A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies




1
Department of Twin Research and Genetic Epidemiology, Kings College London, London SE1 7EH, UK
2
First Department of Internal Medicine, Division of Endocrinology and Metabolism, Diabetes Center, Medical School, AHEPA University Hospital, 546 21 Thessaloniki, Greece
3
Department of Hypertension, Chair of Nephrology and Hypertension, Medical University of Lodz, 93-338 Lodz, Poland
4
Polish Mother’s Memorial Hospital Research Institute (PMMHRI), 93-338 Lodz, Poland
5
Cardiovascular Research Centre, University of Zielona Gora, 65-046 Zielona Gora, Poland
*
Author to whom correspondence should be addressed.
Nutrients 2020, 12(8), 2350; https://doi.org/10.3390/nu12082350
Submission received: 12 July 2020
/
Accepted: 23 July 2020
/
Published: 6 August 2020
(This article belongs to the Section Phytochemicals and Human Health)
Abstract
:Introduction: The links between flavonoid intake and mortality were previously evaluated in epidemiological studies. The aim of the present study was to perform a systematic review and meta-analysis of cohort studies evaluating the link of flavonoid consumption with total and cause-specific mortality. Methods: Prospective cohort studies reporting flavonoid intake and mortality data published up to 30th April 2019 (without language restriction) were searched using PubMed, Scopus and EMBASE database. Generic inverse variance methods and random effects models were used to synthesize pooled and quantitative data. Sensitivity analysis was also performed by a leave-one-out method. Results: Overall, 16 articles met the inclusion criteria (nine studies were performed in Europe, five in the USA, one in Asia and one in Oceania); a total of 462,194 participants (all adults aged >19 years) with 23,473 mortality cases were included in the final analysis. The duration of follow-up ranged from 4.8 to 28 years. Most of the studies assessed flavonoid intake using food frequency questionnaires, whereas four studies used interviews and 1 study used 4-day food records. The meta-analysis showed that flavonoid consumption was inversely and significantly associated with total (relative risk (RR): 0.87, 95% confidence interval (CI) = 0.77–0.99) and cardiovascular disease mortality risk (RR: 0.85, 95%CI = 0.75–0.97), but not cancer (0.86, 95%CI = 0.65–1.14) mortality risk. These findings remained robust in sensitivity analyses. Conclusions: The present findings highlight the potential protective role of flavonoids against total and cause-specific mortality. These results support the recommendations for flavonoid-rich foods intake to prevent chronic diseases.
1. Introduction
Cardiovascular disease (CVD) remains the leading cause of death worldwide; however, in the high-income countries, cancer deaths have exceeded it [1]. The total number of deaths from non-communicable diseases increased from 2007 to 2017 by 22.7%; there were 7.61 million additional deaths estimated in 2017 (in comparison to 2007) [1]. The beneficial role of a healthy, balanced diet (i.e., rich in fruits and vegetables) on preventing CVD and cancer morbidity and mortality has been demonstrated in several large cohort studies [2,3].
Flavonoids present in foods may contribute to CVD protection [4]. Flavonoids are characterized by a shared skeleton of diphenylpropane, found in flavones, flavonols, flavanones, flavan-3-ols, etc., commonly present in vegetables, fruits, herbs and teas [4]. Flavonoids exert antioxidant properties and thus they may reduce plasma low-density lipoprotein (LDL) oxidation [5]. Furthermore, flavonoids may beneficially affect the vascular endothelium by inhibiting platelet aggregation and thus reducing the risk of clot formation [5]. However, available data on the association between flavonoid intake and all-cause, cancer and CVD mortality are limited and inconsistent [4,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]. In this context, with regard to the risk of total mortality, studies reported inverse [17], insignificant [4,9,11,16,18] or positive associations with flavonoid consumption [7]. For example, among 93,145 young and middle-aged women in the Nurses’ Health Study II (NHS-II), those in the highest fifth of flavonoid intake had an insignificantly lower total (risk ratio (RR): 0.92, 95% confidence interval (CI): 0.80-1.06), cancer (RR: 0.84, 95%CI: 0.67–1.04) and CVD (RR:0.83, 95%CI: 0.53–1.29) mortality risk compared with those in the lowest fifth [20].
A previous meta-analysis (n = 10 studies) showed a protective role of flavonoid intake in relation to total mortality (RR: 0.82, 95% 0.72–0.92), but no significant correlation with CVD mortality (RR: 0.85, 95%CI: 0.70–1.03) [21]. Regarding cancer mortality, data are also scarce with contradictory results: two studies reported a non-significant association [7,16], while another one supported a protective role for flavonoid intake [17]. Another meta-analysis (n = 15 cohort studies) found that flavonoid intake significantly decreased total and CVD mortality but did not investigate the association with cancer mortality [5].
In the present meta-analysis, we systematically reviewed current data from prospective studies on flavonoid consumption in relation to the risk of total, cancer and CVD mortality.
2. Methods
2.1. Literature Search and Study Selection
The Observational Studies in Epidemiology (MOOSE) guidelines were followed to design, conduct and report the present meta-analysis [22]. The primary exposure of interest was flavonoid intake, while the primary outcome of interest was alterations in cause-specific and total mortality subsequent to flavonoid consumption. Prospective cohort studies published up to 30 April 2019 (without language restriction) were searched in the EMBASE, PubMed and Scopus databases. The query syntax of the search is shown in Supplementary Table S1. We excluded duplicates, studies with participants aged ≤18 years at baseline and animal studies. Eligible studies were selected by using the predefined inclusion criteria of prospective cohort studies and original articles on the association of flavonoid intake and all-cause, cancer and CVD mortality. Furthermore, the reference list of eligible articles was searched and email correspondences with authors for additional data were performed, if needed.
2.2. Study Selection
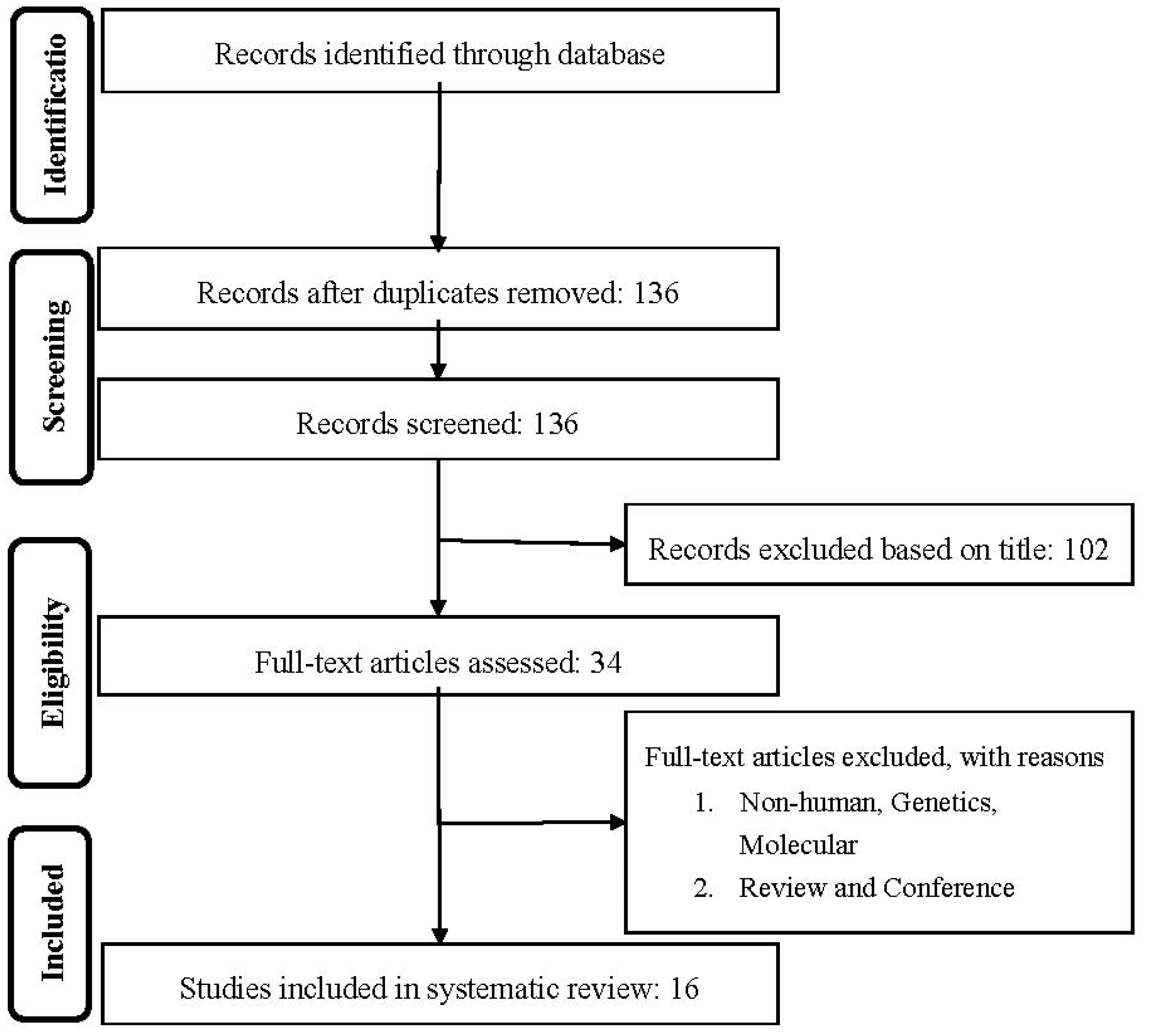
First, duplicates were removed, and then titles and abstracts were screened by two reviewers (MM and NK) who were blinded to the qualifications, names or the institutional affiliations of the study authors to avoid bias. Between these two reviewers, agreement was excellent (Kappa index: 0.91; p < 0.001), and any disagreements were resolved between the reviewers before the selected articles were retrieved (Figure 1 shows the flow chart of study selection).
