Eating Behavior, Physical Activity and Exercise Training: A Randomized Controlled Trial in Young Healthy Adults

 , ,
, , 
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Design
2.2. Assessment of Time Spent in Sedentary Behaviour and in Physical Activity
2.3. Eating Behaviour Traits
- The Binge Eating Scale (BES). This was used to assess eight feelings/cognitive actions (e.g., guilt, worry over excess eating of certain foods) and eight behavioural manifestations (e.g., eating rapidly, eating in secret) related to binge eating. The weight of each statement (0–3) is then summed. A higher total score reflects more severe binge-eating problems [8].
- The Three-Factor Eating Questionnaire-R18 (TFEQ). This was used to assess three “dimensions” of eating behaviour: (i) cognitive restraint (six questions), i.e., the conscious restriction of food intake in order to control body weight or to promote weight loss; (ii) uncontrolled eating (nine questions), i.e., the tendency to eat more than usual due to a loss of control over intake, accompanied by subjective feelings of hunger, and (iii) emotional eating (three questions), characterized by the inability to resist emotional cues, or eating as a response to different negative emotions. This questionnaire involves 18 questions each measured on a 4-point response scale (definitely true: 1, mostly true: 2, mostly false: 3, definitely false: 4). The scores are summed for each dimension. This shortened version of the original questionnaire maintains its validity and internal consistency [10].
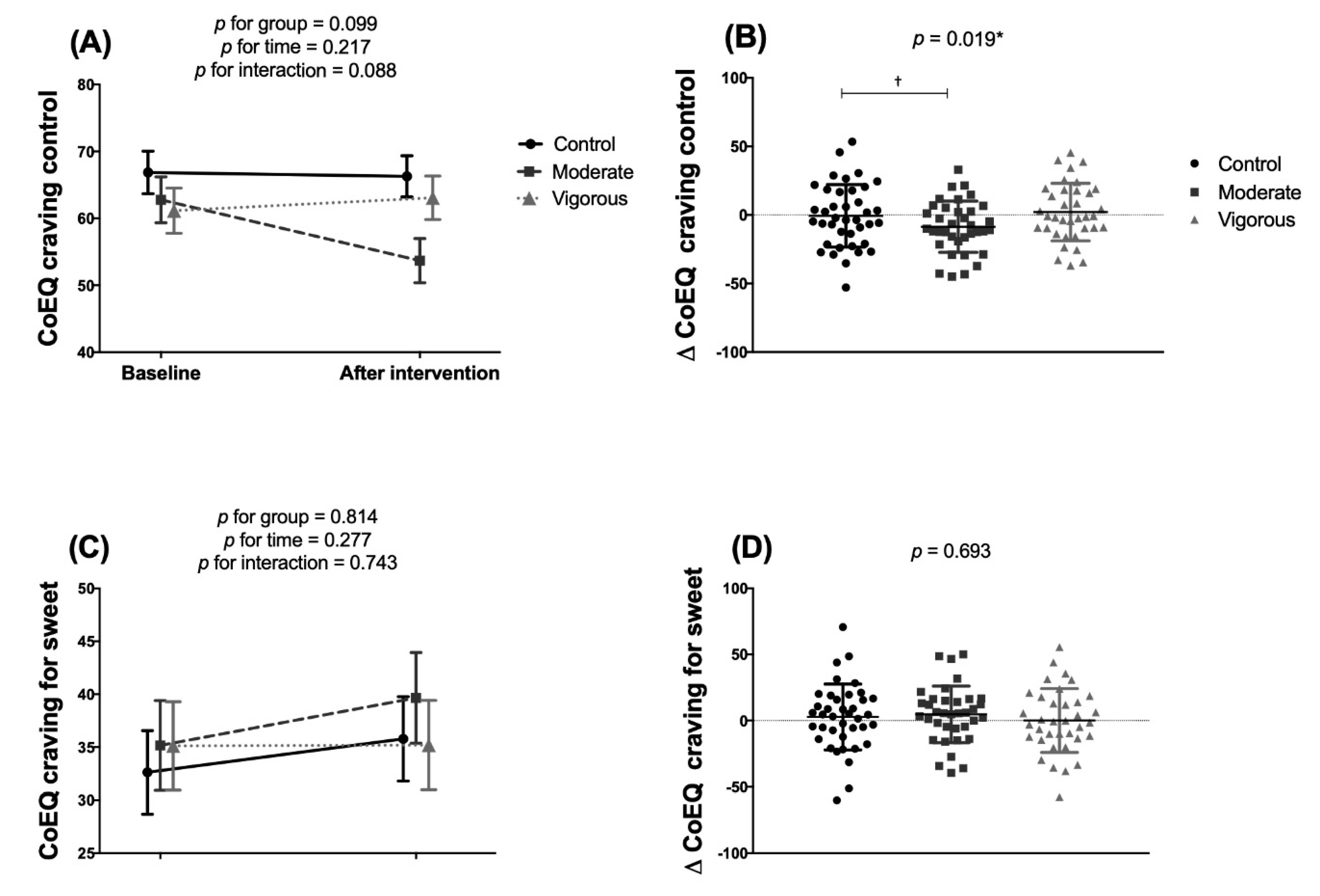
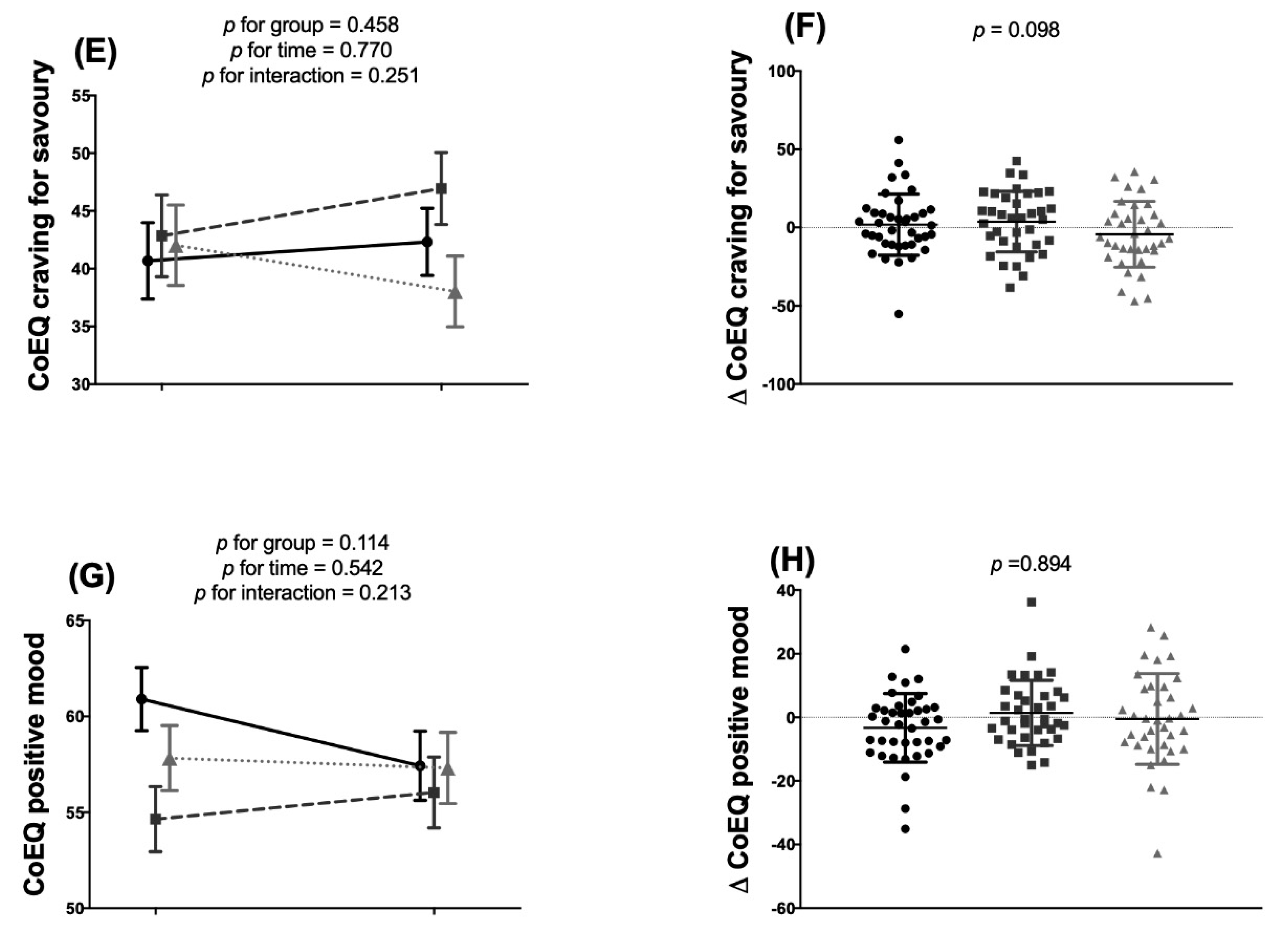
- Control of Eating Questionnaire (CoEQ). This questionnaire comprises 21 questions designed to assess the type and intensity of food cravings experienced, as well as subjective sensations regarding appetite and mood [11]. Subjects answered according to their experiences over the previous seven days; all answers were provided using a visual analogue scale (0–100). The scores for the subscales Craving Control, Craving for Sweet, Craving for Savoury and Positive Mood were then calculated.
