Consumption of Lactose, Other FODMAPs and Diarrhoea during Adjuvant 5-Fluorouracil Chemotherapy for Colorectal Cancer

Abstract
1. Introduction
2. Materials and Methods
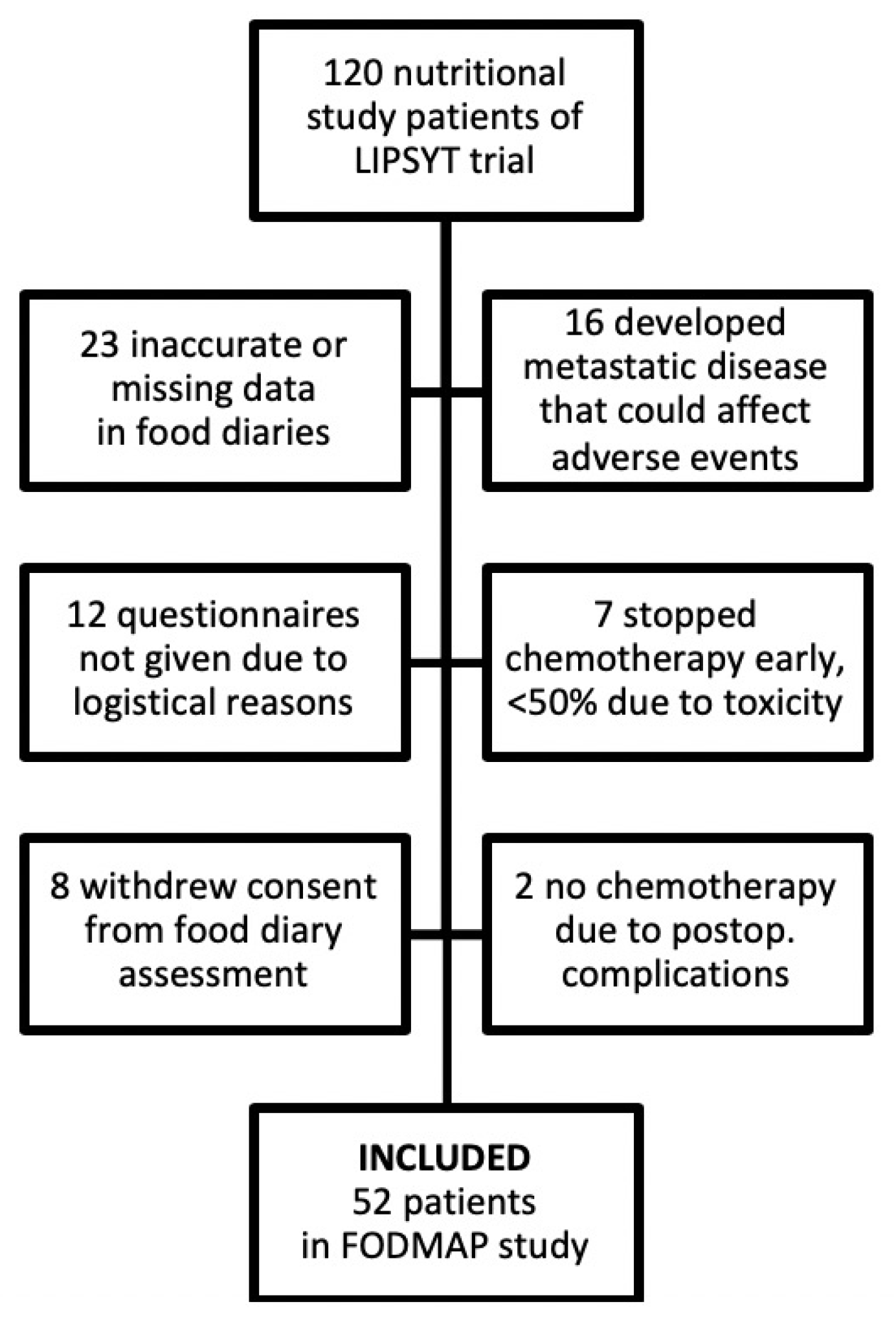
2.1. Subjects and Study Design
2.2. Concurrent Medications, Assessment of Methane Production and Oral Lactose Tolerance Test
2.3. Analysis of Food Diaries
2.4. Assessment of Gastrointestinal Symptoms
2.5. Statistical Analysis
3. Results
3.1. Dietary Intakes
3.2. Association of Dietary Intakes with Gastrointestinal Symptoms
3.3. Association of Patient Characteristics with Gastrointestinal Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Davila, M.; Bresalier, R.S. Gastrointestinal complications of oncologic therapy. Nat. Clin. Pr. Gastroenterol. Hepatol. 2008, 5, 682–696. [Google Scholar] [CrossRef] [PubMed]
- Andreyev, H.J.; Davidson, S.E.; Gillespie, C.; Allum, W.H.; Swarbrick, E. Practice guidance on the management of acute and chronic gastrointestinal problems arising as a result of treatment for cancer. Gut 2012, 61, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Wright, E.M.; Martı́n, M.G.; Turk, E. Intestinal absorption in health and disease—Sugars. Best Pr. Res. Clin. Gastroenterol. 2003, 17, 943–956. [Google Scholar] [CrossRef]
- Gibson, P.R.; Newnham, E.; Barrett, J.S.; Shepherd, S.J.; Muir, J.G. Review article: Fructose malabsorption and the bigger picture. Aliment. Pharmacol. Ther. 2007, 25, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, H.M.; Whelan, K. The low FODMAP diet: Recent advances in understanding its mechanisms and efficacy in IBS. Gut 2017, 66, 1517–1527. [Google Scholar] [CrossRef] [PubMed]
- Osterlund, P.; Ruotsalainen, T.; Peuhkuri, K.; Korpela, R.; Ollus, A.; Ikonen, M.; Joensuu, H.; Elomaa, I. Lactose intolerance associated with adjuvant 5-fluorouracil-based chemotherapy for colorectal cancer. Clin. Gastroenterol. Hepatol. 2004, 2, 696–703. [Google Scholar] [CrossRef]
- Jones, H.F.; Butler, R.N.; Brooks, D.A. Intestinal fructose transport and malabsorption in humans. Am. J. Physiol. Liver Physiol. 2011, 300, G202–G206. [Google Scholar] [CrossRef]
- Gibson, P.R.; Shepherd, S.J. Food Choice as a Key Management Strategy for Functional Gastrointestinal Symptoms. Am. J. Gastroenterol. 2012, 107, 657–666. [Google Scholar] [CrossRef]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome. Gastroenterol. 2014, 146, 67–75.e5. [Google Scholar] [CrossRef]
- Viswanathan, C.; Truong, M.T.; Sagebiel, T.L.; Bronstein, Y.; Vikram, R.; Patnana, M.; Silverman, P.M.; Bhosale, P.R. Abdominal and pelvic complications of nonoperative oncologic therapy. Radiographics 2014, 34, 941–961. [Google Scholar] [CrossRef]