Studies were included if they met all the following criteria: (1) the primary exposure of interest was flavonoid consumption; (2) the studies were population-based cohort studies, reporting total, CVD and cancer mortality; (3) hazard ratio (HR), RR or odds ratio (OR) estimates with 95%CI adjusted for multivariable parameters were provided or were able to be calculated; and (4) original articles with full texts in English.
We excluded: (1) letters, reviews, comments, editorials, expert opinion papers, methodological articles, unpublished data or any publication lacking primary data and/or explicit method descriptions; (2) non-English papers; (3) studies other than population-based cohorts; and (4) studies in which HR, RR or OR estimates with 95%CI were not available or not able to be calculated.
2.3. Data Extraction
The full texts of the included studies were retrieved and screened for eligibility by two reviewers (Mohsen Mazidi, Niki Katsiki). The Newcastle–Ottawa Scale (NOS, Supplementary Table S2) was used to assess the quality of the included studies [23], considering dietary survey methods of flavonoid intake; representativeness of the exposed cohort; assessment of outcome; comparability of cohorts (adjustment for important confounders); duration and adequacy of follow-up. By evaluating selection, comparability and outcome, the study score ranged from 0 (highest degree of bias) to 9 (lowest degree of bias). Following methodological quality assessment, the 2 reviewers extracted data by using a purpose-designed data extraction form. They also independently produced a summary of the most important outcomes from each study. Any differences of opinion in relation to these summaries were resolved by consultation with a third reviewer (Maciej Banach). The first reviewer (Mohsen Mazidi) conducted any further necessary calculations on data, checked by the second reviewer (Niki Katsiki). The data extracted from each eligible study included: author, study name, year, country, references, mean age, men (%), the number of cases and participants, follow-up time (years), main confounders and outcomes.
2.4. Data Synthesis and Statistical Analyses