2.4. Anthropometric and Body Composition Assessments
2.5. Energy Intake
2.6. Exercise Intervention
2.7. Statistical Analysis
3. Results
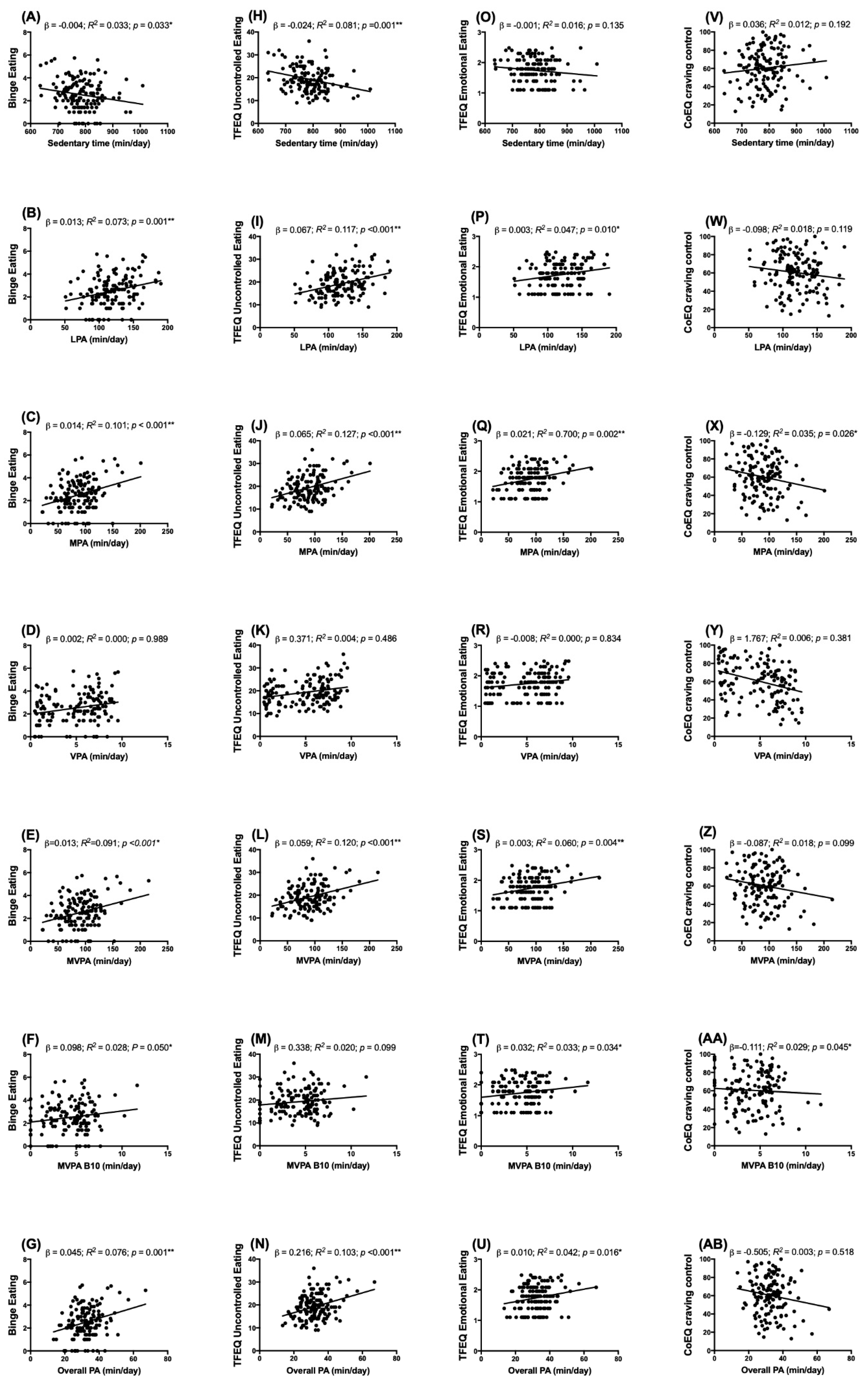
3.1. Cross-Sectional Analyses
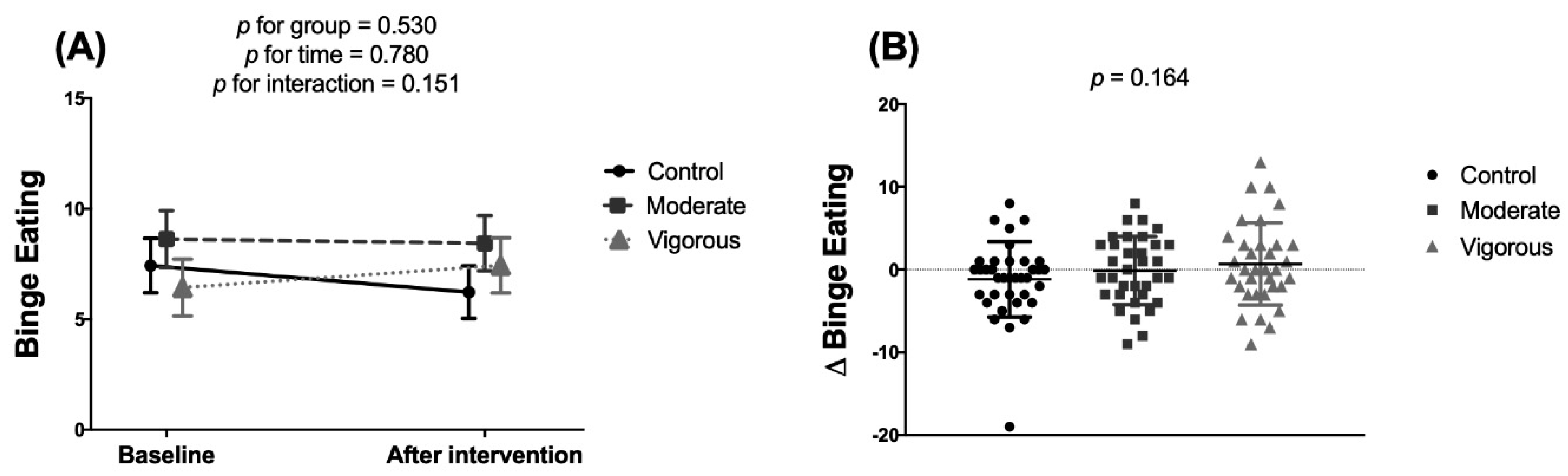
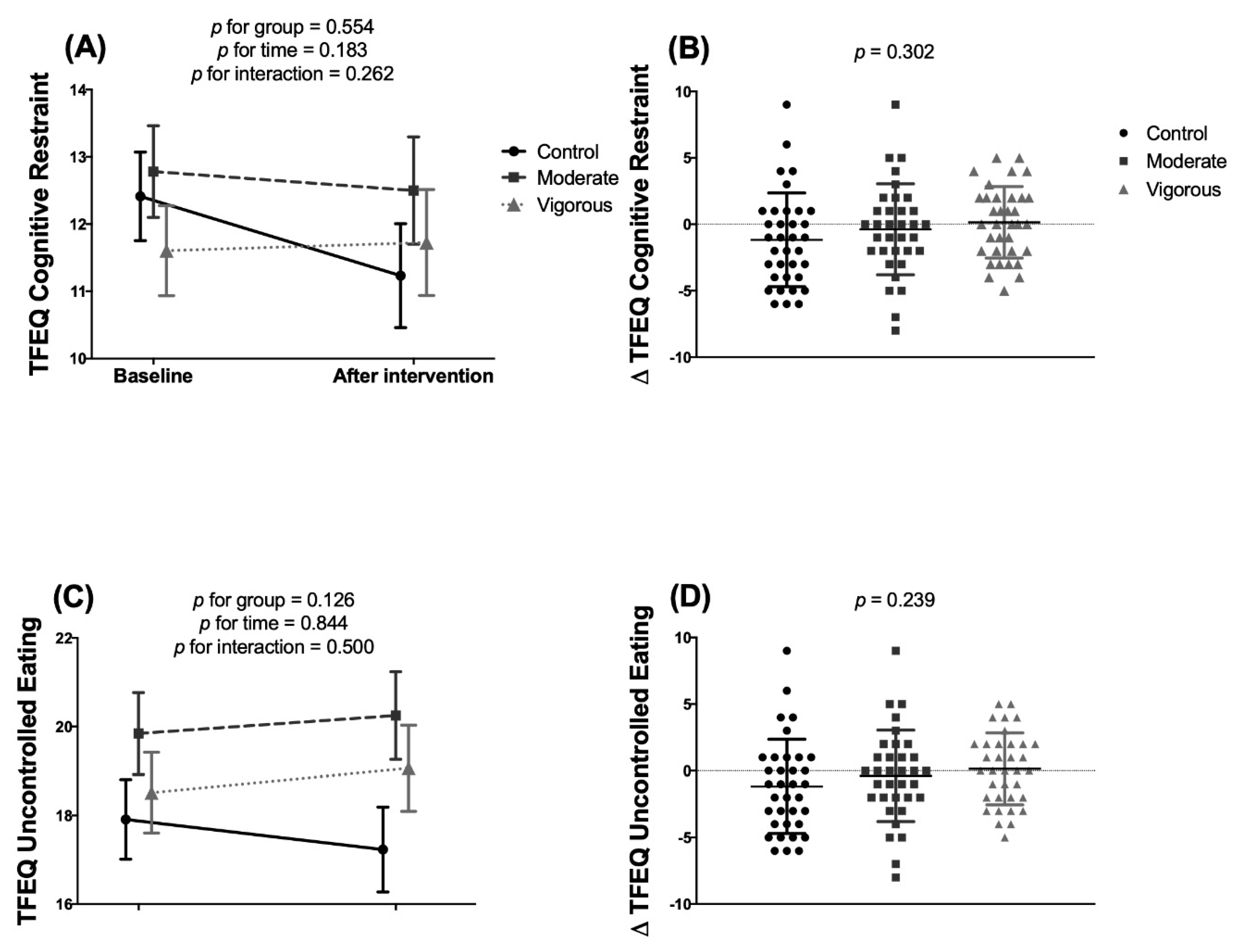
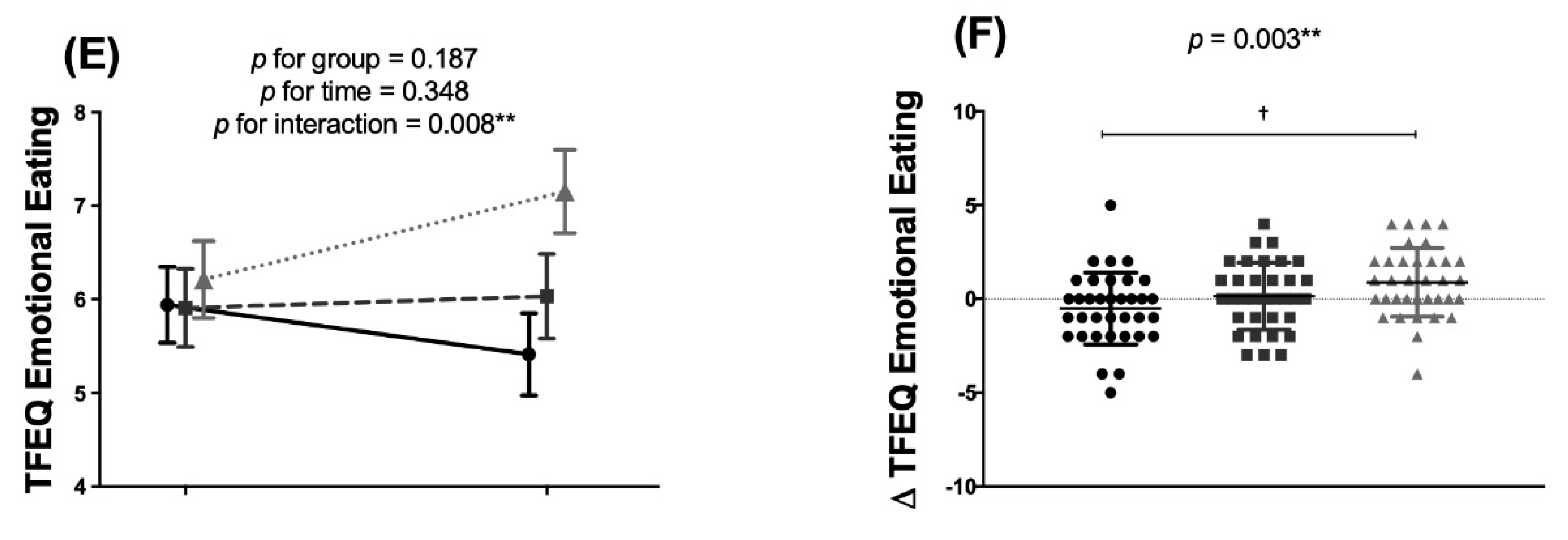
3.2. Longitudinal Analysis
4. Discussion
4.1. Association of Eating Behaviour Traits with Time Spent in Sedentary Behaviour and Physical Activity
4.2. Effect of the Exercise Intervention on Eating Behaviour Traits
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chaput, J.P.; Tremblay, A. Obesity and Physical Inactivity: The Relevance of Reconsidering the Notion of Sedentariness. Obes. Facts 2009, 2, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.E. The Control of Appetite: Basic Concepts and Practical Implications. Schweiz. Med. Wochenschr. 1999, 129, 182–188. [Google Scholar] [PubMed]
- Bond, M.J.; McDowell, A.J.; Wilkinson, J.Y. The Measurement of Dietary Restraint, Disinhibition and Hunger: An Examination of the Factor Structure of the Three Factor Eating Questionnaire (TFEQ). Int. J. Obes. Relat. Metab. Disord. 2001, 25, 900–906. [Google Scholar] [CrossRef] [PubMed]
- De Castro, J.M. How Can Eating Behavior Be Regulated in the Complex Environments of Free-Living Humans? Neurosci. Biobehav. Rev. 1996, 20, 119–131. [Google Scholar] [CrossRef]
- Martins, C.; Morgan, L.; Truby, H. A Review of the Effects of Exercise on Appetite Regulation: An Obesity Perspective. Int. J. Obes. 2008, 32, 1337–1347. [Google Scholar] [CrossRef]
- Bryant, E.J.; King, N.A.; Blundell, J.E. Disinhibition: Its Effects on Appetite and Weight Regulation. Obes. Rev. 2008, 9, 409–419. [Google Scholar] [CrossRef]
