
AGREEing on Nutritional Management of Patients with CKD—A Quality Appraisal of the Available Guidelines

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Guideline Appraisal
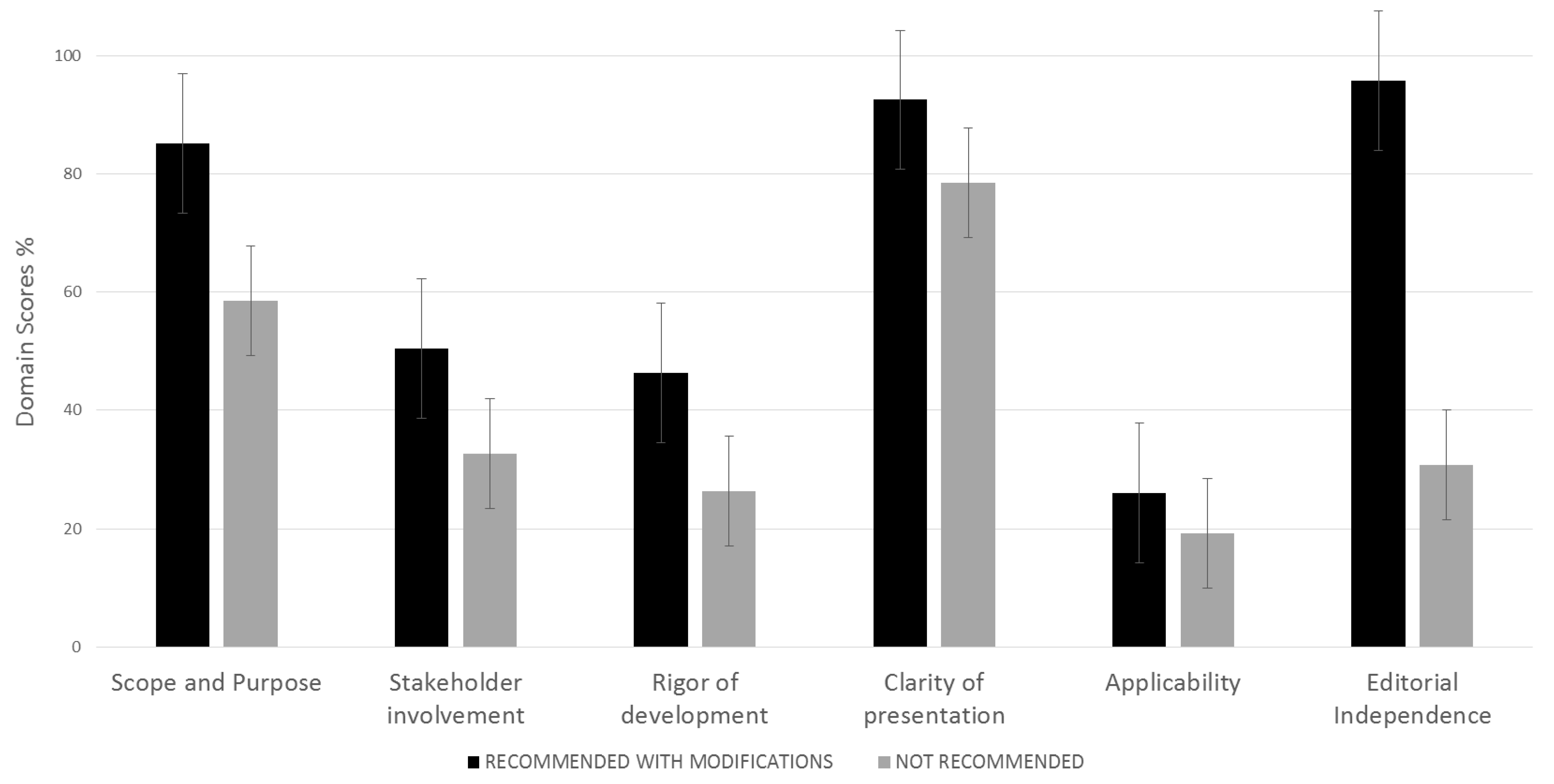
3. Results
3.1. Scope and Purpose Domain
3.2. Stakeholder Involvement Domain
3.3. Rigor of Development
3.4. Clarity of Presentation
3.5. Applicability
3.6. Editorial Independence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASPEN | American Society for Parenteral and Enteral Nutrition |
| CKD | Chronic kidney disease |
| DAA | Dietitians Association of Australia |
| EBPG | European best practice guidelines |
| EDTNA-ERCA | European Dialysis and Transplantation Nurses Association-European Renal Care Association |
| ESPEN | European Society for Clinical Nutrition and Metabolism |
| KDOQI | Kidney disease outcomes quality initiative |
| MNT | Medical nutrition therapy |
| QoL | Quality of life |
| RRT | Renal replacement therapy |
| SIN-ANDID-ANED | Italian Society of Nephrology-Association of Dieticians-Italian Association of Hemodialysis, Dialysis and Transplant |
References
- GBD Chronic Kidney Disease Collaboration; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; Zhao, M.-H.; Lv, J.; Garg, A.X.; Knight, J.; et al. Worldwide access to treatment for end-stage kidney disease: A systematic review. Lancet 2015, 385, 1975–1982. [Google Scholar] [CrossRef]
- Manns, B.; Hemmelgarn, B.; Tonelli, M.; Au, F.; So, H.; Weaver, R.; Quinn, A.E.; Klarenbach, S.; Canadians Seeking Solutions and Innovations to Overcome Chronic Kidney Disease. The Cost of Care for People With Chronic Kidney Disease. Can. J. Kidney Health Dis. 2019, 6, 2054358119835521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanholder, R.; Annemans, L.; Brown, E.; Gansevoort, R.; Gout-Zwart, J.J.; Lameire, N.; Morton, R.L.; Oberbauer, R.; Postma, M.J.; Tonelli, M.; et al. Reducing the costs of chronic kidney disease while delivering quality health care: A call to action. Nat. Rev. Nephrol. 2017, 13, 393–409. [Google Scholar] [CrossRef]
- Elia, M.; Normand, C.; Norman, K.; Laviano, A. A systematic review of the cost and cost effectiveness of using standard oral nutritional supplements in the hospital setting. Clin. Nutr. 2016, 35, 370–380. [Google Scholar] [CrossRef] [Green Version]
- Freijer, K.; Bours, M.J.; Nuijten, M.J.; Poley, M.J.; Meijers, J.M.; Halfens, R.J.; Schols, J.M. The economic value of enteral medical nutrition in the management of disease-related malnutrition: A systematic review. J. Am. Med Dir. Assoc. 2014, 15, 17–29. [Google Scholar] [CrossRef]