When study results were from different multivariable-adjusted models, the model with the majority of the confounding parameters was used for the present meta-analysis. Pooled RR, 95%CI and p value for heterogeneity were calculated with the random-effect model. RRs comparing the highest with the lowest flavonoid intake category were combined across studies to generate the summary associations. The I2 test [24,25,26] and I2 > 50% together with p (two-sided) < 0.05 indicated significant heterogeneity across studies [24,25,26]. A sensitivity analysis, excluding one study at a time, was conducted to examine whether the present results were affected by a single study.
2.5. Publication Bias
The presence of publication bias was evaluated by the visual inspection of Begg’s funnel plot asymmetry and Egger’s weighted regression tests. Furthermore, the Duval and Tweedie trim method was applied to adjust the analysis for the effects of publication bias [27]. The present meta-analysis was conducted with the use of the Comprehensive Meta-Analysis (CMA) V3 software (Biostat, Englewood, NJ, USA) [28].
3. Results
Overall, of the 34 eligible full articles, 16 articles met the inclusion criteria (Figure 1). An overview of the key characteristics of these 16 prospective cohort studies is shown in Table 1. A total of 462,194 participants, with 23,473 mortality cases were included in the final analysis. The duration of follow-up ranged from 4.8 to 28 years. Quality assessment results are shown in the Supplementary Table S3. All participants were adults (aged >29 years) at baseline. With regard to geographical region, seven studies were carried out in Europe [4,7,8,10,14,18,19], five in the USA [6,11,12,15,20] one in Asia [13] and one in Oceania [17]. Six studies included both male and female individuals [9,10,15,16,18,19], and nine studies included only male [4,6,7,8,14] or female [11,12,17,20] participants. In the majority of the studies, flavonoid intake was assessed by food frequency questionnaires [6,8,11,12,13,14,15,17,18,19,20], whereas four studies used interviews [4,9,10,16] and one study used 4-day food records [7].
3.1. Associations of Flavonoid Intake with All Cause, CVD and Stroke Mortality
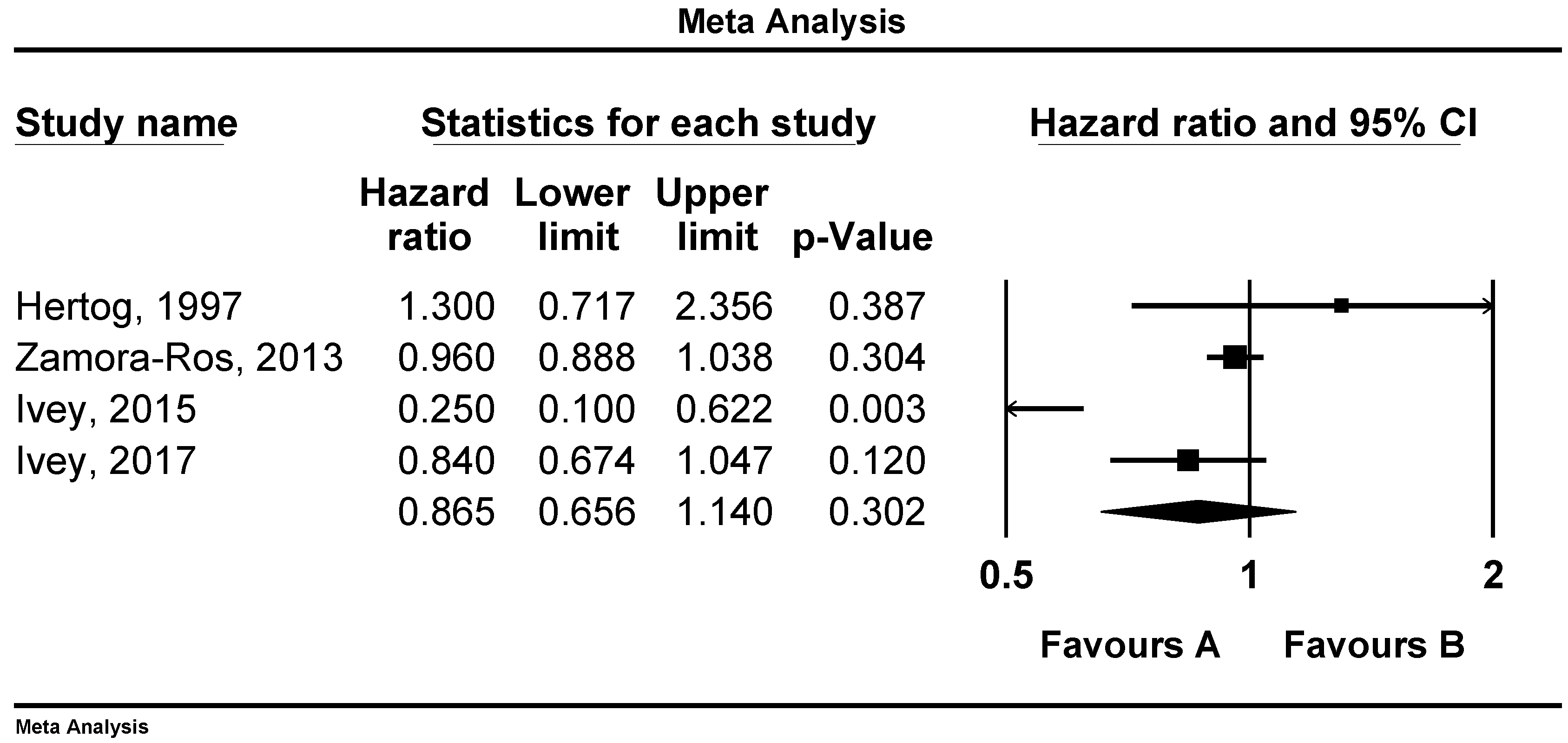
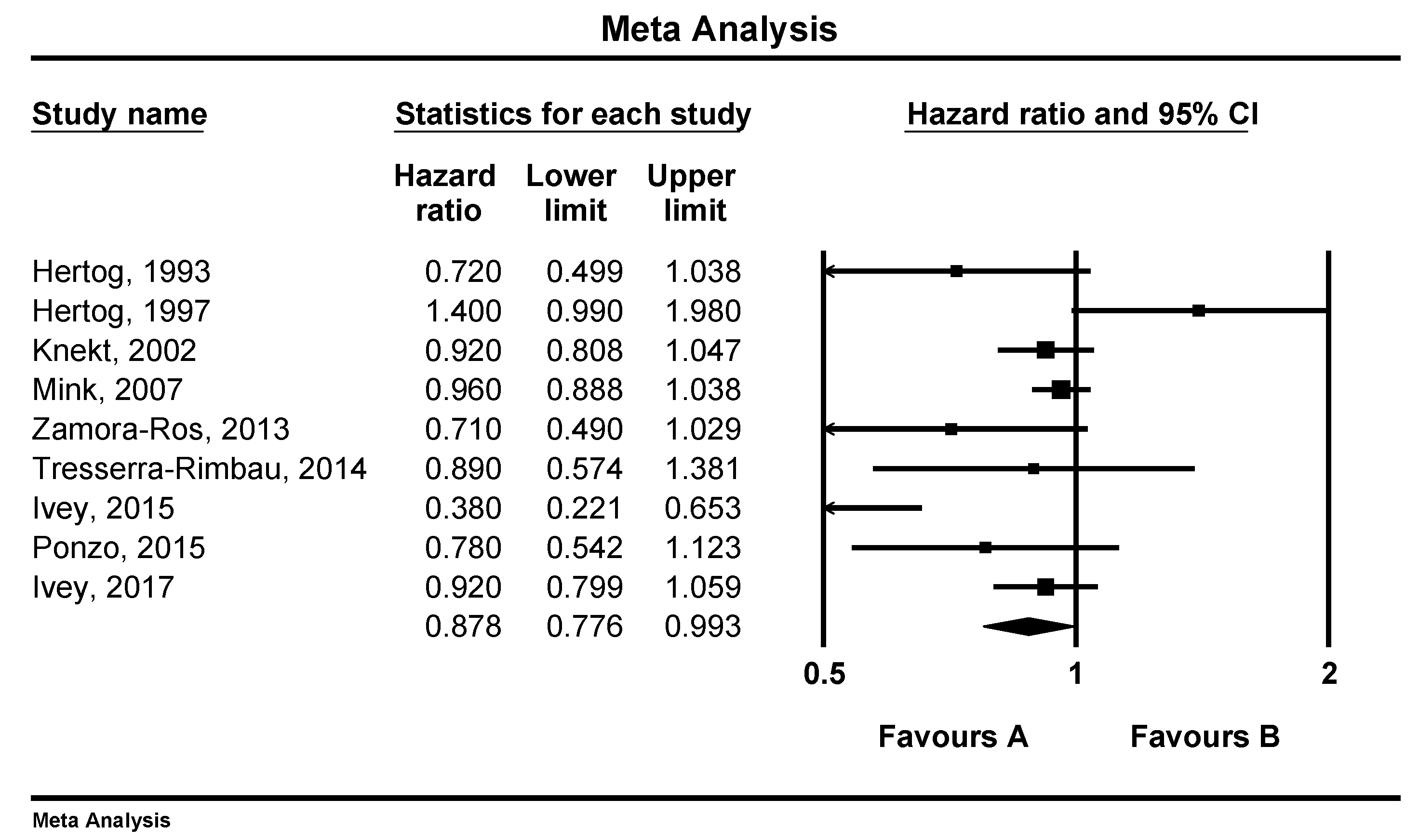
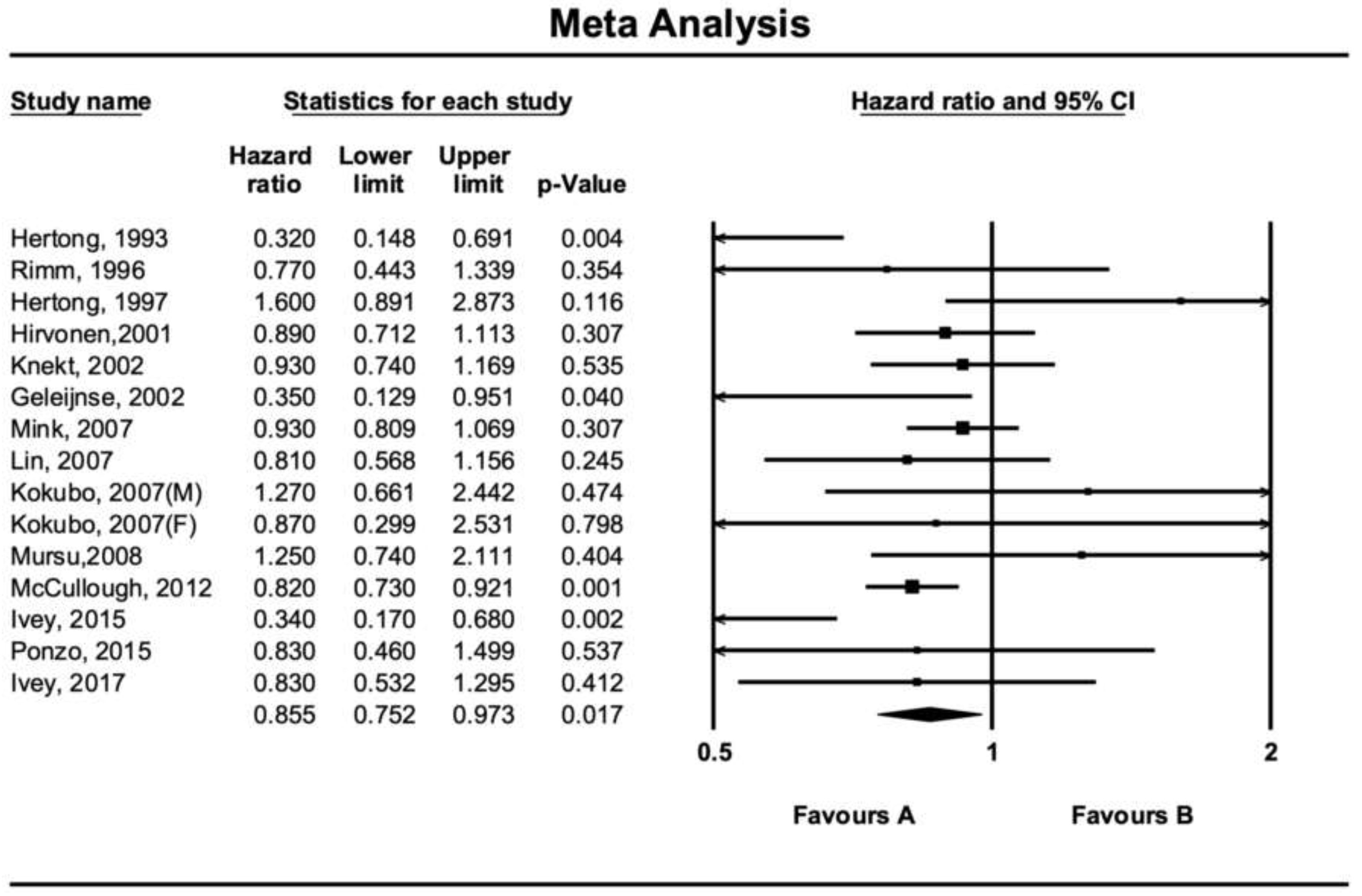
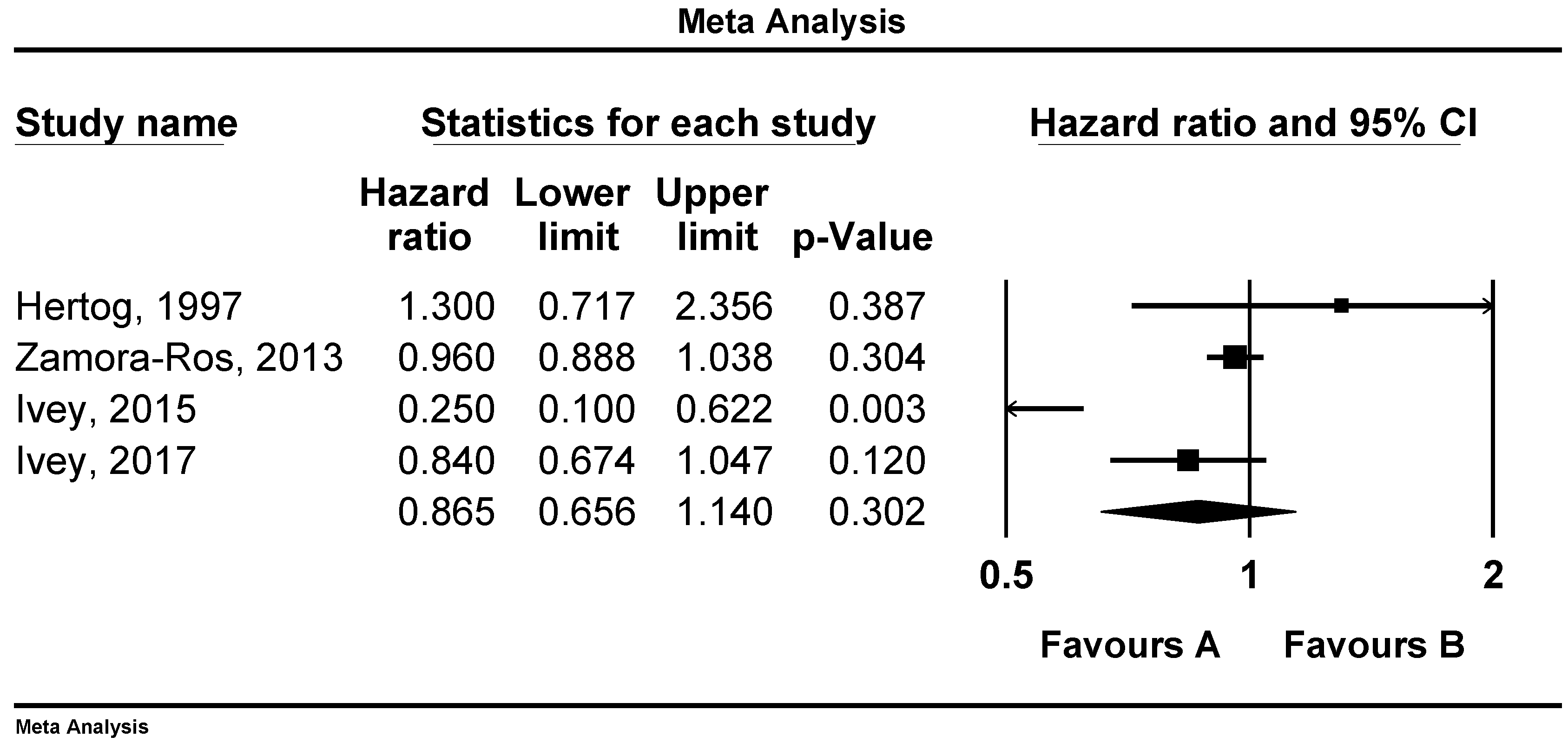
There was a reverse and significant association between flavonoid consumption and all-cause mortality (RR: 0.87, 95%CI = 0.77–0.99, p = 0.039, n = 9 studies, Figure 2). Similar associations were observed between flavonoid intake and CVD mortality (RR: 0.85, 95%CI = 0.75–0.97, p = 0.017, n = 15 studies, Figure 3), but not with cancer mortality (RR: 0.86, 95%CI = 0.65–1.14, p = 0.302, n = 4 studies, Figure 4).