- Drenowatz, C.; Evensen, L.H.; Ernstsen, L.; Blundell, J.E.; Hand, G.A.; Shook, R.P.; Hébert, J.R.; Burgess, S.; Blair, S.N. Cross-Sectional and Longitudinal Associations between Different Exercise Types and Food Cravings in Free-Living Healthy Young Adults. Appetite 2017, 118, 82–89. [Google Scholar] [CrossRef]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The Assessment of Binge-Eating Severity among Obese Persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Messick, S. The Three-Factor Eating Questionnaire to Measure Dietary Restraint, Disinhibition and Hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Jáuregui-Lobera, I.; García-Cruz, P.; Carbonero-Carreño, R.; Magallares, A.; Ruiz-Prieto, I. Psychometric Properties of Spanish Version of the Three-Factor Eating Questionnaire-R18 (Tfeq-Sp) and Its Relationship with Some Eating- and Body Image-Related Variables. Nutrients 2014, 6, 5619–5635. [Google Scholar] [CrossRef]
- Dalton, M.; Finlayson, G.; Hill, A.; Blundell, J. Preliminary Validation and Principal Components Analysis of the Control of Eating Questionnaire (CoEQ) for the Experience of Food Craving. Eur. J. Clin. Nutr. 2015, 69, 1313–1317. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.J.; Alonso-Alonso, M.; Bond, D.S.; Pascual-Leone, A.; Blackburn, G.L. The Neurocognitive Connection between Physical Activity and Eating Behaviour. Obes. Rev. 2011, 12, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, K.; Hopkins, M.; Long, C.; Blundell, J.; Finlayson, G. High Habitual Physical Activity Improves Acute Energy Compensation in Nonobese Adults. Med. Sci. Sport. Exerc. 2017, 49, 2268–2275. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.E.; Gillett, A. Control of Food Intake in the Obese. Obes. Res. 2001, 9, 263S–270S. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Delgado, G.; Martinez-Tellez, B.; Olza, J.; Aguilera, C.M.; Labayen, I.; Ortega, F.B.; Chillon, P.; Fernandez-Reguera, C.; Alcantara, J.M.A.; Martinez-Avila, W.D.; et al. Activating Brown Adipose Tissue through Exercise (ACTIBATE) in Young Adults: Rationale, Design and Methodology. Contemp. Clin. Trials 2015, 45, 416–425. [Google Scholar] [CrossRef]