- Sharma, Y.; Thompson, C.; Miller, M.; Shahi, R.; Hakendorf, P.; Horwood, C.; Kaambwa, B. Economic evaluation of an extended nutritional intervention in older Australian hospitalized patients: A randomized controlled trial. BMC Geriatr. 2018, 18, 41. [Google Scholar] [CrossRef]
- Campbell, K.L.; Ash, S.; Bauer, J.D. The impact of nutrition intervention on quality of life in pre-dialysis chronic kidney disease patients. Clin. Nutr. 2008, 27, 537–544. [Google Scholar] [CrossRef]
- Lopes, I.M.; Martín, M.; Errasti, P.; Martínez, J.A. Benefits of a dietary intervention on weight loss, body composition, and lipid profile after renal transplantation. Nutrition 1999, 15, 7–10. [Google Scholar] [CrossRef]
- Palmer, S.C.; Maggo, J.K.; Campbell, K.L.; Craig, J.C.; Johnson, D.W.; Sutanto, B.; Ruospo, M.; Tong, A.; Strippoli, G.F.M. Dietary interventions for adults with chronic kidney disease. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine Committee on Nutrition Services for Medicare Beneficiaries. The Role of Nutrition in Maintaining Health in Nation’s Elderly; National Academies Press: Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Management of protein-energy wasting in non-dialysis-dependent chronic kidney disease: Reconciling low protein intake with nutritional therapy. Am. J. Clin. Nutr. 2013, 97, 1163–1177. [Google Scholar] [CrossRef] [Green Version]
- Woolf, S.H.; Grol, R.; Hutchinson, A.; Eccles, M.; Grimshaw, J. Clinical guidelines: Potential benefits, limitations, and harms of clinical guidelines. BMJ Clin. Res. Ed. 1999, 318, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.; Mancher, M.; Miller Wolman, D.; Greenfield, S.; Steinberg, E. (Eds.) Institute of Medicine Committee on Standards for Developing Trustworthy Clinical Practice, Guidelines. In Clinical Practice Guidelines We Can Trust; National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. J. Clin. Epidemiol 2010, 63, 1308–1311. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.O.; Compher, C. A.S.P.E.N. clinical guidelines: Nutrition support in adult acute and chronic renal failure. JPEN J. Parenter Enter. Nutr. 2010, 34, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Ash, S.; Campbell, K.; MacLaughlin, H.; McCoy, E.; Chan, M.; Anderson, K.; Corke, K.; Dumont, R.; Lloyd, L.; Meade, A.; et al. Evidence based practice guidelines for the nutritional management of chronic kidney disease. Nutr. Diet. 2006, 63, S33–S45. [Google Scholar] [CrossRef] [Green Version]