3.2. Sensitivity Analysis
In the leave-one-out sensitivity analyses, the pooled effect estimates remained similar for the effect of flavonoid intake on total (RR: 0.87, 95%CI = 0.77–0.99), CVD (RR: 0.85, 95%CI = 0.75–0.97) and cancer (RR: 0.86, 95%CI = 0.65–1.14) mortality.
3.3. Publication Bias
Visual examination of the funnel plot symmetry showed no publication bias for the association between flavonoid intake and total mortality. Similarly, the Egger’s linear regression (intercept = −1.30, two-tailed p = 0.170) indicated the absence of publication bias. After using the ‘trim and fill’ correction to adjust the effect size for potential publication bias, there were no potentially missing studies in the funnel plot. According to the ‘fail-safe N’ test, 20 studies would be needed for the RR to become non-significant (p > 0.05).
4. Discussion
In the present study, we evaluated the impact of flavonoid intake on total and cause-specific (CVD and cancer) mortality. Pooled data from observational prospective studies showed a significant and negative relationship between flavonoid intake and the risk of all-cause and CVD mortality.
Previous studies on flavonoid consumption and mortality have reported conflicting findings. Our results are in agreement with previous meta-analyses of randomized controlled trials (RCTs) and observational studies on flavonoids, suggesting that their intake might be protective against CVD, cancer and total mortality [5,29,30,31]. Furthermore, consuming fruits and vegetables (the main source of flavonoids) has been associated with a decreased risk of mortality in a meta-analysis [32]. Flavan-3-ols (from cocoa products and green tea), as well as anthocyanins (from berry fruits), were related to a reduced risk of CVD [33,34]. In addition, wine and beer (one of the main source of flavonoids) consumption have been reported to have a J-shaped relationship with CV-related outcomes; the degrees of potential protection by the phenolic or alcoholic content remain unclear [35]. Studies on soy products (rich in isoflavones) and mortality are scarce, but a few available investigations reported no significant association [36,37]. With regard to the impact of flavonoids on CV risk factors, meta-analyses of RCTs suggest that the benefits related to green tea and cocoa products (main sources of flavan-3-ols) was due to a reduction in LDL-C and improvements in endothelial function and insulin sensitivity [33,38]. Flavonoid intake has also been inversely associated with hypertension [39].
In contrast with our findings, another study (n = 93,145 young and middle-aged US women in the NHS-II) found an insignificant relationship between total-flavonoid intake and risk of all-cause mortality [20], a finding similar to the Iowa Women’s’ Health Study [11]. The authors of the NHS-II commented that the lack of any beneficial effect of flavonoids on CVD may be due to the cohort characteristics itself, namely the low CVD mortality rate in this middle-aged female population [20]. It should be noted that the complexity of the methods assessing flavonoid intake (total or specific), as well as regional differences in the food composition of dietary flavonoids [16], shaping the pattern of over 4000 different flavonoid compounds consumed on a daily basis [40], may have contributed to the inconsistent results. Furthermore, data on these differences in the food sources of flavonoids and the methods used to estimate total or specific flavonoid intake were not always available. A meta-analysis including 10 studies reported an inverse relationship between flavonoid intake with total mortality (RR: 0.82, 95% 95%CI: 0.72–0.92), with no significant association between flavonoid consumption and CVD mortality (RR: 0.85; 95%CI: 0.70–1.03) [21]. Of note, the number of studies evaluating CVD death in this meta-analysis was only five [22].
Several possible mechanisms through which flavonoids may benefit health and decrease mortality risk have been suggested [41,42,43]; the basic pathways involve their antioxidant and anti-inflammatory actions [44,45]. Flavonoids inhibit several processes implicated in disease progression, such as oxidative stress and inflammation, that are the main determinants of CVD [45]. Based on the in vitro data, flavonoids can decrease oxidative damage through free radical scavenging activity [46]. Furthermore, non-human studies reported that high flavonoid intake was related to low levels of established biomarkers of inflammation such as the nuclear factor kappa-B (NF-kB) and C-reactive protein [47]. We have previously reported a detrimental impact of inflammation and oxidative stress on cardiometabolic risk factors [48,49,50,51,52]. We suggested that flavonoids may also prevent CVD via (1) affecting endothelial function and vascular homeostasis with the production of factors that act locally in the vessel wall and lumen, e.g., prostacyclin, nitric oxide and endothelin; (2) exerting antifibrotic effects and regulating fibrinolytic factors, e.g., the tissue plasminogen activator and plasminogen activator inhibitor-1; and (3) affecting platelet aggregation and coagulation by influencing the production of adhesion molecules and inflammatory cytokines [44]. Nevertheless, theses mechanisms need to be further investigated in human studies.
Our non-significant results regarding the link between flavonoids intake and cancer mortality may be attributed, at least partly, to the small number of studies. However, flavonoids were reported to protect against cancer by a direct inhibition of oxidative stress and damage [53]. Moreover, flavonoids can exert anti-proliferative, anti-angiogenic and anti-metastatic properties by modulating several receptors and enzymes in several signal transduction pathways related to cellular proliferation, differentiation and apoptosis [53]. Overall, in vitro evidence supports the potential role of dietary flavonoids as protective compounds, but further observational studies and RCTs are needed to confirm the associations of flavonoid intake with all-cause, CVD and cancer mortality found in the present study, as well as to elucidate the underlying mechanisms of these links.
Consistent with our findings, previous meta-analyses highlighted possible negative associations between flavonoid intake and incidence of certain cancers, such as breast [29,54], prostate [55], lung [55], stomach and colorectal cancer [56], as well as smoking-related cancer [30]. In contrast, the link between total cancer mortality and flavonoid consumption has been rarely (four studies) investigated [7,16,17,20]. In one study, a strong inverse association between flavonoid intake and all-cancer mortality was observed (RR = 0.25, 95% CI: 0.10, 0.62) [17], but the other three studies showed non-significant correlations [7,16,20]. The protective effects of flavonoids on cancer risk may be explained by several mechanisms [57,58]. Although flavonoids, mainly isoflavones, are mostly characterized by their weak estrogenic activity, they also exert several other biologic actions that might influence cancer risk, such as antioxidant, anti-proliferative [59] and anti-angiogenic properties [60], together with the capacity to inhibit cytokines, growth factors, and several enzymes [61]. For example, flavonoids can effectively reduce various types of oxidants [62], subsequently reducing cancer risk. The direct antioxidant activities of dietary flavonoids may not be the only explanation for their protection against cancer mortality [63,64]. Another pathway involves the impact of flavonoids on the regulation of enzymes. Carcinogens are metabolized to more active forms by phase I enzymes such as the cytochrome P450 (CYP); the active forms are subsequently detoxified by phase II enzymes such as the UDP-glucuronyl transferase, glutathione S-transferase, and quinone reductase [65]. Flavonoids can inactivate phase I and phase II enzymes [65]. Therefore, flavonoids may exert anticancer effects, which could be influenced by established risk factors for cancer, such as alcohol consumption [66], energy intake, smoking, menopausal status and the use of hormonal replacement therapy [67].