- Van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.M.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of Accelerometer Data for Free-Living Physical Activity Assessment Using Local Gravity and Temperature: An Evaluation on Four Continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef]
- van Hees, V.T.; Sabia, S.; Anderson, K.N.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.G.; Kivimäki, M.; Trenell, M.I.; Singh-Manoux, A. A Novel, Open Access Method to Assess Sleep Duration Using a Wrist-Worn Accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef]
- Hildebrand, M.; Van Hees, V.T.; Hansen, B.H.; Ekelund, U. Age Group Comparability of Raw Accelerometer Output from Wrist-and Hip-Worn Monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef]
- Hildebrand, M.; Hansen, B.H.; van Hees, V.T.; Ekelund, U. Evaluation of Raw Acceleration Sedentary Thresholds in Children and Adults. Scand. J. Med. Sci. Sports 2017, 27, 1814–1823. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Ruiz López, M.D.; Artacho Martin-Lagos, R. Guía Para Estudios Dietéticos: Álbum Fotográfico de Alimentos; Editorial Universidad de Granada: Granada, Spain, 2010. [Google Scholar]
- Oh, H.; Taylor, A.H. A Brisk Walk, Compared with Being Sedentary, Reduces Attentional Bias and Chocolate Cravings among Regular Chocolate Eaters with Different Body Mass. Appetite 2013, 71, 144–149. [Google Scholar] [CrossRef]
- Sim, A.Y.; Lee, L.L.; Cheon, B.K. When Exercise Does Not Pay: Counterproductive Effects of Impending Exercise on Energy Intake among Restrained Eaters. Appetite 2018, 123, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Rabia, M.; Knäuper, B.; Miquelon, P. The Eternal Quest for Optimal Balance between Maximizing Pleasure and Minimizing Harm: The Compensatory Health Beliefs Model. Br. J. Health Psychol. 