effects of a nutraceutical combination (berberine, red yeast rice and policosanols) on lipid levels and endothelial function randomized, double-blind, placebo-controlled study. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 656–661. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; De Sando, V.; Benedetto, D.; Cevenini, M.; Grandi, E.; Borghi, C. Long-term efficacy and tolerability of a multicomponent lipid-lowering nutraceutical in overweight and normoweight patients. Nutrafoods 2012, 11, 55–61. [Google Scholar] [CrossRef]
- D’Addato, S.; Scandiani, L.; Mombelli, G.; Focanti, F.; Pelacchi, F.; Salvatori, E.; Di Loreto, G.; Comandini, A.; Maffioli, P.; DeRosa, G. Effect of a food supplement containing berberine, monacolin K, hydroxytyrosol and coenzyme Q10 on lipid levels: A randomized, double-blind, placebo controlled study. Drug Des. Dev. Ther. 2017, 11, 1585–1592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galletti, F.; Fazio, V.; Gentile, M.; Schillaci, G.; Pucci, G.; Battista, F.; Mercurio, V.; Bosso, G.; Bonaduce, D.; Brambilla, N.; et al. Efficacy of a nutraceutical combination on lipid metabolism in patients with metabolic syndrome: A multicenter, double blind, randomized, placebo controlled trial. Lipids Heal. Dis. 2019, 18, 66. [Google Scholar] [CrossRef] [Green Version]
- Gentile, M.; Calcaterra, I.; Strazzullo, A.; Pagano, C.; Pacioni, D.; Speranza, E.; Rubba, P.; Marotta, G. Effects of Armolipid Plus on small dense LDL particles in a sample of patients affected by familial combined hyperlipidemia. Clin. Lipidol. 2015, 10, 475–480. [Google Scholar] [CrossRef] [Green Version]
- Gonnelli, S.; Caffarelli, C.; Stolakis, K.; Cuda, C.; Giordano, N.; Nuti, R. Efficacy and Tolerability of a Nutraceutical Combination (Red Yeast Rice, Policosanols, and Berberine) in Patients with Low-Moderate Risk Hypercholesterolemia: A Double-Blind, Placebo-Controlled Study. Curr. Ther. Res. 2015, 77, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marazzi, G.; Campolongo, G.; Pelliccia, F.; Quattrino, S.; Vitale, C.; Cacciotti, L.; Massaro, R.; Volterrani, M.; Rosano, G. Comparison of Low-Dose Statin Versus Low-Dose Statin + Armolipid Plus in High-Intensity Statin-Intolerant Patients with a Previous Coronary Event and Percutaneous Coronary Intervention (ADHERENCE Trial). Am. J. Cardiol. 2017, 120, 893–897. [Google Scholar] [CrossRef]
- Marazzi, G.; Cacciotti, L.; Pelliccia, F.; Iaia, L.; Volterrani, M.; Caminiti, G.; Sposato, B.; Massaro, R.; Grieco, F.; Rosano, G. Long-term effects of nutraceuticals (berberine, red yeast rice, policosanol) in elderly hypercholesterolemic patients. Adv. Ther. 2011, 28, 1105–1113. [Google Scholar] [CrossRef]