- Larsen, T.; Hausken, T.; Otteraaen Ystad, S.; Hovdenak, N.; Mueller, B.; Lied, G.A. Does the low FODMAP diet improve symptoms of radiation-induced enteropathy? A pilot study. Scand. J. Gastroenterol. 2018, 53, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Osterlund, P.; Ruotsalainen, T.; Korpela, R.; Saxelin, M.; Ollus, A.; Valta, P.; Kouri, M.; Elomaa, I.; Joensuu, H. Lactobacillus supplementation for diarrhoea related to chemotherapy of colorectal cancer: A randomised study. Br. J. Cancer 2007, 97, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Holma, R.; Korpela, R.; Sairanen, U.; Blom, M.; Rautio, M.; Poussa, T.; Saxelin, M.; Österlund, P. Colonic Methane Production Modifies Gastrointestinal Toxicity Associated With Adjuvant 5-Fluorouracil Chemotherapy for Colorectal Cancer. J. Clin. Gastroenterol. 2013, 47, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Gibson, P.R.; Shepherd, S.J. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. J. Gastroenterol. Hepatol. 2010, 25, 252–258. [Google Scholar] [CrossRef]
- Barrett, J.S. Extending Our Knowledge of Fermentable, Short-Chain Carbohydrates for Managing Gastrointestinal Symptoms. Nutr. Clin. Pr. 2013, 28, 300–306. [Google Scholar] [CrossRef]
- Stryker, J.A.; Bartholomew, M. Failure of lactose-restricted diets to prevent radiation-induced diarrhea in patients undergoing whole pelvis irradiation. Int. J. Radiat. Oncol. 1986, 12, 789–792. [Google Scholar] [CrossRef]
- Pettersson, A.; Johansson, B.; Persson, C.; Berglund, A.; Turesson, I. Effects of a dietary intervention on acute gastrointestinal side effects and other aspects of health-related quality of life: A randomized controlled trial in prostate cancer patients undergoing radiotherapy. Radiother. Oncol. 2012, 103, 333–340. [Google Scholar] [CrossRef]
- Forsgård, R.A.; Korpela, R.; Holma, R.; Lindén, J.; Frias, R.; Spillmann, T.; Österlund, P. Intestinal permeability to iohexol as an in vivo marker of chemotherapy-induced gastrointestinal toxicity in Sprague-Dawley rats. Cancer Chemother. Pharmacol. 2016, 78, 863–874. [Google Scholar] [CrossRef]
- Touchefeu, Y.; Montassier, E.; Nieman, K.; Gastinne, T.; Potel, G.; Bruley des Varannes, S.; Le Vacon, F.; de La Cochetière, M.F. Systematic review: The role of the gut microbiota in chemotherapy- or radiation-induced gastrointestinal mucositis–current evidence and potential clinical applications. Aliment. Pharmacol. Ther. 2015, 40, 409–421. [Google Scholar] [CrossRef]