2006, 11, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Shook, R.P.; Hand, G.A.; Drenowatz, C.; Hebert, J.R.; Paluch, A.E.; Blundell, J.E.; Hill, J.O.; Katzmarzyk, P.T.; Church, T.S.; Blair, S.N. Low Levels of Physical Activity Are Associated with Dysregulation of Energy Intake and Fat Mass Gain over 1 Year. Am. J. Clin. Nutr. 2015, 102, 1332–1338. [Google Scholar] [CrossRef] [PubMed]
- Myers, A.; Gibbons, C.; Finlayson, G.; Blundell, J. Associations among Sedentary and Active Behaviours, Body Fat and Appetite Dysregulation: Investigating the Myth of Physical Inactivity and Obesity. Br. J. Sports Med. 2017, 51. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as Medicine - Evidence for Prescribing Exercise as Therapy in 26 Different Chronic Diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Messerli-Bürgy, N.; Stülb, K.; Kakebeeke, T.H.; Arhab, A.; Zysset, A.E.; Leeger-Aschmann, C.S.; Schmutz, E.A.; Meyer, A.H.; Ehlert, U.; Garcia-Burgos, D.; et al. Emotional Eating Is Related with Temperament but Not with Stress Biomarkers in Preschool Children. Appetite 2018, 120, 256–264. [Google Scholar] [CrossRef]
- Blundell, J.E.; Stubbs, R.J.; Golding, C.; Croden, F.; Alam, R.; Whybrow, S.; Le Noury, J.; Lawton, C.L. Resistance and Susceptibility to Weight Gain: Individual Variability in Response to a High-Fat Diet. Physiol. Behav. 2005, 86, 614–622. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 139) | CG (n = 53) | MIIG (n = 43) | VIIG (n = 43) | ||
|---|---|---|---|---|---|
| Women (n, (%)) | 95, (68.35) | 34, (64.20) | 31, (72.10) | 30, (69.80) | |
| Men (n, (%)) | 44, (31.65) | 19, (35.80) | 12, (27.90) | 13, (30.20) | |
| Age (years) | 22.06 ± 2.26 | 21.8 ± 2.17 | 22.08 ± 2.19 | 22.35 ± 2.45 | |
| Body composition | |||||
| BMI (kg/m2) a | 24.95 ± 4.57 | 24.47 ± 5.03 | 25.58 ± 4.13 | 24.91 ± 4.40 | |
| Lean mass (kg) b | 41.22 ± 9.15 | 41.43 ± 10.11 | 40.90 ± 8.05 | 41.28 ± 9.12 | |
| Fat mass (kg) b | 25.03 ± 8.65 | 23.87 ± 8.75 | 26.90 ± 8.77 | 24.65 ± 8.29 | |