- Mercurio, V.; Pucci, G.; Bosso, G.; Fazio, V.; Battista, F.; Iannuzzi, A.; Brambilla, N.; Vitalini, C.; D’Amato, M.; Giacovelli, G.; et al. A nutraceutical combination reduces left ventricular mass in subjects with metabolic syndrome and left ventricular hypertrophy: A multicenter, randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2020, 39, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Ruscica, M.; Gomaraschi, M.; Mombelli, G.; Macchi, C.; Bosisio, R.; Pazzucconi, F.; Pavanello, C.; Calabresi, L.; Arnoldi, A.; Sirtori, C.R.; et al. Nutraceutical approach to moderate cardiometabolic risk: Results of a randomized, double-blind and crossover study with Armolipid Plus. J. Clin. Lipidol. 2014, 8, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Sola, R.; Valls, R.-M.; Puzo, J.; Calabuig, J.-R.; Brea, A.; Pedret, A.; Moriña, D.; Villar, J.; Millán, J.; Anguera, A. Effects of Poly-Bioactive Compounds on Lipid Profile and Body Weight in a Moderately Hypercholesterolemic Population with Low Cardiovascular Disease Risk: A Multicenter Randomized Trial. PLoS ONE 2014, 9, e101978. [Google Scholar] [CrossRef] [Green Version]
- Pirro, M.; Mannarino, M.R.; Bianconi, V.; Simental-Mendía, L.E.; Bagaglia, F.; Mannarino, E.; Sahebkar, A. The effects of a nutraceutical combination on plasma lipids and glucose: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2016, 110, 76–88. [Google Scholar] [CrossRef]
- Millán, J.; Cicero, A.F.; Torres, F.; Anguera, A. Effects of a nutraceutical combination containing berberine (BRB), policosanol, and red yeast rice (RYR), on lipid profile in hypercholesterolemic patients: A meta-analysis of randomised controlled trials. Clín. Investig. Arterioscler. 2016, 28, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Pirro, M.; Lupattelli, G.; Del Giorno, R.; Schillaci, G.; Berisha, S.; Mannarino, M.R.; Bagaglia, F.; Melis, F.; Mannarino, E. Nutraceutical combination (red yeast rice, berberine and policosanols) improves aortic stiffness in low-moderate risk hypercholesterolemic patients. PharmaNutrition 2013, 1, 73–77. [Google Scholar] [CrossRef]
- Izzo, R.; De Simone, G.; Giudice, R.; Chinali, M.; Trimarco, V.; De Luca, N.; Trimarco, B. Effects of nutraceuticals on prevalence of metabolic syndrome and on calculated Framingham Risk Score in individuals with dyslipidemia. J. Hypertens. 2010, 28, 1482–1487. [Google Scholar] [CrossRef] [PubMed]
- Trimarco, B.; Benvenuti, C.; Rozza, F.; Cimmino, C.S.; Giudice, R.; Crispo, S. Clinical evidence of efficacy of red yeast rice and berberine in a large controlled study versus diet. Med. J. Nutrition. Metab. 2011, 4, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Rovati, L.C.; Setnikar, I. Eulipidemic effects of berberine administered alone or in combination with other natural cholesterol-lowering agents: A single-blind clinical investigation. Arzneimittelforschung 2007, 57, 26–30. [Google Scholar] [CrossRef]