- Zhou, S.-Y.; Gillilland, M.; Wu, X.; Leelasinjaroen, P.; Zhang, G.; Zhou, H.; Ye, B.; Lu, Y.; Owyang, C. FODMAP diet modulates visceral nociception by lipopolysaccharide-mediated intestinal inflammation and barrier dysfunction. J. Clin. Investig. 2017, 128, 267–280. [Google Scholar] [CrossRef]
- Muir, J.G.; Shepherd, S.J.; Rosella, O.; Rose, R.; Barrett, J.S.; Gibson, P.R. Fructan and Free Fructose Content of Common Australian Vegetables and Fruit. J. Agric. Food Chem. 2007, 55, 6619–6627. [Google Scholar] [CrossRef] [PubMed]
- Nencioni, A.; Caffa, I.; Cortellino, S.; Longo, V.D. Fasting and cancer: Molecular mechanisms and clinical application. Nat. Rev. Cancer 2018, 18, 707–719. [Google Scholar] [CrossRef] [PubMed]
- Ravasco, P.; Monteiro-Grillo, I.; Vidal, P.M.; Camilo, M.E. Dietary Counseling Improves Patient Outcomes: A Prospective, Randomized, Controlled Trial in Colorectal Cancer Patients Undergoing Radiotherapy. J. Clin. Oncol. 2005, 23, 1431–1438. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Included Patients (n = 52) | Excluded Patients (n = 68) | |||
|---|---|---|---|---|---|
| No. of Patients | % | No. of Patients | % | P-Value * | |
| Age (years; median [range]) | 59 | 35–74 | 60 | 31–76 | 0.41 |
| Gender | 1.00 | ||||
| Male | 26 | 50 | 35 | 51 | |
| Female | 26 | 50 | 33 | 49 | |
| Lactase deficiency status | 0.26 | ||||
| Normolactasia | 35 | 71 | 49 | 75 | |
| Borderline | 5 | 10 | 2 | 3 | |
| Hypolactasia | 9 | 18 | 14 | 22 | |
| Not available | 3 | 3 | |||
| Methane producer status | 0.58 | ||||
| Producer | 18 | 41 | 20 | 36 | |
| Non-producer | 26 | 59 | 35 | 64 | |
| Not available | 8 | 13 | |||
| Cancer stage | 0.44 | ||||
| Stage II | 9 | 17 | 20 | 29 | |
| Stage III | 36 | 69 | 40 | 59 | |
| Stage IV | 7 | 14 | 8 | 12 | |
| Site of cancer | 0.76 | ||||
| Colon | 32 | 62 | 40 | 59 | |
| Rectum | 20 | 38 | 28 | 41 | |
| Type of surgery | 0.89 | ||||
| Right hemicolectomy | 13 | 25 | 13 | 19 | |
| Left hemicolectomy or sigma Resection | 15 | 29 | 19 | 28 | |
| Rectum resection | 20 | 38 | 29 | 43 | |
| Subtotal colectomy | 4 | 8 | 7 | 10 | |
| Abdominal stoma | 0.38 | ||||
| Yes | 16 | 31 | 16 | 24 | |
| No | 36 | 69 | 52 | 76 | |
| Time since surgery to study entry (weeks; median [range]) | 5 | 2.5–14 | 8 | 4–16 | 0.61 |
| Chemotherapy | 0.87 | ||||
| Mayo regimen | 26 | 50 | 35 | 51 | |
| sLV5FU2 ** | 26 | 50 | 33 | 49 | |
| Pelvic radiotherapy | 0.17 | ||||
| Preoperative short course | 6 | 12 | 2 | 3 | |
| Postoperative chemoradiation | 14 | 27 | 22 | 32 | |
| None | 32 | 61 | 44 | 65 | |