- Druml, W.; Contzen, B.; Joannidis, M.; Kierdorf, H.; Kuhlmann, M.K.; das DGEM Steering Committee. S1-Leitlinie der Deutschen Gesellschaft für Ernährungsmedizin (DGEM) in Zusammenarbeit mit der AKE, der GESKES und der DGfN. Aktuelle Ernahrungsmed. 2015, 40, 21–37. [Google Scholar] [CrossRef] [Green Version]
- Fouque, D.; Vennegoor, M.; Ter Wee, P.; Wanner, C.; Basci, A.; Canaud, B.; Haage, P.; Konner, K.; Kooman, J.; Martin-Malo, A.; et al. EBPG Guideline on Nutrition. Nephrol. Dial. Transplant. 2007, 22, ii45–ii87. [Google Scholar] [CrossRef] [Green Version]
- James, G.; Jackson, H. European Guidelines for the Nutritional Care of Adult Renal Patients. EDTNA-ERCA J. 2003, 29, 23–43. [Google Scholar] [CrossRef]
- Cano, N.; Fiaccadori, E.; Tesinsky, P.; Toigo, G.; Druml, W.; Kuhlmann, M.; Mann, H.; Hörl, W.H. ESPEN Guidelines on Enteral Nutrition: Adult renal failure. Clin. Nutr. 2006, 25, 295–310. [Google Scholar] [CrossRef]
- Cano, N.J.; Aparicio, M.; Brunori, G.; Carrero, J.J.; Cianciaruso, B.; Fiaccadori, E.; Lindholm, B.; Teplan, V.; Fouque, D.; Guarnieri, G. ESPEN Guidelines on Parenteral Nutrition: Adult renal failure. Clin. Nutr. 2009, 28, 401–414. [Google Scholar] [CrossRef]
- Alhambra-Expósito, M.-R.; Molina-Puerta, M.-J.; Olveira, G.; Arraiza-Irigoyen, C.; Fernández-Soto, M.; García-Almeida, J.-M.; García-Luna, P.-P.; Gómez-Pérez, A.-M.; Irles-Rocamora, J.-A.; Molina-Soria, J.-B.; et al. Recomendaciones del grupo GARIN para el tratamiento dietético de los pacientes con enfermedad renal crónica. Nutr. Hosp. 2019, 36, 183–217. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Cupisti, A.; Brunori, G.; Di Iorio, B.R.; D’Alessandro, C.; Pasticci, F.; Cosola, C.; Bellizzi, V.; Bolasco, P.; Capitanini, A.; Fantuzzi, A.L.; et al. Nutritional treatment of advanced CKD: Twenty consensus statements. J. Nephrol. 2018, 31, 457–473. [Google Scholar] [CrossRef] [Green Version]
- Wright, M.; Southcott, E.; MacLaughlin, H.; Wineberg, S. Clinical practice guideline on undernutrition in chronic kidney disease. BMC Nephrol. 2019, 20, 370. [Google Scholar] [CrossRef]
- Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: The AGREE project. Qual. Saf. Health Care 2003, 12, 18–23. [CrossRef]
- Masi, D.; Risi, R.; Basciani, S.; Tuccinardi, D.; Mariani, S.; Lubrano, C.; Gnessi, L.; Watanabe, M. Very Low-Calorie Ketogenic Diets to Treat Patients With Obesity and Chronic Kidney Disease. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2020. [Google Scholar] [CrossRef]