- Pisciotta, L.; Bellocchio, A.; Bertolini, S. Nutraceutical pill containing berberine versus ezetimibe on plasma lipid pattern in hypercholesterolemic subjects and its additive effect in patients with familial hypercholesterolemia on stable cholesterol-lowering treatment. Lipids Heal. Dis. 2012, 11, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banach, M.; Patti, A.M.; Giglio, R.V.; Cicero, A.F.; Atanasov, A.G.; Bajraktari, G.; Bruckert, E.; Descamps, O.; Djuric, D.M.; Ezhov, M.; et al. The Role of Nutraceuticals in Statin Intolerant Patients. J. Am. Coll. Cardiol. 2018, 72, 96–118. [Google Scholar] [CrossRef]
- Fogacci, F.; Banach, M.; Mikhailidis, D.P.; Bruckert, E.; Toth, P.P.; Watts, G.F.; Reiner, Ž.; Mancini, J.; Rizzo, M.; Mitchenko, O.; et al. Safety of red yeast rice supplementation: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2019, 143, 1–16. [Google Scholar] [CrossRef]
- Marazzi, G.; Campolongo, G.; Pelliccia, F.; Calabrò, P.; Cacciotti, L.; Vitale, C.; Massaro, R.; Volterrani, M.; Rosano, G. Usefulness of Low-Dose Statin Plus Ezetimibe and/or Nutraceuticals in Patients with Coronary Artery Disease Intolerant to High-Dose Statin Treatment. Am. J. Cardiol. 2019, 123, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [Green Version]
- Gerards, M.C.; Terlou, R.J.; Yu, H.; Koks, C.; Gerdes, V. Traditional Chinese lipid-lowering agent red yeast rice results in significant LDL reduction but safety is uncertain—A systematic review and meta-analysis. Atherosclerosis 2015, 240, 415–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, S.P.; Liu, L.; Cheng, Y.C.; Shishehbor, M.H.; Liu, M.H.; Peng, D.Q.; Li, Y.L. Xuezhikang, an Extract of Cholestin, Protects Endothelial Function Through Antiinflammatory and Lipid-Lowering Mechanisms in Patients with Coronary Heart Disease. Circulation 2004, 110, 915–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, A.F.G.; Fogacci, F.; Banach, M. Red Yeast Rice for Hypercholesterolemia. Methodist Debakey Cardiovasc. J. 2019, 15, 192–199. [Google Scholar] [PubMed]
- Cicero, A.F.; DeRosa, G.; Borghi, C. Red Yeast Rice and Statin-Intolerant Patients. Am. J. Cardiol. 2010, 105, 1504. [Google Scholar] [CrossRef]
- Cicero, A.F.; Fogacci, F.; Zambon, A. Red Yeast Rice for Hypercholesterolemia. J. Am. Coll. Cardiol. 2021, 77, 620–628. [Google Scholar] [CrossRef]
- Varady, K.A.; Wang, Y.; Jones, P.J. Role of policosanols in the prevention and treatment of cardiovascular disease. Nutr. Rev. 2003, 61, 376–383. [Google Scholar] [CrossRef]
- Guardamagna, O.; Abelló, F.; Baracco, V.; Stasiowska, B.; Martino, F. The treatment of hypercholesterolemic children: Efficacy and safety of a combination of red yeast rice extract and policosanols. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 424–429. [Google Scholar] [CrossRef]
- Liang, Y.; Xu, X.; Yin, M.; Zhang, Y.; Huang, L.; Chen, R.; Ni, J. Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: A systematic literature review and a meta-analysis. Endocr. J. 2019, 66, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Pirro, M.; Francisci, D.; Bianconi, V.; Schiaroli, E.; Mannarino, M.R.; Barsotti, F.; Spinozzi, A.; Bagaglia, F.; Sahebkar, A.; Baldelli, F. NUtraceutical TReatment for hYpercholesterolemia in HIV-infected patients: The NU-TRY(HIV) randomized cross-over trial. Atherosclerosis 2019, 280, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Keech, A.C.