| Type of supplementation | 0.82 | ||||
| Lactobacillus only | 18 | 34 | 23 | 34 | |
| Lactobacillus + fibre | 15 | 29 | 25 | 37 | |
| No supplements | 19 | 37 | 20 | 29 | |
| Diarrhoea * | Constipation | Vomiting | Flatulence | Dyspepsia | Stomatitis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| Consumption of lactose-rich foods † | |||||||||||||
| Cycle I | Low (n = 26) | 6 | 23 | 6 | 23 | 15 | 58 | 12 | 46 | 4 | 15 | 19 | 73 |
| High (n = 26) | 15 | 58 | 6 | 23 | 17 | 65 | 6 | 23 | 7 | 27 | 14 | 54 | |
| Cycle III | Low (n = 26) | 11 | 42 | 8 | 31 | 16 | 62 | 8 | 31 | 6 | 23 | 11 | 42 |
| High (n = 26) | 14 | 54 | 4 | 15 | 14 | 54 | 4 | 15 | 1 | 4 | 19 | 73 | |
| High vs. Low ‡ | OR 95% CI | 2.63 1.09–6.37 | 0.73 0.30–1.78 | 1.00 0.46–2.15 | 0.38 0.15–0.95 | 0.79 0.28–2.22 | 1.24 0.58–2.64 | ||||||
| P-value | 0.03 | 0.48 | 1.00 | 0.04 | 0.65 | 0.58 | |||||||
| Consumption of FODMAP-rich foods § | |||||||||||||
| Cycle I | Low (n = 24) | 9 | 38 | 5 | 21 | 14 | 58 | 8 | 33 | 3 | 13 | 16 | 67 |
| High (n = 28) | 12 | 43 | 7 | 25 | 18 | 64 | 10 | 36 | 8 | 29 | 17 | 61 | |
| Cycle III | Low (n = 26) | 10 | 38 | 8 | 31 | 15 | 58 | 4 | 15 | 4 | 15 | 11 | 42 |
| High (n = 26) | 15 | 58 | 4 | 15 | 15 | 58 | 8 | 31 | 3 | 12 | 19 | 73 | |
| High vs. Low ‡ | OR 95% CI | 1.82 0.72–4.56 | 0.68 0.29–1.64 | 1.07 0.60–1.92 | 1.74 0.67–4.47 | 1.77 0.59–5.32 | 1.65 0.66–4.14 | ||||||
| P-value | 0.20 | 0.39 | 0.81 | 0.25 | 0.31 | 0.28 | |||||||
| Consumption of Foods Rich in * | Diarrhoea † | Constipation | Vomiting | Flatulence | Dyspepsia | Stomatitis | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| Cycle I | None, Lactose Low − FODMAP Low (n = 14) | 3 | 21 | 3 | 21 | 7 | 50 | 7 | 50 | 1 | 7 | 10 | 71 |
| Lactose High − FODMAP Low (n = 10) | 6 | 60 | 2 | 20 | 7 | 70 | 1 | 10 | 2 | 20 | 6 | 60 | |
| Lactose Low − FODMAP High (n = 12) | 3 | 25 | 3 | 25 | 8 | 67 | 5 | 42 | 3 | 25 | 9 | 75 | |
| Lactose High − FODMAP High (n = 16) | 9 | 56 | 4 | 25 | 10 | 63 | 5 | 31 | 5 | 31 | 8 | 50 | |
| Cycle III | None, Lactose Low − FODMAP Low (n = 15) | 4 | 27 | 5 | 33 | 10 | 67 | 4 | 27 | 3 | 20 | 6 | 40 |
| Lactose High − FODMAP Low (n = 11) | 6 | 55 | 3 | 27 | 5 | 45 | 0 | 0 | 1 | 9 | 5 | 45 | |
| Lactose Low − FODMAP High (n = 11) | 7 | 64 | 3 | 27 | 6 | 55 | 4 | 36 | 3 | 27 | 5 | 45 | |
| Lactose High − FODMAP High (n = 15) | 8 | 53 | 1 | 7 | 9 | 60 | 4 | 27 | 0 | 0 | 14 | 93 | |
| Lactose High − FODMAP Low vs. None ‡ | OR 95% CI P-value | 4.16 1.25–13.81 0.02 | 0.89 0.26–3.07 0.85 | 0.76 0.33–1.77 0.53 | 0.10 0.02–0.54 0.01 | 0.93 0.16–5.57 0.94 | 0.95 0.28–3.25 0.94 | ||||||