| Fat mass (%) b | 36.08 ± 7.45 | 34.95 ± 7.34 | 37.95 ± 8.04 | 35.65 ± 6.76 | |
| Eating behaviour traits | |||||
| Binge Eating (BES) | 8.10 ± 7.25 | 7.81 ± 7.87 | 9.4 ± 6.27 | 7.16 ± 7.35 | |
| TFEQ | Cognitive Restraint | 12.07 ± 3.78 | 12.34 ± 3.39 | 12.56 ± 4.15 | 11.26 ± 3.82 |
| Uncontrolled Eating | 19.32 ± 5.43 | 19.09 ± 5.49 | 19.79 ± 4.89 | 19.14 ± 5.95 | |
| Emotional Eating | 6.17 ± 2.43 | 6.08 ± 2.48 | 6.16 ± 6.16 | 6.28 ± 2.36 | |
| CoEQ | Craving control | 60.34 ± 20.60 | 62.34 ± 20.82 | 57.83 ± 19.50 | 60.40 ± 21.56 |
| Craving for sweet | 36.65 ± 24.23 | 36.64 ± 25.03 | 36.61 ± 23.11 | 36.71 ± 24.90 | |
| Craving for savoury | 44.47 ± 19.96 | 44.35 ± 22.89 | 44.85 ± 17.18 | 44.23 ± 19.12 | |
| Positive mood | 58.15 ± 11.72 | 61.07 ± 12.43 | 54.89 ± 10.81 | 57.80 ± 11.02 | |
| Time spent in sedentary behaviour/habitual PA intensity | |||||
| Valid days (days) | 6.77 ± 0.54 | 6.77 ± 0.54 | 6.74 ± 0.58 | 6.79 ± 0.51 | |
| Wear time (min/day) | 19.91 ± 25.59 | 19.30 ± 24.02 | 18.80 ± 29.37 | 21.80 ± 23.85 | |
| Waking time (min/day) | 995.86 ± 49.56 | 992.47 ± 57.30 | 1009.66 ± 45.45 | 986.22 ± 40.42 | |
| Sedentary time (min/day) | 785.40 ± 63.88 | 788.38 ± 71.10 | 788.71 ± 63.50 | 778.43 ± 55.18 | |
| LPA (min/day) | 119.40 ± 27.85 | 114.90 ± 28.08 | 124.72 ± 27.48 | 119.64 ± 27.63 | |
| MPA (min/day) | 88.19 ± 30.02 | 86.63 ± 33.59 | 92.87 ± 26.91 | 85.43 ± 28.42 | |
| VPA (min/day) | 2.86 ± 3.50 | 2.57 ± 3.28 | 3.36 ± 4.25 | 2.71 ± 2.83 | |
| MVPA (min/day) | 91.05 ± 31.61 | 89.19 ± 35.24 | 96.23 ± 28.37 | 88.15 ± 30.02 | |
| MVPA B10 (min/day) | 24.00 ± 20.64 | 26.20 ± 22.10 | 23.49 ± 15.34 | 21.80 ± 23.44 | |
| Overall PA (ENMO, mG/5s) | 32.56 ± 8.06 | 31.72 ± 8.76 | 33.68 ± 7.45 | 32.49 ± 7.81 | |
| Binge Eating | TFEQ | CoEQ | ||||||
|---|---|---|---|---|---|---|---|---|
| CR | UE | EE | Craving Control | Craving for Sweet | Craving for Savoury | Positive Mood | ||