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design | Follow-Up | Main Inclusion Criteria | Study Group | Participants (n) | Background Lipid-Lowering Treatment (Percentage of Subjects) | Male (n (%)) | Age (years; mean ± SD) | BMI (Kg/m2; mean ± SD) | Waist Circumference (cm; mean ± SD) | SBP (mmHg; mean ± SD) | DBP (mmHg; mean ± SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Affuso, 2012 [26] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 18 weeks | Metabolic syndrome 18–65 years of age | Armolipid Plus® | 29 | Statins (28%) | 20 (69) | 53 ± 7 | 32.2 ± 4.6 | 110 ± 9 | 125 ± 13 | 78 ± 8 |
| Placebo | 30 | Statins (27%) | 18 (60) | 50 ± 11.9 | 34.7 ± 5.1 | 115 ± 13 | 125 ± 14 | 81 ± 8 | ||||
| Affuso, 2010 [27] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 6 weeks | 18–70 years of age TC > 220 mg/dL LDL-C > 130 mg/dL | Armolipid Plus® | 25 | None | 13 (52) | 55 ± 8 | 28 ± 3.8 | NA | 125 ± 13 | 78 ± 8 |
| Placebo | 25 | None | 13 (52) | 55 ± 7 | 28 ± 3.3 | NA | 125 ± 14 | 81 ± 8 | ||||
| Cicero, 2012 [28] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 12 months | Primary prevention for CVD overweight | Armolipid Plus® | 71 | None | NA | NA | 26.95 ± 0.86 | NA | 134.4 ± 6.2 | 86.3 ± 6.1 |
| Placebo | 64 | None | NA | 24.17 ± 0.99 | NA | 133.2 ± 5.3 | 84.1 ± 6.8 | |||||
| D’Addato, 2017 [29] | Multicenter, randomized, double-blind, placebo-controlled, parallel-group clinical study | 4 weeks | Primary prevention for CVD 18–75 years of age TC ≥ 200 mg/dL and ≤260 mg/dL LDL-C ≥ 115 mg/dL and ≤180 mg/dL | Armolipid Plus® | 51 | None | 17 (33) | 53.7 ± 11.6 | 24 ± 4 | NA | NA | NA |
| Placebo | 51 | None | 17 (33) | 49.7 ± 12.3 | 24.9 ± 4.6 | NA | NA | NA | ||||
| Galletti, 2019 [30] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 24 weeks | Metabolic syndrome Left ventricular mass >48 g/m2,7 for men and >44 g/m2,7 for women 18–70 years of age | Armolipid Plus® | 71 | Statins (62%) | 42 (59) | 55.6 ± 8.9 | 29.4 ± 3.6 | 100.8 ± 9.3 | 130.6 ± 10.5 | 80.7 ± 8.1 |
| Placebo | 70 | Statins (63%) | 37 (53) | 55.6 ± 9.3 | 29.2 ± 3.5 | 100.3 ± 8.7 | 131.4 ± 10.6 | 81.6 ± 8 | ||||
| Gentile, 2015 [31] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 8 weeks | Familial combined hyperlipidemia | Armolipid Plus® | 15 | None | (77) | 44.1 ± 13 | 26 ± 2.8 | 92 ± 10.2 | 123 ± 12.3 | 77.9 ± 8.3 |
| Placebo | 15 | None | 26.7 ± 2.8 | 97.3 ± 8.5 | 122.5 ± 9.2 | 78.1 ± 6.9 | ||||||
| Gonnelli, 2014 [32] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 24 weeks | Estimated 10-year CV risk <20% according to Framingham risk scoring 18–60 years of age BMI ≥ 19 Kg/m2 and <30 Kg/m2 LDL-C > 150 mg/dL | Armolipid Plus® | 30 | None | 15 (50) | 46.4 ± 9.7 | 26.9 ± 4.9 | 89.9 ± 10.9 | 120.1 ± 11.1 | 77.2 ± 7 |
| Placebo | 30 | None | 14 (47) | 46.4 ± 10.1 | 26.4 ± 4.1 | 88.7 ± 10.9 | 119.1 ± 19.7 | 75.2 ± 10 | ||||