| Lactose Low − FODMAP High vs. None ‡ | OR 95% CI P-value | 2.59 0.77–8.71 0.13 | 0.80 0.22–2.86 0.73 | 0.85 0.32–2.28 0.75 | 1.35 0.45–3.99 0.59 | 2.16 0.41–11.21 0.36 | 1.34 0.40–4.43 0.63 | ||||||
| Lactose High − FODMAP High vs. None ‡ | OR 95% CI P-value | 4.18 1.28–13.67 0.02 | 0.54 0.18–1.59 0.26 | 1.07 0.49–2.31 0.87 | 0.71 0.22–2.32 0.57 | 1.35 0.29–6.38 0.71 | 1.90 0.65–5.54 0.24 | ||||||
| Diarrhoea * | Flatulence | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P-Value | OR | 95% CI | P-Value | |
| Consumption of foods | ||||||
| Lactose High − FODMAP Low † | 10.08 | 0.85–119.2 | 0.07 | 0.09 | 0.01–1.10 | 0.06 |
| Lactose Low − FODMAP High † | 1.73 | 0.16–18.51 | 0.65 | 0.39 | 0.05–3.11 | 0.37 |
| Lactose High − FODMAP High † | 17.69 | 1.74–179.7 | 0.02 | 0.79 | 0.14–4.55 | 0.79 |
| Covariates: | ||||||
| Chemotherapy regimen (simplified de Gramont vs. Mayo) | - | 0.09 | 0.02–0.51 | 0.01 | ||
| Lactobacillus GG intervention (yes vs. no) | - | - | ||||
| Fibre supplement (yes vs. no) | - | - | ||||
| Baseline lactose intolerance (yes vs. no) | 4.96 | 0.88–28.02 | 0.07 | 4.03 | 0.70–23.22 | 0.12 |
| Presence of stoma (yes vs. no) | - | - | ||||
| Methane-producer status (yes vs. no) | 0.26 | 0.05–1.25 | 0.09 | - | ||
| Postoperative chemoradiation (yes vs. no) | - | - | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holma, R.; Laatikainen, R.; Orell, H.; Joensuu, H.; Peuhkuri, K.; Poussa, T.; Korpela, R.; Österlund, P. Consumption of Lactose, Other FODMAPs and Diarrhoea during Adjuvant 5-Fluorouracil Chemotherapy for Colorectal Cancer. Nutrients 2020, 12, 407. https://doi.org/10.3390/nu12020407
Holma R, Laatikainen R, Orell H, Joensuu H, Peuhkuri K, Poussa T, Korpela R, Österlund P. Consumption of Lactose, Other FODMAPs and Diarrhoea during Adjuvant 5-Fluorouracil Chemotherapy for Colorectal Cancer. Nutrients. 2020; 12(2):407. https://doi.org/10.3390/nu12020407
Chicago/Turabian StyleHolma, Reetta, Reijo Laatikainen, Helena Orell, Heikki Joensuu, Katri Peuhkuri, Tuija Poussa, Riitta Korpela, and Pia Österlund. 2020. "Consumption of Lactose, Other FODMAPs and Diarrhoea during Adjuvant 5-Fluorouracil Chemotherapy for Colorectal Cancer" Nutrients 12, no. 2: 407. https://doi.org/10.3390/nu12020407
APA StyleHolma, R., Laatikainen, R., Orell, H., Joensuu, H., Peuhkuri, K., Poussa, T., Korpela, R., & Österlund, P. (2020). Consumption of Lactose, Other FODMAPs and Diarrhoea during Adjuvant 5-Fluorouracil Chemotherapy for Colorectal Cancer. Nutrients, 12(2), 407. https://doi.org/10.3390/nu12020407