Nevertheless, we cannot be certain that the inverse association between flavonoid consumption and CVD, cancer and all-cause mortality is casual, representing the effect of flavonoids only. In the present study, our model was adjusted for the main compounds of the diet, including fiber, protein, fat and carbohydrates. This adjustment attenuated our results but there was still an inverse link between flavonoid consumption, total, CVD and cancer mortality, thus highlighting the protective effect of flavonoids on the risk of death.
Study Strengths and Limitations
The present study has strengths and limitations. A very low level of heterogeneity of the studies included to the meta-analysis was found, highlighting the validity of our results. Since the majority of the studies assessed flavonoid intake by food frequency questionnaires and flavonoids are present in several different foods, some misclassification of flavonoid consumption is inevitable. However, this misclassification could be non-differential and bias our results towards the null. Therefore, the pooled RR of the relationship between flavonoid intake and mortality could have been underestimated rather than overestimated. Secondly, we cannot rule out the possibility that unmeasured or residual confounding (characteristic of original studies) might have affected the observed associations, although we controlled for potential confounding variables with the use of RRs. Furthermore, the reliability of the available data may have been affected by (1) a small number of cases in some studies, possibly affecting the statistical power of the analyses; (2) a single baseline assessment of dietary intake, with a lack of specific information over time related to mortality; and (3) a lack of data on the associations between different flavonoid types and causes of mortality. Finally, some of the included studies involved specific groups of individuals, limiting the generalizability of these results to the general population [11].
5. Conclusions
Our findings highlighted the potential protective role of flavonoids against total, cancer and CVD mortality. These results further support the recommendations for flavonoid-rich foods intake to prevent cardiovascular diseases and cancers. Due to the potentially different effects of flavonoids, recommendations should also highlight the importance of dietary variety, including diverse flavonoid sources. Further research is required to establish the specific role of individual flavonoid classes as well as the quantities needed to be consumed to achieve health benefits.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6643/12/8/2350/s1. Table S1: Full search terms and strategy for papers indexed in PUBMED, Table S2: Newcastle – Ottawa Quality Assessment Scale Cohort Studies, Table S3: Quality assessment of cohort studies on flavonoid intake, all-cause and cause-specific mortality.
Author Contributions
Conceptualization, M.M. and M.B.; methodology, M.M.; software, M.M.; validation, M.M., N.K. and M.B.; formal analysis, M.M.; investigation, M.M., N.K. and M.B.; resources, M.M., N.K. and M.B.; data curation, M.M., N.K. and M.B.; writing—original draft preparation, M.M., N.K. and M.B.; writing—review and editing, M.M., N.K. and M.B.; visualization, M.M., N.K. and M.B.; supervision, M.M., N.K. and M.B.; project administration, M.M., N.K. and M.B.; funding acquisition, M.M., N.K. and M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
N.K. has given talks, attended conferences and participated in trials sponsored by Angelini, Astra Zeneca, Bausch Health, Boehringer Ingelheim, Elpen, Mylan, NovoNordisk, Sanofi, Servier and WinMedica. The other authors have no conflict of interest to declare.
References
- Roth, G.A.; Johnson, C.O.; Abate, K.H.; Abd-Allah, F.; Ahmed, M.; Alam, K.; Alam, T.; Alvis-Guzman, N.; Ansari, H.; Arnlov, J.; et al. The Burden of Cardiovascular Diseases Among US States, 1990–2016. JAMA Cardiol. 2018, 3, 375–389. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am. J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertog, M.G.; Feskens, E.J.; Hollman, P.C.; Katan, M.B.; Kromhout, D. Dietary antioxidant flavonoids and risk of coronary heart disease: The Zutphen Elderly Study. Lancet 1993, 342, 1007–1011. [Google Scholar] [CrossRef]
- Kim, Y.; Je, Y. Flavonoid intake and mortality from cardiovascular disease and all causes: A meta-analysis of prospective cohort studies. Clin. Nutr. ESPEN 2017, 20, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Katan, M.B.; Ascherio, A.; Stampfer, M.J.; Willett, W.C. Relation between intake of flavonoids and risk for coronary heart disease in male health professionals. Ann. Intern. Med. 1996, 125, 384–389. [Google Scholar] [CrossRef]
- Hertog, M.G.; Sweetnam, P.M.; Fehily, A.M.; Elwood, P.C.; Kromhout, D. Antioxidant flavonols and ischemic heart disease in a Welsh population of men: The Caerphilly Study. Am. J. Clin. Nutr. 1997, 65, 1489–1494. [Google Scholar] [CrossRef]
- Hirvonen, T.; Pietinen, P.; Virtanen, M.; Ovaskainen, M.L.; Hakkinen, S.; Albanes, D.; Virtamo, J. Intake of flavonols and flavones and risk of coronary heart disease in male smokers. Epidemiology 2001, 12, 62–67. [Google Scholar] [CrossRef]
- Knekt, P.; Kumpulainen, J.; Jarvinen, R.; Rissanen, H.; Heliovaara, M.; Reunanen, A.; Hakulinen, T.; Aromaa, A. Flavonoid intake and risk of chronic diseases. Am. J. Clin. Nutr. 2002, 76, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Geleijnse, J.M.; Launer, L.J.; Van der Kuip, D.A.; Hofman, A.; Witteman, J.C. Inverse association of tea and flavonoid intakes with incident myocardial infarction: The Rotterdam Study. Am. J. Clin. Nutr. 2002, 75, 880–886. [Google Scholar] [CrossRef]
- Mink, P.J.; Scrafford, C.G.; Barraj, L.M.; Harnack, L.; Hong, C.P.; Nettleton, J.A.; Jacobs, D.R., Jr. Flavonoid intake and cardiovascular disease mortality: A prospective study in postmenopausal women. Am. J. Clin. Nutr. 2007, 85, 895–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Rexrode, K.M.; Hu, F.; Albert, C.M.; Chae, C.U.; Rimm, E.B.; Stampfer, M.J.; Manson, J.E. Dietary intakes of flavonols and flavones and coronary heart disease in US women. Am. J. Epidemiol. 2007, 165, 1305–1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokubo, Y.; Iso, H.; Ishihara, J.; Okada, K.; Inoue, M.; Tsugane, S. Association of dietary intake of soy, beans, and isoflavones with risk of cerebral and myocardial infarctions in Japanese populations: The Japan Public Health Center-based (JPHC) study cohort I. Circulation 2007, 116, 2553–2562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mursu, J.; Voutilainen, S.; Nurmi, T.; Tuomainen, T.P.; Kurl, S.; Salonen, J.T. Flavonoid intake and the risk of ischaemic stroke and CVD mortality in middle-aged Finnish men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Br. J. Nutr. 2008, 100, 890–895. [Google Scholar] [CrossRef] [Green Version]