| Marazzi, 2017 [33] | Randomized, single-blind, parallel-group clinical study | 3 months | Documented CAD treated with PCI in the previous 12 months high-dose statin intolerance LDL-C > 100 mg/dL <50% reduction in LDL-C with low-dose statin treatment | Armolipid Plus® + low-dose statin | 50 | Statins (100%) Atorvastatin 5 mg (8%) Atorvastatin 10 mg (36%) Simvastatin 10 mg (14%) Simvastatin 20 mg (32%) Rosuvastatin 5 mg (10%) | 26 (52) | 69 ± 10 | NA | NA | NA | NA |
| Low-dose statin | 50 | Statins (100%) Atorvastatin 5 mg (8%) Atorvastatin 10 mg (34%) Simvastatin 10 mg (18%) Simvastatin 20 mg (32%) Rosuvastatin 5 mg (8%) | 28 (56) | 67 ± 12 | NA | NA | NA | NA | ||||
| Marazzi, 2011 [34] | Randomized, single-blind, placebo-controlled, parallel-group clinical study | 12 months | >75 years of age TC> 200 mg/dL LDL-C > 160 mg/dL statin intolerance and refusal of other treatments for hypercholesterolemia | Armolipid Plus® | 40 | None | 21 (53) | 82.5 ± 4.4 | NA | NA | NA | NA |
| Placebo | 40 | None | 20 (50) | 82.5 ± 4.9 | NA | NA | NA | NA | ||||
| Mercurio, 2020 [35] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 24 weeks | Metabolic syndrome echocardiographic evidence of left ventricular hypertrophy 18–70 years of age stable anti-hypertensive and lipid-lowering therapy over the past three months | Armolipid Plus® | 79 | Statins (55%) | 43 (58) | 55.6 ± 9 | 29.1 ± 3 | NA | 131 ± 11 | 81 ± 9 |
| Placebo | 79 | Statins (58%) | 38 (54) | 55.6 ± 9 | 29.3 ± 3 | NA | 131 ± 11 | 82 ± 8 | ||||
| Ruscica, 2014 [36] | Randomized, double-blind, placebo-controlled, cross-over clinical study | 8 weeks | Primary prevention for CVD metabolic syndrome >18 years of age LDL-C ≥ 130 mg/dL and ≤170 mg/dL | Armolipid Plus® | 30 | None | 23 (77) | 55.4 ± 9.7 | 26.8 ± 2.4 | 96.3 ± 7.9 for men; 91.7 ± 5.1 for women | 123 ± 12.3 | 80.7 ± 5.7 |
| Placebo | ||||||||||||
| Solà, 2014 [37] | Randomized, double-blind, placebo-controlled, parallel-group clinical study | 12 weeks | Primary prevention for CVD ≥18 years of age LDL-C ≥ 130 mg/dL and <190 mg/dL | Armolipid Plus® | 51 | None | 18 (35) | 49.9 ± 11.6 | 25.4 ± 4.1 | 86.2 ± 11.8 | 122.2 ± 18.1 | 76.5 ± 12.2 |
| Placebo | 51 | None | 14 (28) | 52.4 ± 11.2 | 28 ± 8.7 | 90.4 ± 11.6 | 123.8 ± 17.6 | 76.8 ± 11.2 |
| Author, Year | Study Group | TC (mg/dL; mean ± SD) | TG (mg/dL; mean ± SD) | HDL-C (mg/dL; mean ± SD) | LDL-C (mg/dL; mean ± SD) | FPG (mg/dL; mean ± SD) | FPI (mU/L; mean ± SD) | HOMA-IR (mean ± SD) | hs-CRP (mg/L; mean ± SD) |
|---|---|---|---|---|---|---|---|---|---|
| Affuso, 2012 [26] | Armolipid Plus® | 209 ± 39 | 156 ± 76 | 42 ± 10 | 135 ± 7 | 103 ± 22 | 9 ± 4.2 | 3.2 ± 1.5 | NA |
| Placebo | 197 ± 40 | 170 ± 74 | 46 ± 14 | 118 ± 39 | 85 ± 12 | 9 ± 6.9 | 2.7 ± 2.2 | NA | |
| Affuso, 2010 [27] | Armolipid Plus® | 255 ± 29 | 57 ± 32 | 58 ± 18 | 176 ± 25 | 84 ± 12 | NA | NA | NA |
| Placebo | 252 ± 31 | 65 ± 28 | 53 ± 14 | 171 ± 22 | 87 ± 12 | NA | NA | NA | |