- Watanabe, M.; Tuccinardi, D.; Ernesti, I.; Basciani, S.; Mariani, S.; Genco, A.; Manfrini, S.; Lubrano, C.; Gnessi, L. Scientific evidence underlying contraindications to the ketogenic diet: An update. Obes. Rev. 2020, 21, e13053. [Google Scholar] [CrossRef]


{kind=link}
| No. | Developer # | Year | Region | Intended Population | Scope/Grading System | Number of References | Disciplines Involved in the Group |
|---|---|---|---|---|---|---|---|
| 1 | ASPEN | 2010 | USA | Adult patients with AKI and CKD | Provision of nutrition support to patients with AKI and CKD/Level of evidence I–V | 64 | Physicians, nurses, pharmacologists, dieticians |
| 2 | DAA * | 2006 | Australia | Adults with CKD | Dietetic management of adult patients with CKD/Level of evidence I–IV | 19 | Dietitians, nephrologists, renal nurses |
| 3 | DGEM * | 2015 | Germany | Adults with AKD, CKD, dialysis and transplant patients | Nutrition support and metabolic management in the care of patients with renal dysfunction/No info | 77 | Physicians |
| 4 | EBPG | 2007 | Europe | Adult patients on dialysis | Prevalence, diagnosis and treatment of malnutrition of patients on dialysis/No info | 337 | Dietitians, nephrologists |
| 5 | EDTNA-ERCA | 2003 | Europe | Adults with CKD | Support healthcare professionals on the task of nutrition advice of renal patients/No info | 53 | Physicians, dietitians, nurses |
| 6 | ESPEN | 2006 | Europe | Adult patients with renal failure and patients on dialysis | Recommendations for the use of ONS and TF in nephrology patients/Grade A–C | 72 | No info |
| 7 | ESPEN | 2009 | Europe | Adult patients with renal failure and patients on dialysis | Indications for parenteral nutrition in renal patients with malnutrition/Grade A–C | 123 | Physicians, dietitians |
| 8 | GARIN | 2018 | Spain | Adult patients with CKD stages 1–5 (including patients on dialysis) | define dietary characteristics for adults with renal diseases/GRADE-ASPEN | 96 | Endocrinology and nutrition specialists |
| 9 | KDOQI * | 2020 | International | Adult patients with CKD stages 1–5, (including patients on dialysis), and patients with functional kidney transplant | Provision of MNT guidelines for patients with CKD to assess, prevent, and treat protein-energy wasting, mineral and electrolyte disorders, and other metabolic comorbid conditions associated with CKD/Grade A-D | 531 | Physicians, registered dietitians- nutritionists, researchers, methodologists with expertise in the renal and nutrition field |