- McCullough, M.L.; Peterson, J.J.; Patel, R.; Jacques, P.F.; Shah, R.; Dwyer, J.T. Flavonoid intake and cardiovascular disease mortality in a prospective cohort of US adults. Am. J. Clin. Nutr. 2012, 95, 454–464. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Jimenez, C.; Cleries, R.; Agudo, A.; Sanchez, M.J.; Sanchez-Cantalejo, E.; Molina-Montes, E.; Navarro, C.; Chirlaque, M.D.; Maria Huerta, J.; et al. Dietary flavonoid and lignan intake and mortality in a Spanish cohort. Epidemiology 2013, 24, 726–733. [Google Scholar] [CrossRef]
- Ivey, K.L.; Hodgson, J.M.; Croft, K.D.; Lewis, J.R.; Prince, R.L. Flavonoid intake and all-cause mortality. Am. J. Clin. Nutr. 2015, 101, 1012–1020. [Google Scholar] [CrossRef] [Green Version]
- Tresserra-Rimbau, A.; Rimm, E.B.; Medina-Remon, A.; Martinez-Gonzalez, M.A.; Lopez-Sabater, M.C.; Covas, M.I.; Corella, D.; Salas-Salvado, J.; Gomez-Gracia, E.; Lapetra, J.; et al. Polyphenol intake and mortality risk: A re-analysis of the PREDIMED trial. BMC Med. 2014, 12, 77. [Google Scholar] [CrossRef] [Green Version]
- Ponzo, V.; Goitre, I.; Fadda, M.; Gambino, R.; De Francesco, A.; Soldati, L.; Gentile, L.; Magistroni, P.; Cassader, M.; Bo, S. Dietary flavonoid intake and cardiovascular risk: A population-based cohort study. J. Transl. Med. 2015, 13, 218. [Google Scholar] [CrossRef] [Green Version]
- Ivey, K.L.; Jensen, M.K.; Hodgson, J.M.; Eliassen, A.H.; Cassidy, A.; Rimm, E.B. Association of flavonoid-rich foods and flavonoids with risk of all-cause mortality. Br. J. Nutr. 2017, 117, 1470–1477. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.M.; Liu, Y.J.; Huang, Y.; Yu, H.J.; Yuan, S.; Tang, B.W.; Wang, P.G.; He, Q.Q. Dietary total flavonoids intake and risk of mortality from all causes and cardiovascular disease in the general population: A systematic review and meta-analysis of cohort studies. Mol. Nutr. Food Res. 2017, 61, 1601003. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferretti, G.; Bacchetti, T.; Sahebkar, A. Effect of statin therapy on paraoxonase-1 status: A systematic review and meta-analysis of 25 clinical trials. Prog. Lipid Res. 2015, 60, 50–73. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A. Are curcuminoids effective C-reactive protein-lowering agents in clinical practice? Evidence from a meta-analysis. Phytother. Res. PTR 2014, 28, 633–642. [Google Scholar] [CrossRef]
- Sahebkar, A.; Serban, M.C.; Mikhailidis, D.P.; Toth, P.P.; Muntner, P.; Ursoniu, S.; Mosterou, S.; Glasser, S.; Martin, S.S.; Jones, S.R.; et al. Head-to-head comparison of statins versus fibrates in reducing plasma fibrinogen concentrations: A systematic review and meta-analysis. Pharmacol. Res. 2016, 103, 236–252. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Metaanalysis (Vers. 2); Biostat. Inc.: Englewood Cliffs, NJ, USA, 2005. [Google Scholar]
- Hui, C.; Qi, X.; Qianyong, Z.; Xiaoli, P.; Jundong, Z.; Mantian, M. Flavonoids, flavonoid subclasses and breast cancer risk: A meta-analysis of epidemiologic studies. PLoS ONE 2013, 8, e54318. [Google Scholar] [CrossRef]
- Woo, H.D.; Kim, J. Dietary flavonoid intake and smoking-related cancer risk: A meta-analysis. PLoS ONE 2013, 8, e75604. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Micek, A.; Godos, J.; Pajak, A.; Sciacca, S.; Galvano, F.; Giovannucci, E.L. Dietary Flavonoid and Lignan Intake and Mortality in Prospective Cohort Studies: Systematic Review and Dose-Response Meta-Analysis. Am. J. Epidemiol. 2017, 185, 1304–1316. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ Clin. Res. Ed. 2014, 349, g4490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrime, M.G.; Bauer, S.R.; McDonald, A.C.; Chowdhury, N.H.; Coltart, C.E.; Ding, E.L. Flavonoid-rich cocoa consumption affects multiple cardiovascular risk factors in a meta-analysis of short-term studies. J. Nutr. 2011, 141, 1982–1988. [Google Scholar] [CrossRef] [PubMed]
- van Dam, R.M.; Naidoo, N.; Landberg, R. Dietary flavonoids and the development of type 2 diabetes and cardiovascular diseases: Review of recent findings. Curr. Opin. Lipidol. 2013, 24, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, S.; Di Castelnuovo, A.; Donati, M.B.; Iacoviello, L.; de Gaetano, G. Wine, beer or spirit drinking in relation to fatal and non-fatal cardiovascular events: A meta-analysis. Eur. J. Epidemiol. 2011, 26, 833–850. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Takatsuka, N.; Shimizu, H. Soy and fish oil intake and mortality in a Japanese community. Am. J. Epidemiol. 2002, 156, 824–831. [Google Scholar] [CrossRef]
- Yamasaki, K.; Kayaba, K.; Ishikawa, S. Soy and Soy Products Intake, All-Cause Mortality, and Cause-Specific Mortality in Japan: The Jichi Medical School Cohort Study. Asia-Pac. J. Public Health 2015, 27, 531–541. [Google Scholar] [CrossRef]
- Kim, A.; Chiu, A.; Barone, M.K.; Avino, D.; Wang, F.; Coleman, C.I.; Phung, O.J. Green tea catechins decrease total and low-density lipoprotein cholesterol: A systematic review and meta-analysis. J. Am. Diet. Assoc. 2011, 111, 1720–1729. [Google Scholar] [CrossRef]
- Cassidy, A.; O’Reilly, E.J.; Kay, C.; Sampson, L.; Franz, M.; Forman, J.P.; Curhan, G.; Rimm, E.B. Habitual intake of flavonoid subclasses and incident hypertension in adults. Am. J. Clin. Nutr. 2011, 93, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Ruel, G.; Couillard, C. Evidences of the cardioprotective potential of fruits: The case of cranberries. Mol. Nutr. Food Res. 2007, 51, 692–701. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Colletti, A.; Bajraktari, G.; Descamps, O.; Djuric, D.M.; Ezhov, M.; Fras, Z.; Katsiki, N.; Langlois, M.; Latkovskis, G.; et al. Lipid-lowering nutraceuticals in clinical practice: Position paper from an International Lipid Expert Panel. Nutr. Rev. 2017, 75, 731–767. [Google Scholar] [CrossRef]
- Giglio, R.V.; Patti, A.M.; Cicero, A.F.G.; Lippi, G.; Rizzo, M.; Toth, P.P.; Banach, M. Polyphenols: Potential Use in the Prevention and Treatment of Cardiovascular Diseases. Curr. Pharm. Des. 2018, 24, 239–258. [Google Scholar] [CrossRef] [PubMed]