| Cicero, 2012 [28] | Armolipid Plus® | 218.3 ± 14.4 | 225.2 ± 42.7 | 38.6 ± 4.5 | 134.6 ± 15.2 | 109.6 ± 12 | 11.49 ± 4.34 | 3.2 ± 1.4 | 2.05 ± 0.31 |
| Placebo | 213.5 ± 17 | 192.8 ± 44.4 | 39 ± 4.3 | 136 ± 18.9 | 92.2 ± 10.3 | 7.47 ± 3.14 | 1.7 ± 0.8 | 1.85 ± 0.43 | |
| D’Addato, 2017 [29] | Armolipid Plus® | 234.6 ± 18 | 110.8 ± 41.5 | 65.1 ± 13.3 | 147.5 ± 16.3 | NA | NA | NA | NA |
| Placebo | 235.6 ± 17.9 | 110.5 ± 41.9 | 70 ± 16.2 | 143.6 ± 15 | NA | NA | NA | NA | |
| Galletti, 2019 [30] | Armolipid Plus® | 224.3 ± 44.7 | 151.3 ± 82.5 | 50.7 ± 11.9 | 132.9 ± 36.5 | 103.9 ± 14.5 | 15.7 ± 11.6 | 4.1 ± 3.2 | 1.85 ± 2.34 |
| Placebo | 218.4 ± 38.2 | 159.6 ± 86.6 | 50.4 ± 12.1 | 128.4 ± 28.6 | 105.7 ± 17.9 | 16.3 ± 9 | 4.2 ± 2.4 | 1.35 ± 1.01 | |
| Gentile, 2015 [31] | Armolipid Plus® | 228.8 ± 41.1 | 290.3 ± 104.3 | 40.8 ± 6.6 | 134.7 ± 46.5 | 91.5 ± 17.5 | NA | NA | NA |
| Placebo | 241.9 ± 42.1 | 204.2 ± 80.9 | 38.2 ± 9.1 | 162.8 ± 41.2 | 93 ± 5.9 | NA | NA | NA | |
| Gonnelli, 2014 [32] | Armolipid Plus® | 238.4 ± 26.9 | 132.1 ± 55.2 | 53.1 ± 13.2 | 162 ± 22.5 | 92.5 ± 8.8 | NA | NA | NA |
| Placebo | 248.1 ± 32.4 | 119 ± 50.4 | 55.7 ± 14.5 | 165.8 ± 29 | 94.4 ± 10 | NA | NA | NA | |
| Marazzi, 2017 [33] | Armolipid Plus® | 198 ± 9 | 177 ± 51 | 35 ± 4 | 127 ± 15 | NA | NA | NA | NA |
| Placebo | 199 ± 11 | 176 ± 51 | 35 ± 4 | 129 ± 17 | NA | NA | NA | NA | |
| Marazzi, 2011 [34] | Armolipid Plus® | 252 ± 23 | 179 ± 48 | 44 ± 12 | 172 ± 16 | 94 ± 6 | 7.2 ± 2.4 | 1.7 ± 0.6 | NA |
| Placebo | 253 ± 19 | 179 ± 50 | 44 ± 8 | 173 ± 10 | 91 ± 7 | 6.5 ± 2.4 | 1.5 ± 0.6 | NA | |
| Mercurio, 2020 [35] | Armolipid Plus® | 227 ± 44 | 160 ± 88 | 49 ± 11 | 138 ± 34 | 105 ± 16 | NA | 4.2 ± 3 | NA |
| Placebo | 218 ± 40 | 151 ± 83 | 53 ± 13 | 124 ± 30 | 104 ± 16 | NA | 4 ± 3 | NA | |
| Ruscica, 2014 [36] | Armolipid Plus® | 240 ± 31 | 216 (171, 284)* | 40 ± 9 | 151 ± 24 | 88 ± 16 | 6 ± 4 | 1.3 ± 0.9 | 2 ± 1 |
| Placebo | 240 ± 39 | 230 (173, 307)* | 41 ± 7 | 150 ± 29 | 86 ± 18 | 6.4 ± 4.4 | 1.3 ± 1 | 2 ± 3 | |
| Solà, 2014 [37] | Armolipid Plus® | 243.6 ± 24.4 | 107.2 ± 61.3 | 66.5 ± 21.2 | 155.7 ± 14.6 | 90.6 ± 9.3 | 8.2 ± 9.2 | 1.8 ± 2.6 | NA |
| Placebo | 243.4 ± 19.5 | 115 ± 56 | 61.1 ± 14.1 | 159.3 ± 15.7 | 92.8 ± 10.3 | 7.5 ± 5.4 | 1.7 ± 1.3 | NA |
| First Author, Year | Sequence Generation | Allocation Concealment | Blinding of Participants, Personnel, and Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | Other Potential Threats to Validity |
|---|---|---|---|---|---|---|
| Affuso, 2012 [26] | L | L | L | L | L | U |
| Affuso, 2010 [27] | L | L | L | L | L | U |
| Cicero, 2012 [28] | L | L | L | L | L | L |
| D’Addato, 2017 [29] | L | L | L | L | L | L |
| Galletti, 2019 [30] | L | L | L | L | L | L |
| Gentile, 2015 [31] | L | L | L | L | L | U |
| Gonnelli, 2014 [32] | L | L | L | L | L | U |
| Marazzi, 2017 [33] | L | L | L | L | L | L |
| Marazzi, 2011 [34] | L | L | L | L | L | U |