| 10 | Renal Association | 2019 | UK | Adult patients with CKD stages 4 and 5 (including dialysis) | Prevalence, diagnosis and treatment of undernutrition in chronic kidney disease/The modified GRADE system | 75 | No information |
| 11 | SIN-ANDID-ANED | 2018 | Italy | Adult patients with advanced renal insufficiency | Promotion of a successful and safe implementation of nutritional treatment for CKD patients/No info | 167 | Nephrologists, dietitians, patients |
| Domains | Clinical Practice Guidelines | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ASPEN [16] | DAA [17] | DGEM [18] | EBPG [19] | EDTNA-ERCA [20] | ESPEN (EN) [21] | ESPEN (PN) [22] | GARIN [23] | KDOQI [24] | SIN-ANDID-ANED [25] | The Renal Association [26] | |
| 1. SCOPE AND PURPOSE | 34.7 | 88.9 | 88.9 | 0.00 | 62.5 | 77.8 | 81.9 | 86.1 | 88.9 | 55.6 | 5.6 |
| a. Overall objectives | 75.0 | 85.7 | 82.1 | 14.3 | 75.0 | 71.4 | 89.3 | 89.3 | 89.3 | 60.7 | 25.0 |
| b. Health questions | 17.9 | 96.4 | 89.3 | 14.3 | 53.6 | 85.7 | 89.3 | 89.3 | 100 | 67.9 | 14.3 |
| c. Population to apply | 39.3 | 89.3 | 100 | 14.3 | 75.0 | 85.7 | 75.0 | 89.3 | 92.0 | 57.1 | 17.9 |
| 2. STAKEHOLDER INVOLVEMENT | 62.5 | 63.9 | 44.4 | 16.7 | 34.7 | 36.1 | 12.5 | 15.3 | 51.4 | 43.1 | 18.1 |
| a. Guideline development group | 85.7 | 75.0 | 64.3 | 53.6 | 32.1 | 53.6 | 42.9 | 39.3 | 100 | 71.4 | 32.1 |
| b. Views and preferences of target population | 28.6 | 71.4 | 14.3 | 17.9 | 32.1 | 14.3 | 14.3 | 14.5 | 17.9 | 53.6 | 14.3 |
| c. Users of guidelines | 89.3 | 60.7 | 78.6 | 14.3 | 67.9 | 67.9 | 17.9 | 28.6 | 57.1 | 28.6 | 42.9 |
| 3. RIGOR OF DEVELOPMENT | 31.3 | 30.2 | 48.9 | 21.9 | 13.0 | 36.5 | 18.2 | 47.4 | 72.4 | 3.6 | 33.3 |
| a. Research methodology | 32.1 | 32.1 | 82.1 | 14.3 | 14.3 | 17.9 | 14.3 | 50.0 | 96.4 | 14.3 | 60.7 |
| b. Selecting criteria | 14.3 | 17.9 | 14.2 | 14.3 | 14.3 | 14.3 | 17.9 | 75.0 | 100 | 14.3 | 14.3 |
| c. Strengths and limitations of evidence | 14.3 | 14.3 | 14.3 | 28.6 | 14.3 | 14.3 | 17.9 | 85.7 | 85.7 | 14.3 | 42.9 |
| d. Formulating methods | 46.4 | 42.9 | 50.0 | 14.3 | 17.9 | 39.3 | 25.0 | 32.1 | 82.1 | 14.3 | 53.6 |
| e. Health benefits, side effects and risks stated in recommendations | 75.0 | 14.3 | 92.9 | 82.1 | 67.9 | 75.0 | 75.0 | 57.1 | 32.1 | 25.0 | 25.0 |
| f. Explicit link of recommendations | 89.3 | 82.1 | 92.9 | 82.1 | 46.4 | 96.4 | 60.7 | 96.4 | 100 | 28.6 | 71.4 |
| g. Review of guideline | 42.9 | 57.1 | 14.3 | 14.3 | 14.3 | 28.6 | 14.3 | 28.6 | 100 | 14.3 | 60.7 |
| h. Updating procedure | 14.3 | 60.7 | 89.3 | 14.3 | 14.3 | 78.6 | 14.3 | 14.3 | 14.3 | 14.3 | 14.3 |