- Michalska, M.; Gluba, A.; Mikhailidis, D.P.; Nowak, P.; Bielecka-Dabrowa, A.; Rysz, J.; Banach, M. The role of polyphenols in cardiovascular disease. Med. Sci. Monit. 2010, 16, Ra110–Ra119. [Google Scholar] [PubMed]
- Vita, J.A. Polyphenols and cardiovascular disease: Effects on endothelial and platelet function. Am. J. Clin. Nutr. 2005, 81, 292s–297s. [Google Scholar] [CrossRef]
- Visioli, F.; Davalos, A. Polyphenols and cardiovascular disease: A critical summary of the evidence. Mini Rev. Med. Chem. 2011, 11, 1186–1190. [Google Scholar]
- Middleton, E., Jr.; Kandaswami, C.; Theoharides, T.C. The effects of plant flavonoids on mammalian cells: Implications for inflammation, heart disease, and cancer. Pharmacol. Rev. 2000, 52, 673–751. [Google Scholar] [PubMed]
- Wallace, T.C. Anthocyanins in cardiovascular disease. Adv. Nutr. 2011, 2, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazidi, M.; Kengne, A.P.; Mikhailidis, D.P.; Toth, P.P.; Ray, K.K.; Banach, M. Dietary food patterns and glucose/insulin homeostasis: A cross-sectional study involving 24,182 adult Americans. Lipids Health Dis. 2017, 16, 192. [Google Scholar] [CrossRef] [Green Version]
- Mazidi, M.; Gao, H.K.; Kengne, A.P. Inflammatory Markers Are Positively Associated with Serum trans-Fatty Acids in an Adult American Population. J. Nutr. Metab. 2017, 2017, 3848201. [Google Scholar] [CrossRef] [Green Version]
- Mazidi, M.; Karimi, E.; Rezaie, P.; Ferns, G.A. Effects of conjugated linoleic acid supplementation on serum C-reactive protein: A systematic review and meta-analysis of randomized controlled trials. Cardiovasc. Ther. 2017, 35. [Google Scholar] [CrossRef]
- Mazidi, M.; Gao, H.K.; Vatanparast, H.; Kengne, A.P. Impact of the dietary fatty acid intake on C-reactive protein levels in US adults. Medicine 2017, 96, e5736. [Google Scholar] [CrossRef]
- Mazidi, M.; Kengne, A.P.; Mikhailidis, D.P.; Cicero, A.F.; Banach, M. Effects of selected dietary constituents on high-sensitivity C-reactive protein levels in U.S. adults. Ann. Med. 2017, 50, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ravishankar, D.; Rajora, A.K.; Greco, F.; Osborn, H.M. Flavonoids as prospective compounds for anti-cancer therapy. Int. J. Biochem. Cell Biol. 2013, 45, 2821–2831. [Google Scholar] [CrossRef] [PubMed]
- van Die, M.D.; Bone, K.M.; Williams, S.G.; Pirotta, M.V. Soy and soy isoflavones in prostate cancer: A systematic review and meta-analysis of randomized controlled trials. BJU Int. 2014, 113, E119–E130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.H.; Liu, Z. Soy food consumption and lung cancer risk: A meta-analysis using a common measure across studies. Nutr. Cancer 2013, 65, 625–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, H.D.; Kim, J. Dietary flavonoid intake and risk of stomach and colorectal cancer. World Gastroenterol. 2013, 19, 1011–1019. [Google Scholar] [CrossRef]
- Yang, P.M.; Tseng, H.H.; Peng, C.W.; Chen, W.S.; Chiu, S.J. Dietary flavonoid fisetin targets caspase-3-deficient human breast cancer MCF-7 cells by induction of caspase-7-associated apoptosis and inhibition of autophagy. Int. J. Oncol. 2012, 40, 469–478. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.; Spagnuolo, C.; Tedesco, I.; Bilotto, S.; Russo, G.L. The flavonoid quercetin in disease prevention and therapy: Facts and fancies. Biochem. Pharmacol. 2012, 83, 6–15. [Google Scholar] [CrossRef]
- Thomas, C.M.; Wood, R.C., 3rd; Wyatt, J.E.; Pendleton, M.H.; Torrenegra, R.D.; Rodriguez, O.E.; Harirforoosh, S.; Ballester, M.; Lightner, J.; Krishnan, K.; et al. Anti-neoplastic activity of two flavone isomers derived from Gnaphalium elegans and Achyrocline bogotensis. PLoS ONE 2012, 7, e39806. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.K.; Singh, A.P.; Singh, R.K.; Demartino, A.; Brard, L.; Vorsa, N.; Lange, T.S.; Moore, R.G. Anti-angiogenic activity of cranberry proanthocyanidins and cytotoxic properties in ovarian cancer cells. Int. J. Oncol. 2012, 40, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Toledo, A.C.; Sakoda, C.P.; Perini, A.; Pinheiro, N.M.; Magalhaes, R.M.; Grecco, S.; Tiberio, I.F.; Camara, N.O.; Martins, M.A.; Lago, J.H.; et al. Flavonone treatment reverses airway inflammation and remodelling in an asthma murine model. Br. J. Pharmacol. 2013, 168, 1736–1749. [Google Scholar] [CrossRef] [Green Version]
- Bravo, L. Polyphenols: Chemistry, dietary sources, metabolism, and nutritional significance. Nutr. Rev. 1998, 56, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Hollman, P.C.; Cassidy, A.; Comte, B.; Heinonen, M.; Richelle, M.; Richling, E.; Serafini, M.; Scalbert, A.; Sies, H.; Vidry, S. The biological relevance of direct antioxidant effects of polyphenols for cardiovascular health in humans is not established. J. Nutr. 2011, 141, 989s–1009s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, J.N., 3rd; Colantonio, L.D.; Howard, G.; Safford, M.M.; Banach, M.; Reynolds, K.; Cushman, M.; Muntner, P. Healthy lifestyle factors and incident heart disease and mortality in candidates for primary prevention with statin therapy. Int. J. Cardiol. 2016, 207, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Moon, Y.J.; Wang, X.; Morris, M.E. Dietary flavonoids: Effects on xenobiotic and carcinogen metabolism. Toxicol. In Vitro 2006, 20, 187–210. [Google Scholar] [CrossRef]
- Touvier, M.; Druesne-Pecollo, N.; Kesse-Guyot, E.; Andreeva, V.A.; Fezeu, L.; Galan, P.; Hercberg, S.; Latino-Martel, P. Dual association between polyphenol intake and breast cancer risk according to alcohol consumption level: A prospective cohort study. Breast Cancer Res. Treat. 2013, 137, 225–236. [Google Scholar] [CrossRef]
- Luo, J.; Gao, Y.T.; Chow, W.H.; Shu, X.O.; Li, H.; Yang, G.; Cai, Q.; Li, G.; Rothman, N.; Cai, H.; et al. Urinary polyphenols, glutathione S-transferases copy number variation, and breast cancer risk: Results from the Shanghai women’s health study. Mol. Carcinog. 2012, 51, 379–388. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flow chart of literature search for meta-analysis on flavonoid intake with total and cause specific mortality for the studies selection.
Figure 1.
Flow chart of literature search for meta-analysis on flavonoid intake with total and cause specific mortality for the studies selection.
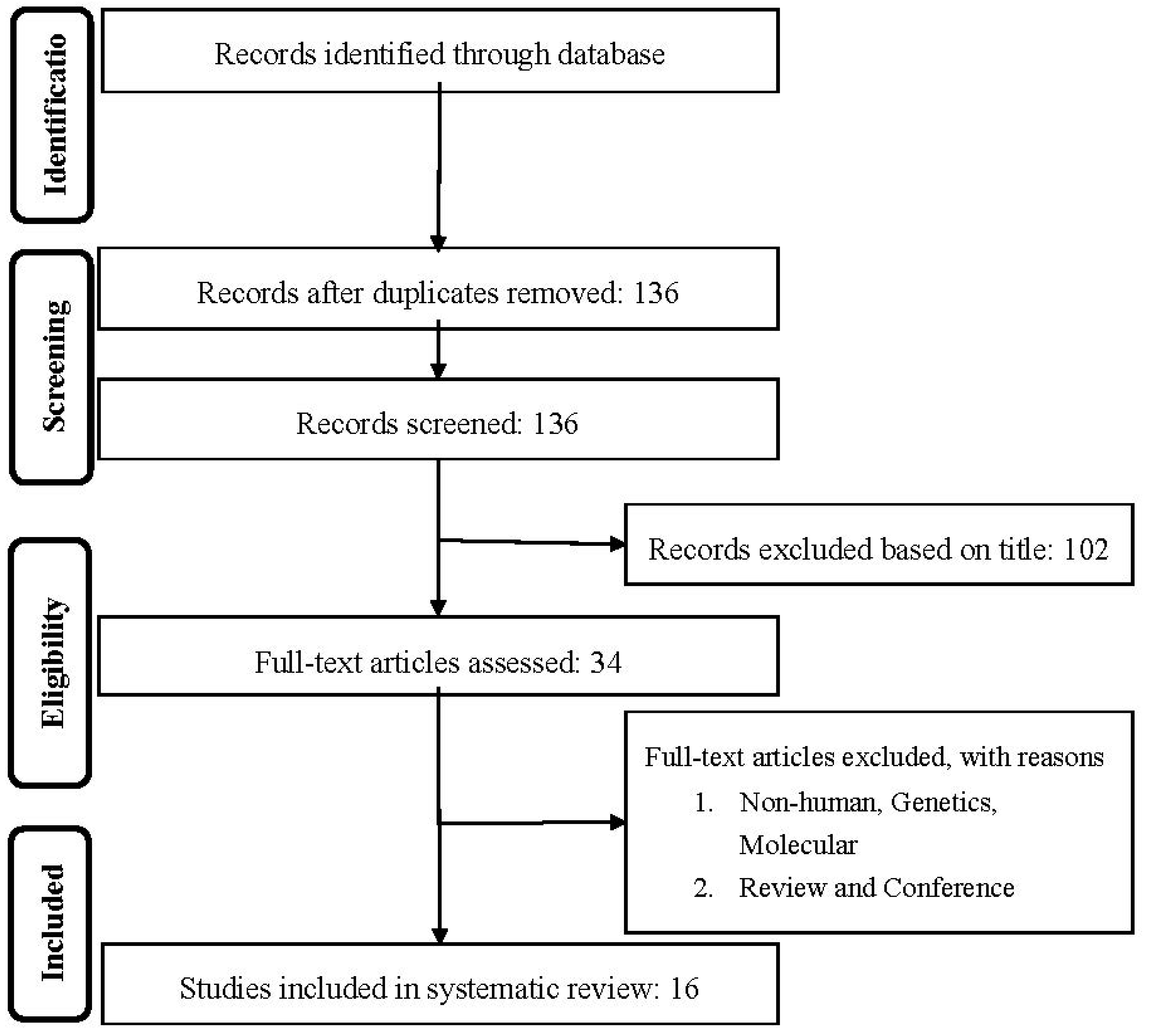
Figure 2.
Forest plot of flavonoid intake and risk of total mortality.