| Mercurio, 2020 [35] | L | L | L | L | L | L |
| Ruscica, 2014 [36] | L | L | L | L | L | U |
| Solà, 2014 [37] | L | L | L | L | L | L |
| Outcomes | Adjustment with Duval and Tweedie’s Trim-and-Fill Method | Begg’s Rank Correlation Test | Egger’s Linear Regression | |||
|---|---|---|---|---|---|---|
| Number of Trimmed Studies | Adjusted Effect Sizes | |||||
| MD | 95% Confidence Interval | p-Value | p-Value | |||
| Lower Bound | Upper Bound | |||||
| Weight | - | - | - | - | 0.602 | 0.672 |
| BMI | 2 | −0.262 | −0.440 | −0.085 | 1 | 0.174 |
| Waist circumference | 1 | −0.819 | −3.10 | 1.462 | 0.174 | 0.6 |
| SBP | 2 | 1.044 | −1.287 | 3.374 | 0.624 | 0.485 |
| DBP | 3 | −1.764 | −3.192 | −0.336 | 0.624 | 0.186 |
| TC | 1 | −26.708 | −29.212 | −24.203 | 0.815 | 0.981 |
| TG | 2 | −10.559 | −16.861 | −4.257 | 0.337 | 0.238 |
| HDL-C | 2 | 1.658 | 0.778 | 2.537 | 0.484 | 0.587 |
| LDL-C | 2 | −29.049 | −31.667 | −26.432 | 0.392 | 0.478 |
| FPG | 2 | −4.007 | −5.521 | −2.492 | 0.532 | 0.563 |
| FPI | - | - | - | - | 0.652 | 0.842 |
| HOMA-IR | - | - | - | - | 0.851 | 0.852 |
| Safety Parameters | Adjustment with Duval and Tweedie’s Trim-and-Fill Method | Begg’s Rank Correlation Test | Egger’s Linear Regression | |||
|---|---|---|---|---|---|---|
| Number of Trimmed Studies | Adjusted Effect Sizes | |||||
| MD | 95% Confidence Interval | p-Value | p-Value | |||
| Lower Bound | Upper Bound | |||||
| ALT | 1 | 2.275 | 0.851 | 3.699 | 0.497 | 0.611 |
| AST | 1 | 0.583 | −0.983 | 2.15 | 0.497 | 0.601 |
| CPK | 1 | 7.868 | − 0.365 | 16.101 | 0.174 | 0.552 |
| Treatment-Emergent Adverse Events | Adjustment with Duval and Tweedie’s Trim-and-Fill Method | Begg’s Rank Correlation Test | Egger’s Linear Regression | |||
| Number of Trimmed Studies | Adjusted Effect Sizes | |||||
| OR | 95% Confidence Interval | p-Value | p-Value | |||
| Lower Bound | Upper Bound | |||||
| Musculoskeletal disorders | - | - | - | - | 1 | 0.759 |
| Gastrointestinal disorders | 1 | 1.014 | 0.321 | 3.201 | 0.602 | 0.951 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicero, A.F.G.; Kennedy, C.; Knežević, T.; Bove, M.; Georges, C.M.G.; Šatrauskienė, A.; Toth, P.P.; Fogacci, F. Efficacy and Safety of Armolipid Plus®: An Updated PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Nutrients 2021, 13, 638. https://doi.org/10.3390/nu13020638
Cicero AFG, Kennedy C, Knežević T, Bove M, Georges CMG, Šatrauskienė A, Toth PP, Fogacci F. Efficacy and Safety of Armolipid Plus®: An Updated PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Nutrients. 2021; 13(2):638. https://doi.org/10.3390/nu13020638
Chicago/Turabian StyleCicero, Arrigo F. G., Cormac Kennedy, Tamara Knežević, Marilisa Bove, Coralie M. G. Georges, Agnė Šatrauskienė, Peter P. Toth, and Federica Fogacci. 2021. "Efficacy and Safety of Armolipid Plus®: An Updated PRISMA Compliant Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials" Nutrients 13, no. 2: 638. https://doi.org/10.3390/nu13020638