| 4. CLARITY OF PRESENTATION | 52.8 | 84.7 | 100 | 86.1 | 91.7 | 94.4 | 91.7 | 94.4 | 98.6 | 33.3 | 68.1 |
| a. Specific and unambiguous recommendations | 67.9 | 83.3 | 100 | 89.3 | 96.4 | 89.3 | 100 | 96.4 | 100 | 46.4 | 85.7 |
| b. Different options for management | 14.3 | 92.9 | 100 | 75.0 | 85.7 | 96.4 | 96.4 | 89.3 | 96.4 | 25.0 | 60.7 |
| c. Identifiable key recommendations | 96.4 | 96.4 | 100 | 100 | 96.4 | 100 | 82.1 | 100 | 100 | 57.1 | 71.4 |
| 5. APPLICABILITY | 0.0 | 11.5 | 12.5 | 27.1 | 36.5 | 4.2 | 33.3 | 25.0 | 62.5 | 0.0 | 0.0 |
| a. facilitators and barriers of application | 14.3 | 14.3 | 14.3 | 17.9 | 32.1 | 14.3 | 14.2 | 14.3 | 28.6 | 14.3 | 14.3 |
| b. guideline implementation advice and tools | 14.3 | 21.4 | 14.3 | 60.7 | 67.9 | 14.3 | 67.9 | 57.1 | 96.4 | 14.3 | 14.3 |
| c. Resource implications | 14.3 | 21.4 | 14.3 | 28.5 | 28.6 | 14.3 | 14.3 | 17.9 | 57.1 | 14.3 | 14.3 |
| d. Monitoring and/or auditing criteria | 14.3 | 39.3 | 57.1 | 42.9 | 53.6 | 28.6 | 75.0 | 53.6 | 89.3 | 14.3 | 14.3 |
| 6. EDITORIAL INDEPENDENCE | 35.4 | 100 | 47.9 | 0.00 | 36.5 | 95.8 | 6.3 | 39.6 | 91.7 | 50.0 | 47.9 |
| a. Views of funding body | 75.0 | 100 | 21.4 | 14.3 | 17.9 | 96.4 | 14.3 | 82.1 | 85.7 | 42.9 | 14.3 |
| b. Conflicts of interests | 14.3 | 100 | 89.3 | 14.3 | 17.9 | 96.4 | 25.0 | 14.3 | 100 | 71.4 | 96.4 |
| OVERALL QUALITY | Low | Moderate | Low | Low | Low | Moderate | Low | Low | Moderate | Low | Low |
| RECOMMENDATIONS | |||||||||||
| Recommended | |||||||||||
| With modifications | X | X | X | ||||||||
| Not recommended | X | X | X | X | X | X | X | X | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakaloudi, D.R.; Chrysoula, L.; Poulia, K.A.; Dounousi, E.; Liakopoulos, V.; Chourdakis, M. AGREEing on Nutritional Management of Patients with CKD—A Quality Appraisal of the Available Guidelines. Nutrients 2021, 13, 624. https://doi.org/10.3390/nu13020624
Bakaloudi DR, Chrysoula L, Poulia KA, Dounousi E, Liakopoulos V, Chourdakis M. AGREEing on Nutritional Management of Patients with CKD—A Quality Appraisal of the Available Guidelines. Nutrients. 2021; 13(2):624. https://doi.org/10.3390/nu13020624
Chicago/Turabian StyleBakaloudi, Dimitra Rafailia, Lydia Chrysoula, Kalliopi Anna Poulia, Evangelia Dounousi, Vassilios Liakopoulos, and Michail Chourdakis. 2021. "AGREEing on Nutritional Management of Patients with CKD—A Quality Appraisal of the Available Guidelines" Nutrients 13, no. 2: 624. https://doi.org/10.3390/nu13020624