| Sedentary Time | −0.181 * | −0.031 | −0.286 ** | −0.127 | 0.111 | −0.073 | −0.025 | −0.071 |
| LPA | 0.270 ** | 0.107 | 0.340 *** | 0.218 * | −0.133 | 0.090 | 0.088 | 0.028 |
| MPA | 0.317 *** | 0.095 | 0.359 *** | 0.264 ** | −0.188 * | 0.115 | 0.121 | −0.071 |
| VPA | 0.001 | −0.001 | 0.060 | −0.018 | 0.075 | −0.061 | −0.050 | 0.091 |
| MVPA | 0.302 *** | 0.091 | 0.346 *** | 0.245 ** | −0.170 * | 0.105 | 0.109 | −0.059 |
| MVPA B10 | 0.167 * | 0.152 | 0.140 | 0.180 * | −0.055 | 0.124 | −0.014 | −0.092 |
| Overall PA (ENMO, mG/5s) | 0.275 ** | 0.059 | 0.321 *** | 0.204 * | −0.152 | 0.085 | 0.071 | −0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Avila, W.D.; Sanchez-Delgado, G.; Acosta, F.M.; Jurado-Fasoli, L.; Oustric, P.; Labayen, I.; Blundell, J.E.; Ruiz, J.R. Eating Behavior, Physical Activity and Exercise Training: A Randomized Controlled Trial in Young Healthy Adults. Nutrients 2020, 12, 3685. https://doi.org/10.3390/nu12123685
Martinez-Avila WD, Sanchez-Delgado G, Acosta FM, Jurado-Fasoli L, Oustric P, Labayen I, Blundell JE, Ruiz JR. Eating Behavior, Physical Activity and Exercise Training: A Randomized Controlled Trial in Young Healthy Adults. Nutrients. 2020; 12(12):3685. https://doi.org/10.3390/nu12123685
Chicago/Turabian StyleMartinez-Avila, Wendy D., Guillermo Sanchez-Delgado, Francisco M. Acosta, Lucas Jurado-Fasoli, Pauline Oustric, Idoia Labayen, John E. Blundell, and Jonatan R. Ruiz. 2020. "Eating Behavior, Physical Activity and Exercise Training: A Randomized Controlled Trial in Young Healthy Adults" Nutrients 12, no. 12: 3685. https://doi.org/10.3390/nu12123685
APA StyleMartinez-Avila, W. D., Sanchez-Delgado, G., Acosta, F. M., Jurado-Fasoli, L., Oustric, P., Labayen, I., Blundell, J. E., & Ruiz, J. R. (2020). Eating Behavior, Physical Activity and Exercise Training: A Randomized Controlled Trial in Young Healthy Adults. Nutrients, 12(12), 3685. https://doi.org/10.3390/nu12123685