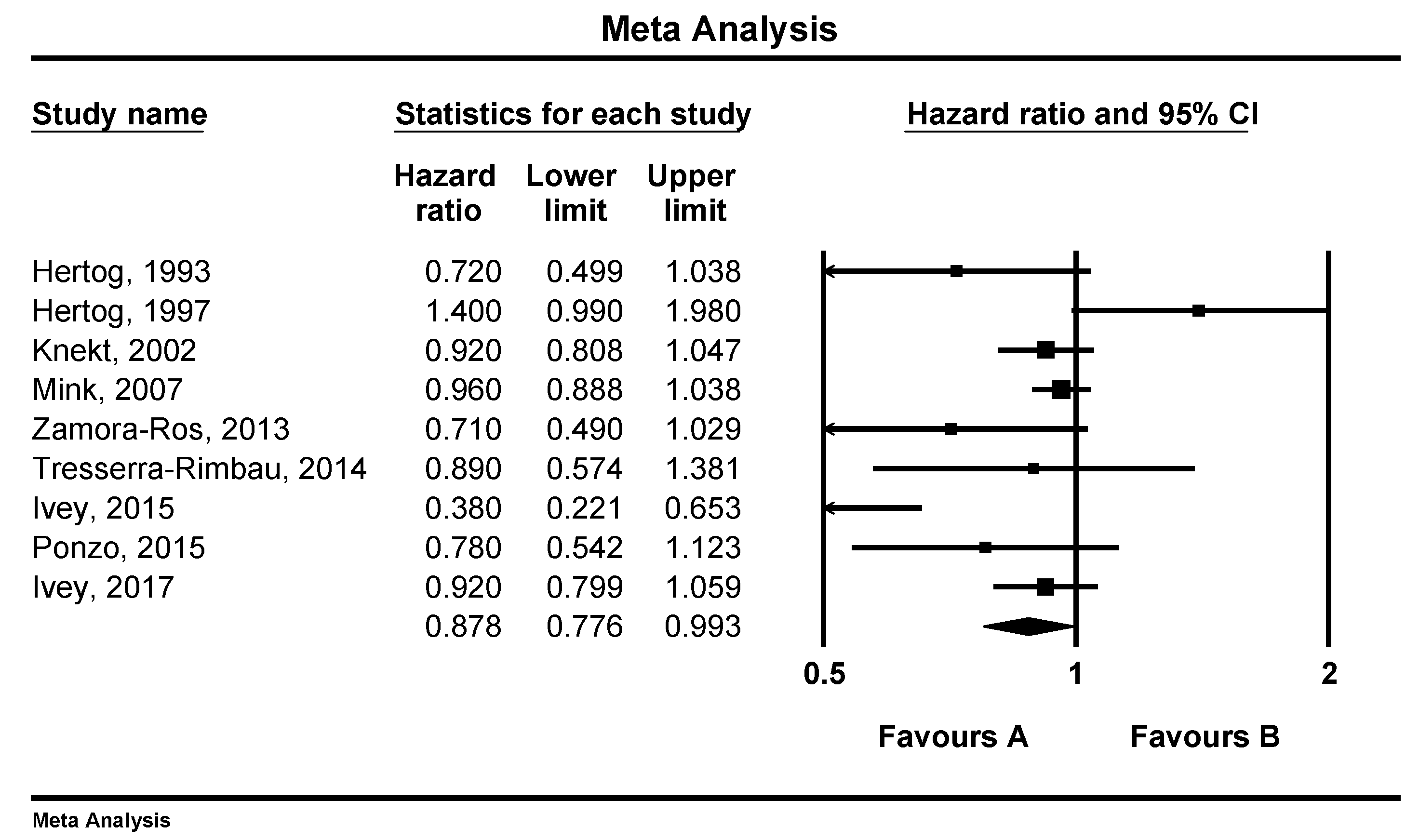
Figure 3.
Forest plot of flavonoid intake and risk of cardiovascular disease mortality.

Figure 4.
Forest plot of flavonoid intake and risk of cancer mortality.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of the 16 prospective cohort studies included in the meta-analysis.
| Author, Year and Reference | Country, Region/Cohort | Men (%) | Mean Age (Years) | Follow-Up Time (Years) | No. of Cases (Outcomes) | No. of Subjects | Outcomes (Mortality) | Main Confounders |
|---|---|---|---|---|---|---|---|---|
| Hertog (1993) [4] | Netherlands, Zutphen Elderly Study | 100 | 65–84 | 5 | 43, 185 | 805 | CHD, All-cause | Age, BMI, smoking, serum total and HDL-C, systolic blood pressure, intake of total energy, saturated fatty acids, cholesterol, alcohol, coffee, vitamin C, vitamin E, beta-carotene, dietary fiber, history of MI |
| Rimm (1996) [6] | USA, Health Professionals follow-up Study | 100 | 40–75 | 6 | 140 | 34,789 | CHD | Age, BMI, smoking, diabetes, profession, hypertension, high cholesterol levels, family history of CHD, intake of vitamin E, alcohol, dietary fiber, carotene and saturated fat |
| Hertog (1997) [7] | UK, Caerphilly study | 100 | 45–59 | 14 | 131, 334 | 1900 | IHD, All-cause | Age, BMI, smoking, systolic blood pressure, serum total cholesterol, history of IHD at baseline, social class, intakes of total energy, alcohol, fat, vitamin C, vitamin E, and beta-carotene |
| Hirvonen (2001) [8] | Finland, Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study | 100 | 50–69 | 6.1 | 815 | 25,372 | CHD | Age, BMI, smoking, systolic and diastolic blood pressure, serum total cholesterol, HDL-C, diabetes, CHD history, marital status, educational level and physical activity |
| Knekt (2002) [9] | Finland, Finnish mobile clinic health examination survey | -- | 54.0 ± 10.6 | 28 | 681, 2085 | 9131 | IHD, All-cause | Age, sex, geographic area, occupation, blood pressure, smoking, serum cholesterol, BMI, diabetes, intakes of energy, cholesterol, saturated fatty acids, fiber, vitamin E, vitamin C and beta-carotene |
| Geleijnse (2002) [10] | Netherlands, Rotterdam Study | 38.3 | >55 | 5.6 | 30 | 4807 | MI | Age, sex, BMI, smoking, education level, daily intakes of alcohol, coffee, polyunsaturated fat, saturated fat, fiber, vitamin E, and total energy |
| Mink (2007) [11] | USA, Iowa Women’s Health Study | 0 | 55–69 | 16 | 2316, 7091 | 34,489 | CVD, All-cause | Age, BMI, waist-to-hip ratio, smoking, energy intake, marital status, education, blood pressure, diabetes, physical activity and estrogen use |
| Lin (2007) [12] | USA, Nurses’ Health Study | 0 | 30–55 | 12 | 324 | 66,360 | CHD | Age, BMI, current smoking, parental history of MI at an age <60 years, history of hypertension, hypercholesterolemia and diabetes, menopausal status, hormone replacement therapy, use of aspirin, multivitamin and vitamin E supplements, physical activity, alcohol consumption and total energy intake |
| Kokubo (2007) [13] | Japan, Japan Public Health Center-Based Study | 25.8 | 40–59 | 12.5 | 1538 | 40,462 | CVD | Age, sex, BMI, smoking, alcohol use, history of hypertension or diabetes, hypolipidemic drugs, education level, sports, dietary intake of fruits, vegetables, fish, salt, and energy |
| Mursu (2008) [14] | Finland, Kuopio Ischemic Heart Disease Risk Factor Study | 100 | 42–60 | 15.2 | 153 | 1950 | CVD | Age, examination years, BMI, systolic blood pressure, hypertension medication, serum HDL-C and LDL-C, serum TAG, maximal oxygen uptake, smoking, CVD in family, diabetes, alcohol intake, energy-adjusted intake of folate and vitamin E, total fat (percentage of energy) and saturated fat intake (percentage of energy) |
| McCullough (2012) [15] | USA, Cancer Prevention Study II Nutrition Cohort | 38.8 | 69.5 | 7 | 2771 | 98,469 | CVD | Age, sex, BMI, smoking, beer and liquor intake, history of hypertension and dyslipidemia, family history of MI, physical activity, energy intake, aspirin use, hormone replacement therapy (in women only) |
| Zamora-Ros (2013) [16] | Spain, EPIC-Spain cohort | 38 | 29–70 | 13.6 | 1915 | 40,622 | All-cause | Age, sex, BMI, education level, physical activity, smoking, lifetime alcohol consumption, total energy, vitamin C and fiber intake |
| Tresserra-Rimbau (2014) [18] | Spain, PREDIMED study | 45.3 | 55–80 | 4.8 | 327 | 7172 | All-cause | Age, smoking, BMI, diabetes, alcohol, total energy intake, physical activity, family history of CVD or cancer, aspirin use, antihypertensive drug use, use of oral hypoglycemic agents, insulin, other medication, intake of protein, saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids and cholesterol |
| Ivey (2015) [17] | Australia, Calcium Intake Fracture Outcome Age Related Extension Study | 0 | >75 | 5 | 78, 129 | 1063 | CVD, All-cause | Age, prevalent CVD and cancer, overweight or obesity, low fruit and vegetable intake, physical inactivity, current cigarette smoking, alcohol consumption |
| Ponzo (2015) [19] | Italy, Local Health Units of the province of Asti | - | 45–64 | 12 | 84, 220 | 1658 | CVD, All-cause | Age, sex, BMI, education, living in a rural area, METs, fiber and saturated fatty acid intakes, alcohol intake, smoking, systolic and diastolic blood pressure, total and HDL-c, fasting glucose, CRP, statin and aspirin use |
| Ivey (2017) [20] | USA, Nurses’ Health Study II. | 0 | 36.1 | 18 | 189, 1894 | 93,145 | CVD, All-cause | Age, BMI, smoking, menopausal status, family history of diabetes, cancer and MI, multivitamin supplement use, aspirin use, race, diabetes, hypercholesterolemia, hypertension, physical activity, energy intake, alcohol consumption and the Alternative Health Eating Index (minus alcohol) score |
CHD: coronary heart disease, CVD: cardiovascular disease, IHD: ischemic heart disease, BMI: body mass index, METs: metabolic equivalents, MI: myocardial infarction, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, TAG: triacylglycerol, CRP: C-reactive protein.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mazidi, M.; Katsiki, N.; Banach, M. A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies. Nutrients 2020, 12, 2350. https://doi.org/10.3390/nu12082350
AMA Style
Mazidi M, Katsiki N, Banach M. A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies. Nutrients. 2020; 12(8):2350. https://doi.org/10.3390/nu12082350
Chicago/Turabian StyleMazidi, Mohsen, Niki Katsiki, and Maciej Banach. 2020. "A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies" Nutrients 12, no. 8: 2350. https://doi.org/10.3390/nu12082350
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.